
Abstract
Summary
When elderly patients are admitted to a hospital, they may require support from medical social workers during hospitalization. This study examined the association between patient characteristics and support provided by medical social workers in applications for social welfare benefits during hospitalization. We conducted a retrospective observational study of patients aged 65 years or older between October 2018 and September 2021 who had involvement by a medical social worker during their hospitalization at a tertiary care hospital in Japan. We evaluated associations between background factors and support in applying for social welfare benefits by medical social workers using logistic regression analysis.
Findings
Among 485 eligible patients, 79 (16.3%) received support from a medical social worker in an application for social welfare benefits. Early elderly age (65–74 years) and living alone were independently associated with receiving support from medical social workers (adjusted odds ratio [OR] 1.98, 95% confidence interval [CI] 1.16–3.37, P = .012; 3.86, 95% CI 2.26–6.62, P < .001, respectively), regardless of sex, activities of daily living before admission, and presence of a regular doctor.
Application
The findings suggest that early elderly individuals who live alone may not be able to utilize the available welfare benefits and not have adequate support from family members when admitted to a tertiary care hospital, even if they have adequate activities of daily living and a regular doctor. Early intervention to improve social vulnerability may be required for early elderly individuals who live alone.
Introduction
Population aging is a global phenomenon and raises many challenges (United Nations Department of Economic and Social Affairs, 2020; World Health Organization, 2021). Japan is one of the leading countries to deal with population aging as citizens aged over 65 years accounted for 28.4% in 2019 (Ministry of Health Labour and Welfare, 2021). Although there are various medical care policies for the elderly in Japan, including a long-term care insurance system, healthy older people may be poorly prepared for sudden hospitalization and may not be aware of or utilize available welfare programs, resulting in the social vulnerability of the elderly to sudden hospitalization (Ikegami, 2019; Iwagami et al., 2019). A previous study in Sweden showed that one-third of elderly patients hospitalized due to heart failure did not know which healthcare provider to contact in the event that their condition deteriorated after discharge (Säfström et al., 2018). Elderly individuals are particularly vulnerable to emergency hospitalization due to sudden injuries and illnesses when they live alone, which can delay the time of detection and access to medical care. Even with a family member to contact, the quality of support can vary according to proximity and can be influenced by changes in the family structure (Sigurdardottir et al., 2021).
When elderly individuals suddenly suffer a severe injury or illness, they can be brought to the emergency department and hospitalized in the intensive care unit. However, it is often the case that the elderly individual cannot directly return home after the acute phase of their condition; they are often discharged home with a great deal of support or transferred to other facilities (Ferrante et al., 2015; Hartman-Shea et al., 2011; Ringer et al., 2018). In this process, the patient often requires assistance from a medical social worker, to a degree that depends on their surrounding circumstances (Hass et al., 2017). Multidisciplinary care in the emergency department and intensive care unit is increasingly needed to meet various demands in the medical care and welfare of the elderly (Arai et al., 2015; Fan et al., 2015; Rose & Shelton, 2006). Medical social workers in hospitals play an important role in providing patient and family support, and the higher the social vulnerability of elderly patients, the greater the need for support. Previous studies describe the usefulness of support provided by medical social workers for elderly patients treated in the emergency department (Adamson et al., 2020; Puig Campmany et al., 2019).
Although there are several approaches to assessing frailty and multimorbidity, there is a paucity of research on the factors associated with social vulnerability to emergency hospitalization in the elderly (Carpenter et al., 2015; Goldstein et al., 2012; Jørgensen & Brabrand, 2017). Medical social workers at the hospital where this study was conducted have been continuously supporting the discharge and transfer of hospitalized elderly patients for more than 10 years, using empirically developed standardized assessment forms to provide appropriate assistance, including support in the application for available welfare benefits. When patients did not utilize the available welfare benefits before admission, and when they did not have effective support from family members, medical social workers supported them in applying for various social welfare benefits or in managing payments and necessities during hospitalization. Those patients are socially vulnerable to sudden hospitalization. In order to identify the factors associated with social vulnerability in the elderly, we analyzed the patient characteristics and support provided by medical social workers in relation to the application for social welfare benefits and the management of payment and necessities.
Methods
Study design and setting
We conducted a retrospective observational study based on a review of health records. The institutional ethics committee of Osaka University Graduate School of Medicine approved this study. It waived the requirement for informed consent due to the nature of the retrospective chart review, and the data used in this study were anonymized (approval number: 20278).
