
Abstract
Among non-gender conforming populations, there is a subgroup of individuals who experience significant distress associated with their gender incongruity, commonly referred to as gender dysphoria (GD). In the UK, there is a recognised pathway for individuals experiencing GD. This has traditionally been initiated by a referral to the Gender Identity Development Service (GIDS) for children and adolescents or to a Gender Identity Clinic (GIC) for adults. This pathway can potentially involve several specialties and treatment modalities, including the prescription of various hormones. It is important for orthodontists to have an understanding of this field, as well as the potential treatment modalities, so that they can support this often marginalised patient group. Inherent differences between male and female facial features may also lead patients with GD to present to orthodontists, wishing to change their facial appearance. This article highlights the current national pathway for GD and the orthodontic considerations for these individuals.
Introduction
In recent decades, the traditional gender categories of male and female have been replaced by a more fluid, non-binary concept of gender identity. Transgender individuals represent those whose own internal sense of gender is incongruent with their outward appearance, with affected individuals often reporting feelings of psychological alienation from their own body (Ong et al., 2017). This represents a much more complex phenomenon than a simple lifestyle choice.
According to the DSM-V criteria, gender dysphoria (GD) occurs when a fundamental incongruity exists between an individual’s assigned birth sex and their perceived gender. For a diagnosis to be made, the discrepancy must have existed for over six months and resulted in clinically significant levels of distress or functional disability (American Psychiatric Association, 2013). Importantly, GD exists across a wide spectrum and is not experienced by all non-gender-conforming individuals. Although the aetiology of GD is not fully understood, it is likely to be multifactorial in nature (NHS England, 2020).
The prevalence of GD is also difficult to substantiate, with differences arising from the various assessment methods used by researchers to define a case. Such figures are underestimated with the aforementioned DSM-V criteria and overestimated when based upon self-reporting. Current estimates suggest that almost 0.5% of the UK and US adult population are transgender (Meerwijk and Sevelius, 2017; Titman, 2014), although no accurate figures have been reported among children (Zucker, 2017).
Within the UK, the number of referrals to the Gender Identity Development Service (GIDS), the UK tertiary centre responsible for children and adolescents with GD, has increased 10-fold over the last decade (GIDS, 2021). This is likely to be attributable to a combination of widening societal acceptance of transgenderism and improvements in the availability of safer treatments (Aitken, 2017). This increase has been accompanied by a change in UK referral demographics; from a predominant case-mix of assigned males at birth presenting during early childhood towards a case-mix consisting primarily of assigned females at birth, presenting in their early teens (de Graaf et al., 2018). The increase in referrals and tendency towards adolescent presentation makes it particularly important for orthodontists to possess a working knowledge of this field, as it is likely to affect an increasing proportion of our adolescent patient base.
Considering that gender reassignment is a protected characteristic under the Equality Act (2010), reports of barriers and discrimination within healthcare settings among this patient group are disappointing (Quinn et al., 2015). GD and its related management, a topic that is rarely integrated into healthcare teaching programmes (Aitken, 2017), is likely to represent unfamiliar territory for many orthodontists. There is therefore a need to educate and support clinicians in this area.
An overview of GD
Gender identity refers to our own internal sense of belonging to a particular gender (NHS England, 2020). This differs from sexual orientation, which is our romantic and sexual attraction to others (Figure 1). As gender identity is usually acquired by the age of three years, most individuals who experience symptoms of GD will have done so by early childhood (NHS England, 2020). GD is of particular concern if it occurs during adolescence, due to the onset of puberty and the widening social divide between teenage boys and girls. In this age group, GD is associated with an increased risk of self-harm, social isolation and relationship difficulties (NHS England, 2016). Fortunately, in most instances, symptoms of GD resolve after adolescence.
