
Abstract
Significant variations in infection, testing, and mortality rates have exposed key differences in the initial COVID-19 response by Indian states. At the onset of the pandemic, states like Gujarat, known for its large economic output, suffered high COVID-19 case fatality rates, a disorganized response, and poor access to healthcare. In contrast, Kerala, a less industrialized state on India’s southwestern coast, experienced low infection rates and fatalities. The low case fatality rate was accompanied by widespread access to care, extensive testing, and an organized response by the state. The emergence of the COVID-19 pandemic provides an opportunity to compare how the Gujarat and Kerala models performed. Since 2000, the Gujarat model has emphasized industrialization and economic development, often at the expense of social development. In contrast, the Kerala model emphasizes social development, often at the expense of economic development. This article analyses the initial response to COVID-19 by Kerala and Gujarat and finds that the Kerala model and its emphasis on social development helped the state respond more effectively to the first wave of the pandemic compared to Gujarat.
Introduction
On 30 January 2020, India reported its first case of COVID-19 in Kerala, a state of 35 million people on the southwestern coast. Patient zero was a student returning home from Wuhan University (Perappadan, 2020). Despite being asymptomatic, the student was advised to self-quarantine in her home for 28 days and given a contact number in case she developed a fever, cough, or other flu-like symptoms (Ghosh and Philip, 2020). Two days later, the student contacted the District Surveillance Officer after developing flu-like symptoms, and the district team went to her home and moved her to an isolation unit at the Thrissur General Hospital. The same day, the student was administered a COVID-19 test and her sample sent to the National Institute of Virology (NIV) in Pune, Maharashtra (Vaman et al., 2020). A few days later, the NIV confirmed that the student had the novel coronavirus. Individuals who were in contact with patient zero were told to quarantine in their homes and the Kerala Health Department began tracking and identifying persons who may have come into contact with patient zero (Desai, 2020). The period of time from patient zero’s arrival in Kerala to her isolation in a hospital was an impressive 3 days with an additional 3 days to receive a diagnosis.
In contrast, Gujarat, a state with a population of approximately 63 million in western India, performed poorly in its initial response to the COVID-19 pandemic. Gujarat’s first COVID-19 cases were two residents also returning home from abroad. The state government attempted to contact those who came into contact with the two patients but faced difficulty due to the lack of cooperation from citizens and inadequate resources (Dabhi and Brahmbhatt, 2020). Within 3 days of its first case, Gujarat announced its first COVID-19 related death of a previously undiagnosed patient. In fact, despite its nearly two-month head start to prepare for the arrival of the virus in the state, Gujarat had only tested a total of 150 samples by mid-March 2020 (Ghosh, 2020b). Gujarat’s low rate of testing meant that the coronavirus had been spreading throughout communities without being observed. Although Gujarat eventually implemented some restrictions such as partial lockdowns of major cities, it was not until India’s national lockdown on 24 March 2020 that strict measures were put in place. The countrywide lockdown resulted in the closure of all public transportation in Gujarat, meaning that traveling to a clinic for testing or care became even more difficult, especially for those living in rural communities with limited clinics. Additionally, not until the national lockdown did Gujarat begin a concerted effort to procure ventilators, train healthcare workers, and reserve hospitals for COVID-19 treatment. By 7 April, Gujarat had a case fatality rate of 7.88%, the highest of any state in India at that stage in the pandemic (Kumar, 2020).
Kerala’s initial success at containing the virus and flattening the curve has been attributed to its unique model of development, the ‘Kerala model’, which focuses on human development (Chakraborty, 2005; Devika, 2010; Parayil, 1996; Véron, 2001). Specifically, the Kerala model is characterized by large government investment in health and education and a high rate of social mobilization led by strong labour organizations and popular movements resulting in improved living conditions for the poor (Heller et al., 2007; Parwez, 2016: 106). Even more striking is the fact that Kerala has been able to achieve impressive developmental milestones in the areas of maternal health and primary school education, despite being a relatively poor state, often ranking in the bottom half of economically developed states in India (Ministry of Statistics and Programme Implementation, 2019).
In contrast, Gujarat’s initial poor response to the COVID-19 pandemic, including low and restricted testing, limited medical facilities, inadequate contact tracing, and high cost of care, reflected its economically focused developmental model, called the ‘Gujarat model’. Unlike the Kerala model, the Gujarat model prioritizes economic, rather than social, development and the privatization of education and healthcare. Gujarat is one of India’s wealthiest states, contributing around 8% of India’s total domestic output (Rai, 2020). Since 2000, Gujarat’s Gross/Net State Domestic Product (GSDP) growth has averaged 10% (Rai, 2020). In Gujarat’s health sector, religious minorities, scheduled castes, and the indigenous Adivasis remain especially vulnerable to any unexpected healthcare expenses. In short, Gujarat’s model of development did not translate into a robust healthcare system capable of containing, monitoring or reducing the adverse effects of the emergence of COVID-19 in the state.
The two states’ differing approaches to the COVID-19 pandemic highlight the importance of proactive government policies, high public trust in government, and effective health infrastructure in producing positive health outcomes such as low mortality and infection rates. Kerala’s timely and effective initial response to the pandemic underscores that level of economic development is not a reliable indicator that a country or state will have better healthcare outcomes in comparison to less developed countries or states.
In this article we compare the initial COVID-19 responses of Kerala and Gujarat. Specifically, we compare and contrast the Kerala and Gujarat development models and assess how each model guided its respective states’ initial COVID-19 response. We define each state’s initial response as the period starting on 11 March 2020, when the World Health Organization (WHO) declared the novel coronavirus a global pandemic, to 19 June 2020, 100 days after the WHO’s declaration (Ghebreyesus, 2020). We chose to cover these 100 days because it covers the critical phase from global awareness of the danger posed by the virus to the period where Kerala and Gujarat had begun testing, contact tracing, and quarantining COVID-19 cases in an effort to stem the spread of the virus. More formally, our research question is, how did the contrasting development models in Kerala and Gujarat shape their initial responses to the COVID-19 pandemic?
We make several contributions to the development literature and discuss how various features of the Kerala and Gujarat models respectively, led to different responses in dealing with the COVID-19 pandemic. First, Kerala’s proactive and interventionist state policies in combination with previous experience with the deadly Nipah Virus Outbreak in May 2018, meant that state officials were able to quickly mobilize healthcare workers, create quarantine and testing protocols, and enforce strict lockdown measures to help stem the initial wave of COVID-19 infections. Second, Kerala’s history of broad-based coalitional social movements meant that members of different communities had a history of working together to attain common goals, which was important in enforcing public health directives. Third, Kerala’s strong civil society meant that the government was able to gain the cooperation of other powerful societal actors in communicating important information to the public concerning the virus. Finally, the Kerala model’s focus on inclusive social development and economic growth meant that vulnerable populations were not left out of the government response to COVID-19.
The findings from Gujarat and Kerala have impacts beyond Kerala, Gujarat, and India. Because the COVID-19 pandemic impacted Kerala and Gujarat at the same time, it provided an opportunity to compare the effectiveness of the two development models in states with broadly similar historical and cultural contexts. The models selected by each state represent contrasting, yet popular, development models that have been utilized throughout the world. Kerala reflects a model with heavy state involvement in the public sector. This interventionist model has been used throughout the world from Scandinavia to Cuba. Likewise, Gujarat reflects the popular neoliberal model that relies upon economic development and private sector investment to promote social development. Similar models have been used historically throughout Latin America (Panizza, 2013) and Southeast Asia (Springer, 2009) with varying levels of success and backlash (Silva, 2009).
The remainder of the article proceeds as follows, Section II compares the Kerala and Gujarat Development Models. Section III examines the healthcare model in each state while section IV examines Kerala and Gujarat’s COVID-19 response in the first 100 days. Section V concludes with an overview of the contributions of the article and insights into the broader debates within the literature.
