
Abstract
This cross-sectional study utilises an explanatory-sequential, mixed-methods design, using quantitative surveys (N = 275) and semi-structured interviews (N = 17) to explore the psychological impacts of investigation type on a sample of UK police senior investigating officers (SIOs). Prevalence rates of post-traumatic stress disorder (PTSD) (5.4%) and complex post-traumatic stress disorder (CPTSD) (4.1%) are also established. Analyses demonstrate that organisational stress (B = 1.15), experiencing trauma 6 to 12 months ago (B = −1.72) and child homicide investigations (B = 1.76) predict PTSD, whereas operational stress (B = 1.82), experiencing trauma 6 to 12 months ago (B = −1.45) and 10 to 20 years ago (B = 3.92) predict CPTSD. Child homicide is the only investigation type to predict all three PTSD symptoms, while adult homicide predicts lower re-experiencing (B = −1.50) and sense of threat (B = −1.07). The qualitative analysis suggests that although SIOs may become more resilient to traumatic experiences through coping processes of avoidance and detachment, this career-long experience of trauma exposure leads to psychological vulnerability. Supporting the quantitative findings, increased PTSD resulting from child homicide investigations appears to be related to levels of personal resonance. Many SIOs that maintained it is not any particular type of investigation, however. It is thus argued that the relationship between child homicide and PTSD is influenced by Lazarus and Folkman's concept of ‘centrality’. The practical findings of this paper are discussed, and implications for police practice and supporting officer well-being moving forward are considered.
Introduction
It has been suggested that 80% of police have encountered what could generally be considered a traumatic event as part of their work (Brewin et al., 2022), such as attending the scene of a road traffic collision or investigating a sudden and unexplained death (Roach et al., 2017, 2018). Brewin et al. (2022) further suggest that 20% of police officers in the UK may have clinical levels of post-traumatic stress disorder (PTSD) or complex post-traumatic stress disorder (CPTSD). A systematic review by Sherwood et al. (2019) identified several individual, organisational and operational risk factors for PTSD, including: female sex; specific personality traits; passive, emotional and avoidant coping; lack of support; lack of control and higher job stress; high workload; cumulative exposure; and threats to life. UK police-focused research has identified how different roles can negatively impact police well-being; how police culture remains a significant influence on the relationship between role, stress and trauma; and importantly, individual ways and methods for dealing with stress and trauma, particularly peer support. Indeed, social support has been constantly identified as one of the most important post-trauma factors for coping and maintaining police well-being, including peer and organisational support (Foley and Massey, 2021). Other studies (Foley and Massey, 2021; Maguire and Sondhi, 2024) also identify the emotional investment that officers commonly direct towards victims of crime as having a very real and potentially negative impact on police in terms of provoking feelings of stress and/or trauma; for example, when supporting the family of a missing person, or having to convey to a family the death of a loved one after a road traffic collision. However, one particularly unexplored role, is that of the senior investigating officer (SIO) (Curran, 2024) in serious and complex criminal investigations.
In 2003, the College of Policing (2018: 5) introduced the Professionalising Investigations Programme (PIP), intended to ‘deliver registration, examination, training, workplace assessment and accreditation to a national standard at each level’ that ‘provides a structured and consistent development and maintenance programme for investigative skills’. There are four levels of qualification: PIP1, priority and volume crime investigations; PIP2, serious and complex investigations; PIP3 (SIO accreditation), management of major and serious organised crime investigations; and PIP4, SIOs who are responsible for the strategic management of highly complex investigations (College of Policing, 2018). A prospective SIO must complete the SIO development programme consisting of either (or both) a ‘major crime’ or ‘serious and organised crime’ learning module, portfolios and subsequent panel discussions. Registration is then maintained on an annual basis (College of Policing, 2018).
This paper builds on a currently emerging area of police well-being research by exploring whether, when and how, SIOs leading different types of criminal investigation might experience PTSD and CPTSD symptoms. This is done by reporting the findings of an electronic survey completed by 275 UK SIOs, which then supported the construction of a further study comprising 17 semi-structured interviews with UK SIOs, to identify lived experiences.
Literature review
The essential features of a PTSD diagnosis according to the International Classification of Diseases 11 are: ‘Exposure to an event or situation (either short- or long-lasting) of an extremely threatening or horrific nature’ and developing a characteristic syndrome consisting of the following symptom clusters: re-experiencing, deliberate avoidance and heightened threat (World Health Organization, 2022). CPTSD differs from PTSD in that it must occur as a result of a series of ‘extremely threatening events’ such as torture, slavery, genocide, domestic abuse or repeated childhood sexual abuse. As well as meeting PTSD criteria, CPTSD is marked by severe and persistent ‘problems in affect regulation; beliefs about oneself as diminished, defeated or worthless, accompanied by feelings of shame, guilt or failure related to the traumatic event; and difficulties in sustaining relationships and in feeling close to others’ (World Health Organization, 2022).
Most extant police well-being research consistently points to police officers and staff being at high risk of encountering a traumatic event in their routine duties. Although other occupations are also identified as being high risk – for example, paramedics, soldiers and nurses – those working in the diverse roles and tasks within policing have become a particular focus for research. Studies have evidenced that 80% of police officers have been exposed to trauma in their role (Brewin et al., 2022; Hartley et al., 2013). Compared with non-policing samples in the UK, approximately one-third of adults in England reported experiencing at least one potentially traumatic event during their lifetime (National Health Service, 2014). Moreover, police officers are likely to undergo repeated exposure to potentially traumatic situations (Foley and Massey, 2019). These repeated exposures can manifest in CPTSD, which has greater implications than PTSD for daily functioning and mental health (Foley et al., 2022; Violanti et al., 2017). However, while the frequency of trauma exposure is consistent across studies, prevalence rates for PTSD and CPTSD are not. The purpose of the current paper was to focus specifically on PTSD and CPTSD in a sample of UK SIOs.
Estimates of PTSD and CPSTD in police officers vary significantly. In the UK, 26% of police officers working with victims of child abuse, rape and sexual exploitation had possible PTSD (Foley et al., 2022), and Brewin et al. (2022) estimated prevalence rates of 8% and 12% for PTSD and CPTSD respectively in a sample of UK officers. This is contrasted against a prevalence rate of 4% in Stevelink et al. (2020). For female UK police officers, prevalence rates were in fact lower (3.74%) than for the general population (Irizar et al., 2023). Reasons for the discrepancies across studies are argued to be due to a combination of sampling bias, framing effects and the use of different psychometric scales (Stevelink et al., 2020).
Consideration has been given to the impact of different roles in policing, and their relationship to trauma frequency, severity and impact on symptomology (Hesketh and Tehrani, 2019). In their review, Cartwright and Roach (2022) cover general investigations (e.g. burglary, motor vehicle theft), child abuse and child sexual exploitation, and crime scene investigation. It is suggested that child homicide is one of the most emotionally challenging and traumatising investigations (Roach et al., 2017, 2018). Although their research started to consider the impact of different types of investigations, Roach et al. (2017, 2018) did not include psychometric measures of well-being, stress or trauma. The idea that role is an important factor has been developed by Foley et al., and investigations involving children are a recurring theme in the literature (Foley and Massey, 2021; O’Brien et al., 2024).
