
Abstract
Background
Digital transformation in healthcare requires nurses to use new technologies while maintaining care quality. Adaptation becomes challenging in resource-limited settings where training, support, and infrastructure vary and where nurses often face competing demands.
Objective
This study aimed to develop a grounded theory explaining how nurses progressively adapt to digital transformation, the conditions that facilitate or hinder their movement, and the strategies they use to manage challenges.
Methods
A grounded theory design guided the study. Thirty nurses in an Egyptian private hospital participated in in-depth semi-structured interviews conducted over four months. Data collection and analysis followed constant comparison and continued until theoretical saturation.
Results
The study produced the Progressive Digital Adaptation theory. Two trajectories were identified. The sustaining trajectory showed confident and continuous integration, while the struggling trajectory reflected resistance or stalled movement. Five themes shaped adaptation. These were recurring resistance to technology, iterative learning and skill acquisition, integration into clinical routines, contextual factors influencing progression, and mechanisms supporting sustained transformation.
Conclusions
Effective digital adaptation depends on consistent organizational commitment. The theory clarifies how nurses progress or regress between stages and identifies practical targets for interventions that strengthen digital transformation in varied healthcare settings.
Keywords
Introduction
The rapid advancement of digital technologies has significantly transformed healthcare delivery, impacting the roles and responsibilities of nurses.1–4 Digital transformation in healthcare encompasses the integration of electronic health records (EHRs), telehealth services, artificial intelligence (AI)-driven decision support, and various other digital tools aimed at enhancing patient care and operational efficiency.5–7 However, the introduction of these tools presents numerous challenges, particularly for nurses who must navigate the complex interface between traditional care practices and new technological demands.3,8
As frontline caregivers, nurses are at the forefront of adopting digital technologies to enhance patient care, streamline workflow, and improve clinical decision-making. 9 The integration of digital tools requires nurses to develop new competencies, navigate changes in workflow, and manage potential resistance to technology adoption.4,6 Additionally, concerns regarding data security, ethical considerations, and the digital divide among nurses with varying levels of technological proficiency further complicate the adaptation process.3,8,10
The rapid integration of digital technologies into healthcare systems has created significant challenges for nurses, who must adapt to new ways of working while maintaining high standards of patient care. 11 In many cases, digital transformation has been met with both enthusiasm and resistance within healthcare settings. Nurses are tasked not only with learning new systems but also maintaining high-quality care for their patients, often without sufficient time for training or adjustment. This pressure can result in frustration, burnout, and decreased job satisfaction.11,12 Although digital transformation promises efficiency and improved outcomes, it requires nurses to develop new technical skills and adjust their workflows, often without adequate preparation or support.2–4
Digital transformation not only requires nurses to acquire new technical skills, but also challenges traditional conceptions of nursing work and professional identity.13,14 Research suggests that nurses’ professional identity—rooted in direct patient care, clinical judgment, and therapeutic relationships—may be perceived as threatened by technologies that seem to prioritize documentation over care or efficiency over human connection.13,14 When digital systems introduce unfamiliar processes that disrupt established workflows and create potential for errors, nurses experience this not merely as a technical challenge but as a threat to their core professional competence and their ability to fulfill their fundamental responsibility of ensuring patient safety. As nurses navigate digital transformation, they must simultaneously develop digital competence while reconstructing their professional identity to encompass technological proficiency as a legitimate dimension of nursing expertise. 15 Understanding how nurses negotiate this identity transformation during digital adaptation is crucial to supporting successful adaptation.
While this study adopts grounded theory for nurses’ adaptation to digital transformation, it is important to acknowledge that several implementation science frameworks already examine how change unfolds in healthcare settings. Models such as the Normalisation Process Theory (NPT), the Consolidated Framework for Implementation Research (CFIR), and the Promoting Action on Research Implementation in Health Services (PARIHS) framework16,17 provide structured approaches for understanding how innovations are embedded, sustained, and integrated into organizational practice. These theories offer valuable insights into contextual factors, mechanisms, and processes that influence implementation. However, most implementation models emphasize system-level outcomes or organizational readiness, rather than the evolving, subjective experiences of frontline nurses—especially in developing countries navigating infrastructural and cultural transitions.18,19 This highlights the contribution of grounded theory in capturing the nuanced, processual, and emotionally embedded nature of nurses’ adaptation.
Despite the importance of understanding how nurses adapt to these changes, there remains a significant gap in understanding how nurses adapt to digital transformation in developing countries. In these contexts, resource constraints, infrastructure limitations, variable technological literacy, limited access to training, insufficient managerial support, time constraints, and different organizational cultures create unique adaptation challenges that may not be fully captured by existing frameworks developed primarily in well-resourced settings.11,18–20 Understanding these experiences is essential, as concerns about technology reducing face-to-face interactions with patients and disrupting therapeutic relationships may hinder adoption and affect empathetic care.3,12,21 If technology is perceived as a tool that enhances rather than replaces compassionate care, nurses may be more willing to integrate it into practice.
Theoretical framework
In the context of digital transformation in healthcare, understanding how nurses adapt to new technologies is crucial.5,6,12 A theoretical framework that explains this adaptation process can provide valuable insights for both practice and research. This study was guided by the Diffusion of Innovations (DOI) theory developed by Rogers, 22 which provides a theoretical lens to understand how nurses adopt and integrate digital tools into their practice. Rogers defined innovation as “an idea, practice, or project that is perceived as new by an individual or other unit of adoption” (p. 12). 22 Individuals tend to engage with innovations when they perceive them as new, whether they are entirely novel ideas or existing concepts newly introduced to society. As Rogers explained, “innovation may have been invented a long time ago, but if individuals perceive it as new, then it may still be an innovation for them” (p. 12). 22 Typically, individuals do not adopt innovations unless they evaluate their comparative advantages, ease or complexity of use, and opportunities for testing, often discussing these aspects with peers. 22
Rogers 22 further explains that the adoption of innovations is a gradual process, even when their benefits are evident. New ideas, practices, or technologies spread within a social system over time through five key stages: knowledge, persuasion, decision, implementation, and confirmation (p. 170). 22 In the context of nursing, these stages help explain how nurses encounter, evaluate, and eventually integrate digital technologies into their daily workflows. 22
Applying Rogers’ framework to nursing practice, nurses’ adaptation to digital transformation could follow a progressive sequence, beginning with knowledge acquisition, where they become aware of new digital technologies through training programs, peer discussions, and organizational support. This is followed by persuasion, where they assess the potential benefits and challenges of technology adoption based on perceived usefulness, ease of use, and compatibility with nursing workflows. In the decision stage, nurses actively choose whether to adopt or reject the technology, influenced by managerial support, confidence in handling digital tools, and perceived professional advantages. When adoption occurs, nurses proceed to implementation, integrating digital tools into their practice while addressing technical issues, workflow disruptions, and adaptation challenges. Finally, in the confirmation stage, nurses reinforce their decision based on observed benefits in practice, determining whether to sustain or modify their use of technology. 22 Although Rogers’ original framework describes adoption by individuals generally, these stages have been adapted here to specifically reflect nursing practice contexts. 22
However, existing literature identifies multiple factors shaping nurses’ adaptation to digital transformation. These include innovation-related attributes, such as relative advantage, compatibility, complexity, trialability, and observability; individual characteristics, including personal motivation, confidence, and familiarity with digital tools; organizational conditions, such as hospital policies, managerial support, and access to resources; and technological features, including system reliability, usability, and access to training.2,3,22–24 While these factors align broadly with Rogers’ Diffusion of Innovation framework, 22 the model does not fully capture nurses’ lived and processual experiences of digital adaptation. In particular, it does not account for the cyclical and non-linear movement between adoption states, the emotional and identity-related challenges nurses encounter, or the ways contextual constraints in resource-limited settings shape divergent adaptation trajectories.19,20,25
This study therefore addresses this gap and employed a methodology to develop a substantive theory grounded in nurses’ experiences of adaptation to digital technologies, identifying what mechanisms enable or obstruct progression through adaptation stages, and why some nurses achieve sustained integration while others experience prolonged resistance or partial adoption. The findings could enhance understanding of the adaptation process in resource-limited settings and inform development of targeted support interventions that address both technical and psychosocial dimensions of digital transformation. Additionally, the study could contribute a theoretical framework that captures the dynamic, non-linear nature of nurses’ digital adaptation, providing a foundation for future comparative research across diverse healthcare contexts.