Comparing Kerala and Gujarat’s Development Models
Kerala
The Kerala model reflects the state’s social democratic system of government, which features proactive government intervention in the economy to ensure the equitable distribution and provisions of services such as primary healthcare, broad-based coalitional social movements, strong civil society and inclusive social policies (Chathukulam and Tharamangalam, 2021: 9–10). Scholars of the Kerala model have called the participatory democracy ‘vibrant’ and ‘high energy’ (Heller, 1996; 2000). Kerala’s social pact to provide basic welfare to all its citizens arose partly in response to a strong popular mobilization movement such as the temple entry movement of the 1930s, workers movements in the 1950s and 1960s, literacy movements in the 1980s, and gender, caste, people’s movements from the 1990s onward (Heller, 2020)
The Kerala model is an example of a human development (HD) approach where a society’s development is measured using human well-being rather than GDP per capita or other economic indicators (Sen, 1999; Tharamangalam, 2010: 365; ul Haq, 1995). Based on ideas from scholars such as Mahbub ul Haq and Amartya Sen, the premise underlying the HD approach is that wealth alone does not result in human well-being or an equitable society (Sen, 1999; Tharamangalam, 2010: 365; ul Haq, 1995). The HD approach’s more comprehensive approach to development considers ‘human, ethical, social, and even political dimensions’ of public policy, thereby making this approach more effective at handling large societal problems, such as how to contain a pandemic.
A cornerstone of the Kerala model is the ‘extensive intervention by a well-developed and well-organized state and bureaucratic apparatus’ that acts in response to mobilized pressure from below (Tharamangalam, 1998: 29). Kerala’s interventionist state model has resulted in the effective and extensive administration of education, health and welfare programs. In fact, state intervention in Kerala since the mid-1970s significantly reduced poverty (Tharamangalam, 1998). One example of a successful interventionist program is Kudumbashree, the State Poverty Eradication Programme of the Government of Kerala, which had the dual purpose of finding solutions to deprivation faced by less-educated, poor women from disadvantaged households and community development issues (Chathukulam and Thottunkal, 2010).
The Government of India’s ‘mindless privatization unleashed by neoliberal reforms’ of the past three decades has been cited as one of the factors driving Kerala’s proactive and interventionist policy making (Chathukulam and Tharamangalom, 2021: 9). However, some privatization in combination with a countrywide push for decentralization from state government to local government level in the mid-1990s benefited Kerala’s healthcare system by making it more efficient and accessible. In fact, despite local government becoming more involved in the policy making process, the proactive nature of policy making in the state ensures that Kerala maintains a level of social development that is ‘not only decades ahead of India, but on par with the middle-developed countries’, for example, Brazil or Argentina (Chathukulam and Tharamangalom, 2021: 9)
Well-organized, broad-based social movements are another feature of the Kerala model that has helped in its success. Social movements in Kerala predate the creation of the Indian state in 1947 and go back to the nineteenth century, when southern Kerala consisted of the princely states of Travancore and Cochin, both of which had a long history of social reform movements and anti-caste associations (Tharamangalam, 2010). These reform-oriented organizations would later become trade unions and socialist movements, resulting in a mobilized ‘socially and politically conscious population’ and the establishment of strong political parties (Chathukulam and Tharamangalam, 2021: 9). Social movements played a major role in the creation of the Communist Party that developed a ‘universalistic and class ideology that remained purposive and programmatic and retained its mass base across caste and religion…in one of the most pluralist societies in the world’ (Chathukulam and Tharamangalam, 2021: 9). The Communist Party would come to resemble the social democratic parties of Western Europe and has shifted state politics to the left, meaning right-leaning parties and conservative elements have had to accept some basic social programs favoured by the Communist Party and their supporters (Chathukulam and Tharamangalam, 2021). However, the flip side of Kerala’s strong social and labour movements has been the perception that these groups exercise a hegemonic role over the political agenda whether or not the political party in power is dependent on their support (Kannan, 1998). Kannan argues that much of the Kerala’s time and resources are spent mediating conflicts between capital and labour, resulting in a government that is best described as a ‘soft’ institution. In other words, these strong labour movements have created a political system where the government is not always viewed as the primary driver of change (Kannan, 1998).
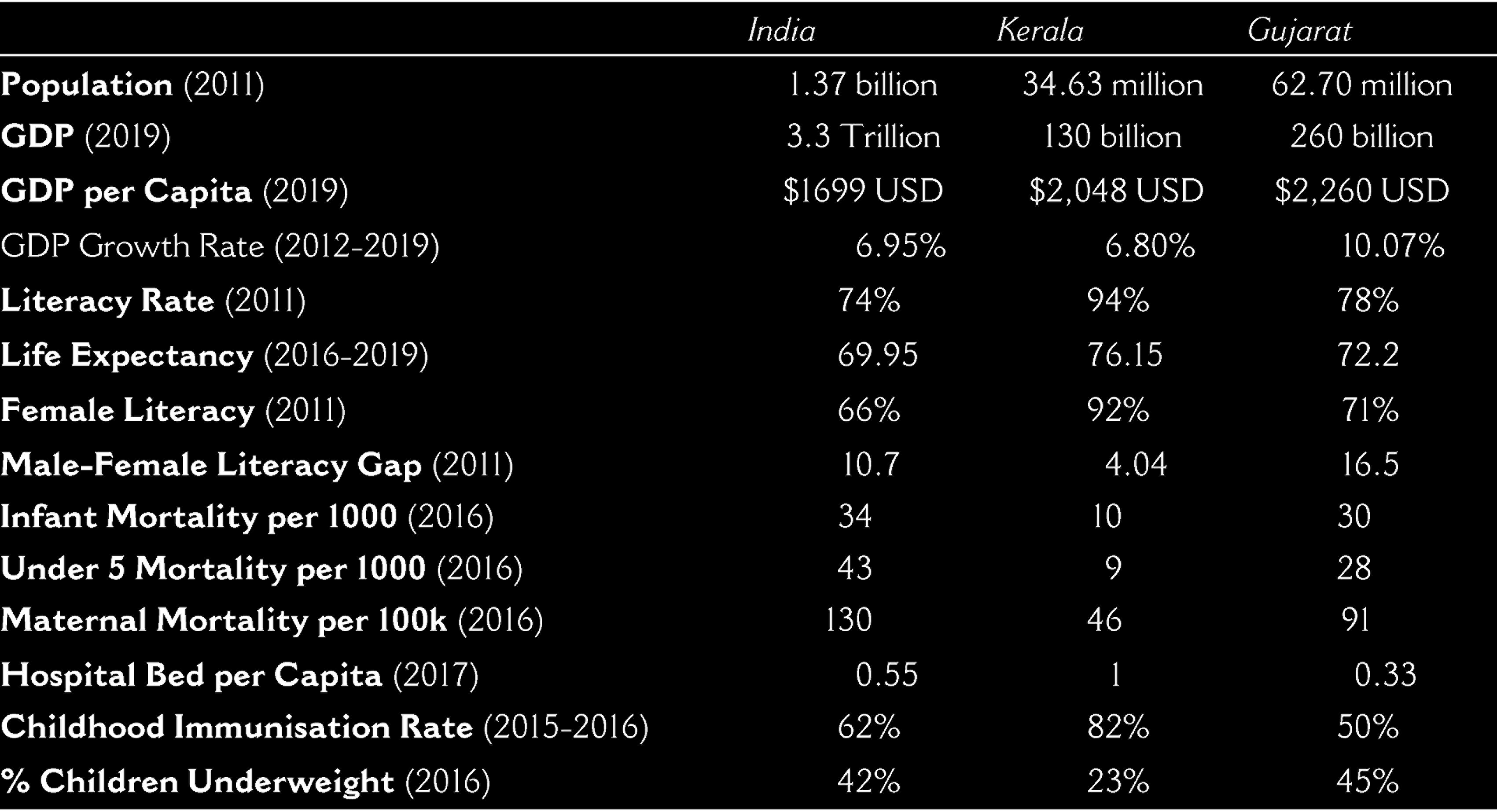
Another key feature of the Kerala model is its inclusivity of traditionally overlooked social groups such as women, Dalits, Non-Scheduled Castes and Tribes, and religious minorities in the development of its social programs. The model’s deliberate inclusion of women in its development goals has yielded impressive results for example, Kerala has a female literacy rate of 92.9% in rural areas and 94.9% in urban areas and the average age for marriage for females is basically the same for women living in rural and urban areas (Parwez, 2016: 116). Most tellingly of the model’s inclusivity is the absence of large disparities between rural and urban populations in the areas of child immunizations, infant mortality rates, life expectancy, and maternal mortality rates. As table one demonstrates, when comparing Kerala’s social development indicators to Gujarat and India, Kerala performs substantially better on all social indicators. The Kerala model has helped uplift society across multiple indicators even though Kerala’s economic indicators fall short compared to economically advanced states like Gujarat.
