
Abstract
The COVID-19 pandemic brought about changes to the lives of families with young children. It has been associated with physical and psychological risk, yet the impact on younger children is poorly examined. The aim of this qualitative study was to examine how the COVID-19 pandemic impacted the day-to-day life of parents of young children living in a small northern city in British Columbia, Canada. Ten mothers with children aged 0–5 years participated in a six-week longitudinal study between November 2020 and March 2021. This article presents data from entry and exit interviews that were analysed using Todorov's narrative theory. Three key themes were identified: (1) gaps in health services; (2) gaps in early childhood education and programs; and (3) changes to/lost social interactions. Limited opportunities to engage with providers caused frustration and left parents feeling disempowered or dissatisfied. Family support and well-being were negatively impacted by a loss in social connectivity. Despite unpredictability and worries about child development, most of the mothers found ways to cherish the time to ‘stop and refocus’. Overall, the families evidenced resilience, despite a loss in relational habits.
Introduction
The COVID-19 pandemic brought about global and local changes to the lives of parents/caregivers/guardians and their children (here described as family), resulting in major modifications to health and social care engagement. Stay-at-home messaging (Chiesa et al., 2021), in combination with a reconfiguration of the delivery of health and early years programs, resulted in reduced access to health services (De Araújo et al., 2020), therapies (Charney et al., 2020) and early educational opportunities (Davies et al., 2021; Spiteri, 2021) globally and specifically in British Columbia (BC), Canada (Human Early Learning Partnership, 2021). With the early years being a critical stage in child and family development (Center on the Developing Child, 2016), these changes are impactful for families with young children. Reduced access to health and social care has the potential to impact child health (Beno et al., 2021), parental health literacy and relationship-building, resulting in maternal mental health risks (Venta et al., 2021).
To understand the impact of COVID-19 on families, the rapid survey designs that have been deployed have focused on the mental health of school-aged children and adolescents, largely in urban settings (Bray et al., 2021; Rider et al., 2021), neglecting the needs of children aged 0–5 years and those living in more rural contexts.
The pandemic and service provision context
The system of early years services in BC is complex, drawing on several government ministries, local and provincial health authorities, Indigenous communities, municipalities and community organizations (Koopmans et al., 2021). The services available vary by community but typically include universal health services provided by primary care and/or public health teams; universal early learning drop-in programs funded by the Ministry of Education; and preschool early childhood education programs and childcare facilities provided at a cost to families. Eligible families may access the Affordable Child Care Benefit in BC to help with the cost of childcare. This subsidy is determined by factors including income, family size and type of care. Families may also access referral-based programs for specialized support such as Infant Development Programs for children up to three years of age who are delayed in certain skills or at risk of potential delays. As the largest city in northern BC, the study community (Prince George) has a wider breadth of services, including access to a local child development centre providing specialized services for children and families such as physiotherapy, occupational therapy, speech language pathology and supported child development programs, as well as a First Nations Friendship Centre with early childhood programs.
The pandemic restrictions during this data collection period began with a ‘safe six’ policy where families could gather with up to six other close contacts external to the household, and later transitioned to restrictions of no social gatherings outside of the immediate household on 19 November 2020. These restrictions remained in place until March 2021. Early years preschool programming was initially closed, with varied ‘reopening’ options in line with the BC Centre for Disease Control’s (2021) guidelines.
Geographical context
Prince George is the largest city in northern BC, with a population of approximately 76,000 living on the traditional unceded lands of the Lheidli T’enneh First Nation (Statistics Canada, 2022). Families living in northern and/or rural communities (including Prince George) experience higher rates of vulnerability in early childhood development domains (Human Early Learning Partnership, 2020).
Situating the study
In examining emerging evidence surrounding COVID-19, we acknowledge the major reorganization it brought to families’ lives (Proulx et al., 2021; Weaver and Swank, 2021). Early reports of the financial burden on families, shifts in parental home-care activities, increased child screen time, decreased physical activity and increased food insecurity (Pelletier et al., 2021; Proulx et al., 2021) concurred with observations from our clinical collaborators. We recognized both knowledge and methodological gaps regarding COVID-19 research with families with young children. Recognizing the need and in partnership with our community stakeholders, we collaboratively designed this pilot study. Care was taken to ensure that families were able to participate fully while adapting to the pandemic circumstances and challenges.
The aim of the study was to apply qualitative participatory research in order to examine the impact of the COVID-19 pandemic on families' lives by exploring their day-to-day experiences. We were interested in understanding interactions with services and providers, changes in family routine, breaks in the continuity of care or early learning opportunities, missed significant life events, loss of security and safety, and parental early childhood literacy gaps.