Sheard (2019) highlights that those police working on ‘response’ often have the highest levels of stress, burnout and secondary traumatic stress (STS) compared with those in other roles, such as communications, firearms, crime, and child and adult safeguarding. Similarly, Curran (2021) demonstrates the unique stressors involved in covert and undercover policing. MacEachern et al. (2019) and Gray and Rydon-Grange (2020) demonstrate the impacts of working with victims of sexual violence and child abuse. However, their research found generally low levels of STS. More recent research expands on this, noting a ‘burnout cascade’ effect (Sondhi et al., 2025), often compounded by high job demands and low resources (Maguire and Sondhi, 2024). In an interesting comparison piece, Brown et al. (1999) found that the most impactful investigations were (in decreasing order): disaster body recovery; being shot at; witnessing a colleague’s death; fatal road collision; cot death; serious injury; accident body recovery; and child fatal road collisions. Miller et al. (2022) found that the most frequently reported ‘worst traumatic events’ tend to involve children (fatalities, abuse and sexual exploitation); sudden death, including murder; and road traffic collisions. The most frequently cited situational contexts were gruesome experiences (such as gore and mutilation); organisational pressure; cumulative exposure, personal resonance, first on scene and victim vulnerability.
Although research to date has begun to identify and explore the impact of role, investigation type and the potential negative effects on investigator well-being (including trauma), it is, to our knowledge, yet to focus on the intersection of all three. The current paper seeks to address this gap in the literature, by looking at how investigation type can impact on the well-being of SIOs.
Research design
This cross-sectional study used an explanatory-sequential, mixed-methods design (Creswell and Plano Clark, 2017). The survey findings influenced the direction of the interview questions, helping to focus on important relationships. The interviews further sought to explain the quantitative findings. The research set out to understand primarily whether investigation type is associated with PTSD and CPTSD (and symptoms); whether there are differences between male and female SIOs’ PTSD and CPTSD scores; and whether there are differences according to PIP level. The qualitative method sought to understand the underlying processes and relationships between the above (Creswell and Plano Clark, 2017). Ethical approval for the survey and the interviews was sought and granted in 2021.
Study 1: Electronic survey
Participants
A simple random sampling strategy was adopted, in which an electronic survey was distributed by the College of Policing to all officers and staff on the PIP register (Census) in April 2021, running until June 2021. This includes those under assessment, PIP3 and PIP4 (or equivalent) accredited officers across England, Wales, Police Scotland and Police Service of Northern Ireland. Those who were PIP2, but not under assessment were not eligible. To mitigate non-response bias, communications were sent out four times following publication of the survey. SIOs who had completed the quantitative survey were invited to email the lead researcher at the end of the questionnaire.
In total, 372 responses were recorded; however, 97 had to be excluded because they were incomplete, leaving 275 responses remaining. This equates to an approximate response rate of 28%, from a population of approximately 1000 SIOs. The full breakdown is presented in Table 1.
Survey sample personal and occupational demographics.
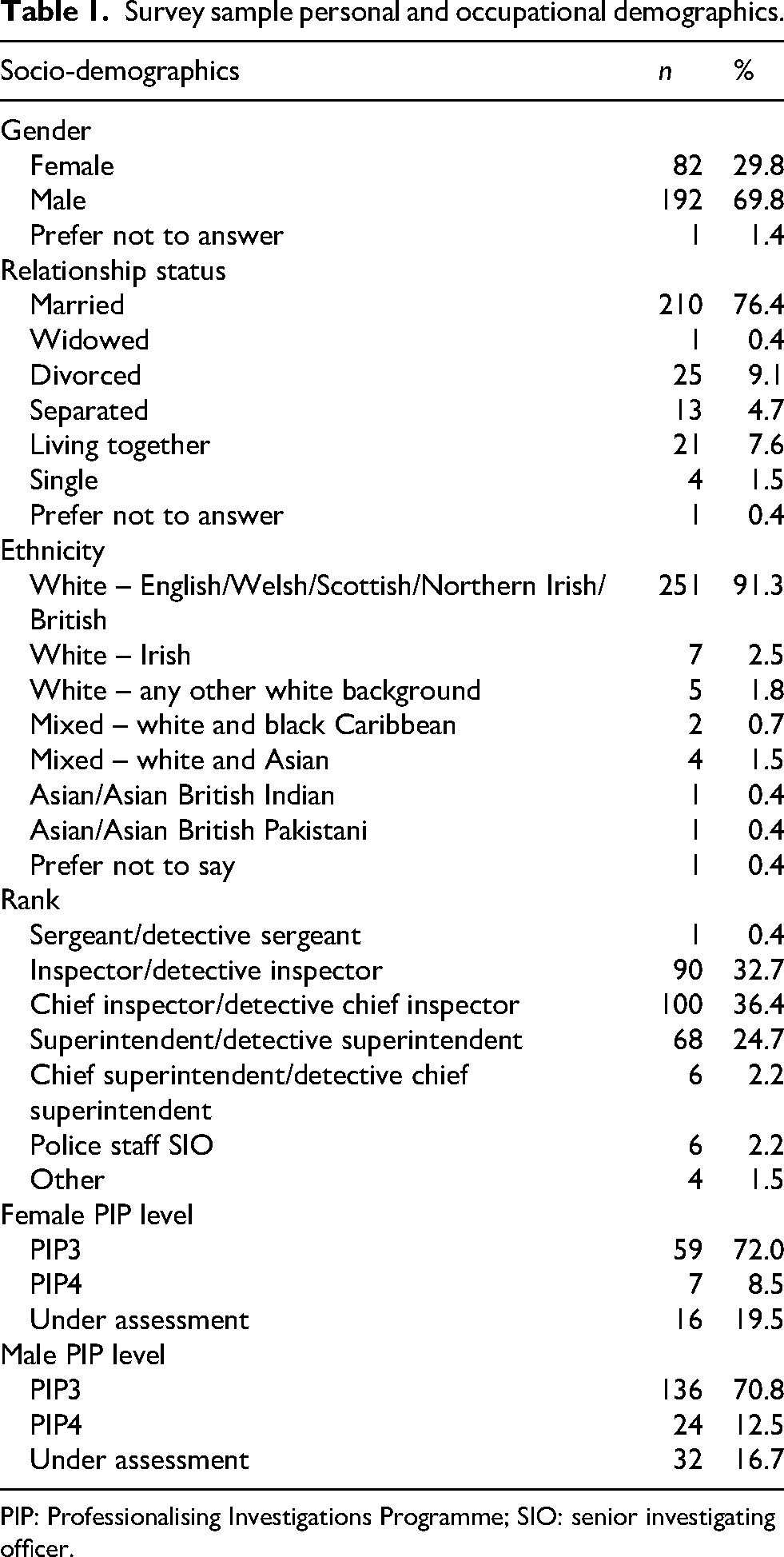
PIP: Professionalising Investigations Programme; SIO: senior investigating officer.
