
Abstract
Objective
Prescription checking is becoming increasingly prevalent in medical institutions. However, the prescription-checking ability of pharmacists requires improvement. The study aim was to explore the main aspects of prescription-checking training and provide an empirical reference for the training of pharmacists in medical institutions.
Methods
Participants were pharmacists willing to complete a Likert questionnaire. Descriptive statistics were used to examine percentages and composition ratios. The chi-square test and exploratory factor analysis were used for inferential analysis.
Results
The questionnaire showed good internal consistency reliability and validity. A total of 90% of participants were satisfied with the training. Exploratory factor analysis extracted three satisfaction dimensions: training organization, teaching method, and knowledge consolidation and assessment. The average examination score for the 20 courses was 89.21/100. Regarding trainee needs, 94.66% preferred face-to-face lectures, 89.33% expected high professional skills of the lecturers and 62.67% believed that clinical expertise was highly desirable.
Conclusions
There was a high demand for prescription-checking training among pharmacists. Trainees in this study showed high satisfaction. The most important aspects of prescription-checking training were training organization and knowledge consolidation and assessment. It is recommended that training should be stratified. Pharmacists preferred face-to-face and interactive lectures as a supplement to clinical knowledge.
Keywords
Introduction
Prescription errors are common in clinics and pose a substantial risk to patients. Approximately 29.3% of drug-related events were reported between January 2005 and June 2006 in the UK, 1 causing patients serious harm and even death. There is a therefore a high risk of prescription errors, even in hospitals. 2 Approximately 6% of inpatients in Finland have experienced adverse drug events. 3 Glanzmann et al. 4 showed that in a paediatric intensive care unit in Switzerland, 14% of prescriptions contained errors (50% were dose errors), most of which should have been avoided. Prospective prescription checking by pharmacists can ensure the safety and rationality of medication5–7 and reduce non-rational drug treatment, drug waste8,9 and the number of emergency department visits and hospital readmissions. 10 Concerns about prescription checking and the need for improvement are global.
Prescription checking is also an important aspect of the changing role of pharmacists. 11 A study in France showed that the rate of prescription change after checking varies widely among hospitals (1% to 37%). 12 Recently, three national departments issued a Regulation for Prescription-checking for Medical Institutions in China (No. 14 [2018] of the Ministry of Health), which clarifies that pharmacists have the primary responsibility for prescription checking. The principles of this regulation were already implemented, but at different levels, in Chinese hospitals. However, the regulation highlights the importance of the role of medication advice and checking as it is currently implemented worldwide.4,13–15
Prescription checking requires optimal clinical knowledge, pharmaceutical knowledge and work experience. However, pharmacists in medical institutions receive chemistry-based pharmacy-centred education, 16 which is not closely related to their work. 17 Pharmacists in China and many other countries must complete continuing education,18–21 but the traditional continuing education is not very useful, a situation similar to that in Lebanon 22 and Scotland. 21 In addition, practical experience is based on supplying medicine and studying cases; pharmacists lack knowledge and experience of medication (e.g., knowledge of medical review, pharmaceutical monitoring and rational drug use). 23 Although prescriptions involve all hospital departments, the clinical knowledge of pharmacists is far below that required for checking prescriptions. Hence, prescription checking presents a substantial challenge for pharmacists.
Pharmacists must continue to study and improve their skills and knowledge to adapt to changes as the pharmacy develops.14,24 Therefore, medical institutions should conduct frequent and intense prescription-checking training to increase pharmacists’ clinical medication experience and improve their comprehensive skills and competency.18–21
To effectively improve the ability of pharmacists in our province, the Shanxi Pharmaceutical Specialty Alliance organized a phase 1 class for prescription-checking training of pharmacists in medical institutions. This class ended in May 2019 and promoted clinical rational drug use. As pre-requisite prescription checking is still in an exploratory stage in China, 25 and the standardized training is in a nascent stage, 26 training interventions can refer only to the training experience of individual hospitals that have already conducted training, and on the current training experience of pharmacists. In response to the need for prescription-checking training in our province, we surveyed training satisfaction and requirements of pharmacists from different types of medical institutions, and of different ages and positions. The aim of the training was to provide a reference for follow-up training, build a team of pharmacists and improve prescription-checking ability. We hope that this training can be exported to other countries, as prescription errors are an international problem.
