
Abstract
Previous literature on advice-resistance in medicine and welfare has tended to focus on patients’ or callers’
Introduction
A problem for anyone giving advice is that what they offer may not be readily accepted by the recipient. The problem becomes potentially damaging when the advice is being offered by a welfare advisor, and even life-threatening if by a medical practitioner. Our interest in this article is to explore a particularly weighty kind of resistance to advice which has so far received very little attention: explicit objection.
Objection as a weighty kind of resistance
Previous studies of resistance to advice tended, as Butler et al observed in 2010, to focus on occasions where the client’s resistance was ‘embodied . . with unmarked acknowledgements (such as “mhm”) or assertions of competence’ (Butler et al., 2010: 282). But explicit objections, unlike mute resistance, require the practitioner to deal with substantial information – not just silence or hesitation and so on – in order to overcome the client’s unwillingness to follow their advice. Another difference is that they also afford the practitioner with a clue to what needs to be done to make the advice more palatable. So it’s time to swing the attention onto concrete, specific things that clients bring up, and see how practitioners deal with them. The approach we shall be taking is an ethnomethodological and conversation-analytic one, looking to see how, in the exact delivery of talk, the participants bring off the business that they are transacting with each other.
First, the background. There are a good dozen or so studies which (with one exception) while not actually making anything of the objection as such, do provide examples in the transcripts that they report for analysis. The next paragraph lists the relevant studies, which are a mix of studies of welfare helplines and medical consultations (We shall be using data published in some of these studies, along with some new data of our own, when we come to the analysis).
Previous studies The only previous study that identifies objections as such is Barton et al. (2016) .They identified two examples of what they called ‘candidate obstacles’ in diabetes consultations: that the advice would be incompatible with the patient’s lifestyle; and that the patient was ‘too busy’ to follow it. The other studies we list have reported objection-like complaints, but usually only en passant. The principal studies of this type are Butler et al. (2010) who report the client to a child health helpline saying that the advice was liable to have bad consequences, or was unfeasible (also Costello and Roberts, 2001, oncology; Niemant et al., 2020 in obstetric and gynaecological consultations); Hepburn and Potter (2011) who report clients to a child-protection helpline complaining that the advice would cause problems, be too expensive, or had already been tried; and Pilnick and Coleman (2003) who likewise report patients claiming that their physicians’ advice about smoking had already been unsuccessful. Elsewhere in the literature we find quasi-objections such as the client seeing no problem (Cohen et al., 2011, in health behaviour counselling; Connabeer, 2021, in primary care consultations; Karhila et al., 2003 in diabteic lifestyle counselling; Pilnick and Coleman, 2003, as above), the patient replying that they have already heard the advice (Bergen, 2020, in primary care consultations); the patient ‘waiting and seeing’ (Kettunen et al., 2006, in diabetic lifestyle counselling, Landqvist, 2005 example 12, in poison control helpline) or questioning the advice and offering their own alternative (Costello and Roberts, 2001, general medicine; Landqvist, 2005, example 11; Zhao and Ma, 2020, in an outpatient clinic) or simply rejecting the advice out of hand (Iversen, 2017, medical interactions in various settings; and for the earliest account, see Silverman’s, 1996 study of HIV/AIDS counselling).
Our research question
The question, then, is in two parts. First, how can we create some order in the variety of objections that have come up unsystematically in our own and others’ studies? And, more analytically, what can we say about clients’ and practitioners’ solutions to the problem that these objections pose? Does the practitioner use the material in the objection itself to tailor a rebuttal? If so, how?
Data
We shall be using some examples form the published literature in our analyses, but, because published articles don’t always show the full sequence of the talk which bears on the giving of the advice, its objection, and the subsequent work the advisor does, we shall use as our primary data calls to the Parkinson’s UK helpline. Here we have data on the entire call, allowing us to see how the client describes their problem, how the practitioner designs their advice, how it is met by an objection, and then what the practitioner does to handle it.
