
Abstract
The quality and robustness of childcare professionals’ thinking about protective factors is crucial to interventions with vulnerable children. Yet, protective factors in childcare are under-conceptualized in policy and practice and have been overshadowed by the concept of risk. This study uses discourse analysis to examine how childcare professionals discuss protective factors in response to risk and in a way that demonstrates critical thinking. Findings Data was collected from 30 consultation meetings, which involve a total of 109 professionals. The consultation meetings focus on the assessment of a child who presents a serious risk of harm to others and who are themselves at risk. The findings suggest that professionals do discuss protective factors in response to risk, however, it occurs on a ratio of approximately one to nine, which suggests a level of separation in the way these terms are conceptualized in practice. Application It is suggested that a professional construct of “protective factors versus risk,” which is applied with critical thinking, will offer a more robust way of conceptualizing the support provided to vulnerable children. While professionals have to analyze risk in terms of what is wrong, it is equally crucial to include protective factors in a strategy for it to work. A starting point is for professionals to re-construct protective factors and risk and apply it with critical thinking to core elements of social work practice, such as assessments, multi-disciplinary meetings and the verbal communications with service users.
Introduction
Given the paramount importance of children's safety and well-being any meaningful understanding and application of protective factors in childcare requires professionals to utilize critical thinking skills (Brandon et al., 2008; Turney & Ruch, 2016). Despite the value attributed to examining the way social workers think in their day-to-day work (White, 2009) there remains considerable uncertainty about the quality of professionals’ thinking in relation to protective factors. This study examines the way childcare professionals discuss protective factors in response to risk and in a way that demonstrates critical thinking. This has relevance for childcare interventions in terms of the way professionals make decisions and judgments while trying to reduce errors that might result in catastrophic consequences for vulnerable children. To date, much of the literature on protective factors adopts a broad-based approach whereby changes to the individual child, family, and community are options when reducing risk to the child or other people (David-Ferdon et al., 2016). While this serves to highlight the wide-ranging factors involved when protecting children, there is an absence of research from a practice context demonstrating the nature of professionals’ critical thinking in relation to protective factors. This gap in understanding reflects a wider practice issue. According to Sheppard et al. (2018), social work has focused on an evidence base around knowledge content with insufficient attention afforded to the cognitive processes involved in the application of such knowledge. This is of some concern given the longstanding criticisms about the quality of childcare practice, especially the ability of professionals to protect children (Saltiel, 2016). While the study is conducted in Scotland, its focus on protective factors and the quality of professionals’ thinking will be of relevance across the United Kingdom (UK) and internationally in welfare systems that have a responsibility for child care and protection.
Understanding protective factors in response to risk
Any analysis of protective factors has to recognize the different national and international influences that exist across a country's child welfare systems. Childcare systems are a product of a society's history, culture, and response to priorities about children (Freymond & Cameron, 2006). This creates a changing context in which protective factors are located. For example, a comparative study by Gilbert et al. (2011) of 10 countries over a 15-year period found the child welfare systems oscillate between “child protection,” “family services,” and “child focused” orientations depending on the relationship between the child, family, and the nation-state. Within this broader and changing context, professionals have to apply protective factors in response to the risk experienced by vulnerable children (Munro, 2010).
Applying protective factors to children who pose a serious threat of harm to others requires practitioners to balance the child's vulnerability and underlying problems (e.g. attachment issues, trauma) with controls and sanctions that manage the risk generated by the child (Barter, 2013). For Baker (2008, p. 1475) an integral feature of this process is for practitioners to understand the “multidimensional nature of the risks” in the assessment and intervention with children who harm others, whereby risk can have negative and positive consequences. The way professionals perceive and understand risk will influence, at least to some extent, their choice of protective factors. Protective factors are defined as one or more variables that “act as a buffer to the negative effects of adverse experiences” (Daniel et al., 2010, p. 105). The buffering effect of protective factors has been shown to reduce risks for children and enhance resilience (Sattler & Font, 2018) and having more protective factors are predictive of better outcomes (Evans et al., 2010). Protective factors are also best understood within an ecological approach in that they operate at the level of the individual (e.g. high self-esteem), peers (e.g. kind friends), family (e.g. loving parents), school (e.g. supportive teachers), and wider community (e.g. poverty reduction strategies) (Hawkins et al., 1995; Luthar et al., 2015). The relevance of these levels is supported by a variety of research studies (e.g. Timshel et al., 2017), however, it is unclear how childcare professionals think about and discuss the most suitable protective factors for children who pose a serious threat to others. Wilkins (2015) study uses vignettes and found social workers have difficulty identifying protective factors and their understanding is much less sophisticated compared to risk. Issues highlighted in these findings are reflected in a series of high-profile inquiries in the UK where the failure to protect children has been identified (Turney & Ruch, 2016). While there are rarely simple solutions to protecting vulnerable children, Gray and Schubert (2013) point to the growing level of interest in the thinking and reasoning used by practitioners and how they conceptualize childcare cases. The current study aims to contribute to this important area by examining the way professionals demonstrate critical thinking when applying protective factors in response to risk.