Materials and methods
Participants
Shanxi Pharmaceutical Specialty Alliance, the most influential third-party pharmacy organization in Shanxi Province, issued a notice about the availability of prescription-checking training. The organization planned to enrol 80 trainees. Of all the pharmacists in Shanxi Province, 826 signed up for the training. Owing to the large demand for training, 150 trainees were finally enrolled. There are 11 administrative regions in Shanxi Province, and pharmacists from all these regions registered. The number of trainees from each administrative region was allocated according to the proportion of registered pharmacists in each region (e.g., if region A represented 15% of the pharmacists in Shanxi, then 15% of the participants from region A would be enrolled). The inclusion criterion was resident hospital pharmacists. There were no exclusion criteria.
This was an observational study, and the confidentiality and autonomy of participants was respected. Therefore, the ethics committee of the Second Hospital of Shanxi Medical University waived the need for ethical approval and for written informed consent. However, all participants provided verbal informed consent.
Training
The training was divided into theoretical study, practice and assessment. The theoretical study involved 20 courses. These were arranged in four sets according to the different types of medications for different diseases. The courses were completed via face-to-face lectures over 33 hours on 4 rest days. There were 20 classes of 1 or 2 hours each (mean class duration: 1.65 hours). The practice was completed on working days. The 20 courses were as follows: 1. Regulatory documents relevant to prescription checking; 2. Basic points of prescription checking; 3. Key points of checking prescriptions of high-alert drugs; 4. Key points of checking prescriptions of drugs requiring a skin test; 5. Key points of checking prescriptions of off-label medication use; 6. Literature retrieval tools and their use; 7. Key points of checking prescriptions of hypertension drugs; 8. Key points of checking prescriptions of intravenous drugs; 9. Key points of checking prescriptions of commonly used paediatric drugs; 10. Key points of checking prescriptions of anticancer drugs; 11. Key points of checking prescriptions of antimicrobial drugs; 12. Key points of checking prescriptions of drugs used during pregnancy and lactation; 13. Key points of checking prescriptions of drugs for cerebrovascular diseases; 14. Key points of checking prescriptions of Chinese medicine (Chinese patent medicine); 15. Key points of checking prescriptions of digestive system drugs; 16. Key points of checking prescriptions of drugs for coronary heart disease; 17. Key points of checking prescriptions of drugs for chronic disease for elderly people; 18. Key points of checking prescriptions of glucocorticoid drugs; 19. Key points of checking prescriptions of diabetes medication; 20. Key points of checking prescriptions of antiarrhythmic drugs.
To consolidate their knowledge, the trainees reviewed and commented on the prescriptions of their institutions based on what they had learned. Each of the 20 assessments (one assessment per course) was an online open test using single-choice or multiple-choice questions; the total possible test score was 100. Each course was tested online on the working day following the face-to-face training lectures. The test link was opened at 18:00 on a working day and closed at 18:00 on the next day. On a particular day, an answer query link became active when the test link was closed, to provide extra tuition.
Questionnaire
From 9 June to 20 June 2019, the questionnaire link was available on a WeChat group through the Sojump website platform. Trainees could complete the questionnaire (Supplementary File 1) on their mobile phones. A total of 150 questionnaires were returned. All questionnaires were valid, as all questions had to be answered or the questionnaire could not be submitted.
The questionnaire consisted of three parts. The first part introduced the survey background and objective. The second part recorded the following participant demographic information: gender, age, work experience, educational background, job title, hospital level and position in the hospital. The third part assessed satisfaction with the training, training needs of pharmacists and teaching effect. The questionnaire comprised 23 items. Of these, 19 items were scored on a Likert scale. Questions were phrased positively and scored from 1 to 5; higher scores indicated a more positive tendency regarding the measured content and higher satisfaction or demand. The other four items were open-ended questions. The trainees reported on the training content and requirements for improvement. To assess the effect of the teaching, the trainees evaluated their own competency in prescription checking; a score of 100 indicated fully competent and 60 indicated competent.