The Parkinson’s UK helpline
Data from this source will be what we draw on most for the detailed analysis, so a word is in order about the helpline. It is not designed to offer medical diagnoses or prescribe interventions for this neurological disease, but call-takers may give information and support. Clients contact the telephone line with for example, a medication query, a benefits query or a general Parkinson’s health-related question. For more detail on the service, and how the call-takers give advice while not overstepping their medical competence, see Bloch and Antaki (2019). All clients who gave initial verbal consent subsequently gave written consent. Recording protocols and ethics procedures were approved by the University College London Research Ethics Committees. The data examined here comprises audio-recorded telephone conversations between two specialist nurses and 30 clients – most (n = 22) are people with Parkinson’s disease with the rest (n = 8) being close family members. 1
Descriptive preamble: What kind of objection?
When we sort through a collection of objections to practitioners’ advice, harvested from our own Parkinson’s UK data and the studies referred to above, one dimension seems to jump out from the list: objections which fall squarely within the client’s own domain – things they know intimately, are under their control, and have greater entitlement to ‘own’ – versus things which are much less so, or indeed fairly obviously within the expertise and authority of the practitioner. As an example of a client-owned objection, the client might report that they’ve tried a medication (suggested by the call taker) previously and it failed; whereas if they claim that they don’t know how to get an appointment, then that falls more readily into a domain that the practitioner will know more about. We have set out a list in Table 1, glossing the actual detail of the clients’ words just for the convenience of treating them as examples of objection of these two kinds.
Epistemic spectrum of clients’ objections to advice, from what are arguably clients’ and practitioners’ epistemic domains (Examples glossed from Parkinson’s UK and transcripts published in various helpline and medical interaction studies).
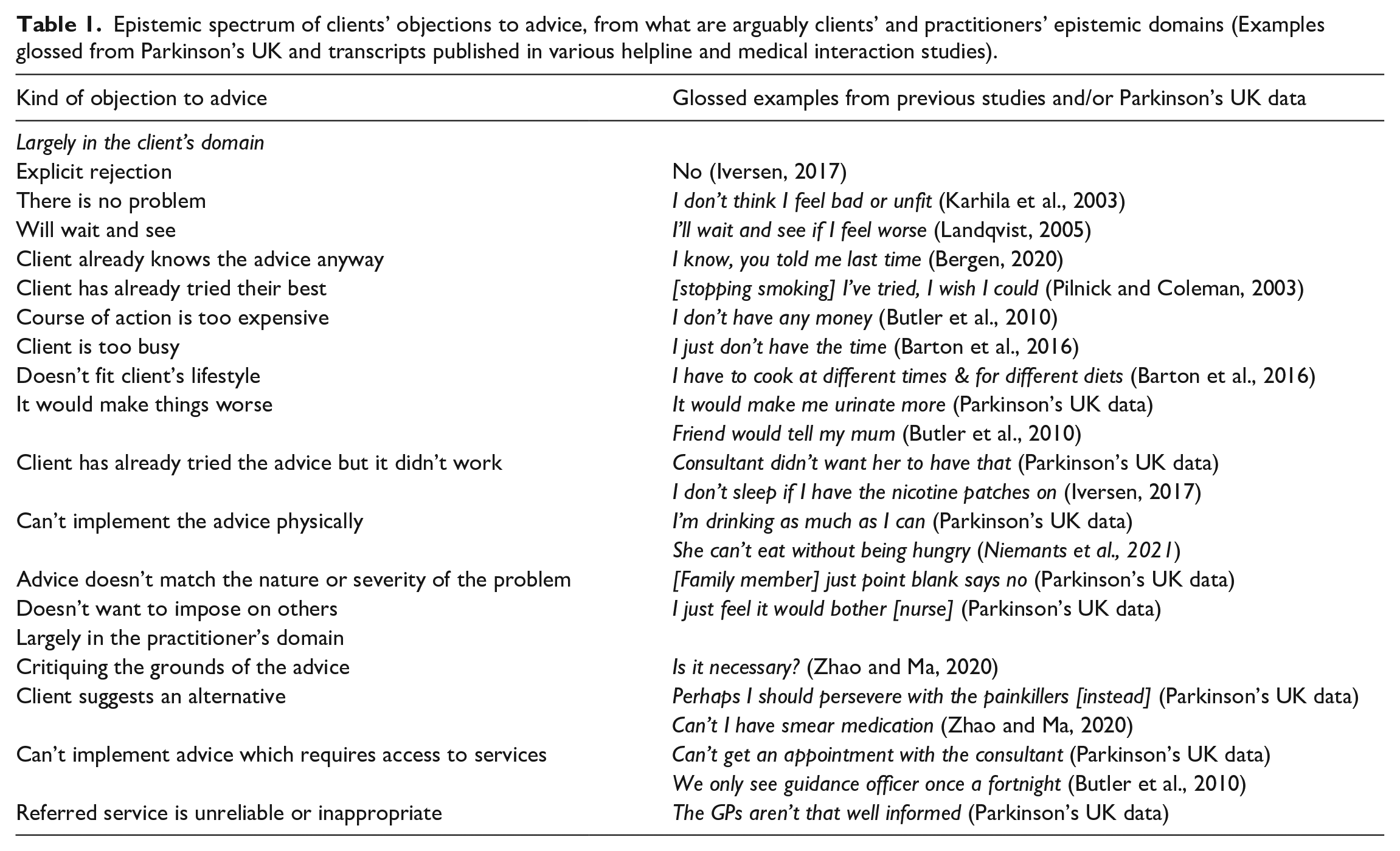
But does that apparent difference – what Heritage calls a difference in ‘epistemic status’ (Heritage, 2012), where one person has greater authority than another by dint of greater experience or expertise – actually cash out in the interaction? That is what the analysis will show.
Analysis: How did the call-takers deal with these objections? The role of epistemic entitlement
We can start with two examples to set the scene.
Consider how the call-taker reacts to these two very different objections: the problem is just getting an appointment (a bureaucratic contingency that the nurse call-taker will be very familiar with), and I have to spend a penny in the night anyway (urination at night, something the client will know only too intimately).
Example 1a. “Just getting an appointment”
Parkinson’s UK case 078