Aim of the study
The aim of this study was to develop a grounded theory explaining the process through which nurses progressively adapt to digital transformation in healthcare settings, including the conditions that facilitate or hinder progression, and the strategies nurses employ.
Methods
Research design
The study employed Corbin and Strauss’s 26 grounded theory methodology to develop a theory explaining how nurses adapt to digital transformation in healthcare settings. Grounded theory is an inductive qualitative approach that allows for the development of theory directly from data. It is especially suited for understanding processes that unfold over time and are shaped by interaction, such as nurses’ engagement with digital technologies in clinical environments.
Grounded theory methodology was appropriate for developing a theory explaining the process of nurses’ digital adaptation, including the conditions influencing this process and the strategies employed at different stages. This approach enabled systematic data collection and analysis to generate theory grounded in participants’ lived experiences. 26 The constant comparative method was central to the study, enabling ongoing analysis of data from the first interview through to saturation and theory generation.
The grounded theory methodology employed in this study is underpinned by symbolic interactionism, which posits that individuals act based on the meanings they attribute to their experiences, and these meanings are shaped through interaction with others and their social environment. 27 This theoretical foundation allowed the study to examine how nurses construct meaning around digital transformation and how their interpretations and responses evolve through interaction with technology, colleagues, and organizational structures.
Data collection and analysis were iterative and concurrent. Coding followed Corbin and Strauss’s structured approach, including open coding, axial coding, and selective coding, with continuous refinement of emerging categories. 26 The study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines 28 to ensure transparency, rigor, and comprehensive reporting of qualitative methods.
Setting and context of the study
This study was conducted at a well-established private hospital in Egypt, a developing country context where digital health infrastructure is rapidly evolving but faces distinct implementation challenges. Over the past two years, the hospital has actively integrated a range of digital systems into its clinical operations, including electronic health records (EHRs), digital documentation tools, and telehealth services. As a multi-specialty institution serving diverse patient populations, it has positioned itself as a regional leader in healthcare digitization.
The hospital utilizes an integrated electronic health record (EHR) system for patient documentation, computerized physician order entry (CPOE), digital medication administration systems, and telehealth platforms for remote consultations. Clinical practices at the hospital follow national healthcare standards, with nursing staff working in 8–12-hour shifts across medical, surgical, and critical care units. Digital documentation is mandatory for all patient encounters, requiring nurses to input vital signs, assessments, medications, and care plans electronically.
Nurses employed at this hospital had direct exposure to a wide array of digital innovations, making the setting ideal for exploring their adaptation processes. While the hospital administration provided structured training programs and technical support, the extent of digital engagement and the challenges encountered varied across departments and individual nurses.
Researcher context
The research team consisted of female nurse scholars with backgrounds in healthcare, nursing administration, and qualitative research methodology. Prior to data collection, the researchers had no existing relationships with participants. Throughout the research process, the team-maintained reflexivity through regular meetings to discuss emerging insights, examine assumptions, and critically evaluate their positionality in relation to the data. 26 Reflexive memos were maintained to document how the researchers’ backgrounds and perspectives might influence data interpretation, and peer debriefing sessions were conducted to challenge emerging categories and strengthen analytical integrity.
Participants and sampling
Participants were selected using a combination of sampling strategies consistent with grounded theory methodology. 26 Nurses were recruited from medical units, surgical units, and critical care units, with clinical experience ranging from less than two years to over fifteen years, and recruitment continued until data saturation was achieved at thirty interviews.
Inclusion and exclusion criteria
Inclusion criteria consisted of registered nurses employed at the study hospital with a minimum of six months’ experience using digital systems such as electronic health records, telehealth platforms, or digital documentation tools. Participants were required to be currently working in clinical practice, willing to participate, able to provide informed consent, and able to communicate in Arabic. Exclusion criteria included nurses on extended leave or not actively practicing during the study period, nurses who declined to participate, and nurses with less than six months of experience with digital systems.
The recruitment process began by contacting unit nurse managers from the target clinical units to identify potential participants. Unit managers were provided with study information and inclusion criteria. Eligible nurses were then approached individually by the research team, provided with written and verbal information about the study, and invited to participate willingly. Those who expressed interest were given time to consider participation before providing written informed consent.
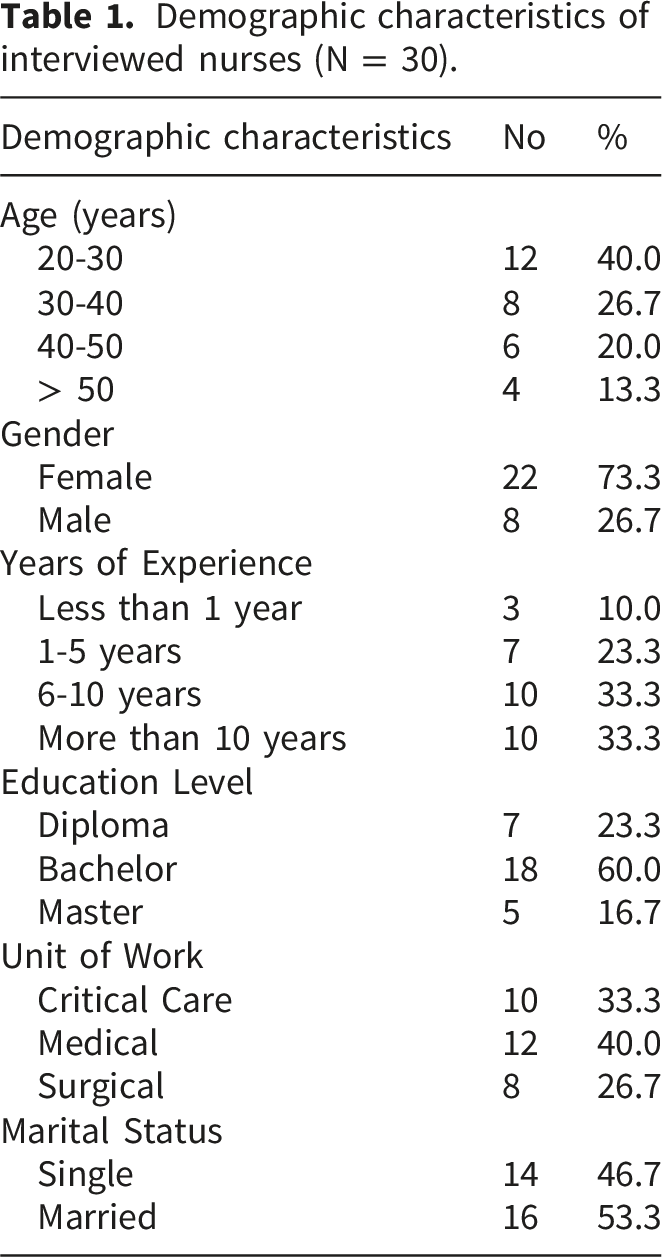
Theoretical saturation was achieved after thirty interviews, when additional interviews no longer produced new codes, themes, or properties, and the emerging theory was well-developed and conceptually dense.29,30 The final sample included eleven nurses from medical units, ten from surgical units, and nine from critical care units. Educational preparation included twelve diploma, fifteen bachelor’s, and three master’s degree holders. The sample included twenty-four female and six male nurses.
Data collection
Data were collected over a four-month period using in-depth, semi-structured interviews developed by the researchers based on literature review.3,31,32 A pilot interview was conducted with one nurse to test the interview guide; minor adjustments were made based on feedback, and the pilot was not included in the final analysis.
Interview Guide
The interview guide consisted of two sections within a single integrated form. The first section gathered demographic information including age range, gender, educational qualification, clinical unit, years of nursing experience, and duration of digital system experience. The second section comprised open-ended questions exploring the process of adaptation (“How did you first feel when digital systems were introduced?”, “How has your use changed over time?”), conditions influencing adaptation (“What training did you receive?”, “What challenges have you encountered?”, “What support did you receive?”), and strategies employed (“How did you learn to use these systems?”). Follow-up probing questions explored emerging themes in depth.
Interview procedures
Face-to-face interviews were conducted in a private hospital setting after obtaining written informed consent. Each session lasted forty-five to sixty minutes and was audio-recorded with participants’ explicit consent for verbatim transcription. Demographic responses were recorded on the interview guide using only participant identifiers (P1, P2, P3); no names, employee IDs, or other identifying information appeared on research materials.