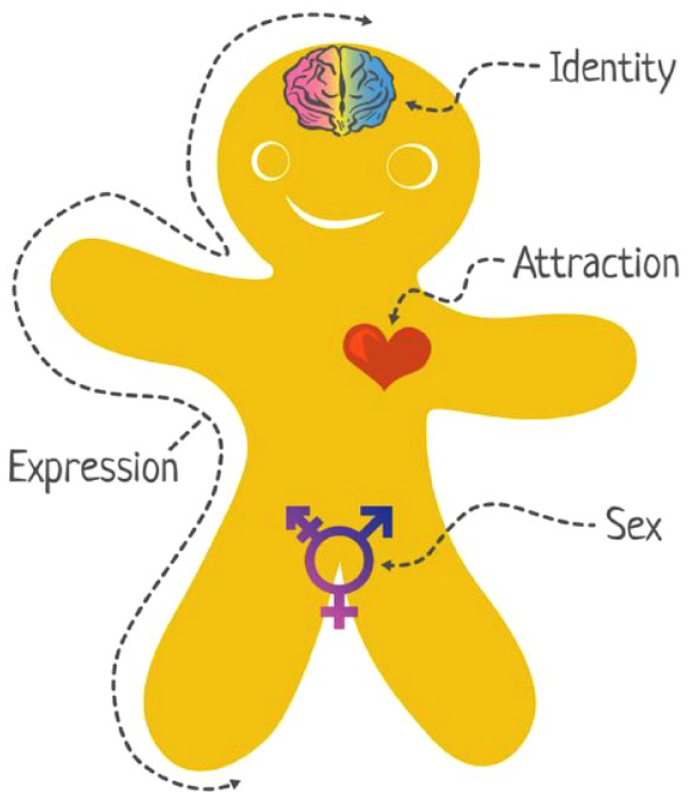
The Genderbread person. Available at: https://www.genderbread.org/.
The World Professional Association for Transgender Health (WPATH) has developed guidelines for the management of children and adolescents with dysphoria, based on the principle that individuals will vary in the type and extent of interventions required to alleviate symptoms (Coleman et al., 2012). These guidelines emphasise the importance of a multidisciplinary approach, potentially involving hormonal therapy, surgery and mental health support. Additional input from speech and language therapists, dermatologists and sexual health physicians may also be required.
Within the UK, children and adolescents with GD have been managed by GIDS since its inception in 1989 (NHS England, 2020). This service has been based at the Tavistock and Portman NHS Foundation Trust since 2009, with the subsequent development of two satellite sites in Leeds and Bristol to cope with the aforementioned increased service demands (The Cass Review, 2022). Due to the vast geographical boundaries covered by these units, care has often been shared between GIDS and local Child and Adolescent Mental Health Services (CAMHS). After referral, the pathway begins with a psychosocial assessment to confirm a diagnosis of GD and to establish its severity, before a period of monitoring over the initial stages of the Tanner classification, an adolescent physical development scale. Significant changes to this pathway are anticipated as a result of an ongoing independent review into the management of children and adolescents with gender dysphoria (The Cass Review, 2022).
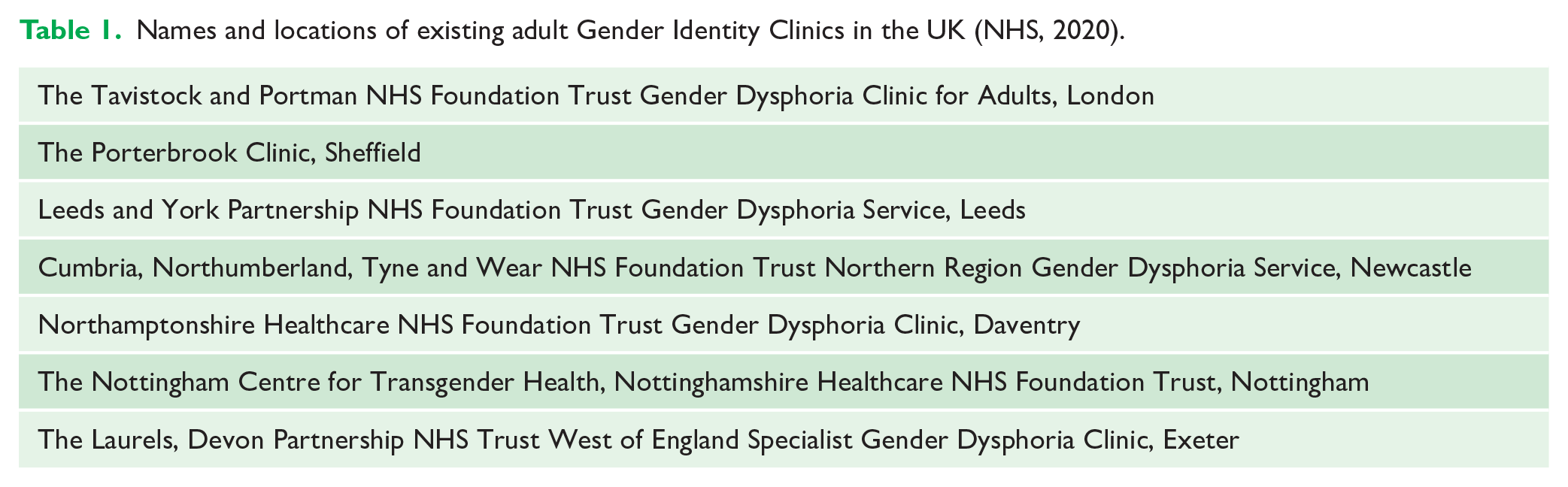
This pathway contrasts with the management of adults experiencing GD in the UK, which is via a number of regional adult Gender Identity Clinics (GICs) (Table 1). In England, there is currently no requirement for either prior funding approvals from commissioners or for a mental health assessment before these patients are referred (Ahmad et al., 2013).