The study was conducted at the Department of Traumatology and Acute Critical Medicine, Osaka University Graduate School of Medicine, Suita, Osaka, Japan, a tertiary care university hospital with 1,086 total beds and 20 intensive care unit beds dedicated to emergency patients. The emergency department admitted 3,315 patients brought by ambulance or physician-staffed helicopter during the study period (October 2018 to September 2021). Two dedicated medical social workers employed by the hospital are assigned to the emergency department and assist in solving and adjusting the economic, psychological, and social problems that patients and their families face in relation to social welfare in order to facilitate their reintegration into society. These medical social workers play an important role in discharge planning in the department. In this role, they collaborate with physicians, nurses, local government offices, and the community. Medical social workers provide information on available social welfare benefits to patients’ family members in order to address the economic and social problems that should be solved before hospital discharge. If the patient does not have support from family members or the family members cannot proceed to apply for the necessary social welfare benefits or manage payments and necessities, the medical social workers assist the patients.
Community services for elderly people in Japan
Most of the services such as home help and welfare facilities for the elderly are provided under the Act on Social Welfare for the Elderly introduced in 1963 and the Long-Term Care Insurance Act introduced in 2000. There are income restrictions on the use of facilities and services by the Act on Social Welfare for the Elderly because the basic philosophy is to support vulnerable people who need help at public expense. In order to use services under the Long-Term Care Insurance Act, it is necessary to be certified as requiring long-term care with regard to the need for and amount of long-term care, and municipalities are responsible for this service.
In addition to long-term care insurance under the Long-Term Care Insurance Act, there are a variety of other laws and systems that provide safe and secure living and medical support for the elderly. For example, there are high-cost medical expense benefits under the Health Insurance Act, disability certificates under the Act on Mental Health and Welfare for Persons with Mental Disorders or Disabilities and the Act on Welfare of Physically Disabled Persons, adult guardianship under the Civil Code, public assistance under the Public Assistance Act, designed intractable diseases under the Act on Medical Care for Patients with Intractable Diseases, and pensions under the National Pension Act and the Employees’ Pension Insurance Act. Adult guardianship is a legal arrangement where a court-appointed guardian is assigned to make decisions on behalf of an individual who is deemed incapable of making their own decisions due to mental disability. The guardian is responsible for managing the individual's assets, finances, and personal affairs, and ensuring that their rights and best interests are protected. A designated intractable disease is a rare and serious medical condition that has been designated by the government as requiring special medical care and support. Patients with designated intractable diseases are eligible to receive government-funded medical care, financial support, and other types of assistance to help them manage their conditions.
Participants
Patients over 65 years of age who were transported by ambulance to the emergency department and admitted to the hospital from October 2018 to September 2021 and who had any involvement with a medical social worker during their hospitalization were included in this study. Patients who died during hospitalization were excluded from the study because those who died in the hospital cannot receive social welfare benefits.
Variables
We collected information on patient background factors (e.g., age, sex, activities of daily living [ADL] before admission, living conditions [living alone or living with someone], presence of a regular doctor, reason for admission [trauma or nontrauma], having a family member to contact, length of hospital stay, and discharge location [another hospital, home, and nursing home]) from standardized assessment sheets used by medical social workers and from electronic medical records. We categorized age into two groups—early elderly (65–74 years of age) and late-elderly (≥75 years of age)—according to the long-term care insurance classification (Orimo et al., 2006).
Support by medical social workers in applying for available social welfare benefits and in managing payments and necessities during hospitalization due to the unavailability of family support was treated as the outcome of this study. The outcome was binary, which was based on whether the patient had at least one support by medical social workers during hospitalization. This support included an application for long-term care insurance, high-cost medical expense benefits, a disability certificate, adult guardianship, public assistance, a designated intractable disease, pension, other welfare benefits, and other support provided by medical social workers such as management of payment and necessities, looking for a required document, and looking for a family member.
