
Abstract
Objective:
In this study, various micro-osteoperforation (MOP) approaches were designed and their impacts on dentoalveolar structures were evaluated during maxillary canine distalisation in clear aligner (CA) treatment using a three-dimensional (3D) finite element method (FEM).
Design:
A 3D analysis was conducted of displacements and stresses in canine distalisation with various MOP approaches in CA.
Setting:
Computational study.
Methods:
In CA treatment, a FEM model was created to simulate distalisation of the maxillary canine by extraction of the first premolar. A total of 12 MOP approach designs were simulated for variations in the location, number and distance of the MOPs. MOP was not applied in one model; a total of 13 models were created. Canine and aligner displacement, and stresses on the periodontal ligament (PDL) were calculated under 0.24 CA activation.
Results:
The effect of MOPs on canine displacement was non-significant. The movement was observed as tipping. Localisation, MOP–canine distance and MOP depth parameters did not affect canine and aligner displacement. Canine and aligner displacement was the same across all models. Moreover, the compression stresses within the PDL were minimal and showed no significant variations among the models, whereas the tensile stresses displayed only minor differences.
Conclusion:
MOPs did not alter the biomechanical responses of dentoalveolar structures concerning the canine and aligner but had a small and non-clinically significant effect on PDL.
Keywords
Introduction
There are two main challenges in orthodontic treatment for adult patients: treatment duration and the risk of adverse effects, such as root resorption and bone loss. The extended duration of orthodontic treatment is a major concern for the current generation, often leading individuals to avoid treatment or seek alternative options (Ren et al., 2007). Clear aligners (CAs) are transparent, removable appliances that gradually guide teeth into desired positions. They are aesthetic alternatives, especially for adults who have concerns about the visibility of traditional braces (Wall et al., 2024).
Canine distalisation is a time-consuming procedure for patients undergoing premolar extraction in orthodontic treatment. The traditional approaches used to achieve this movement result in relatively slow rates of canine distalisation, typically in the range of 0.5–1 mm per month. Consequently, the complete distalisation of the canine may take anywhere from 5 to 9 months (Abbas et al., 2016). Pharmaceutic, electromagnetic, laser and surgical stimuli have gained attention in the literature for their potential to accelerate orthodontic tooth movement. Various surgical techniques have been developed over the years to speed up treatment time, including the use of additional dentoalveolar surgeries (Keser and Naini, 2022). Corticotomy decorticates bone and increases metabolic turnover, reducing orthodontic tooth movement resistance. Through the regional acceleratory phenomenon, this technique increases osteoclast and osteoblast numbers, decreasing localised bone density in adults. In addition to the regional acceleration phenomenon (RAP) caused by the injury, breaking alveolar bone continuity can change stress/strain distribution in dento-alveolar structures (Liu et al., 2020). Micro-osteoperforation (MOP) represents a form of conservative corticotomy. MOP is a minimally invasive technique that involves creating small perforations without raising a mucogingival flap (Golshah et al., 2021).
There are case reports in the literature in which corticotomy is used to accelerate tooth movement in CA treatment (Caruso et al., 2020; Hannequin et al., 2020). To our knowledge, no studies have evaluated the effectiveness of different approaches of MOPs in the treatment of canine distalisation using CA.
Finite element analysis (FEA) is a very precise method of analysing structural stress and strain and further understanding the mechanics of solids and structures. FEA can reconstruct the shape and size of a model similar to the actual object, which helps investigate stress distributions and displacements in various systems with complex structures and properties. By using FEA, researchers can evaluate different treatment strategies, optimise treatment planning and predict the mechanical effects on the surrounding structures (Romanyk et al., 2020).
Due to substantial differences in geography, materials, boundaries and loading conditions between real-world and virtual simulations, clinical practice needs more informative and quantifiable data. Comparative results are valuable, as most factors can be adjusted or standardised—except for the key influencing variables. FEA allows for the simulation of orthodontic forces and surgical techniques without ethical concerns, thereby reducing the need for large experimental and clinical sample sizes (Liu et al., 2020).
The use of MOP to accelerate orthodontic tooth movement has been investigated in several studies, using either the Propel device (Excellerator; Propel Orthodontics, Propel Company, USA) (Alikhani et al., 2013; Fattori et al., 2020) or conventional mini-screws (Aboalnaga et al., 2019; Alkebsi et al., 2018; Babanouri et al., 2020; Feizbakhsh et al., 2018; Sivarajan et al., 2019). These studies employed different protocols, including perforation depths in the range of 1–8 mm, varying numbers of buccal and palatal perforations, and single versus repeated applications, leading to conflicting results. In addition, different anchorage mechanics and methods used to evaluate tooth movement make it difficult to compare these studies (Aboalnaga et al., 2019; Alikhani et al., 2013; Alkebsi et al., 2018; Babanouri et al., 2020; Fattori et al., 2020; Feizbakhsh et al., 2018; Sivarajan et al., 2019).
In this study, it was hypothesised that different MOP approaches, perforation depths, localisations, numbers of buccal and palatal perforations, and extents could affect the aligner, tooth movement and periodontal ligament (PDL) force system biomechanical status. Thus, this study used FEA to assess the biomechanical effects of various MOP approaches in CA treatment on canine distalisation, aligner displacement and PDL principal stresses.
Materials and methods
This study investigated the biomechanical impacts of MOPs on orthodontic tooth movement through finite element method (FEM) analysis. The choice of MOP parameters—localisation, distance between the canine and MOPs, number and depth of MOPs—was guided by previous clinical findings.
The literature has evaluated the effectiveness of different numbers of MOP applications (Shahabee et al., 2020), MOP depth (Ozkan and Arici, 2021) and MOP applications at different localisations (Babanouri et al., 2020). In corticotomy, a more invasive approach, it has been reported that the canine tooth–corticotomy distance affects the amount of tooth movement (Yang et al., 2015).
Localisation is a particularly critical parameter. Studies, such as those by Babanouri et al. (2020), have demonstrated that combining buccal and palatal MOPs can enhance the rate of tooth movement due to increased surgical trauma, which intensifies the inflammatory response and promotes osteoclastic activity. In addition, Yang et al. (2015) reported that the proximity of interventions like corticotomy significantly influences biomechanical effects, suggesting that interventions closer to the moving tooth yield better outcomes. Accordingly, in this study, MOPs were positioned distal to the canine root at distances of either 3 mm or 5 mm (as shown in Table 1) to optimise biomechanical effects while ensuring procedural safety.
MOP approaches.