Critical thinking is regarded as a highly desirable process of practical reasoning for social work (Sheppard, 2006) and essential for professionals to make the best quality decisions in complex situations (Brown & Rutter, 2008). It therefore seems plausible that critical thinking is important for practitioners when applying protective factors in response to risk, especially in minimizing errors of judgment and ensuring children's safety. Critical thinking is however, an elusive concept and Taylor and White (2001) remind us that it is influenced by a range of individual and situational factors in practice. Kuhn's (1991, p. 4) definition of critical thinking embodies reasoned argument and is “a process of weighing pros and cons or positive and negative evidence regarding alternatives has at some level of consciousness gone into an argument.” A study specific to social work by Sheppard et al. (2018) also emphasizes the “conscious” and “deliberative” nature of critical thinking as being distinct from more intuitive or heuristic forms of thinking. The distinction between these types of thinking is important for understanding the choice and application of protective factors in a practice context. Studies by Taylor (2017) and Whittaker (2018) show that heuristics and intuition are compatible with critical thinking, however, Helm (2011) found that social workers are more ready to utilize the former over the latter. This is problematic because the spontaneous and automatic aspects of intuitive and heuristic thinking are more prone to errors, particularly in terms of practitioners’ tendency to focus on the familiar and obvious rather than more complex and unpredictable elements of practice (Gambrill, 2012). Examining protective factors in terms of the way professionals demonstrate critical thinking provides insight into the robustness of their reasoning when discussing children who pose a serious threat to others.
Methodology
The study examines data from a project based in Scotland that provides a psychological and social work service for the assessment and management of children who pose a serious risk of harm to other people. The project offers a range of services, however this study focuses on the consultation meetings (hereafter, referred to as meetings) that contribute to the assessment and intervention strategies of those professionals who are working directly with the children. Although the project operates out with mainstream social services, the meetings are relevant to social work practice because the staff attending are employed mainly in social work, health and education. Further relevance for social work is apparent in (1) the children being discussed have previous and/or ongoing social work intervention due to experiences of abuse and neglect; (2) most of the children have been removed from their family home and are under the care of the local authority; and, (3) the harm the children present to other people often includes children, which requires child care and protection. While risk has both positive and negative dimensions, its concern for social work links primarily to harm, likelihood, reduction, and prevention (Hardy, 2017). Given children are referred to the project because of the risk of harm they present to others, this study focuses only on the negative dimension of risk when examining protective factors. By focusing on the discussions of professionals in the meetings the study aims to examine the:
extent to which protective factors are discussed in response to risk and patterns of critical thinking demonstrated by professionals when discussing protective factors.
Data is collected from 30 meetings. Approximately 200 meetings have taken place over a five-year period with more frequent referrals for boys (86%) than girls (14%). The meetings are scheduled for a duration of two hours and are audio recorded. Purposive sampling is used to randomly select 15 females and 15 males for this study. The audio recording for each child's meeting is stored digitally in a file. The researchers randomly select files until they have a list of 15 boys and 15 girls. Although the number of girls selected is disproportionate to the higher referral rate of boys, it allows for gender issues to be considered in relation to protective factors. Referrals to the project are accepted for children aged between 12 and 18 years and each meeting focuses on one child. Almost all of the children's ethnicity was white and one child had Asian ethnicity.
There is a total of 109 professionals involved in the 30 meetings: 99 have direct involvement with the children and 10 are project staff. While those attending the meetings are from various professions there is no attempt to differentiate between professional groups when examining the data. As such, the professionals are not part of any selection process and their involvement in the study arises from the selection of the 30 children. Many of the professionals in the project appear in several of the meetings, whereas those who have direct involvement with a child appear in only one meeting. The meetings comprise of between three and nine professionals. There are usually three professionals attending the project, comprising of at least one social worker and one psychologist, and two or more professionals who are seeking the consultation (i.e. social worker, residential worker, teacher, psychologist, police officer, psychiatrist, and nurse). Social workers and psychologists are the most commonly represented professionals at each meeting. Although service user involvement and participation in social work has been a significant theme for over two decades (D’Cruz & Gillingham, 2017), there are no children or family members attending the meetings. The rationale for excluding service users is to create a forum where professionals are more able to be open about their feelings, honest about mistakes, and openly challenge each other. Analyzing 30 meetings appears to allow for data saturation to be reached using the criteria cited in qualitative studies (e.g. Fusch & Ness, 2015): the study can be replicated; patterns of data are established prior to all of the meetings being analyzed; and, the coding used in the study is applicable and relevant. The study adheres to internationally accepted ethical guidelines and is approved by the University Ethics Committee. All of the professionals attending the meeting gave consent for interviews to be used for research purposes. All names have been changed to protect those individuals discussed at the meetings and those professionals taking part.
