
Abstract
Summary
Social rehabilitation is conceived to encompass services that concentrate specifically on the social aspect of the rehabilitation process. This interpretive qualitative meta-synthesis of 25 social scientific research papers published between 1980 and 2019 dealing with the concept of social rehabilitation aims to unpack the different dimensions of the social within social rehabilitation in different contexts.
Findings
In most of the articles, the causes for social rehabilitation are located in the rehabilitee’s social environment, community, or structure, and for the rehabilitation to be successful, a change is expected to take place also in these parties. Moreover, personally significant values and wishes are emphasized in many approaches viewing the rehabilitee as an agent in his/her own rehabilitation process. In a few articles, however, the individual is viewed as aberrant, and his/her conforming to societal norms is seen as forming the core of social rehabilitation. In this approach, the individual is viewed as the object of rehabilitation without much control over his/her own rehabilitation process.
Applications
The results of our study suggest that, to improve existing social rehabilitation practices, more effort should be put into acknowledging and considering the rehabilitee’s autonomy as a relational concept. Also, the needs for, foci, and aims of social rehabilitation should not be reduced to a certain kind of practice directed to certain kinds of client groups, but, rather, social rehabilitation should be understood as an entity consisting of interrelated and interdependent components forming a constantly shifting assemblage.
Introduction
The purpose of this study is to explore the diversity of social rehabilitation as a form of service as it appears in research literature: What is meant by the concept of ‘social rehabilitation', for whom it is intended, and what kinds of practices it refers to? Moreover, this article aims to explore the origins of the need for social rehabilitation and make sense of its focus and objectives. The purpose of this investigation is to make an interpretive integration of earlier research findings (see Sandelowski & Barroso, 2007) to propose a new theoretical framework for understanding the multiplicity of the existing forms of social rehabilitation (Aguirre & Bolton, 2014).
In principle, the social aspect of rehabilitation could be located within the field of social work as part of its agenda and practices. However, the concept is not widely used within the discipline of social work. Rather, claims have recently been made that the social aspect is disappearing from social work (Kam, 2014) or even from society in general (Lorenz, 2016).
Because social work and social rehabilitation are both engaged in a holistic perspective trying to promote human well-being by strengthening opportunities and facilitating the interaction between individuals and their environment, social rehabilitation should be discussed more extensively especially in the field of social work research.
The history of rehabilitation can be seen as nonlinear and complex with several stages and paradigm shifts (Gzil et al., 2007). Rehabilitation was defined in 1969 by the World Health Organization (WHO) Expert Committee on Rehabilitation Medicine as “combined and co-ordinated use of medical, social, educational, and vocational measures for training or re-training the individual to the highest possible level of functional ability” (WHO Expert Committee on Medical Rehabilitation, 1969, p. 6). In the definition set out in 1981, the social as a separate form of rehabilitation was no longer explicitly mentioned, but the social aspect of rehabilitation was expressed more generally: “Rehabilitation includes all measures aimed at reducing the impact of disabling and handicapping conditions, and at enabling the disabled and handicapped to achieve social integration” (WHO Expert Committee on Disability Prevention and Rehabilitation, 1981, p. 9). Nevertheless, social rehabilitation continues to be discussed to some extent in research literature and in rehabilitation practices.
In the 1970s and 1980s, there was growing criticism of the medical model of rehabilitation (e.g., Anderson, 1975; DeJong, 1979). This criticism was intertwined with an ideological shift from the ‘medical' to the ‘social' model of disability, whereby the focus was redirected from the perceived limitations of persons toward the societal and environmental barriers (Dobren, 1994; Stubbins & Albee, 1984). This paradigm shift to ecologically oriented rehabilitation entailed an extended understanding of rehabilitation as quintessentially empowering work in which disabilities are seen through a wider lens—not in terms of the disability or disease itself (e.g., Dobren, 1994; Oliver, 1996).
The introduction of the International Classification of Functioning, Disability and Health in 2001 has also been argued to have meant a paradigm shift due to its considerable implications for rehabilitation (Stucki, 2016). Later, the United Nations (2006) validated the new approach in 2006 with the Convention on the Rights of Persons with Disabilities, which further directed national legislations toward more social focus on rehabilitation. For example, in Finland, social rehabilitation was adopted in Social Welfare Act in 2014 (Sosiaalihuoltolaki, 2014), the purpose of which was to clarify the complex service system of rehabilitation, strengthen the social aspect of rehabilitation, develop the services to meet people’s complex needs in complex environments, and promote interprofessional collaboration (Kananoja, 2012).
Interestingly, there have been policy-level discussions on the social aspect of rehabilitation already from the 1960s onward, and it seems that the meaning of the social has strengthened over time through these discussions. However, discussions on the actual concept of social rehabilitation and its meaning have remained scarce. Similarly, in research addressing the social aspect of rehabilitation, ample reference is made, for example, to social interaction, community participation, achieving or maintaining social roles, or understanding the social demands of the environment (e.g., Hammel et al., 2015; Phillips et al., 2016). However, in these studies, the potential client groups, forms, and aims of social rehabilitation include so much variation and interpretation that its practical implementation remains challenging (Phillips et al., 2016).