Methods
Our overarching framework for this study focused on relational practices and recognized the participation of younger children in their families' lives within a model of citizenship (Hultgren and Johansson, 2019; Larkins, 2014). While younger children are afforded a membership role in society, this is commonly situated within the family and preschool education contexts. Bioecological models recognize the environmental and interrelated systems (Ashiabi and O’Neal, 2015) that influence anticipatory health-care practices to inform health and well-being. In combination, health and social equity contribute to a child's developmental trajectory by supporting everyday choices and practices that build resilience.
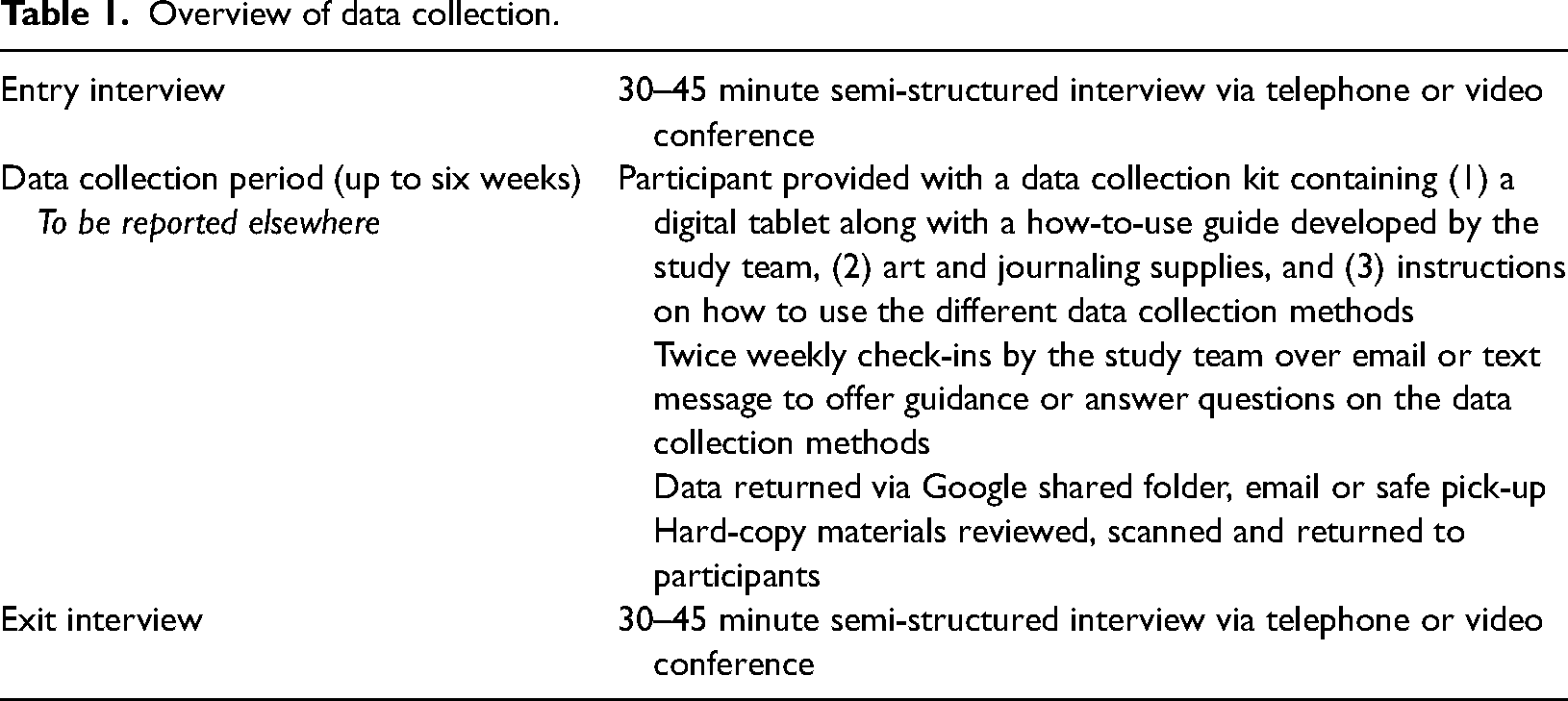
We applied qualitative methods to capture rich descriptive data, consisting of semi-structured entry and exit interviews and asynchronous data collected over a six-week period (to be reported elsewhere; Polit and Beck, 2014; Sandelowski, 2010). In the interviews, the participants were asked about their experiences of COVID-19 in their role as parents, its impact on family day-to-day life, and their experiences of engagement with provider services during COVID-19 (see Appendix 1). A longitudinal approach supported the natural capture (Kim et al., 2017) of parents’ narrative day-to-day experiences. The ongoing data collection over the six-week period supported parents’ recall of important events during the exit interviews. The participants were given a choice of compensation at the end of the study period. They could either keep the data collection tablet or receive a gift card of equal value ($150 Canadian dollars). A summary of the data collection methods is provided in Table 1.
