
Abstract
Introduction:
This survey was undertaken as a second part to ‘Barriers to Post-CCST training in orthodontics: A survey of trainee perceptions’. Recruitment of Post-CCST trainees in certain areas of the country has attracted concerns as it has become increasingly difficult. This survey was undertaken to assess trainee satisfaction with Post-CCST training and to look at possible ways to improve trainee satisfaction and make Post-CCST training more desirable.
Methods:
The Training Grades Group (TGG) committee of the British Orthodontic Society (BOS) produced an online survey that was sent to all TGG members and newly qualified consultants in May 2021. All Post-CCSTs who entered training between February 2017 and October 2020, were asked to complete the survey.
Results:
There were 37 respondents, which gave a response rate of 62%. While 61% of respondents were satisfied with their Post-CCST training, 17% were ‘neither satisfied or dissatisfied’ and 6% were either ‘dissatisfied’ or ‘very dissatisfied’. Of the 37 respondents, 25 (67%) would apply for Post-CCST training again, 6 (16%) would not and 6 (16%) did not answer this question. When asked for possible suggestions for improvements to Post-CCST training to encourage greater satisfaction, the responses could be grouped into the following themes: Part-time training; Teaching; Time commitment; Salary; and Experience.
Conclusion:
In general, respondents were satisfied with Post-CCST training. There was a significant range of positive and negative responses to various aspects of training including multidisciplinary team clinic preparation, support, supervision and management experience. Suggestions for improvements echo the barriers to Post-CCST training survey.
Keywords
Introduction
This survey was undertaken as a second part to ‘Barriers to Post-CCST training in orthodontics: A survey of trainee perceptions’.
To be registered with the General Dental Council (GDC, 2022) as a specialist in orthodontics, a dentist is required to undergo specialty training on an approved three-year full-time (or equivalent part-time) specialty training programme or show equivalence via mediated entry, although this pathway is currently paused. Once training has completed, the trainee is issued with a Certificate of Completion of Specialist Training (CCST). To be eligible for appointment as a National Health Service (NHS) consultant, a further two-year full-time (or equivalent part-time) Post-CCST training programme needs to be undertaken.
In the recent survey on barriers to Post-CCST training (Quach et al., 2021), the reasons behind this decline in applications has been attributed mainly to financial, geographical and personal factors. There were concerns about the intensity of training in 58% of respondents and job satisfaction as a consultant was a concern for 50% of respondents.
Recruitment of Post-CCST trainees, in certain areas of the country, has attracted concerns as it has become increasingly difficult. Along with the short-term difficulties in terms of service provision, there is the long-term consequence on the consultant workforce. Between February 2015 and September 2022, there were 14 rounds of national recruitment for Post-CCST in orthodontics, 12 of which were left with vacant posts (Table 1).
Post-CCST fill rate from September 2015 to the present.
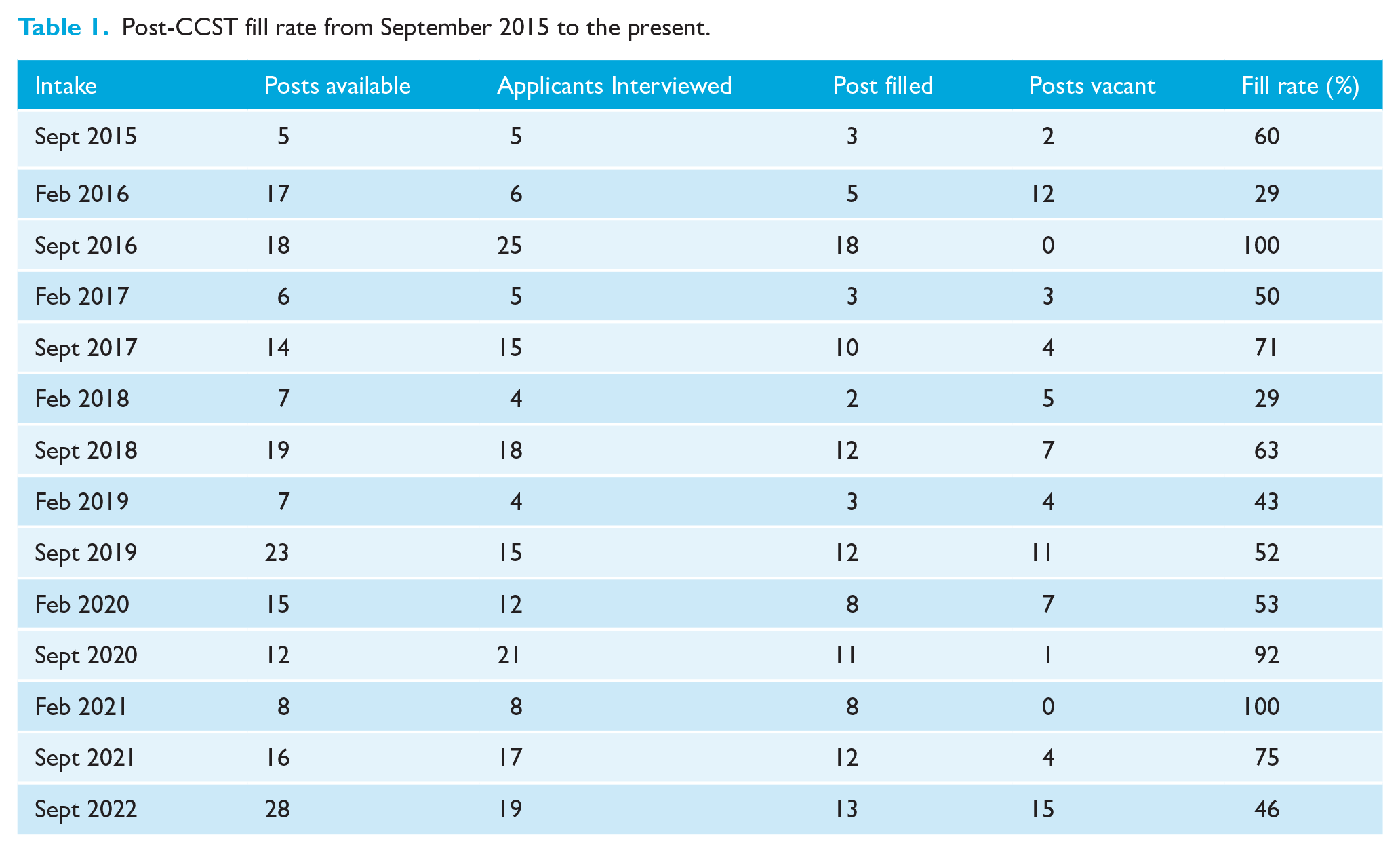
The overall ratio of consultant headcount versus whole time equivalent (WTE) within orthodontics has been increasing, indicating an increasing number of consultants employed on part-time contracts between 1997 and 2019 (Quach et al., 2021); therefore, there is a need for more consultants to enter the workforce.
This survey was undertaken to assess trainee satisfaction with Post-CCST training and to look at how to improve Post-CCST trainee satisfaction and make Post-CCST training more desirable.
The aims of the survey were as follows: (1) to ascertain motivation for applying for Post-CCST training; (2) to assess working patterns and if this has an impact on training; (3) to compare the difference in trainee rota and if this is in line with Specialty Advisory Committee (SAC) recommendations; (4) to assess trainee satisfaction in relation to teaching, case mix, work load, study leave, support and supervision, and management experience; and (5) to explore potential changes to make Post-CCST training a more desirable option.