In addition to these assessments, we recorded the trainees’ scores on each course, which reflected their mastery of the corresponding course.
A Cronbach’s α coefficient of >0.7 indicates consistency reliability. 27 The questionnaire was reviewed by several pharmacy experts (pharmacy education experts and directors of the pharmacy departments of tertiary hospitals in Shanxi Province). Eight experts were asked to score each item and evaluate the relevance of the item to its dimension. Each item was evaluated according to four levels of relevance that reflected weaker to stronger correlation. The ratio of items with a score of 3 or 4 to the total number of items (scale-level content validity index, S-CVI) reflected the content validity of the scale. Structural validity was measured using the Kaiser–Meyer–Olkin (KMO) index and Bartlett’s test of sphericity.
The following pharmacist titles are used in China (in order): assistant pharmacist, pharmacist, pharmacist-in-charge, associate chief pharmacist (associate professor of pharmacy) and chief pharmacist (professor of pharmacy). The title of pharmacist can be used 1 year after graduating from university and after passing an examination. A pharmacist can become a pharmacist-in-charge 5 years after receiving the title of pharmacist and after passing an examination.
Data analysis
The survey data were exported from the Sojump platform and analysed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). Quantitative data were expressed as means ± standard deviations. Data with non-normal distributions were described using medians (quartiles) and analysed using the Mann–Whitney U-test. Qualitative data were described using percentages and composition ratios and analysed using the chi-square test or Fisher’s exact test. Exploratory factor analysis was used to analyse latent variables for the satisfaction items. A multivariable analysis was performed using self-evaluated prescription-checking competency as the dependent variable and the factors identified in the factor analysis as independent variables. Correlations were examined using Pearson’s correlation test. A value of p < 0.05 was considered statistically significant.
Results
Basic characteristics of trainees
A total of 826 pharmacists from different medical institutions were registered for training in Shanxi Province, of which 150 (18.16%) participated in the phase 1 training. The average age of participants was 36.9 ± 6.7 years. Participant background characteristics are shown in Table 1.
Background characteristics of the trainees (n = 150).
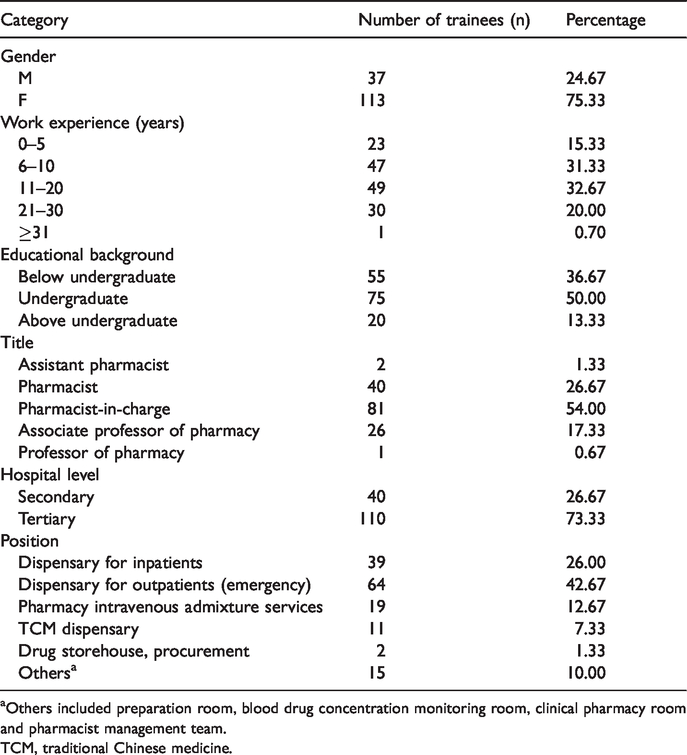
aOthers included preparation room, blood drug concentration monitoring room, clinical pharmacy room and pharmacist management team.
TCM, traditional Chinese medicine.