The call-taker has advised the client (in the tentative manner described in Antaki and Bloch, 2020) to see a rheumatologist (lines 210–213); but after a delay of 1 second and a minimal acknowledgement (line 215), the client raises the objection that there would be a delay even in seeing their general practitioner (GP), let alone, they imply, seeing a specialist. This bureaucracy is squarely in the call-taker’s domain of expertise; she is a nurse with long standing experience of the health system, so let us see how she finds a ready solution to the objection.
Example 1b (continues directly from 1a)
The objection is easily overcome. The call-taker assures the client of what the client can do (note the contrastive emphasis (Bing, 1983), marking her acknowledgement of the client’s objection while sidelining it) is to get the GP on the phone. Indeed, she claims, this might even be easier for the doctor (and hence more liable to succeed). This extra revelation may seal the matter; in any case, the client assents, and the talk moves on.
Consider now the difficulties facing the call-taker when the objection is firmly in the client’s experiential domain, as in example 2. The call-taker recommends drinking more water; but the client objects that she already has to get up and urinate (‘spend a penny’ in the British idiom) at night, implying that her water intake must be sufficient, or that more would mean still greater disturbance and inconvenience.
Example 2a: I have to spend a penny [urinate]
Parkinson’s UK case 073 (line 103–108)
Unlike arranging a medical appointment, a matter on which the call-taker can pull rank, the client’s problem with urination is intimately their own. The call-taker must temporise, as we shall see.
Example 2b: (follows on directly from 2a)
We see again, as we saw in line 219 in example 1b, an acknowledgement (in line 109); but then there is a disjunctive but prefacing a move away from the personal specificities of the client’s experience and onto the general ground of the (medical?) we and the overarching impersonal principle, applicable to anyone, of not getting dehydrated. The call-taker seems to have overcome the objection by this move to generality, but, unlike the case in example 1, here the objection is in the client’s domain, and extra detail of their life-world can always be provided, as they do below in line 120.
Example 2c: (follows on directly from 2b)
The call-taker had tried to move onto her own areas of expertise but the client’s insistence on their own area of entitled experience at 120 baulks them. Once again the call-taker defers to the caller, issuing yet another acknowledgement (line 122). The solution she finds out of the impasse is to restate the problem as seen by the client, making a show of appreciating their complaint by, in line 129, ventriloquising their dismay in direct reported speech (for more on such thought-reporting, see Webb et al., 2018). This affiliative move cedes ground, but allows the call-taker to pivot (line 131) on to a more medical domain, and the talk continues on her terms - objections, if not overcome, then at least bypassed.