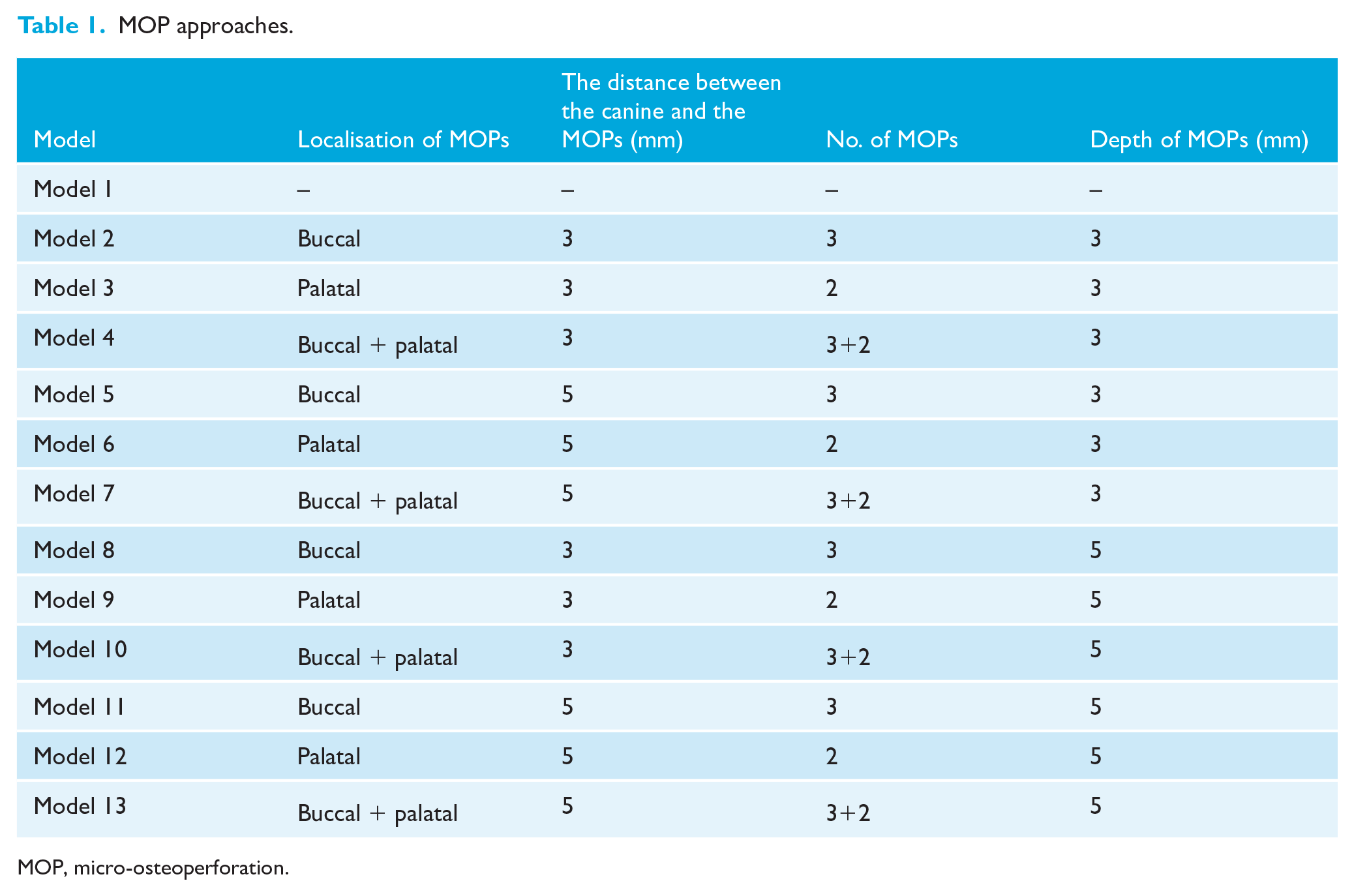
MOP, micro-osteoperforation.
The depth of MOPs was selected based on evidence indicating its ability to trigger the RAP without excessive invasiveness. For instance, Ozkan and Arici (2021) reported no significant differences between depths of 4 mm and 7 mm, suggesting that deeper perforations do not offer additional benefits. Similarly, Li et al. (2022a) found that a depth of 5 mm slightly increased tooth movement without clinical significance over 12 weeks. Therefore, the depth chosen for this study reflects a balance between efficacy and invasiveness.
Studies have shown that increasing the number of MOPs enhances tooth movement up to three perforations, beyond which no additional benefits are observed (Babanouri et al., 2020). This finding is supported by Li et al. (2022a), who reported no significant differences between two and three perforations, supporting the practicality of a minimal yet effective protocol.
FEM modelling was designed to simulate conditions reflective of clinical settings, incorporating a distalisation force applied perpendicular to the mesial surface of the canine attachment simulating 0.24 mm aligner activation, and boundary conditions with constrained superior maxillary nodes and symmetry along the X-axis to mimic orthodontic force application. Although this approach allowed for controlled analysis of MOP parameters, it is acknowledged that using a single set of linear material properties may not fully capture the complexity of biological tissues. Future studies will aim to refine the material models and validate the findings through experimental and clinical data, thereby enhancing the accuracy and applicability of the results.
According to our knowledge, no study has evaluated the effectiveness of all these variables in CA treatment with MOP applications. Therefore, we designed 12 models of 14 teeth with their PDLs, alveolar bones and aligners using various MOP approaches; MOP was not performed on a single model (Table 1, Supplementary Figure 1).
The development of finite element (FE) models involved a series of systematic steps. First, a geometric representation of the maxillary dentition was created, which included the periodontal structures, such as the PDL, cortical and trabecular bone, along with the aligner, attachments and MOPs. These geometric models were then transformed into FE models. Next, the material properties of the teeth, bones, PDL, aligner and attachments were integrated into the models. Boundary conditions were then established, and loading conditions were defined. Finally, the simulation results were analysed and interpreted (Bohara et al., 2017). FEM modelling enabled a standardised evaluation of biomechanical responses, overcoming the interindividual variability inherent in clinical studies. The model replicated clinically relevant conditions, including force application and biological responses to MOPs, offering a controlled setting to isolate the effects of specific MOP parameters.
Modelling of the maxilla, orthodontic materials and MOPs
We used a publicly available database of images of anatomical and computed tomography (CT) sections of female cadavers, made available through the Visible Human Project (The National Library of Medicine, FACT SHEETS Office of Communications and Public Liaison National Library of Medicine, Maryland, ABD), to create a three-dimensional (3D) FE model.
CT data were processed in 3DSlicer software (BWH, MA, USA; https://www.slicer.org/) (Fedorov et al., 2012), with segmentation based on appropriate Hounsfield unit (HU) values to create 3D models, which were then exported for further analysis.
The segmentation process was performed using 3DSlicer software with a HU threshold range of 426.50–3193.04 to segment the relevant anatomical structures accurately. This threshold range was selected because it encompasses the HU values corresponding to the density of the target structure while effectively excluding surrounding tissues and undesired regions.
This range was selected based on a trial-and-error approach. Different HU ranges were tested during the segmentation process, and the resulting images were evaluated for anatomical accuracy. The final threshold values were determined as those that most effectively preserved the integrity and detailed representation of the target structure. This approach ensured precise segmentation and minimised the inclusion of irrelevant regions.
The 3D model was transferred to SpaceClaim software (Version 22.0; ANSYS, Canonsburg, PA, USA). The geometry of the maxillary bone and teeth was modelled. By providing a 2-mm offset to the maxillary bone model, a 2-mm-thick cortical bone model was created (Xue et al., 2014). The inner surfaces of the adjusted 3D cortical bone were used as references to obtain trabecular bone structures. The teeth were modelled based on the Wheeler atlas (Wheeler, 1969). PDLs with a thickness of 0.25 mm were modelled based on the outer surfaces of the teeth (Cortona et al., 2020). All prepared models were placed in a 3D space with correct coordinates and the modelling process was completed using SpaceClaim software (Version 22.0) (Figure 1a–d).