Reliability and validity tests
Cronbach’s α for the scale in this study was >0.8, indicating good internal consistency reliability (Table 2). Cronbach’s α coefficient for ‘teaching effect’ was not calculated, as this part of the questionnaire contained only one item. The S-CVI of the scale was 0.91, which indicates good content validity. The KMO was 0.905, which was >0.8, and Bartlett’s test of sphericity produced a chi-square value of 10169.46 (p < 0.001), which indicated good validity and suggested the feasibility of factor analysis.
Reliability of the questionnaire and its components.

Cronbach’s α for teaching effect was not calculated, as this part of the questionnaire contained only one item.
Satisfaction analysis
The personal satisfaction data showed that 135 trainees (90%) had an overall satisfaction score of ≥4, 112 (75%) were very satisfied, 13 (8.7%) indicated dissatisfaction ( < 3 points) and 2 (1.3%) expressed basic satisfaction (3 points). The mean score was 4.51; this was higher than a score of 4 (‘satisfied’), which was defined as indicating satisfaction.
The composition ratio and mean value of satisfaction for each teaching aspect were analysed (Table 3). Trainees were most satisfied with the staff services and the lecturers’ professional skills and least satisfied with the amount of training assignments and the 1 day duration for each training element.
Satisfaction scores for each aspect of the training.
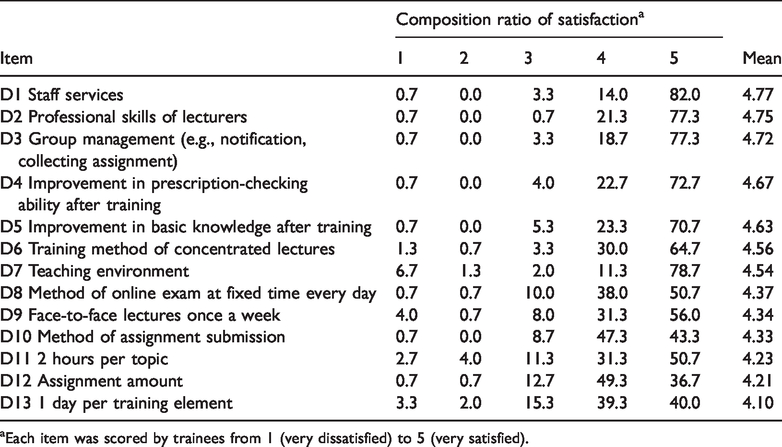
aEach item was scored by trainees from 1 (very dissatisfied) to 5 (very satisfied).
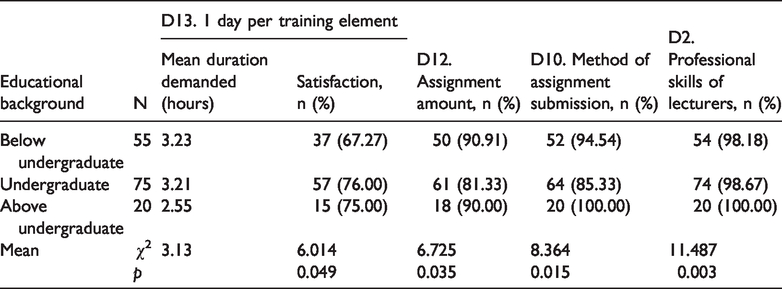
Trainees were divided into subgroups according to their educational background. The effect of educational background on responses to items D2, D10, D12 and D13 was statistically significant (p < 0.05). Trainees with an educational level below undergraduate showed low satisfaction with the 1 day per training element (p < 0.05) and dissatisfaction with the use of 20 classes of 1 or 2 hours each. They recommended that each class be longer than 3.13 hours. Trainees with an undergraduate education showed low satisfaction with the number of assignments (p < 0.05) and the method of assignment submission (p < 0.05). Trainees with higher educational levels showed greater satisfaction with the lecturers’ professional skills (p < 0.05) (Table 4).
Effect of educational background on course satisfaction (number and percentage of trainees with a satisfaction score of ≥4).