Names and locations of existing adult Gender Identity Clinics in the UK (NHS, 2020).
Transitioning
Transitioning refers to the process by which an individual actively chooses to live in a gender role that differs from their assigned birth gender. There are three well-defined aspects of transitioning: social, biological and surgical. Whatever individual preconceptions we may have towards this treatment, clinicians should be aware that transitioning improves quality of life and reduces symptoms of dysphoria for approximately 80% of patients (Zucker et al., 2016).
Social
Social transitioning tends to involve an individual making changes to their appearance, preferred pronouns and name to align with their preferred gender identity. While families will vary in the extent to which they enable children to socially transition, UK nationals can change their name legally at any time via the Gender Recognition Panel (Ahmad et al., 2013). There is a lack of evidence into the long-term effectiveness of enabling social transitioning during early childhood (Coleman et al., 2012). For some individuals, social transitioning is sufficient to address their dysphoria and no form of additional treatment is sought.
Biological
Biological transitioning refers to the prescription of exogeneous sex hormones that can be divided into puberty blockers (PBs) and cross-sex hormones (CSHs) (Aitken, 2017). Importantly, while these are generally considered to be safe, there is currently limited evidence to support their long-term effectiveness (NICE, 2020a, 2020b).
Gonadotropin-releasing hormone analogues (GnRH), also known as PBs, can be used to suppress hormone production and therefore the development of sexual characteristics during puberty. PBs are only used for adolescents as adult patients will have already developed sexual characteristics related to their assigned birth gender. The aim of this approach is to reduce the distress associated with pubertal changes and to provide breathing space for affected adolescents to consider whether transitioning is the correct course of action for them (Ahmad et al,. 2020). There are additional proposed benefits of PBs; for example, by pausing breast development, an individual may manage to avoid having invasive surgery later on.
Although PBs are considered to be reversible, if stopped then there will still be a delay in returning to normal fertility levels. As a result, the decision to prescribe PBs is not taken lightly and should be made in a multidisciplinary team environment (NHS England, 2020). This decision is based upon several factors, including the severity of dysphoria and the individual’s Tanner stage, with prescription delayed until Tanner stage 2 (i.e. when the patient has reached puberty).
For assigned males at birth, PBs pause growth of facial and body hair, laryngeal prominence and the sexual organs. They also halt the development of any characteristic vocal changes. For assigned females at birth, PBs will pause breast development and the menstrual cycle. In both instances, somatic growth, libido development and fertility levels will be affected.
After further psychological assessment, if an adolescent then wishes to proceed with the transitioning process, CSHs may be prescribed (Delemarre-van de Waal and Kettenis, 2006). These are gender-affirming hormones consistent with an individual’s experienced gender. For example, a trans male may be prescribed testosterone for the hormone’s masculinising effects. Importantly, CSHs have several irreversible effects, including sterility. Before commencing CSHs, patients may therefore be referred to fertility specialists for advice regarding gamete retrieval and storage (Ahmad et al., 2020). As a result of their irreversible nature, CSHs can only be prescribed from an individual’s 16th birthday in the UK (NHS England, 2016).