Statistical methods
Continuous variables are presented as the median and interquartile range (IQR), and categorical variables are presented as the number and percentage. We assessed the association between exposures at baseline, including age group, sex, ADL before admission, living condition, and presence of a regular doctor, and the outcome using univariable and multivariable logistic regression analyses and calculated the odds ratios (ORs) and 95% confidence intervals (CIs). All reported P values were two-sided, with P values of <.05 considered to indicate statistical significance. All statistical analyses were conducted using the R software program (version 3.6.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
During the study period, 1,711 elderly patients aged 65 years and older were brought to the emergency department, all of whom were hospitalized, and 529 patients received some form of assistance from a medical social worker. Of these patients, 44 patients who died during hospitalization were excluded. In total, 485 patients were eligible for inclusion in the study (Figure 1).
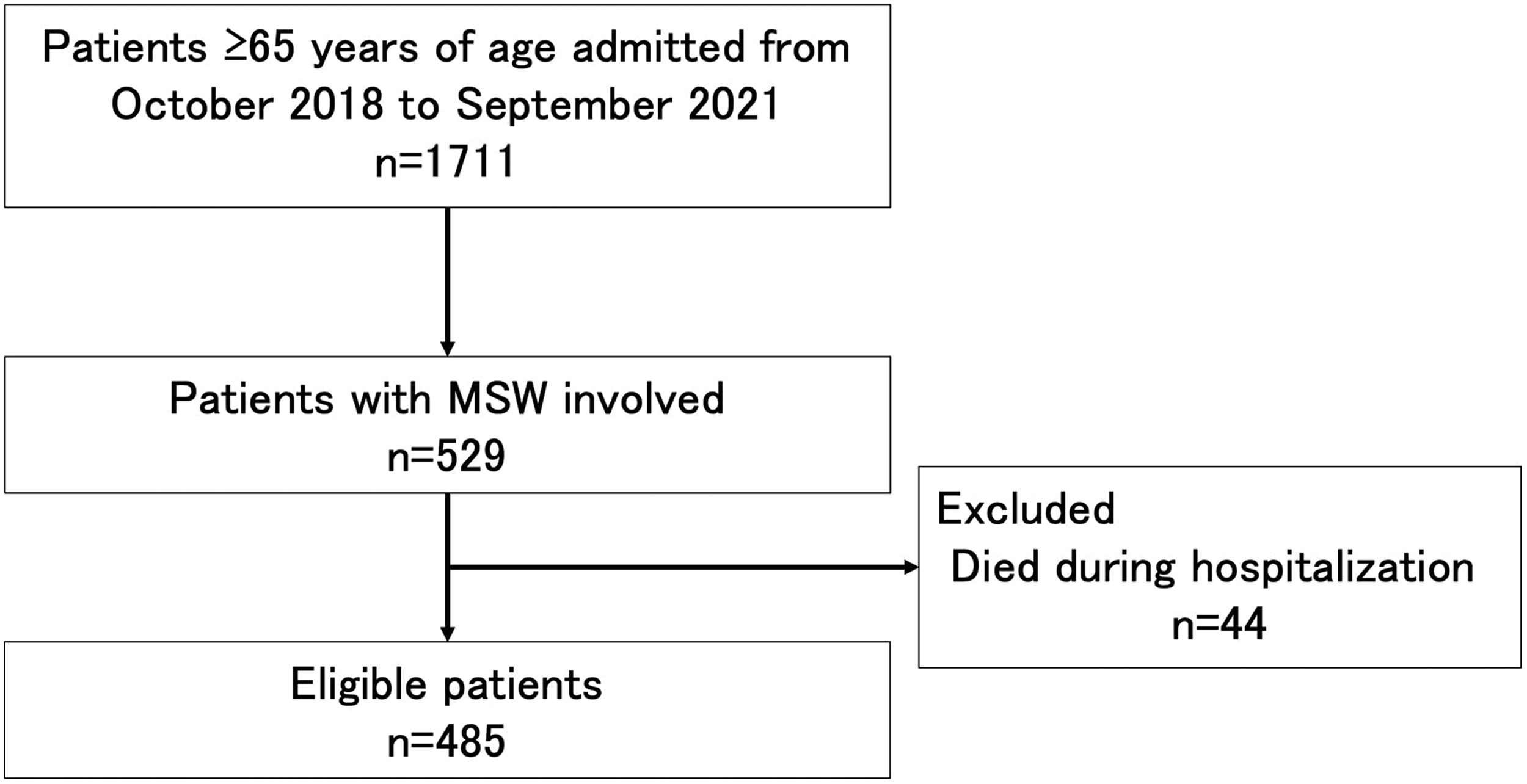
Patient flow.