Gujarat
The Gujarat model is anchored in neoliberal economic policies that focus on ‘private sector driven growth, high economic growth rates, business-friendly policies, foreign investment, urbanization and industrial development’ (Chacko, 2018: 554). Critics call the development style characteristically corporatist, authoritarian, and statist (Chacko, 2018), while others contend that the model centralizes power into the hands of the Chief Minister while further marginalizing minorities and implementing restrictions on universities, the press, and political rivals (Guha, 2020). In other words, the Gujarat model features: reactive state policymaking that does little to ensure socio-economic equity; highly stratified social movements based on caste or religion; a weak civil society with little influence on the creation of public policy; and exclusionary development policies that overlook vulnerable populations.
In 2014, the Bhartiya Janata Party (BJP) platform emphasized the rapid economic and industrial growth of ‘Glowing Gujarat’ under the leadership of Narendra Modi, the Chief Minister of Gujarat from 2001 to 2014. According to the BJP, Gujarat’s growth was ‘miraculous’ and could be applied to the rest of the country to help make India an economic superpower. The BJP later won the 2014 and 2019 general elections and Modi became the Prime Minister. Modi’s philosophical approach is one of limited government intervention. Throughout his tenure he has frequently repeated his catchphrase ‘government has no business being in business’ (Aiyar, 2021). During Modi’s time as Gujarat’s Chief Minister, the state government transferred several key industries, including roads, schools, manufacturing, ports, power, and healthcare to private companies (Chacko, 2018).
The privatization of key sectors in Gujarat can be demonstrated in several cases. In the energy sector, from March 2004 to January 2013, the share of private sector management went from 25% to 60% (Singh, 2014). In Dahod, a key state-run hospital was transferred to Zydus Cadilla, a pharmaceutical company (Narayanan, 2019). In Ahmedabad, a new private hospital was opened at the sacrifice of the Vadilal Sarabhai General Hospital and Chinai Maternity Home, an 88-year-old public charitable hospital, which primarily served the poor (Narayanan, 2019). This occurred alongside a change in the nature of Gujarat’s healthcare industry. For example, in 1996 23% of the population utilized government run healthcare facilities. By 2014, the percentage of the population receiving care in government run facilities dropped to 15%, among the lowest in the country (National Statistical Office, 2019). Outside of Gujarat the percentage of the population utilizing public healthcare facilities was rising (National Statistical Office, 2019). But in Gujarat, the population relied upon private healthcare. The majority of pregnant women in Gujarat, 72%, gave birth in a private facility compared to India’s national average of 48%. Finally, in the education sector, nearly all of Gujarat’s expansion occurred in the private and for-profit sector. For example, Gujarat’s engineering colleges grew four-fold during the Modi era, but 76% of the new institutions were private while only 15% were run by the state (Hirway et al., 2014).
Sood (2013) claims that the emphasis on investors meant that private equity heavily influenced state spending priorities. In other words, Gujarat’s government was rarely the instigator of important public policy decisions, leaving many decisions concerning important social development issues, including healthcare, in the hands of private capital. Under the Gujarat model, the state experienced impressive economic growth in nearly every sector (Kotwal and Chaudhari, 2014). Despite the emphasis on Gujarat’s economic success, there were many shortcomings. For instance, improvements in infrastructure failed to provide much improvement in poverty rates, with most projects focused on providing access to special economic zones and shipping ports (Guha, 2020).
Although many middle and upper-class people experienced an improved quality of life under the Gujarat reforms, the most vulnerable groups became further marginalized (see Joshi and McGrath, 2015; Jaffrelot, 2015). For example, while much of India made dramatic improvements with maternal mortality, Gujarat rates remained much higher than their neighbours. In fact, Gujarat’s maternal mortality rates worsened between 2013–2017, increasing to 85 deaths per 100,000 in 2016 from 72 per 100,000 in 2013 (Press Trust of India, 2017). Caste, socio-economic status, and education level were also significantly associated with unequal access to maternal care and health outcomes (Saxena et al., 2013). These statistics are not surprising considering that growth without social justice is central to the Gujarat experience.
While social movements played a central role in pushing for Kerala’s development, this was not the case for Gujarat. Social movements do have a strong historical presence in Gujarat, with the most popular being the anti-colonial agitations led by Gandhi. However, since independence, social movements in Gujarat have been mostly exclusionary and dominated by the landowning Hindu elite (Shah, 2004). Since the 1990s, social movements in Gujarat have taken an increasingly nationalist and exclusionary tone. Hindu nationalist movements like the Rashtriya Swayamsevak Sangh (RSS), have been the most impactful organizations. The RSS, founded in 1925, seeks to maintain and advance Hindu culture and identity in India. Gujarat has been the epicentre of the movement and the organization has had a strong influence on the Bhartiya Janata Party (BJP). Between 2012 and 2019, the number of RSS chapters (shakhas) in Gujarat increased from 1039 to 3500 (Saini, 2019). The RSS has been criticized for its anti-Muslim rhetoric and communalism, but RSS members maintain that they are not anti-Muslim, only pro-Hindu (Jaffrelot, 2009). The type of labour and lower caste movements that were successful in states like Kerala failed to launch in Gujarat. Instead, upper caste Hindus launched movements rallying against the adoption of bureaucratic reservations and economic mobilization schemes for low caste and scheduled tribes (Desai, 1981; Shah, 2004). Leftist movements that pushed for land reforms and workers’ rights in other states never gained traction in Gujarat.
Gujarat’s exclusionary policies and movements have put low and non-scheduled castes, Dalits, scheduled tribes, religious minorities, and women at a disadvantage. The failure to focus on women’s health has led to Gujarat having among the worst infant, child, and maternal mortality rates in the country. For instance, as table one indicated, Gujarat’s infant and under 5 mortality rates in 2016 were more than three times that of Kerala and the percentage of the female population that were underweight and/or had anaemia was one of the highest in the country (National Family Health Survey, 2019). Likewise, maternal mortality of women in Gujarat was nearly double that of Kerala as of 2016 (National Family Health Survey, 2019). Women continue to experience high levels of discrimination in access to education, further limiting their options and chances for social and economic advancements.
While states like Kerala emphasize social development often at the cost of economic development, Gujarat did the opposite. In fact, social progress stalled or worsened according to many indicators, making only marginal improvements since the turn of the century and during the first half of Modi’s tenure, respectively. Gujarat allocated less money to its social services budget than all but two states (Sood, 2013). Education also received decreasing attention, with Gujarat utilizing 14.3% of its budget on education in 2019–2020 with only four other states spending less on education (PRS Legislative Research, 2020)
Widespread caste-based discrimination remains a problem throughout all of India, but especially so in Gujarat. In Gujarat, Dalits face difficulty accessing social facilities, particularly healthcare facilities (Acharya, 2010). A study examining the delivery of health care services to Dalit children in Gujarat found that 91% had experienced caste-based discrimination in access to medicine (Acharya, 2010). Another study examining distribution of polio vaccines in Gujarat found that millions of Dalit children have not received their vaccine, given orally, due to beliefs about their untouchability. Despite aggressive polio eradication campaigns throughout India, 16% of Dalit children in urban areas of Gujarat, and 20% in rural Gujarat, have not received their polio vaccination, with Dalit girls at the highest risk of non-vaccination (East-West Management Institute and Navsarjan Trust, 2013). The government has not made an active effort to increase Dalit vaccination rates. In fact, the overall proportion of children in Gujarat with no vaccinations has increased from 5% in 2005 to 9% in 2016 (Goli et al., 2020).