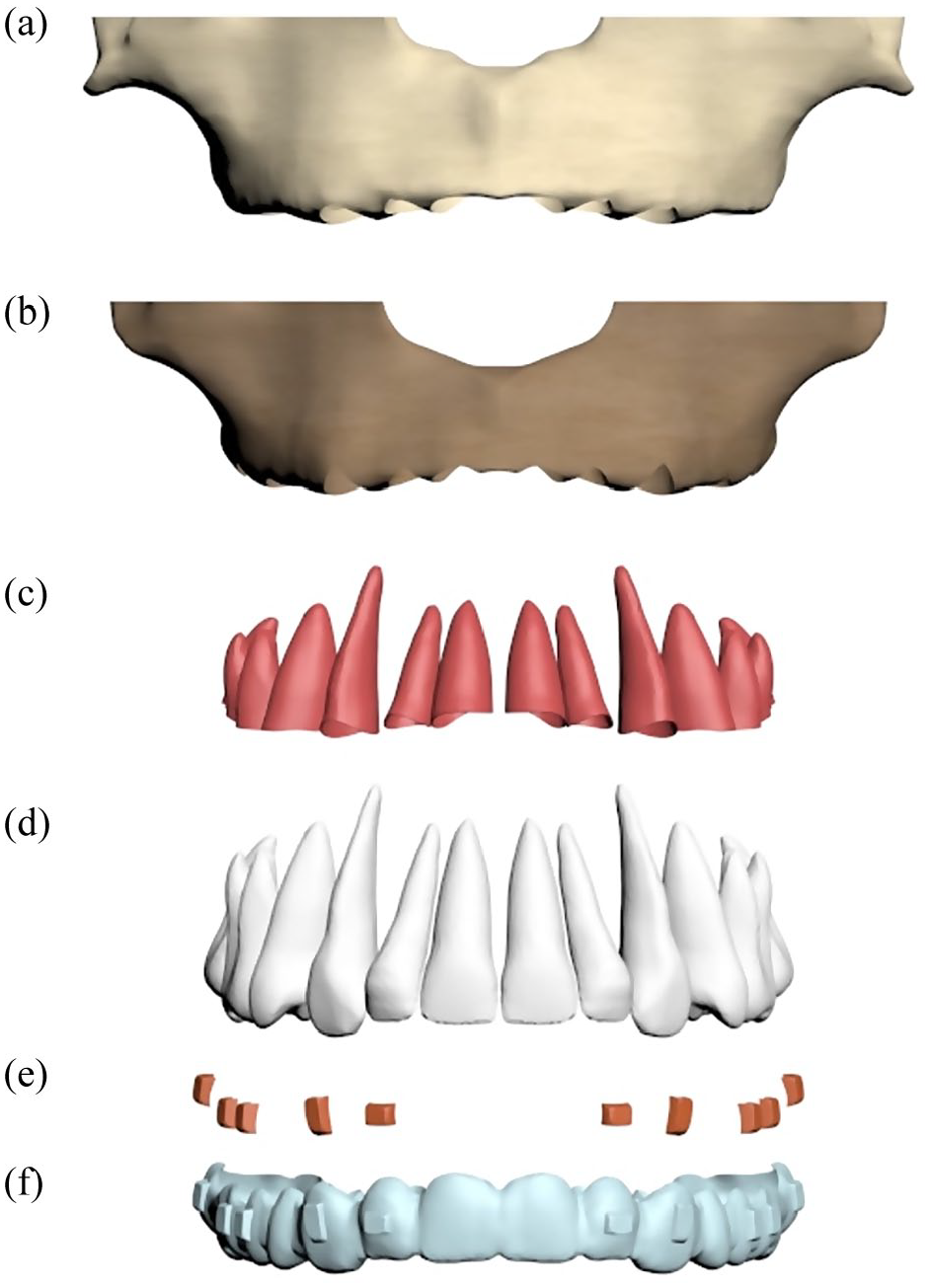
Demonstration of the model: (a) cortical bone, (b) trabecular bone, (c) periodontal ligament, (d) teeth, (e) attachments and (f) aligner.
The CA and attachments utilised in this study were modelled using SpaceClaim software (Version 22.0). The aligner had a thickness of 0.75 mm and completely covered the tooth surfaces. A CA was designed with an external offset of 0.5 mm (Cortona et al., 2020). A horizontal rectangular attachment, measuring 2 mm (height) × 3 mm (width) × 1 mm (thickness), was placed on the buccal surface of the lateral incisor. Vertical rectangular attachments, measuring 4 mm (height) × 2 mm (width) × 1 mm (thickness), were placed on the buccal surface of the canine, while attachments measuring 3 mm (height) × 2 mm (width) × 1 mm (thickness) were applied to the buccal surfaces of the premolars and molars (Figure 1e and f).
A total of 13 models were created, including one model without MOP and 12 models with different localisation, number, distance and depth MOPs (Table 1). The MOP diameter was determined as 1.5 mm. Buccal MOPs were created perpendicular to the buccal plate, and palatal MOPs were created perpendicular to the palatal plate. The MOPs’ locations were set at 3 mm from the alveolar crest in the buccal region and 4.5 mm from the alveolar crest in the palatal region for the first MOP. Both buccal and palatal MOPs were adjusted parallel to the crown–root axis and positioned at a 3-mm distance from each other. These models are shown in supplementary content.
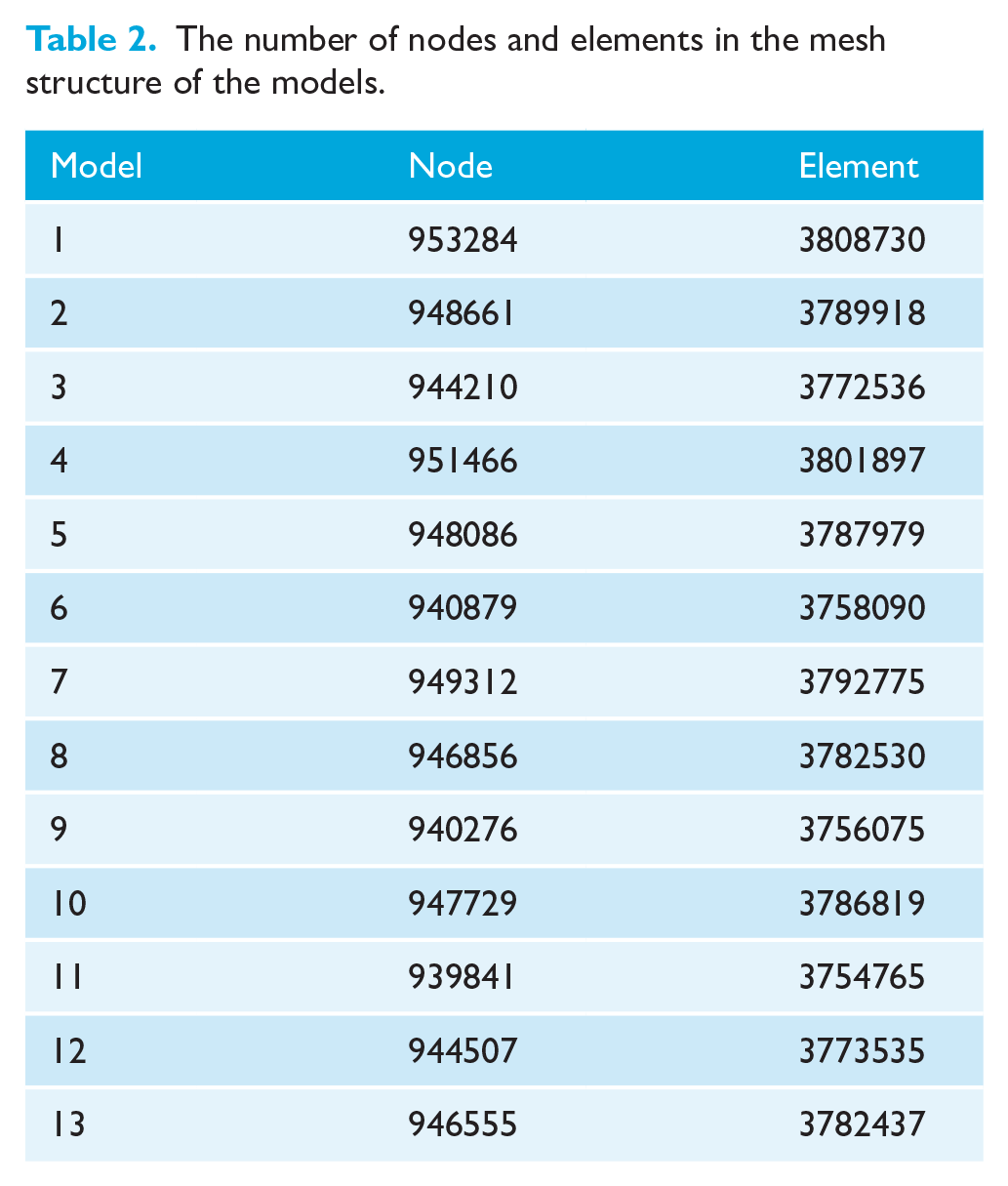
The FE models were transformed into mathematical models using Workbench software (Version 22.0; ANSYS). To create these mathematical models, highly sensitive tria mesh sizes in the range of 0.1–0.25 mm were utilised. After the surfaces of the models were generated with tria mesh structures, solid mesh structures were constructed using linear four-node tetrahedral elements. The number of nodes within the mesh structures is shown in Table 2. The models were then processed through the LS-DYNA solver.