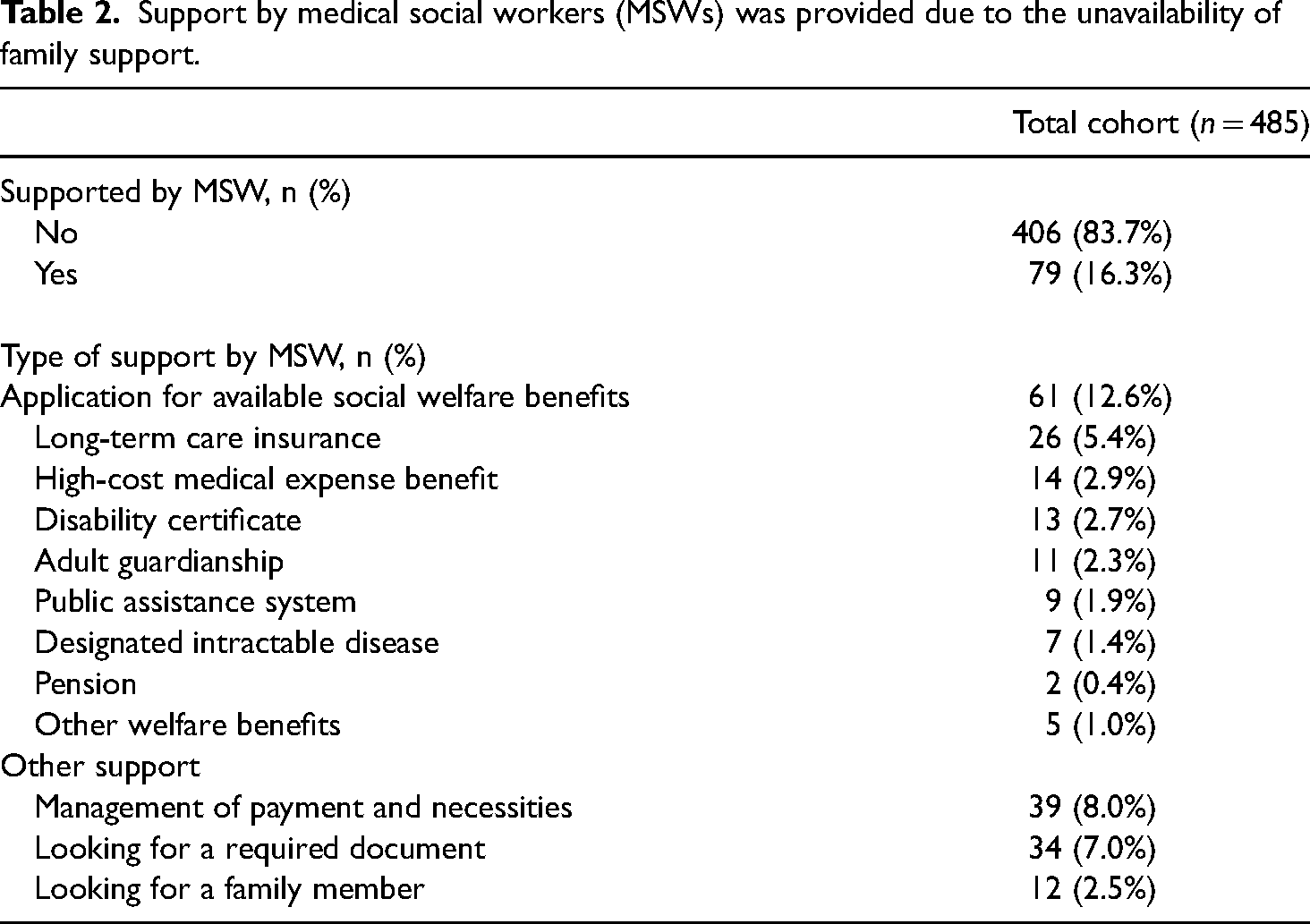
The patient characteristics are displayed in Table 1. The median age was 78 years (IQR 72–84 years); 154 (31.8%) were classified into the early elderly group and 331 (68.2%) were classified into the late-elderly age group. Two hundred eighty-three (58.4%) patients were male. Before admission, 341 (72.8%) were independent in ADL, 104 (21.4%) were living alone, and 459 (94.6%) had a regular doctor. The reason for admission was trauma in 82 cases (16.9%) and nontrauma in 403 cases (83.1%). A family member was available to contact in 473 cases (97.5%), and there were no homeless patients. The median length of hospital stay was 13 days (IQR 4–25 days). The discharge location was another hospital in 422 cases (87.0%), home in 52 cases (10.7%), and a nursing home in 11 cases (2.3%). Support by medical social workers, which was required due to unavailability of family support, was provided to 79 patients (16.3%; Table 2). The medical social workers applied for available social welfare benefits for 61 patients (12.6%). Among these, they most commonly applied for long-term care insurance, followed by high-cost medical expense benefits.