To further explore potential relationships between the 13 satisfaction items, the data were subjected to factor analysis. After oblique rotation (Tables 5 and 6), the cumulative variance contribution of each factor was 73.78% (factors corresponding to an eigenvalue >1 were included). The communality of the 13 variables over the three factors exceeded 0.5, indicating that these three factors provided the best summary of the structure of the 13 items (i.e., the 13 indicators measured three dimensions of satisfaction).
Variance contributions of factors.

Factor loading matrix after rotation.

As shown in Table 6, each item loaded highly on one or more factors. Factor 1 loaded mainly items D1, D2, D3, D4 and D5, which reflect the organization and effectiveness of the training. The main items loading on Factor 2 were D6, D7, D9, D11 and D13, which reflect the teaching method. Factor 3 comprised D8, D10 and D12, which reflect the consolidation and assessment of knowledge. These results indicated that training should be mainly focused on these three factors to improve overall satisfaction.
Course assessment results
The training comprised 20 courses, all of which had a total possible score of 100 points. The average score was 89.21 ± 2.62. The highest scores were for the key points of prescription checking for cerebrovascular diseases (mean 93.63) and the lowest scores were for the key points of prescription checking for antimicrobial drugs (mean 77.63).
Self-evaluation of prescription-checking competency
At the time of enrolment, trainees were asked to rate their own perceived competency in prescription checking; 90% of trainees believed they were not competent and their self-evaluation score was below 60. After the training, the mean self-evaluation score was 70.21, and 73.33% trainees believed that they were competent (Figure 1).

Participant self-evaluation of prescription-checking competency. The histogram shows the self-evaluation of competency in prescription checking (possible score range: 0 to 100). The x axis represents five score categories and the y axis represents the number of trainees.
Multivariate regression was performed using the three factors identified in the factor analysis of the satisfaction analysis as independent variables and self-evaluation of prescription-checking competency as the dependent variable. The result was statistically significant (F = 2.715, p = 0.047), with the equation y = 70.267 + 3.736X1 − 1.055X2 + 2.105X3. This result indicated that greater focus is needed on the organization and development of training and on knowledge consolidation and assessment.
Perceived need for improvement in prescription-checking abilities
Notably, 48% of the trainees felt a need to improve their abilities, particularly to improve their clinical expertise and practical ability, and their communication skills and ability to search the English-language literature.
Demand for training knowledge
Trainees expressed the highest demand for clinical expertise (62.67%) and the lowest demand for pharmacy basics (Table 7). Trainees were asked to score the 20 courses according to their perceived importance. The results are shown in Table 8. Trainees did not think that course 1.6 was important and paid less attention in this course; thus, the assignment scores for this course were low. Correlation analysis of the association between online assessment scores for each training category and the importance ratings for that category showed two significant correlations: for course 1–4 (prescription checking for drugs that require a skin test, Pearson’s r = 0.163, p = 0.047) and for course 1–5 (prescription checking for off-label drugs, Pearson’s r = −0.161, p = 0.049). This indicates that trainees with a greater need for training should strengthen their knowledge in these two categories.
Demand for training in each topic.

aTrainees scored each item from 1 (very dissatisfied) to 5 (very satisfied).
bCalculated average of the scores.
Summary of rated importance of training courses.

aRank is the order of the average assessment scores. bOrder is the order of average score of importance (as evaluated by trainees).
TCM, traditional Chinese medicine.
Work experience affected the evaluation of the importance of the courses. Ten of the courses (related regulations, basic elements, key points of prescription checking for high-alert drugs, drugs requiring a skin test, off-label drugs, common paediatric drugs, anticancer drugs, antimicrobial drugs, chronic senile disease drugs and drugs for arrhythmia) were significantly associated with work experience (all p < 0.05) (Table 9).
Effect of work experience on evaluation of course importance (number and percentage of trainees with a satisfaction score of ≥4) (n = 150).

aNumber of trainees in each work experience category. *Significant at p < 0.05.