Even this very abbreviated account of the two examples shows the differences between them: an objection on the call-taker’s turf is easily set aside, while an objection where the client has, in Heritage’s (2012) terms, primary epistemic entitlements, requires work to overcome.
Ways to concede and bring the objection onto the practitioner’s territory
The data reveal that various practices are open to the practitioner in dealing with objections that fall somewhere along the cline of epistemic priority, from those in their own domain to those in their advisees’. Basically, the objection is usually acknowledged, perhaps even conceded; then, if possible, the practitioner finds a way to bring the matter into an area of their own expertise.
We offer a list of ways the practitioner does that, based on analysis of our Parkinson’s UK data, but showing the generality of the practices by giving examples taken from interactions noted in other studies (listed above) where the original transcriptions allow. We set them out as a crude list, but, of course, they can be mixed together; and, indeed, we’ll see that concession is a useful preface for at least three of the others.
(a) conceding the objection’s validity but moving on;
(b) proposing a ‘work-around’ that effectively repeated the original course of action by different means;
(c) selecting an aspect of it that could be remediated;
(d) correcting and minimising the client’s understanding of the challenges or costs of the advice; and
(e) stressing the importance or urgency of the original course of action.
Analytically, we shall try and bring out how it is that, in all these practices, the practitioner manoeuvres (if possible) the objection onto their own grounds, while orienting to the client’s epistemic rights.
Conceding the validity of the objection
Concession, though occasionally noted by previous analysts, seems to play a systematic part in prefacing responses to objections. We have already seen it in the examples above: in example 2b, line 109 ‘I know’, example 2c ‘right yeh erm (.4) that that can occur’; and even when the objection was in the call-taker’s domain, there was an implicit acknowledgement (‘I think what you can do. . .’) of the client’s troubles. Concession can preface either a withdrawal of the advice or a side-ways move to re-issue it in different terms, as the call-taker does in Example 1. In both cases, its explicit acknowledgement of the client’s rights repairs the rupture in affiliation temporarily caused by the objection.
In this example from case 069, the call-taker has advised the client to ask their GP to inform the consultant of changes in the patient’s symptoms.
Example 3 Parkinson’s UK case 069
The client objects (lines 110–111) that this hasn’t worked before (I thought that would’ve happened). The call-taker affiliates with a news receipt and what seems to be a concessionary assessment (oh no) affirming the negativity of the client’s experience (see Heritage on Oh-prefaced responses to questions (Heritage, 1998, but more generally Heritage, 2002). But she then immediately reasserts the advice in general, impersonal terms as a matter of modal necessity (lines 119–124). Concession can be seen more dramatically in this next example, from the study by Cohen et al. (2011).
Example 4 (Cohen et al., 2011, p 11) (transcription as in original)
The practitioner issues what of what Butler et al. (2010) call advice-implicative questions.
It implies, as Butler et al argue, that the client ought to eat less, or less bad things; but the client’s objection (line 2) is squarely in terms of their own wants and desires. Note the call-taker’s concessionary retreat in the face of the client’s unassailable epistemic entitlement; this is one of the few cases where the practitioner is baulked. This might be due to the fact that the advice was unsolicited; we shall return to that later.
Reissuing the advice in a work-around
A very common practice by the call-taker was to acknowledge or concede the objection, and then to re-issue it in a different form. We have already seen that in the Parkinson’s call-taker re-issuing the advice to make an appointment with the consultant via the client’s GP (see example 1, above). In this next example, the practitioner is again on their own epistemic ground.
Example 5. Parkinson’s UK case 073
The client’s objection at 211 is met with a confirmatory negative (Heritage and Raymond, 2021) at line 213 which prefaces an immediate workaround by recommending a different person to see – one who, cementing the call-taker’s knowledge of the scene, can ‘provide just as much if not more’. Here is another case of a work-around, from a different data-set.