Discourse analysis is used to examine the way childcare professionals discuss protective factors in response to risk. A discourse analysis enables written or verbal language to be analyzed in relation to the context in which it is used (Hardy et al., 2004). There is no single definition or approach to using discourse analysis, however, Potter's (1996) approach is of value given its emphasis on the socially constructed and interpretative nature of concepts, which is relevant to protective factors, risk, and critical thinking. A particular feature of discourse analysis is in enabling coding to show the frequency and patterns in the way language is used between speakers (Crawford, 2004). In order to examine professionals’ discourse, Maclellan and Soden's (2001) framework of critical thinking is used because it offers a concise set of categories for coding. Although various other frameworks and approaches (see for example Barnett, 1997) might provide a more comprehensive understanding of critical thinking they are not readily applicable or adaptable for a practical study. There are six categories to Maclellan and Soden's (2001) framework of critical thinking:
unpacking concepts—ability to unpack or break down ideas, concepts, or theories; recognizing contradictions—differentiating between viewpoints and counterarguments; development—explaining a phenomenon, joining ideas together to form lines of arguments; providing evidence—supporting or justifying assertions; examining implications of evidence—generating hypotheses about consequences and examining the relationships between key factors; and alternative interpretation—questioning or challenging an interpretation of the evidence and offering an alternative.
The framework was devised to identify critical thinking in student assignments, however, the generic nature of the categories means they can be applied to key concepts such as protective factors. This does involve an assumption that categories used for examining students’ thinking and written work are suitable for examining professionals’ discussions about important matters such as protective factors within a practice context. Using a framework of critical thinking will hopefully allow for a broader exploration of the topic and while it is recognized that one or more categories do not necessarily demonstrate critical thinking per se, each category contributes to the way professionals think and reason about protective factors.
The harm generated by the children allows for four key domains to be examined. This involves instances where harm has occurred or is likely to occur and where it relates to the children or other people. These four domains are used to examine the way professionals discuss protective factors.
Risk of harm—the protective factors that are discussed when there is a chance or likelihood of harm occurring in the future. Actual harm—the protective factors that are discussed following the occurrence of harm. Children—those protective factors relating specifically to the 30 children who are the focus of the meetings. Other people—those protective factors relating to any other adults or children in the community.
The four domains of “risk of harm,” “actual harm,” “children,” and “other people” are examined in relation to the six categories of critical thinking, providing 24 permutations for coding protective factors. This allows for comparisons to be made in the way professionals discuss protective factors across each of the domains and the extent to which critical thinking is applied. This is important because it allows us to know how protective factors are discussed when there is a risk of harm compared to actual harm and whether it is linked to the children in the study or other people in the community. The researchers use the 24 permutations to devise a matrix to code protective factors and critical thinking for the meetings. The audio recording for each meeting is listened to by the researchers and the data from the 30 matrices are compiled. Protective factors are, as previously stated, any actions that act as a buffer to the risks generated and/or experienced by a child. The protective factors can be applied to the child or any other individual, group, or community who is affected by the risk or who has a role in its reduction/management. Protective factors are coded using the following process: (1) when a protective factor is discussed in response to risk it is coded in relation to the six categories of critical thinking; (2) the coding differentiates between protective factors for the children and other people; and, (3) there is further differentiation in the coding between the risk of harm and actual harm. The coding from the 30 matrices is compiled and analyzed.
A particular limitation of this methodology is that the categories of protective factors and critical thinking are imposed and interpreted by the researchers in ways which may not fully encapsulate the intended meanings of those attending the meetings. Analyzing protective factors only in response to the negative dimension of risk is limited because the study ignores the way protective factors can be applied to support positive risk-taking, which is more in alignment with a strength-based approach. There is also a level of subjectivity and judgment involved when coding and conveying specific data to the reader. Differences in coding are reviewed by both researchers as a means of enhancing reliability. Where the same protective factors are discussed at various points in the meeting, it is coded only once. Given the professionals did not know the recordings would be examined in relation to protective factors, there is no obvious bias which might influence the nature of their thinking and discussion. Finally, there is no consideration of the differences that exist between professions (e.g. status, identity, power, and confidence) and how these aspects might impact the discussion of protective factors.
Results
Findings from the discourse analysis show that protective factors are discussed in response to risk in ways that differentiate between the risk of harm and actual harm and in relation to the child or other people. This application of protective factors in a practice context is reassuring in that professionals are able to differentiate between important aspects when responding to risk. However, the frequency of protective factors compared to risk is considerably lower. There was a total of 1,187 instances of critical thinking about risk and protective factors in the 30 meetings: 1,050 (88.4%) instances related to risk and 137 (11.6%) instances related to protective factors. This shows that professionals discuss protective factors in response to risk in a way that demonstrates critical thinking in a ratio of approximately one to nine. The instances of critical thinking are highest for actual harm (n: 612, 51.5%) than the risk of harm (n: 438, 37%) with protective factors being considerably lower (n:137, 11.5%). Hence, within a practice context, the overwhelming majority of risks discussed by professionals about vulnerable children are not linked to protective factors, even where most of the risk refers to actual harm.
A comparison between the children and other people shows further differences in terms of the frequencies of protective factors and risk (Figure 1).