To gain insights into the concept itself, research on the definitions in concrete applications of social rehabilitation as well as stronger theoretical and model-driven base for analyzing the social aspect of rehabilitation are needed (Hammel et al., 2015; Phillips et al., 2016). Our article contributes to this discussion by providing an overview of the descriptions and applications of the concept of social rehabilitation in different contexts and settings in light of research literature from 1980 to 2019. To capture the diversity of the descriptions and applications and their underlying philosophies, we look for answers to the following questions:
What are the client groups, physical settings, and forms of services in social rehabilitation practices? On what kinds of quintessential premises are the needs for, foci and aims of social rehabilitation based?
Data search and management
To grasp how the concept of social rehabilitation has been defined and applied in previous social science research literature, we have conducted a qualitative interpretive meta-synthesis. Our aim is to make an interpretive synthesis of qualitative findings, and for that reason, we use the term meta-synthesis (Finfgeld, 2003; Sandelowski & Barroso, 2007; Thorne et al., 2004). Aguirre and Bolton (2014) see qualitative interpretive meta-synthesis as enabling “synergistic understanding of phenomena with richness in diversity of settings, participants, and qualitative traditions” (p. 279). According to Finfgeld (2003), meta-synthesis is conducted to build a theory, to explicate a theory, or to describe a theory. Our study is the most closely tied to the last-named one, but as Schreiber et al. (1997) claim, these entities are complementary and overlapping. Through creating a meta-synthesis of the concept of social rehabilitation and its applications to practices, we bring the created entity to current theoretical discussion. Following Schreiber et al. (1997), we see our study as “bringing together and breaking down of findings, discovering essential features and producing a new and integrative interpretation of findings” (p. 314). As Saini and Shlonsky (2012) have argued, systematic syntheses of qualitative social work studies with their context-dependent approach and unique focus should be favored to transparently and rigorously wrap up their yields for evidence-based social work practice and policy.
For this article, we conducted searches using four large databases that are ProQuest: International Bibliography of the Social Sciences & Social Science Database; EBSCO: Academic Search Elite, AgeLine & PsycINFO; Web of Science: Social Science Citation Index; and Scopus. The searches were conducted in January 2019 in four stages. Figure 1 shows an adaptation of the standard PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram of the data search process (see Moher et al., 2009). The primary search was performed by entering the search term ‘social rehabilitation' in the default search field. 1 The inclusion criteria for the first stage were that the article had to be (a) peer reviewed and published in a scholarly journal, (b) written in English, and (c) published between 1980 and 2019. This search yielded a wide spectrum of articles (n = 422). Therefore, in the second stage, the search strategy was to include articles based on the occurrence of ‘social rehabilitation' as an author-given keyword. If the author-given keywords were not available for an article, the inclusion was based on the occurrence of the term ‘social rehabilitation' in the abstract or the title of the article. This strategy yielded 90 articles, and, after removing duplicates, 76 articles remained for further review.
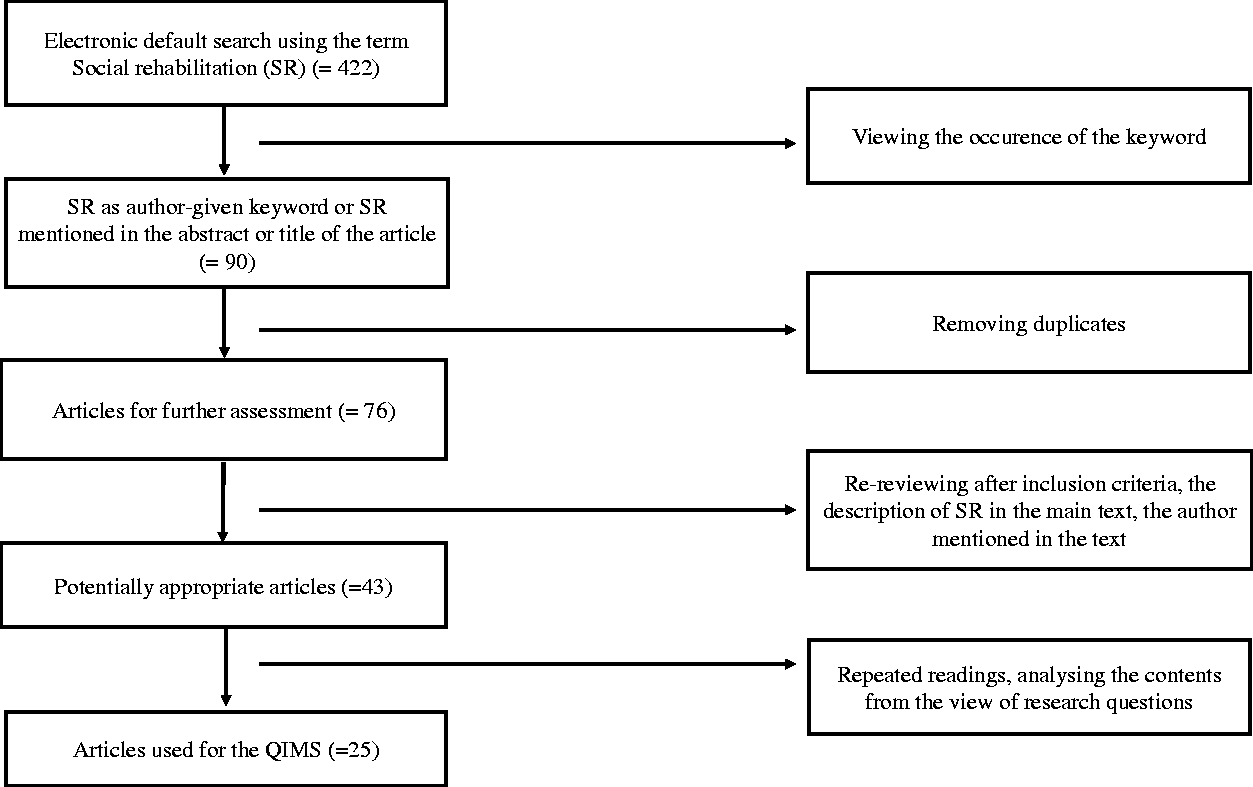
A PRISMA diagram of the data search process from four different databases.
