
Abstract
This article critically reviews the literature on urban informality, inequity, health, well-being and accountability to identify key conceptual, methodological and empirical gaps in academic and policy discourses. We argue that critical attention to power dynamics is often a key missing element in these discourses and make the case for explicit attention to the operation of power throughout conceptualization, design and conduct of research in this space. We argue that: (a) urban informality reflects the exercise of power to confer and withhold advantage; (b) the dominant biomedical model of health poorly links embodied experiences and structural contexts; (c) existing models of accountability are inadequate in unequal, pluralistic governance and provision environments. We trace four conceptual and empirical directions for transformative approaches to power relations in urban health equity research.
I. Introduction
Improving life in cities is central to several Sustainable Development Goals (SDGs) on health and well-being (3), reducing inequalities (10) and improving sustainability (11). An estimated 881 million people in low- and middle-income countries (LMICs) live in precarious, marginalized urban areas (UN-Habitat, 2012). These residents experience worse health outcomes than those elsewhere in the city and in rural areas (Ezeh et al., 2017; Nunes et al., 2016). Living in informal urban areas fundamentally affects health and well-being, as both prerequisites and outcomes of sustainable development.
Residents of urban informal spaces are characterized as the ‘urban poor’, or people living or working in precarious locations, colloquialized as ‘slums’ or ‘informal settlements’. The terms ‘slum’ or ‘informal settlement’ refer to areas with high population density, insecurity of land or housing tenure, precarious legal designation by the state and limited inclusion in state urban planning or provision (UN-Habitat, 2012). These depictions obscure huge variations between settlements in terms of state recognition, duration of establishment, population ‘churn’, land ownership, security of housing tenure and geographic features. The most marginalized people may live within or outside the boundaries of recognized urban settlements, for example, on pavements. Our use of terms such as ‘urban poor’ or ‘informal’ is not indicative of our acceptance of the problematic binaries associated with these terms, and we seek to problematize them. We use the concept of ‘urban informal spaces’, as coined by Chiodelli and Tzfadia (2016).
Urban informal conditions harmful to health and well-being are proliferating and social inequalities are increasing (TLP Health, 2020). It is clear that a radical rethink is required to progress towards the SDGs (World Bank, 2020). In this article, we argue, in line with Gupte and Mitlin (2020), that there are critical conceptual deficiencies and empirical gaps in the dominant approaches to health, well-being and inequities in informal urban spaces. Attention to the underlying drivers of the problem is central to the realization of the SDGs. This necessitates interrogation of the concepts of informality, health, well-being, equity and accountability and their macro-level determinants in informal urban space.
This article reviews the literature on urban informality, inequity, health, well-being and accountability to identify key conceptual gaps and deficiencies in relation to scholarship and academic discourses on accountability for equity in health and well-being in informal urban spaces. The authors are members of a research consortium, Accountability for Urban Informal Equity (ARISE). ARISE spans 13 institutions from five countries (Bangladesh, India, Kenya, Sierra Leone and the UK), including universities and NGOs ensuring extensive, multi-disciplinary expertise. Members are diverse in terms of gender, nationality, ethnicity and professional identity. We make the case for explicit attention to the operation of power throughout conceptualization, design and conduct of research in this space.
We begin by elaborating how we understand power. We then illustrate gaps in the literature on informality, health, well-being and accountability in relation to power. Such conceptual and empirical gaps can foster problematic assumptions about urban informal spaces that perpetuate policy discourses and practices that ultimately may hinder the achievement of the SDGs.’
Finally, we propose conceptual directions needed for advancing research for action in this area and argue that reflexive, intersectional analyses of practices of power and methodologies that actively engage with these dynamics are required for researchers to contribute towards positive change.
II. Our Understanding of Power
Investigations of ‘power’ aim to understand people’s abilities to affect outcomes relevant to their lives and to assign responsibility and answerability to engender desirable outcomes (Hayward and Lukes, 2008). Power is dynamic, relational and exercised in daily life through social practices. However, in exercising power, individuals draw on a range of historically and contextually specific social, economic, institutional and political resources which are unequally distributed. Intersectionality is a relational, analytical and political approach that explores ‘how each individual and group occupies a social position within interlocking structures of oppression’ as well as being ‘concerned with the macro-level connections linking systems of oppression such as race, class, and gender’ (Hill Collins, 2002). We conceptualize intersectionality as multiple interacting forms of social hierarchy — based on gender, age, class, caste, religion, (dis)ability or sexuality for example—working simultaneously at multiple levels. These intersecting inequalities: (a) shape individuals’ and associated groups’ identities (which are often overlapping), (b) are expressed and evolve through processes of negotiation, contestation, inclusion and exclusion, (c) make it difficult for marginalized people to assert power either individually or collectively, in order to overcome structural and social discriminations and are (d) structurally embedded in multiple inequitable systems of social organization—simultaneously patriarchal, elitist, nativist and/or heteronormative to varying degrees (Crenshaw, 1989).
Intersectionality operates ‘simultaneously at intrapersonal, interpersonal, institutional and society-wide levels’ (Connell, 2012: 1677) to constitute unique social locations. Caste, class and gender do not interact as separate entities; they mutually constitute a particular form of embodied social practice within the caste system that is also shaped by histories of colonialism and globalized capitalism. For example, waste-picking communities in India are among the most marginalized in urban informal spaces. They belong to a range of oppressed castes (broadly called Dalits), whose role is ‘naturalised’ within the caste system. The lives of both female and male waste-pickers are shaped by patriarchal power relations. Waste-picking tasks are segregated by gender, with poorly remunerated tasks labelled women’s work. Female waste-pickers are subject to violence and harassment in public spaces that is seen as justified by their gender, occupation and caste, while male waste-pickers often suffer police harassment. Female waste-pickers, in common with other women, also suffer further disadvantages in the private sphere, including intimate partner violence and unequal divisions of labour within the household (Ambedkar, 1989).