The number of nodes and elements in the mesh structure of the models.
3D coordinate system and defining boundary conditions
In this study, the x-axis corresponded to the transverse plane, with positive movement indicating a shift towards the mesial side or tooth surface. The y-axis represented the sagittal plane, where positive movement was directed towards the palatal surface. Meanwhile, the z-axis was associated with the vertical plane, and its positive movement was oriented towards the alveolar bone.
The models were constrained by limiting all degrees of freedom at the nodal points in the bone’s upper region. A boundary condition was set to maintain symmetry along the X-axis, originating from the mesial area of the central tooth in the midline of the maxilla. This condition was consistently applied throughout the model, ensuring symmetry along the x-axis in relation to the y–z plane (Figure 2).
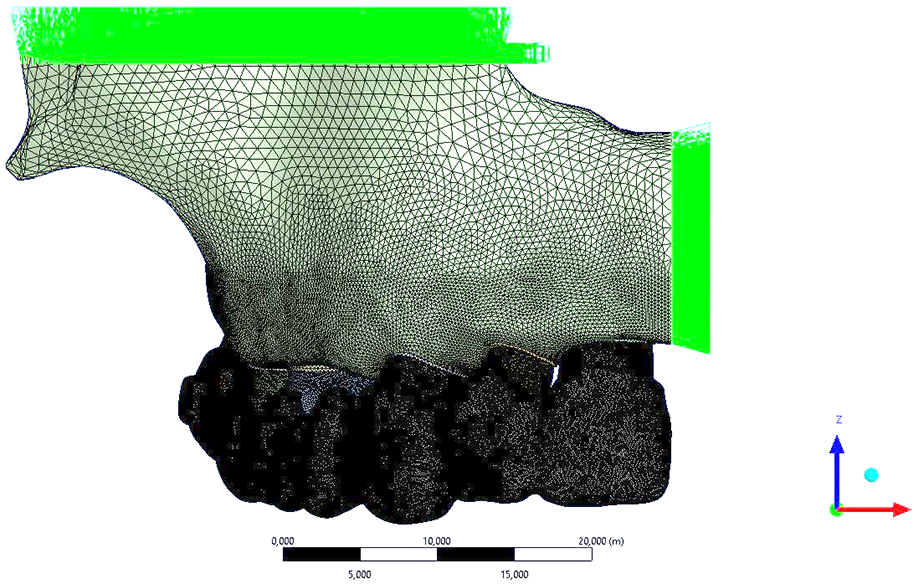
Boundary condition.
Material definitions and force loading
The linear material properties, such as the elastic modulus and Poisson’s ratio, are shown in Table 3. All materials in the models were assumed to be homogeneous and isotropic, with the PDL represented as a linear isotropic material (Jiang et al., 2020; Xu et al., 2018). A non-linear friction contact, with a coefficient of µ = 0.2, was applied at the aligner–attachment and aligner–tooth interfaces (Ramalho and Antunes, 2007). Bonded-type contact was established at the interfaces between the tooth and PDL, as well as the tooth and attachment, assuming that these elements would move in complete correlation during motion (Kaya et al., 2023).
Material properties used in the finite element model.
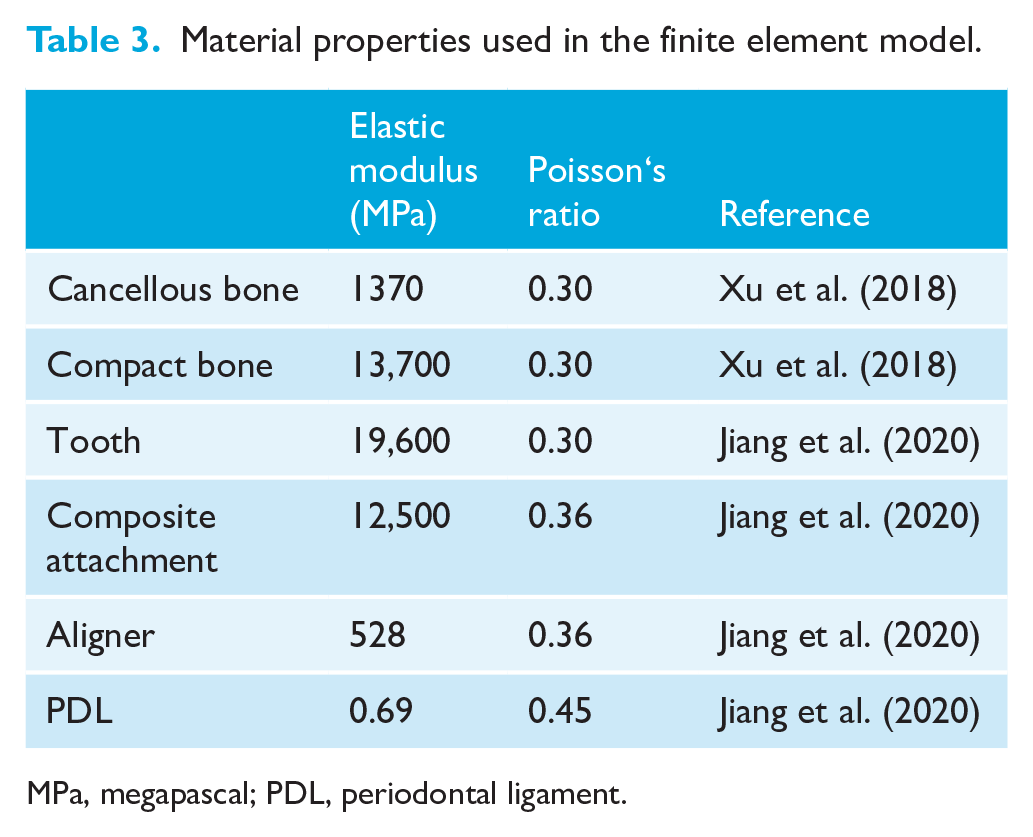
MPa, megapascal; PDL, periodontal ligament.
According to Li et al., the recommended range for aligner activation in canine distalisation using CAs is in the range of 0.21–0.24 mm, and the optimal stress and strain for effective canine distalisation were provided in this range (Li et al., 2022b). In all models, a distalisation force was applied perpendicular to the mesial (active) surface of the canine tooth attachment, simulating a 0.24 mm activation of the aligner in this study.