Overview of data collection.
Recruitment
The purposeful sampling involved recruiting participants from Prince George with at least one child aged 0–5 years. Recruitment was through community partners and local community organizations’ social media platforms. The interested participants contacted the study coordinator via text or email. Participant selection took place based on neighbourhood and the age of the children to ensure a diversity of experiences among the sample (maximum variation sampling). The recruitment and data collection for this study took place between November 2020 and March 2021.
Ethics
The study was approved by the University of Northern British Columbia’s Research Ethics Board (reference number E2020.0707.034.00). All of the participants provided written or verbal informed consent.
Analysis
The verbatim transcripts were reviewed in depth by three members of the study team, applying the six-step technique outlined by Braun and Clarke (2006). This approach enabled identification of common narratives between the transcripts. Following familiarization, notes were presented and discussed at weekly team meetings. Manual coding was applied by three team members. Realistic and descriptive longer narrative codes based on Todorov's theory were utilized (Bingley, 2020). While often applied in media or literary studies as an analysis approach for fiction, Todorov's theory was considered an adjunct to Braun and Clarke (2006) since living in the pandemic was noted to be an unimaginable event. Todorov's narrative theory applies a model that is focused on the disruption experienced by a character (Todorov and Weinstein, 1969) – in our case, the participants. The five stages (see Figure 1) of a narrative begin with an equilibrium (in our case, the world as it was pre COVID), which is followed by a disruption (the COVID pandemic), a recognition (the experience of change in daily life), a repair attempt (trying to reorder living in new circumstances) and restoration (the new normal).
Three of the authors (TF, TA, CS) applied pattern-based analysis (Braun and Clarke, 2006) to identify salient features focused on answering the key study questions (Braun and Clarke, 2006). The theme content was considered important if it affected most of the participants. Consensus was reached by reviewing the data and collective discussion. In applying Todorov's theory, the ‘heart’ of families' day-to-day life and the cyclical impact of COVID-19 was broadly framed within the framework's five stages. Direct quotes are used to illuminate the narratives. The participants were assigned random numbers from 1 to 10.
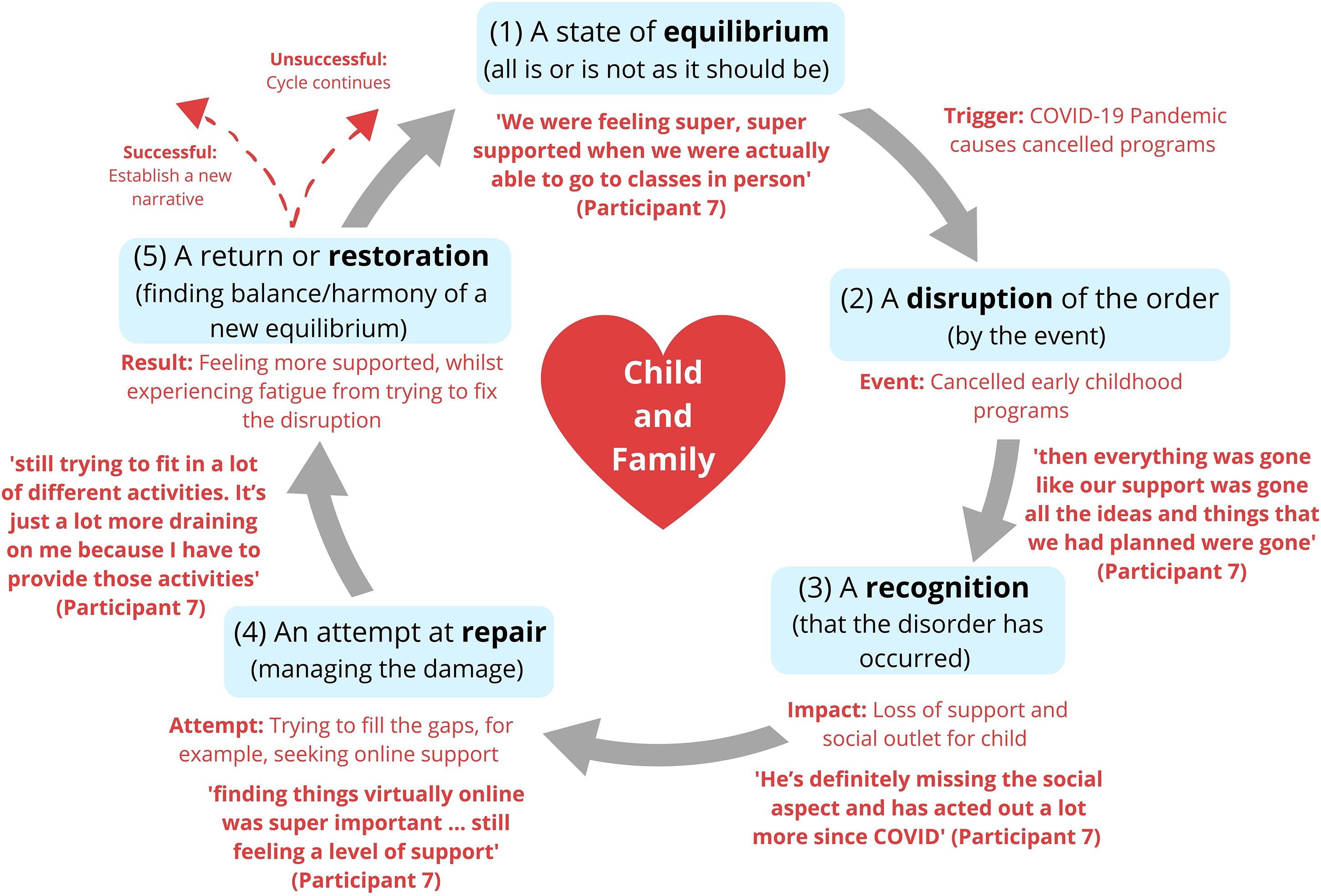
Adapted Todorov narrative theory with an example of analysis.