Of the trainees, 38.67% believed that the following topics needed to be added to the training: perioperative administration, rheumatism and immunology, nephropathy, microorganisms, respiratory disease, liver disease, narcotic drugs, psychoactive drugs, oestrogen, oculopathy, dermatologic disease, enteral and parenteral nutrition, gynaecological drugs, mental disease, analgesics, ancillary drugs and other drugs for specialized diseases.
Preferences for teaching organization
The trainees favoured face-to-face training and this received a very high mean score. Notably, 94.66% of trainees preferred this method of teaching and 63.33% of the trainees reported that they liked this teaching method very much (Table 10).
Rating of teaching organization.
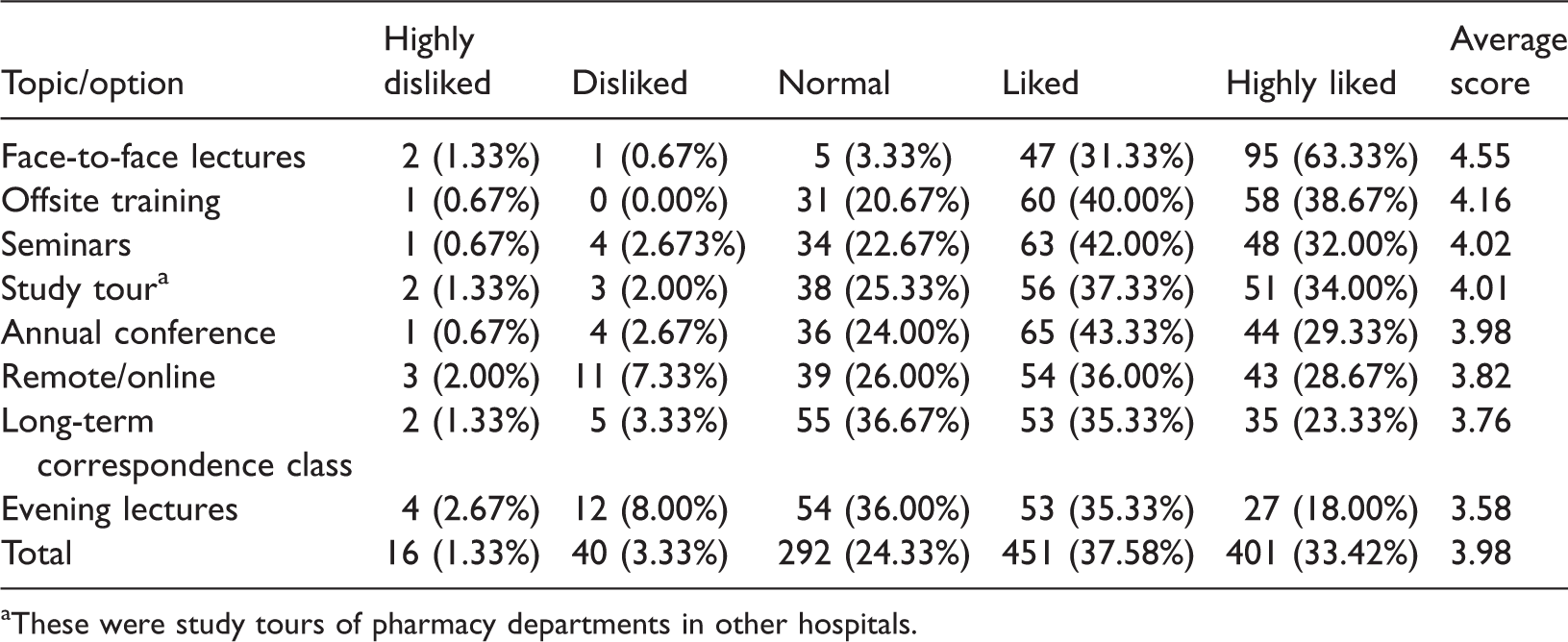
aThese were study tours of pharmacy departments in other hospitals.
Trainer requirements
Trainees felt the most important quality of a trainer was professional skills (89.33%), followed by teaching attitudes, teaching methods or means, organization, teaching style and appearance (Table 11).
Professional ability requirements of trainers.