Methods
The British Orthodontic Society (BOS) Training Grades Group (TGG) Committee developed a survey with input from the Consultant Orthodontic Group (COG). Approval was obtained from the BOS Clinical Governance Directorate.
The survey was piloted by three Post-CCST trainees and adjustments were made to the questions before distribution following feedback.
TGG membership includes trainees who are Post-CCST and Pre-CCST. The survey was set up on an online platform (www.surveymonkey.co.uk) and an access link was sent to the TGG mailing list as well as COG mailing list to include newly qualified consultants. Two reminder emails were sent two and four weeks after the initial link was sent. The survey was completed anonymously. The survey was open for completion between May 2021 and June 2021. The survey link (now closed) can be found online (https://www.surveymonkey.co.uk/r/GSPZB97).
Participants
All Post-CCSTs who entered training between February 2017 and October 2020 were invited to complete the survey. Those who started around the time of October 2020 would have been in training for approximately six months at the time of the survey. Those who had started after October 2020 were not asked to participate as they would not have undergone a significant amount of training to truly comment on training. To capture newly qualified consultants, those who entered training after February 2017 were asked to complete it. These newly qualified consultants would have been consultants for a maximum of 18 months at the time of survey.
Results
Sample
From TGG records, there were 60 trainees/newly qualified consultants who were eligible to participate in the survey. There were 37 respondents (30% men, 70% women), which gave a response rate of 62%.
The majority of respondents (41%) were in their second year of training, followed by first year of training (27%). Newly qualified consultants made up 24% of the respondents and there was a small number of trainees (8%) who were in their ‘period of grace’, where they have passed their exam and completed the minimum time required in training and are currently still in their training post while they seek a consultant post.
Of the participants, 4 (11%) were on run-through posts. When asked about working patterns, 89% were working full time, 8% were less than full time (LTFT) and 3% were part-time.
Motivation for applying for Post-CCST training
Free-text boxes were given when asked about motivation to applying for Post-CCST training. The most popular themes were the desire for further training and wanting to treat more complex/MDT cases. Other popular themes included wanting to work in a hospital setting, job variety, and delivering teaching and training. Table 2 shows examples of comments made by participants.
Motivation for applying for Post-CCST training.
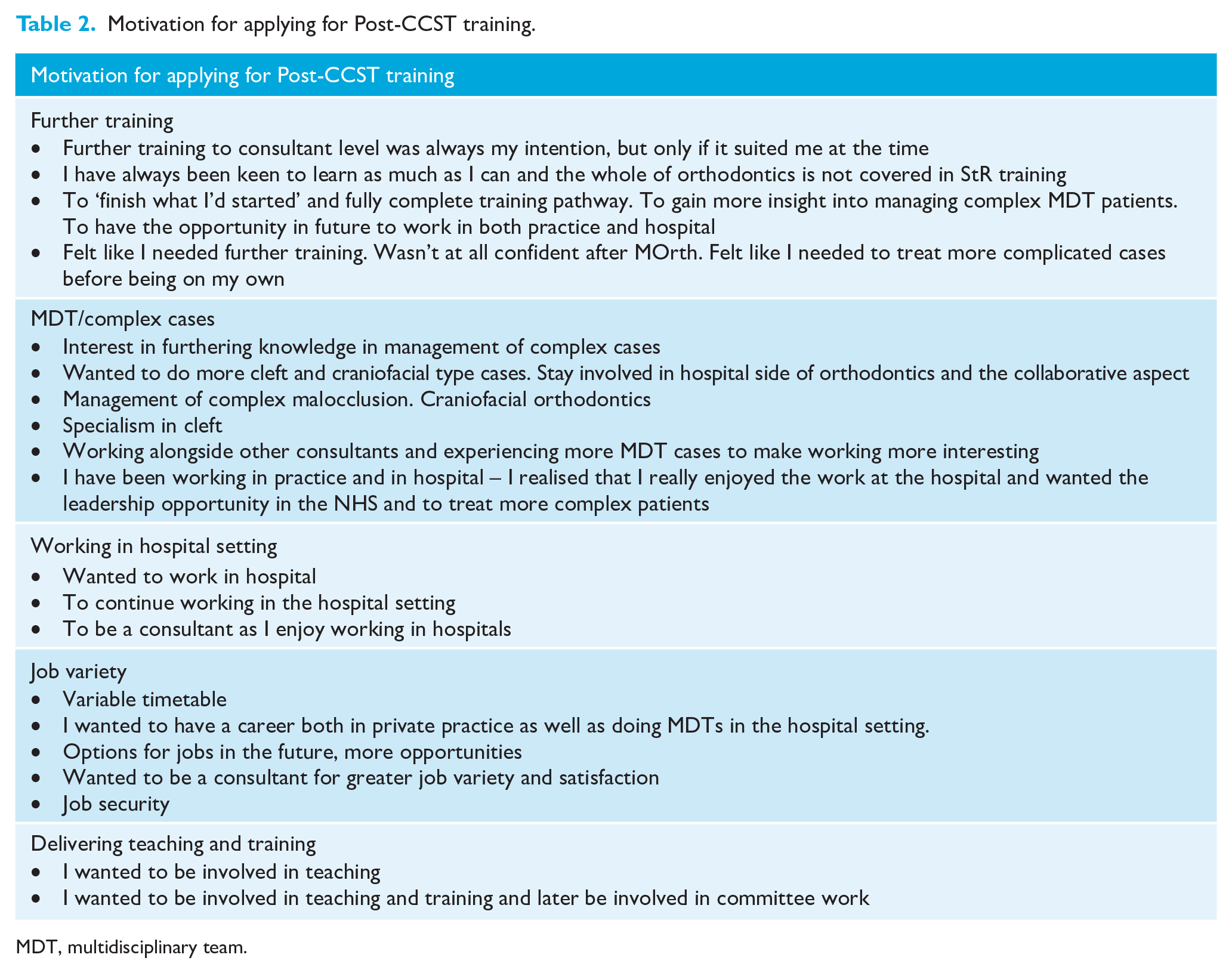
MDT, multidisciplinary team.