To summarize the argument so far, the juxtaposition of these two development models highlights the advantages that the Kerala model had over the Gujarat model heading into the COVID-19 pandemic. Kerala’s proactive state policies meant that the government had a system in place to deal with health crises, policies that were improved upon after experiencing the Nipah Virus Outbreak in May 2018 (Sadanandan, 2020: 2). Equally important to controlling the spread of the virus has been public trust in government directives and information concerning the virus, which has been nurtured through decades of government responsiveness to broad based social movements and strong civil society that have made the public partners in managing difficult societal issues (Sadanandan, 2020: 2). Finally, Kerala’s inclusive social policies meant that there was the necessary infrastructure in terms of rural health clinics in place to reach vulnerable populations that would be hardest hit by the novel coronavirus.
On the other hand, Gujarat’s caste and religion-based movements and exclusionary policies meant there was a lack of cross-cutting mobilization throughout the state providing a concerted effort against COVID-19. Consequently, coordination across social groups and a general distrust toward each other, minorities, and the government, made a coordinated response to the pandemic even more difficult. Furthermore, Gujarat’s underfunding and lack of investment in social programs like healthcare, meant that the state did not have the infrastructure in place to deal with outbreaks in rural areas or in overpopulated urban areas where the poor and the most vulnerable populations live (Table 1).
Social and Economic Development Indicators
Social and Economic Development Indicators
Kerala
Kerala’s human development approach has resulted in a healthcare system that is among the best in India, setting the stage for a successful initial response to the COVID-19 pandemic. Scholars have put forward several explanations for Kerala’s achievements in the health sector, including expanded access to medical centres with a focus on women’s health and investments in girl’s education (Kumar, 1993; Levesque, 2006). Underscoring these explanations is the state government’s consistent commitment to investing in health and education regardless of the ideological leanings of the party in power (Kutty, 2000: 103). Kerala’s per capita government expenditure on health was among the highest of any state in India (Garg, 1998; Levesque, 2006: 18).
A fiscal crisis from the mid-1970s to the early 1990s caused the state government to reduce its spending on health and other social sectors (Madore et al., 2018: 5). Reluctant to cut salaries or lay off healthcare workers, Kerala’s health department ‘lowered costs by reducing spending on drugs and other medical supplies and froze infrastructure growth and hiring’ (Kutty, 2000; Madore et al., 2018: 5). Although Kerala’s public health system remained superior to the public health systems in many other states, the ‘quality and capacity of government primary and secondary health care facilities began to decline as a result’ (Madore et al., 2018: 5). Then, from 1986 to 1996, the growth of the private health care system surpassed growth in the public sector healthcare system by a large margin (Madore et al., 2018: 5). This rapid growth in the private health sector resulted in a vast network of medical facilities, with Kerala having one health facility per 2.6 sq. km (Government of India Planning Commission, 2009; Madore et al., 2018: 5). In short, the deficiencies of the public healthcare system caused by the fiscal crisis paved the way for the privatization of healthcare in Kerala (Basu et al., 2012).
In the past few years however, Kerala has sought to reinvigorate its public health sector. In 2016, a new chief minister was elected and with the help of his health minister, the health department was able to launch Mission Aardram in 2017. The purpose of this new initiative was to ‘strengthen quality and expand capacity in government health facilities to increase utilization and, in doing so, lower out-of-pocket spending by forcing the private sector to lower its prices to remain competitive’ (Madore et al., 2018:11). Additionally, the Kerala health department piloted an electronic health record system that would enable patient tracking and follow-up and regular screening for non-communicable diseases for adults aged 30 and older (Madore et al., 2018: 11). Beyond Mission Aardram, Kerala began creating emergency departments and trauma units in public facilities, ‘spurred in part by the high incidence of accidents/injuries and related public protests in mid-2017 after a widely publicized death due to insufficient hospital equipment and poor treatment’ (Madore et al., 2018: 12).
Kerala’s efficient and rapid initial response to the arrival of COVID-19, however, would not have been possible by relying on its healthcare system alone (Sadanandan, 2020: 2). Instead, it is the state’s successful integration of local government into its healthcare system that has proved central to Kerala’s initial success response (Sadanandan, 2020: 2). Research has found that decentralized health care systems, like Kerala’s, empower communities in the health decision-making process, thereby making basic health care more responsive to local needs (Dutta and Fischer, 2021: 2; Muñoz et al., 2017). Local officials are often seen as more legitimate and trustworthy than other external actors for carrying out different regulatory functions, such as enforcing quarantine restrictions (Dutta and Fischer, 2021: 2). The implicit trust that citizens place in their local officials are an important factor in effective communication management in times of disaster (Longstaff and Yang, 2008). In Kerala, all primary health centres and many secondary hospitals are managed by the three-tiered Panchayat system, the lowest form of rural local administrative government in India (Dutta and Fischer, 2021; Sadanandan, 2020: 2). Another institution in Kerala that enjoys a high level of trust in local communities is the Kudumbashree program, a woman-focused anti-poverty programme that has given women a strong and institutionalized presence in local government in the state (Dutta and Fischer, 2021: 5). Together, these two local institutions play a key role in the state’s healthcare system with the panchayats implementing directives issued by national, state and district officials and the Kudumbashree providing a support network mobilizing volunteers for disaster relief and providing information on which households are in need of help (Dutta and Fischer, 2021: 5).
These improvements in Kerala’s public healthcare system in the last few years have yielded impressive results. For example, in a 2018 national index of health development that was released after the start of Mission Aardram, Kerala’s overall health performance was 11 points higher than Punjab, the next closest state and more than 40 points higher than the lowest performing state, Uttar Pradesh (Madore et al., 2018: 12; NITI Aayog, 2019). And although Keralites still express a preference for private healthcare, one study found that among the two-thirds of people who opted for private healthcare, the most common reasons given for this choice was access to specialty services and less crowded facilities (Ghosh, 2014). Only 2% of respondents cited better quality as a reason for choosing private over public healthcare, an indicator that overall trust in the public healthcare system in Kerala remains high (Ghosh, 2014).
Gujarat
Nobel winning economist Amartya Sen has long warned of the potential consequences of the Gujarat model on public health (Sen, 2015). Specifically, Sen was concerned that India’s broader embrace of the corporatist Gujarat model would make the country become a global economic power with an uneducated and unhealthy population (Sen, 2015). Gujarat lags behind other states in terms of immunization rates and healthcare expenditure. Immunization rates are among the lowest in the country, with only 50% of the population being fully vaccinated. Under Modi’s economic reforms, Gujarat’s per capita healthcare expenditure declined to 11th place after being fourth prior to reforms (Kumar, 2020). Likewise, the Modi economic reforms reduced healthcare spending from 4.4% of GDP to .77% (Kumar, 2020). While other states throughout India focused on expanding access to healthcare in the 21st century, Gujarat instead focused on increased privatization. By 2020, Gujarat had only .33 hospital beds per 1,000, compared to the national rate of .55 (Singh et al., 2020). The high costs and limited access prevented many from seeking care unless the situation was dire.
In addition to decreased public expenditure on healthcare, the Gujarat model resulted in increased reliance on private healthcare. Scholars have dubbed Gujarat’s healthcare approach a ‘corporate model’ because it provides a ‘lucrative’ business opportunity (Thiagarajan, 2020). The private corporate healthcare model resulted in Gujarat having among the highest medical costs in the country with an average cost of $57 per visit compared to $22 in other states (Kalaiyarasan, 2014). Gujarat also ranks last in terms of individual out of pocket costs on medicine (NHSRC, 2014). Not only were many government hospitals transferred to the private sector, but the overall number of health centres remained among the lowest in the country, with poor states like Bihar having nearly twice as many facilities per capita. By the end of Modi’s term, state spending on the social sector was ranked 17th out of the 18th largest states (Kumar, 2020).