Measures
The quantitative survey used several validated psychometric instruments to measure police stress, anxiety, depression, PTSD and CPTSD. The instruments include the Police Stress Questionnaires (Organisational (PSQ-Org) and Operational (PSQ-Op)) (McCreary et al., 2017; McCreary and Thompson, 2006) and the International Trauma Questionnaire (ITQ) (Cloitre et al., 2018). Participants were not informed of their survey results, because the principal researcher at the time of data collection was not a qualified psychologist.
The PSQ comprises 40 items; however, following consultation with the National Police Chiefs Council Homicide Working Group, an item was added to the scale; to reflect stress resulting from ‘on-call’ duties (whereby an officer is expected to respond to incidents outside their rostered shift). Both the PSQ-Org (α = .89) and PSQ-Op (α = .93) demonstrated very good and excellent reliability. For the PSQ-Op and PSQ-Org, items were measured on a 5-point scale and summed.
The ITQ (Cloitre et al., 2018) is a clinical diagnostic tool for providing diagnosis of PTSD and CPTSD based on symptom clusters, as well as total scores. Clinical indicators of PTSD are re-experiencing (e.g. upsetting dreams that replay the experience), avoidance (e.g. avoiding external reminders of experience) and a sense of current threat (e.g. feeling jumpy or easily startled). These must be combined with an element of functional impairment; for example, affected work or ability to work. CPTSD is indicated by the presence of PTSD, but also disturbances in self-organisation: affective dysregulation (e.g. feeling numb or emotionally shut-down); negative self-concept (e.g. feeling worthless); disturbances in relationships (e.g. feeling distance or cut off from people), in combination with functional impairment (e.g. creating concern about relationships or social life. Items are measured on a 4-point scale. PTSD and CPTSD prevalence are calculated through the presence/absence of symptoms (diagnostic), whereas PTSD and CPTSD scores (for regressions) are summed ordinal symptom values (dimensional). The PTSD (α = .90) and CPTSD (α = .87) scales of the ITQ represent excellent and very good reliability, respectively. Other variables measured in the quantitative analysis comprised demographics, including personal and occupational data, such as rank and years of police service.
Procedure
Statistical analyses were conducted using the IBM Statistical Package for the Social Sciences (SPSS) version 28, R and RStudio, and utilising the WRS2 package (Mair and Wilcox, 2020) to conduct robust t-tests and analyses of variance (ANOVA). Bootstrapping (1,000) techniques were used to estimate confidence intervals (CI), and trimming (20%) was used to reduce the influence of outliers. Regression analyses were conducted using SPSS, with the PROCESS tool (Hayes, 2018), for estimating robust unstandardised beta coefficients, utilising heteroskedasticity-consistent standard errors, and percentile-bias corrected bootstrapped CIs.
Analysis
Prevalence of trauma
The analysis indicates that 80% of the sample have experienced a potentially traumatic event. Some 84.9% of male SIOs indicated that they had experienced a potentially traumatic event, in comparison with 70.7% of female SIOs. There were statistically significant associations between gender and experiencing a potentially traumatic event χ2 (1, n = 253) = 7.62, p = .006, V = .17. Overall, 5.4% of those asked met the clinical threshold for PTSD, and 4.1% met the clinical threshold for CPTSD. Prevalence is higher among male SIOs: 6.9% and 4.6% of those completing the ITQ met the clinical thresholds for PTSD and CPTSD respectively, compared with 1.5% and 3.1% of female SIOs meeting diagnostic thresholds.
Factors influencing trauma symptomology
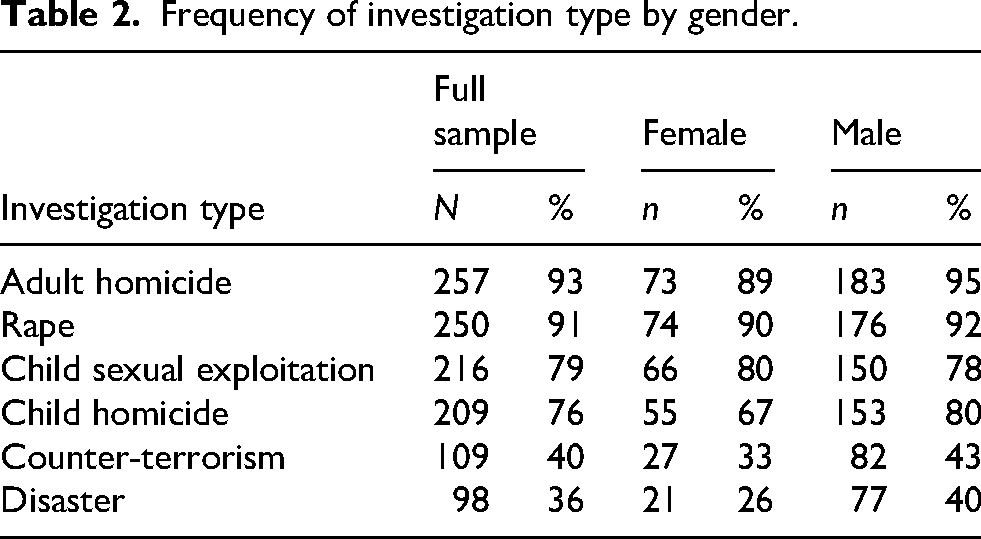
Table 2 provides the proportion of male and female officers who have been involved in each type of investigation. There were statistically significant associations between gender and the type of investigation conducted: child homicide χ2 (1, n = 262) = 4.77, p = .029, V = .13; and disaster investigation χ2 (1, n = 262) = 4.52, p = .034, V = .14. The results suggest that, except for child sexual exploitation investigations, male SIOs more frequently investigate serious and complex offences; however, only child homicide and more disaster investigations were statistically significant.
Frequency of investigation type by gender.
Robust one-way ANOVAs were conducted on mean differences for PTSD and CPTSD across PIP levels (Table 3).
PTSD and CPTSD mean differences by PIP level.