Discussion
This study aimed to investigate the training-related experiences and needs of 150 pharmacists and to explore the key aspects of training (i.e., training organization, knowledge consolidation and assessment). The results indicated that this prescription-checking training course in Shanxi Province quickly and effectively improved the ability of pharmacists using a combination of key theory teaching, practical application and online assessment. The survey revealed a high demand for prescription-checking training among pharmacists. Trainees showed high satisfaction with the training. The participants recommended that the training should be conducted in a stratified way, and they preferred the use of face-to-face and interactive lectures to supplement clinical knowledge.
The questionnaire showed good internal consistency reliability and validity. Participants were drawn from all districts and counties of Shanxi Province, and so the sample reflected the characteristics of pharmacists across the whole province. Therefore, these survey results could be a useful reference for other researchers. Three aspects of the training effects were evaluated: satisfaction, examination scores and self-evaluation of competency. In addition, the needs of the trainees were analysed in terms of four dimensions: perceived need for improvement in prescription-checking ability, training content requirements, teaching method and trainer requirements. These dimensions covered the main aspects of training; therefore, the findings could provide a reference for training and improve the quality of continuing education for pharmacists. 28 Of the trainees, 90% were satisfied and 75% were very satisfied. In contrast to previous continuing education courses, the present training linked learning with the practical work of prescription checking. As such, it functioned as continuing professional development (CPD). There is evidence that CPD encourages pharmacists to be more autonomous 29 and greatly benefits their work.30–32 The pharmacists in the present study were generally very satisfied with the training; however, satisfaction levels varied. Participants were most satisfied with the services of staff and the professional skills of lecturers, and less satisfied with the assignment amount and the 1 day per training element. Additionally, trainees with different educational backgrounds expressed different levels of satisfaction with the various aspects of the training. The satisfaction evaluation focused on the factors of training organization, teaching method, knowledge consolidation and assessment. The analysis showed that we should focus on strengthening the organization and development of training to improve the satisfaction of trainees.
Owing to the limited duration and tight schedule, the effects of this type of training on pharmacists’ skills and knowledge may be limited. The training is more likely to increase confidence in pharmacists who lack confidence in their abilities of prescription checking and medication suggestions.33,34 After the training, the average prescription-checking competency score was 70.2, and 73.3% of the trainees believed they were competent in prescription checking. The analysis showed that to improve competency, training should focus on training organization, knowledge consolidation and assessment.
In addition to pharmacist skills, prescription checking relies on the information platform, as pharmacists must consult medical records, test results, medical orders and other information. Such software acts as a communication platform between pharmacists and doctors. 33 Some medical institutions have the facilities to perform risk pre-assessment using embedded rational drug use monitoring software to help pharmacists complete prescription checking during peak hours. Therefore, support from the leadership of medical institutions is essential. However, owing to the complexity and variability of clinical diagnosis and treatment, the utility of rational drug use software is very limited and the final results must be assessed by pharmacists after comprehensive analysis. Hence, pharmacists need to strengthen and update their medical knowledge. Matching the main features of training with pharmacists’ knowledge requirements would help to provide more focused training that would help pharmacists.
The training comprised 20 courses and lecturers spent 1 to 2 hours sharing relevant clinical knowledge and typical cases. Each course was assessed (total possible score: 100). The trainees performed well in the assessment, with an average score of 89.2, which indicated a good grasp of the information provided in the courses. The training contents included medication for common clinical diseases, medication for special populations, use of special medicines and relevant laws and regulations. Pharmacists demonstrated different levels of knowledge and needs owing to their varied work experience. For example, the knowledge of drugs that require skin tests constitutes basic pharmaceutical knowledge and the clinical use of such drugs is associated with a high risk to patients. Pharmacists considered it important to acquire knowledge, and made efforts to acquire knowledge during work hours, which resulted in a good grasp of knowledge and high assessment scores. Off-label medications are commonly used in the clinic. Information about most of these medications belongs to the frontiers of clinical treatment. Pharmacists thought that knowledge about these medications was important, but they lacked this knowledge, which resulted in lower scores on this topic. Pharmacists underestimated the importance of literature search tools and applications, and paid less attention to this topic, which led to a poor grasp of knowledge and low examination scores. Pharmacists with greater work experience placed greater importance on drug-related laws and regulations and on commonly used drugs for clinical diseases. This suggests that trainees expect training to be related to their practice. 35 The survey showed that pharmacists had less exposure to clinical knowledge and frontier knowledge in their continuing education and daily work. Therefore, there was a high demand for information about medications for common clinical diseases, 18 frontier knowledge of pharmacy, and key points in prescription checking, followed by regulations, query tools and other aspects. The lowest demand was for training in basic pharmaceutical knowledge. Furthermore, there was a need for supplementary knowledge of tools, such as those used in pharmacy consultation, communication skills, 18 drug incompatibility, clinical tests and popular scientific knowledge of pharmacy. To meet the needs of pharmacists, training needs to be patient-centred, and to include clinical and therapeutic contents. 36 This training focused on basic clinical knowledge and classic prescription cases, which met the trainees’ needs and was well received.