These poor healthcare indicators are surprising considering Gujarat’s experience with public health crises. In 1994, Gujarat received international attention when the commercial city of Surat was the epicentre of an outbreak of the pneumonic plague that resulted in over 1,000 cases and 56 deaths (Leo, 2020). Although the state was able to quickly address many of the underlying sanitary issues that led to the outbreak, the response was indicative of the state’s historical reactive response to public health emergencies. Disease outbreaks in Gujarat during Modi’s tenure as Chief Minister were also poor, with Gujarat having double the national average for four diseases including viral hepatitis, cholera, dengue and chikungunya (Iyer et al., 2017). During the H1N1 outbreak of 2009–2010, Gujarat also had a higher case fatality rate than the rest of the world (Rana et al., 2012)., Despite Gujarat’s extensive experience responding to disease outbreaks, state officials were still underprepared for the COVID-19 pandemic.
Comparing Kerala and Gujarat’s First 100 days
Kerala
Even before the first COVID-19 case arrived in Kerala in January, Kerala’s state government and healthcare system were prepared. Kerala’s Health and Family Welfare Department issued an addendum for the novel coronavirus on 5 January 2020 providing additional guidance to an earlier directive from 1 February 2010, on how to handle testing, quarantine, hospital admission and discharge for COVID-19 patients (Directorate of Health Services, 2020). On 26 January, the state government released a longer, more detailed set of guidelines for dealing with the coronavirus, before there were any confirmed cases of the virus in the state. Then in February, when additional cases came from abroad, Kerala implemented mandatory quarantines for visitors arriving from overseas or from other states, weeks before similar measures were taken in the rest of the country (The Hindu, 2020).
Kerala’s proactive response is partly attributable to the fact that the state has a particularly high risk for the widespread outbreak of a contagious respiratory virus (Menon et al., 2020). First, Kerala is a small state with a population density of 859 people per square kilometre, which is more than twice the national average of 382 people per square kilometre (Census India, 2011). Second, international travel and tourism is a large part of the culture of the coastal state, which is served by four international airports that process an estimated 17 million passengers annually (Sulaiman et al., 2020: 4). Third, Kerala hosts around 2.5 million migrant labourers from other states and an equally large number of Keralites work abroad or out of state (Dutta and Fischer, 2021). In short, Kerala’s risk assessment necessitated quick and decisive action.
Kerala adopted a multipronged strategy to contain the spread of the virus and ‘flatten the curve’ including mass testing, quarantine, and support for the poor (Menon et al., 2020). For example, Kerala promoted wearing masks from as early as January and by the beginning of March, the government took additional precautionary measures including shutting down secondary and tertiary schools, asking religious and other groups to cancel all gatherings, including marriages and encouraging social distancing (Chathukulam and Tharamangalam, 2021). In terms of social welfare, the state government home-delivered free meals for school children and instructed internet service providers to increase bandwidth to encourage work from home (Sadanandan, 2020). Additionally, Kerala provided food rations, healthcare, and shelter for migrant workers and set up over 15,000 camps for them, accounting for 65% of India’s total number of camps displaced workers (Biswas, 2020a; Bloomberg, 2020; Sadanandan, 2020: 3). In other words, government officials in Kerala made sure that their COVID-19 response was inclusionary and protected the state’s most vulnerable populations including the poor, the elderly, women, children and those living in rural areas.
Kerala’s testing protocols were rigorous and aided by the state’s extensive network of public and private hospitals and clinics in urban and rural areas. The first hurdle the state faced was how to identify cases of COVID-19 and so intensive training was offered to doctors and healthcare workers throughout the state (Rahim and Chacko, 2020). Next, the state installed health check-up booths in all railway stations, state borders, and airports to help monitor people entering the state (World Health Organization, 2020). Testing laboratories were set up around the state to ensure quicker testing and Kerala had the highest test average of any state (Kaul, 2020). Kerala also prioritized the testing of high-risk groups rather than testing the entire population. This selective approach to testing, ensured that Kerala optimized the use of its limited testing kits and lessened the volume of tests processed by laboratories.
Another component of Kerala’s strategy was contact tracing. According to Heller (2020), Kerala’s COVID response was effective because it relied on the state’s strong civil society including grassroots level organizations and an established social system that encourages community cooperation. Additionally, volunteers were trained and deployed to deliver food and perform check-ups on those in quarantine (Rahim and Chacko, 2020; Vijayanand, 2020). Individuals who arrived in Kerala after 14 January from countries with COVID-19 infections were traced and scanned by local authorities and a mandatory quarantine of 28 days was instituted for everyone entering the state (Rahim and Chacko, 2020). High risk individuals who were in contact with those infected with COVID-19 were tracked and quarantined, further lowering the need for additional testing (Rahim and Chacko, 2020).
The state government established isolation wards in medical colleges as well as ‘COVID war-rooms’ throughout the state (Bhagat, 2021). Kerala also partnered with Indian multinational conglomerate, Tata Group to develop a 500-bed coronavirus treatment centre in Kasaragod (Poikayil, 2020). In fact, Sulaiman et al. (2020: 11) found that roughly 90% of people who were isolated in their own homes received necessary support including food, medical check-ups, and counselling. Individuals who were unable to quarantine in their home, were quarantined in isolation facilities in hostels, schools, and unoccupied buildings (Raghunath, 2020).