Hesitations in applying to Post-CCST training
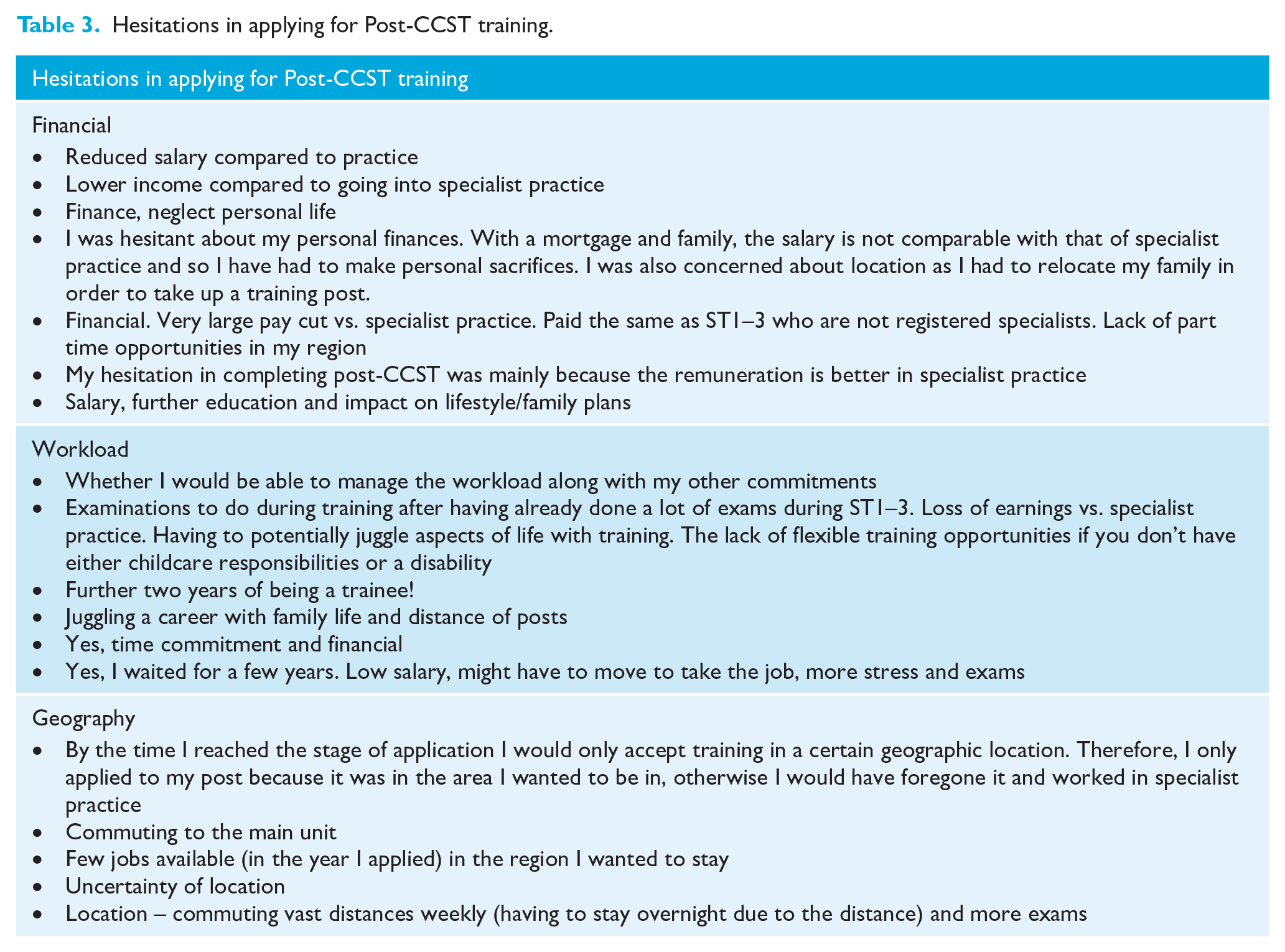
Participants were asked to state if they had any hesitations in applying for Post-CCST training and were given free-text boxes to answer. The answers could be easily separated into three main themes: financial; workload/time commitment; and geography. Table 3 shows sample answers that were given.
Hesitations in applying for Post-CCST training.
Working pattern
For those whose working patterns are LTFT/part-time, 50% found it straightforward to arrange while the other 50% found it ‘neither easy or difficult’. A respondent noted that their post was advertised as part-time and so they did not have to arrange it. Additional comments made were that a respondent was made to feel that LTFT was an inconvenience for all those involved (although the department was supportive) and they found it difficult to fit all the necessary sessions into fewer days as the rota had to work around joint clinics.
Reasons for requesting/applying for a LTFT/part-time post were mainly due to family commitments and wanting experience in primary care as well as secondary care. The only hesitation around opting for LTFT/part-time training was that the training would take longer.
Timetable
Table 4 shows a typical weekly timetable for a full-time trainee. The average number of certain types of clinics is in line with that advised by the SAC in orthodontics. However, it can be seen that some respondents are undertaking more treatment clinics (up to eight clinics) and/or new patient clinics (up to three clinics) and deliver less or zero new patient clinics, teaching or admin, indicating that there can be an imbalance in the timetable between clinical and non-clinical sessions.
Balance of sessional commitments within trainee timetables.
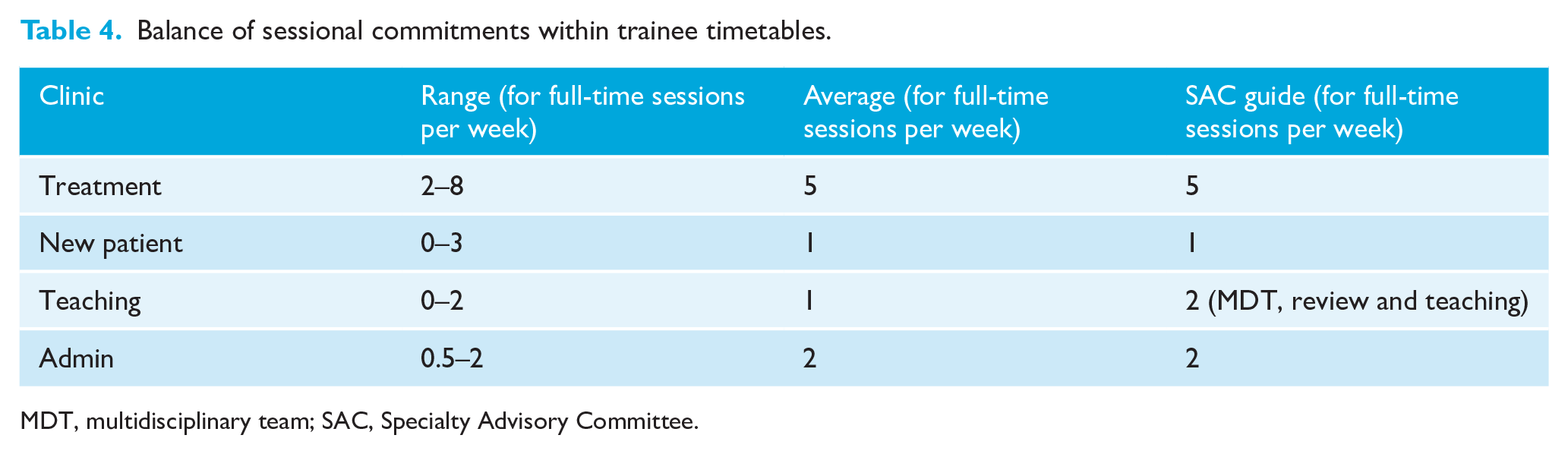
MDT, multidisciplinary team; SAC, Specialty Advisory Committee.