Results
Displacements
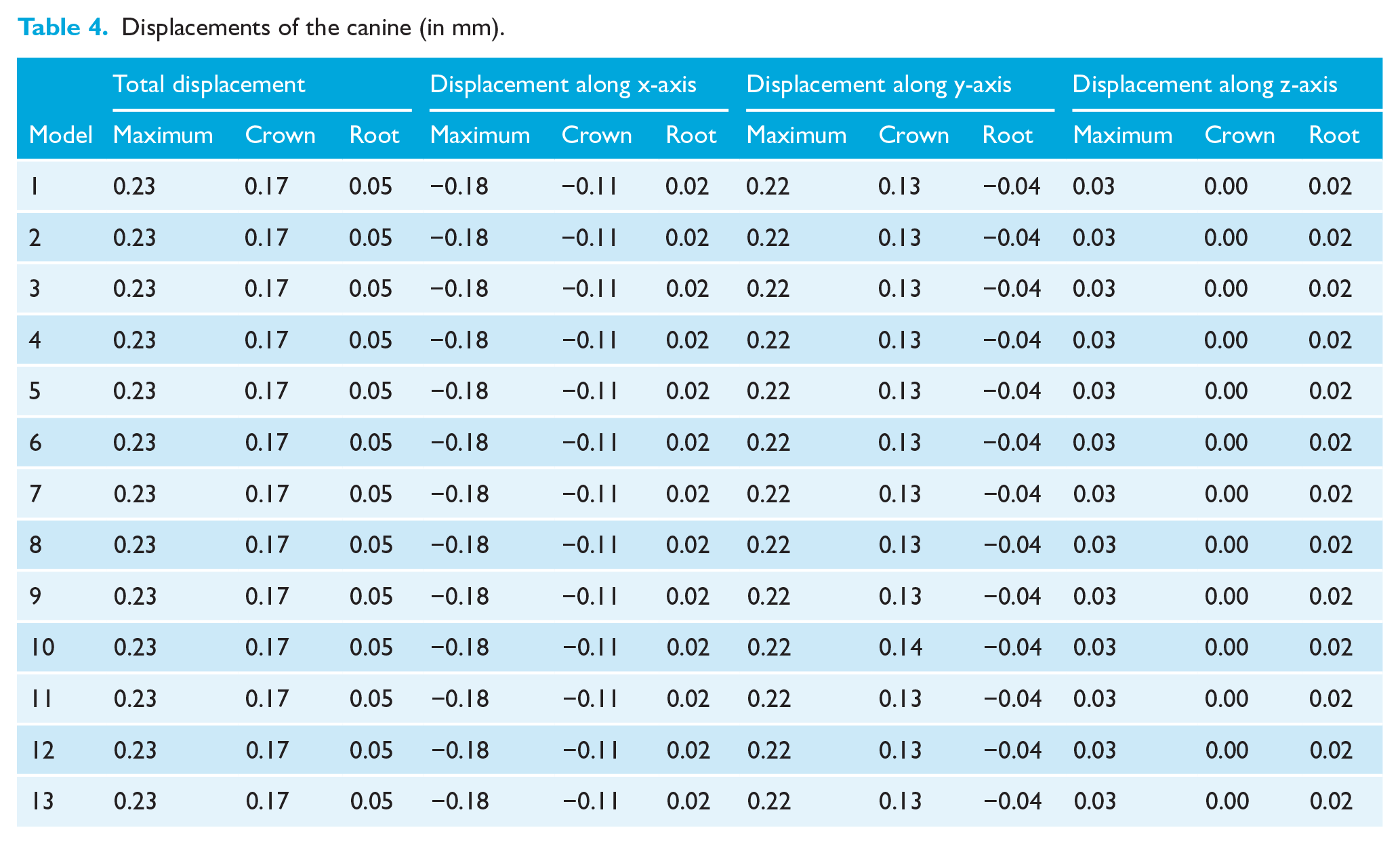
In addition to the total and axial displacements, the crown and root tip displacements are shown in Table 4 and Figure 3. All models demonstrated the maximum canine displacement of 0.23 mm, crown tip displacement of 0.17 mm and root tip of 0.05 mm.
Displacements of the canine (in mm).
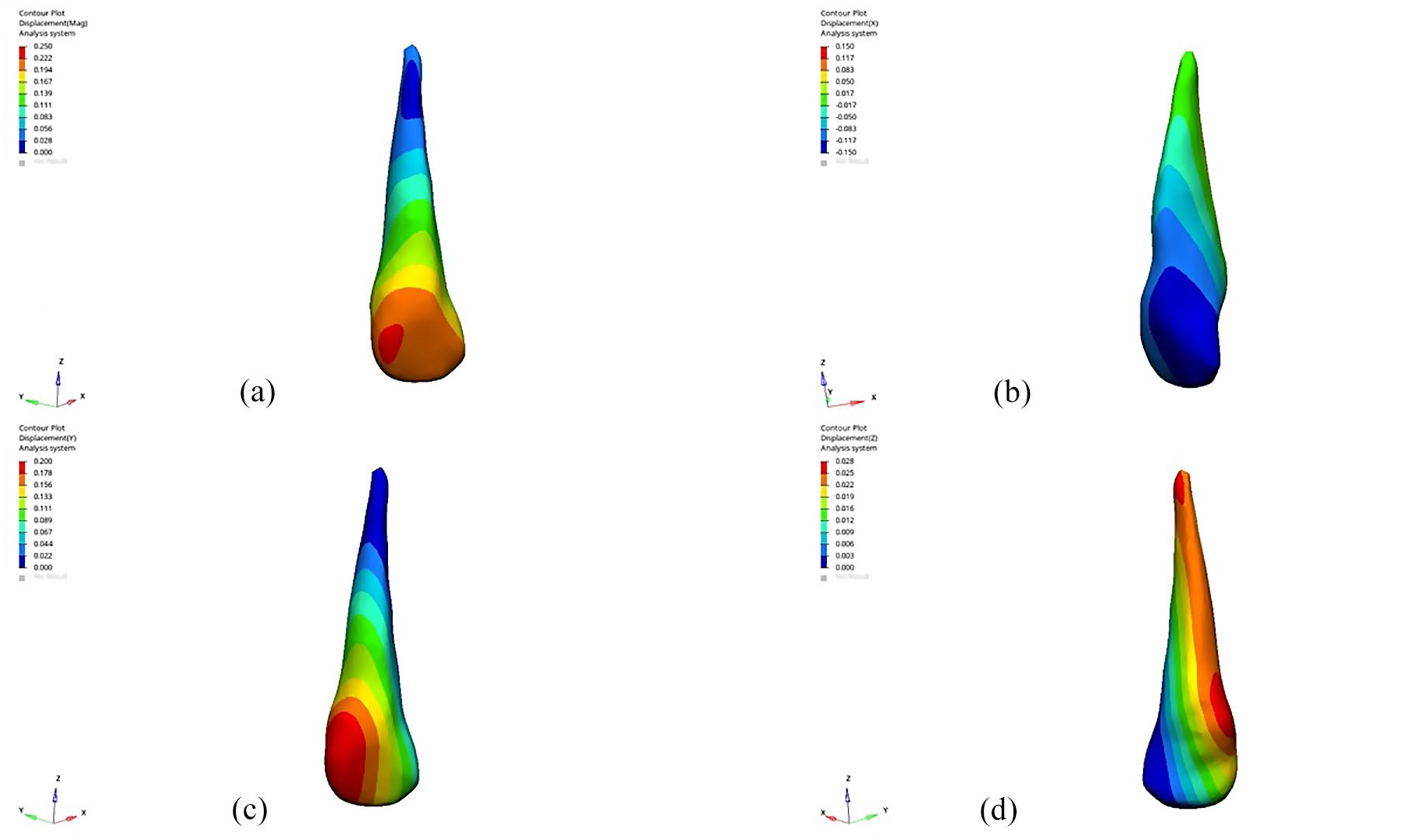
Displacements of canine: (a) total, (b) along the x-axis, (c) along the y-axis and (d) along the z-axis.
In all models along the x-axis, displacement was observed buccally at the mesio-incisal surface and mesial edge of −0.18mm (Table 4, Figure 3b). The canine’s crown tip displaced −0.11 mm buccally, and the root tip displaced 0.02 mm palatally along the x-axis
Comparing axis-based displacement, the y-axis showed the highest movement. In all models along the y-axis, displacement was observed distally at the distobuccal surface of the crown of 0.22 mm (Table 4, Figure 3c). The canine’s crown tip displaced 0.13 mm distally, and the root tip displaced −0.04 mm mesially along the y-axis.
In all models along the z-axis, the highest canine displacement involved intrusion movement of 0.03 mm at the gingival region at the disto-palatal collar of the canine (Table 4, Figure 3d). The tip of the root of the canine showed intrusion movement of 0.02 mm.
In all models, the maximum displacement of the aligner occurred in the gingivobuccal region of the first premolar and the distobuccal region of the canine, measuring 0.44 mm (Table 5, Figure 4).