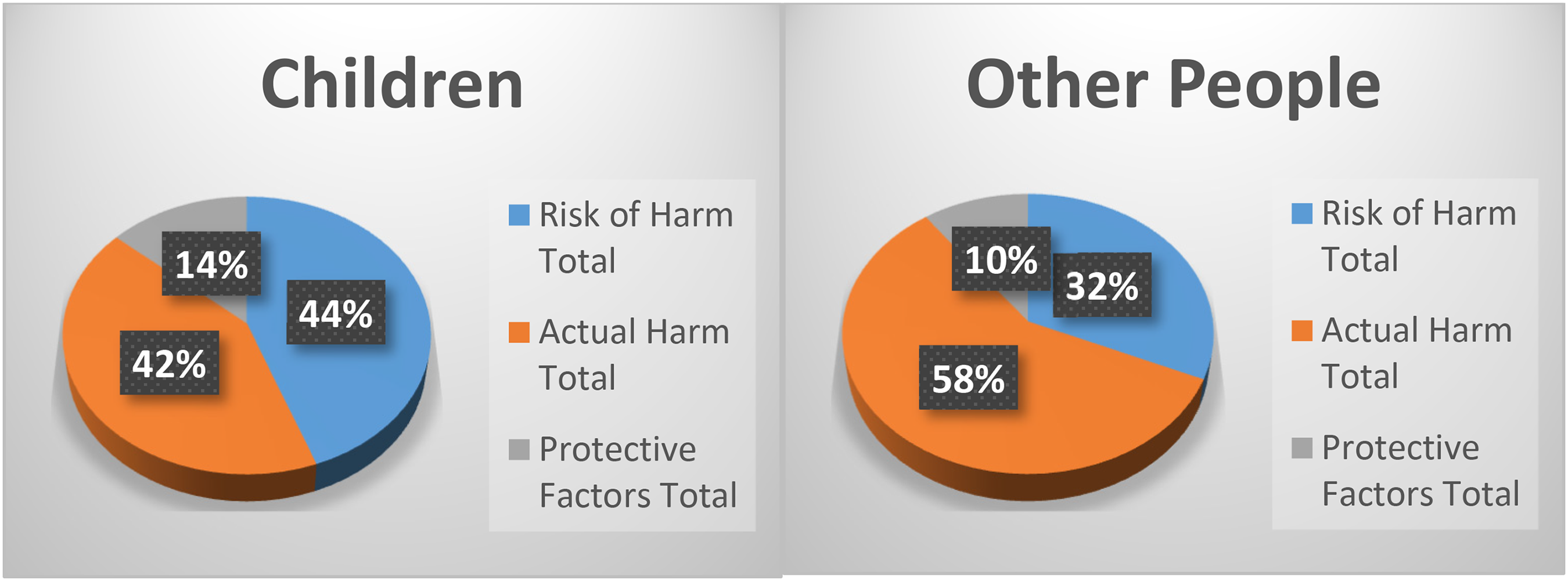
Frequency of protective factors, risk of harm, and actual harm and in relation to the children or other people.
Critical thinking is demonstrated for the children with a similar frequency between the risk of harm (n: 219, 44%) and actual harm (n: 208, 42%) with much fewer instances of protective factors (n: 67, 14%). In relation to other people, critical thinking is more frequent for actual harm (n: 404, 58%) than the risk of harm (219, 32%) and again, with much fewer instances for protective factors (n: 70, 10%). This suggests that protective factors are seldom discussed in response to the risk of harm or actual harm either in relation to the children or other people in ways that demonstrate critical thinking. Of the 30 meetings in this study, 22 had at least one category of critical thinking that demonstrated a protective factor in relation to a risk to the child or other people. However, given there were no categories of critical thinking demonstrated for eight children (four girls and four boys) it does raise questions about the quality or standard of thinking about protective factors, especially when these children are considered to present a serious threat to other people.
In terms of gender, protective factors are discussed more frequently for boys (n: 77) than girls (n: 60). This gender difference is more apparent when the risk relates to other people with protective factors for boys (n: 57) more frequent than girls (n: 13). This might reflect the higher risk that boys present to other people (e.g. physical assaults, sexual violence). In contrast, where the risk relates to the children, protective factors are more likely to be demonstrated for girls (n: 47) than boys (n: 20). This might reflect the higher risk that girls present to themselves both in terms of their own actions (e.g. self-harming, drug misuse) and danger from other people (e.g. sexual abuse). Overall, protective factors are seldom linked to risk in ways that demonstrate critical thinking, however, when they are discussed by professionals it is more likely to relate to the harm boys cause other people.
In order to examine protective factors and critical thinking in more detail, extracts are selected from the discussions at the meetings. Figure 2 shows the frequency of the six categories of critical thinking in relation to protective factors for children and other people.