In order to identify challenges and opportunities to contribute towards social justice in urban informal spaces, researchers need to conduct reflexive, intersectional analyses, which unpack how particular configurations of macro-meso-micro forces create power regimes that facilitate or impede equity and social justice in particular contexts and times. These power relations draw on multiple intersecting and multi-scalar orders, which play out in historical and context-specific ways. In the following sections, we analyse how far these understandings are reflected in the current literature on urban informality, health and well-being and accountability and identify critical gaps.
III. Understanding Accountability for Equity in Health and Well-being in Informal Urban Spaces
Urban Informality and the Exercise of Power
For decades theories of urbanism have juxtaposed the formal and the informal, with informality habitually viewed as a policy problem (McFarlane, 2012; Porter et al., 2011). The formal/informal binary offers a powerful heuristic device (McFarlane, 2012), which remains pervasive in policy discourses. However, it often functions to delegitimize the claims to housing, work and livelihoods that the urban poor make on the city and minimise their contribution to city functioning. The inadequacies of this formal/informal binary are well-recognized in academic debates (Banks et al., 2019). Khan et al. (2023) argue that in labelling ‘slums’ stigmatization is mobilized by the state as an instrument of power. In alternative critical conceptualizations, formality and informality are seen as parts of an interconnected system, within which ‘advantage and disadvantage are conferred…[creating] winners and losers in urban development’ (Banks et al., 2019).
Recent debates about conceptual and empirical (inter)dependencies highlight that ‘Notions of “formal” and “informal” are rarely neutral, and reflect dominant forms of state, corporate, legal, residential, and activist power’ (McFarlane, 2012: 103). The state is typically seen as having legitimate authority to define the boundaries between formality and informality, through laws and regulations, public policy, licensure and urban planning. Roy (2005) asserts that the state both perpetuates and takes advantage of the ambiguity in such boundaries to suit its own ends. The designation ‘informal’ itself therefore reflects the exercise of power.
How urban informality is framed and treated varies through space and time, since it reflects the exercise of power by governing elites and the outcomes of ongoing contestations between a context-specific array of state and non-state actors (Harriss-White, 2019). For example, the language used by the Indian state has shifted. It once recognized the presence of people living in informal urban spaces and acknowledged responsibility for providing shelter and access to services. It now frames them as illegally squatting on state land (Bhan, 2020; McFarlane, 2012). In contrast, in low- income neighbourhoods in four sub-Saharan African cities, ‘Residents here, once seen by authorities as illegitimate squatters, are now considered legitimate customers’ (Mitlin and Walnycki, 2019).
People living and working in these spaces need to navigate and negotiate with diverse actors to pursue their interests, mobilise resources and gain access to a range of services to promote their well-being. These include government officials at various administrative levels, NGOs, CSOs, neighbourhood or market trader associations and self-help groups. Their tactics for this navigation and negotiation vary widely and are influenced by the strength of their networks, the potential sources of power available and the relational dynamics between them (Banks et al., 2019; Recio et al., 2017).
Analyses of power dynamics have tended to focus on the role of class in shaping opportunities for urban residents in their engagements with state and non-state actors (Briggs, 2011). The literature also underlines the importance of brokers, from local mafias to political leaders, in enabling residents to take advantage of informal practices to gain or consolidate the privilege bestowed by the state. For example, brokers can facilitate access to government water and electricity or other services, enhance elites’ preferential access to health services, or provide unlicensed street vendors’ access to public space (Anjaria, 2011; Chatterjee, 2004; Jha et al., 2005; te Lintelo, 2017). Brokers exploit niches in the shifting formal/informal boundaries, for entrepreneurial and/or community benefits, depending on the actors and their interests (Corbridge and Jones, 2005). For example, in Dhaka, Bangladesh, both NGOs and private individuals supported marginalized urban people to access COVID-19 vaccination by assisting them to navigate complex online government systems (Alam et al., 2023).
Theorization of urban informality is gathering pace and complexity. However, much of the literature is implicitly grounded in a homogenous conceptualization of class/socio-economic differences which juxtaposes ‘the urban poor’ with ‘the elite’ or the ‘haves’ with the ‘have nots’ (Khan et al, 2023). To inform strategic action, further research should focus on how intersecting power relations influence how successfully people with different social identities are able to navigate the city to improve their health and well-being and their priorities and strategic opportunities for change.
Navigating Health and Well-being
Understanding Health, Well-being and Power in Informal Urban Spaces
There is growing evidence that people living in informal settlements suffer worse health outcomes than both their rural and formal urban counterparts, (Lilford et al., 2017; Sverdlik, 2011), including for infant and under-five mortality, child under-nutrition, injury, acute and chronic infectious disease and non-communicable disease (Corburn, 2016; Ezeh et al., 2017).