Displacement of the clear aligner.
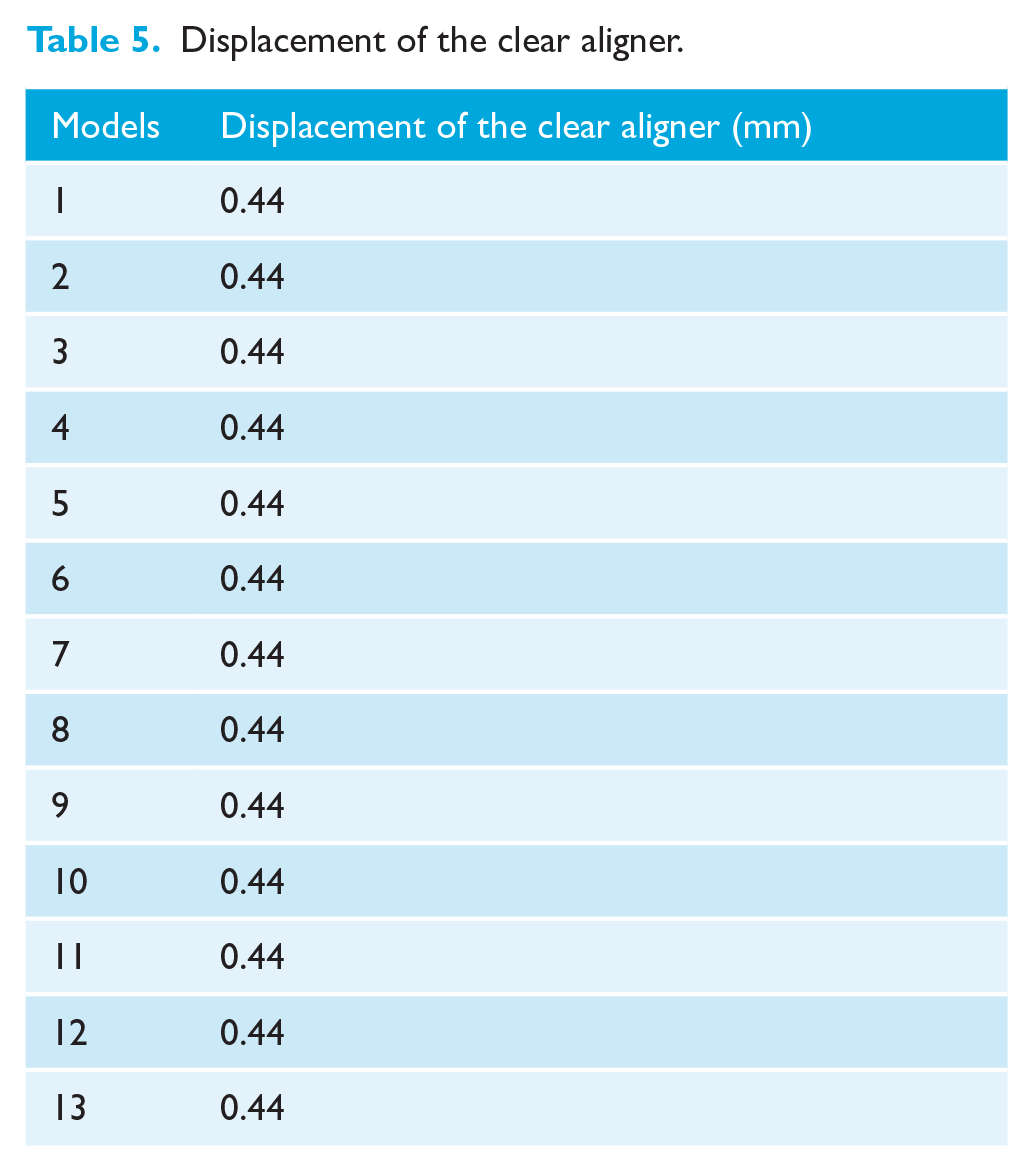
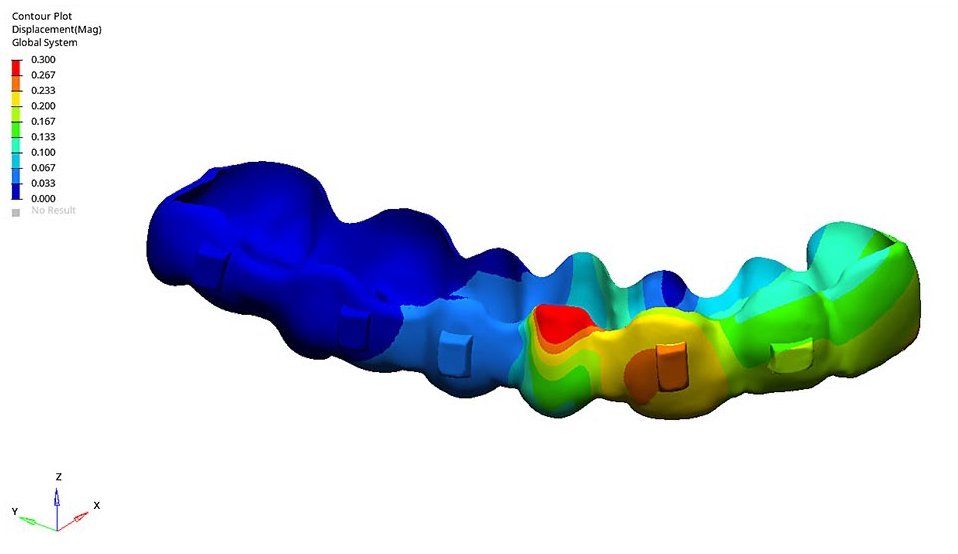
Displacement of the aligner.
Stress distributions
In all models, the highest maximum principal stress within the PDL was localised around the mesiobuccal collar of the canine crown. Principal stress analysis revealed consistent results across the models, with maximum principal stress values in the range of 1.30–1.31 MPa, indicating negligible variations. Similarly, the highest minimum principal stress was observed in the PDL surrounding the distobuccal collar of the canine crown, with values uniformly measured at −1.20 MPa across all models (Table 6, Figure 5a and b).
Principal stresses of the canine on the periodontal ligament.
