
Abstract
Objective:
To investigate clear aligner therapy (CAT) practice among orthodontists in the British Orthodontic Society (BOS).
Design:
A cross-sectional online survey.
Methods:
An electronic survey was distributed to members of the BOS in 2022. The survey comprised questions regarding respondent demographics, general use of CAT, the choice of proprietary CAT appliances, CAT planning, case selection, treatment protocols and orthodontist-reported CAT problems.
Results:
Overall, there were 233 (19.5%) respondants with the majority (n = 121, 53.1%) being female. Most respondents reported practising in England (n = 171, 74.7%). The majority (n = 177, 77.3%) indicated that they used CAT in their practice, with 48.1% (n = 81) treating 1–20 patients with CAT annually. The most frequently prescribed CAT system was Invisalign (n = 138, 81.2%). One to three changes to the initial digital treatment plan were made by 72.9% (n = 121) with final tooth positions being the most common reason for adjustment (64.4%). Most (n = 97, 60.3%) rarely or never performed premolar extractions with CAT. Of the respondents, 23 12.7%) reported that they always or mostly used a remote monitoring system in conjunction with CAT, with a wide range of aligner change protocols reported. The median number of months required to complete non-extraction CAT reported by the respondents was 12. Most respondents (n = 77, 51.7%) did not feel that CAT provides superior outcomes compared with fixed appliance therapy.
Conclusion:
CAT practice varied widely among the surveyed orthodontists. A predilection for the use of Invisalign and utility in less severe cases was noted.
Introduction
Since the introduction of Invisalign (Align Technology, Santa Clara, CA, USA) in the late 1990s, clear aligner therapy (CAT) has become increasingly popular (Weir, 2017). It offers the potential advantages of easier management of oral hygiene, more acceptable aesthetics and greater comfort compared with fixed appliance therapy (FAT), while also being amenable to remote oversight using tele-orthodontic technology (Hansa et al., 2020). Reported disadvantages associated with CAT include the requirement for patient adherence to prescribed wear protocols and the difficulty in addressing some features of malocclusion (Blundell et al., 2021; Gaddam et al., 2021; Meade and Weir, 2022).
The effectiveness of CAT in addressing severe rotations and in managing deep overbites has been questioned (Blundell et al., 2021; Gaddam et al., 2021; Meade and Weir, 2022). Most studies have alluded to a predictability of no more than 50% relative to simulated outcomes formulated as part of digital treatment planning (Haouili et al., 2020; Kravitz et al., 2009). These limitations have ensured that multiple refinements are commonplace, while hybrid approaches requiring completion with FAT are also occasionally used. Specifically, in a recent study, a hybrid approach with fixed appliances was needed to detail the outcome in 17% of cases with an average of 2.5 additional aligner scans needed in each case. The mean overall number of aligners was 64 with an average treatment duration of 22.8 months (Kravitz et al., 2023).
Data regarding CAT practices among dentists and orthodontists are limited. Recent investigations have suggested that CAT is provided by up to 93% of general dental practitioners and orthodontists in Australia, the United States, Canada and France (Abu-Arqub et al., 2023; Balteau et al., 2021; Keim et al., 2020; Meade and Dreyer, 2022; Meade and Weir, 2022). Despite the ubiquity of information related to CAT and the plethora of available CAT systems, detailed knowledge regarding CAT practices is lacking, with just one recent survey in Australia providing information in this regard (Meade and Dreyer, 2020; Meade and Weir, 2022). The aim of this cross-sectional survey was to investigate CAT practices and protocols among orthodontist members in the British Orthodontic Society (BOS).
Participants and methods
Ethical approval
Ethical approval was granted by Kings College London (MRA-22/23-33947) with prior approval from the BOS Clinical Governance Committee.
Questionnaire development
A cross-sectional, anonymous electronic survey (e-survey) was developed via the use of SurveyMonkey® (SurveyMonkey, San Mateo, CA, USA) software. The design and conduct of the survey aimed to align with the relevant guidance described by Burns et al. (2008) and Eysenbach (2004). The use of cookies on web browsers by the platform aimed to minimise the risk of repeat survey submissions by the same respondents.
Pilot questionnaire
A pilot e-survey was adapted, with permission, from a questionnaire distributed to members of the Australian Society of Orthodontists in May and June 2022 (Meade and Weir, 2022) by the authors and included pre-testing among specialist orthodontist colleagues.
Validity testing
The validity of the survey was determined by circulating the pilot survey and participant information sheet to four orthodontists (two hospital consultants and two specialist orthodontists) working in the UK or Republic of Ireland. The orthodontists provided feedback regarding the relevance and clarity of questions included, survey length and the time taken to complete the survey. The mean time reported by the orthodontists taken to complete the survey was 15 min.
Readability evaluation
The readability of the survey was evaluated using the Flesch Reading Ease score. A score of 41.4 indicated that it was difficult to read, but was appropriate for the target population.
Content of the finalised survey
The survey included the following parts: Part 1 related to the demographic details of the survey respondents. Part 2 explored the frequency of use of CAT within practice. Respondents who indicated that they did not use CAT were asked a series of questions regarding the reasons that influenced their decision not to use CAT (Part 9). Parts 3–8 were completed by only those reporting regular use of CAT and explored preferred systems (Part 3), digital treatment plans (DTP), case selection and treatment protocols (Parts 4–6), and refinement and respondent opinions (Part 7).
Population and sampling
The BOS is the sole national representative body for orthodontists and dentists with a special interest in orthodontics in the UK and includes orthodontists working in the Republic of Ireland among its membership (Oliver et al., 2020). In total, 1196 members of the Society’s Consultant Orthodontists’ Group, University Teachers Group, Community Group, Orthodontic Specialist Group and Training Grades Group were invited to participate by email in order to optimise response rates from the UK and Republic of Ireland specialist orthodontic profession. BOS members working in countries other than the UK or Republic of Ireland were not invited to participate. An expected response rate of 15%–20% was determined, as this aligned with targeted response rates in recent e-surveys among the same population (Ong et al., 2023).
Disseminating the survey
The BOS members were invited to participate by email, with a link to the survey, on 5 October 2022. Two email reminders (1 and 29 November 2022) followed, and the survey was closed on 16 December 2022. Survey responses were exported from the SurveyMonkey® Microsoft Excel (version 16.0; Microsoft, Redmond, WA, USA) spreadsheet for data cleaning and initial analysis. The responses from those identifying as non-specialist orthodontists were excluded from further analysis. The responses from the complete (n = 201) and incomplete (n = 32) surveys were assessed.
Statistics
Descriptive statistics were expressed in frequencies and percentages and were calculated via GraphPad Prism® (GraphPad Software Inc., La Jolla, CA, USA) statistical software. As the relevant datasets showed a non-parametric distribution, a Mann–Whitney test was carried out to determine whether there were any differences between respondents according to whether they worked in the UK or Republic of Ireland, based on the number of years in orthodontic practice. A chi-square test was also carried out to determine whether a difference existed in the provision of CAT between respondents working in the UK and Republic of Ireland.
Results
An overall response rate of 19.5% (n = 233) was recorded, with data from four respondents excluded as they were not specialist orthodontists. Not all respondents provided responses to every question and the percentages given related to the proportion of respondents who answered the relevant questions.