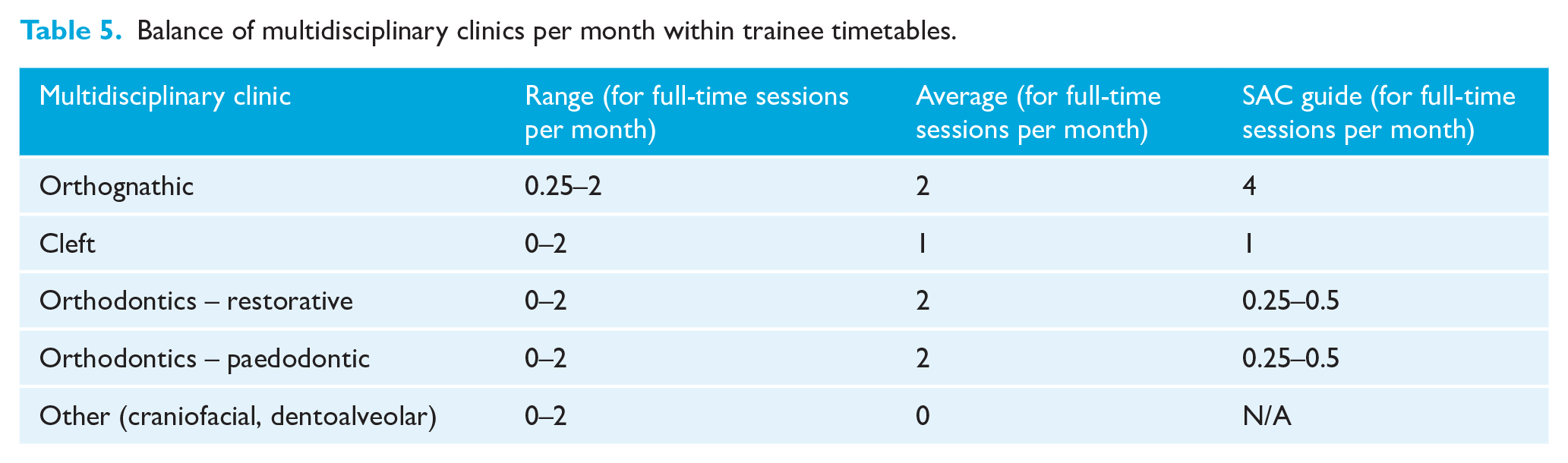
The SAC recommends that half of the time allocated for MDT clinics/review clinics/teaching be spent on orthognathic clinics. All respondents fell short of this as they are not undertaking one orthognathic clinic per week (Table 5). This is likely to be due to the fact that most departments only run orthognathic clinics once or twice per month. The SAC recommendation of 24 cleft clinics and 12 restorative/paedodontic clinics during training is being met overall. However, some respondents get very little exposure to MDT clinics, e.g. 0.25 orthognathic clinics per month or zero cleft, restorative or paedodontic clinics.
Balance of multidisciplinary clinics per month within trainee timetables.
Joint clinic preparation
On average, respondents are preparing four joint clinics per month (range = 1–8 clinics) spending an estimated 6 h on average (range = 2–10 h) per month.
Clinic preparation most commonly involves a crib sheet (78%) and planning the case (73%). A PowerPoint presentation was also required to be created by 30% of respondents.
Table 6 shows the free-text answers from respondents when asked what they felt the benefits of clinic preparation were. A large number commented that there were negatives rather than positives and so the comments have been separated into positive and negative comments.
Benefits of clinic preparation.
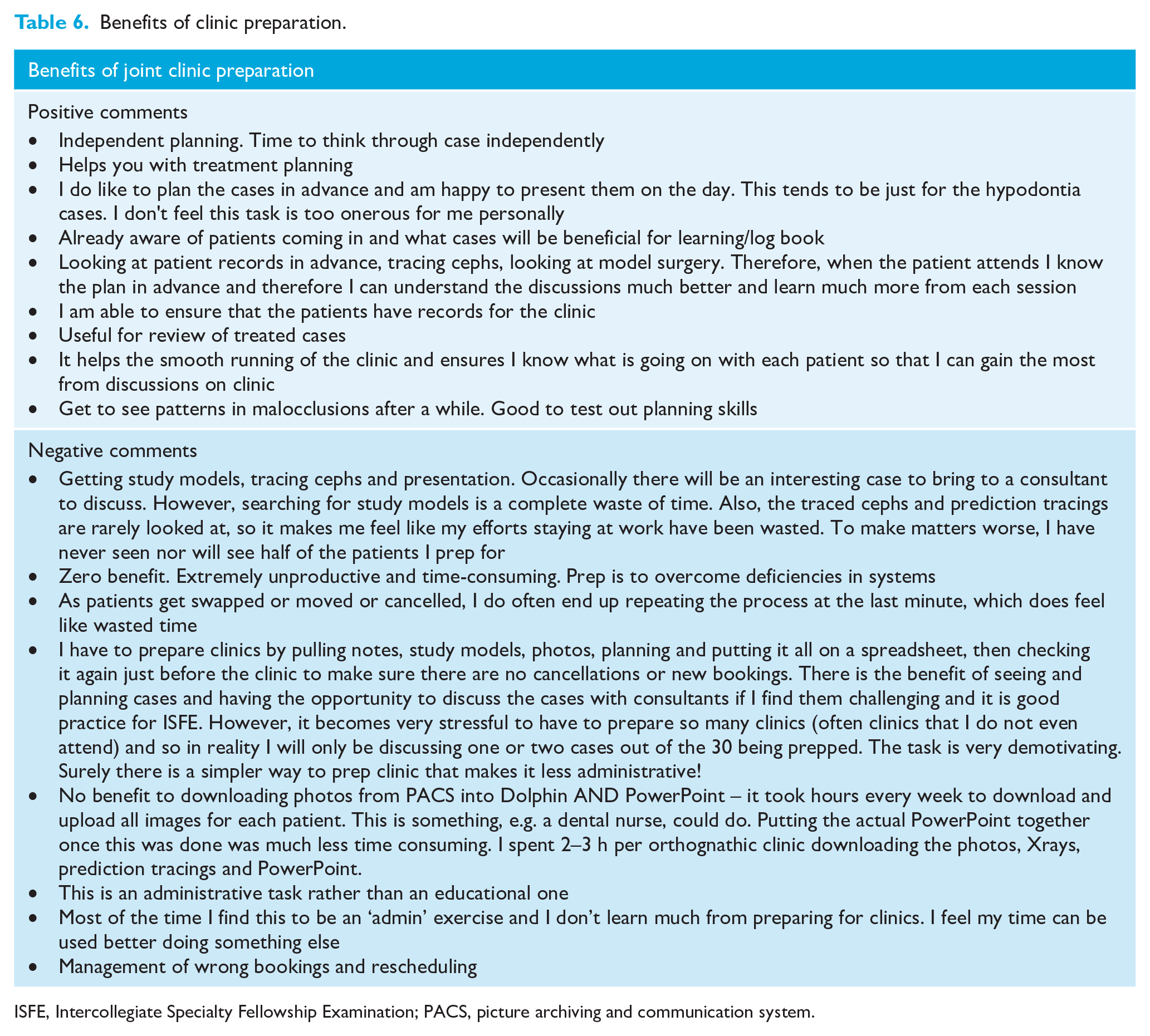
ISFE, Intercollegiate Specialty Fellowship Examination; PACS, picture archiving and communication system.
Assigned educational supervisor
All respondents had an assigned educational supervisor (AES) and 97% had met with their AES at the start of the training programme and regularly throughout. Of the respondents, 89% were either very satisfied or satisfied with their AES and meetings. Free-text comments about AES were all very positive where respondents felt very supported by their AES.
Teaching programme
Just under half of the respondents reported that their training had no formal teaching programme. Regional teaching programmes were available to 34% of respondents and local teaching programmes to 27% of respondents.
Study leave
The range of study leave per year was 8–30 days, with some respondents having unlimited days. The budget allocated to study leave was £600–2000, with again some respondents having an unlimited amount subject to approval. Over half (55%) of the respondents found it very easy/easy to gain approval for study leave. Of the respondents, 24% reported that it was either difficult or very difficult to gain approval for study leave. Gaining approval for study leave funding was reported as being difficult or very difficult by 35% of respondents.
Case load
The majority of respondents (84%) were happy with their case load/mix of patients they have to treat. Of respondents, 17% were ‘neither satisfied nor dissatisfied’ or ‘dissatisfied’. Reasons for being dissatisfied included the following: difficulties getting a good case mix due to COVID; lack of cleft and MDT patients; limited exposure to protraction headgear; temporary anchorage devices (TADs); fixed functionals if it is not regularly done in the department; and the majority of orthognathic cases not being ready for surgery by the time training has ended.