There are some important side effects of these hormonal medications upon wider health. PBs can influence mood, potentially leading to depression, and can reduce bone density in the short term (Cohen-Kettenis and Klink, 2015). CSHs can affect liver function and are associated with an increased risk of thrombo-emboli (Aitken, 2017). As a result, clinicians should make appropriate recommendations regarding consumption of alcohol and smoking cessation (Ahmad et al., 2020). Blood tests are used to monitor for these unwanted side effects. This is usually performed by general practitioners, outlining the importance of effective communication channels between primary care and tertiary gender services.
There has been a renewed media interest surrounding hormonal treatments as a result of the UK High Court case against the Tavistock and Portman Trust (Bell v Tavistock, 2020). During the trial, several post-transition patients successfully argued that they lacked capacity as adolescents to understand the mid- to long-term consequences of the PBs that they had previously been prescribed. The case was centred around the evidence that a very high proportion of patients who commence PBs will ultimately progress onto irreversible CSHs (de Vries et al., 2011). Three High Court judges initially ruled that patients aged younger than 16 years were unlikely to be able to give informed consent and that this age group should therefore only be prescribed PBs if they were deemed to have capacity after an individual court hearing. This outcome had a significant impact on the UK population of children and adolescents awaiting treatment by GIDS, before the ruling was subsequently overturned by the Court of Appeal. The current state of affairs is therefore that PBs can still be prescribed in adolescents, provided that their treating healthcare professionals deem that they have capacity to understand the implications of this decision.
Concerns regarding GIDS have led to an independent review of the service (The Cass Review, 2022). In her interim report, Hillary Cass made recommendations to transform the current national pathway to a model encompassing regional centres. This recommendation was related to a combination of GIDS’ difficulties in dealing with increased waiting lists and concerns over individuals with GD not always being managed holistically within the broader context of any additional healthcare issues (The Cass Review, 2022). As a result, the GIDS is expected to close by spring 2023 and will be replaced by new ‘early adopter’ centres in London and Liverpool, with more to follow. Significant changes are therefore expected in the UK care pathway for adolescents in the near future.
Surgical
The irreversible step of gender alignment surgery may follow hormonal therapy but only for individuals aged over 18 years. In the UK, this aspect of care is managed by adult services. Most individuals will have lived in their preferred gender role for some time before considering surgery. These procedures range from the relatively simple, such as hair removal, to more complex operations including chest reconstruction, genital reassignment and facial feminisation surgery. Many transgender patients will have little desire to undergo this aspect of transitioning.
Orthodontic implications
Mental health
Individuals with GD represent a potentially vulnerable patient group due to the association with psychosocial difficulties and mental health issues, with over 50% experiencing psychopathology during their lifetime (Zucker et al., 2016). Although transitioning treatments are associated with improvements in mental health, issues can persist, particularly for those with mood and anxiety disorders (Constantino et al., 2013). Self-harm and suicide ideation are also more frequently reported among transgender patients. Orthodontists should be able to discuss mental health support with any transgender patient in distress. The higher incidence of safeguarding cases among transgender populations should also be borne in mind when managing this patient group (Salkind et al., 2019).
The prevalence of autistic spectrum disorder (ASD) and other types of neurodiversity among gender dysphoric individuals is significantly higher compared to the general population: 10% versus 1% (NHS England, 2020). The frequency of this co-occurrence has even led to the development of guidelines for the co-management of ASD and GD (Strang et al., 2018).
From an orthodontic perspective, patients with ASD should ideally be treated by the same clinician throughout and waiting times should be minimised (Alawsi et al., 2020). Orthodontists should also consider treatment plans with manageable objectives to establish patient cooperation levels. ASD is associated with a tendency towards oral sensitivity and there is an increased association with epilepsy.
Influence on growth
Orthodontists should be aware of the potential impact of PBs upon the onset and progression of the adolescent growth spurt. This is of particular relevance for adolescents with Class II skeletal and incisal relationships being treated with a functional appliance and for patients with Class III malocclusions. In such instances, orthodontists should liaise directly with the treating paediatric endocrinologist to clarify the intended transitioning plan and its potential to impact upon that individual’s adolescent growth spurt. This interaction is fairly complex and is influenced by the direction of gender transition, the type and dosage of hormones prescribed, the developmental stage at which they are prescribed and individual response to these medications.