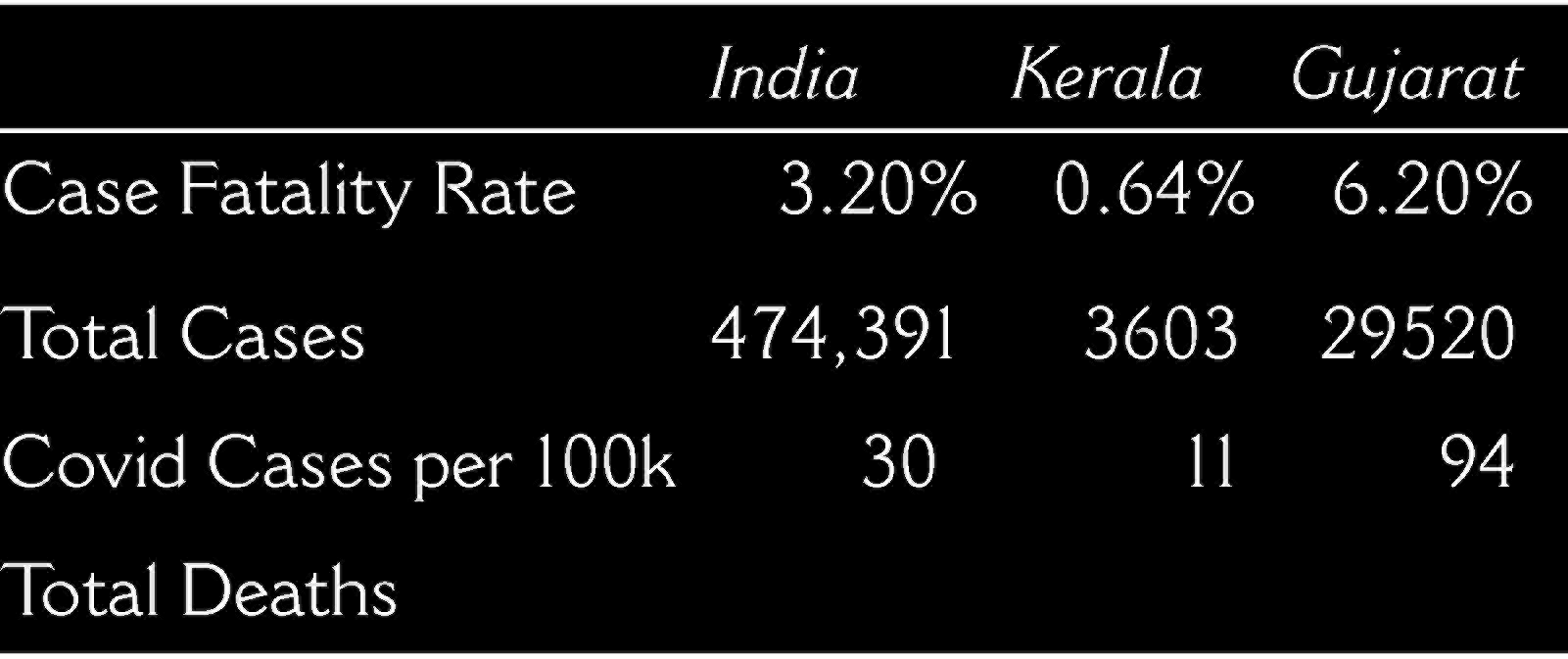
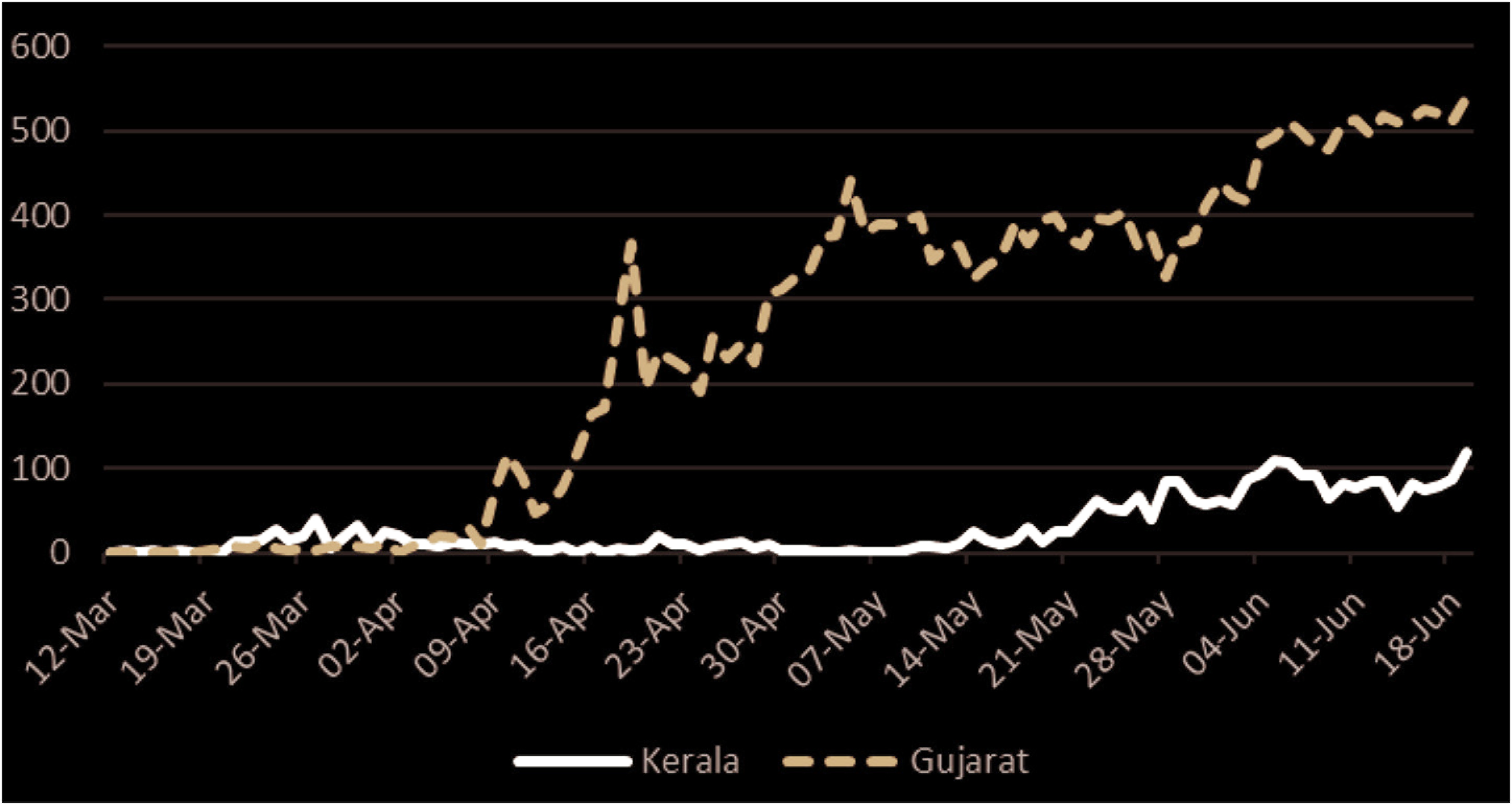
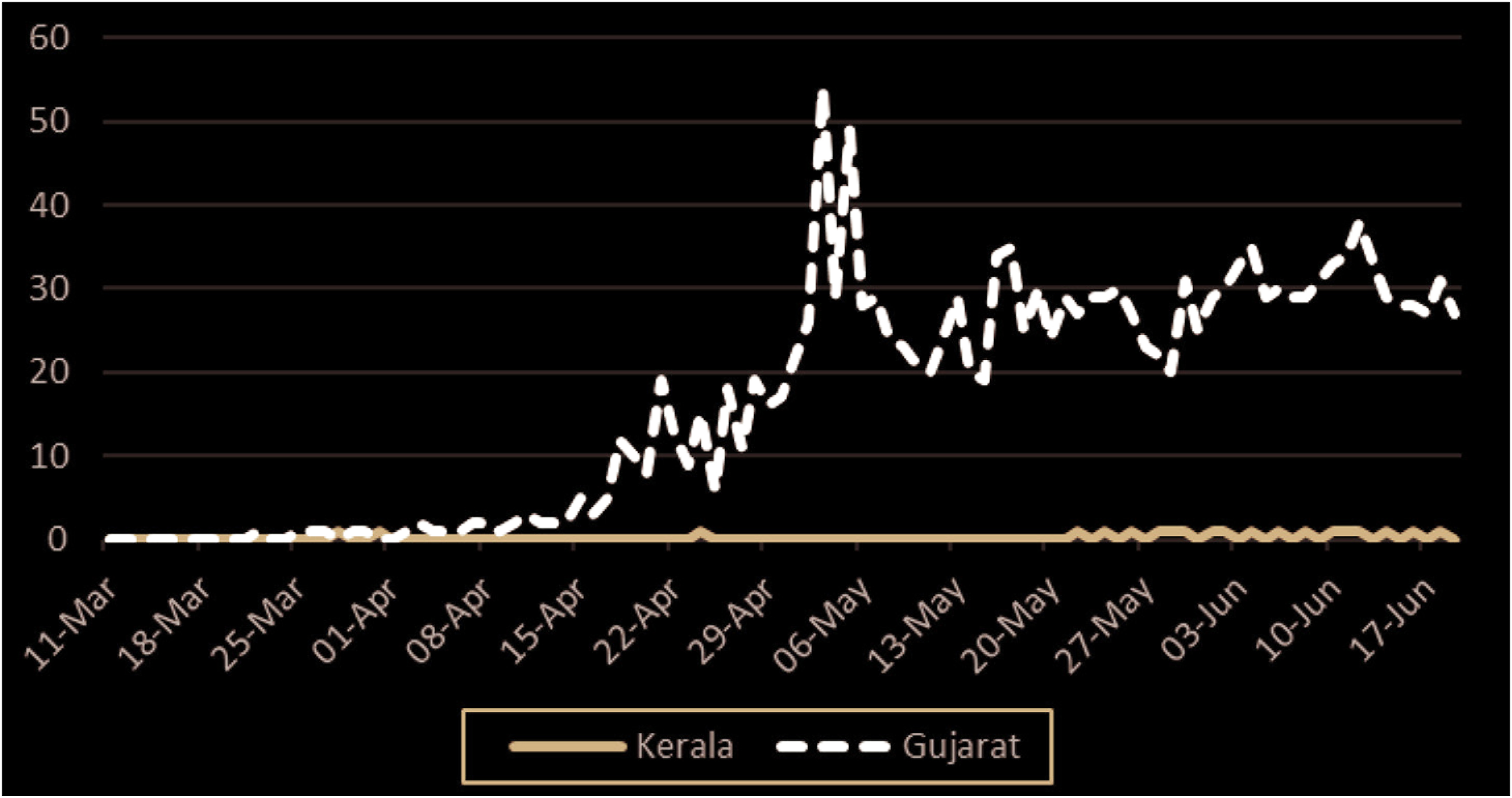
By the time the national government instituted a nationwide lockdown on 25 March, Kerala had already instituted their own lockdown and started the ‘Break the Chain’ campaign to promote social distancing (Sarkar, 2021). Additionally, the state government held a press conference every evening to answer questions from the public regarding the outbreak as well as to dispel myths and reduce rumours about the coronavirus. Local authorities also mandated that individuals hold an umbrella when outside and distributed umbrellas to promote social distancing (Sulaiman et al., 2020: 12). In high-risk areas, the police created an online delivery system of essential food items. Other innovations to help reduce community spread was the creation of smart bins called ‘BIN-19’ to collect and disinfect used facemasks (DD News, 2020). The state also took action to establish approximately 1,200 community kitchens to feed the poor and unemployed (Sarkar, 2021). Table two demonstrates how Kerala’s preparedness and background translated into its strong initial performance. Figures one and two also demonstrate how Kerala was able to keep cases and deaths low during the first 100 days of the pandemic. In contrast, Gujarat had the second highest rates in the country and among the highest death rates in the world.