Existing approaches have largely taken a ‘territorial view of informality’, focusing on ‘slums’ or ‘informal settlements’ and on biomedically defined ill-health and access to healthcare (Ezeh et al., 2017; Mberu et al., 2016). The immediate determinants of many common health burdens are well-documented, including environmental hazards, violence, lack of water and sanitation and alcohol and drug misuse (Ezeh et al., 2017; Karuga et al, 2022; Smit et al., 2016; Zerbo et al., 2020). However, the complex interactions between these proximal social determinants and more distal sociopolitical, legal and economic marginalization, are less thoroughly explored (Lumagbas et al., 2018). While informal settlements’ heterogeneity is acknowledged, existing epidemiological literature has concentrated on comparing indicators for ‘slums’ with rural and other urban communities and has made the case for the importance of ‘neighbourhood effects’ beyond individual and household risk factors (Ezeh et al., 2017). Understanding how heterogeneity and social inequities within informal spaces shape inequities in health remains under-theorized (Khan et al., 2023).
A focus on biomedically defined health and its links to material conditions in informal urban spaces risks excluding other important dimensions of well-being such as exclusion, social and political connectivity and the lived experience of impoverishment and indignity. These dimensions are captured in the concept of well-being (Gough and McGregor, 2007; McGregor et al., 2007; McGregor et al., 2009; Rojas, 2008; White, 2010). Well-being has been conceptualized as an interplay between material, subjective and relational dimensions of lived experience which is dialectically produced in relation to social, economic and political structures of power (White, 2010). While there are many frameworks and tools for well-being measurement, their application in informal urban spaces and relation to governance structures has been limited (quantitative exceptions are te Lintelo et al. [2018] and Woodcraft et al. [2020] while qualitative exceptions include Karuga et al. [2022] and Kakar et al. [2022]). Psycho-social distress and mental health conditions are often under- recognized and stigmatized elements of health and well-being. Some studies have begun to trace the ways in which physical, psychological and social stressors engendered by structural power relations in turn shape mental ill-health and distress in informal urban spaces (Ayeb-Karlsson et al., 2020; Corburn, 2016; Ezeh et al., 2017; Greif and Nii-Amoo Dodoo, 2015; Lumagbas et al., 2018; Mendenhall, 2014; Mendenhall et al., 2015; Satterthwaite, 1993; Subbaraman et al., 2012). Biomedical discourses and their narrow focus on empirically observable phenomena are themselves entwined in colonial, patriarchal power relations (Sowemino, 2023). In order to counter the power of biomedical discourse to define which health outcomes are valued, the gap in existing approaches could also be narrowed by research methodologies that are oriented to creating space for urban informal residents’ own subjective perceptions, lived experiences and priorities with regard to their health and well-being.
Complexity, Plurality and Power Relations Among Healthcare Providers
There is evidence that although some informal settlement residents have better geographical access to formal health facilities than those living in rural areas, access constraints remain, particularly for marginalized people (MSJ Centre, 2020). These include discrimination (for example, against persons with disabilities and pregnant adolescents), direct financial barriers and indirect costs (Mberu et al., 2016; Smit et al., 2016; Snyder et al., 2017). High out-of-pocket expenditures for private providers in particular, exacerbate ill-health-related ‘poverty traps’ (Ezeh et al., 2017; Shafique et al., 2018; Siqueira et al., 2022).
In the context of limited access to formal healthcare, people seek care from a plurality of providers including private, informal, religious or ‘traditional’ sectors (Fotso and Mukiira, 2011; Mahmud et al., 2015; Shafique et al., 2018; Wilkinson et al., 2020). The term ‘informal’ denotes unregistered, often unqualified and unregulated providers, aligning to the formal/informal binary and obscuring substantial variety in qualifications and scale of operation (Conteh and Hanson, 2003; Cross and MacGregor, 2009). For many informal urban residents, ‘informal providers’ are relied upon because they are approachable, supportive, and less costly (Conteh et al, 2021; Harpham and Molyneux, 2001; Macarthy et al., 2018; Okoth et al, 2023; Rashid et al., 2017). ‘Medical syncretism’ 1 also shapes health-seeking practice and, particularly for those experiencing chronic ill-health, can result in oscillation between ‘formal’ and ‘informal’ providers (Kolling et al., 2010). Furthermore, blurred or ‘porous’ boundaries challenge binary conceptualizations of formal/informal and public/private. For example, formal ‘public’ providers channel patients into private practice and the formal public sector relies on private and informal provision of medicines (Bloom et al., 2008; Harpham and Molyneux, 2001).
The formal/informal binary is hierarchical and reflective of the exercise of power; because of this, not all actors and their contributions are recognized by the health system, which lacks policies for engaging with informal providers and improving their services. While quality in the informal sector is usually assumed to be poor, regulatory frameworks and capacity often limit action to improve this (Wallace et al., 2022). Cross-disciplinary engagement with concepts of informality and intersectionality is needed to inform nuanced analyses of how power relations shape marginalized urban people’s access to trusted, quality providers and strategic opportunities to improve this.
Visibility of Informal Settlements, Inequities and Well-being Within Dominant Urban Approaches
The epidemiological evidence based on health in informal spaces is limited for several reasons that are underpinned by power/knowledge links. First, informal or ‘illegal’ settlements and people living on the margins, including pavement dwellers and people with disability are often excluded from routine household surveys (Subbaraman et al., 2012). Second, city-level health service data are unlikely to be collected from the small private or informal health providers and pharmacies used disproportionately by the urban poor. Third, data are usually aggregated at the city level, with no possibility of disaggregation to show area-level inequities (Elsey et al., 2016; Lucci et al., 2018). A relative lack of formal data and documentation contributes towards the poor visibility of health and well-being challenges in informal urban spaces. However, this lack of data and disaggregation may be strategic, enabling state practices of informality that advantage elites and reduce accountability for service provision (Khan et al., 2023).