Example 6 Barton et al. (2016) p 1160 (transcription as in original, line numbers and boldening added)
Again the practitioner’s acknowledgement (including the non-lexical ‘tut’, hearable perhaps as sympathetic (see Keevallik and Ogden, 2020 for an interactional account of such vocalisations in general) prefaces the alternative course of action in line 9; it is the same advice to take exercise, altered only to a more convenient time.
Selecting an aspect of the objection that can be reformulated
As with formulations (Heritage and Watson, 1979), restatements of the objection can edit out the irremediable parts and leave something that the call-taker can deal with. In this example, the call-taker has advised that the client see their GP, only to be told that the GP ‘never does anything without getting any correspondence for the hospital’, in a designedly extreme-case (and, as Edwards, 2000 notes, therefore unassailable) description. However, on home epistemic ground, the call-taker can rework the client’s objection in such a way as to take the wind out of their sails.
Example 7
Parkinson’s UK case 099 line 84
The call-taker issues the now-familiar acknowledgement on line 93, and then on lines 95 restates the client’s problem in a way that grants her the opportunity to provide a bureaucratic solution - it’s not that they need to ask for a change of medication as such, so much as a simple change to a propriety rather than the generic brand. She then proceeds without the objection resurfacing.
Correcting and minimising the client’s understanding of the challenges or costs of the advice
A client may object to the course of action on the basis that they would find it too challenging or costly, and although that seems to be a matter of their own competence or abilities (and therefore in their own epistemic domain), the practitioner can tailor the course of action to remove its more demanding elements, as in the example below, where the advice is to profit from an information leaflet.
Example 8 Parkinson’s UK case 114
But although the practitioner can edit the advice, the client is nevertheless able to resist again, this time upgrading the incapacity from the implicit worry of line 12 to an explicit assertion (line 16) she would ‘get lost in it all’.
Here is an equivalent example from a medical consultation. The client reacts to the advice to drink water (line 2–5) with a response cry and the objection that ‘stomach big’ and they ‘don’t feel better’.
Example 9 Niemants et al. (2021) ‘OBSf’ is a female obstetrician, ‘PATf’ a female patient. Neither has English as their first language. Lines renumbered and boldening added.
Clearly, the client is uniquely entitled to report the bad effects of the advice; nevertheless, again after the initial acknowledging ‘yes’ (line 10) the practitioner can adjust the dosage, as it were, and re-issue the advice in more acceptable form.
Stressing the importance or urgency of the original course of action
The practitioner can trump an objection by stressing the importance or indeed the urgency of the course of action, on the basis of the practitioner’s acknowledged expertise. In the next example, the client objects (lines 162–165) that they can’t rely on the GP and psychiatrist to work together.
Example 10 Parkinson’s UK Case 069
The client’s objection (162–165) seems to index a personal frustration with the service that they’re receiving. The practitioner orients to the frustration (167–169) but deletes it in favour of stressing the medical benefits of the advice (169 and ff.)
Perhaps the most unilateral display of the practitioner operating from a position of strength is when the matter is urgent and clearly both in the practitioner’s expertise, and to the client’s advantage. Example 11 below comes from a poisons helpline:
Example 11 (Landqvist, 2005: 230) Original with Swedish and English translation; only the English given here. “Ph” is the pharmacist. Boldening added.
The pharmacist does give the client time to withdraw the objection, and there is a hint that they might be doing so in 184; but equally, the abandoned sentence might be ‘so it should settle down’ or words to that effect. In any case, after a further gap of 1 second, the practitioner makes a unilateral judgement that rides roughshod over the objection. After all, it was the client who called for advice about what to do after ingesting something potentially lethal.
Solicited and unsolicited advice
The last example above suggests that advice which the client has not themselves solicited may be easier for them to object to, and make their objections carry. If we look at our collections of objections through that lens, we do indeed find that there seems to be some connection. Consider the first six objections that we listed in Table 1 above: No (Iversen, 2017); I don’t think I feel bad or unfit (Karhila et al., 2003); I’ll wait and see if I feel worse (Landqvist, 2005); I know, you told me last time (Bergen, 2020) I’ve tried, I wish I could. (Pilnick and Coleman, 2003); and I don’t have any money (Butler et al., 2010).