Field notes were maintained throughout data collection. During interviews, brief observational notes captured non-verbal cues, emotional reactions, and contextual details. Within thirty minutes after each interview, these notes were expanded to include reflections on interview dynamics, emerging patterns, and questions for subsequent data collection.
Data analysis
Data analysis in this study followed Corbin and Strauss’s grounded theory methodology,
26
using a systematic, inductive, and iterative approach to generate theory grounded in participants’ experiences. Interviews were transcribed verbatim and reviewed immediately following each session to inform subsequent sampling and questioning. The analysis began alongside data collection, following the principle of constant comparison—a core principle of grounded theory—which involves systematically comparing each segment of data with all others to identify patterns, variations, and relationships, thereby refining emerging categories.
26
See Figure 1. Constant comparative methods between data collection and data analysis.
Consistent with Morse’s 29 recommendation, all data were given equal consideration during analysis, with new data continuously compared with existing categories to further refine and expand the developing theory. This iterative process ensured analytical consistency and depth throughout the study.
Open coding
The first phase involved open coding, in which transcripts were examined line-by-line to identify significant statements, actions, or meanings. Each segment of data was labelled with descriptive codes, many of which reflected participants’ own words. These initial codes were written in the margins, colour-coded, and organised manually into clusters based on similarities in content. Through this process, early conceptual categories were identified, such as “fear of making errors,” “lack of confidence,” and “support from peers.”
Focused and axial coding
Following open coding, focused coding grouped significant codes into broader categories. Concurrently, the axial coding phase examined relationships among these categories to develop subcategories and specify conditions, contexts, interactions, and consequences associated with each phenomenon. 26 For example, the subcategories “formal training” and “self-directed learning” were linked under the broader category of “learning and skill acquisition,” revealing how different support mechanisms shaped nurses’ adaptation over time. Throughout this phase, constant comparison continued to ensure that relationships between categories were empirically grounded and theoretically coherent.
Selective coding
The final stage, selective coding, involved identifying the core category that unified all emerging themes and subthemes. This central phenomenon—nurses’ adaptive journey to digital transformation—captured the dynamic process through which nurses navigated technological change, balancing barriers and facilitators to ultimately integrate digital tools into clinical practice.
Memo writing was used throughout all coding phases to support reflexivity, document coding decisions, and capture evolving theoretical insights. 26 Although no qualitative software was employed, the manual coding process facilitated deep immersion in the data and strengthened analytical rigour.
Theoretical saturation was achieved when no new codes or categories emerged from subsequent interviews, and the relationships between concepts were well-developed and clearly understood.29,30 This process ensured that the emerging theory was both contextually rich and empirically grounded, offering a comprehensive explanation of how nurses adapt to digital transformation within healthcare settings.
Rigour and trustworthiness
To enhance trustworthiness, multiple strategies aligned with qualitative research standards were embedded in the study design.29,33
Credibility was strengthened through prolonged engagement with participants, iterative data collection, and member checking. After initial analysis, summaries of findings were shared with selected participants to validate interpretations. Dependability was supported by maintaining a detailed audit trail including interview protocols, memo notes, coding decisions, and analytical reflections. The research team held regular reflexive meetings to examine assumptions and critically evaluate positionality. Confirmability was addressed by documenting all analytical decisions, ensuring findings remained rooted in data rather than researcher preconceptions. Memos were used to bracket assumptions, and peer debriefing with an external qualitative expert challenged emerging categories. Field notes were recorded after each interview session rather than during interviews to maintain natural conversational flow and minimise participant distraction; these notes captured contextual observations, non-verbal cues, and initial analytical impressions. Transferability was supported through rich, contextualised descriptions of the study setting, participants, and methods, enabling readers to assess applicability to other healthcare contexts.29,30
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (2008). Ethical approval was obtained from the Ethics Research Committee of the Faculty of Nursing, Alexandria University (IRB approval No. [IRB00013620]). Written informed consent was obtained from all participants prior to data collection. Participants were fully briefed on the study’s purpose, procedures, and their rights, including the right to withdraw at any point without consequences. At the start of each interview, researchers reiterated these points and obtained explicit consent for audio recording. To ensure confidentiality, participants were assigned alphanumeric codes (e.g., P1, P2), and all identifying information was removed from transcripts. All recordings, transcripts, and forms were stored securely in password-protected files and accessed only by the research team.
Results
Participants’ characteristics
Demographic characteristics of interviewed nurses (N = 30).
Overview of the emerged theory
Emerged themes and categories.
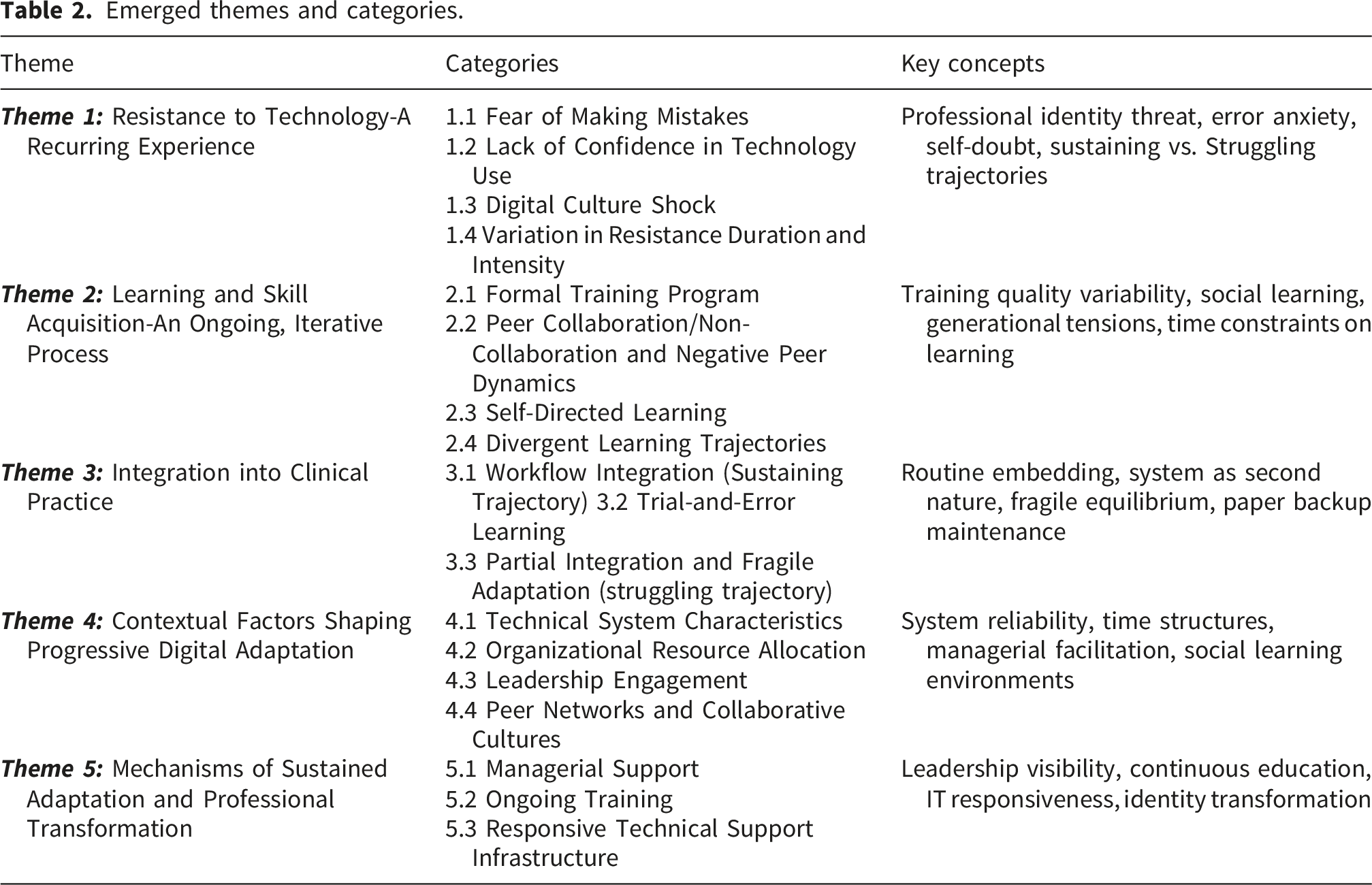
Critically, nurses’ experiences of digital adaptation followed a non-linear and cyclical trajectory. While some moved from resistance to integration, others experienced setbacks, stalled progress, or recurring challenges. Analysis revealed two distinct pathways: a sustaining trajectory characterized by relatively rapid progression toward confident digital use, and a struggling trajectory characterized by prolonged resistance, stalled learning, partial adoption, or regression to earlier stages. Strategies employed by nurses included formal training participation, peer collaboration, self-directed learning, trial-and-error experimentation, and seeking managerial support. Facilitating conditions included technical system reliability, protected time for learning, responsive leadership, and collaborative peer networks. Hindering conditions included system instability, time constraints, managerial disengagement, and absence of peer support. Approximately 15-20% of participants (n=5-6) experienced sustained resistance that never fully resolved.