Existing approaches to the collection of health data are challenged by the dynamic realities of urban informality, which include highly mobile and transient populations and the need for very context-specific indicators of dis/advantage. Traditional methods of classifying wealth by assets, as used by Demographic and Health Surveys, risk misclassifying urban residents who may be relatively asset-rich (owning televisions or mobile phones), but income-poor due to high accommodation or healthcare expenditure and unstable daily incomes (Zeeb et al., 2020). Furthermore, quantitative research in informal settlements often focuses on specific diseases and only disaggregates on a small number of social strata (e.g. gender, age, wealth quintile). Good sampling and data disaggregation allowing for robust intersectional analysis are rare. One innovative approach that aims to operationalize intersectionality analysis within informal settlements using survey data is the Multilevel Analysis of Individual Heterogeneity and Discriminatory Accuracy (MAIHDA) framework, which was used to analyse intersecting social determinants of children’s health in informal settlements in Bangladesh (Barua et al., 2023). Currently data sources are often insufficient to explain and make visible how the power relations of urban informality shape marginalized people’s experiences of health and well-being, including through the power dynamics that shape pluralistic healthcare. Making power dynamics more visible is a necessary, though not sufficient, step towards change. The next section explores efforts to shift these dynamics by holding governance actors accountable for health and well-being.
Accountability and Governance
SDG Goal 11 recognizes the importance of civic participation in planning and management in cities; specifically reflected in indicator 11.3.2. 2 However, for marginalized urban people, opportunities, processes and potential impacts of such participation depend on power dynamics embedded in their relationships with the state and others.
Accountability Challenges in Informal Urban Spaces
Long-standing bodies of research emphasize the agency of ‘the urban poor’, both in terms of their (often individual) ‘strategies for survival’ (Banks et al., 2019; Mitlin, 2018) and their (often collective) struggles for improvements in their condition and legitimacy (Lines & Makau, 2018; Mitlin 2008; Patel & Mitlin 2004).
However, there are both conceptual and empirical gaps in academic conceptualizations and policy framings of social accountability for rights to health and well-being in informal urban spaces (Patel and Mitlin, 2004). Social accountability literature focuses primarily on holding the state to account via service users’ direct engagement with providers, rather than via the ‘long route’ of citizens mandating politicians to demand accountability on their behalf (Ahmad et al., 2003). Literature on accountability and health focuses even more narrowly on service provision and the tools to assess service quality, such as community score cards and citizen report cards (Björkmanyand and Svenssonz, 2006; Edward et al., 2015). Several influential studies (Fox, 2015; Holland, 2017; Joshi and Houtzager, 2012; Tembo, 2014) have concluded that an initial focus on deploying social accountability tools has overshadowed the wider aim of transforming citizen–state relationships. People in informal spaces find it difficult to draw on the benefits of citizenship. This means that pursuing accountability via the ‘long route’ depends less on conventional democratic representation and more on informal political bargaining, described as ‘the politics of the governed’ (Chatterjee, 2004). Such bargaining may employ a range of visible, invisible, conventional and unorthodox tactics by individuals, groups and organized social movements including peaceful protests; evidence-based advocacy; brokerage and mediation; and ‘rude accountability’ through rioting and violent action (Hossain and Scott-Villiers, 2017). For example, there was looting in Dhaka during the trauma experienced in COVID-19 lockdowns (Rashid et al., 2020) and protesters attacked businesses and government offices in Freetown in August 2022 as part of demonstrations against soaring costs of living, including doubling of food prices (Akinwotu, 2022).
Though evolving, studies on accountability in health systems tend to focus on rural settings, where ‘formal’ provision tends to be dominated by state or state-contracted primary care facilities (Cross and MacGregor, 2009). Most of the health systems accountability literature in urban settings focuses on ‘short route’ accountability mechanisms targeting government facilities (Few et al., 2003; Mosquera et al., 2001; Mcnamara, 2006; Paul, 2002). Yet, the pluralism of providers in informal urban spaces creates specific kinds of challenges for people seeking accountability in relation to their rights as service users (Bloom et al., 2008). Private-public partnerships are often presented as a solution to limited government service provision capacity (Parker et al., 2019). While in some contexts some formal private services are available, they are often unaffordable for the poorest and most marginalized, who lack both mechanisms and leverage to hold them accountable. Limited evidence on efforts to hold private sector organizations accountable via ‘short route’ mechanisms in Nairobi suggests that relations between service users and childcare providers are purely contractual, thus responsiveness by providers is dependent on users’ capacity to pay (Chumo et al., 2022). In some cases, layering sub-contracts may be a neo-liberal strategy to avoid state accountability for the well-being of urban marginalized people, as observed in the sub-contracting of urban waste workers in India where multiple sub-contracts distance the responsibility of the state for the occupational health of waste workers (Saligram, 2022).
An analysis of private sector participation in the control of COVID-19 in four LMIC health systems also identified a lack of government regulatory capacity as a key challenge to governments holding private providers accountable (Wallace et al., 2022). There are some examples of initiatives to improve the quality of the informal private service providers who are most accessible to the urban poor and develop referral links to public services (Simwaka et al., 2012; van de Vijver et al., 2013). Efforts to systematize these initiatives, for example, by accrediting informal providers, are in their infancy and face significant challenges of mistrust between the state and informal providers, limited state supervision, monitoring and regulation capacity (Onwujekwe et al., 2022).