Results
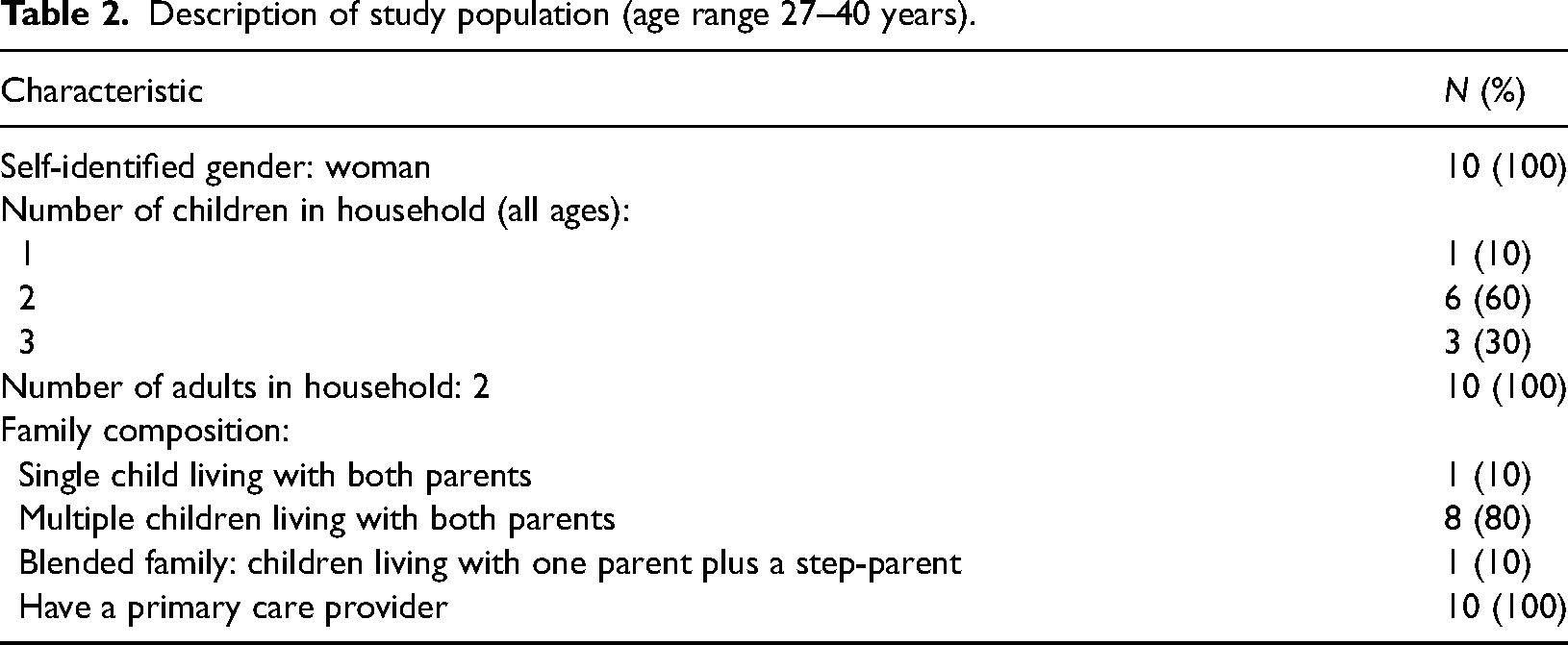
Interest to participate was received from 86 families. Ten families were selected for participation based on the available funding and purposeful sampling (Table 2). Entry and exit interviews were conducted via Zoom and lasted between 20.45 and 50.12 minutes (M = 32.15 minutes). As the pandemic restrictions remained unchanged over the data collection period, there were no changes in circumstances in the parents’ day-to-day lives. The following sections report on the key themes: (1) gaps in health services; (2) gaps in early childhood education and programs; and (3) lack of and changes in social interaction.