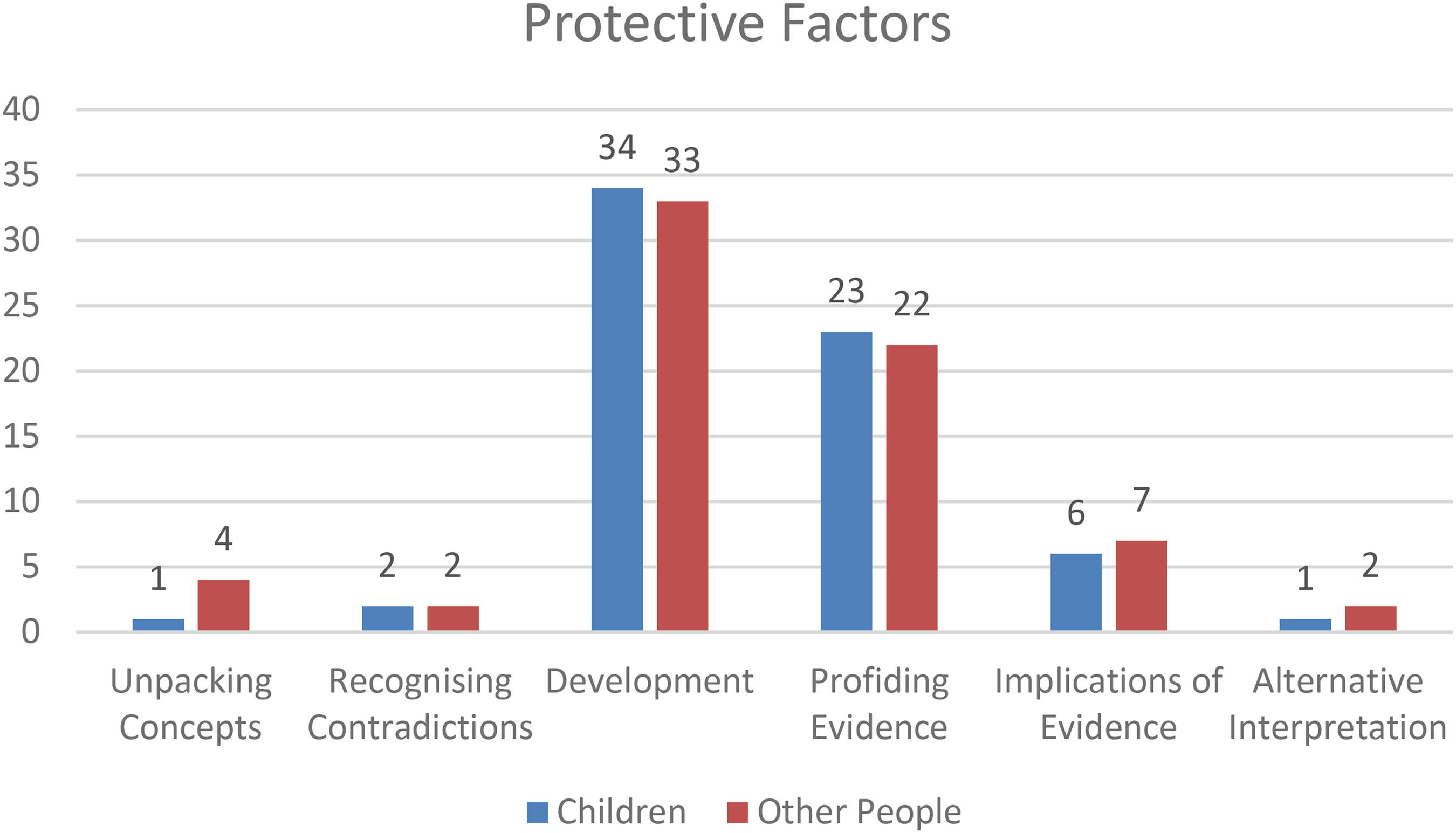
Instances of protective factors and categories of critical thinking.
The categories of critical thinking for the 137 instances of protective factors are presented in order of frequency (high to low). Critical thinking about protective factors is most frequent for the category of “development” (n: 67) with protective factors for children (n: 34) only slightly more frequent for other people (n: 33). In the following example, the category of development is demonstrated in relation to a protective factor, which comprises of the supervision of Paul (15 years) who is in residential care and has a history of sexual abuse towards younger children.
Psychologist: generally, there has been a reduction in problematic behavior, apart from the time in July. Residential worker: he has not had the opportunity. Residential manager: he is essentially a prisoner in the house supervised 24/7. Social worker: that's what you are meaning when you say you’ve not had the opportunity to test it out [self-control]. Everything is about containment.
The critical thinking demonstrated in this extract explains the link between supervision as a protective factor and the extent to which it might be linked to Paul's self-control and associated reduction in problematic behavior. The category of development is demonstrated in each of the 22 meetings. This suggests professionals are able or willing to explain a phenomenon and join ideas together to form an argument in relation to at least one protective factor with the majority of children. It also suggests that the category of development might be a precursor or link for other categories of critical thinking to be demonstrated when professionals consider protective factors.
The category of “providing evidence”’ (n: 45) has protective factors for children (n: 23) slightly more frequent than for other people (n: 22). The category of providing evidence generally follows from the category of development when the discussion explores an issue in more depth. The following extract is about Cathy (13 years) who is in residential care and displays emotional outbursts and violence, including assaults with a knife on police officers.
Residential worker: whenever things are really tough with Cathy we all try to put ice-skating in place for her. It's the one thing we can get her to go and do that can maybe bring her back down again. It boosts her self-esteem … because she is really good at ice-skating.