Research may contribute to promoting social accountability initiatives that effectively tackle the barriers experienced by marginalized urban people, by mapping formal as well as informal power relations that shape the wider accountability ecosystem (Halloran, 2016), which often comprises a complex landscape of shifting regimes (Trajber Waisbich et al., 2019). It is important such analysis for action is informed by insights from people with different social positionalities in urban informal spaces to avoid unintended consequences of interventions, since arrangements are embedded within local moral economies and power relations.
Power, Intersectionality and Participation
Most social accountability mechanisms, whether state-initiated (e.g., health councils, public hearings) NGO-led (e.g., community scoring of services, social audits), rely on the participation of citizens, service users and communities. Participation is mediated by existing hierarchical socio-cultural structures and relations. This means that issues facing less powerful people are less likely to be raised or prioritized (Domingo, 2015; Lodenstein et al., 2017; Rashid, 2004). For example, explorations with female waste workers in Shimla, India, identified that while they experienced significant occupational challenges with menstrual health, they did not raise these in discussions within male-dominated unions (Dash and Garimella, 2022). Some marginalized people are excluded from such meetings altogether; for example, inaccessible meeting spaces limit participation for many people living with disabilities and invisible social and spatial barriers may reinforce caste-based exclusion (Castán Broto and Neves Alves, 2018). Furthermore, dominant ideologies shape perceptions of what is acceptable and possible, through the exercise of ‘invisible power’ (Gaventa, 2006). Systematic discrimination and marginalization may limit the political voice and agency required to meaningfully participate in shaping agendas in ‘invited spaces’ created by the state and/or NGOs. For example, informal waste workers in Vijayawada and Guntur are highly dependent on local NGOs for basic survival in crises, which in combination with their location at the apex of multiple systems of social and political marginalization severely limits their capacities to voice their priorities (Kakar et al., 2022). An intersectional approach to accountability may inform understanding of how power relations and social indices of difference shape meaningful participation in existing accountability spaces and how these can be transformed.
Self-enumeration’ and neighbourhood mapping have been a critical strategy used by social movements of the urban poor as tools for advocacy and visibility and for building individual and collective legitimacy, political and social awareness (Patel et al., 2012; Porter, 2011). These movements have demonstrated that mobilization, coalition-building and campaigning are as important as knowing how to use formal, legal mechanisms (Mitlin, 2018). Collective advocacy and political pressure by the organized urban poor have, in some contexts, prompted state responsiveness to demands for services, often resulting in various types of ‘co-production’ of ‘solutions’. Local residents’ grassroots collectives, in alliances with other city-stakeholders, have engaged and collaborated with the state to negotiate challenges such as sanitation, land tenure, housing, environmental risk and security (Mitlin, 2018).
Social mobilization and collective agency depend on a sense of shared interests and, to some extent, shared identities. There is insufficient knowledge generated ‘from below’ about the ways in which processes of recognizing and managing multiple, sometimes apparently conflicting, interests within urban social movements play out over time.
The effectiveness of accountability processes is influenced by local political dynamics, and the degree to which issues raised are amenable to local action. Local ‘actions’ may well be ineffective in addressing ‘upstream’ determinants and require ‘scaling up’ (Fox, 2016) either through federating struggles to the sub-district, state or national levels, or through networking with other civic groups for larger collective political bargaining. Intersectional analyses highlight the role of forces beyond the nation-state in shaping ‘local’ deprivations. For example, in Dhaka, Bangladesh the livelihoods of millions of women living in informal settlements and working in the garment industry were suddenly curtailed by the withdrawal of orders by global firms during the COVID-19 pandemic, with significant health and well-being impacts on women and their families (Rao et al., 2022). However, to date, there are few examples of effective strategies to demand and achieve accountability beyond state boundaries.
The pursuit of health accountability requires marginalized people to navigate complex, pluralistic systems and informal practices of governance and service provision. Existing models of accountability offer insufficient accounts of how contextually specific power relations shape meaningful participation that expands the scope for agency, and how these can be transformed in urban informal spaces.