Theme 1: Resistance to technology—a recurring experience
Many nurses in this study initially resisted digital systems, expressing fear of making mistakes and limited confidence in their technical abilities. These expressions of insecurity were intrinsically connected to professional identity. For nurses, professional identity is fundamentally constructed around their capacity to provide competent, safe patient care through clinical judgment and therapeutic relationships. As presented in the Introduction, unfamiliar digital workflows were perceived as threats to safe practice; in the Results, this concern emerged as a recurring experiential driver of resistance. The fear of making mistakes thus represented a deeper concern about maintaining professional credibility as competent caregivers. This identity threat was further compounded when digital systems were perceived as prioritizing documentation over direct patient interaction, creating tension between relational care values and technical demands of digital documentation.
Fear of making mistakes
For many nurses, the first and most pressing challenge was the fear of making errors when using the new digital systems. This fear was rooted in concerns over documentation accuracy, patient safety, and the irreversible nature of mistakes in real-time systems. It was not merely a matter of technical skill—it reflected a perceived threat to professional credibility and patient outcomes. At first, I was afraid I would enter something wrong and cause a serious problem in patient care. – (P3)
Lack of confidence in technology use
This fear often evolved into a broader lack of confidence, particularly among older nurses or those with minimal prior exposure to technology in their education or early careers. The confidence gap created a reluctance to fully engage with digital tools, reinforcing avoidance behaviors and dependence on colleagues. I wasn’t confident at all. I didn’t grow up with computers like some of the younger nurses, so I found it much harder to learn. – (P7)
Digital culture shock
For some, this lack of confidence was compounded by a profound “digital culture shock,” particularly among nurses transitioning from entirely paper-based environments. With little or no foundational exposure to digital systems, even basic tasks such as navigating an electronic health record felt alien, exhausting, and mentally taxing. It felt like being thrown into icy water—one day I was writing notes with a pen, and the next I was expected to master a whole electronic system. – (P012)
Variation in resistance duration and intensity
The duration and intensity of initial resistance varied considerably among nurses, shaped by the convergence of multiple contextual factors. These divergent experiences mark the emergence of two distinct trajectories: a sustaining trajectory characterized by rapid reduction in resistance and progression toward active learning, and a struggling trajectory characterized by prolonged or unresolved resistance.
Sustaining Trajectory: For nurses who received comprehensive initial training, responsive technical support, and protected time to explore the system gradually, fear and uncertainty diminished within weeks. These nurses described managerial understanding and peer mentorship as critical buffers against overwhelming anxiety. Nurses on this pathway experienced abbreviated resistance phases, typically lasting 2-4 weeks, before transitioning to active skill-building. Supportive conditions—comprehensive initial training, accessible peer mentors, responsive management, and technical stability—facilitated rapid confidence building and forward momentum. My manager made sure we had extra time in the beginning to practice. That really helped reduce my fear of making mistakes. – (P19) Having a colleague walk me through it step-by-step in the first week made all the difference. I didn't feel alone. – (P9)
Struggling trajectory: In stark contrast, nurses who encountered technical failures during their first attempts—combined with limited immediate support and competing time pressures—remained in a prolonged state of heightened resistance lasting months or, in some cases, never fully resolving. System crashes during initial use reinforced fears and validated their distrust of digital tools. The confluence of technical failures during initial encounters, absence of immediate support, and competing time pressures created a self-reinforcing cycle: initial failures confirmed fears, avoidance prevented skill development, and continued anxiety perpetuated resistance. The system crashed during my first shift using it. After that, I was terrified to touch it again for weeks. – (P27) There was no one to ask when I got stuck at first. I felt completely lost and wanted to avoid the system as much as possible. – (P11)
Unresolved resistance
For some nurses, particularly those close to retirement age with minimal prior computer exposure, initial resistance never fully resolved. These individuals continued to rely heavily on colleagues for basic tasks, viewing digital adaptation as an insurmountable burden rather than an achievable goal.
While the preceding section described resistance as if it were a discrete initial phase, the boundary between resistance and learning was permeable and unstable. Some nurses moved quickly from resistance to active learning, while others oscillated between the two states for months. Nurses who had entered the learning phase sometimes returned to resistance when encountering significant challenges. The following theme describes learning experiences while acknowledging that resistance remained a constant possibility, ready to re-emerge when conditions deteriorated.
Theme 2: Learning and skill acquisition—an ongoing, iterative process
As nurses moved beyond initial resistance, they entered an active learning phase. The transition was neither automatic nor universal, depending on training quality, support availability, and practice time. Learning recurred cyclically with each system update or workflow modification.
This period was marked by a gradual shift from apprehension to engagement, as nurses developed familiarity and confidence with the technology. Learning was not a one-dimensional process—it involved a combination of formal training, peer collaboration, and self-directed strategies. Descriptive words such as “training,” “familiarity,” “peer,” and “self-learning” were repeatedly used by participants to describe their experiences in this phase. However, the pace and success of skill acquisition diverged sharply between nurses following sustaining versus struggling trajectories. For nurses on sustaining trajectories, the learning phase represented genuine progression—building on reduced resistance to achieve functional competence within 2-3 months. For nurses on struggling trajectories, the learning phase was characterized by repeated setbacks, stalled progress, and in some cases, regression back to active resistance.
Formal training programs: Divergent impacts
For most nurses, the first step toward competence came through structured training provided by the hospital. These sessions not only built technical skills but also created a psychologically safe environment for practice, helping to reduce fear and uncertainty. The formal scaffolding gave nurses a clear starting point and reassured them that institutional support was available during the transition. The hospital organized a few workshops, and those were really helpful. I learned how to use the system efficiently, which boosted my confidence. – (P18)
However, the quality and adequacy of formal training varied considerably, directly impacting nurses' ability to progress. Several nurses described training sessions as insufficient, rushed, or poorly timed—occurring long before systems were implemented or covering too much content too quickly. They trained us three months before we actually started using the system. By the time we needed it, I had forgotten most of what they taught us. – (P26)
These inadequacies left many nurses reliant entirely on trial-and-error or peer support to develop even basic competencies, significantly prolonging the learning phase.
Peer collaboration: Sustaining vs. struggling experiences
Sustaining experiences
As nurses began applying what they learned, peer support became a vital bridge between training and confident use. More digitally proficient colleagues often assumed informal mentoring roles, guiding others in real time during daily tasks. This collaborative learning environment reinforced skills, reduced anxiety, and cultivated a sense of solidarity. Adaptation, in this sense, was not an isolated process but a socially mediated one embedded in team interactions. We helped each other a lot. Those who understood the system better taught the rest of us, and we worked together to figure things out. – (P20)
Yet peer support was not uniformly available across all work contexts. Nurses working night shifts, in chronically understaffed units, or alongside colleagues who were themselves struggling with the technology described isolation in their learning journey. Without accessible peers to consult in real-time, these nurses progressed more slowly and experienced greater anxiety: On night shifts, there aren’t many people around. When I got stuck, I just had to wait until morning or skip that task entirely. – (P17)
This absence of collaborative support created divergent learning trajectories even among nurses with similar baseline capabilities and motivation.
Instances of non-collaboration and negative peer dynamics
While peer support facilitated adaptation for many nurses, not all peer interactions were collaborative or supportive. Instances of non-collaboration emerged across multiple forms, each with distinct consequences for learning trajectories.