In the third stage of the search process, the set of 76 articles was reexamined according to the original inclusion criteria. Articles were excluded if the author was not mentioned and in cases where ‘social rehabilitation' did not appear in the main text. In a few cases, ‘social rehabilitation' was not an author-given keyword, but a conceptual description (Sandelowski & Barroso, 2007) could be found in the article. In such cases, we decided to keep the articles for further examination. In this stage, the number of articles was 43. Finally, to ensure the inclusion of all relevant articles, the reference lists of the articles were scanned, and one relevant additional article was found in this way.
In the fourth, and final, stage of the search, the articles were thoroughly read and considered for relevance based on their overall content. This phase can be described as ‘into and between the lines' which means repeated readings and discovering the key elements from view of research questions (Horton, 2019). Finally, 25 articles were selected for the final study. The final sample of the articles along with their specific client groups, countries, and the level at which the concept of social rehabilitation is dealt with in each article is shown in Table 1.
Articles included in the study, their client groups, countries, and how social rehabilitation is dealt with in them.
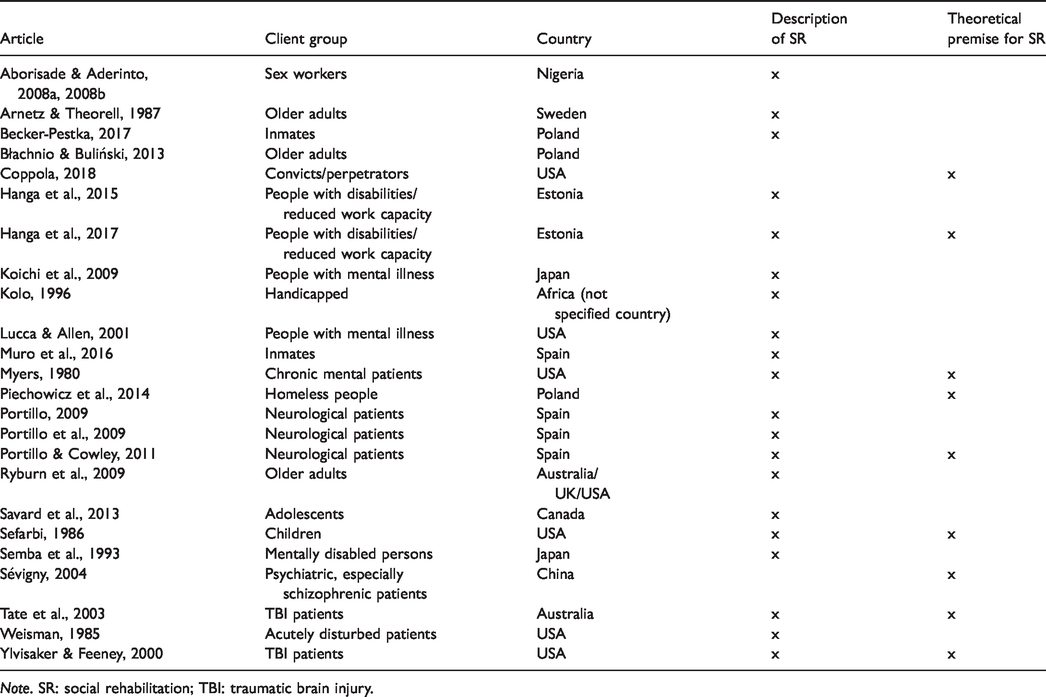
Note. SR: social rehabilitation; TBI: traumatic brain injury.
Technically, the analysis was conducted by carefully reading the papers of the final sample, disentangling the excerpts that deal with the client groups, physical settings, and the forms of services as well as any utterances considering the needs for, foci and aims of social rehabilitation. Thereafter, these contents were located in upper categories that finally could be placed into a continuum of different dimensions (see Thorne et al., 2004). All the three authors participated in the process of synthesis and interpretation, and the dimensions are a result of collective negotiation, which was needed especially in cases of contradicting opinions.
In the analysis, we wanted to form an overall synergistic picture of the articles and also highlight the found ideological differences. For this reason, the results presented in the next chapters represent somewhat simplified points of view. However, within the limits of our chosen mode of analysis and presentation, we have made every effort to deal with the articles in a manner that respects the varied content and nuances within.