Orthognathic surgery
Current guidelines recommend that when transgender patients require procedures not directly related to their dysphoria, they can be referred directly to the relevant specialty and not via a GIC (Wylie et al., 2013). Some patients with gender identity concerns may initially present to an orthodontist seeking to change their facial appearance using orthognathic surgery. If these patients have not already been seen by a tertiary gender service, then they should be referred at this point. Although the mandatory use of psychologists has been suggested as part of the normal orthognathic surgical pathway (Ryan et al., 2011), these are currently the exception rather than the norm. Due to the impact that orthognathic surgery has upon facial appearance, we recommend early psychology involvement at the decision-making stage.
It is important to consider the influence of gender upon the acceptability of facial appearance and form during the surgical planning stage. Females tend to have rounder, softer faces, with less prominent foreheads, while males tend to have more prominent squarer chins, flatter cheeks and larger noses (Altman, 2012). A Class II skeletal pattern is often more suited to females, while a Class III skeletal pattern can often be carried better by males (Parker et al., 2019). This is important to bear in mind for transitioning patients whose skeletal pattern is less cohesive with their preferred gender identity. Similarly, the planned final amount of incisal show may be influenced by an individual’s new gender, with a slightly greater amount of gingival show on smiling often more desirable in females.
Orthognathic teams should also consider the impact of CSHs on liver function and therefore bleeding risk and drug metabolism, which require investigation before elective surgery (Ahmad et al., 2013). CSHs are also associated with an increased risk of thrombo-embolism and smoking cessation advice should be given to patients. For transgender patients having orthognathic surgery or adjunctive oral surgery procedures, it is important to specifically check which hospital ward the patient would prefer to be on (General Medical Council, 2016).
A separate entity is facial feminisation surgery (FFS), which aims to feminise an individual’s facial features. This encompasses a number of procedures that can be performed for both trans females and females wishing to further feminise their facial appearance (Parker et al, 2019). These include forehead reduction, rhinoplasty, implant-assisted cheek augmentation, lip lifts and thyroid shaves (Altman, 2017). Trans females may undergo FFS before any other form of gender reassignment surgery as it assists them in passing as female in society.
FFS is usually undertaken by orthognathic or craniofacial surgeons, with NHS eligibility dependent upon a prior approval process (Parker et al., 2019). Access to this treatment may therefore be somewhat of a postcode lottery dependent upon local commissioning guidelines. There are competing interests between performing several FFS procedures simultaneously to mitigate against the risks of repeated general anaesthetics and performing individual operations to allow patients to reassess their desire for further intervention without over-treating.
Referrals to tertiary gender services
Referrals related to GD can be made by a general medical practitioner (GMP), local CAMHS or by another health professional. If an orthodontist is the first point of access for a patient with significant GD, then it may be appropriate for them to make a referral to a tertiary gender clinic. While adults can be referred directly to a GIC, children and adolescents should ideally be referred via CAMHS initially (Ahmad et al., 2013). Clinicians must ensure that consent has been obtained before making a referral. Self-referrals are not accepted.
The increased demand for this service, coupled with the impact of the COVID-19 pandemic, has resulted in significant waiting times (GIDS, 2021). This is a particular concern for the subgroup of dysphoric individuals with co-existing mental health issues. If required, GMPs are permitted to prescribe bridging endocrine treatments for adults with more severe GD as an interim measure. Therefore, if orthodontists are considering making a referral for a patient with GD where mental health is an acute concern, they should also liaise directly with the relevant GMP so that patients can be supported appropriately.