Regarding other aspects of the training organization, of the traditional teaching methods used, 22 pharmacists preferred face-to-face teaching to online teaching, a finding similar to those of Gelayee et al., 37 Driesen et al. 22 and Kassab et al. 38 Advantages of face-to-face lectures are that they are onsite and involve full interaction between lecturers and trainees. Online courses are constantly evolving and also have several advantages, such as freedom of study, anonymity and ease of use. 39 However, online teaching does not permit interaction; 39 as such, it can be considered a complementary teaching approach. 40 There is evidence from other studies in other countries that some pharmacists prefer to learn alone online. 18 Regarding teaching frequency and duration, pharmacists with different educational backgrounds expressed different needs. It is recommended that training be organized in a stratified way according to trainees’ educational backgrounds. The duration of most of the training courses (e.g., those on TCM drugs, drugs for cerebrovascular disease and drugs for digestive disease) was 2 hours (average 1.65 hours). However, trainees felt that the sessions were too short and recommended that teaching sessions for special courses, such as diabetes medication, 41 should last more than 3.14 hours. In terms of knowledge consolidation and assessment, pharmacists with different backgrounds showed differences in their evaluation of the assignment amount and examination method. This training was based on the practice of checking prescriptions. However, some departments in specialized secondary medical institutions contained fewer patients, so some trainees had difficulty completing the assignments and expressed low satisfaction.
The issues discussed in the 20 courses are encountered in all countries,1–4 despite global differences in healthcare systems and resources. Prescription errors are an international problem with serious consequences,5–7 and so must be addressed. This study demonstrated the usefulness of an intensive CPD that helped pharmacists in their prescription-checking tasks. Although it was implemented in China, this training program and its principles are relevant to any region of the world, as prescription errors are a global issue. Future research will include a nationwide study of this training program and its quantitative effects on the rate of prescription accuracy. The main principles of this training could be implemented and explored in hospitals in other countries.
There were several study limitations. Trainees avoided selecting extreme response options, which resulted in central tendency bias. They also tended to repeat the same responses, which led to decision inertia bias. It is possible that trainees expressed the responses expected, so the results may be characterized by social desirability bias. A higher proportion of trainees came from tertiary hospitals and a smaller proportion from primary medical institutions, so the results may be more representative of the experiences of pharmacists in tertiary hospitals. Finally, many of the correlations were low and of borderline significance. This may reflect the sample size and the use of self-evaluations. These findings should therefore be interpreted with caution pending validation.
In conclusion, pharmacists expressed a high demand for prescription-checking training. Pharmacists enrolled in this training showed high satisfaction and good examination results. The key points of this prescription-checking training were training organization and knowledge consolidation and assessment. It is recommended that training be conducted in a stratified way according to pharmacists’ educational backgrounds, to improve pharmacists’ prescription-checking competency. The trainees favoured face-to-face lectures and interactions. Therefore, training in clinical disease-related knowledge should be supplemented with more interactive learning.
Footnotes
Acknowledgements
The authors thank the experts who provided valuable comments about questionnaire design, and the respondents who participated in the survey.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Declaration of conflicting interest
The authors declares that there is no conflict of interest.