The category of providing evidence relates to the effectiveness of sport within an anger management strategy for Cathy. The importance of this category is in providing concrete and verifiable information about the protective factor. The category of providing evidence is apparent in two-thirds (67%) of those occasions where the category of development is demonstrated. This is clearly positive and the evidence usually refers to certain behaviors or actions in relation to a single protective factor, however, it is not linked to other protective factors or a broader method of intervention.
The category of “implications of evidence” (n: 13) is demonstrated for protective factors slightly more often for other people (n: 7) than the children (n: 6) and occurs less than one-third of those instances where the category of evidence is demonstrated. This suggests that when professionals present evidence they are much less likely to hypothesize and consider any consequences when discussing protective factors. To illustrate, Susan (17 years) has recently left residential care and is homeless and the social worker considers the implications of evidence in terms of existing protective factors and the reasons why Susan does not want to go to prison. Social Worker: she said to me on a number of occasions, ‘is there males in prison?’ I said ‘no’. She has put herself in the middle of a circle of male friends that protect her. So if she gets into an argument with a female, then she just has to phone her crew. They come and protect her. So therefore, she feels untouchable … That's the reason she doesn’t want to go to prison.
While Susan uses men as a protective factor in certain areas of her life, the implications are extremely damaging. Discussing the implications of evidence allows the social worker to hypothesize about the consequences of Susan's actions and examine the relationship between protective factors and her criminal activity. Interpreting and explaining the implications of evidence might be considered a key professional activity, yet it is not a frequent occurrence when protective factors are discussed.
The remaining three categories of critical thinking are demonstrated in discussions about protective factors much less frequently: unpacking concepts (n: 5), alternative explanations (n: 3) and recognizing contradictions (n: 4). Yet, on the few occasions where these categories are demonstrated they provide important information about protective factors. Subsequently, an example of each category is presented. The category of “unpacking concepts” is more likely to be demonstrated for other people (n: 4) than the children (n: 1). The following extract illustrates this category of critical thinking in relation to Anne's (14 years) “controlling” behavior.
Social worker: when she went into the unit [residential home] at first staff were trying to be firm with her. Then staff really struggled to deal with her behavior and there were communication problems and staff started to give into her and let her away with things.
Residential worker: This is the behaviors that we were seeing. That whole control thing. When she was admitted, she wasn’t in control of anything, but then she got to rule the roost. She was refusing to deal with basic grade staff and only deal with management. And they were allowing that …. It's not going to work, it's going to end in tears. I often think the behaviors she displays are down to withdrawal. She is withdrawing [from drugs].
Senior social worker: She certainly has a gift in replicating the dynamics in her home life wherever she goes. If she is constantly trying to control situations, what is she getting from that?
Unpacking the term “control” gives additional knowledge about the way Anne deals with those who try to protect and care for her. It also shows the complexity of Anne's behaviors, especially when she is violent and aggressive, and the problems staff have in providing a consistent approach across the team. The category of unpacking concepts is therefore, useful in ensuring a more in-depth understanding exists between professionals when using specific terminology.
The category of “recognizing contradictions” is demonstrated when discussing protective factors on only a few occasions (n: 4) with the frequency to other people (n: 2) the same as the children (n: 2). An extract in relation to Martin (14 years) shows a response by a psychologist to the teachers’ concern about his threats of violence and that he will do something “serious.”
Psychologist: there is a real issue in this particular case which I don’t see very often, but it is an organizational, policy, procedure and education issue that needs to empower staff …. If I’m being really blunt about it, the system is acting in a way that there is a self-fulfilling prophecy here with this boy. I think potentially the system is compounding the risk…. These are really difficult discussions to have, because the easy thing is to pathologise the child.
The category of recognizing contradictions helps to convey inherent tensions where protective factors might be formulated by professionals in relation to risk with the best intentions, but can be ineffective or indeed damaging. Differences of opinion between professionals are often a positive feature of assessment, especially in illuminating a range of perspectives, however, such difference may be particularly problematic when it manifests as a contradiction or limitation in the intervention process, especially when protective factors are concerned.
The category of “alternative explanations” is demonstrated when discussing protective factors on only a few occasions (n: 3) and slightly more with other people (n: 2) than for the children (n: 1). An extract in relation to Joseph (15 years), whom the social worker suspects of having suffered from sexual abuse and parental neglect and who has also alleged to have sexually abused another child, shows an alternative explanation for his “immaturity.”
Social worker: he tends to gravitate to younger kids, especially younger girls…. When he was 14 he would say that he was going out with an 11 year old, but to be fair Joseph would be like an 11 year old. For him it would be someone at his maturity level …
Psychologist: there is part of me wondering if he has just regressed and it is quite healthy (when playing alone with toys), so you might want to leave him regressed and let him come at his own pace. The other question I have to ask, is there a cognitive impairment?