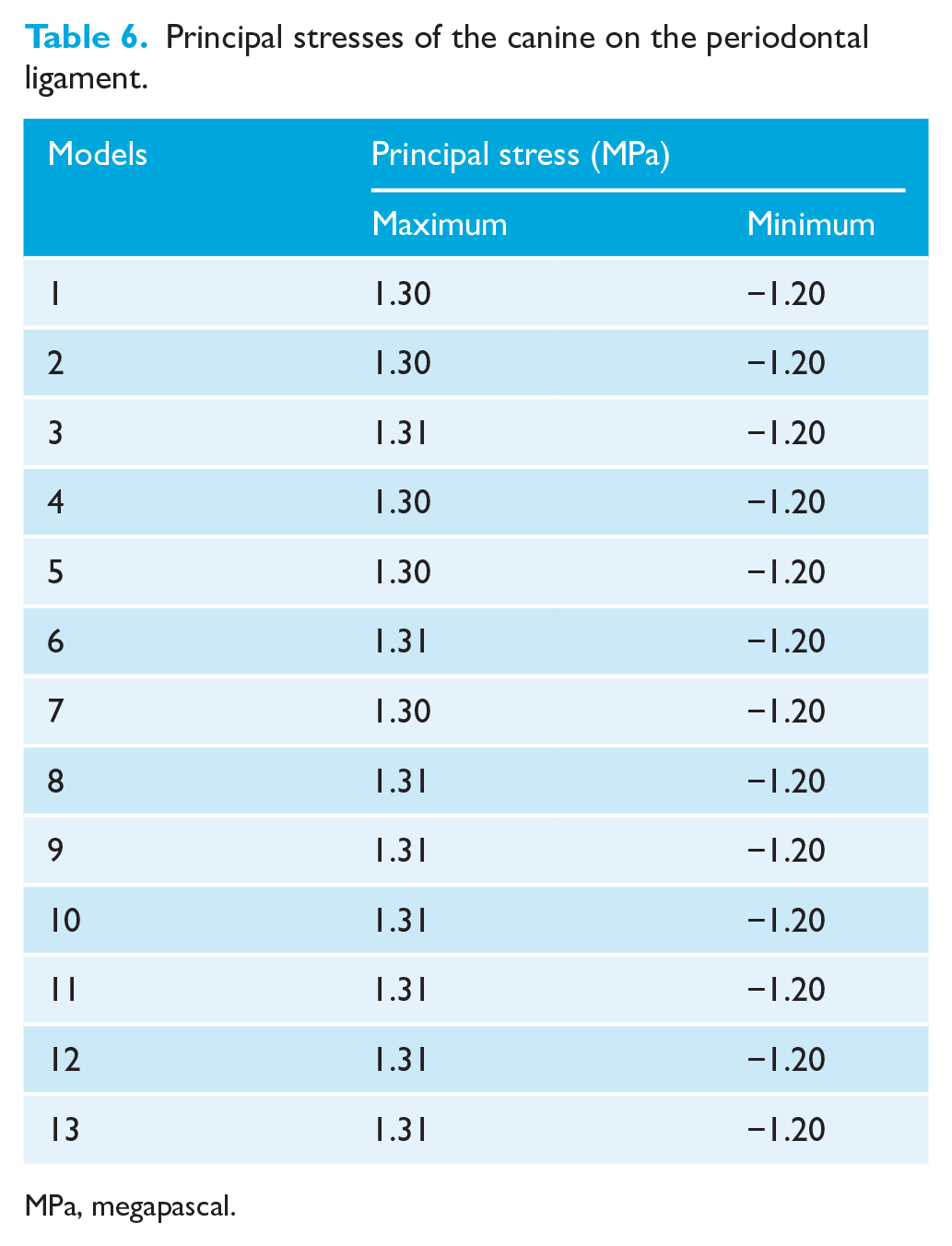
MPa, megapascal.
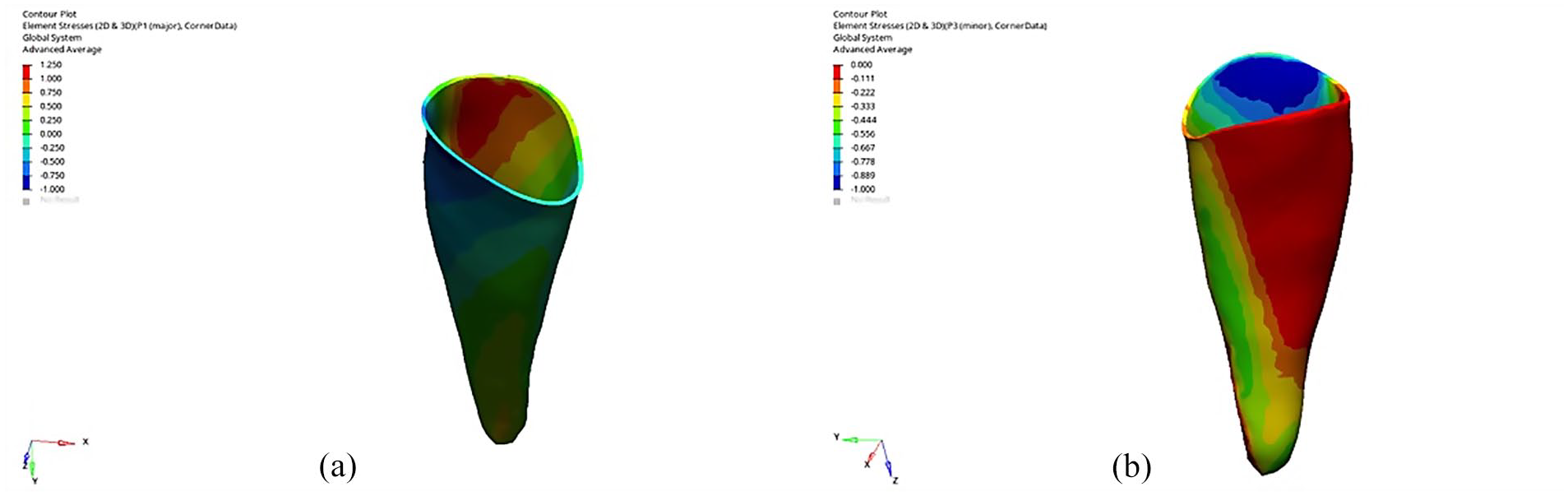
(a) Maximum and (b) minimum principal stress on the periodontal ligament.
Discussion
Summary
This study assessed the effects of various MOP approaches on canine distalisation using CAs through FEA. MOP studies have generally used fixed orthodontic treatment techniques on patients (Shahabee et al., 2020; Sivarajan et al., 2020) whereas this study specifically evaluated MOP approaches in CA treatment.
Generalisability
Our findings revealed that MOPs did not significantly alter tooth movement magnitude, stress distribution in the PDL or aligner deformation patterns, irrespective of the MOP parameters. Notably, canine movement consistently exhibited a tipping pattern across all tested MOP parameters. These results align with previous research suggesting that MOPs have limited or no clinically significant impact on accelerating tooth movement. Consistent with our findings, Alkebsi et al. (2018) and Aboalnaga et al. (2019) reported negligible differences in tooth movement rates after MOP application. This suggests that MOPs may not sufficiently modify the biomechanical environment to overcome the inherent resistance of dentoalveolar structures.
Mohaghegh et al. (2021) confirmed that MOPs increased the rate of canine retraction, reporting a standardised mean difference of 0.42 (95% confidence interval = 0.20–0.63) in their meta-analyses. These studies emphasise that although MOPs can enhance tooth movement rates, the clinical significance of these improvements remains limited in many cases. This meta-analysis highlights that MOPs can accelerate tooth movement, particularly in canine retraction treatments. However, in four split-mouth-designed studies with a low risk of bias, no significant difference in the rate of tooth movement was observed between MOP and control groups.
Conversely, studies such as Alikhani et al. (2013) and Feizbakhsh et al. (2018) documented a significant acceleration in tooth movement, with rates increasing up to 2- to 2.3-fold.
These discrepancies likely arise from variations in study design, including differences in MOP repetition, depth, number and application protocols. MOPs aim to induce localised bone remodelling through controlled trauma to stimulate RAP. Although repeated, more numerous or deeper perforations may theoretically enhance RAP, their clinical benefits remain uncertain. Increasing the magnitude of the trauma by repeated increasing of the number or depth of MOPs may amplify the inflammatory response or reduce bone resistance (Alikhani, 2017; Chang et al., 2012; Venkatachalapathy et al., 2022).
Studies examining repeated MOP applications highlight more pronounced benefits. Venkatachalapathy et al. (2022) demonstrated a two-fold increase in the rate of canine retraction when MOPs were applied every 28 days. This underscores the importance of maintaining a sustained biological stimulus to maximise the effectiveness of MOPs. Such sustained stimulation is particularly critical given the transient nature of biological responses, as observed in studies on cytokine dynamics. Although repeated applications show promising results, studies on single MOP applications, such as those by Mheissen et al. (2021) and Raghav et al. (2022), provide insights into the temporary nature of these effects. Mheissen et al. (2021) reported that, compared to the control group, MOPs significantly but temporarily increased the rate of lower canine retraction by 0.25 mm/month and en masse retraction by 0.31 mm/month. Similarly, Raghav et al. (2022) found that MOPs significantly accelerated tooth movement during the initial 4 weeks of treatment but noted diminishing effects thereafter, reinforcing the time-sensitive nature of these interventions.