Demographics
Most respondents were female (n = 121, 53.1%) with the majority of respondents gaining their specialist orthodontic qualification in England (n = 171, 74.7%). Other respondents were trained in Scotland (n = 15, 6.6%), Wales (n = 13, 5.7%), Republic of Ireland (n = 6, 2.6%), Northern Ireland (n = 3, 1.3%) and other countries (n = 21, 9.1%). The majority of respondents practised in England (n = 174, 76.3%) with others being based in Scotland (n = 21, 9.2%), Republic of Ireland (n = 16, 7.0%), Northern Ireland (n = 11, 4.8%) and Wales (n = 5, 2.2%). The median number of years each orthodontist has practised as a specialist orthodontist was 19 (interquartile range [IQR] = 11–24 years). There was no difference in the number of years in orthodontic practice between respondents according to whether they worked in the UK or Republic of Ireland (P = 0.30), with most respondents (n = 125, 54.4%) working in a mix of private and National Health Service settings (Figure 1).
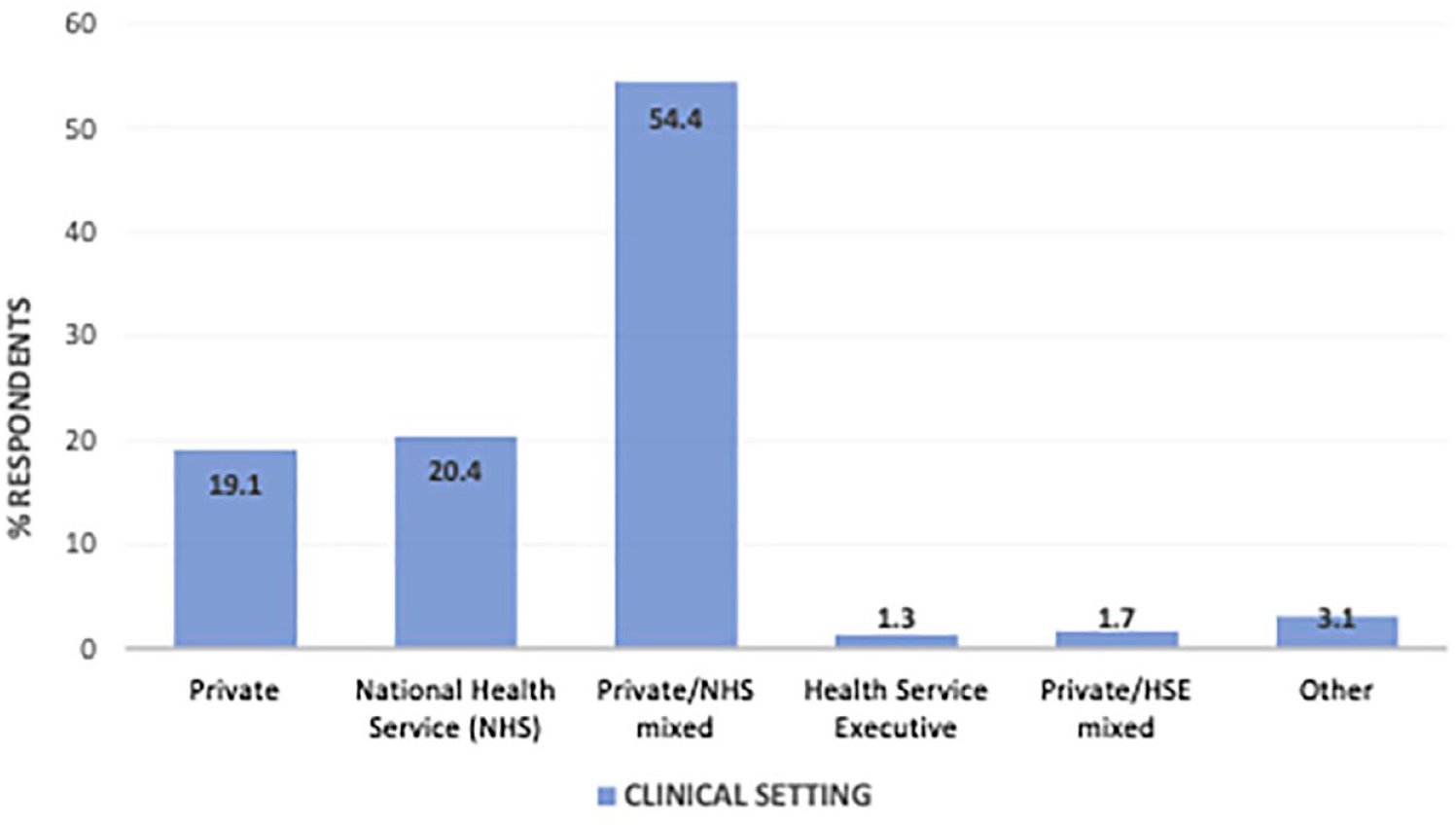
Clinical settings of respondents (n = 230).
Frequency of use of CAT
More than three-quarters (n = 177, 77.3%) of respondents reported using CAT. A chi-square test indicated there was no difference in the provision of CAT according to whether the respondents worked in the UK or Republic of Ireland (P = 0.52). The median percentage of annual caseload treated with CAT was 10% (IQR = 5%–35%), with no statistical difference between the UK and Republic of Ireland (P = 0.15). Almost half of the respondents treated 1–20 patients with CAT annually (Figure 2).
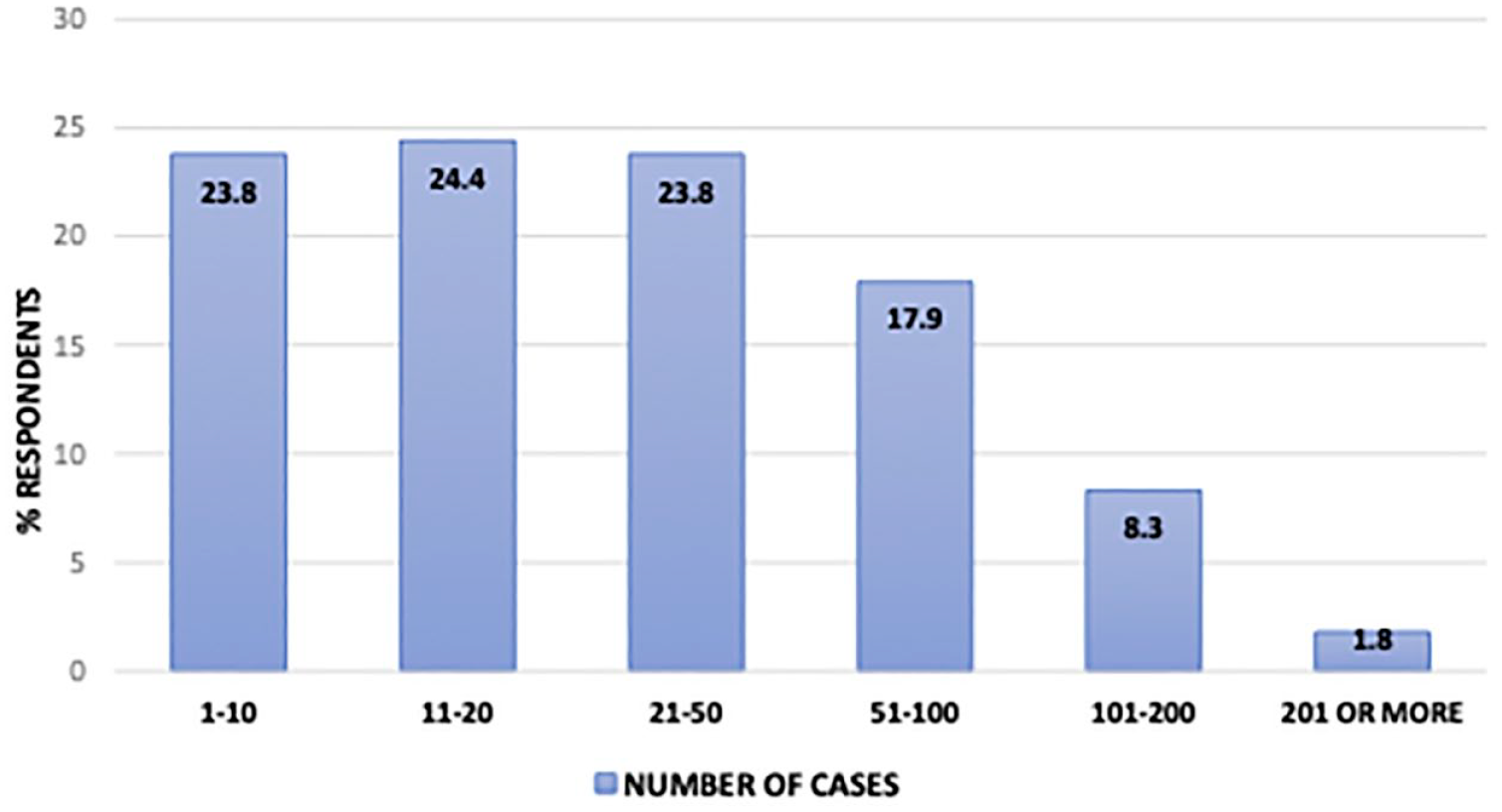
Number of cases treated with clear aligner therapy annually per respondent (n = 168).