Support and supervision
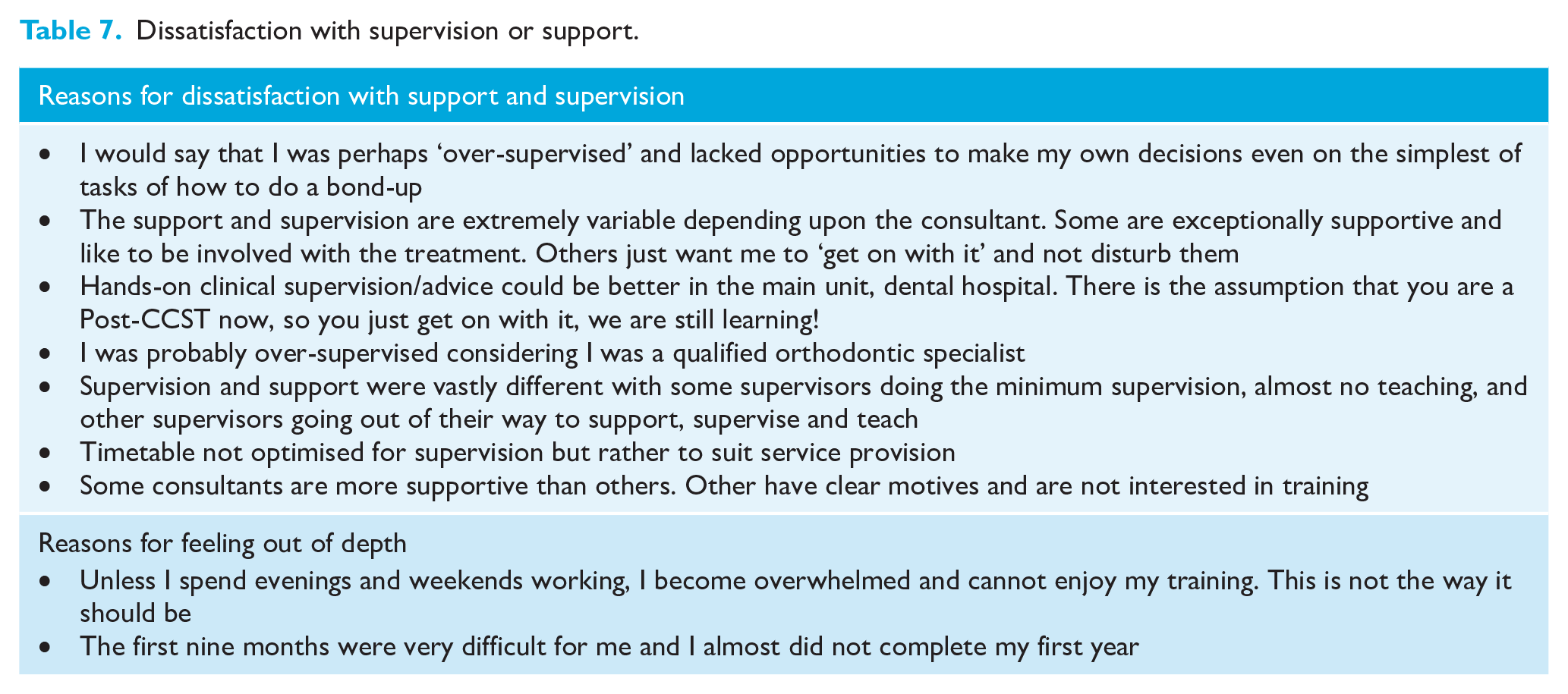
Regarding supervision and support, the vast majority of respondents were very satisfied (30%) or satisfied (43%) with the level of supervision they received during their training. This is reflected in the response to whether trainees felt ‘out of depth’ in their post, with 47% responding ‘rarely’; 25% ‘sometimes’ and 25% ‘never’. Unfortunately, 3% (n = 1) ‘always’ felt out of depth and were very dissatisfied with their support and supervision. When asked for comment on dissatisfaction with supervision, there was a range of comments regarding either feeling ‘over-supervised’ or feeling that supervisors were not interested in supervision. Table 7 shows some of the free-text responses for questions relating to supervision and support.
Dissatisfaction with supervision or support.
Management experience
There were a range of responses relating to how much management experience respondents were exposed to during their training. Of the respondents, 32% were ‘neither satisfied or dissatisfied’, while 30% were satisfied. The majority of respondents felt that their experience was limited to Intercollegiate Specialty Fellowship Examination (ISFE)-style scenarios in preparation for examinations rather than real-life experience of the inner workings of NHS departments (Table 8). Despite this, 65% of respondents said they were allowed/encouraged to develop non-clinical interests during their training. One respondent commented that they had very little additional time available as they were ‘prepping so many joint clinics’.
Comments regarding management experience.
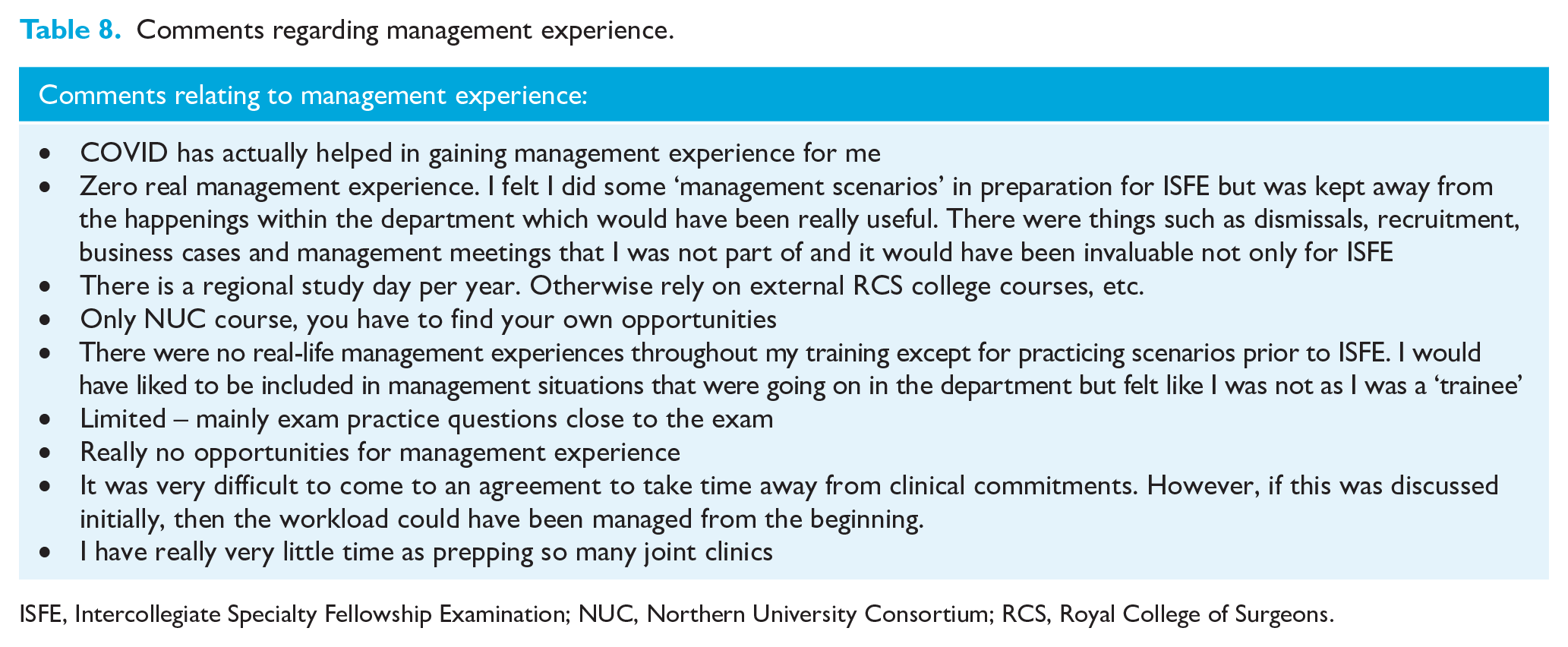
ISFE, Intercollegiate Specialty Fellowship Examination; NUC, Northern University Consortium; RCS, Royal College of Surgeons.