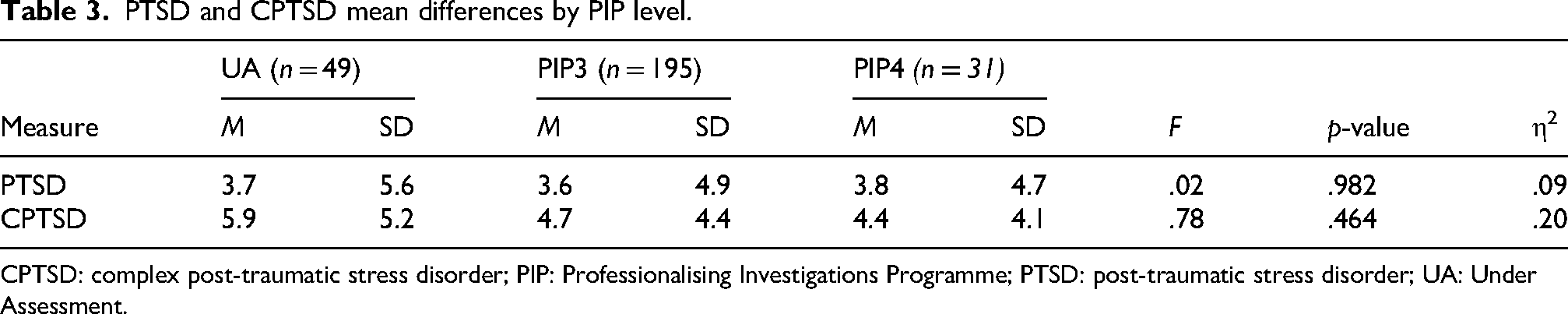
CPTSD: complex post-traumatic stress disorder; PIP: Professionalising Investigations Programme; PTSD: post-traumatic stress disorder; UA: Under Assessment.
The analysis revealed no statistically significant differences; however, those under assessment have the highest levels of CPTSD, but the lowest levels of PTSD. The results suggest that PTSD increases as SIOs move from being under assessment to PIP4, which would be consistent with the view that SIOs accumulate increasing levels of trauma. However, given that the reverse is true for CPTSD, the relationship becomes unclear. This could be an artefact of the fact that CPTSD is characterised by increasing levels of symptomology, and has greater implications for an SIO’s well-being, and their psychological functioning. This may, therefore, represent a ‘drop off’ effect, in which repeated exposure to traumatic events supports an accumulation effect.
Next of interest were gender differences on PTSD, CPTSD and their respective symptom clusters. Robust t-tests with boostrapped confidence intervals were conducted to test group differences, and the results can be found in Table 4.
PTSD and CPTSD symptom mean differences by gender.
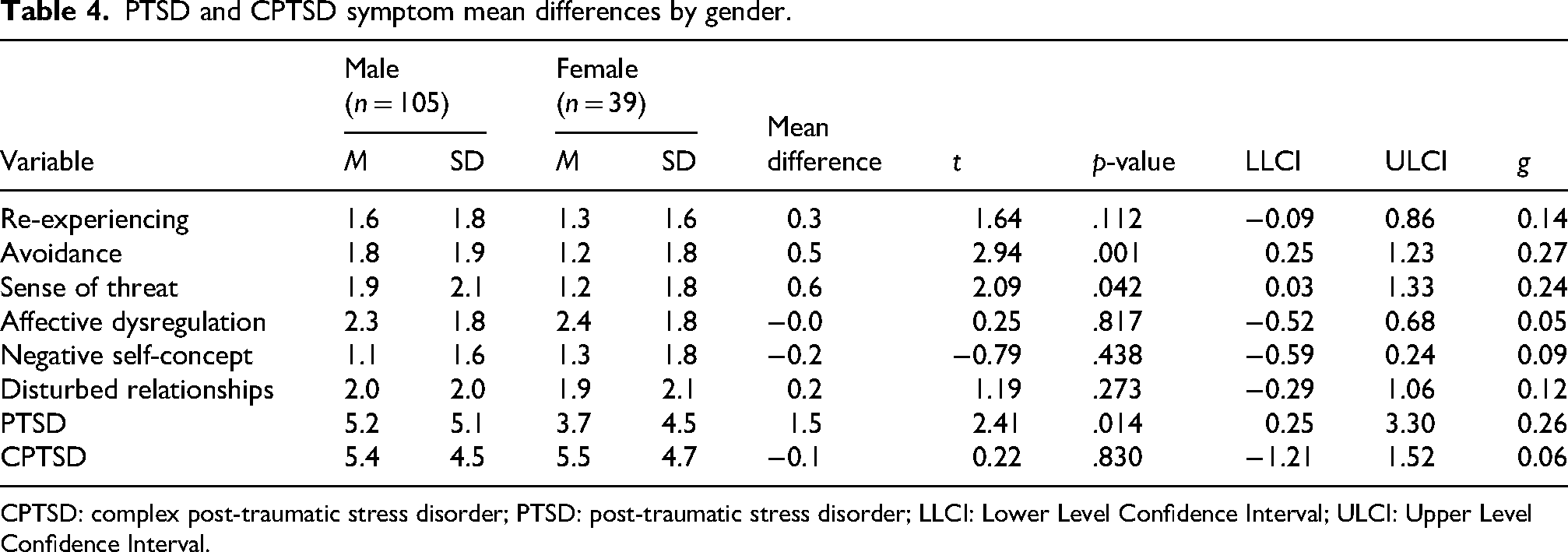
CPTSD: complex post-traumatic stress disorder; PTSD: post-traumatic stress disorder; LLCI: Lower Level Confidence Interval; ULCI: Upper Level Confidence Interval.
Analysis demonstrates that male SIOs scored higher on the avoidance and sense of threat clusters than their female counterparts. Although male SIOs tended to report higher scores on all measures (except for negative self-concept), this suggests that male SIOs are at a greater risk for PTSD than female SIOs.
Spearman's rho correlations were computed to test the relationship between length of service, hours worked per week and all the trauma-related variables. There were no statistically significant relationships between length of service and the trauma variables, therefore these were not entered into subsequent regressions.
Multiple linear regression analyses were conducted to see whether PTSD, CPTSD and PTSD symptom clusters could be predicted by several variables. Given the presence of heteroscedasticity, standard errors (SE) were calculated with bootstrapped CIs. The null hypothesis being tested is that there is no relationship between PTSD/CPTSD scores, operational and organisational police stress, time since experiencing a potentially traumatic event, and investigation type. The latter two sought to explore Roach et al.'s (2017) finding that there is a negative relationship between time since last investigation and well-being.
The model predicting PTSD was significant, F(14, 217) = 5.00, p = <.001, SE = 4.48. The model predicting CPTSD was also significant, F(14, 217) = 8.03, p = <.001, SE = 3.88. The full coefficients can also be found in Table 5.
Regression predicting total PTSD and CPTSD scores.