Case complexity (79.9%) and predicted patient cooperation (83.4%) had a moderate or major influence on the decision to offer CAT (Figure 3). Adults were the patient cohort most commonly treated with CAT (Table 1).
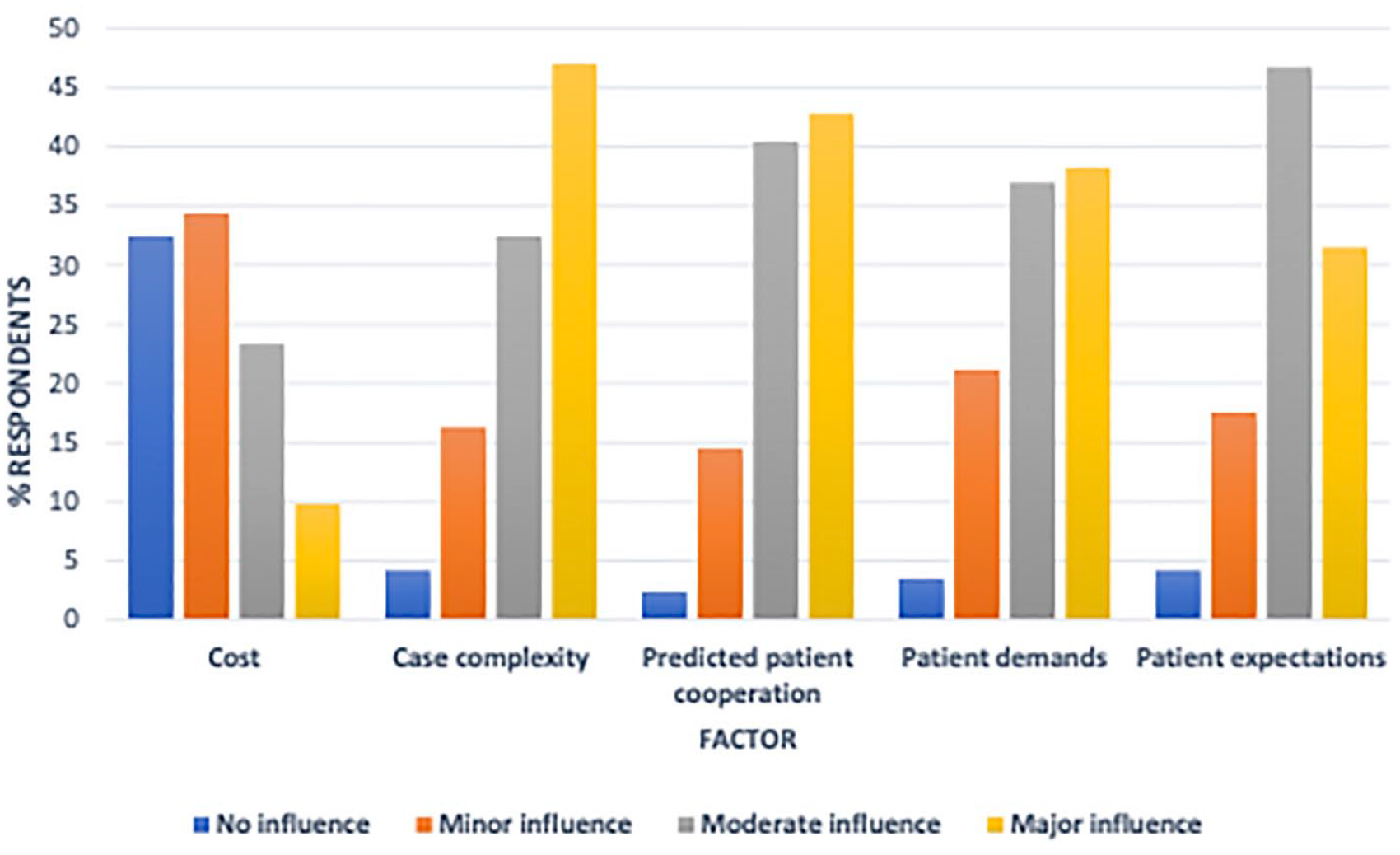
Factors influencing the decision to offer clear aligner therapy (n = 169).
Patient cohort treated with CAT (n = 169).
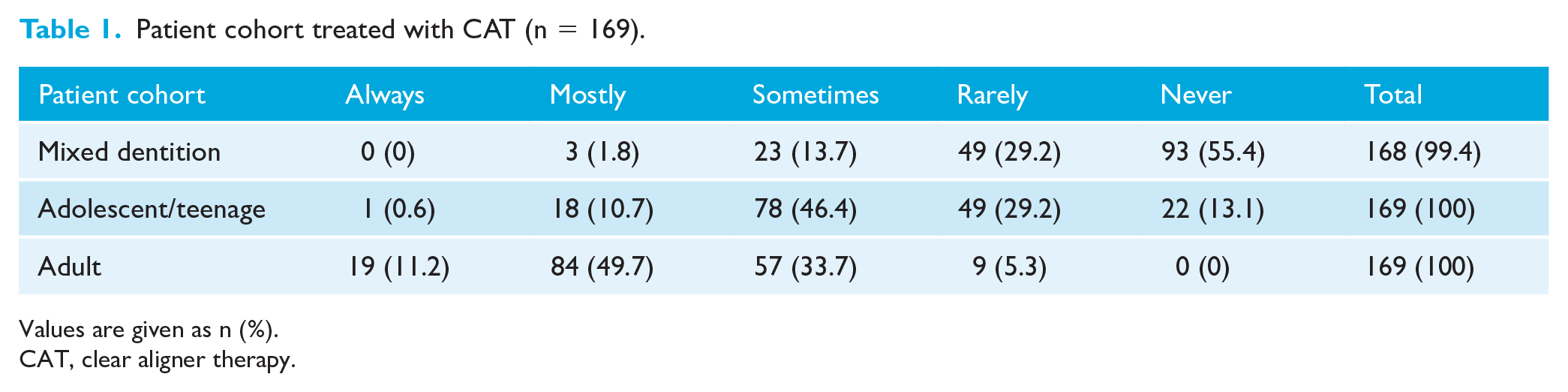
Values are given as n (%).