Future consultant life
A large proportion of respondents (86%) felt that their Post-CCST training had prepared/will prepare them for life as an NHS consultant. The majority of respondents (60%) expected to work on a part-time basis of roughly 70% WTE; 43% of respondents currently in a consultant post were working as part-time (mode 0.7 WTE) NHS consultants. Table 9 shows the free-text comments.
Comments on how prepared respondents felt towards being an NHS consultant.
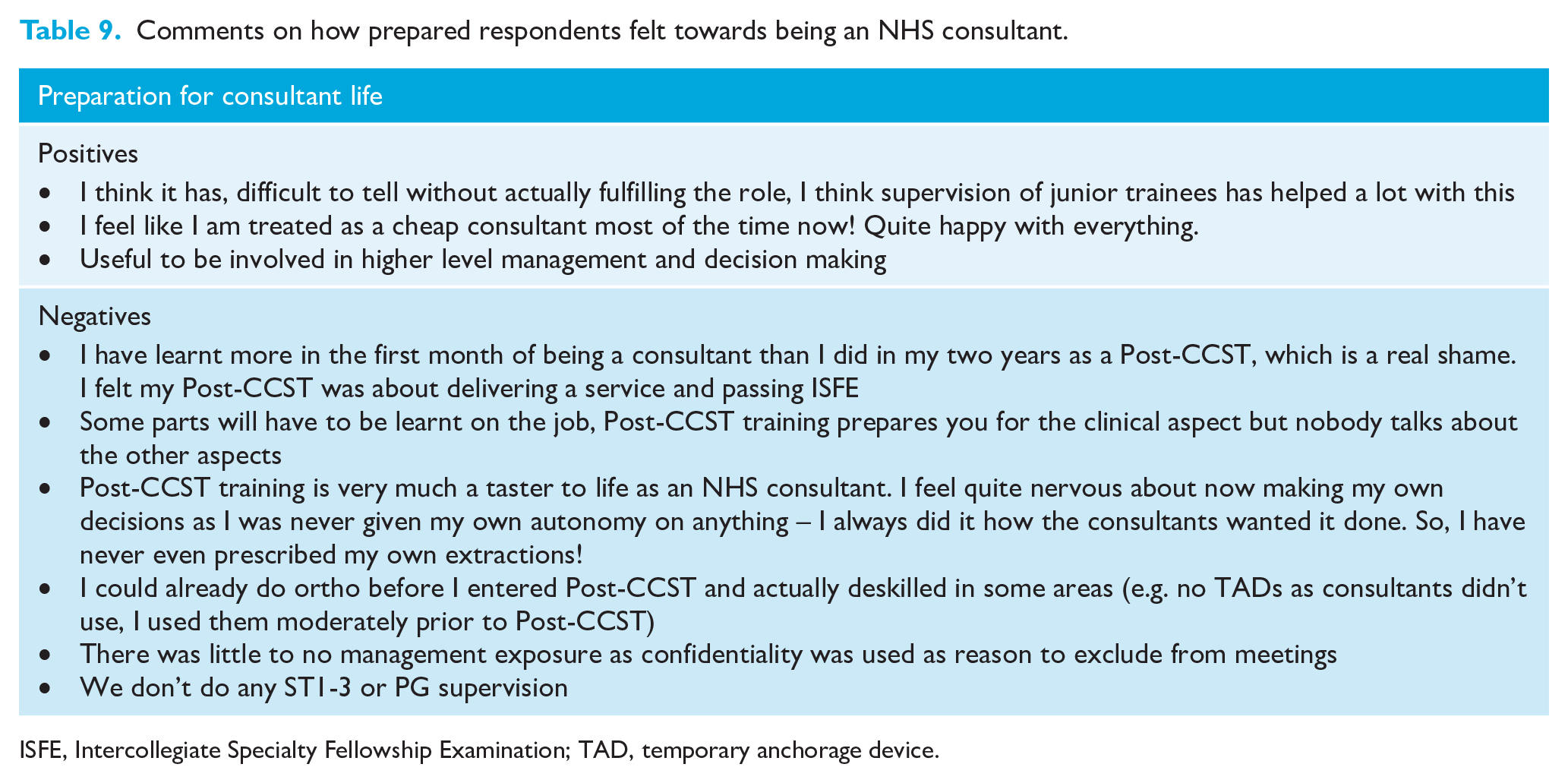
ISFE, Intercollegiate Specialty Fellowship Examination; TAD, temporary anchorage device.
Overall satisfaction with Post-CCST training and comments
While 61% of respondents were satisfied with their Post-CCST training, 17% were ‘neither satisfied or dissatisfied’ and 6% were either ‘dissatisfied’ or ‘very dissatisfied’. Of 37 respondents, 25 (67%) would apply for Post-CCST training again, 6 (16%) would not and 6 (16%) did not answer this question. Reasons are summarised in Table 10.
Comments on whether a trainee would still apply for Post-CCST training, if they had their time again.
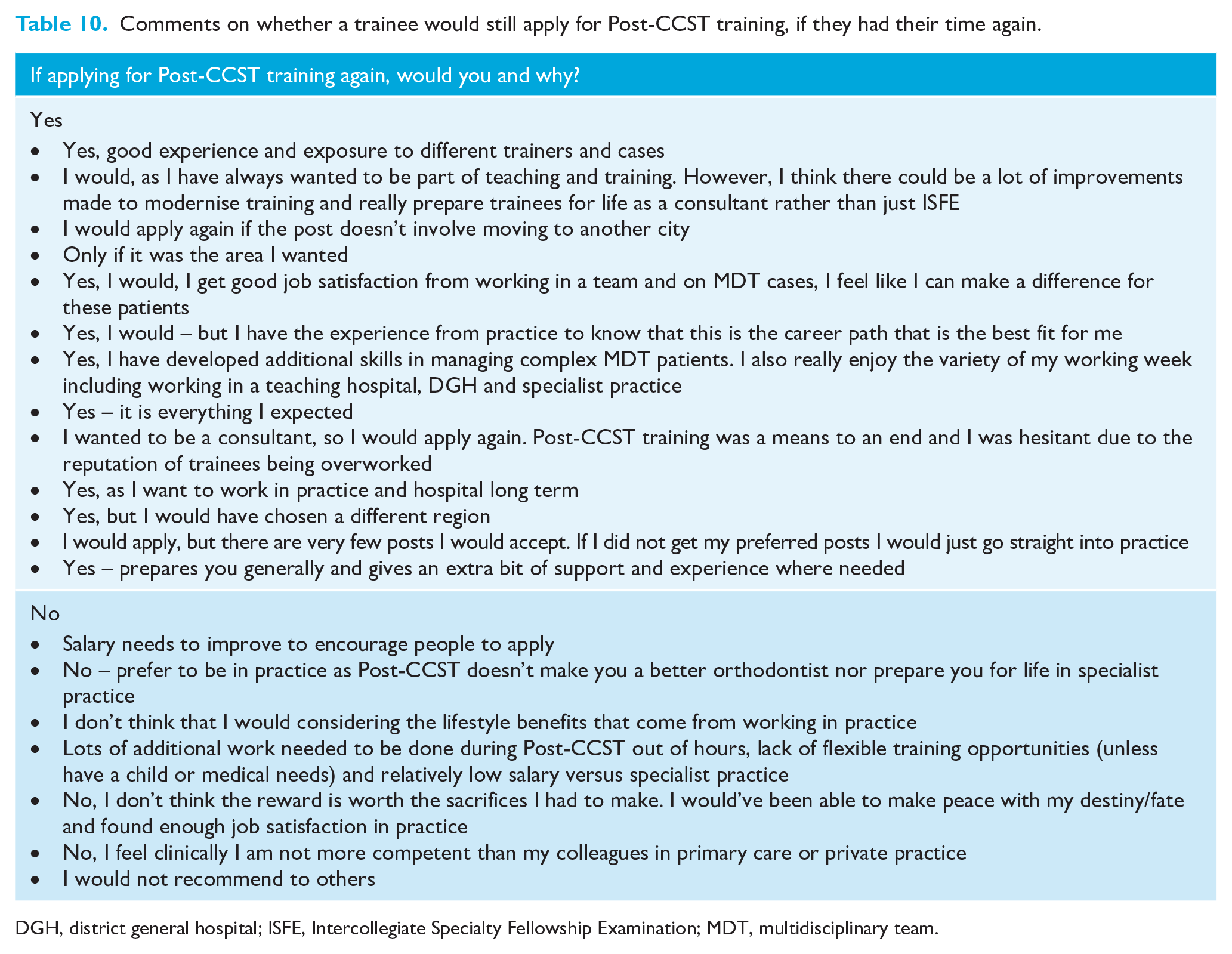
DGH, district general hospital; ISFE, Intercollegiate Specialty Fellowship Examination; MDT, multidisciplinary team.