Results
The client groups, physical settings, and services of social rehabilitation
In the articles analyzed for this study, the concept of social rehabilitation is elaborated on, discussed, or referred to in relation to various groups of people. The largest distinctive client group of social rehabilitation efforts is patients with a clear medical diagnosis or an impairment, which, by extension, affects their social life. This group includes people with neurological problems (e.g., traumatic brain injury; Tate et al., 2003; Ylvisaker & Feeney, 2000), neurological patients (Portillo & Cowley, 2011), psychiatric patients with mental illness (Koichi et al., 2009; Lucca & Allen, 2001; Myers, 1980; Semba et al., 1993; Weisman, 1985), and people with disabilities (Hanga et al., 2015, 2017; Kolo, 1996). Hanga et al. (2015, p.32) also use the expression people with “reduced work capacity”, which can refer to either a medical diagnosis or some other cause such as emotional problems.
Another distinctive group that emerged in the studied literature is people with various psychosocial problems due to a difficult background or a history of behavior that does not fit into the standard norms of society, such as criminal activity or other kinds of socially unconventional behavior. Individuals falling into this category include convicts (Becker-Pestka, 2017; Coppola, 2018; Muro et al., 2016), people with a background in sex work (Aborisade & Aderinto, 2008a, 2008b), homeless people (Piechowicz et al., 2014), and teenagers or children with multiple emotional, behavioral, or psychiatric problems (Savard et al., 2013; Sefarbi, 1986).
Social rehabilitation is also discussed in relation to older adults (Arnetz & Theorell, 1987; Błachnio & Buliński, 2013; Ryburn et al., 2009), in which case the concept is not associated with medical diagnosis or aberrant behavior, but rather with social hindrance or passivity seen as related to the stage of life or institutionalization.
Challenges in the social realm (e.g., relationships, employment, or housing) connect all of the aforementioned groups. In many of the articles analyzed in this study, problematic social interaction emerged as the main challenge leading to difficulties in finding or maintaining employment, continuing independent living, and establishing and maintaining relationships (Ylvisaker & Feeney, 2000). The need for social adjustment emerged as a common characteristic of the contexts mentioned in the articles. Something—a traumatic injury, an illness, physical decline, aberrant behavior, or institutionalization—has interrupted the standard life course and brought about challenges to an individual’s social life.
The articles give an overview of how social rehabilitation is organized in practice. Social rehabilitation efforts can be roughly divided into three systems. On one end of the continuum, there are residential social rehabilitation facilities, for example, for the mentally ill (Lucca & Allen, 2001), acutely disturbed patients (Weisman, 1985), adolescents with emotional and behavioral problems (Savard et al., 2013), or trafficked women with a background in sex work (Aborisade & Aderinto, 2008a, 2008b). These vary in nature from total institutions to home-like facilities with a daily program. On the other end of the continuum, there are community-based services or programs, which include interventions by and meetings with different professionals as well as other activities. Most of them take place in settings such as the home of the client, a café, a community center, or other communal facility, for example, in case of discharged traumatic brain injury patients (Ylvisaker & Feeney, 2000), persons with disabilities or reduced work capacity (Hanga et al., 2015), homeless persons (Piechowicz et al., 2014), children with multiple problems (Sefarbi, 1986), and mentally ill patients (Koichi et al., 2009). In addition to the practices described earlier, social rehabilitation takes place within other institutions such as prisons (Becker-Pestka, 2017; Muro et al., 2016), residential facilities for older adults (Arnetz & Theorell, 1987), or hospitals (Portillo et al., 2009; Portillo & Cowley, 2011). A common characteristic of the different social rehabilitation programs is the emphasis on collaboration between different professionals, institutions, and organizations (e.g., Piechowicz et al., 2014; Portillo, 2009; Portillo & Cowley, 2011; Tate et al., 2003).
The actual services offered under the title ‘social rehabilitation' are manifold. Social rehabilitation covers services from social assessments to therapy (e.g., Hanga et al., 2017; Portillo et al., 2009; Portillo & Cowley, 2011), counseling, and coaching (e.g., Hanga et al., 2015; Piechowicz et al., 2014; Ylvisaker & Feeney, 2000); from educative groups (e.g., Becker-Pestka, 2017) to actual vocational training (e.g., Aborisade & Aderinto, 2008a; Hanga et al., 2015; Koichi et al., 2009) or job hunting (Sefarbi, 1986); and from solving relationship or communication problems (e.g., Savard et al., 2013; Ylvisaker & Feeney, 2000) to recreational activities and outings (e.g., Arnetz & Theorell, 1987; Lucca & Allen, 2001).
The dimensions of social rehabilitation: Needs, foci, and aims
While the client groups, settings, and services led us to perceive the heterogeneous nature of the social rehabilitation practices, our main interest focuses on what kinds of meaning ‘the social' is given in these contexts. After having read through the articles, various interpretations of it emerged.
First, the social aspect was associated with the need for social rehabilitation. The need for social rehabilitation can be seen as stemming either from social deviance, illness, or disability of an individual or from environmental factors. This, in turn, dictates whether the focus of social rehabilitation will be on the individual or, by extension, on the wider community and societal structures and, further, whether social rehabilitation is viewed as an individual endeavor or as a collective effort.
Second, ‘the social' seemed to comprise social norms and as such affecting the aims of social rehabilitation. An interesting question is who determines these norms one must conform to and how much room there is for individualism or agency within the realm of social standards.
Third, it is interesting to ponder how broadly the social element is generally understood in the context of social rehabilitation. In the narrowest sense, it might refer merely to social interaction, whereas in a broader sense, it could be seen as encompassing, for example, vocational, educational, housing, and relationship aspects.