CAT, clear aligner therapy.
Preferred CAT systems
The most frequently prescribed CAT system reported by the respondents was Invisalign (Align Technology Inc., CA, CA) (n = 138, 81.2%), followed by Spark™ Clear Aligners (Ormco Corporation, Orange, CA, USA) (n = 18, 10.6%) and ‘InHouse’ aligners (n = 5, 2.9%). Approximately one-third (n = 54, 31.8%) of respondents reported that they used more than one CAT system, with 91.8% (n = 156) reporting that they used Invisalign and 20% (n = 34) used Spark™ Clear Aligners. The quality of DTPs and patient satisfaction influenced the choice of CAT provider (Table 2).
Factors that influence respondent decisions to use a CAT system provider (n = 169).
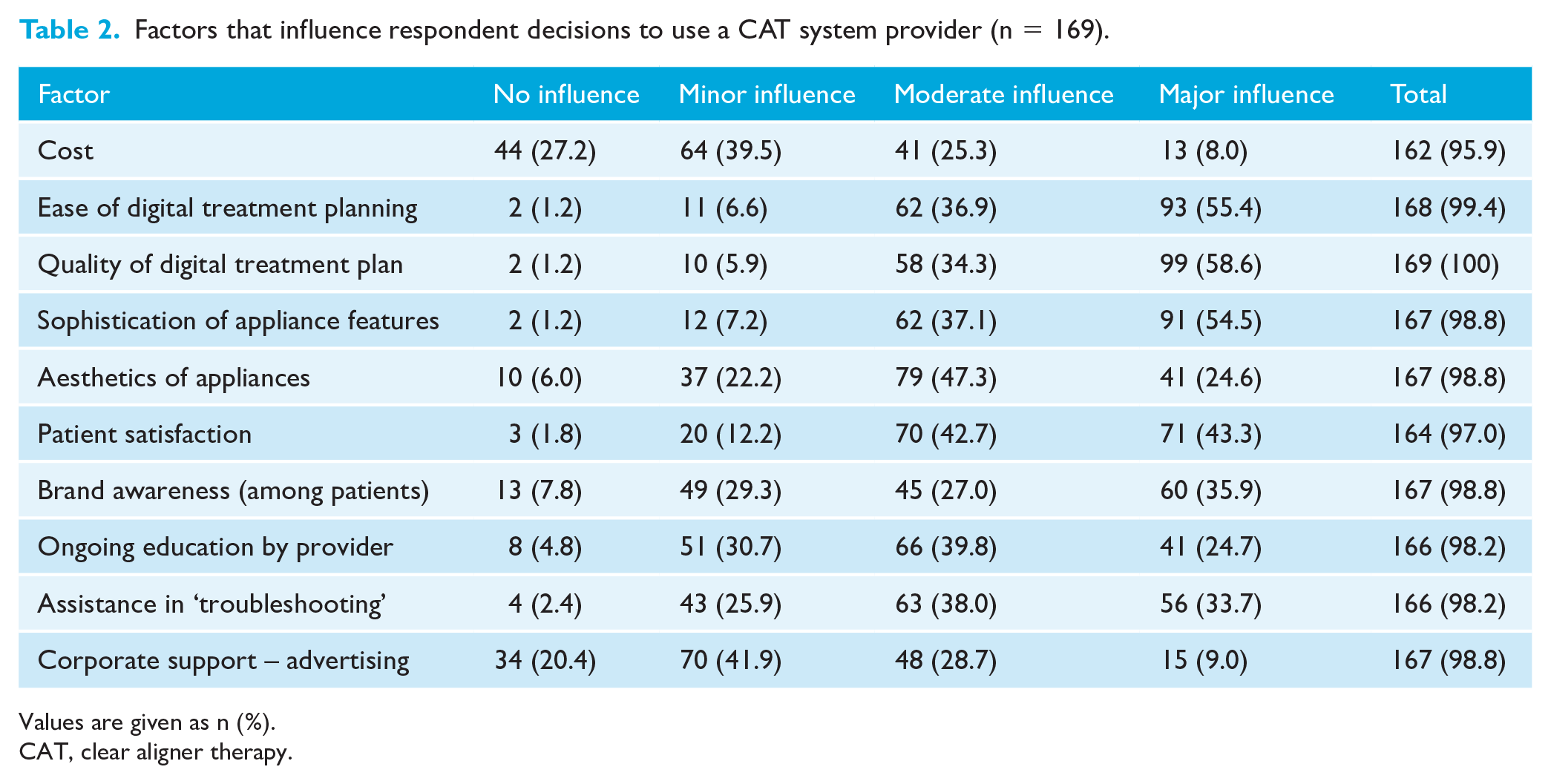
Values are given as n (%).
CAT, clear aligner therapy.
Digital treatment planning
Only 1 (0.6%) respondent reported routinely making no changes to the initial DTP, whereas 1–3 changes were typically made by 121 (72.9%) respondents, 4–6 changes by 39 (23.5%) respondents and >6 changes were made by 5 (3.0%) respondents before the acceptance of the initial DTP.
Aspects most in need of change from the initial DTP are presented in Figure 4. Among the ‘Other’ areas, 11 (6.6%) respondents reported issues regarding interproximal reduction amount and timing, and 5 (3.0%) respondents reported challenges with the planning of torque expression.