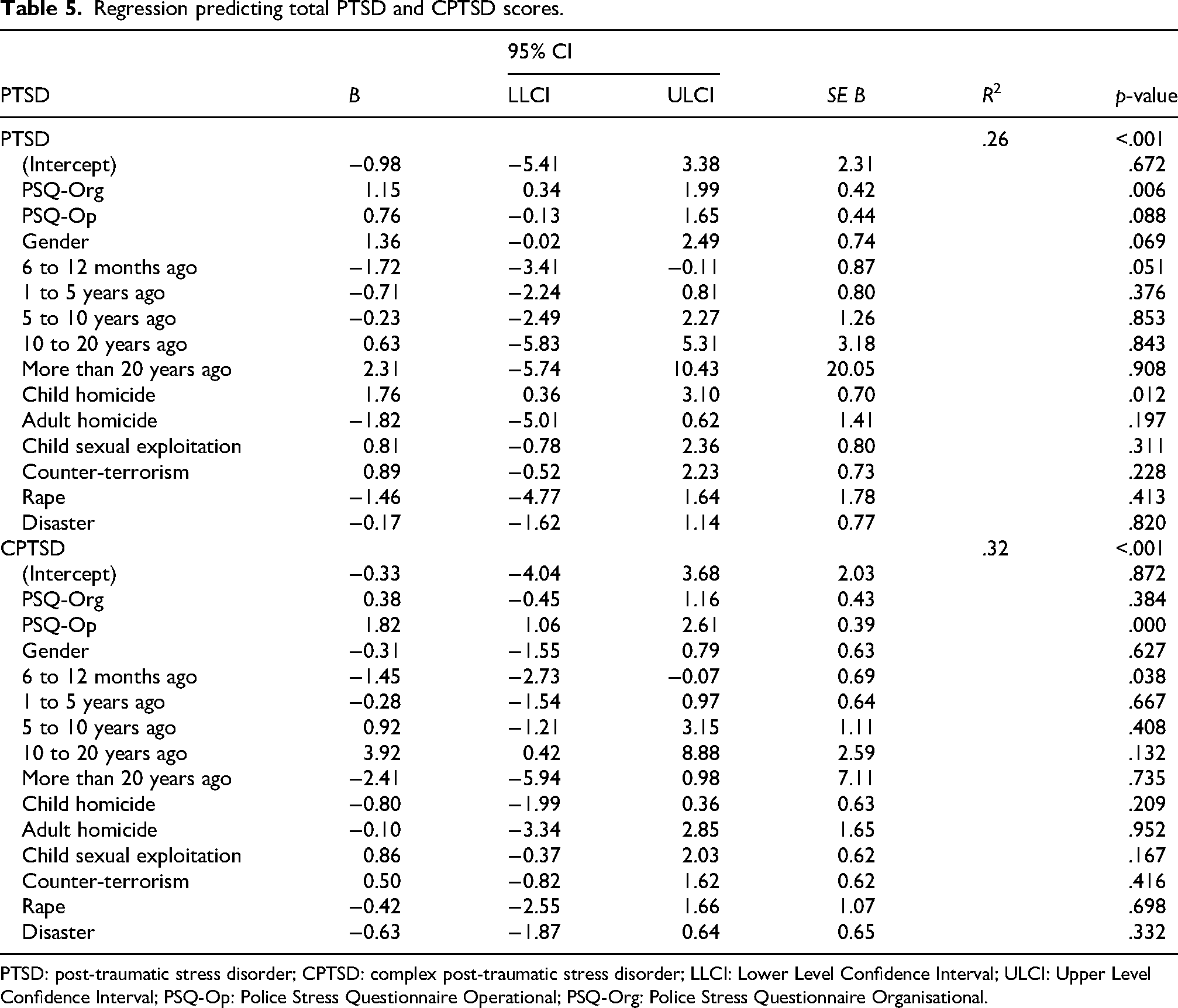
PTSD: post-traumatic stress disorder; CPTSD: complex post-traumatic stress disorder; LLCI: Lower Level Confidence Interval; ULCI: Upper Level Confidence Interval; PSQ-Op: Police Stress Questionnaire Operational; PSQ-Org: Police Stress Questionnaire Organisational.
Bootstrapped CIs show that organisational police stress, 6 to 12 months ago, and child homicide investigations predict PTSD scores. Interestingly, operational police stress does not predict PTSD scores. Investigating adult homicide and rape is associated with lower PTSD scores. Albeit the CIs do not cross 0. Regarding CPTSD, operational police stress and experiencing trauma ‘6 to 12 months ago’ (compared with less than 6 months ago) negatively predict CPTSD. Experiencing trauma 10 to 20 years ago is positively associated with CPTSD. The change from negative, to positive, and back to a negative relationship indicates a curvilinear relationship. This is expanded upon in the qualitative findings.
Finally of interest was the relationship between investigation type and PTSD symptoms – gender and all investigation types were entered into the model. The model predicting re-experiencing was significant F(7, 224) = 3.72, p = <.001, as was the model predicting avoidance F(7, 224) = 2.63, p = .013, and sense of threat F(7, 224) = 2.65, p = .012.
The analyses in Table 6 support previous research (Roach et al., 2017, 2018) showing child homicide as the most important predictor of all PTSD symptoms in SIOs. However, results show that adult homicide investigations predict lower re-experiencing and threat symptoms, while male gender predicts an increased sense of threat. Nevertheless, the results lend strong support to the idea that child homicides have greater negative impacts on SIO well-being, as shown by previous research (Roach et al., 2017, 2018).
Predicting PTSD symptom cluster scores by gender and investigation type.
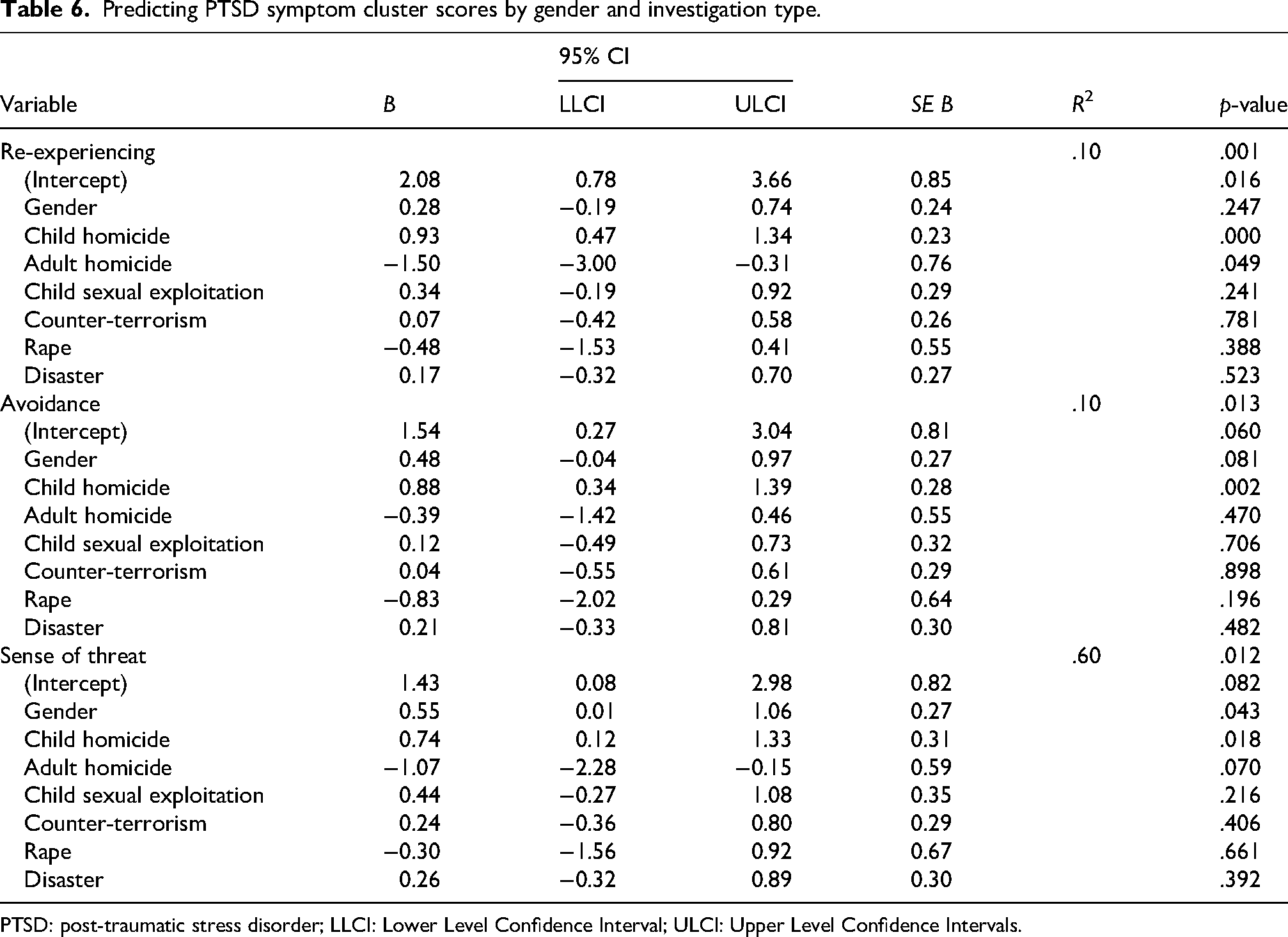
PTSD: post-traumatic stress disorder; LLCI: Lower Level Confidence Interval; ULCI: Upper Level Confidence Intervals.