Recommendations for clinicians
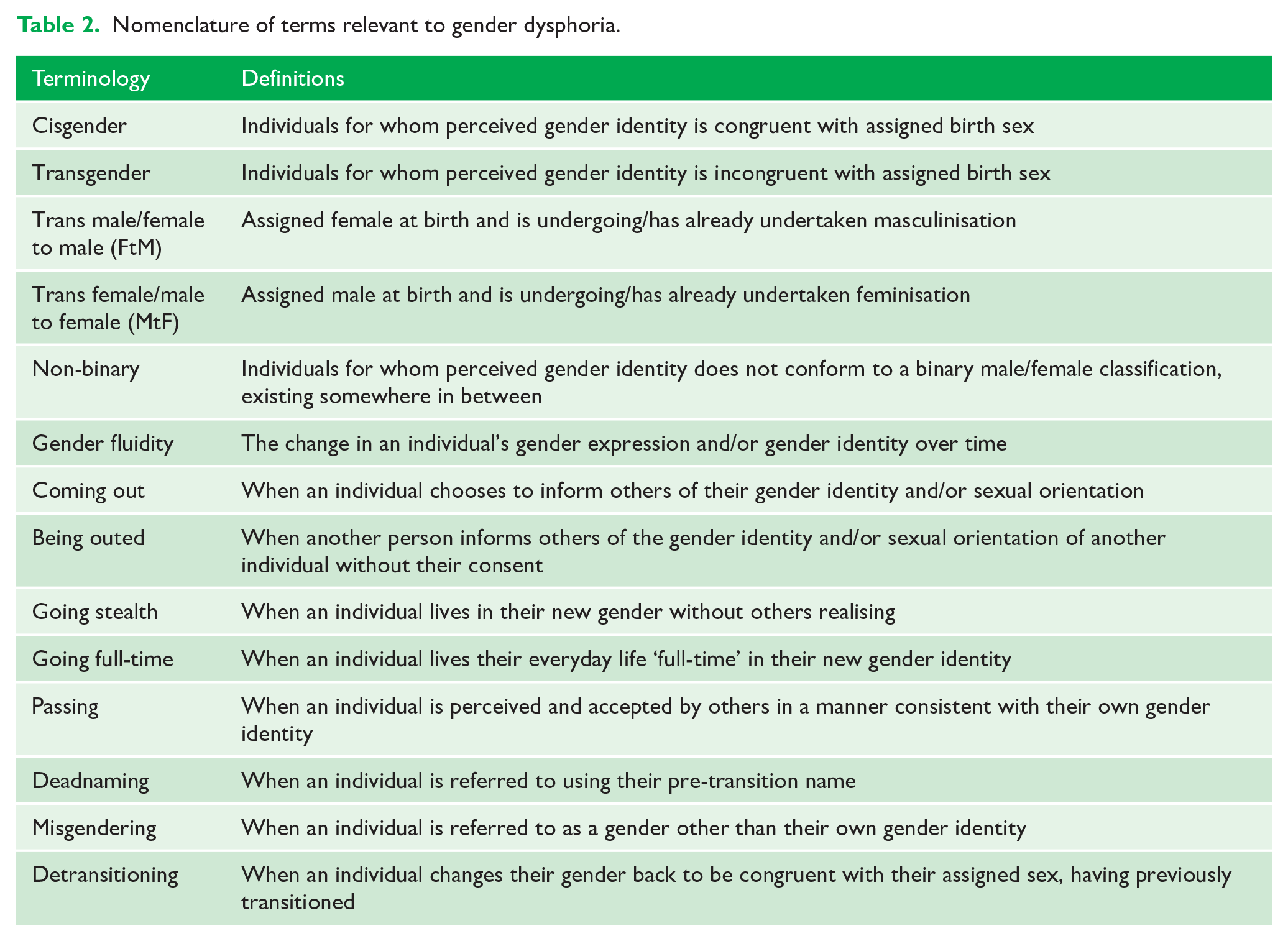
There is no shared consensus about the best language to use in this area and the terminology is constantly evolving; however, we recommend readers familiarise themselves with the nomenclature highlighted in Table 2. Paying careful attention to language is likely to make patients feel more comfortable in the clinical environment. This extends to accurate recording of preferred gender, names and pronouns in clinical records, which should be easily detected at future appointments. The potentially damaging effects that misgendering or deadnaming can have upon an individual and their subsequent trust in healthcare professionals should not be underestimated (General Medical Council, 2016).
Nomenclature of terms relevant to gender dysphoria.
If transitioning occurs partway through orthodontic treatment, then patients may choose to update their medical records to reflect this. This can be done without having to wait for a new NHS number, birth certificate or gender recognition certificate and should be universally applied by all staff. Inflexible medical forms have been highlighted as an additional hurdle for these patients when accessing healthcare (Shepherd and Hanckel, 2021). Patient labels should be reprinted with up-to-date, accurate information.
Lead clinicians should consider how they can improve the accessibility and acceptability of their services to transgender patients and should also consider how to educate staff appropriately on this as part of their equality, diversity and inclusion training.