IV. Future Conceptual and Empirical Directions
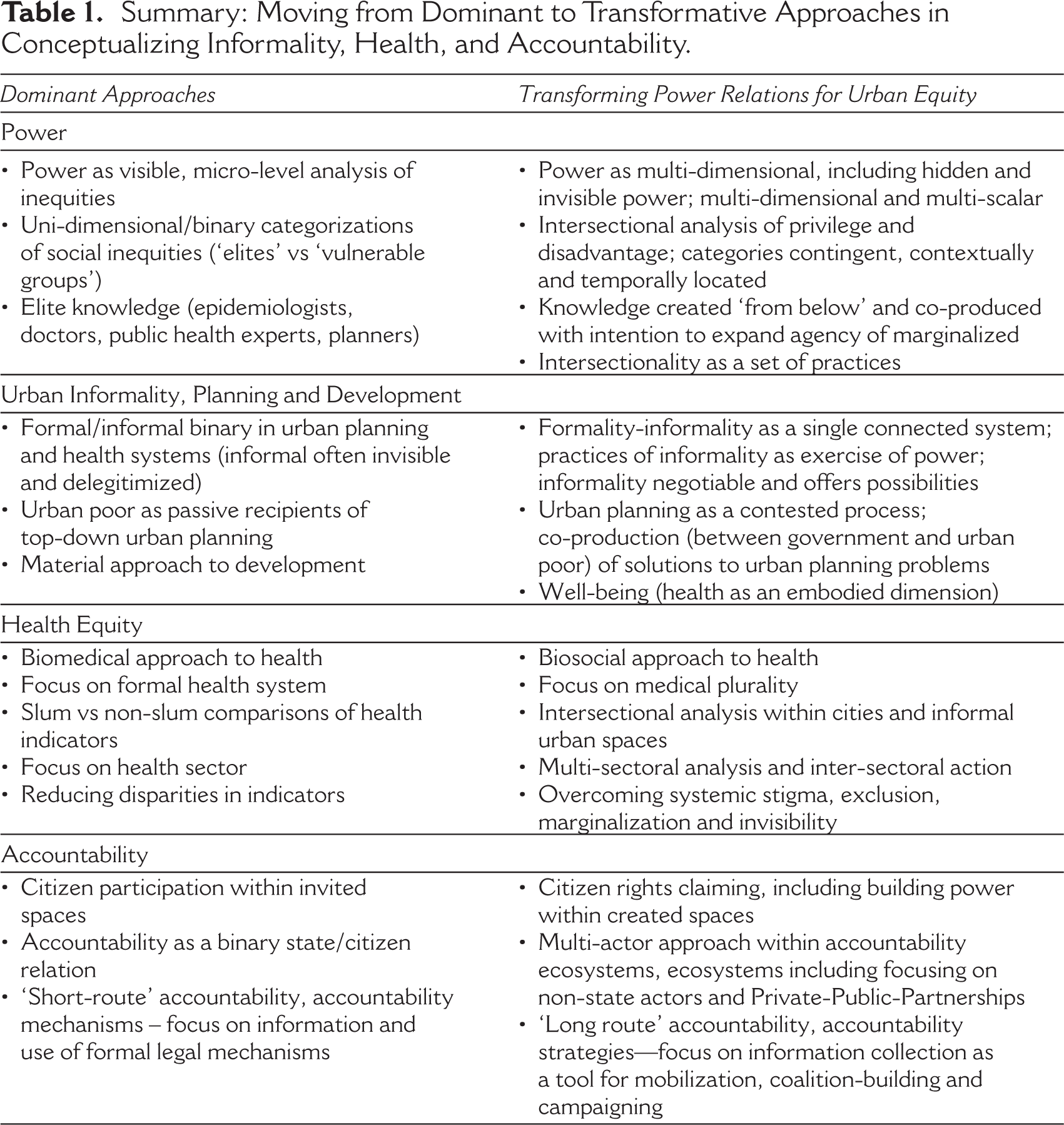
This section identifies potential conceptual and empirical directions that integrate insights from the fields of urban informality and planning, health and accountability. These directions represent the radical shift in approaches needed to achieve the SDGs in cities. Table 1 juxtaposes the dominant approaches to informality, health and accountability with these transformative directions, centred on alternative, intersectional approaches to power analysis.
In this section, we identify and discuss four main directions with regard to operationalizing a research approach that is informed by intersectional power analysis at all levels from conceptualizing health, health systems and social inequalities amongst people in informal spaces to conducting research-to-action processes. These are: (a) a bio-social framing of health as a dimension of well-being; (b) an acknowledgement of plurality and moving beyond binaries; (c) reflexive, intersectional analyses of power relations and (d) intersectionality as a set of practices aimed at transforming power relations.
A Bio-social Framing of Health as a Dimension of Well-being
Research on health in informal urban spaces requires a framing of health that moves beyond the limitations of the biomedical model to acknowledge the lived realities of health and well-being. This framing should move beyond Cartesian dualism to the recognition and exploration of the interrelationships between the physical, mental and social dimensions of health. Conceptualizing health as integral to well-being recognizes the importance of its subjective, relational and material aspects (White, 2010). The concept of ‘embodiment’ (Csordas, 1995), which foregrounds bodily perception as a starting point for individuals’ subjective experiences, offers a counterpoint to biomedical understandings and situates bodily experience within social worlds.
A growing literature on ‘syndemics’ provides empirical connections between chronic social, structural and environmental stressors, including marginalization, mental and physical health and well-being (Singer and Clair, 2003). Syndemics have been described as ‘a synergistic interaction of social, contextual, and disease-related factors that escalate the burden of suffering and disease on marginalized groups in a way that exceeds the impact of any single factor’ (Mendenhall, 2014: 3). They occur where social and structural inequalities create a material and social environment that fosters clustered vulnerabilities to more than one element of ill-health and that amplify poor health and well-being outcomes amongst vulnerable people (Singer et al., 2017). Stress and stigma are identified as ‘primary route[s] through which oppressive social conditions find expression in clinical outcomes’ (Singer and Clair, 2003: 430).
Summary: Moving from Dominant to Transformative Approaches in Conceptualizing Informality, Health, and Accountability.
This framing is particularly valuable when considering strategies for moving beyond disease control or prevention to address ‘structural violence’ (Farmer, 1996), that is for understanding how unequal global and local political, economic and social forces inflict harm on people (Bilgin, 2005; Farmer, 1996; Mendenhall et al., 2017; Singer et al., 2017; Tsai, 2018). An emphasis on the embodied nature of both health and well-being requires the exploration of marginalized and disadvantaged people’s own physical and mental experiences and their interpretations of these experiences. These perceptions may or may not align with biomedically defined diseases or syndromes and may link to multiple, hybrid and ‘syncretic’ treatment regimes (Dean et al, 2022; Hausmann Muela et al., 2002; Shaw, 2017).