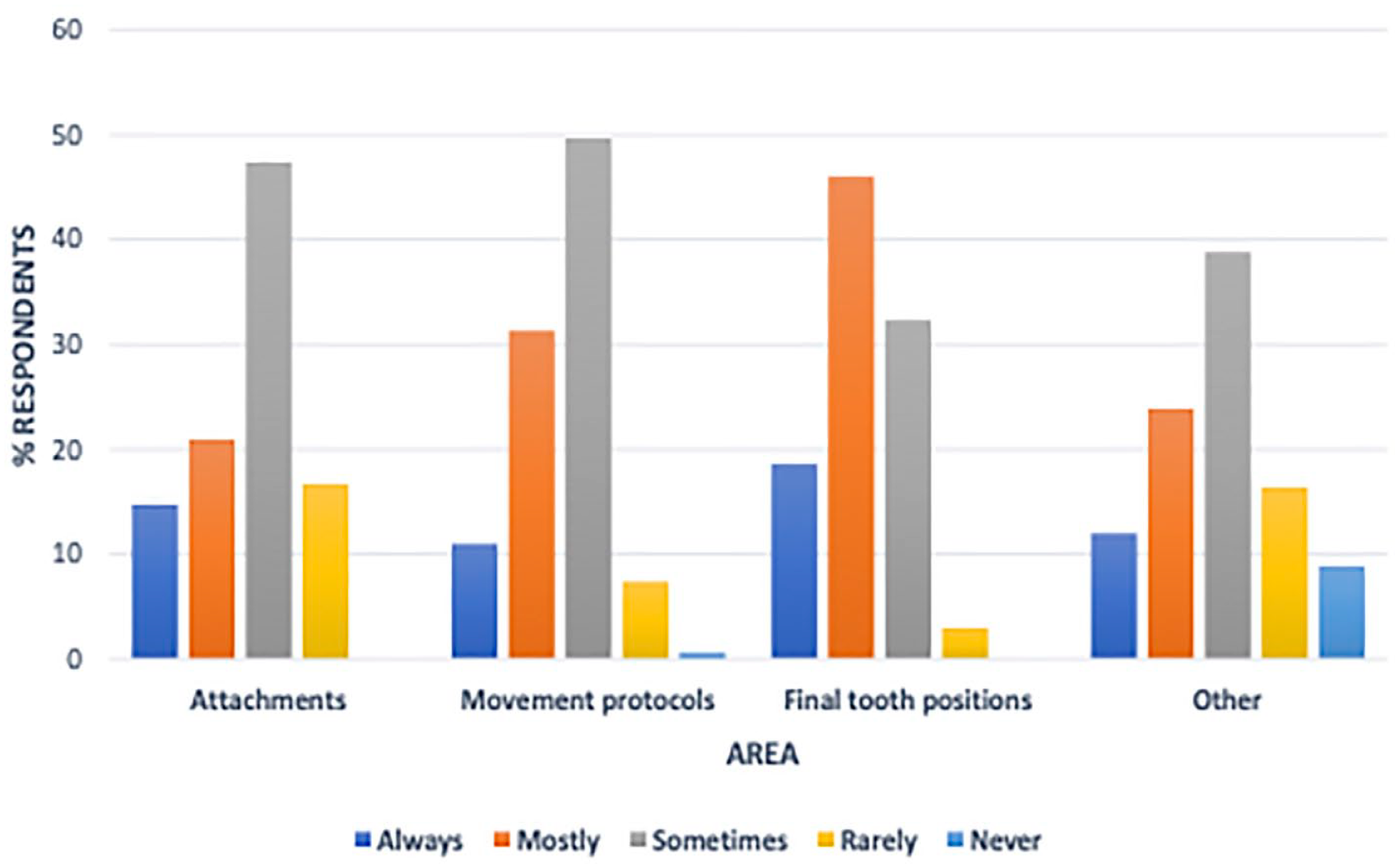
Areas most in need of change from the original digital treatment plan received from the clear aligner therapy provider (n = 166).
Case selection
Most respondents were comfortable treating spaced dentitions with CAT (Table 3). Among the ‘other’ case types, 5 (3.5%) respondents reported that they were not comfortable managing ectopic teeth with CAT. Table 4 shows that respondents appear to carry out CAT combined with lower incisor extraction more commonly than combined with premolar extractions and that CAT use in conjunction with TADs or orthognathic surgery was also limited.
‘Comfort ‘with treating different case types with or without premolar extractions.
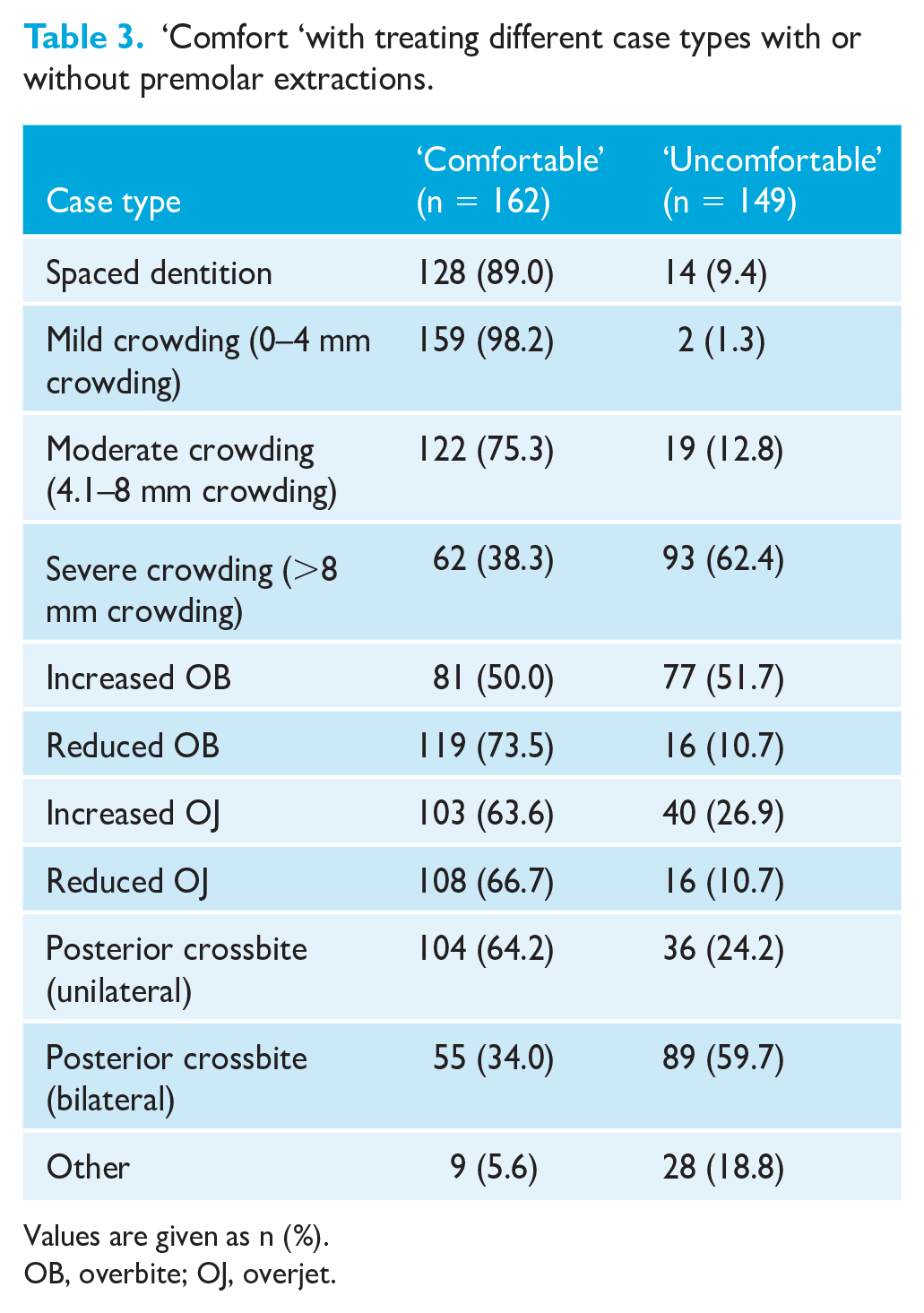
Values are given as n (%).
OB, overbite; OJ, overjet.
Treatment type treated with CAT (N=162).