On the basis of the initial findings, we formulated three dimensions that reflect these questions. The dimensions are the needs for, the foci and the aims of social rehabilitation (see Table 2).
The needs, foci, and aims related to social rehabilitation.
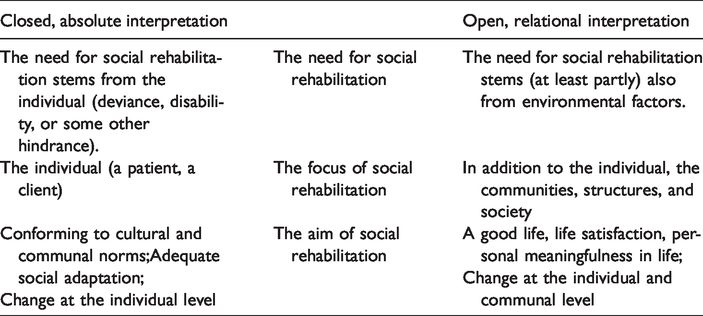
The left column represents a closed, absolute interpretation of social rehabilitation. In this interpretation, the need for social rehabilitation lies in the deviance, disability, illness, or other kind of problem of the individual, and thus, the social rehabilitation efforts are targeted at the individual with the objective of producing a change in the individual for him/her to be able to adapt to the community in a socially acceptable manner and conform to the expected cultural and moral norms and values. The power in the process lies with the professionals—the individual undergoing rehabilitation is more of an object than an agent of the rehabilitation process.
The right column of Table 2 represents an open, relational interpretation of social rehabilitation. In addition to individual challenges, the need for social rehabilitation is seen as rising from a number of environmental factors such as harmful childhood circumstances or inflexible studying and working conditions. Hence, the focus of social rehabilitation is not only on the individual but also on his/her social networks, the wider community, and societal structures. The aims of rehabilitation, such as living a good life, being satisfied with one’s life, and being able to make authentic choices, stem from the unique life-context and values of the rehabilitee. Thus, he/she is seen as a capable agent and an active subject in the rehabilitation process. In the following paragraphs, we explain and illustrate our synthesis in more detail, deploying examples of the studied articles.
The need for social rehabilitation and the actual practice of social rehabilitation is associated with the presumption of the nature of the difficulty that leaves an individual in need of social rehabilitation. In most of the articles examined, the reasons that have led to the situation in which an individual is in need of social rehabilitation are seen as located in the environment. In a few articles, the reasons are seen as located within the individual.
Coppola (2018), who discusses social rehabilitation in the context of convicts, argues that socioemotional competencies and skills are intertwined with environmental, social, and economic factors. Thus, the lack of such competencies and skills is linked with the background, environment, and experiences of the individual, and, consequently, such competencies and skills are seen as malleable if the environment is suitable and offers social support. According to this view, change can be fostered by influencing the environmental factors that support the rehabilitation goals.
Similar views were found in many other articles we examined. Disability, problematic behavior, or other social problems are perceived as grounded in the interaction between the individual and his/her environment (Hanga et al., 2015; Kolo, 1996; Piechowicz et al., 2014; Sefarbi,1986). According to Myers (1980), society plays its part in the creation of “socio-cultural deviance” (p. 42). Sévigny (2004) points out that the entire phenomenon of social rehabilitation—and the people seen in need of it—are always shaped and understood within the social, political, and cultural movements and ideologies of the time.
The examples mentioned earlier reflect a rather relational conception of human being, according to which the strengths and challenges of the individual take shape in and through their relationships or their membership of various communities. However, some other authors stress that the need for social rehabilitation lies within the individual.
Portillo and her research team (Portillo, 2009; Portillo et al., 2009; Portillo & Cowley, 2011), whose studies focus on the clinical setting, represent a view somewhere between the two ends of the continuum. On one hand, Portillo and her colleagues acknowledge that the scope of the focus of social rehabilitation must be wider than the individual—for example, an individual’s family members must be involved in the process—but, then again, their view of the very definition of social rehabilitation as a process “through which a person becomes aware of his/her own social limitations” places emphasis on the individual’s condition (Portillo & Cowley, 2011, p. 1330).
Referring to problems such as social stigma, corruption, lack of finances, and dysfunctional politics, Aborisade and Aderinto (2008a, 2008b) acknowledge the role of society in creating the problems which increase the need for social rehabilitation and worsen the situation of the rehabilitees. However, the social rehabilitation programs presented by them place more emphasis on the individual. Similarly, Becker-Pestka (2017) views the individual (a convict) as a deviant person who has violated the rules of society and is, thus, in need of social rehabilitation.
The focus of social rehabilitation can be on the individual or, by extension, on the surrounding network, community, or social structures. Many of the articles examined mention the need to change the community, environment, or social structure as a pivotal part of social rehabilitation (Coppola, 2018; Portillo & Cowley, 2011; Sefarbi, 1986; Tate et al., 2003; Ylvisaker & Feeney, 2000). Kolo (1996) and Piechowicz et al. (2014) mention attitudinal change toward the population in rehabilitation as the core of social rehabilitation. Sefarbi (1986, p. 40) refers to this broader view as an “eco-structural” philosophy.