Description of study population (age range 27–40 years).
Gaps in health services
Changing equilibrium resulting in disruptions to health services
In line with Todorov's narrative theory (Todorov and Weinstein, 1969), family took the central role in securing equilibrium. However, this was disrupted by the pandemic in a range of ways. The parents were confronted with the rapid shifting of health-care appointments to online or telephone formats. With the disruption to typical in-person service delivery, several parents reported that additional steps were now required to be ‘granted’ an in-person appointment. This meant that parents had to find new ways to resolve health-care access obstacles. Participant 10 shared her frustrations with the extra work needed to secure an appointment: ‘You have to have a phone conversation before … they decide’. Others talked about calls not being returned: ‘My doctor's amazing but … four appointments uncalled [no call back] … because of emergencies’ (Participant 9). The participants also talked about either losing access to anticipatory or routine check-ups or putting off such visits. For some, the loss of anticipatory care was ‘frustrating’ (Participant 6) as they were now on the ‘back-burner’ (Participant 3). The parents understood that limiting exposure reduced risk but they did not believe that a telephone consultation was equivalent to a face-to-face experience, especially for allied health-care services such as speech and language therapy. For example, Participant 3 commented: ‘I’ve, like, put stuff off because I’m, like, “Oh, it has to be done over the phone and that's not feasible”’.
The participants also talked about the worry when they needed to make a more ‘urgent’ health-care visit. Participant 9 shared a story of how ‘awkward’ visiting a walk-in clinic was with her young child: Once we got in the room, I seen her kind of release a little bit and calm down. I think it's just because the hype of, like, being aware of other people and germs and stuff, so when we were in the waiting room knowing there's sick people, it's overwhelming … getting tested and sitting in the room and having someone come in fully geared up and swab your brain.
Recognizing the changes to ‘being in charge’ of one’s child's health
For some of the participants, access changes or cancelled scheduled health-care visits resulted in a feeling of lost agency over their child's health. The variation between providers was perceived as confusing, with Participant 3 reflecting on when the family could not access the same health-care service: My fiancé and my son go to one doctor and me and [daughter] go to another doctor, and he's been able to go into his doctor's but my doctor's office is only doing phone appointments unless it's deemed absolutely necessary.
Learning to navigate different service changes meant that some of the participants had to be adaptive as they attempted to repair the disruption, while others were ‘thankful’ that they did not need health services. Some of the parents tussled with the decision-making that focused on their child's best interests. For example, decision-making about when and where to access health care became ‘more of an internal kind of thought process’ (Participant 4), which relied on parents having greater knowledge about their child's health. Others spoke about ways they perceived they had to increase their advocacy skills to restore order: Our doctor is, like, ‘Well, that's not considered essential’, but I’m, like, ‘Well, we have this report, this report and this report to go over’. Because [names] are part of an Infant Development Program … so I have some reports and stuff to discuss, like, because there's some concerns. They were, like, ‘Oh yeah, well bring her in’, and I brought them both in at the same time … One and done. So that was fine but, at first, they were, like, ‘We won't be seeing her’. (Participant 8)
The participants discussed how they could no longer have a supportive ‘other’ with them during health-care visits. This often resulted in the exclusion of fathers; according to the participants we spoke to, their partners felt left out of health matters concerning their child. For example, Participant 6 shared: ‘The amount of involvement that men feel with COVID, and all of the new policies and procedures, is really disappointing’. There was no opportunity for fathers to find a resolution to this disruption, and so there was a break in the cycle that could afford the opportunity for the family to find a new equilibrium.
Managing the unexpected; thinking about restoring services
Despite the difficulties brought on by the changes, the new approaches were recognized and welcomed. Participant 2 described it as follows: ‘They are almost kind of triaging you over the phone to decide if they should actually see you in person or not. … I think it's actually a really great system. I think it unclogs the health-care system’. Phone appointments were identified as more convenient because the parents did ‘not have to bundle the kids up and be in the waiting rooms and actually like to have just a conversation and then move on’ (Participant 6). Participant 10 had a very good relationship with her family doctor and his office, describing them as ‘very easy [to] access … [having] a wealth of knowledge … He has just been great, so any time I ever need anything, I call his office; they are all super wonderful’ – which was very important when justifying why access was at times difficult. For the participants with high health-care literacy, access to evidence-informed health-care messaging via health authority sites filled the gaps: ‘I use my [provider] sites so [I know about] precaution[s] and I know how to because I’m a health-care worker’ (Participant 1).