Patient characteristics.
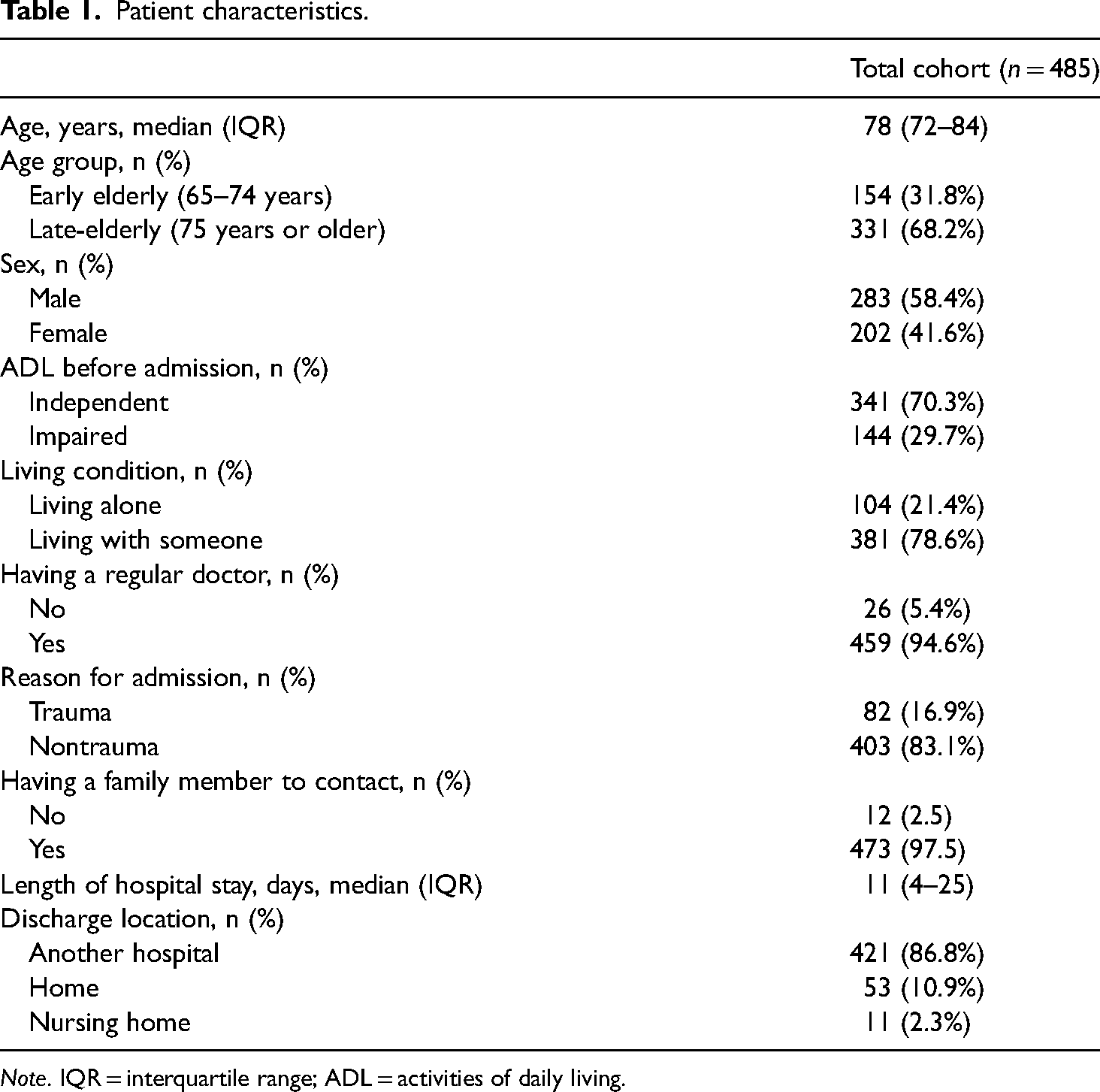
Note. IQR = interquartile range; ADL = activities of daily living.