The alternative explanation of his immaturity in relation to protective factors highlights the complexities around managing risk and supporting a child's healthy development. The discussion of Joseph's immaturity as a developmental delay shows that no specific intervention is necessary because the child is able to overcome the difficulties within a safe and nurturing environment. In contrast, an assessment which shows a cognitive impairment might warrant intervention in the form of additional support. The tension for professionals is how to respond to the immaturity of a 15-year-old boy who wants to play with 11-year-old girls, especially when concerns exist about his sexual abuse as a victim and perpetrator. The different perspectives that might lead to contradictions are also essential to alternative explanations when examining complex issues relating to protecting children. The task for professionals is to allow for alternative explanations while reducing contradictions around protective factors.
Overall, protective factors are discussed in response to risk in ways that often differentiate between risk of harm and actual harm and in relation to the child or other people. This is positive and suggests that professionals are selective in the application of protective factors. The variation in frequency of the categories of critical thinking also suggests that some categories are more relevant, easier to apply or a relatively narrow conceptualization of critical thinking about protective factors prevails in a practice context. Given the children were referred to the project because of the serious threat they present to other people, it is concerning that protective factors and risk are discussed in a ratio of approximately one to nine, and one-quarter of the children are discussed with no protective factors specific to risk to themselves or other people.
Discussion
The findings in this study suggest the “imbalance” between protective factors and risk as shown by Wilkin's (2015) study using vignettes might be more acute and perhaps akin to a “separation” when examined in a practice context. Given the meetings are attended by a range of professionals, it also appears that social workers are not alone in having difficulty identifying and conceptualizing protective factors in response to risk. It is not clear from this study why professionals seldom discuss protective factors with children who present a serious threat to others, however, it is likely to limit their understanding of the reality and complexity of issues when intervening in the children's lives, thereby reducing the need for critical thinking.
A way of addressing this separation is for professionals to conceptualize protective factors and risk as opposing sides of the same construct. George Kelly's (1955/1991) Personal Construct Psychology (PCP) offers a way for professionals to re-conceptualize risk and protective factors and in a way that enhances the potential for critical thinking. While PCP has been given little attention in social work, Butt and Parton (2005) argue that it is ideally suited to helping professionals understand the complexities of theory and practice. PCP is a constructivist theory that aims to show how an individual's personal constructs provide a lens to anticipate, construe and predict events around them and which determine his/her behavior, thoughts, and feelings. This has clear relevance for the way practitioners understand protective factors in response to risk, especially when personal constructs are cognitive dimensions that are formed by two opposite poles (e.g. strong–weak, happy–sad), neither of which can be understood in isolation from the other. While constructs are personal, Kelly's “sociality corollary” is a recognition of the need to move beyond the individual and understand constructs in groups or social settings, including those used by professionals in their capacity to help clients. A professional construct of “protective factors versus risk” provides a more robust way of connecting these concepts in practice both for the individual practitioner and in discussion with others. Firstly, an assessment of risk does not in itself keep children safe (e.g. Warner, 2003), hence it is not always pragmatic for risk to be the starting point for an assessment or be conceptualized separately from protective factors in a childcare context. Secondly, the identification and categorization of risk as a mechanism for rationing limited resources (e.g. Wilkins, 2015) serve an organizational and bureaucratic need which deprioritizes protective factors and increases the likelihood of children being perceived as overly vulnerable and/or dangerous. Hence, this construct is not merely an attempt to establish a link between these two concepts, it emerges from a recognition that as poles on either side of a construct, neither protective factors nor risk can be understood in isolation from the other.