At times, other health-care providers, like pharmacists, helped to manage care-and-repair communication gaps between the participants and physicians. Access to pharmacists was not disrupted and was highly valued, as Participant 9 clearly articulated: ‘Thank God for pharmacies doing, like, emergency refills. They are awesome’. Thinking to the future, the participants were eager to bring back scheduled appointments and rebuild relationships. Despite balancing new approaches, they continued to ‘miss’ connection, and attempts to repair were viewed as temporary innovative solutions rather than the restoration of equilibrium.
Gaps in early childhood education and programs
Disruption to services and the impact of disturbances in support
The parents’ experiences with early childhood education programs were comparable to their experiences with health-care services. For an example of how this can be represented as a model in line with Todorov and Weinstein's (1969) theory see Figure 1.
At the start of the pandemic, families encountered a disruption to early childhood programs (such as playgroups or early learning opportunities). Some were cancelled without replacement; others underwent changes in their structure (online rather than in person) and/or availability (sign-up required versus drop in). Program cancellation or reduced availability was reported as problematic, as Participant 4 observed: ‘CDC [Child Development Centre] has said “I[’ll] see you in a year” and IDP [Infant Development Program] not so much … I haven't really found anything to kind of fill that void yet’.
In many instances, drop-in options were discontinued, and programs required parents to commit to regular attendance at specific times, which was not always feasible, as described by Participant 7: Being a mom of two boys, drop-in was way more preferred. Some days I just don't want to make the commitment; some days my kids are just not in the mood, so to have to commit to a day is a little bit more difficult when it comes to Strong Start, so we opted not do it. The girls were asking questions about why they couldn’t have this … trying to explain to a three-year-old that … she can’t go to the pool and she can't do this because one has to book three months in advance with the pool and you have to book a spot, and just the challenges, like, of trying to book this far in advance.
Recognition of missing out on early years activities, new adjustments and repair attempts
A particular kind of grief over missing out on certain programs was experienced by a new mother, Participant 4: ‘The idea of what we wanted it to be like, especially for our first kid, has completely [changed]. Like, it’s nothing like we wanted it to be’. This sentiment was shared by Participant 9, a mother of three, who said: ‘Your kid is only gonna be a certain age for so long and having to miss out on doing those things at that particular age I think was a bit shitty, for lack of a better word’. There was a realization that the pandemic resulted in a disruption that was irreparable, and recognizing that these missed early experiences would never be recaptured was emotionally draining for the parents.
Despite the negative aspects of changes to programming, some positives were discussed. Participant 10 commented: ‘I do not miss the drop-in aspect. I actually enjoy the smaller groups. You make more of a connection with people that way’. Having to slow down served as a lesson for Participant 2, who said: I still have a million things to do but it's just a little bit less. And I think taking that time to really be mindful and thoughtful about what I continue with after all this is over is really important.
Lack of and changes in social interactions
Disruption in connectivity with friends and family
All 10 mothers experienced periods of social instability and spoke about the impact of changed, reduced or absent social interactions – for themselves, their young children and the wider family. Most of the participants recognized that socialization informally with friends and family, at daycare or in early years activities supported child development and was a critical aspect in how they maintained equilibrium before the pandemic. Physical and mental activity was a critical aspect of social play and engagement, as described by Participant 7: My four-and-a-half-year-old is very spirited … So, it was very important to have him enrolled in a lot of different things so that he could expel his energy and he could kind of fill his bucket because he needs a lot of social stimuli. So, prior to COVID, we were very, very busy.
Recognizing – ‘Is my child doing OK?’
Fewer or no social interactions led some of the participants to think about their child's development: I don't know if he's ahead or behind where he would’ve been in preschool as far as that goes but I feel like a little more ahead than the other two were at this age [because of] more family time. (Participant 5)
Having siblings, especially close in age, was a perceived benefit: ‘We are grateful to have more than one child’ (Participant 5). For families with one child, the social disruption created worry, as voiced by Participant 2: ‘I don't know if [not seeing others is] going to turn her into some, like, freak or, like, totally selfish only child’. The participants noted emotional changes in their children and how the absence of child-to-child relationships influenced well-being: ‘There's some big emotions coming from my daughter and … I think she's feeling a little stir-crazy because we haven't been able to see her friends in a long time’ (Participant 6).
The participants had to balance the risks and benefits of social isolation with short- and longer-term child development and well-being goals. At times, the participants deemed socialization more important than following public health guidance – for example, having a small network and making judgements as to who to meet in a ‘bubble’: ‘We have let one of our best friends in our bubble. As long as, like, cause I know they are just as strict with everything as we are’ (Participant 9). This approach to decision-making required a recognition of risk balanced against a need to restore relationships, as described by Participant 9: ‘There's a lot of trust being put on the other person that you are also visiting with. That they’re doing … that their threshold is the same as yours, I guess’.