Refusal to share knowledge: Several nurses described colleagues who possessed digital expertise but actively withheld assistance. These digitally proficient nurses viewed helping others as additional unpaid labor that detracted from their own clinical responsibilities: Some of the younger nurses who knew the system well acted like we were interrupting them when we asked questions. They’d give you short answers or tell you to figure it out yourself. – (P15)
Generational Tensions and Judgment: Age-related dynamics sometimes created barriers to seeking help. Older nurses reported feeling judged by younger colleagues for their digital struggles, while younger nurses perceived older colleagues as resistant or unwilling to learn: Some of the older nurses would just refuse to even try. They'd complain constantly instead of learning, and it was frustrating for those of us trying to help them. – (P6)
Consequences of Non-Collaboration: When collaborative support was absent or hostile, nurses experienced prolonged learning phases, increased anxiety, and in some cases, complete disengagement. The absence of peer support meant these nurses had only inadequate formal training to rely on, significantly delaying or preventing skill acquisition: After being brushed off several times, I just stopped asking. I stayed stuck at the same level for months because I didn't know who to turn to. – (P17)
These findings illustrate that peer networks do not uniformly function as supportive learning environments. When collaboration fails—whether through active refusal, judgmental attitudes, or generational tensions—nurses become isolated in their adaptation journey, often resulting in stalled learning, sustained resistance, or withdrawal from digital engagement entirely.
Self-directed learning: When possible vs. When impossible
Over time, many nurses took greater ownership of their learning, engaging in self-directed activities to deepen their understanding of digital systems. This proactive approach reflected a growing sense of autonomy and intrinsic motivation to master new tools. For some, it also marked a redefinition of professional identity, signaling their adaptation to the realities of modern, technology-driven healthcare. I spent some time after my shift practicing on the system. I didn’t want to rely entirely on the training. It helped me a lot. – (P25)
However, the capacity for self-directed learning was significantly constrained by time availability and system stability. Many nurses expressed a genuine desire to explore the system more thoroughly and develop advanced skills, but found it impossible to do so within the demands of their clinical shifts: Even when I want to explore the system more, I can’t. There's no time during shifts, and we’re always understaffed. – (P21)
Additionally, persistent technical glitches interrupted practice attempts, undermining both confidence and motivation to continue self-directed learning. When systems crashed or logged nurses out unexpectedly, the mental and emotional energy required to restart made continued exploration feel punishing rather than productive: Sometimes the system logs you out while documenting, and all the data disappears. After that happens twice, you don't want to experiment anymore. – (P18)
Divergent learning trajectories: Nurses who stalled
Not all nurses progressed to confident, independent use of digital systems. Some remained reliant on colleagues for extended periods, their learning stalled by a confluence of barriers. Persistent time constraints made deliberate practice impossible, leaving nurses perpetually reactive rather than proactive in skill development: There’s just not enough time. Between patient care and all the digital documentation, I feel like I’m always behind. – (P13)
Others experienced repeated technical failures that eroded their motivation to continue learning. Each system crash or data loss reinforced a sense of futility: When the system crashes every other day, it’s hard to stay motivated to learn new features. You just want to get through the basics and move on. – (P9)
For nurses nearing retirement, the substantial investment required to achieve competence felt disproportionate to the remaining years of their career. Several nurses in this group explicitly stated they would do the minimum required and wait for retirement rather than fully engage with digital transformation: I have three years until retirement. I’ll do what I must, but I’m not going to master this system. It'’s too much effort for too little time left. – (P29)
These nurses often described feeling ‘stuck’ in a state of minimal competence—able to perform only the most basic functions while avoiding complex features entirely, relying heavily on colleagues, and experiencing ongoing anxiety about making errors. Not all participants described complete resolution of resistance. For some, unease persisted even during later phases of learning or integration: I don’t trust it fully… sometimes I still keep paper notes, just in case. – (P16)
Trajectory Outcomes: Nurses on sustaining trajectories developed functional competence and reliable support networks. Those on struggling trajectories remained dependent on colleagues, avoided complex features, and experienced ongoing anxiety. The shift from active learning to workflow integration was neither automatic nor permanent. Many nurses described achieving initial integration only to lose it following technical disruptions, organizational changes, or sustained high workload periods. The following theme describes integration experiences while emphasizing their fragile, conditional nature—integration was not a stable endpoint but a dynamic state that could be disrupted, requiring nurses to cycle back to intensive learning or even resistance.
Theme 3: Integration into clinical practice
As nurses developed digital competencies, they began integrating technology into clinical routines. However, integration was neither stable nor irreversible—it represented a fragile equilibrium disrupted by technical, organizational, or contextual changes, causing nurses to cycle back into resistance or intensive learning. Some achieved integration, lost it following disruptions, and rebuilt it multiple times. Others oscillated between integrated use and minimal engagement based on workload pressures. Integration was therefore not an endpoint but a temporary state requiring continuous organizational support, technical reliability, and protected practice time.
Integration experiences diverged dramatically between sustaining and struggling trajectories. Nurses on sustaining trajectories achieved relatively smooth embedding of digital tools, describing them as becoming “second nature” within 4-6 months. Nurses on struggling trajectories experienced fragile, incomplete integration characterized by selective use, parallel paper documentation, and regression when pressures intensified. For many, integration represented a transformation where technology became normalized in care delivery, reshaping workflows and reinforcing professional identity.
Workflow integration (sustaining trajectory)
With sustained exposure and familiarity, many nurses described digital systems as an embedded part of their professional practice. Over time, these tools were no longer perceived as separate or disruptive but as integral to efficient patient care. This change represented both a behavioral and cognitive shift—technology moved from being an obligation to becoming an ally in clinical decision-making and care coordination. After a few months, it became part of my routine work. I can now manage patient records faster, and it’s become second nature. – (P14)
Trial-and-error learning
For many, the path to integration was paved with experimentation. In situations where immediate guidance was unavailable, nurses developed personal strategies for navigating systems, refining their techniques through repeated use and learning from mistakes. This trial-and-error approach fostered a sense of ownership over the adaptation process and strengthened problem-solving skills in a real-world context. I had to figure out the best way to input patient information. It took some time, but now I have a system that works for me. – (P28) Sometimes I discover quicker ways of doing things just by exploring the system on my own. – (P19)
Partial integration and fragile adaptation (struggling trajectory)
While many nurses described achieving routine use of digital systems, integration was often incomplete, selective, or fragile. Technical problems continued to disrupt established workflows even after months of use, forcing nurses to maintain paper backup systems or develop elaborate workarounds. The inability to fully rely on digital tools during high-pressure clinical situations undermined confidence and prevented complete integration: It's hard to trust the system when it crashes every other day. It adds stress when you’re already trying to do so much. – (P9)
System updates periodically destabilized established routines, requiring nurses to re-learn interfaces, adapt to new workflows, and rebuild efficiency they had worked months to achieve. These disruptions sometimes triggered regression to earlier stages of uncertainty and frustration: Just when I got comfortable, they updated the whole system. It felt like starting over. – (P23)
For some nurses, integration remained deliberately limited to essential functions. Competing time demands made exploration of advanced features impossible, and the pressure to complete documentation quickly discouraged any experimentation: I use it for the basics—labs, medications, vital signs. But all the other features? I don’t have time to figure those out. – (P16)
The absence of sustained managerial engagement also undermined integration for some nurses. Without continued encouragement, recognition of effort, or visible institutional commitment to supporting digital workflows, maintaining engagement with digital tools felt like an ongoing burden rather than a normalized professional practice: It felt like we were thrown into the deep end without much support from management. We needed more time and guidance. – (P22)
These findings illustrate that integration is not a definitive end-state but rather a dynamic, context-dependent process that requires ongoing technical reliability, organizational support, and protected time to sustain. The contextual factors described in the following theme determined whether nurses could achieve sustained transformation or remained trapped in cycles of resistance, stalled learning, and fragile integration. Sustained transformation was not the inevitable outcome of progression through earlier stages, but rather the result of continuously favorable conditions that prevented cyclical regression.
Theme 4: Contextual factors shaping progressive digital adaptation
Throughout the adaptation journey, nurses’ experiences were profoundly shaped by contextual factors—organizational, technical, and social—that either facilitated or hindered their progression through the stages of digital adaptation. These factors did not emerge only at specific points in the trajectory but operated continuously, influencing initial resistance, learning pace, integration depth, and sustained engagement in complex and interconnected ways. Understanding these contextual dimensions is essential for explaining why nurses followed divergent pathways despite encountering the same digital transformation initiative.