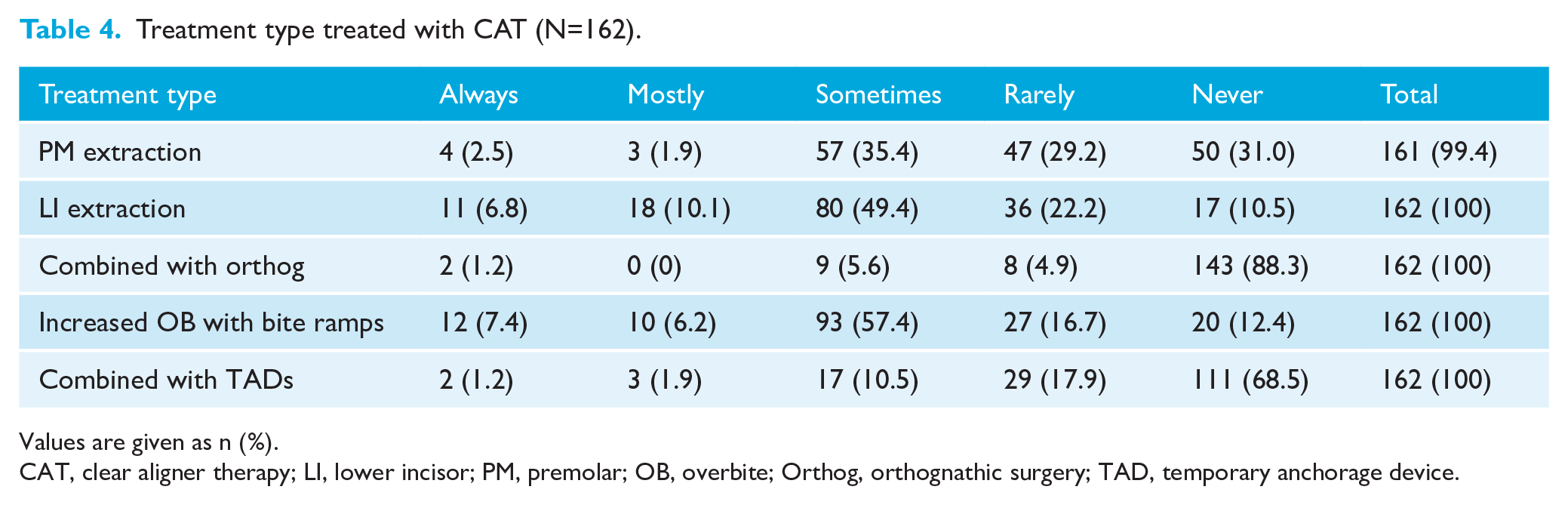
Values are given as n (%).
CAT, clear aligner therapy; LI, lower incisor; PM, premolar; OB, overbite; Orthog, orthognathic surgery; TAD, temporary anchorage device.
Treatment protocols
Just over one-quarter (n = 44, 27.9%) of the respondents reported that they sometimes combined CAT with FAT as part of the original DTP, while 44.3% (n = 70) rarely and 25.95% (n = 41) never combine CAT with FAT. A weekly change of aligners was most commonly recommended among the respondents for all patient cohorts (Figure 5). In addition, 5.7% (n = 9) of all respondents reported a change protocol that was informed by a remote monitoring system. Other protocols involved aligner change at periods ranging from 5 days to 4–5 weeks, with a recommended change every 10 days being reported by 20 (12.7%) respondents.
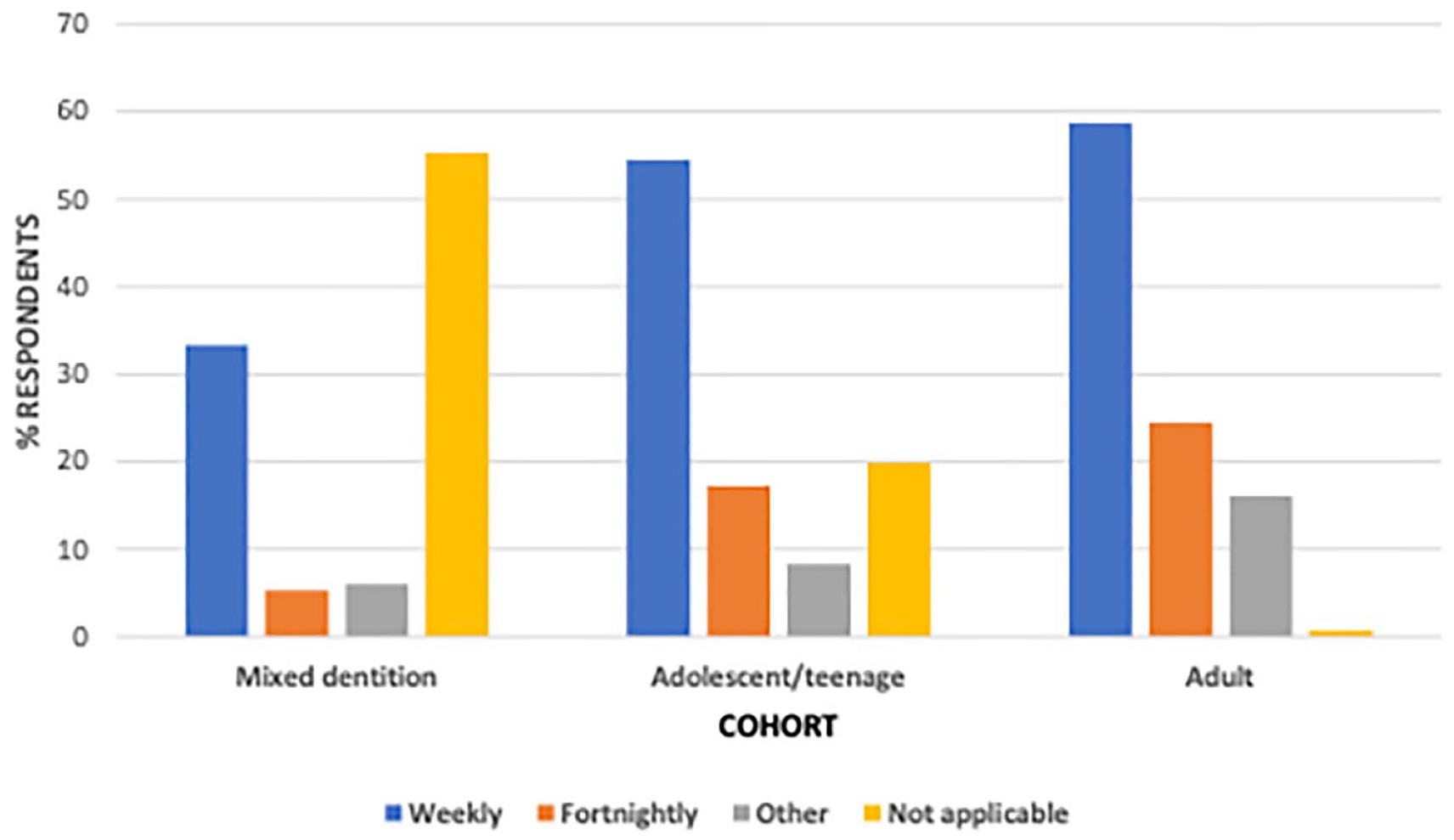
Frequency of recommended aligner changes among different patient cohorts by percentage of respondent (n = 158).
Almost half (n = 76, 48.1%) of the respondents reported that they recommended patients to attend the surgery for progress checks every 8 weeks compared with 17.1% (n = 27) and 15.8% (n = 25) who recommended checks every 6 weeks and 12 weeks, respectively.