Getting back to being social, repairing relationships and generating new narratives.
The participants reflected on their story, lamenting that their previous normality was altered by the pandemic. For example, they expected that a return to social activities would be a challenge. This was exemplified by Participant 2, I'm concerned about the way we automatically react to children trying to have social interaction with other children now. Whereas before you just wouldn't care if they touch other children or play with other things that other children would play with.
Participant 9 expressed worry that the current situation was ‘confusing for kids because at home you try to show them compassion and empathy and how to love each other. Then you go outside and then it's different’.
Again, despite the downsides, the parents consistently reported enjoying ‘more family time’ (Participant 5) as a restorative approach. They took the opportunity from absent social obligations to engage more with family, as Participant 6 recounted: ‘We spend a lot more time together and try to make it more meaningful’. This acted as an adaptation to lost emotional support, fostering an environment for families to ‘bond more’ (Participant 8) and attempt to restore a supportive equilibrium.
Discussion
This longitudinal qualitative study examined the impacts of the COVID-19 pandemic on the day-to-day life of parents of young children living in a small northern city in BC. Three key themes were identified to describe the impacts of the pandemic on the families’ day-to-day lives: (1) gaps in health services; (2) gaps in early childhood education and programs; and (3) a lack of and changes in social interaction. Our findings are reflected in the international literature, including health-care gaps reported in low-, middle- and high-income countries (Arsenault et al., 2022), changes and loss of early years education (Malta Campos and Vieira, 2021), and significant altering of social experiences for early years children (Watson et al., 2020).
Gaps in health services
When the parents recognized that their child needed unavailable health-care access, it limited their agency in meeting their child's health needs. The dichotomy of ‘essential’ and ‘non-essential’ runs the risk of obstructing our view of the indirect health consequences that may have lifelong impacts on younger children (Fung and Ricci, 2020). Some mothers considered anticipatory health visits essential, while others believed they could reinstate these later, possibly because of confidence in their health-literacy skills. Access to speech and language therapy services via early years programming was perceived as essential, which resulted in stress when this was no longer available or only offered in a manner that was not valued by the parents. Such limitations influence childhood adversity, which has an impact on children's health and well-being outcomes (Hertzman, 2013). For the mothers in our study, identifying who was able to decide on solutions to fill these new ‘gaps’ was worrisome. Since doctors were less accessible, pharmacies increased in importance for the families. Our analysis highlighted that pharmacy services were not disrupted and provided low-threshold opportunities for emergency refills and consultation throughout the pandemic, which resonates with reports by Grosman-Dziewiszek et al. (2021).
Similarly to Nobile and Drotar (2003), relational health encounters were valued by the participants in our study and fostered effective parent–provider communication, which improved care satisfaction. While generally appreciated, the telemedicine offered during COVID-19 was viewed as a repair approach that did not substitute for in-person care completely, especially for anticipatory guidance visits or speech and language appointments. Although not fully realized during the pandemic period, we recognize that telemedicine has the potential to be a supplementary approach in paediatric ambulatory settings (Rajani, 2017) and may be comparable to follow-up in-person visits for subspecialty or chronic childhood conditions, such as asthma (Shah and Badawy, 2021). The parents in our study recognized that telemedicine could streamline care and increase access, which Haleem et al. (2021) suggest is important in rural settings. Establishing a consistent approach that is family- and child-centred and values parents’ tacit knowledge about their child, a hybrid model combining telemedicine and in-person care, as outlined by Reingold et al. (2021), may offer a promising service-design approach.
The parents in our study valued their children as citizens within the context of their family and wider society, aware of the bioecological influence on family life and child well-being (Ashiabi and O’Neal, 2015; Larkins, 2014). To this end, they applied relational autonomy in decision-making about their children by adapting prior knowledge to develop new skills when navigating the changing health system. The parents recognized that the pandemic was disrupting services, which resulted in readjustments that focused on improving their health-literacy skills (Centers for Disease Control and Prevention, 2021) in finding, filtering, understanding and then applying information to inform health-related decisions.
Gaps in early childhood education and programs
Across the globe, other countries encountered similar challenges with the closure of childcare centres and early learning programs and restructuring of delivery, with a select few remaining open for the children of essential workers (Gromada et al., 2020). A survey of US early childhood education teachers found that they were able to maintain communication with families through phone calls, email and messaging applications whilst providing activities and online lessons for families to complete at home. However, more time was spent planning and communicating with families than providing instruction to children (Steed and Leach, 2021). These changes created new challenges in access to early years programming, similar to those identified by our participants. The landscape of programs and services for the early years in Canada is ‘a bewildering mix that is difficult for parents to navigate’ (Beach and Bertrand, 2009: 666), and the pandemic has only increased the complexity of navigating this landscape.