Covid Data First 100 Days (March 11-June 19, 2020)
Covid Data First 100 Days (March 11-June 19, 2020)
After Kerala’s initial success however, the state reported a sharp spike in COVID-19 cases in July, calling into question the Kerala model and the government’s initial success. State officials identified community spread in coastal communities, which apparently had not been as closely monitored as airports and borders with other states, as one cause of the spike in July (Biswas, 2020a). The nearly half a million Keralites returning home from jobs in the Gulf countries and from other states in India after the easing of the nationwide lockdown in June also contributed to the increase (Biswas, 2020a). In fact, more than 7,000 of the reported cases in July had a history of travel, which likely caused a surge in local community transmission (Biswas, 2020b).
Most epidemiologists believe Kerala did a good job dealing with the initial pandemic response. Acharya and Porwal (2020) created a social vulnerability index to determine a district and state’s vulnerability related to COVID-19. The vulnerability index ranked states along five dimensions relating to their management and response to COVID-19, these are: socioeconomic condition, demographic condition, housing and hygiene condition, availability of health-care facilities and COVID-19-related epidemiological factors. Using this index, Kerala was assigned a relatively low vulnerability score of 0.314 out of a maximum score of 1.0 (Acharya and Porwal, 2020). This index shows that the Kerala model with its emphasis on public investment in health, strong ties between the government and citizens through social movements and civil society and inclusionary social policies have had a positive impact on Kerala’s COVID-19 response and its robust health infrastructure was better prepared than more economically developed states to handle the later surge that occurred (Biswas, 2020a).
Gujarat
According to Acharya and Porwal (2020), several factors can increase a state’s vulnerability to coronavirus including: poverty, education levels, the percentage of the population who were elderly, population density, household size, access to sanitation, health insurance, access to public hospitals, available hospital beds, and the percentage of the population immunocompromised or with underlying health conditions. Gujarat performed poorly overall in Acharya and Porwal’s (2020) study of vulnerability to coronavirus. Gujarat was among the worst performing states in terms of housing, hygiene, and access to healthcare. Gujarat also has among the lowest number of healthcare facilities per 100,000 people in India, making access to healthcare difficult even under normal circumstances (Singh et al., 2020). The state’s initial response was so problematic that the Gujarat High Court remarked that conditions at local hospitals were ‘pathetic’ and ‘as good as a dungeon, maybe worse’ (Ghosh, 2020a). Gujarat’s initial case fatality rate was also higher than other states. In April 2020, the fatality rate was listed as 7.88%, among the highest in the world and more than double the national average of 2.8%, which was still high by global standards (Kumar, 2020). With Gujarat’s limited number of beds, hospitals had limited or no capacity to admit and isolate symptomatic patients.
Many patients failed to receive an early diagnosis and were admitted to the hospital only once severe symptoms had escalated and their viral load was high. The President of the Indian Medical Association in Gujarat said that rather than going to receive professional medical care, many patients chose to self-medicate (Grewal and Jain, 2020). The lack of access to healthcare and early onset healthcare, reflects several failures in Gujarat’s medical system. Many citizens lack access to clinics and must travel long distances for care, which is cost and time prohibitive, especially for those working in the informal sector. According to a local legislator, residents feared going to the hospital because they associated it with an increased fatality rate alongside low levels of existing trust in the medical facilities (Langa, 2020). Unclear guidelines at both the national and state level also contributed to confusion that overburdened the hospitals in the early days of the pandemic.
Testing was also severely, and perhaps artificially, limited. The Ahmedabad Medical Association (AMA) filed a Public Interest Litigation (PIL) challenging the decision of the government to limit testing in the state. While the state encouraged the use of private facilities to treat COVID-19 patients, they limited the amount of testing at private laboratories and required government approval of tests ordered by private doctors (Express News Service, 2020). Only twelve private laboratories were permitted to test COVID-19 samples in the entire state in addition to the nineteen government laboratories (Press Trust of India, 2020a). Although the state increased testing after May 2020, the government was accused of deliberately limiting testing. The state also failed to employ enough contact tracers, making it difficult to identify community spread and contain the spread of the virus (Times of India, 2020). On 29 May 2020, the High Court of Gujarat again criticized the state’s coronavirus response and limits on testing. In response, government officials defended its low testing rate stating that testing should not be done for ‘asymptomatic individuals, asymptomatic contacts of a positive patient or asymptomatic family of those in quarantine’ (The Indian Express, 2020).
When responding to the state high court’s inquiry into possible attempts by the government to artificially limit the data through low testing, the government responded:
‘The likelihood of fear psychosis being crept in cannot be ruled out, if COVID-19 testing is allowed in all asymptomatic cases, just for acquiring a feeling of safety and security’ (The Indian Express, 2020).
Gujarat officials also attempted to stifle criticism from journalists. As previous critics have contended, freedom of press has slowly deteriorated in Gujarat (Guha, 2020). While the connection between freedom of press and the coronavirus may not be immediately clear, the government has used the health emergency as a pretext to punish journalists that are critical of the government. For example, a journalist that criticized the state government’s coronavirus response was charged under the Sedition Law and the Disaster Management Act (CPJ, 2020). The penalties under the law are quite harsh with life in prison for violating the Sedition Law if convicted and imprisonment for two years if found to be spreading false information.
In addition to its reactionary response and limited testing, the government also acted punitively to enforce the lockdown and limit criticism of its response. When residents were found violating orders, the police often responded with violence. Migrant workers who had been left with no income due to the lockdown were especially targeted and had their stock destroyed by police when found working outside selling fruits and vegetables (Dharni, 2020). Police clashed with crowds and used violent measures to disperse crowds, including rubber bullets and tear gas in the Shahpur area of Ahmedabad, a city with a history of communal violence (Khanna, 2020). Government officials also used religious minority groups as scapegoats, blaming them for the spread of the virus. Vijay Rupani, the Chief Minister of Gujarat, blamed the Muslim organization Tablighi Jamaat for the increase in cases in the state and cited the Muslim neighbourhoods in Ahmedabad as the primary driver of the virus (India Today, 2020). The Tablighi Jamaat also came under national scrutiny in mid-March after the group had a large conference prior to the national lockdown that was later tied to several positive cases. A Bombay court later struck down the response against the Tablighi Jamaat saying the propaganda against the group was unwarranted (Chaudhari, 2020). The scapegoating of the Tablighi Jamaat likely delayed critical response time while taking focus away from the government failure to respond.