Quite a few programs described in the articles also involve the family or relatives of the rehabilitee in the process of rehabilitation. In a program described by Portillo (2009), one of the distinctive features of social rehabilitation (in comparison to clinical health-care) was focus on rehabilitees and carers as dyads, whereby the relatives, too, needed to recognize both the rehabilitee’s and their own social needs. In some instances, the family is recognized as needing social care as much as the rehabilitee (Piechowicz et al., 2014; Sefarbi, 1986). Relational support and proper environmental conditions are acknowledged as pivotal for social rehabilitation to be effective (Coppola, 2018; Myers, 1980; Piechowicz et al., 2014; Portillo & Cowley, 2011).
Focus on the individual and change in an individual’s behavior is highlighted especially in an institutional context. The goal of social rehabilitation is to consolidate change “in inmates’ habits, attitudes and values” (Muro et al., 2016, p. 714, see also Weisman, 1985). Also, Becker-Pestka (2017) mentions convicts’ attitudinal change as an expected outcome of a social rehabilitation program. In addition, she mentions other individually focused outcomes: searching for a job, managing stress, and coping with negative emotions. The strong effect of the environment, and, for example, the social stigma, is acknowledged in the rehabilitation of former sex workers, yet the focus of the rehabilitation is centered on what is referred to as the individual’s “positive turnaround” (Aborisade & Aderinto, 2008b, p. 1936). In the context of convicts, the negative consequences of social exclusion and the importance of relationships are recognized (Becker-Pestka, 2017; Muro et al., 2016), but the focus of attention remains on the individual. These articles promote an interesting view that the premises of social rehabilitation are somewhat different in prison or other restricted institutional contexts.
When social rehabilitation efforts focus on the environment in addition to the individual, also the pressure for outcomes does not lie only with the individual. For example, in relation to employment, the employer might alter the work duties, which could contribute to the success of social rehabilitation (Tate et al., 2003). Also, Hanga et al. (2015) recommend modifying the physical environment as part of increasing participation and employment.
The material surroundings, which are selected as the venues for social rehabilitation in practice, also reflect the focus of the procedure. According to Sefarbi (1986), using various locations in the community and involving the rehabilitee’s network in the rehabilitation process signifies that the social aspect is taken seriously. Meetings in the rehabilitee’s home, for example, are mentioned in other articles as well (Portillo, 2009; Ylvisaker & Feeney, 2000). Taking social rehabilitation into the community, into the midst of the daily routines of the rehabilitee, reflects the view that social rehabilitation does not concern only the individual but involves the wider community.
In some of the articles, social rehabilitation also covers the societal level. According to Hanga et al. (2017), the principles of person-centeredness—which is seen as the basis of social rehabilitation—should be implemented in legal frameworks and in the quality standards of social services. Other authors recognize that social change demands sociopolitical perspective and recognition of social and structural (dis)advantages and is thus intertwined with the idea of social justice (Coppola, 2018; Piechowicz et al., 2014; Tate et al., 2003).
On the basis of our analysis, the aims of social rehabilitation can be roughly divided into two contrasting views. In some articles, conforming to standard societal norms and fulfilling an appropriate social role are highlighted. Then again, in some other articles, the emphasis is on finding a good, satisfying life by aligning the rehabilitation goals and activities with the rehabilitee’s personally significant and meaningful values and wishes.
According to Myers (1980), learning to negotiate with society and its institutions for the sake of one’s well-being is part of social rehabilitation. Ylvisaker and Feeney (2000) mention finding a satisfying life as the general goal of social rehabilitation (see also Portillo & Cowley, 2011). Well-being or life satisfaction cannot be defined extrinsically, but rather connote personal grounds for social rehabilitation, which is reflected also in the references to the person-centered or contextualized approach found in some of the articles (Hanga et al., 2017; Tate et al., 2003; Ylvisaker & Feeney, 2000). Person-centeredness means treating the rehabilitee as the expert of his/her own life and being conscious of the individual’s unique characteristics, needs, values, beliefs, and preferences (Hanga et al., 2017). The individual’s “unique constellation of impairments,” personal characteristics and wishes along with the specific environmental circumstances affect the definition of the individual’s personal aims regarding social rehabilitation (Tate et al., 2003, p. 147). This view also incorporates the idea that the individual is the one who can—and must—personally evaluate the outcomes of social rehabilitation, whereby a seemingly small achievement might be a significant outcome from the viewpoint of the rehabilitee.
Person-centeredness does not, however, mean neglecting social rules or structure altogether. Rather, the question is about the degree of societal expectations and normativity in relation to the aims of social rehabilitation. After all, life without adherence to any social norms would, ultimately, mean anarchy. Thus, incorporation of personally meaningful goals within social rehabilitation programs is, to varying extents, affected by the predominant social structure and culture.
In some of the articles, reference to reintegration or readaptation seems to imply a rather normative expectation, whereby acknowledging the unique context of the individual is, for the most part, missing. The goals mentioned include fulfilling “social roles” (Piechowicz et al., 2014, p. 478), following the “principles of social life” (Becker-Pestka, 2017, pp. 129, 131), playing a “proper role” in the community (Muro et al., 2016, p. 713), “internalizing socially accepted rules” (Savard et al., 2013, p. 689), or “spiritual rebirth” (Aborisade & Aderinto, 2008b, p. 1945). References to building independence and strengthening personal resources (Piechowicz et al., 2014) or the inmates’ “improved subjective quality of life” (Muro et al., 2016, p. 713) counterbalance the aforementioned goals, albeit the overall goals of social rehabilitation are of a general and normative nature.