The parents were required to compensate for the lost support, which left them fatigued and concerned about their children's development. The lack of drop-in options and free resources posed particular challenges for some families. Considering the importance of quality care and learning opportunities in the early years (Masten et al., 2006), such a gap in provision is alarming. The threat to children's development is aggravated through the loss of parent-to-parent exchange and support opportunities typically found through early years development and learning programming. Such opportunities provide emotional support, information and a sense of community, supplementing the support offered by professionals (Hartman et al., 1992; Niela-Vilen et al., 2014). Finally, missing out on certain programs evoked a particular kind of grief connected to the fleeting nature of the early childhood years.
Within education, there is an emerging discussion that is focused on children as global citizens (Twigg et al., 2015). This discussion recognizes the significance of children's social experiences as both important and memorable – experiences that have been disrupted during the pandemic. Further, for some countries, emergency federal funding provided critical support to allow programs to be resumed (National Association for the Education of Young Children, 2022). Moving forward, the challenge will be to ensure that early years programs remain and to prevent widespread closures due to diminished funding or staffing issues. Like other countries, access to childcare before COVID within northern BC was difficult (Wearmouth, 2021), with lobbying for investment noted by the Human Early Learning Partnership in 2008 (Goelman et al., 2008). The pandemic may serve as an opportunity to address both the quality of and equitable access to early years opportunities as we build forward, acknowledging how essential early childhood supports are.
Lack of and changes in social interactions
Changed, reduced or periodically absent social interactions had large impacts on children and family life (Kerr et al., 2021). There was a fear among the mothers that the lack of socialization experienced during the pandemic may impact child development over the long term, and the literature confirms their worries (Bloomberg et al., 1994; Moriguchi, 2014; Saracho and Spodek, 2007). These worries were exacerbated in families with a single child. Balancing the risks of social isolation with short- and longer-term child development and well-being goals put mental and emotional strain on the parents. In line with emerging studies, technologies were used to repair and maintain social connectivity (Goldschmidt, 2020; Pelletier et al., 2021), which had some benefits yet were not seen as a replacement for face-to-face family-and-friend contact.
Returning to social activities is the next big challenge awaiting parents as we move out of the pandemic. Unlearning the enforced unsociability mandated by the pandemic in northern BC for 18 months may be challenging. The changes to parents’ networks and social groups because of the pandemic are likely to have ongoing impacts on families’ health and well-being, such as mental health strain (Wade et al., 2020). While we have seen a return of some programming (BC Centre for Disease Control, 2021) that allows for unstructured play, a critical aspect of the business of childhood (Canadian Public Health Association, 2019), ongoing social networking limitations – due to the lowest percentage of fully vaccinated individuals in BC residing in the north (COVID19 Tracker Canada, 2022) – likely heighten parents’ reservations and hesitation to engage with social groups or programs. While we recognize that such constraints limit children’s socio-emotional development and childhood outcomes (Thomson et al., 2021), how we begin to offer parents support in rebuilding safe and timely social connections continues to be an area of study.
Limitations
The key limitations of this study concern the sample. A lack of gender diversity is noted, since all of the participants identified as mothers and no fathers or other caregivers were reached in the recruitment phase. In addition, the family constellation was very homogenous, with both parents living in the household in 9 out of 10 cases and only one household including a step-parent. As an important health determinant, socio-economic status and subjective social status were limited in the present study, despite recruiting from a range of neighbourhoods.
Conclusion
The data analysed over the five-month period evidenced a loss in equilibrium reported by the parents in their day-to-day lives during the COVID-19 pandemic. We identified that for a population of mothers in northern BC, parenting during the pandemic was hard. Disruption to family life and limited access to health services and early years programming influenced child health and development. While the parents were able to recognize gaps in their child's care and relationships with others, there was a limitation in their capacity to repair and restore activities and interactions. Limited opportunities to engage with providers caused frustration and left parents feeling disempowered or dissatisfied. Family support and well-being was negatively impacted by a loss in social connectivity. It will be important to monitor the after-effects of the reduced medical supervision and missing out on early years education and social interactions experienced during the pandemic. Corresponding countermeasures will be crucial in renewing parents’ trust in the health and early years education systems to set children up for healthy development. Despite unpredictability and worries about child development, most mothers found ways to cherish the time and ‘stop and refocus’. Overall, the families evidenced resilience, despite a loss in relational habits.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the parents who participated in the study and shared their experiences. We also extend thanks to the community stakeholders that supported recruitment.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was funded by a BC Ministry of Health competitive grant administered by the University of Northern British Columbia.