The nature of the political system in Gujarat means that the state’s relationship with citizens is organized around delivering economically, which leaves little room to ask citizens to either make sacrifices or mobilize for public health gains. Gujarat’s historical experience with disease outbreaks should have helped prepare it for COVID-19. However, the state responded in a predictable manner, reactively and marginalizing. The marginalization of already disenfranchised communities, particularly migrant workers, Adivasis, and the landless community further demonstrates the disparity in care in states like Gujarat. The migrant crisis spurred by the coronavirus has been called the worst migration crisis since the 1947 partition (Infante, 2020). Following the lockdown, Gujarat provided minimal resources and safety nets for the migrant worker community, which constitutes 3 million of the state’s population and up to 50% of the workforce in large cities like Surat (Kaushik, 2020). The initial lack of support, including basic necessities such as food, shelter, and testing for the migrant community meant the most vulnerable were left with limited help. Rather than establishing widespread relief camps like other states, state officials instructed employers to provide 3 weeks of food and money to their migrant employees but established limited or no enforcement mechanisms (Press Trust of India, 2020b). The poor conditions and lack of food, shelter, and healthcare caused the migrant workers to protest and clash with police throughout Gujarat (Khanna, 2020). And again, relying on punitive measures, the government filed police cases for migrants found traveling during the initial 21-day quarantine (Press Trust of India, 2020b).
This article investigated the relationship between the Kerala and Gujarat development models respectively and how these models shaped each state’s response to the COVID-19 pandemic. We argued that the Kerala model, characterized by proactive state policymaking, broad-based coalitional social movements, strong civil society, and inclusive social policies, performed better than Gujarat in the first 100 days following the WHO’s declaration of COVID-19 as a global pandemic. The state’s long-term investment in healthcare ensured that the state had the capacity to respond to the virus and was able to create a system that allowed for the rapid and efficient testing of large numbers of samples at the same time, train healthcare workers on how to deal with COVID-19 patients and transform existing healthcare facilities to COVID-19 hospitals. Additionally, Kerala’s history of cross-community political mobilization and social movements meant that regardless of the ideological leanings of the party in power, the government maintained a comparatively high level of investment in the health sector. Strong civil society, in combination with decentralization, meant that there was a constant feedback loop between government and citizens, thereby ensuring that aid and policy was responsive to the needs of local communities. Finally, Kerala’s inclusionary social policies, along with state official’s transparency and communicativeness concerning the handling of the pandemic, meant that there was a high level of public trust in the government, ensuring that there would be a high level of citizen cooperation in attempts at ‘flattening the curve’.
As the pandemic continued into 2021, some of the initial successes touted in the Kerala model appeared to diminish, with Kerala reporting over 1.1 million cases as of March 2021. However, as India surged into a deadly second wave in Spring 2021, Kerala did not have the same difficulties facing other states such as procuring oxygen, ventilators, and ICU beds (Bhagat, 2021). Kerala also continued to carry out extensive testing, which perhaps accounts for Kerala’s high COVID-19 case count but reflects a more accurate number compared to states that have been accused of undercounting and undertesting (Biswas, 2020a). Kerala, along with the richest countries in the world, have all struggled to contain COVID-19. Rather than reflecting poorly on the Kerala model, the increase in cases is more a reflection of the nature of pandemics, which is more of a marathon than a sprint.
In contrast, Gujarat’s response to COVID-19 reflects the state’s prioritization of economic development at the expense of investment in health and social development. Years of social welfare cuts, dependence on private healthcare, and limited long-term investment in public health and education meant that the state was inadequately prepared to respond to the pandemic. Private profit driven healthcare cannot provide the strong public health responses needed in the face of a pandemic. Limited access to healthcare facilities, particularly in rural areas, meant healthcare facilities were overwhelmed and unable to address surging cases. Furthermore, Gujarat’s reactive response meant inadequate PPE, insufficient ventilators, ICU beds, and isolation wards. The government’s policy of not testing asymptomatic individuals or those in contact with a positive case means the coronavirus case count was kept artificially low, which let the virus spread through the community unabated. This criticism continued amid the second wave in Spring 2021, multiple reports cited that Gujarat was vastly undercounting infections and deaths (Bhaskar, 2021). The actual number of COVID-19 related deaths in Gujarat or India may never be fully known.
Gujarat’s poor pandemic response may be surprising given the BJP’s longstanding emphasis on Gujarat as a success story. However, the state’s economic emphasis came at the cost of healthcare and other key social platforms. The first wave of the pandemic ultimately helped illuminate the shortcomings of the Gujarat model broadly and of its inadequate healthcare system specifically. Furthermore, the punitive response by the state especially targeting religious minorities and migrant workers further reveals deep seated inequities along economic, caste, and religious lines. The consequences of Gujarat’s decades-long divestment of social spending have been made apparent by the pandemic.
Although this article focused on Gujarat and Kerala, the findings have implications well beyond the two states. First, the findings speak more generally about two competing visions for India. The first, the Hindu nationalist model of the BJP, embraces a neoliberal economic vision where the state is less involved in social affairs and instead prioritizes economic growth, attracting investment, and building capital. This vision has been electorally popular throughout India’s Hindi belt and beyond, including some northeast states like Assam. Under the Modi regime, the Gujarat model has been expanded throughout many Indian states. India’s abysmal response and lack of preparedness in the Spring 2021 second wave reflects the broader failures of a Gujarat style model on a national level.
The Spring 2021 assembly elections in Kerala, Tamil Nadu, and West Bengal provided initial insight into how the population may evaluate the BJP’s management of COVID-19 in India. The results demonstrated that the Hindu nationalist vision has largely been rejected in favour of regional parties in these states. Instead, India’s other competing vision of a robust social welfare system has remained popular, particularly among left leaning and regional parties outside of the Hindi belt, such as the Dravida Munnetra Kazhagam in Tamil Nadu, the All-India Trinamool Congress in West Bengal, and the Communist Parties in Kerala (Bhatnagar, 2021). However, the Indian National Congress (INC), which has historically upheld the Nehruvian ideals of an expansive welfare state that is both socialist and secular, has struggled to maintain support amid the increasing popularity of the BJP and the regional parties (Bhatnagar, 2021)
Beyond India, the outcomes and approaches in Gujarat and Kerala speak to a broader global trend and should be investigated in future research. Neoliberal approaches such as those initiated by the Washington Consensus have dominated much of the Global South’s developmental models. COVID-19, in all its devastation, allowed scholars and policymakers to evaluate the effectiveness of different models when facing a common adversary. When it comes to COVID-19 the developmental model does not appear to be destiny. Some neoliberal countries, like Brazil, faced widespread death, inadequate healthcare infrastructure, and a seemingly unconcerned central government (Ortega and Orsini, 2020). Other neoliberal countries like South Korea were able to minimize deaths from COVID-19 and provide expansive testing and treatment for COVID-19 patients (Dighe, 2020). Social democratic models like the one seen in Kerala are less common in the developing world. In fact, even advanced social democracies like Sweden struggled to respond effectively to the threat (Claeson and Hanson, 2020), indicating that access to greater resources do not necessarily translate to positive pandemic responses. In contrast, Kerala was able to control the early outbreak with a fraction of the resources, demonstrating the viability of the Kerala model in responding to public health crises in the developing world. The success of the Kerala model vis-à-vis the Gujarat model should give international development scholars and organizations pause and serve as further evidence that neoliberal developmental models are not a panacea for all the social and economic inequities found in the Global South.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.