A professional construct of protective factors versus risk will offer a greater level of sophistication in childcare where critical thinking is applied (Diagram 1).
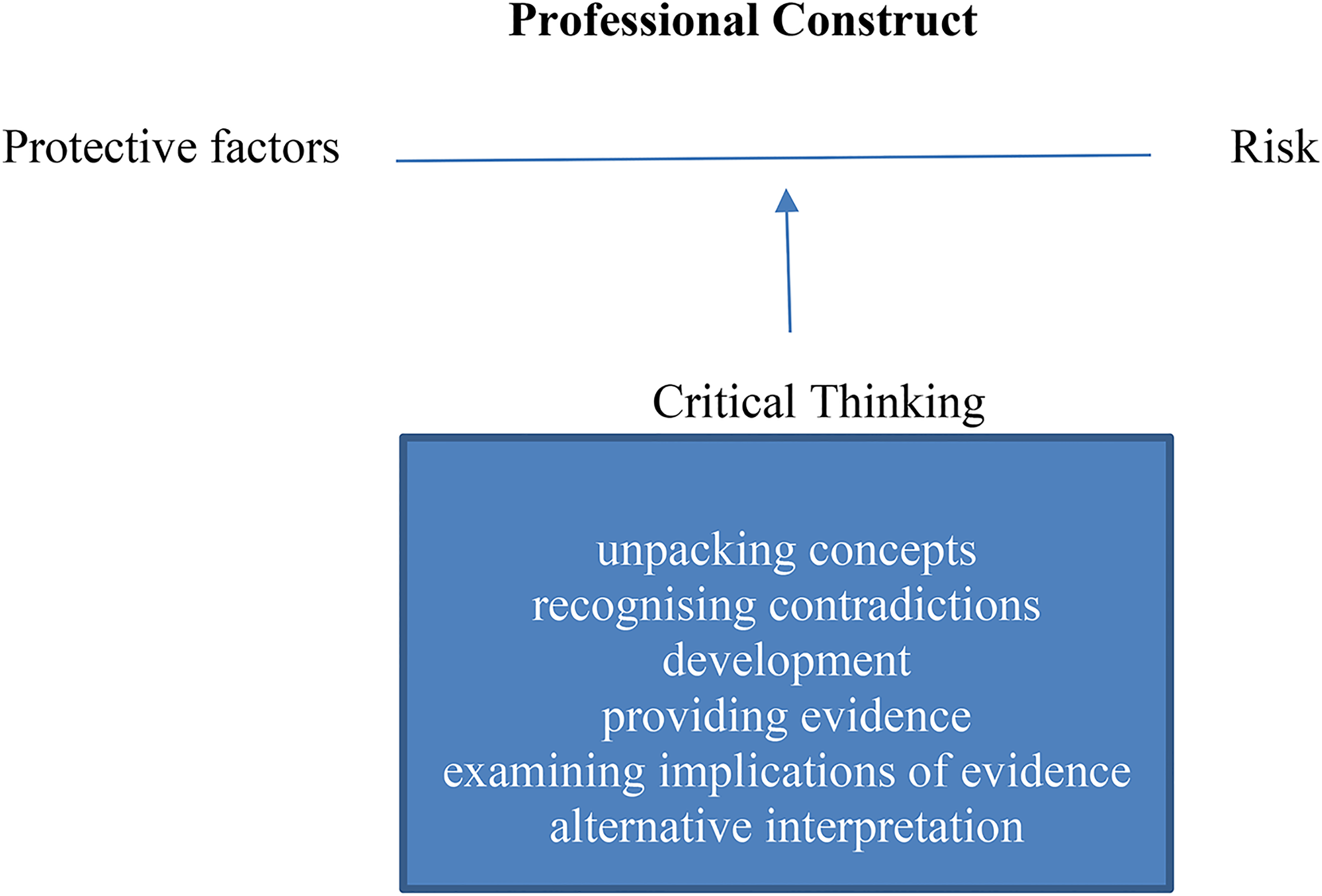
Protective factors and risk as a construct with the application of critical thinking.
In a childcare context, professionals should commence with discussions of the protective factors that exist for a child. This aligns more readily with a strength-based approach (e.g. Saleebey, 2002) which recognizes the variety of supports required for healthy development, rather than perceiving a child predominately in terms of risk. Giving greater parity of thinking between protective factors and risk will also help to address the separation of these concepts. Where professionals are unable or unwilling to commence with a focus on protective factors, they should at least mirror their critical thinking between risk and protective factors. Therefore, when critical thinking about risk is demonstrated by the categories of, for example, development and providing evidence, practitioners should consider protective factors in terms of the same categories. Of course, this is not to suggest that professionals should never have any discussion of risk, or use personal constructs (e.g. low risk–high risk) without discussing protective factors. Neither is it being suggested that the assessment or intervention should be understood from a PCP approach. What is being suggested is that a professional construct of protective factors versus risk offers a useful way to conceptualize a key aspect of childcare that has the potential to enhance the quality of practice.
Limitations
Some caution is necessary when making generalizations from a small-scale study, especially when it focuses on a specific service user group. The children discussed in the meetings are deemed to present a serious threat to other people, hence the demonstration of protective factors might be different (e.g. more readily identifiable) for individuals who are considered lower risk. The framework of critical thinking is sufficiently detailed to provide an insight into the way different categories are applied to protective factors, however, the extent to which any category actually demonstrates critical thinking or results in better outcomes for children remains unclear. Research using other models or frameworks will add a more robust insight into the value of critical thinking within a practice context. Furthermore, there is no attempt to examine factors such as gender and ethnicity in terms of the way professionals discuss protective factors, and this will be an important consideration for future research.
Conclusion
While risk is an essential construct for childcare practice, it may be constrained when discussed in isolation from protective factors. Policy and practice in social work must strive to ensure that both risk and protective factors are connected when assessing vulnerable children, otherwise the efficacy of any intervention strategies is likely to be limited. In particular, protective factors “buffer” risk, hence their limited prevalence in discussions suggests the vulnerability of some children may remain unchanged or even increase despite the involvement of professionals. Talking about risk does not increase the safety of children. As White (2009, p. 223) reminds us, the increasing levels of anxiety and uncertainty in social work result in a greater expectation for professionals to act, “where the imperative is to decide what is wrong, not what works.” While professionals have to analyze risk in terms of what is wrong, it is equally crucial to include protective factors in a strategy for it to work. A starting point is for professionals to re-construct protective factors and risk and apply it with critical thinking to core elements of social work practice, such as assessments, multi-disciplinary meetings, and verbal communications with service users.
Footnotes
Ethics
Ethical approval was provided by the University of Strathclyde's ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Acknowledgements
We would like to thank the staff involved in the Interventions for Vulnerable Youth Project.