Refinement
A median of 90% (IQR = 80%–99.3%) of CAT cases reportedly required a refinement phase, with the median number of reported refinements being 2. Just 1% (IQR = 0%–5%) of CAT cases were reported to require fixed appliances for completion. The majority of respondents (n = 103, 66.5%) reported never starting cases with FAT before changing to CAT compared to 34 (21.9%) who reported that they had done so in 1%–2% of cases and 12 (7.7%) in 2.1%–5% of cases. The median number of months required to complete dual arch non-extraction CAT reported by the respondents was 12 (IQR: 11–15 months).
Orthodontist opinions
Just over 20% (n = 45, 20.2%) (Table 5) of respondents reported that in matched cases (i.e. cases of similar complexity), CAT takes more time than FAT with just over half (n = 77, 51.7%) of the respondents disagreeing or strongly disagreeing that CAT produced superior outcomes, in the judgement of the respondents, in matched cases.
Respondent opinions regarding the treatment duration and quality of CAT and FAT.
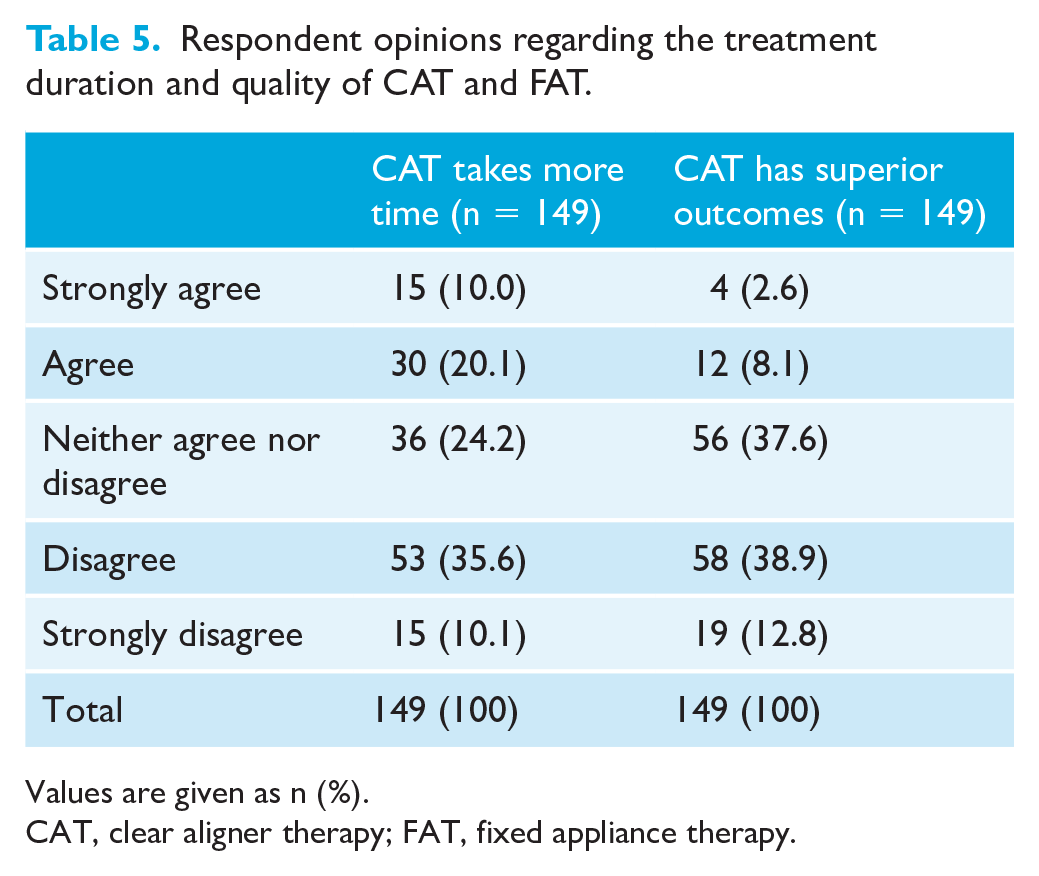
Values are given as n (%).
CAT, clear aligner therapy; FAT, fixed appliance therapy.
The clinical environment in which respondents practised was an important factor in the decision not to provide CAT (Table 6).
Factors that influence respondent decisions to not use CAT (n = 49).
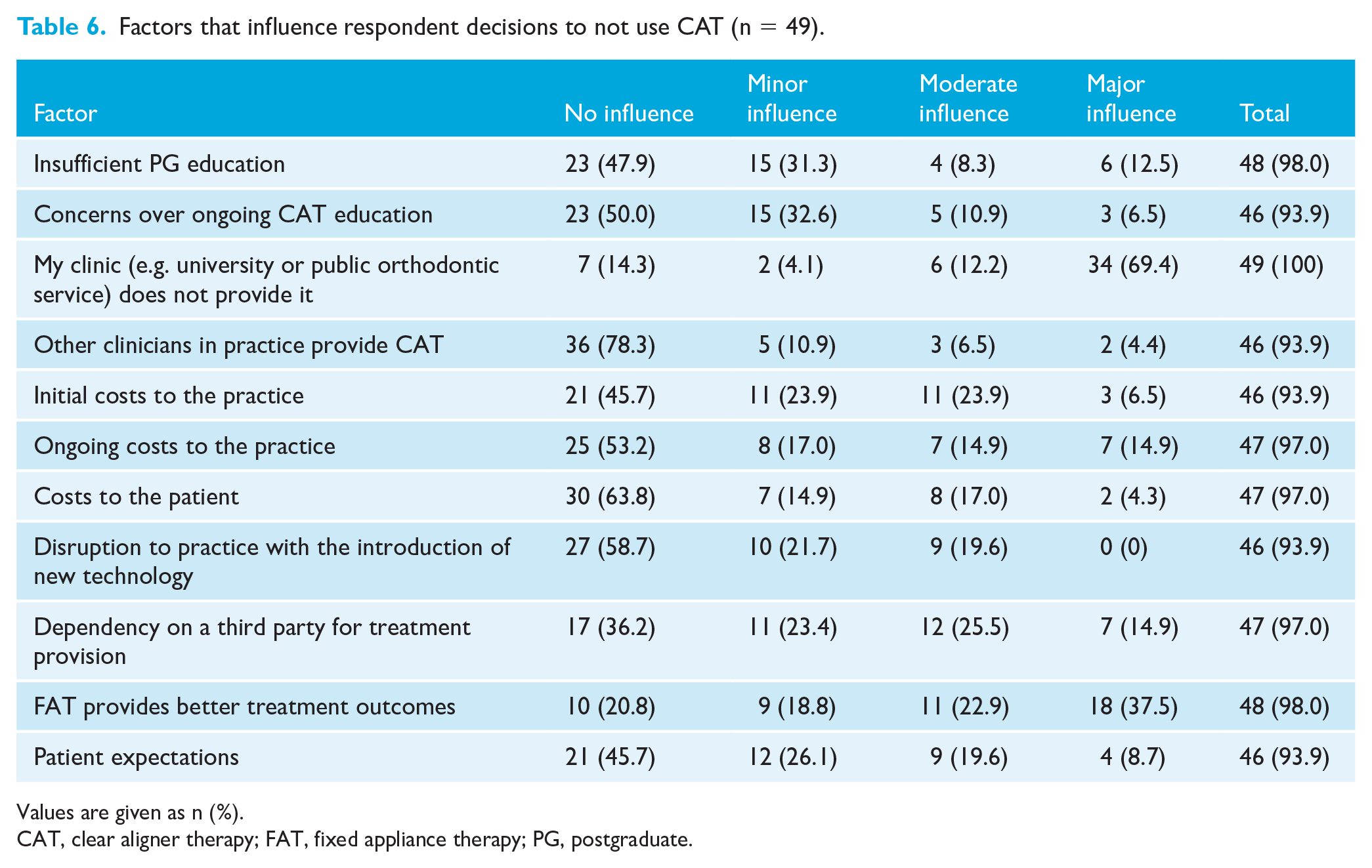
Values are given as n (%).