Suggestions for improvement
When asked for possible suggestions for improvement to Post-CCST training to encourage greater satisfaction, responses could be grouped into themes of Part-time training, Teaching, Time commitment, Salary and Experience (Table 11).
Comments and suggestions for changes to Post-CCST training.
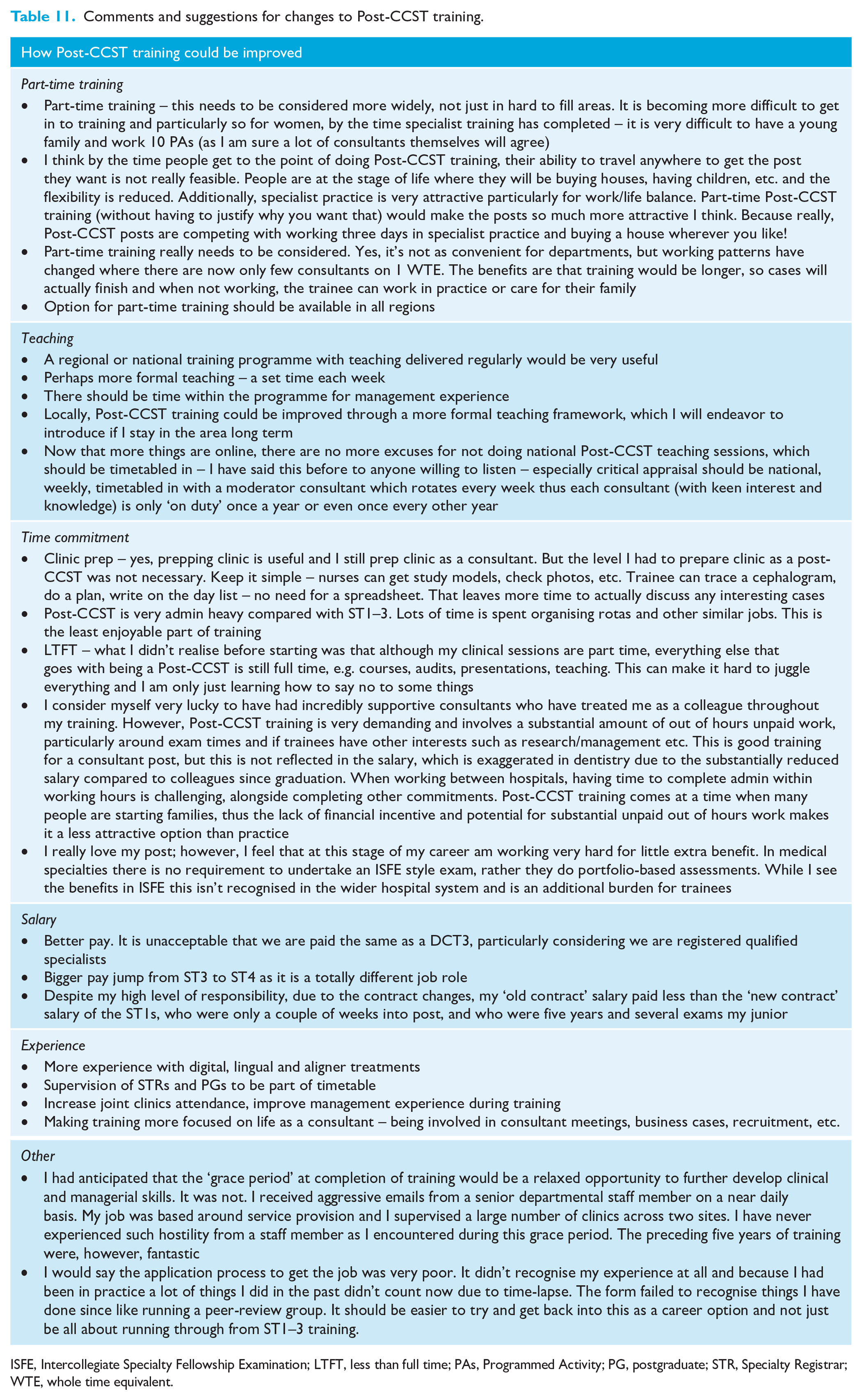
ISFE, Intercollegiate Specialty Fellowship Examination; LTFT, less than full time; PAs, Programmed Activity; PG, postgraduate; STR, Specialty Registrar; WTE, whole time equivalent.
Discussion
To date, there have been no other published surveys investigating satisfaction of specialist orthodontists who are still in training. Previous literature has reported on the satisfaction of either Pre-CCST trainees, (Keith et al., 1997; Oh and Chadwick, 2016; Oliver et al., 2020) orthodontic residents (USA) (Keith and Proffit, 1994) or qualified specialist orthodontists (Bateman et al., 2016).
This survey was distributed and completed between May 2021 and June 2021. As such, the respondents will have been either in training, or recently completed training during the COVID-19 pandemic. Therefore, the results and experiences may not be representative of trainees who undertook and completed training before the COVID-19 pandemic.
Applying to Post-CCST training
Regarding motivation for the completion of Post-CCST training, the main themes that arose were related to ‘completing consultant level training’ in order to provide complex MDT treatment, work in a hospital setting, be involved with training, teaching and committee work. This highlights that most respondents were undergoing further training as part of their career plan and to fulfil the various aspects of the consultant job role. A small number of participants indicated that they felt they needed further training after their specialty training.
Themes relating to hesitation in applying for training include the conflict between work–life balance, control of geographical location of work and financial disparity compared to specialist practice. Surveys of doctors also found the rejection of surgical specialties in favour of GP training due to poor career prospects and work–life balance reasons (Lambert et al., 2003).