Support by medical social workers (MSWs) was provided due to the unavailability of family support.
The results of the logistic regression analyses are shown in Table 3. Early elderly age and living alone were independently associated with receiving support from a medical social worker (adjusted OR 1.98, 95% CI 1.16–3.37, P = .012; 3.86, 95% CI 2.26–6.62, P < .001), regardless of sex, ADL before admission, and presence of a regular doctor, respectively.
ORs of each variable for receiving support by MSW among elderly patients.
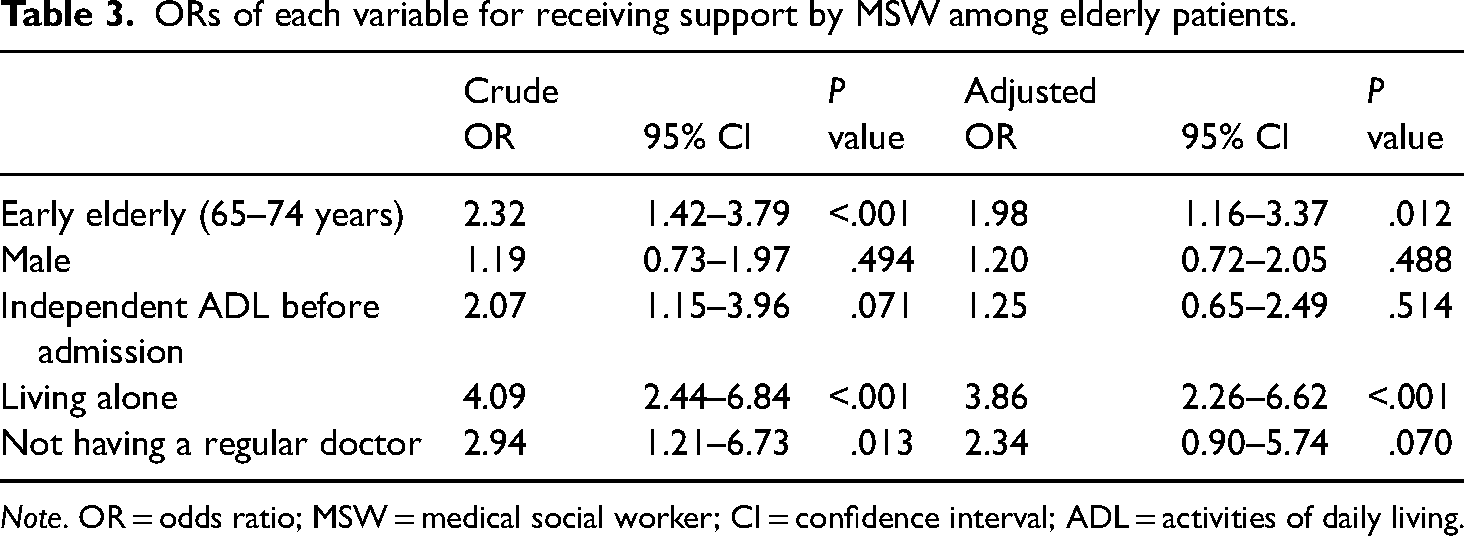
Note. OR = odds ratio; MSW = medical social worker; CI = confidence interval; ADL = activities of daily living.
Discussion
We assessed the support from medical social workers that was required for the application for available social welfare benefits and management of payment and necessities during hospitalization in the elderly who were admitted to a tertiary care hospital in Japan. We found that being early elderly age and living alone were independently associated with the need for medical social worker assistance, regardless of sex, ADL before admission, and the presence of a regular doctor.
According to our results, early elderly age was an independent risk for support from a medical social worker. There are possible reasons as follows: family support may be better prepared for late-elderly individuals, late-elderly individuals may have previously used the available welfare systems, and early elderly age may have been less aware of the available care. Although most patients came to require social welfare benefits because of hospitalization due to serious injury or illness, some patients did not use social welfare benefits that were already available before admission. A report on the underutilization of social services among Japanese family caregivers pointed out the possible influence of concern regarding social appearance, reputation, or dignity in the community or public (Asai & Kameoka, 2005). Further research is needed to clarify the reasons why these patients did not utilize available services.