Approaches to social rehabilitation that aim at finding a good, satisfactory life leave more room for autonomy. Goals such as belonging to a social network, finding work, and living independently are depicted as something that the individual is entitled to, not pressured toward (Tate et al., 2003). Social rehabilitation might aim at socially acceptable and standard goals, such as finding a job or completing a degree, but does so only if these goals are in line with the individual’s own goals. For example, Ylvisaker and Feeney (2000) explicitly stand in opposition to the idea of “socially appropriate behaviour,” fulfilling of extrinsically defined social goals, or life determined by authority figures. They promote the maximum possible choice and control, responsibility, and personally meaningful activities of the rehabilitee as key ingredients of social rehabilitation.
Discussion
The previously discussed different conceptions of social rehabilitation should not be viewed as objective facts but as representing various discourses. For this reason, our findings are not intended to be read in the light of cross-cultural comparison, but rather as conceptions of social rehabilitation disseminating across various geographical locations and cultural and historical settings. These conditions inform the reflection on and discussion of the outcomes of this meta-synthesis presented in the following paragraphs.
To begin with, different paradigms of rehabilitation were clearly represented in the research literature examined. The tendency to interpret rehabilitation via a social model instead of a clinical one (Dobren, 1994; Stubbins & Albee, 1984) is present. In the open interpretation, the focus of rehabilitation is directed toward the environment of the rehabilitee, whereas in the closed interpretation, the focus remains on the disability or disease itself (see Oliver, 1996). As our findings indicate, most of the social rehabilitation programs presented in the literature are inclined to stress the social model of rehabilitation. This may reflect the prevailing social paradigm: The focus has been redirected from medical impairments to wider social elements, both the barriers as well as the opportunities in the recovery of the client. Indeed, attempts to move away from the clinical definition of rehabilitation were clearly articulated in some articles. (Myers, 1980; Portillo, 2009; Portillo et al., 2009; Sévigny, 2004). In some contexts, however, the practice and ideology of social rehabilitation might still be inclined toward medical rehabilitation, for example, when social rehabilitation takes place in a clinical setting (Savard et al., 2013). It is necessary to add that, as Goodley (2001) has pointed out, there is a risk of misreading behavior as an embodied impairment when it is actually essentially shaped by the environment.
Second, it became apparent that the dimensions of the analysis reflect different underlying conceptions of human being (e.g., Stevenson & Haberman, 1998). In the articles that rely on the open interpretation paradigm, the active role and the needs of the individual are emphasized. The rehabilitees are associated with values and qualities such as responsibility, self-determination, independence, autonomy, and self-efficacy. They should own the rehabilitation process and the life they will lead afterward, being ‘critical agents' of their own rehabilitation (Coppola, 2018; Hanga et al., 2017; Tate et al., 2003; Ylvisaker & Feeney, 2000). In this approach, the client is a unique person with “individual characteristics, needs, values, beliefs and preferences” that should be taken into account (Hanga et al., 2017, p. 254). In a similar fashion, Portillo and Cowley (2011) call for acknowledging the client’s perspective. This view is based on philosophy of rights rather than of duties or obligations. Instead, the closed interpretation (of the individual as an object of rehabilitation) represents, to some extent, a rather paternalistic—or correctional—viewpoint, which aims at changing or ‘reforming' the individual. In the context of prison (Becker-Pestka, 2017; Muro et al., 2016; Piechowicz et al., 2014), sex work (Aborisade & Aderinto, 2008a, 2008b), a social rehabilitation center for youth (Savard et al., 2013), and homelessness (Piechowicz et al., 2014), the deviance from normal standards is accentuated. The agency of the individual is viewed in a much narrower sense, leaving only little room for autonomy.
Third, attention should be drawn to the aforementioned concept of autonomy. Enhancing autonomy was stressed in the articles representing the open, relational interpretation, and the principle of respecting personal autonomy is a generally accepted Western ideal (Mackenzie, 2019). However, in the field of social rehabilitation, the concept of autonomy should not be taken for granted, but considered critically, as (social) rehabilitation is intertwined with the need to balance between the rehabilitee’s vulnerabilities and agency. The concept and theory of relational autonomy provides a lens to examine and evaluate autonomy in social rehabilitation efforts. Mackenzie (2019) defines it as a “capacity to lead a self-determining life and as a status of being recognized as an autonomous agent by others” (p. 147). In her thinking, autonomy is embedded in the social realm, dependent on relationships, social norms, structures, and institutions. Social rehabilitation professionals/programs should evaluate how autonomy is understood and whether the rehabilitation practices actually enable individual autonomy or deprive the individual of autonomy, and whether the stressing of autonomy leaves room for addressing the vulnerabilities and dependency of the rehabilitee.
Overall, our meta-synthesis points out that social rehabilitation with its varying definitions, contexts, and underlying values should eventually be understood as an assemblage. Assemblage is a term first introduced by Deleuze and Guattari (1987) by which they refer to a multiplicity, a “one kind of organism, or signifying totality” that, when no longer attributed, “has been elevated to the status of a substantive” (p. 4). According to assemblage theory, these multiplicities—assemblages—are regarded as systemic aggregates composed of constantly shifting interdependent components that work in interaction, encounter temporally and spatially, transform, and then break apart again (DeLanda, 2006; Deleuze & Guattari, 1987).