Timetable
The survey reveals that the timetable for the majority of respondents is in line with SAC recommendations (Specialty Advisory Committee in Orthodontics, 2017). There are respondents who undertake significantly more or fewer clinics than SAC recommendations. Trainees can particularly feel that they are in the role for service provision if they undertake too many treatment clinics, not enough MDT clinics or do not have enough admin time. This should be reviewed between trainees and their AES and also at the annual review of competency progression meetings.
Preparation of MDT clinics
The requirement of trainees to prepare multidisciplinary clinics was an issue that reported both positive and negative feedback. There was a range of responses relating to this question, with some respondents seeing value in the preparation of the clinic and review of the case notes before the patient attendance, and other respondents feeling as though this was an administrative task only. It has been reported that passive involvement in the MDT meeting yields the least value for trainees (Trivedi, 2019) and the lack of involvement significantly reduced the education value of the MDT experience for trainees in medical training (Nally et al., 2021).
With Post-CCST training being undertaken over a two-year time period, it is difficult for trainees to gain experience in personally treating the wide variety of multidisciplinary cases. ‘Preparing’ clinics could be viewed as an opportunity to efficiently increase exposure to assessment and planning of complex cases.
Clinic preparation seems to have evolved to become more administrative, with tasks such as having to find notes, study models and put together presentations. This can be time consuming with some respondents reporting spending up to 10 hours per month preparing clinics. This may take away from the intended educational value. Active involvement in the diagnosis, treatment planning and MDT clinic will likely provide the most benefit for trainees. Satisfaction could be improved through local discussion between trainees and trainers as to the desired educational outcomes for these tasks, see what administrative tasks could be undertaken by other members of the team and assign time for discussion of cases before the clinic.
Case load
Most respondents were happy with their clinical case load, but some respondents felt there was a lack of experience or exposure to some aspects of contemporary or complex orthodontics (e.g. TADs, protraction facemask, fixed functionals). This is likely due to the preferences of clinical supervisors and whether or not they practise certain treatment modalities regularly. It may also be difficult to find the right case to use the treatment modality on.
Support and supervision
Some respondents stated that they felt over-supervised while conversely others felt under-supervised. This highlights the challenging position that a supervisor is in when a new Post-CCST joins their department. While a Post-CCST trainee is a specialist orthodontist, the Post-CCST may be entering a new unit in a new region. Both trainees and trainers will likely have to establish a relationship de novo and this often requires a period of close supervision to ensure the trainee displays all the required competencies and skills. There is a fine balancing act to allow the trainee enough autonomy that they can learn and develop their own consultant approach (Joint Committee for Postgraduate Training in Dentistry, 2012) but also not negatively impact patient care. This relationship could be managed best at the beginning of the Post-CCST training period through discussion with both the AES and clinical supervisors.
Teaching received
The lack of a national teaching programme for Post-CCST trainees was seen as a negative at the time of the survey. However, since then the BOS Education Committee have established a national Post-CCST virtual seminar programme to cover the majority of the Post-CCST curriculum, in addition to situational judgement and management scenarios available on the BOS Virtual Learning Environment. This development should help to address some of the respondent comments regarding a lack of management experience during their Post-CCST training period.
Study leave
A large range of study leave allowance was noted in this survey. According to the Terms and Conditions of Service for doctors and dentists in training, all Post-CCSTs are entitled to up to 30 days of study leave, which can be used for study linked to a course or programme, research, teaching, preparing for and sitting examinations, attending conferences and training events. Statutory or mandatory or departmental training is not included. With the introduction of the national Post-CCST virtual seminar programme, there may be concerns that trainees whose study leave allowance is on the lower end of the scale may not be able to cover all the days within the programme, as well as attend other external courses that are approved by their educational supervisor. The large range in trainees’ study leave budgets potentially disadvantages certain trainees if they are unable to access a full scope of teaching that other trainees can.
Future consultant life, overall satisfaction
While most respondents felt that their training had prepared them for consultant life, some did report that they felt as though there was limited exposure to some aspects of becoming a senior NHS employee. This exposure will undoubtedly vary between units as a reflection of the varied workforce and opportunities in place.
Overall, there was a good level of satisfaction, While 61% of respondents were satisfied with their Post-CCST training, and 67% stating they would apply for Post-CCST training again, citing exposure to complex MDT cases and confidence in treating them as the positive aspects. But negative comments relating to workload, lifestyle, lack of flexible training and salary concerns did come through.
Suggestions for improving Post-CCST training
When respondents were given the opportunity to provide suggestions for improvement of training via free-text boxes, there was a strong theme for the desire for part-time training and the other comments regarding salary, which reflect the barriers to Post-CCST training survey completed recently (Quach et al., 2021).
Part-time training was the most commonly suggested improvement. The majority of respondents who were still in training planned to work part time when they become a consultant. There are typically few consultants who work full time with an increasing number of existing consultants becoming part time. A part-time working pattern would allow trainees to be able to balance hospital work with specialist practice, if desired, and family life. There would also be financial benefits that working part time in specialist practice would provide. This would address the issue of salary that respondents have stated as a suggestion to improve Post-CCST training.
It is clear from the responses to this survey that the comparative salary between working in primary care orthodontics and continuing into Post-CCST training is a significant factor in deciding whether to pursue further training or exit training after CCST. This is potentially comparable to the choice between general practice and hospital specialisation for junior doctors. It has been found that over time following qualification, there is an increase in the importance of working conditions/hours and domestic and financial circumstances for trainees (Lambert et al., 2016) and this increase in the importance of domestic circumstance has become more apparent in recent decades (Smith et al., 2015).
Regarding the comments on time commitment, training appears to be time consuming due to admin tasks, courses, delivering teaching, clinical audits and exams. Apart from exams, these are commitments that come with being a consultant. To help improve training, trainees and their AES should ensure that they have enough protected admin time along with SAC guidelines.
Some respondents noted that they were lacking in certain experiences that they expected from training. These ranged from clinical experience of contemporary orthodontics, attendance at multidisciplinary clinics to supervision of more junior trainees and management experience. Regular meetings between trainees and their AES should allow review of current timetables and experience to ensure that there is access to a wide range of suitable experiences and exposures, or the opportunity to develop interests and rectify any training gaps.
Conclusions
Reasons for applying for Post-CCST mainly included providing further training, MDT treatment, job variety, working in a hospital setting and delivering teaching and training. Hesitations to applying to Post-CCST training were mainly financial, workload and geography. The working patterns for respondents were 89% full time, 8% LTFT and 3% part time. However, 60% expect to work part time once they are a consultant. The majority of respondent timetables are in line with SAC recommendations. However, there are respondents undertaking significantly more or less of certain clinics, which can lead to a lack of balance in clinic experiences and they may not have enough admin time. In general, respondents were satisfied with Post-CCST training (61%). There was a significant range of positive and negative responses to various aspects of training including: MDT clinic preparation, support, supervision and management experience. Two-thirds of respondents would apply again for Post-CCST training. Of those that would not, the reasons included salary, lifestyle, workload, lack of flexible training, personal sacrifices required and not feeling clinically more competent. Suggestions for improvements echo the barriers to Post-CCST training survey. Suggestions included the following: part-time training; less involved MDT clinic preparation; less administrative tasks; improved salary to reflect the level of responsibility; and more clinical experience in contemporary orthodontics/supervision/MDT clinics/management.
Footnotes
Acknowledgements
The authors thank the BOS, TGG and COG for their input and assistance with the development and distribution of the survey
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.