Study 2: Semi-structured interviews
This section reports the findings of reflexive thematic analysis (RTA). This is done by utilising supporting themes and extracts that can help researchers understand the potential relationships between.
Participants
Semi-structured interviews were conducted with 17 SIOs following on from the survey in 2021. Interview participants were primarily recruited from the survey; however, because of the lower number of female SIOs, purposive sampling was conducted to invite a further two female officers. The full demographics of the interview participants is in Table 7.
Interview sample personal and occupational demographics.
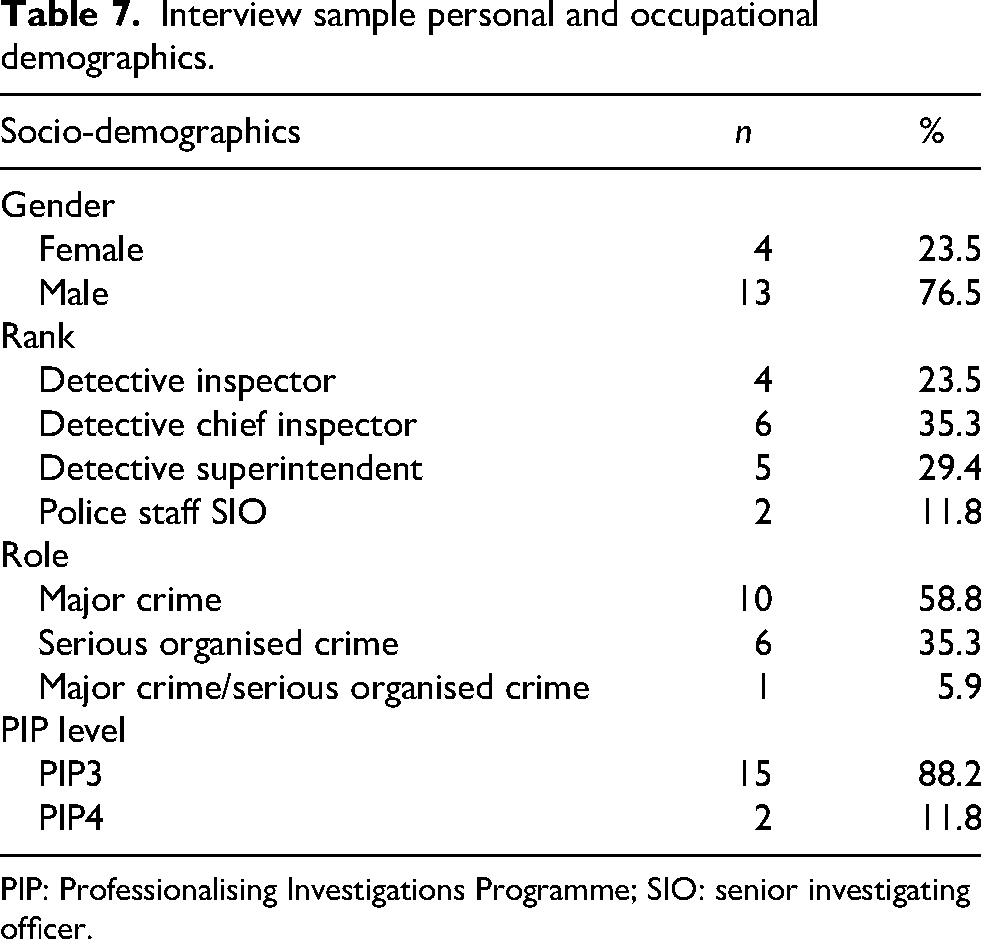
PIP: Professionalising Investigations Programme; SIO: senior investigating officer.
Procedure
RTA was the most appropriate method for analysing the data (Braun and Clarke, 2006). RTA is considered a form of theme-based qualitative analysis. Following guidelines for reporting RTA (Braun and Clarke, 2016, 2019), it is important to identify the guiding frameworks. The philosophical stance taken here is ‘critical realism’, in which experiences are subjectively understood, but are nevertheless a reflection of that person's reality. The framework for understanding the data is Lazarus and Folkman's model of stress and coping, whereby ‘psychological stress is a particular relationship between the person and the environment that is appraised by the person as taxing or exceeding his or her resources and endangering his or her well-being’ (Lazarus and Folkman, 1984: 21).
Analysis
Organisational stress as a contextual factor
The impact of organisational stress was explored in relation to trauma appraisals. This theme relates to the level of demand and burden faced by SIOs, and describes the relationship between demand and how/why greater levels of organisational stress may lead to increased trauma. This theme draws firmly upon Lazarus and Folkman's idea of secondary appraisal, whereby lack of access to coping resources, and a reduced ability to utilise them can result in greater trauma.
Several SIOs detailed how PTSD and trauma can be greater where there is a lack of organisational support, high levels of demand and a lack of training. Regarding levels of support, SIO4 suggested that being blamed for the death of a missing vulnerable person during an investigation led to increased trauma: … that was the beginning of the end, because when he was found, when we eventually found him dead. The finger pointing, you know, when I got a call to say he was found, it was like a dark cloud descending on me, and it was like a culmination of everything over the [years] […] and I just felt sadness, I felt sad …
SIO12 directly connects lack of support from managers to an investigation around serious and organised crime, whereby firearms were shot at members of their team. Following some challenges to a chief officer’s decision-making, the SIO related their subsequent experience to aspects of PTSD, whereby ‘[I] spent the next two years being bullied by [them], so there's been some significant, which ended up being elements of post-traumatic stress that come out as a result of me being off …’.