CAT, clear aligner therapy; FAT, fixed appliance therapy; PG, postgraduate.
Discussion
Summary
This is the first survey to investigate CAT practices and protocols among orthodontist members of the BOS. CAT was reported to be used by the majority of respondents in both the UK and Republic of Ireland, and respondents appear to prescribe it for approximately 10% of patients, with the majority of these being adults.
Comparison with other work
Although 77.3% of respondents reported that CAT was part of their treatment armamentarium, this figure was lower than the 92%–93% recorded in Australia and the United States. (Keim et al., 2020; Meade and Weir, 2022). This discrepancy may relate to the nature of orthodontic treatment provision in the UK and Republic of Ireland as over 80% of the respondents who did not provide CAT attributed this to their practice environment, including constraints associated with government-funded settings.
The surveyed respondents indicated that a median of 10% of their treatment caseload was managed with CAT each year. This contrasted with a mean of approximately 25% in Australia (Meade and Weir, 2022). Almost half (48.2%) of the respondents also reported treating just 1–20 cases of CAT annually. This suggests that respondents in the UK and Republic of Ireland may be later adopters of CAT than their counterparts in Australia. It may also explain why case complexity is an influence in almost 80% of the respondents’ decisions to offer CAT. For the respondents using CAT, the patient cohort most frequently treated with CAT were adults, who were treated ‘always’ or ‘mostly’ using this modality, by just over 60% of these respondents. Although this was less than the corresponding percentage of over 67% in Australia, it underscores the preference for more aesthetic orthodontic appliances among adults (Fenton et al., 2022).
Less than one-third of respondents reported using more than one CAT system, considerably lower than the 60% observed in the Australian study. The Invisalign system was the most frequently used CAT by over 80% of respondents in the present survey, exceeding the figure of 63% recorded in an Australian survey. The popularity of Invisalign in the present survey may, in part at least, be due to its strong brand recognition among patients (Kravitz and Bowman, 2016; Meade and Dreyer, 2022). More than 60% of respondents reported that brand awareness among patients was a moderate or major influence on their decision to choose a CAT system, compared to approximately one-third of respondents in Australia (Meade and Weir, 2022). Over 90% of the respondents acknowledged that the quality and ease associated with formulating DTPs significantly influences the decision to use a specific CAT provider. Virtually all respondents, however, required changes to the initial DTP before acceptance. This agreed with the findings reported by respondents in Australia and emphasises the clinician’s role in the DTP process. The respondents considered that a median of 90% of their cases required a refinement phase, which compared to a mean of 81.2% recorded in the Australian survey and 100% in a 2017 study (Best et al., 2017; Meade and Weir, 2022). A median of two refinements per case was reported by the respondents, again closely mirroring the findings from an Australian survey, which identified a mean of 2.1 refinements per case with slightly lower numbers (range = 0.8–2) identified in other recent studies (Hansa et al., 2020; Lin et al., 2022; Meade and Weir, 2022).
Most respondents reported that they were uncomfortable treating cases with severe crowding. This tallied with the responses regarding extractions and CAT, where over 60% considered that they rarely or never remove premolar teeth in association with CAT.
The most prescribed frequency of aligner change was weekly among the three patient cohorts. The range of aligner change protocols reported by the respondents in the present survey, however, suggested that many respondents consider that variation in the traditional 1- and 2- week aligner change protocols are appropriate for some patients. Most respondents who provided CAT did not feel that they produced superior outcomes compared with FAT. This reflected the findings from a recent systematic review and alluded to the challenges of obtaining orthodontic correction of some malocclusion traits (Blundell et al., 2021; Gaddam et al., 2021; Papageorgiou et al., 2020). Almost one-quarter of the respondents in the present survey reported combining CAT and FAT as part of the initial DTP. While a higher proportion (50%–60%) did this routinely in Australia and the United States (Keim et al., 2020; Meade and Weir, 2022), universally clinicians appear to be using their knowledge of the advantages and limitations of each system adopting a ‘hybrid’ approach. This may become increasingly ingrained as the relative merits of each approach are increasingly recognised (Kravitz et al., 2022).
Limitations
The low response rate was a potential limitation in the present survey. It was comparable to recent surveys involving the responses of 15%–20.1% of BOS members in the UK and 1.6%–18.1% in international studies concerning orthodontic practice protocols (Abu-Arqub et al., 2023; Balteau et al., 2021; Keim et al., 2020; Oliver et al., 2020; Ong et al., 2023; Prithiviraj et al., 2023). Responses, however, were received from respondents working in a wide range of geographical locations and clinical environments, suggesting that the findings are likely to be externally valid.
Researchers, nevertheless, should consider the use of additional types of surveys in addition to online surveys and/or pre-contacting potential respondents in future surveys to improve response rates (Wu et al., 2022). An additional limitation is the risk of those who use CAT being more likely to respond to the survey risking recruitment bias and overestimation of the use of CAT among respondents.
Strengths
A strength of this investigation is the undertaking of pretesting and piloting of the survey before dissemination to ensure its validity and acceptability. In addition, the use of aspects from a similar survey conducted in Australia enables comparison with that country and provides baseline data for future research into CAT practices among orthodontists in the UK and Republic of Ireland and globally.
Implications for clinical practice
In addition to patient opinion and clinical research, clinician practices such as those determined in the present survey are essential to informing evidence-based practice. As such, and particularly in the absence of relevant data among orthodontists in the UK and Republic of Ireland, the findings of the present study are valuable as they provide new insight into relevant practices among orthodontists in the two countries.
Implications for research
Future research is required to ascertain how factors such as the recency of acquirement of specialist orthodontic qualification, length of CAT experience and the different clinical environments in the UK and Republic of Ireland influence CAT practices among orthodontists in the two countries. Additional investigation, ideally using qualitative methodology, is required to determine why orthodontists choose treatment modalities, such as combined CAT and FAT treatment, in some situations.
Conclusion
The majority of survey respondents in the UK and Republic of Ireland provided CAT with a wide variation of treatment numbers and protocols reported by the orthodontists. Overall, approximately 10% of cases were treated with aligners. The most frequently prescribed CAT system by the respondents was Invisalign, with approximately one-third reporting they used more than one system. Over 60% rarely or never performed premolar extractions with CAT. Respondents who did not provide CAT indicated that their practice environment precluded CAT as a treatment option. Most respondents disagreed that CAT provide superior outcomes compared with FAT.
Footnotes
Acknowledgements
The authors gratefully acknowledge the members of the BOS who participated in the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this cross-sectional survey was granted by Kings College London (MRA-22/23-33947).