Living alone was also identified as an independent risk factor in this study, and the negative impact of social isolation has been reported in previous studies (Falvey et al., 2021; Perissinotto et al., 2012; Shah et al., 2022). As noted in the past literature, it is possible that individuals living alone did not look for or did not want to receive assistance (Chan & Hayashi, 2010). Elderly people living alone may need more attention to avoid various emergency conditions and continue to live financially independently (Mudrazija et al., 2020; Yokobori et al., 2020). The findings of the present study seem to be consistent with the previous literature.
The findings of this study may be used to provide advice during interviews with patients and patient families in the hospital about situations that could be improved, which may promote long-term improvement in social vulnerability and reduce the risk of rehospitalization. The findings of the present study could be used in the prehospital setting to address social vulnerability in healthy elderly individuals. A study from the United States reported that placing nurses and social workers in senior housing increased the use of available services and decreased emergency department visits (Nadash et al., 2021). Moreover, community-based support systems in an aging society can improve the quality of life of the elderly. By strengthening social support from the community and the local government for early elderly individuals and elderly individuals who live alone in order to improve their social vulnerability, it may be possible to make the social welfare systems in Japan more effective and promote the health and well-being of the elderly. Population and public health approaches may be essential to address social problems, such as social isolation (Cederbaum et al., 2019). The Long-Term Care Insurance Act in Japan expects local governments to comprehensively support the improvement of healthcare and welfare of local residents by providing necessary assistance to maintain their physical and mental health and secure their lives. Community comprehensive support centers have been established in municipalities since 2005 and their role is to provide professional support in terms of insurance, medical care, and welfare so that elderly people can continue to live healthy and self-sufficient lives for a long time. A chief care manager, public health nurse, and social worker are available at each center to provide professional support, including guidance on various systems and consultation services. The community comprehensive support center provides support to prevent the elderly from needing nursing care.
Japan is one of the most rapidly aging countries in the world and the Japanese government has already implemented innovative policies and solutions, including legislation on support for the elderly. As a report on the epidemiological profile of emergency medical services in Japan showed that 56% of ambulance transports were for patients >65 years of age, our findings may be beneficial for other regions of Japan (Nakao et al., 2020). As the United Nations stated in 2020, well-designed policies to improve the care, living arrangements, and well-being of older individuals are essential in countries with a population aging (United Nations, 2020). Although Japan faces ongoing issues with population aging, our findings may also help other countries with aging populations provide information on potential factors on which they can focus to improve care for the elderly population.
Limitations
The present study was associated with some limitations. First, because it was a single-site study and a small sample size, our findings may not apply to the situation in other regions. They may not be generalizable to other countries, as the social welfare systems may differ. Japanese elderly are reported to have a lower incidence of frailty in comparison to older adults in other countries (Kojima et al., 2017). However, our findings may be helpful in considering how we might reduce the vulnerability of the elderly globally in light of the risks of isolation and the need for early intervention. Second, we analyzed inpatients with medical social worker involvement, which may have introduced a selection bias. However, cases, where medical social workers were not involved, were likely to have had no problems at the time of discharge, which would have had minimal impact on the findings. Third, we could not include some potentially important information such as income, education level, and marital status as variables because the standardized assessment sheet for medical social workers was empirically developed. Further prospective research is needed to evaluate these factors. Furthermore, while our results may apply to critically ill patients transported to a tertiary care hospital, the findings may differ when analyzed in patients with moderate or less severe conditions.
Conclusion
Among the elderly patients admitted to a tertiary care hospital and who were involved with medical social workers, early elderly age and living alone were factors associated with receiving support from medical social workers in applying for social welfare benefits during hospitalization, regardless of sex, ADL before admission, and the presence of a regular doctor. Early intervention to improve social vulnerability might be necessary for the early elderly and elderly individuals who live alone.
Footnotes
Ethics
Ethical approval for this project was given by the Osaka University Graduate School of Medicine (reference number: 20278).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nissei Foundation (grant number N/A).
Authors’ contribution
SN conceived the study. SN, YF, and YT structured the methods and participated in the data collection and statistical analysis. SN prepared the manuscript. SN, YF, YT, HO, and JO performed the data interpretation. All authors critically reviewed and approved the final version of the manuscript.
Acknowledgements
The authors thank Dr. Chihiro Tada and Mr. Kaito Takazoe for their assistance in data collection.