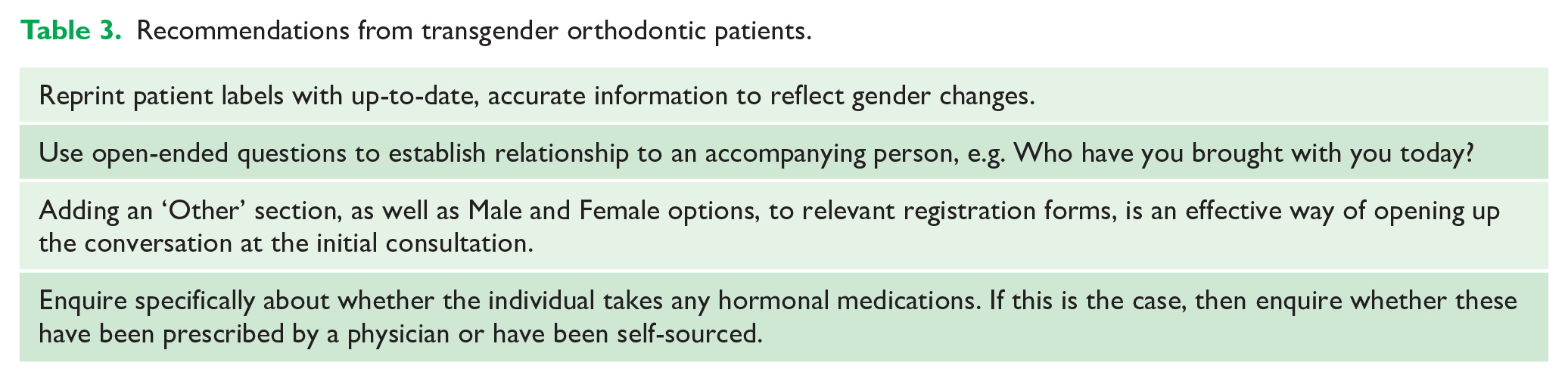
Various recommendations, gleaned from discussions with transgender patients in our services, are outlined in Table 3. These also reflect useful lessons that the authors have learnt in the management of individuals with GD.
Recommendations from transgender orthodontic patients.
Recommendations for orthodontic researchers
The majority of the existing evidence for the effectiveness of GD interventions stems from observational studies with limited follow-up, with a distinct lack of well-designed randomised clinical trials and cohort studies (The Cass Review, 2022). This deficiency is partly related to difficulties in recruiting minority groups into research but is exacerbated by healthcare barriers and differences in the legal status of transgender individuals across countries. Unsurprisingly, this paucity of research extends into the dental and orthodontic implications of gender transitioning (Hania et al., 2021).
The transgender community represents a relatively small patient population. This is compounded by the fact that participants in transgender research often represent those who have actively sought treatment for GD. Greater efforts should be made to ensure that the rest of the transgender population is also included in research to minimise this risk of selection bias. To ensure sufficient participant numbers, research should ideally be conducted between multiple centres at a national or international level.
There are several areas where further research is likely to influence orthodontic practice. These include, but are not limited to:
Qualitative investigation of perceived barriers among transgender individuals accessing dental and orthodontic treatment. Individual interviews and focus groups would enable a deeper understanding of transgender patients’ views of these areas. This research method is particularly relevant given the potential sensitivity of the subject.
Investigation of differences in the peak height velocity of the adolescent growth spurt, and the associated peak in mandibular growth, between transgender patients receiving PBs and cisgender controls. Prospective cohort studies using transgender groups and cisgender control groups matched for age, medication type and dose would be useful to assess the impact of PBs on growth using the Cervical Vertebral Maturation Index (Baccetti et al., 2005).
Qualitative investigation of the perspectives of patients with GD at various stages of the orthognathic pathway.
Conclusion
Significant changes to the existing UK pathway for patients with GD are planned to manage the increase in referrals and to meet the recommendations from The Cass Review (2022). However, the care of transgender patients is not solely the remit of gender identity services; it represents everyone’s business. Orthodontists should be aware that transgender patients face barriers when accessing healthcare and should therefore ensure engagement with this patient group in their own clinical practice. Further research is required to answer clinically relevant questions regarding the impact of hormonal medications upon orthodontic treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.