The only time the client is overruled is in example 11 from Landqvist (2005), when the pharmacist had to come down heavily on the client’s objection when it was literally a matter of life and death. Otherwise, it does seem that the practitioner is on the back foot, and it is the client’s objection which wins the day. Recall, for example, that in the example we saw (as Example 4) from Cohen et al, when the practitioner hints that they should ‘watch their diet’, the client was able to simply assert, and then re-assert that they would eat what they wanted to eat; and such was the strength of their position, they could even jocularly challenge the practitioner to ‘get them to lie’.
There isn’t space to give the whole transcript, but we can give a gloss for another example from Iversen (2017) which shows the licence that the client has, when the ball is in their epistemic court, even in the face of a direct injunction from the practitioner.
Example 12 Iversen (2017) p.12 (from the English translation of the Norwegian)
Although the practitioner has put their advice in the most directive of ways possible, with the unilateral imperative you have to quit, the client has given a bald no and followed it up with their own, subject-side assessment (Edwards and Potter, 2017) of their situation, brooking no argument.
Discussion
We set out to look at the way in which clients raised objections to medical and welfare advice, and how practitioners dealt with them. We first made a list of examples from our own data and from previous studies, and noticed a distinction between an objection which would be in the client’s epistemic domain (such as I’ve tried it and it didn’t work), and one which, although experienced by the client, would yield some authority to the expertise of the practitioner (such as it’s difficult to get an appointment). The first kind have the weight of the service-user’s life-world, blocking the advice with material worries that only the client knows intimately. But the second allows the practitioner to wield their authority.
Our analysis showed that this did indeed happen, but that the practitioner took pains, even when dealing with objections they could easily overcome, to maintain affiliation with the client, perhaps orienting to the moral dimension to advice, as Shaw and Hepburn (2013) find in family advice-giving. It was common in the data we analysed here for the practitioner to acknowledge an objection, at least minimally, perhaps even conceding it, before pulling it onto territory that they better controlled. We saw the practitioner proposing workarounds, selecting an aspect of the objects that could be reformulated, and correcting the client’s understanding of the advice. It was only when the matter could be classed as imminently dangerous (requiring, for example, immediate hospitalisation to treat a poison) that we saw the practitioner forswear concession and invoke the urgency of the advice to push it through.
We may also add that concession will matter to the participants because most of the issues raised, at least those we have examined, are in the context of a chronic disability where the client is often having to make decisions about their health and wellbeing (or that of a family member), extending far beyond the merely medical domain. The problems raised are real, are distressing, and have already generated enough difficulty to prompt advice seeking from a professional. For the call-taker to be effective, they don’t necessarily need their advice to be agreed to; but they do need their advice to be understood and to be treated as credible. Conceding the client’s perspective, particularly their challenges to advice given, both attends to the importance of affiliation and the therapeutic alliance which is growing in influence in some quarters (see, for older adults with neurological disorders, Portacolone et al.’s, 2020 call for medics’ greater communicative co-operation with patients).
It is worth giving some brief consideration, in the space that remains, to the dimension of advice that we addressed only tentatively, and as something of an afterthought in this paper: the difference between objecting to advice which comes unsolicited, and advice for which the client has actually asked. A troubled client who rings a support helpline with a question about what to do is clearly and manifestly expecting to be given advice. On the other hand, a patient who has attended a primary care consultation on a routine matter may be surprised if the doctor starts quizzing them about, for example, their smoking (as in the study by Pilnick and Coleman, 2003). In either case, the client may have reasons to raise an objection to the advice the practitioner gives, but in the latter case, where the client hasn’t even asked for it, the practitioner may have a harder task in overcoming it. If we want a theoretical handle on that, then we can consider who is the ostensible beneficiary of the advice (Clayman and Heritage, 2014) or who it is who has what Potter et al. (1993) called a stake and interest in the matter. The institution has a stake in its advice being taken, and there will be varying degrees of pressure for the practitioner to make sure that it is (to get the case closed, the call terminated, and so on); and it may well be that in some cases, at least, their interests and those of their clients do not coincide. Professionals’ advice giving, and clients’ objections against that advice, may be a battleground of competing entitlements.
Footnotes
Acknowledgements
The authors are indebted to Emma Richardson for very helpful comments on an earlier draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.