According to Deleuze and Guattari’s ontology, ‘body' and ‘health' are concepts that are situated in a web of biological, psychological, cultural, economic, and other relations of objects, technologies, ideas, and social organisations. All these components and their relations influence and are influenced by others in the assemblage (Fox, 2002, 2016). The theory has been applied in many studies on mental health, recovery, and disability, allowing a shift away from reductive and overly individualized accounts and emphasizing the relative character of the phenomenon (e.g., Abrams et al., 2019; Duff, 2014; Gibson et al., 2017). Following this, the conceptual lens of assemblages provides an alternative tool to become aware of and examine the complexity of factors that influence and shape the practices of social rehabilitation over time and place. Viewing social rehabilitation as assemblages attributable to varying heterogeneous components—bodies, meanings, times, places, values, habits, norms, policies, technologies, and so forth—helps us understand the wide variety of its client groups, practices, needs, foci, and aims.
Perceiving social reality as assemblages fundamentally concerns the questions of power (Buchanan, 2015). Social rehabilitation always takes place in a specific context—historical, political, and cultural—and the contexts dictate what is considered as a condition requiring social rehabilitation and what is its aim (Sévigny, 2004). Moreover, sometimes, talking about social rehabilitation may eventually serve other ends than the needs of the rehabilitee. Namely, social rehabilitation programs, regardless of their content, might be a way to achieve respect and a good reputation in the field of international politics (see Aborisade & Aderinto, 2008a) or a way to justify economic decisions (e.g., Ryburn et al., 2009; Weisman, 1985; Ylvisaker & Feeney, 2000). Therefore, evaluating different programs and practices requires critical and contextual reflection.
On the basis of the findings of our study, and to bring about an improvement in the existing social rehabilitation policies, the concept of autonomy as a relational concept should be better acknowledged and considered when developing social rehabilitation programs. It is an approach that might be easily overshadowed, for example, by dominant local agendas and political discourses of social care (Ellis, 2015). Furthermore, the wider assemblage of social meanings, values, technologies, and other relevant elements that are entwined with social rehabilitation efforts (Fox, 2016) should be acknowledged in order not to lose the sight of 'the social' in society (Lorenz, 2016) and especially in social work (Kam, 2014). This task belongs, first and foremost, to the field of social work and within the role and assignments of social workers.
Limitations
The data search using the concept of ‘social rehabilitation' as performed in this study covers several relevant databases provided by ProQuest, EBSCO, Web of Science, and Scopus. Even though our search covered a wide range of relevant databases and yielded a wide sample of research papers, we acknowledge the limitations of the database coverage for this study. There are other databases that were consciously excluded as we aimed to focus especially on the social scientific explorations of social rehabilitation. Also, professional reports on social rehabilitation programs, and other gray literature, may have provided even more up-to-date knowledge about current social rehabilitation practices.
Conclusion
This qualitative interpretive meta-synthesis of 25 social scientific research articles provides an overview of the forms of social rehabilitation and the ways in which it is applied in different contexts. The particular focus of this examination is on the different meanings associated with ‘the social' within the practices of social rehabilitation.
In terms of the client groups of social rehabilitation, three different categories were distinguished: health related (e.g., injury or illness), behavior related (behavior that violates social norms), and life course related (elderly people). With respect to the physical setting of social rehabilitation, three different systems were distinguished: residential social rehabilitation facilities, community-based services or programs, and other institutions (e.g., prisons). The actual practices of social rehabilitation include a wide spectrum of services such as social assessments and therapy, counseling and coaching, education, vocational training, solving communication problems, and recreational activities.
Depending on how ‘the social' is understood in social rehabilitation practices, they could be placed on a continuum with a closed and absolute interpretation of the social aspect of rehabilitation on one end and an open and relative interpretation on the other. In most of the articles, the needs for social rehabilitation are located in the environment in a very relational sense. In these cases, the focus of social rehabilitation is—in addition to the rehabilitee—on the community, environment, or social structure, and a change also in these parties is seen as a pivotal component of social rehabilitation. In the more absolute approaches, the client is viewed as aberrant and therefore in need of social rehabilitation, and conforming him/her to standard societal norms appears as the focus of social rehabilitation.
The findings of our study indicate that social rehabilitation should not be understood as a one-dimensional fixed form of social care but as a constantly shifting assemblage comprised of multiple transforming components. Assemblage thinking conceptualizes social rehabilitation as a phenomenon conditioned by material, economic, technological, political, and cultural influences. It conceptualizes ‘humanity', ‘health', ‘well-being', and ‘life satisfaction' always in relation to the surrounding and prevailing regularities and influences (Fox, 2002, 2016). Accordingly, if one element of an assemblage of social rehabilitation is affected, its premises, foci, and aims are reassembled in the process as well. Thus, as assemblages are always political in nature (Nail, 2017) and policies are always politically enacted (e.g., Ellis, 2015), the meaning of ‘the social' should be more consciously maintained and brought to the forefront not only when formulating and implementing social rehabilitation policies but also, and especially, in those debates on political powers that concern social care. This is crucial to guarantee equality and social justice of different client groups with different needs in different contexts.