Again, SIO2 demonstrates how a lack of organisational processes and support mechanisms for those who experience repeated traumatic exposure, particularly as investigators, means that detectives are not picked up by internal support processes and mechanisms: … they [police service] don’t put processes around accumulative workload that people pick up, that causes and the screening of those kinds of cases, they don’t have sort of the same processes for detectives … specialist units tend to have processes in place, but there isn’t any cumulative process.
Overall, this theme expands upon and explains the quantitative results showing that organisational stress is a significant predictor of PTSD scores. In particular, the theme demonstrates how organisational stress is shaped by a lack of organisational support.
Cumulative trauma, but increasing resilience
What was clear from the findings of Study 2, was the pattern of increasing resilience. This was demonstrated by SIO17: I remember going to my first dead body, and shocked, and oh my god I can’t believe this and then over the years you sort of grow and experience, and interest, so I do think you do become resilient to your experiences.
However, what was also notable was the pattern of accumulating trauma alongside increasing resilience, as argued by SIO10: ‘and that sort of … that really … that was sort of the cumulative things that sort of hit home …’.
What may help bring these two findings together are the coping processes used by SIOs, which loosely describe patterns of exposure, avoidance, detachment and subsequent positive appraisals. It is argued that after these processes ‘kick-in’, the effect of an accumulation of traumatic exposure becomes recognised and acknowledged by an SIO. This is commented on by SIO4 (emphasis added): … that was the start of the beginning of the end for me, insofar as you know, you don’t realise over the years just how much baggage you accumulate. You’ve heard of Locard's theory? Every contact leaves a trace […] but it's also very true emotionally … through all the years of doing things and dealing with things, I’d forgot about myself.
Many other SIOs described similar processes or just desensitisation/avoidance strategies. Some interviewees claimed that this avoidance process was a form of ‘emotion-focused coping’, whereby other SIOs saw it more as a deliberate and purposeful process to facilitate a more problem-focused coping approach. For example, to avoid or minimise the emotional toll experienced, so that they could provide a more-effective investigation. SIO9 demonstrates: … I’ve got a coping mechanism, and I seem … I’m quite good at compartmentalising, I’ll almost look at it as, deal with it, yeah, it's horrendous while you’re dealing with it, get on with it, then you box it off, put it somewhere in your head don’t you and you move on to the next job …
SIO6 also describes this avoidance in greater detail, to facilitate a more-effective investigation, demonstrating that psychological detachment can facilitate ‘putting your work head on’, thus helping to maintain or improve investigative decision-making: … you never forget. Things like going to a [redacted] day-old baby that had died … and I’d not long had a little girl […], and that changes your perspective, you know. I’ve been to stuff before, and you put your work head on. I’m a big believer, you have your work head on, you do your job, because you have to […] I remember my telling my wife, ‘oh god, I’ve got to go to this job’ […] and I had to just switch it off and say, ‘I can’t speak to you, I need to put my game head on’ […] I needed to box that home life, because I couldn’t go into it, thinking of that.
This process may then, for some SIOs, lead to a greater chance of positive appraisal, as noted by SIO17: … the more bodies that you go to, the more … each one, you’re learning and developing, so the first dead body that you go to […] you don’t want to go near, the smell is awful, it stays with you, and then you become more experienced and confident, you become more interested, and therefore you want to be in there to find out are there any marks on the body, have they been strangled, and what's happened, and with the CSI you work together to try establish what's occurred …
The qualitative findings above help to explain the quantitative results, showing that experiencing trauma 6 to 12 months ago predicts reduced PTSD and CPTSD, and further showing how experiencing trauma 10 to 20 years ago predicts increased levels of CPTSD. The qualitative findings explain this by suggesting a pattern of becoming ‘resilient’ to trauma in the earlier portions of a policing career, while simultaneously becoming at greater risk towards the end. Indeed, this was notable in the reflections of SIOs when they compared earlier periods of their career with the time of interview. The findings also explain how adult homicide can predict reduced PTSD, because appraisal processes turn traumatic experiences into ‘learning’ experiences. However, although gender was somewhat implicated in one of the PTSD symptom clusters, this was not strongly borne out in the qualitative research. Indeed, both male and female SIOs described very similar coping processes.
Centrality and child homicide
Centrality refers to a process in which a person may ‘reflect ongoing themes or issues of particular concern in the person's life [which] should have a more important impact on the psychological and physiological economy of the person’ (Gruen et al., 1988: 744). This is relevant because a person's belief systems and values propel them towards certain situations. In addition, ‘central hassles should be more closely related to important patterns of goals, beliefs, and commitment’ (Gruen et al., 1988: 744). This idea has been applied in a recent study in child and sex abuse investigators (Foley et al., 2024a).
An enduring theme throughout the research was the sense of pride, personal achievement and sense of justice that could be achieved by an SIO and their teams, which was a propelling factor, as argued by SIO6: … you’re dealing with real, horrible, nasty paedophiles who are describing intimately what they want to do to a baby, and I mean graphically … that sometimes becomes the motivation for doing the job, and getting the job done, and people drop everything to catch that person, so that becomes sometimes … the vileness and awfulness of it becomes the motivation to do the job well and to do your best.
Ubiquitously, child homicides were considered to be much more stressful than other types of criminal investigation. Indeed, many SIOs felt that child deaths were inherently more traumatising given the innocence of children, but more apparent was the potential for greater personal resonance with child homicides, as shown by SIO15, who described PTSD-like symptoms (re-experiencing): The images of those dead kids really stay with you. You never shake them off. As I’m talking to you now, I’m just replaying one in my head, I can just see that dead child […] It's the innocence of kids, and being a parent yourself […] then you’ve related to something personal then …
The likelihood of this personal–professional transposition occurring increases in the case of a child homicide, as shown by SIO3: … it was a little [child], and he’d been stabbed repeatedly … it was that, again, blurring police head, human, ‘that could have been my son’ […] I saw one tiny part of a photograph, of the post-mortem photographs, and it was his little arm, and he had his pyjamas on […] but all you do is picture is your own kids, and my little boy at the time was wearing those kind of pyjamas …
Finally, the qualitative findings support Study 1, whereby child homicide significantly predicts increased PTSD, and is the only investigation type to predict all three PTSD symptom clusters. The qualitative findings explained this relationship by relating to the concept of ‘centrality’, thus signifying a greater potential for threat.