Expanded concepts of health need to be conceptually and empirically linked to existing well-being frameworks. Drawing on the ‘capabilities’ approach to human development, well-being relates lived experience to power by allowing understanding of what people are able to do and why (Gough and McGregor, 2007; McGregor et al., 2007, 2009; Rojas, 2008; White, 2010). Locating health within well-being highlights the linkages across sectors that shape both and the importance of analysis and action beyond the health sector (Atkinson and Joyce, 2011; van Kamp et al., 2003).
In order to inform processes of accountability that connect the lived experiences of people in informal spaces with the structural power relations that underpin them, researchers need to work with communities both to explore their ‘emic’ constructs of health and well-being and to identify together the locally specific practices of informality, governance and social systems through which their priorities may be addressed. For example, the use of Photovoice with children heading households in Viwandani and Korogocho informal settlements in Nairobi identified the ways in which the social location of children heading households limited their access to material and institutional resources as well as creating psychological pressure and social isolation and stigma, with negative impacts on their physical, emotional and mental health and well-being (Karuga et al., 2022). Working with children heading households and Community Health Workers and Volunteers as immediate supporting actors, researchers are facilitating Quality Improvement Teams to create and strengthen linkages to County Government departments of Health and Social Welfare to improve accountability for basic needs and educational support for these children as well as strengthening health service capacities for mental health service provision (ARISE Consortium, 2022). Further methodological implications are discussed below.
Acknowledging Plurality and Moving Beyond Binaries
The literature discussed above shows how the hierarchical formal/informal binary delegitimizes marginalized urban people’s claims to resources and services that promote health and well-being, and simultaneously obscures multiple practices of informality by state actors and institutions. Alternative critical conceptualizations that destabilize the formality/informality binary have rarely been applied to health services.
A plurality of actors and institutions both within urban health service provision systems and other sectors are central to the production of health. It is critically important for researchers to identify and make visible the multiplicity of state actors, institutions and obligations and to identify allies in navigating these (Elsey et al., 2019). Distinguishing between the accountability of the state as a duty bearer for citizen health and specific strategies to identify lines of accountability within particular ecosystems may also be necessary to hold both state and non-state actors (including non- governmental and private sector institutions) accountable for provision within these arrangements. Creating opportunities for constructive dialogue using research evidence between marginalized people, local government (elected representatives and executive government departments) and private sector providers including non-governmental organizations is likely to be an important first step to identify specific strategies in pluralistic environments, with sensitivity and reflexivity around power dynamics as discussed below.
Reflexive, Intersectional Analyses of Power Relations
Reflexive, intersectional analyses are required to unpack how particular configurations of macro-meso-micro forces facilitate or impede equity and social justice in particular contexts/times. This requires connecting multi-scalar, intersecting regimes of power with individual circumstances of daily life and experiences of health and well-being. Greater attention to the dynamics of power at different levels and the processes whereby poor health and well-being outcomes are produced and perpetuated is also vital to inform action. This should acknowledge marginalized urban people’s agency while identifying the ways that such agency may be constrained by social, economic and political structures and institutions. (Evans et al., 2018). Such analyses must connect with and reflect deeply on power relations within processes of participation and accountability. The same exclusions that exacerbate health and well-being vulnerabilities are also likely to limit participation and its impact.
Castán Broto and Neves Alves identify two key intersectionality insights for understanding the dynamics of exclusion that undermine co-production between communities and government (Castán Broto and Neves Alves, 2018). First, the questioning of bounded, fixed identity categories as indicators of vulnerability, since identities are ‘negotiated alongside other social relations in a given set of circumstances’ (374). This means that we need to focus on dynamic everyday practices as a basis for identifying social categories. For example, a participatory planning process for climate change in Maputo, Mozambique collectively defined groups of people with shared vulnerabilities based on differentiation of tasks and risks in their neighbourhoods, with the resulting groups crosscutting age and gender categories: young people experiencing unemployment, old people with mobility constraints, women who stayed in the house for most of the day, local business owners (mostly women) and people in salaried employment. Participatory research with a diverse range of co-researchers in Korogocho informal settlement in Nairobi, Kenya explored how linked vulnerabilities to Intimate Partner Violence and HIV/AIDS were fluid and relational and shaped by dynamic interactions between gender, age, sexual orientation, (dis)ability and wider social connections (for example to community gatekeepers) in daily struggles for material survival and aspirations (Ringwald et al., 2023). These insights underscore the importance of moving beyond static categories of vulnerability, such as positioning all women as inherently vulnerable, in developing community and institutional responses.
Second, Castán Broto and Neves Alves (2018) point to the significance of co-production as a means to question ‘dominant ways of understanding reality’. This can begin processes that counter the ‘symbolic violence’ of the lack of recognition of people’s lives and problems (375). ‘Co-production processes are part of subjectivity-making processes’ ( 379) and may disrupt existing power relations with regard to identity formation. In Vijaywada and Guntur in Andhra Pradesh, India, researchers and musicians have worked with waste workers to develop songs that express their lived experiences of marginalization, oppression and discrimination as well as capacities, solidarity and hope Chandu (2022). These were found to be powerful ways to build critical consciousness and emotional connection as a basis for identifying priorities and accountability demands since the isolated nature of waste workers reduces their opportunities to make claims on the state. Simultaneously, attention was paid to the ways in which power structures such as patriarchy create inequalities within the community, including child marriage. Recognizing the diversity of actors, and the inclusion of the realities of people which are not reflected in well-established social categories, has the potential to ‘create instability in the dominant structures of power’ (373). In the study of intimate partner violence and HIV/AIDS in Korogocho (Ringwald et al., 2023) regular reflexivity discussions enabled co-researchers to situate their advocacy efforts both within and beyond the community in relation to their insights into their own unique positionalities of co-existing power and vulnerabilities.