Technical system characteristics and infrastructure reliability
The technical characteristics of digital systems themselves—their stability, usability, and integration with clinical workflows—emerged as foundational to adaptation experiences across all stages. System reliability directly influenced nurses’ willingness to trust and engage with technology. During initial encounters, technical failures amplified fear and reinforced resistance. During skill-building, glitches interrupted learning and discouraged practice. Even after achieving routine use, ongoing technical problems fragmented workflows and required continuous compensatory strategies. Poorly designed or non-intuitive system interfaces added another layer of difficulty. Repeated disruptions created a form of “digital fatigue,” where the mental effort required to work around technical failures drained energy and motivation to engage with the system. Sometimes the system logs you out while documenting, and all the data disappears. That’s frustrating and wastes time. – (P18)
Organizational resource allocation and time structures
Organizational decisions about time allocation, staffing levels, and workflow design created distinct adaptation environments that either enabled or constrained nurses’ progression. The availability of protected time for learning, practice, and troubleshooting directly determined whether nurses could build competencies systematically or struggled in the margins of overscheduled shifts.
During initial encounters and early learning, lack of dedicated time prevented exploration and forced nurses to attempt learning during high-pressure clinical moments: There’s just not enough time. Between patient care and all the digital documentation, I feel like I'm always behind. – (P13)
The time pressure intensified during the integration phase as nurses attempted to balance comprehensive digital documentation with direct patient care. Many nurses described staying after shifts to complete charting, contributing to fatigue, burnout, and diminished job satisfaction: You’re constantly torn—do I spend another 10 minutes at the bedside, or do I rush to update the chart so I don’t forget something? – (P8)
Chronic understaffing compounded these time constraints, making it impossible for nurses to seek help, practice new skills, or collaborate with peers. The absence of organizational slack meant that digital adaptation had to occur within already unsustainable workloads, virtually ensuring prolonged difficulty and incomplete integration.
Leadership engagement and managerial facilitation
Leadership approaches varied dramatically across units and shifts, creating starkly different adaptation environments. The presence or absence of visible, engaged leadership emerged as one of the most influential factors determining adaptation success.
Where nurse managers actively facilitated adaptation—allocating time for learning, providing constructive feedback, acknowledging challenges, and creating psychologically safe spaces for questions—nurses described feeling supported and motivated to persist through difficulties: My manager made sure we had the support we needed. They allowed us extra time to attend training sessions, which made a big difference. – (P19)
In sharp contrast, perceived managerial disengagement amplified every difficulty. Without structured guidance, responsive technical support, or acknowledgment of the added workload, many nurses felt abandoned to navigate digital transformation alone. This lack of visible institutional commitment not only prolonged learning curves but also eroded morale, trust, and willingness to invest effort: If leaders had checked in more often, it would have made a big difference—we needed to know they understood the challenges we were facing. – (P4)
Peer networks and collaborative learning cultures
The presence or absence of collaborative learning cultures and accessible peer networks significantly influenced adaptation trajectories. In environments where digitally proficient colleagues assumed informal mentoring roles, learning accelerated, anxiety diminished, and problem-solving became collective rather than individual: We helped each other a lot. Those who understood the system better taught the rest of us, and we worked together to figure things out. – (P20)
However, not all nurses had access to supportive peer networks. Structural factors such as shift patterns, unit staffing levels, and the digital competence distribution of colleagues created vastly different social learning environments. Nurses working night shifts, in chronically understaffed units, or alongside colleagues who were themselves struggling with technology described isolation: On night shifts, there aren't many people around. When I got stuck, I just had to wait until morning or skip that task entirely. – (P17)
The contextual factors described above determined whether nurses could achieve sustained transformation or remained trapped in cycles of resistance, stalled learning, and fragile integration. The following theme describes how specific mechanisms enabled sustained transformation for those nurses fortunate enough to encounter supportive contexts throughout their adaptation journey.
Theme 5: Mechanisms of sustained adaptation and professional transformation
Nurses who successfully navigated adaptation attributed sustained transformation to specific organizational mechanisms maintaining conditions for ongoing digital engagement. This represents the culmination of the sustaining trajectory, where digital competence became embedded in professional identity and practice.
Three mechanisms enabled sustained digital engagement: ongoing training, responsive technical support, and sustained leadership engagement. These stabilizing forces buffered against setbacks, reinforced skill development, and fostered long-term confidence. Critically, these supports were most effective when provided continuously rather than only during initial implementation. For nurses experiencing these mechanisms consistently, technology use evolved from a competency to master into an internalized dimension of professional identity.
Managerial support
Nurses described managerial involvement as pivotal in shaping both their confidence and their sustained engagement with digital systems. Over time, supportive leadership was seen not only as a facilitator of skill acquisition but also as a driver of emotional resilience and professional empowerment during digital transformation. My manager made sure we had the support we needed. They allowed us extra time to attend training sessions, which made a big difference. – (P24) Knowing that leadership understood our struggle and checked in on us made me feel less alone in the process. – (P10)
Ongoing training
Nurses valued refresher sessions, especially when systems were updated or new features were introduced, as these helped retain knowledge, adapt to changes, and maintain confidence. Continued education reinforced the message that adaptation was a shared, supported process rather than an individual burden. The hospital offered follow-up sessions after the initial training, which was helpful as the system changed over time. – (P11)
Responsive technical support infrastructure
Beyond managerial engagement and training, the availability of responsive, accessible technical support emerged as a critical mechanism for sustained adaptation. Nurses who had access to dedicated IT personnel or help desk systems that could quickly resolve technical issues maintained confidence in digital tools even when problems occurred: When something goes wrong, I can call IT and they usually fix it within the hour. That makes me feel like I can rely on the system. – (P14)
In contrast, nurses who lacked responsive technical support described escalating frustration with each unresolved issue, leading to progressive disengagement and return to paper-based workarounds.
Collectively, sustained managerial engagement, ongoing training, and responsive technical support created conditions for transformation. These mechanisms enabled nurses to move from short-term coping to long-term integration. Without them, adaptation remained fragile or stalled.
Theoretical summary: Progressive digital adaptation
The grounded theory developed from this study is encapsulated in the core category Progressive Digital Adaptation, which captures how nurses gradually adjust to the integration of digital technologies within their clinical environments (see Figure 2). This process is complex, iterative, and shaped by intertwined emotional, cognitive, and organizational dimensions. Dual trajectories in digital adaptation: sustaining and struggling pathways.
Dual adaptation trajectories
This grounded theory reveals dual adaptation trajectories: a sustaining trajectory where nurses gradually integrate digital tools with increasing confidence, and a struggling trajectory marked by recurring resistance, avoidance, or stalled progression. These coexisting paths underscore the non-linear nature of digital adaptation, shaped by individual, organizational, and contextual factors. Some nurses progressed smoothly, while others cycled back or disengaged, depending on access to support systems, confidence, and digital familiarity.
Adaptation stages and transition mechanisms
The adaptation journey typically begins with Initial Resistance to Technology, where nurses described fear, uncertainty, and lack of confidence. This stage reflected the emotional labor required to reconcile professional identity with new technological expectations. Critically, resistance was not confined to this initial encounter but recurred cyclically throughout the journey—re-emerging when technical failures, system updates, or high workload periods undermined previously achieved confidence. Resistance was therefore not a stage to be overcome once but a recurring state that nurses moved in and out of repeatedly. Mechanism enabling transition from resistance to learning: Psychological safety creation—when managers normalize errors and provide protected practice time, fear-based avoidance shifts to exploratory engagement, freeing cognitive resources previously consumed by threat monitoring.
As nurses moved into Learning and Skill Acquisition, they shifted from passive resistance to active engagement. Competence was built through formal training programs, peer collaboration, and self-directed learning. This phase was marked by situated learning and collective problem-solving, where social interaction played a central role in reducing anxiety and fostering confidence. Mechanism enabling transition from learning to integration: Procedural automatization through graduated practice—beginning with low-acuity scenarios allows skills to become automatic before facing high-complexity situations. Without protected practice time, skills remain effortful and conscious, never achieving the automaticity required for seamless workflow integration.
In Integration into Clinical Practice, nurses began embedding digital tools into their daily workflows. This process involved workflow adaptation and trial-and-error learning, where digital systems evolved from being perceived as external impositions to becoming natural extensions of care delivery. However, the pace and depth of integration varied depending on system usability, peer support, and institutional facilitation. Mechanism triggering regression from integration: Cognitive overload during high-acuity periods or major system updates forces reversion to deeply ingrained paper-based routines. This regression occurs not due to skill loss but because extreme pressure forces reallocation of cognitive resources to patient care, abandoning recently acquired but still-effortful digital practices.