Discussion
This mixed-method study investigated the impact of experiencing traumatic events for the first time in a representative sample of UK SIOs. In so doing, this study highlighted that 5.4% and 4.1% of SIOs may have PTSD and CPTSD respectively, and that there are tentative relationships between length of service and trauma, as well as child homicide. Furthermore, organisational and operational police stressors are also related to increased PTSD and CPTSD symptoms. Although child homicide is implicated in increased PTSD and PTSD symptomology, adult homicide investigations may lead to decreased ‘re-experiencing’ and ‘sense of threat’. The qualitative analysis contextualised the findings, by showing how SIOs perceive organisational stress as a contextual factor to increased PTSD; how SIOs accumulate traumatic experiences but also become resilient, prior to reaching a ‘cliff edge’; and finally, demonstrated how and why child homicides may be more strongly related to increased PTSD and CPTSD, whereas adult homicides are not.
Support for these findings can be found across the literature. For example, for organisational stress as a contextual factor, Violanti et al. (2017, 2018) show how administrative and organisational pressure significantly predicted PTSD scores. Perceptions of organisational support are further implicated in support-seeking behaviours following traumatic events elsewhere (Heffren and Hausdorf, 2016). Similarly, Foley et al. (2022) have shown that support significantly predicts lower levels of PTSD, and their review (and others) replicates the importance of organisational support (Cartwright and Roach, 2022; Foley and Massey, 2021). Utilising the above findings, alongside descriptions of situations given by SIOs, and wider research, organisational pressures and stressors may be more helpfully understood as ‘situationally’ relevant precursors to trauma symptomology (Maguire and Sondhi, 2024; Miller et al., 2022; Sondhi et al., 2025). Miller et al. (2022: 217) found that one of the most frequently referenced situational contexts for the worst traumatic experience was ‘organisational pressure e.g. lacking resources, support’.
In relation to trauma accumulation and tenure, these findings are replicated elsewhere, as others have noted no relationships were found between tenure and PTSD (Foley et al., 2022), possibly because of survivorship bias. Potential relationships are likely; however, this has been insufficiently investigated (Foley and Massey, 2019, 2021), and causality is difficult to establish (Hartley et al., 2013). Furthermore, Miller et al. (2022) found that cumulative exposure was a frequently occurring situational context in trauma. Most notably, what is replicated is the possibility that coping processes are not mutually exclusive, and that emotion-focused coping can facilitate problem-focused coping, thus leading to positive reappraisal (Folkman et al., 1986; Folkman and Lazarus, 1988a, 1988b; Lazarus, 1999; Lazarus and Folkman, 1984). Similar relationships have been noted in Maguire and Sondhi (2024). Still, the wording used by participants in this study and others (Parkes et al., 2019a, 2019b; Roach et al., 2018; Turner and Jenkins, 2019) is striking.
It is suggested in this paper that the relationship between length of service and trauma is curvilinear (Roach et al., 2018), suggesting that resilience and coping may mediate this relationship. Indeed, the current research supports arguments by Fyhn et al. (2016: 262) that those with increased resilience are able to ‘reframe stressful events into opportunities for growth, and evaluate challenges in a positive way’. Indeed, their research went on to show in a sample of Norwegian investigators that ‘hardiness-commitment’ significantly predicted lower burnout. It is suggested that resilience can be ‘taught’ (Roach, 2023). Early research suggests that resilience and trauma-processing skills training can mitigate against the impacts of trauma on memory, and are operationally relevant to policing (Miller et al., 2020). However, the research was underpowered owing to low sample sizes (Miller et al., 2020).
Finally, the research builds on findings in relation to child homicide. Van Patten and Burke (2001) found that those investigating child homicides had higher PTSD scores than ‘non patients’, including paranoia and psychosis. Similarly, Roach et al. (2017, 2018) reported greater emotional effects, rumination and investigative support in child homicides than adult homicides. There is plentiful research on the impacts of investigations involving children around sexual abuse and exploitation (Bourke and Craun, 2014; Foley et al., 2024b; Hurrell et al., 2018; MacEachern et al., 2019; Redmond et al., 2023), but not on child homicide. However, in a list of ‘worst’ trauma exposures, events including children, such as fatalities, abuse and exploitation were the most frequently mentioned (Miller et al., 2022).
Nevertheless, several limitations exist. First, non-response bias may underestimate the prevalence and nature of associations between the variables of interest, because SIOs self-selected to take part. Second, survivorship bias may impact the estimates again, because those who are on sick leave, and/or have left the police service due to the impact of traumatic incidents may not have been included. The cross-sectional design is also a limitation, because this may reduce the validity of the findings in relation to length of service. The choices of investigations presented to SIOs may have introduced bias, including more categories in a major crime context, and may underrepresent those involved in serious and organised crime investigations. This is reflected in the low proportion of SIOs who had been involved in counter-terrorism investigations. It is unclear as to how representative of the population this is, because a breakdown of qualification by type is not available.
Conclusion
In conclusion, this paper presents the first set of findings from a wider project investigating the well-being of SIO. Although not the first published study featuring SIOs, it is the first with SIOs to use a census sampling approach, alongside validated psychological scales. The study met the research aims by demonstrating that child homicide, and organisational stress are important predictors of increased PTSD symptomology, and CPTSD. The qualitative findings further explain these by drawing on relationships between a lack of organisational support, organisational stress, child homicide and coping strategies. This research highlights several areas of risk for SIOs in relation to their experience of trauma. Primarily, those investigating child homicide are at much greater risk than those investigating other types of crime; that the relationship between trauma and length of service may be curvilinear; and organisational and operational stressors should be considered as exacerbating factors. Police forces should monitor and track the exposure of officers to traumatic events, particularly child homicide, as well as monitoring exposure to organisational stressors, understanding how these shape responses to traumatic stimuli. This could be done by utilising workforce data, audits, supported by the Police Traumatic Events Checklist (Miller et al., 2022), building in practical monitoring of SIOs, and officers more widely, including resilience training. With this, resilience training should adopt a ‘life-cycle’ approach, which is carried out continuously throughout officers’ careers, and not just seen as an ‘introductory’ element of training. These systems could support the automatic flagging of high-risk investigations, potentially supported by Artificial Intelligence. Such work is currently ongoing by the current authors. Finally, consideration should be given to mandatory psychological debriefs following traumatic investigations, particularly child homicide investigations.
Future research could build on these findings by doing the following: (a) measuring trauma exposure longitudinally across investigators; (b) understanding more strongly how centrality and purpose shape psychological responses to traumatic events; (c) understanding the long-term impacts of avoidance- and detachment-based coping strategies; (d) measuring the relationship between resilience, psychological well-being and positive appraisal of traumatic events; and, (e) quantitatively measuring factors such as innocence, deservedness and parental status as examples, and how they relate to child homicide and traumatic disorders.
Footnotes
Acknowledgements
We would like to thank and acknowledge the time given up by those senior investigating officers who supported this work, along with the support and guidance of former senior investigating officers Cheryl Chatterton and Fiona McCormack.
Ethical and consent statement
The University of Huddersfield Ethics Review Committee approved the survey and interviews in March 2021. Respondents consented on the online survey and gave written/verbal consent for review and signature before starting interviews.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
At the time of ethical review, a condition required was that data would only be available to the research team, and written consent by participants was given on this condition.