Ultimately researchers should pursue intersectionality analyses that emerge from participants’ lived experiences and emphasize existing negotiations around identity relationships, rather than promoting, and thereby reinforcing, predetermined identity categories. Marginalized people need to make their own decisions within research-to-action processes about how and when to tackle oppression as they have a deeper understanding of potential risks and outcomes.
Intersectionality as a Set of Practices Aimed at Transforming Power Relations
These analytical insights suggest the importance of researchers engaging in questions of accountability for health equity with marginalized urban people adopting intersectionality as a set of practices (Choo and Ferree, 2010). Attention to the interrelated processes of knowledge production, recognition and material inequities implies the necessity for a reflexive and transformational approach to power within research processes. First, research needs to be values-based. For example, the ARISE consortium has committed to taking an a priori social justice and rights framing of health for action and approaching accountability from a ‘democratic imperative perspective’, aligning with those who have argued for the importance of understanding accountability as inseparable from the realization of rights (Newell, 2006).
As discussed above, the urban poor have developed organizations to represent their interests which have often grown into social movements to resist and transform their position and condition. These depend on building social bonds and cohesiveness alongside developing social and political consciousness and capacities to inform collective action, including negotiation for the fulfilment of rights from state actors. This is a process of empowerment, which we may define simply as ‘as a process of transforming the power relationships among individuals and social groups’ (Batliwala, 2007). Such empowerment processes require individuals to perceive and organize around common interests. The process of doing so may re-produce or contest existing power relations and also develop new forms of power.
Questioning the ideologies that justify inequality across all social identities includes recognizing the dynamic relationship between oppression and privilege within individual circumstances and daily practices. For example, social organizations based on caste interests need to pay attention to women’s, men’s and people of other genders’ different experiences of caste oppression. Transforming gender power relations need not be seen as a zero-sum game, since ‘hegemonic masculinities’ also limit the ‘well-being freedom’ of subordinated men and can also oppress them (Connell and Messerschmidt, 2005). Practices of intersectionality should therefore aim at strengthening our understanding of existing fault lines and how we can work to repair them. Researcher-supported dialogue and exchanges for mutual learning between groups working towards accountability in different contexts or from different social positionalities have shown promise as a process for highlighting and beginning to shift intersectional power relations. For example, exchanges between groups of waste workers and residence-based urban social movements from different cities in India led to insights such as the importance of inclusive participation and leadership across gender and religious divides (ARISE Consortium, 2023).
Building on Paulo Freire’s work on empowerment through critical consciousness-raising and collective action, Kabeer argues that marginalized groups can build new identities through their strategies for recognition, claims for inclusion and the very processes of group formation (Kabeer, 2005). Transversal politics is an approach that may offer a way forward. It is based on first, standpoint epistemology, which holds that ‘the only way to approach “the truth” is by a dialogue between people of differential positionings’ (Yuval-Davis, 1999: 95); second, on the recognition that differences are important, but that notions of difference should encompass, rather than replace notions of equality (Yuval-Davis, 1999) and third, on a differentiation between positioning, identity and values. Similar or compatible values can cut across differences in positionings and identity to form ‘epistemological communities’, which share common value systems and can exist across difference (Yuval-Davis, 1999). Diverse societal groups who share social justice values may identify points of convergence in their political struggle interests and form strategic coalitions at specific points in time without subsuming their various struggles into one. Participatory research processes that operationalize intersectionality practices may provide an important space both for making power relations visible and for identifying strategic epistemological communities across power divides.
V. Conclusion
There are critical conceptual deficiencies and empirical gaps in the dominant ways of conceptualizing the challenge of inequities in health and well-being in informal urban spaces. Radically different approaches are required to research that aim to transform multiple power relations, including between marginalized urban citizens and states, and beyond to supra-state forces such as multinational corporations, and among people living and working in informal urban spaces themselves. To contribute towards these new approaches, as researchers, practitioners and activists working in informal urban spaces we need to think beyond binaries, including those of social inequities (such as gender), physical and mental health, material and subjective well-being, formal and informal governance and providers, professionals and non-professionals in order to shift paradigms in policy, practice and action and so open new pathways to health and well-being for informal urban residents. Reflexive intersectional analyses and practices are a critical first step in taking forward to these transformational approaches. Such paradigmatic shifts are required to tackle the interconnected and mutually reinforcing ways that current configurations of power from macro to micro levels shape opportunities for marginalized urban people to equitably participate in the planning and management of cities to ensure that they are ‘inclusive, safe, resilient and sustainable’, promote health and well-being, and reduce avoidable suffering and death (SDG 3).
Footnotes
Acknowledgements
We acknowledge the support received from the UK Research and Innovation (UKRI). The GCRF Accountability for Informal Urban Equity Hub (“ARISE”) is a UKRI Collective Fund award with award reference ES/S00811X/1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the UK Research and Innovation (UKRI). The GCRF Accountability for Informal Urban Equity Hub (“ARISE”) is a UKRI Collective Fund award with award reference ES/S00811X/1.