Adaptation as a non-linear, cyclical process
The theoretical coding revealed three distinct patterns illustrating the cyclical nature of Progressive Digital Adaptation:
Pattern 1: Regression Following Technical Disruptions. Nurses who had achieved confident integration sometimes reverted to earlier stages when confronted with major technical failures. For instance, P23 described how a system-wide update “felt like starting over”—forcing her to re-learn interfaces and rebuild efficiency. P9 reported that after repeated system crashes, she lost trust in the technology and began maintaining parallel paper documentation, effectively regressing from integration back to partial resistance.
Pattern 2: Stalled Progression and Partial Adoption. Some participants became stalled at intermediate stages, achieving only partial adoption. P29 explicitly stated: “I have three years until retirement. I’ll do what I must, but I’m not going to master this system.” P16 remained in partial integration, using the system “for the basics” but lacking time to explore additional features.
Pattern 3: Cyclical Movement Between Stages. Several nurses described oscillating between stages depending on contextual factors. P8 reported periods of growing confidence punctuated by returns to anxiety when workflow pressures increased, reverting to minimal documentation strategies during high-acuity shifts then returning to comprehensive digital engagement during less demanding periods.
Finally, Sustained Adaptation and Transformation emerged when support systems—particularly consistent managerial engagement and ongoing training—enabled nurses to maintain confidence and internalize digital practices as part of their professional identity.
Mechanism enabling sustained transformation: Continuous organizational reinforcement through visible managerial engagement maintains expectancy-value beliefs—nurses remain certain they can perform digital tasks effectively and convinced the organization values these efforts. When managers disengage post-implementation, these beliefs erode, triggering gradual regression even after months of successful integration.
Theoretical distinctiveness
Progressive Digital Adaptation extends existing theories in three key ways. First, unlike Rogers’ Diffusion of Innovation, 22 which describes adoption as a relatively stable outcome following the decision stage, and TAM/UTAUT34,35 frameworks that predict initial acceptance based on perceived usefulness, our theory reveals that healthcare technology integration is reversible—nurses who achieved confident use regressed to avoidance following disruptions. This addresses a critical gap identified by De Leeuw et al. 19 regarding post-adoption abandonment in healthcare settings.
Second, while Normalization Process Theory 36 describes the implementation “work” required for embedding practices, it does not fully account for individual-level variation within standardized implementations. May et al. 36 focus on collective action and organizational processes; our theory explains why divergent trajectories emerge even when implementation work is adequately performed—specifying enabling and obstructing mechanisms operating at the individual-context interface.
Third, while stage models describe phases, Progressive Digital Adaptation explicates how transitions occur and why they fail. This builds on Corbin and Strauss’s 26 process-oriented approach by specifying mechanisms through which contextual conditions shape individual trajectories.
Discussion
This grounded theory study offers a nuanced understanding of how nurses adapt to digital transformation in clinical settings, conceptualized through the theory of Progressive Digital Adaptation. The findings reveal an iterative process shaped by emotional, cognitive, and organizational dimensions, progressing from initial resistance through learning, integration, and challenge navigation to sustained adaptation and transformation. Consistent with Rogers’ Diffusion of Innovation framework 22 and Corbin and Strauss’s process-oriented lens, 26 the results highlight that adaptation is not linear but cyclical, with movement between stages influenced by contextual enablers and personal drivers. The current study extends existing evidence by illustrating how these processes unfold within a developing country context, where infrastructural constraints, resource limitations, and socio-cultural factors uniquely shape the adaptation trajectory. 3 The following sections discuss each theme, emphasizing mechanisms that enable or obstruct stage transitions.
Initial resistance to technology
Many nurses in this study expressed initial resistance to digital systems due to fear of making mistakes and limited confidence. This resistance reflected more than simple technical insecurity—it represented a threat to professional identity, which for nurses is fundamentally rooted in their ability to provide competent, safe patient care.24,25 Similar findings were reported by Ross et al. 37 who clarified that unfamiliar technology often triggers anxiety among healthcare professionals, and Tawfik et al. 38 who found that frustration with complex systems links to emotional exhaustion in high-pressure clinical settings. Technical problems encountered during initial system use amplified resistance by confirming nurses’ fears that systems were unreliable. Glitches and crashes during early attempts validated avoidance behaviors—nurses reasoned “why invest effort learning something that doesn’t work?” This created self-reinforcing cycles where technical failures prevented the early success experiences necessary for self-efficacy building.
Arnetz et al. 39 highlighted that sociotechnical barriers—inadequate training, lack of intuitive design, and minimal user involvement—exacerbated nurses’ apprehension during COVID-19. Mumtaz et al. 40 emphasized that resistance is rooted in deeper concerns about professional credibility, patient safety, and disruption to established workflows. Burgess and Honey 41 found that without structured support, nurses perceived new technology as burden rather than facilitative tool.
Transition mechanism: The shift from resistance to active learning was facilitated when organizations created psychologically safe environments where errors were normalized and support was immediately available. Conversely, when early technical failures occurred without peer support to buffer their impact, self-efficacy beliefs became fixed around “I cannot do this,” preventing progression regardless of subsequent training.
Critical caveat: Unresolved resistance
While Progressive Digital Adaptation describes a trajectory toward integration, not all nurses followed this pathway. Some participants’ initial resistance never fully resolved. These nurses continued experiencing persistent anxiety, avoided advanced features, and relied heavily on colleagues even months after implementation. Factors associated with sustained resistance included proximity to retirement, minimal baseline digital exposure, repeated technical failures during early encounters, and absence of mandatory competency requirements. Future research should examine factors differentiating sustained resistance from progressive adaptation.
Learning and skill acquisition
Following initial resistance, nurses turned to various learning strategies. Formal training sessions provided foundational technical skills and helped reduce anxiety. This concurs with Walzer et al. 42 who highlight the critical role of needs-based support programs in developing digital competency. Peer collaboration emerged as a powerful facilitator. Participants described how support from experienced colleagues built confidence and fostered mutual problem-solving. This aligns with Coffetti et al. 43 who found that interdisciplinary collaboration and end-user involvement significantly enhance nurses’ acceptance of digital tools. Also, self-directed learning was evident among nurses seeking independent mastery. This resonates with Mlambo et al.'s metasynthesis 44 underscoring the value nurses place on continuing professional development as integral to professionalism and lifelong learning.
Transition mechanism: Progression from learning to integration occurred when nurses could practice under graduated pressure—beginning with low-acuity scenarios that allowed procedural automaticity to develop before facing high-complexity situations.42,44 Without protected time for graduated practice, skills remained effortful and conscious, never achieving automaticity required for seamless workflow integration. 43 This explains why understaffed units showed prolonged learning phases—cognitive load remained high, blocking transition.
Structural barriers to learning
Skill acquisition was significantly constrained by time scarcity and workload pressure. Chronic understaffing and lack of protected training hours limited participation in formal learning opportunities.45,46 Some nurses felt pressure to self-learn during unpaid personal hours, causing frustration and resentment.47–50 This pattern represents both an ethical concern and practical barrier—when self-directed learning becomes an expectation outside compensated hours, it functions as unpaid labor contributing to burnout. Organizations must ensure that time for digital skill development is explicitly allocated within working hours rather than implicitly expected during nurses’ personal time. The absence of such protected time not only undermines fairness but serves as a demotivator prolonging resistance to digital transformation.3,4
The dark side of peer dynamics
While peer collaboration facilitated learning, our findings also revealed significant instances of non-collaboration. Some digitally proficient nurses actively withheld assistance, viewing it as additional unpaid labor. Generational tensions created barriers—older nurses reported feeling judged while younger nurses perceived older colleagues as resistant. These negative peer dynamics had substantial consequences: nurses experiencing non-collaboration reported prolonged learning phases, increased anxiety, and in some cases, complete disengagement.