This transient nature of biological responses, as highlighted by Mosayebi et al. (2023), further underscores the need for repeated applications to maintain efficacy. Mosayebi et al. observed that MOPs trigger localised osteoclast activity and elevate cytokine levels, such as IL-1 and TNF-α, which promote bone remodelling and orthodontic tooth movement. However, they also noted that inflammatory marker levels peak shortly after MOP application and decline within a few weeks, reducing the biological response—and, consequently, the acceleration of tooth movement—over time. The decline in inflammatory markers over time explains why sustained biological stimuli, achieved through repeated MOP applications, are essential to maintain consistent tooth movement acceleration.
A meta-analysis by Shahabee et al. (2020), which included six randomised controlled trials, observed that the difference in tooth movement varied from −0.02 mm to 0.87 mm when two or three MOPs were used. The authors reported that MOPs increased the rate of canine retraction by approximately 0.45 mm per month. Furthermore, comparisons between studies using two or three perforations revealed very similar results (0.45 mm/month vs. 0.42 mm/month mean difference, respectively), suggesting that increasing the number of perforations may not substantially enhance tooth movement. Among the studies reviewed, only the one by Feizbakhsh et al. (2018), which employed two MOPs, reported a difference of 0.62 mm in tooth movement after 28 days. However, Li et al. (2022a) observed that two MOPs did not result in a clinically significant increase in maxillary premolar space closure, highlighting variability in clinical outcomes.
In the literature, MOPs are generally applied buccally. However, Babanouri et al. (2020) investigated the effects of MOPs applied to both buccal and buccal-palatal sides. They found that although buccal-palatal applications produced slightly greater increases in orthodontic tooth movement compared with buccal-only applications, the differences were not clinically significant. Both groups exhibited tipping movements, with no significant difference in the amount of tipping observed.
The divergence in findings also underscores the critical role of MOP depth in determining outcomes. For instance, Alikhani et al. (2013) employed deeper perforations (up to 8 mm), which may have elicited a stronger regional acceleratory phenomenon (RAP). In contrast, Alkebsi et al. (2018) used shallower perforations (3–4 mm), which might have been insufficient to stimulate RAP effectively. Ozkan and Arici (2021) compared perforations of 4 mm and 7 mm and observed similar distalisation rates for both depths, suggesting that increasing perforation depth beyond a certain threshold may not yield additional benefits.
Patient-specific factors, such as bone density, healing capacity and orthodontic appliance types, likely contributed to the observed discrepancies. The variability in mechanics used for canine retraction complicates direct comparisons between studies. For instance, the included studies employed diverse biomechanical approaches, such as different archwires, devices and force application methods. Although NiTi springs provide continuous forces, chains deliver intermittent retraction forces, further contributing to the inconsistencies (Fu et al., 2019). Moreover, most comparisons in the literature are based on fixed orthodontic treatments, whereas our study uniquely evaluates canine retraction outcomes using CAs, representing a significant distinction.
Direct clinical measurements or 3D image scanning on study models are often used to evaluate canine retraction. However, differences in measurement methods and reference points used to calculate movement complicate comparisons across studies (Sivarajan et al., 2020). In this study, FEA enabled the calculation of displacements on the global coordinate system in all three axes under standardised conditions. Both crown and root tip measurements were used to evaluate distal tipping, ensuring more precise comparisons. The inconsistencies between this study and those reporting significant effects of MOPs can also be explained by differences in measurement methodologies. Some studies used cone-beam computed tomography (CBCT) (Aboalnaga et al., 2019) or direct clinical measurements (Sivarajan et al., 2019), while others relied on less precise methods, such as unstable reference points (e.g. lateral incisors, crown tips) (Alikhani et al., 2013). In addition, studies involving fixed appliances may have observed more localised responses to MOPs due to the direct application of force at brackets, whereas aligner systems distribute forces over larger areas, potentially reducing the localised effects of MOPs. Cortona et al. (2020) noted that deformation during CA treatment mainly occurs as a result of tooth movement. The most significant displacement was found in the gingivobuccal region of the first premolar and the distobuccal region of the canine. The reason why the deformation was seen, especially in the distobuccal region of the first premolar, may be that that region contained the extraction space and there was no tooth supporting the aligner.
These findings collectively underscore the nuanced effects of MOPs on orthodontic tooth movement. Although they generally accelerate orthodontic tooth movement, their effectiveness is influenced by procedural factors, patient-specific variables and measurement methodologies. Further high-quality studies are necessary to refine protocols and maximise the clinical benefits of MOPs.
Limitations
Biomechanically, this study revealed that MOPs did not significantly alter stress distribution or strain patterns in the PDL. The consistent tipping observed across all models can be attributed to the mechanical limitations of aligner systems, which exert distributed forces that may dilute the localised effects of MOPs. This finding aligns with studies by Golshah et al. (2021) and Babanouri et al. (2020), who reported similar tipping movements in their clinical and experimental evaluations. Biologically, MOPs aim to stimulate RAP by inducing localised bone remodelling through controlled trauma. However, the degree of RAP activation is influenced by the magnitude of the injury. Although deeper or more numerous MOPs may theoretically enhance RAP, they also increase the risk of adverse effects, such as PDL compression, hyalinisation and root resorption (Mheissen et al., 2021; Mohaghegh et al., 2021). These potential risks highlight the delicate balance between maximising efficacy and minimising invasiveness.
The models used in this study were uniformly homogeneous and isotropic with linear elasticity, unlike the complexity of in vivo situations. Therefore, a 100% in vivo environment could not be created. However, it has been stated that the results of FEA studies are similar to those of in vivo studies (Inan and Gonca, 2023). Intra-oral conditions, such as temperature and humidity, were not accounted for in the FEA. A significant constraint of this research is the evaluation of only mechanical aspects and not biologic factors. The limited clinical significance observed in our study may be attributed to the minimally invasive nature of MOPs, the focus on initial displacements without evaluating repeated applications, and the limitations of FEA in assessing the regional acceleratory phenomenon.
Interpretation
Implications for clinical practice
The findings of this study suggest that the routine use of MOPs in conjunction with CAs may not provide clinically significant benefits in accelerating treatment. Although MOPs might offer marginal advantages in specific scenarios, their overall impact on treatment efficiency appears limited, particularly when applied with aligners. Furthermore, the tipping observed in this study indicates that additional measures may be necessary to achieve parallel tooth movement.
Implications for research
To address these inconsistencies, future studies should focus on standardising MOP protocols, including depth, number and localisation, while accounting for patient-specific factors such as bone density and turnover rates. Combining FEA with well-designed clinical trials could provide deeper insights into the biomechanical and biological mechanisms underlying MOPs and refine their application across different orthodontic systems.
Conclusion
MOPs exerted negligible and clinically non-significant impacts on the biomechanical reactions of dentoalveolar structures. MOPs did not increase the initial displacement of canine distalisation.
Supplemental Material
sj-jpg-1-joo-10.1177_14653125251358834 – Supplemental material for Effects of various micro-osteoperforation approaches on canine and aligner displacements, and the stress in the periodontal ligament: A finite element analysis
Supplemental material, sj-jpg-1-joo-10.1177_14653125251358834 for Effects of various micro-osteoperforation approaches on canine and aligner displacements, and the stress in the periodontal ligament: A finite element analysis by Rauf Valıyev and Merve Gonca in Journal of Orthodontics
Footnotes
Acknowledgements
This article is based on RV’s dissertation titled ‘Evaluation of Different Micro-Osteoperforation Techniques in Canine Distalization with Clear Aligners Using Finite Element Analysis’, submitted in partial fulfilment of the DDS degree requirements. The data and materials utilised in this study were obtained from the Visible Human Project (The National Library of Medicine, FACT SHEETS Office of Communications and Public Liaison, Maryland, USA). Publicly available anatomical and CT images of female cadavers were used to develop the 3D finite element model employed in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding of this study was provided by the RTEU Scientific Research Projects (grant no. TDH-2022-1434).
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.