This finding extends Coffetti et al., 43 who identified team-level influences on technology adoption but did not examine the consequences of negative peer interactions. However, it is important to acknowledge that while peer mentoring is valuable, over-reliance on informal peer support may create additional burden for nurses who are frequently sought out for assistance, potentially disrupting their own clinical responsibilities. 4 43 To address this concern, organizations should consider establishing dedicated digital support roles or ‘superuser’ positions with protected time specifically allocated for supporting colleagues during digital transitions. This approach ensures that support remains accessible while preventing the overburdening of individual nurses who possess strong digital skills. 41
Integration into clinical practice
As nurses developed digital competencies, they began integrating tools into daily workflows. This concurs with Irwin et al. 51 who explored how nurses integrate electronic medical records while maintaining patient care. Wilson et al. 52 highlighted that embedding digital infrastructure into routine care enhances workflow efficiency when implementation aligns with clinical contexts.
However, integration was uneven. For many, skill acquisition led to smoother workflows, but ongoing technical failures and lack of managerial responsiveness hindered full integration in some units. Shan et al. 53 found that frequent workflow interruptions and complex EHR tasks significantly increased nurses’ mental workload. Provenzano et al. 54 described EHR adoption as a “double-edged sword,” balancing enhanced data access with increased technostress.
Regression mechanism: Integration remained fragile rather than permanent because it depended on continuous favorable conditions. When conditions deteriorated—system updates disrupting established routines, manager turnover eliminating supportive oversight, or sustained high acuity overwhelming cognitive capacity—nurses reverted to deeply ingrained paper-based routines. This regression occurred not due to skill loss but because extreme pressure forced reallocation of cognitive resources to patient care.
Technical problems emerged as frequent barriers—glitches, crashes, and poor system usability interrupted clinical routines and eroded confidence. Time constraints further compounded challenges. Berlin et al. 55 suggested that tech enablement and better delegation could free up to 15% of nurses’ time. Aldhafeeri et al. 45 and Alsayed et al. 46 underline that excessive job demands and time pressure are key contributors to burnout. Alobayli 48 found that clinicians experienced stress linked to EHR use due to poor system usability. Asgari 49 noted that documentation demands contribute to clinicians working beyond their shifts.
Perceived lack of managerial support remained a concern. Burgess and Honey 41 emphasized that nurse leaders play crucial roles in bridging digital and clinical worlds—facilitating digital practice, advocating for staff, and providing ongoing support. Without such leadership, nurses felt isolated in navigating complex systems.
Sustained adaptation and transformation
Nurses described reaching a point where digital tools became integral to their professional practice. They attributed sustained adaptation to consistent managerial support and ongoing training. Leaders who allocated time for skill development, provided regular feedback, and maintained open-door policies for troubleshooting were instrumental in building confidence. Periodic refresher sessions helped adapt to system updates, preventing skill decay.
This echoes findings of Laukka et al. 56 who argue that effective digital leadership is characterized by ability to remove adoption barriers, create psychological safety, and align technology with clinical priorities. Konttila et al. 57 found that healthcare professionals’ digital competence depends on both skills and motivation to learn over time. Longhini et al. 58 demonstrated that sustained learning opportunities coupled with supportive team environments correlate with higher long-term digital proficiency.
From a theoretical perspective, these findings align with May et al.'s 36 Normalization Process Theory, emphasizing importance of collective engagement and continuous appraisal for embedding new practices. Sustained adaptation reflects these mechanisms—digital practice became habitual and nurses actively refined system use as part of professional identity. 59
Sustainability mechanism: Sustained transformation occurred only when continuous organizational reinforcement maintained nurses’ expectancy-value beliefs—confidence in ability to perform digital tasks effectively and conviction that the organization valued these efforts. When managers disengaged post-implementation, these beliefs eroded, triggering gradual regression even after months of successful integration. This explains why adaptation proved reversible: it required ongoing enabling conditions rather than one-time training interventions.
Internationally, Shiferaw and Mehari 60 highlight that in low-resource settings, sustained uptake can be hampered by limited infrastructure and baseline skills, even when motivation is high. Both infrastructure reliability and structured ongoing training remain critical—elements strongly emphasized by ICN 5 and WHO 10 as prerequisites for long-term digital transformation.
Strengths and limitations
This study makes a significant contribution to understanding nurses’ adaptation to digital transformation, particularly in developing country contexts where limited research exists on the subject. Using a grounded theory approach allowed for a nuanced, in-depth exploration of nurses’ lived experiences, enabling the emergence of the Progressive Digital Adaptation theory from the data rather than imposing a pre-existing framework. The use of semi-structured interviews generated rich qualitative data, capturing the emotional, cognitive, and organizational factors that shaped each stage of the adaptation process.
Another strength lies in the diversity of the sample, which included nurses from various departments, experience levels, and educational backgrounds. This diversity enriched the findings by revealing how different personal and professional contexts influenced movement through the stages of adaptation—including identification of both sustaining and struggling trajectories rather than presuming uniform progression. The study also addresses a gap in the literature by focusing on the unique challenges faced by nurses in resource-limited healthcare systems, where digital infrastructure, training opportunities, and managerial support structures may be less developed.
Additionally, the explicit focus on mechanisms enabling or obstructing transitions between stages, rather than merely describing stage characteristics, provides actionable insights for healthcare organizations implementing digital transformation initiatives.
Several limitations must be acknowledged. First, the findings are context-specific, as the study was conducted in a single private university hospital in Egypt. This may limit transferability to other healthcare contexts, including public hospitals, primary care settings, or healthcare systems in countries with different digital infrastructure, organizational cultures, or resource availability. The model may require cultural and contextual adaptation before application in other settings. Second, reliance on self-reported data introduces the possibility of recall bias or social desirability bias, which may have influenced how participants described their challenges or successes. Participants may have underreported difficulties or overemphasized positive adaptation experiences. Third, while the sample size of 30 participants achieved theoretical saturation and is adequate for qualitative inquiry, it may not fully capture the diverse experiences of the broader nursing population—particularly nurses with minimal technology exposure who may have been less likely to volunteer for research about digital systems.
Fourth, the cross-sectional nature of data collection captured adaptation experiences retrospectively rather than tracking nurses’ journeys prospectively over time. Longitudinal research could provide richer insight into the temporal dynamics of adaptation, including the stability of sustained transformation and triggers for delayed regression. Fifth, the theory represents the adaptation experience of nurses who engaged with the research process; nurses experiencing the most severe resistance may have declined participation, potentially underrepresenting the struggling trajectory. Additionally, the study focused exclusively on nurses’ perspectives and did not incorporate organizational leaders’ or IT professionals’ viewpoints, which could provide complementary insights into systemic factors shaping adaptation.
Conclusion
This study offers a grounded, in-depth understanding of nurses’ adaptation to digital transformation, mapping their journey through stages of initial resistance, skill acquisition, integration into practice, ongoing challenges, and sustained adaptation. The findings demonstrate that this process is not linear but shaped by a dynamic interplay of emotional, cognitive, and organizational factors, as captured in the Progressive Digital Adaptation theory. Critically, the theory identifies dual trajectories—sustaining and struggling—and explicates the mechanisms that enable progression or trigger regression between stages.
The results highlight that successful digital adaptation requires more than technical training—it demands sustained managerial support, accessible and reliable infrastructure, psychologically safe environments that encourage trial, learning, and collaboration, and protected time for skill development within working hours. When these conditions are met, digital transformation can lead to tangible benefits, including enhanced patient care, improved workflow efficiency, and greater professional satisfaction. When they are absent, even nurses who have achieved integration may regress to earlier stages of resistance or avoidance.
The study also draws attention to the distinctive challenges faced in resource-limited healthcare settings, where infrastructural constraints, limited training opportunities, and variable leadership engagement may hinder progress. Addressing these contextual barriers through targeted, context-sensitive strategies is essential to achieving lasting transformation.
By situating these findings within the Progressive Digital Adaptation theory, this research provides both a descriptive and actionable model for guiding healthcare organizations through the complex process of digital change. The explicit identification of transition mechanisms offers concrete targets for intervention. Future studies should further test and refine this model across diverse settings, ensuring its applicability and effectiveness in advancing nursing practice in the digital era.
Implications of the study
Based on the findings of this study, several recommendations can be made to support nurses in adapting to digital transformation.
For nursing practice
The findings emphasize the importance of structured, ongoing capacity-building for nurses to ensure that digital tools become an integrated part of clinical workflows rather than an added burden. Early resistance—driven by fear of errors, lack of confidence, and digital culture shock—can be mitigated through targeted orientation programs, peer mentoring, and simulation-based practice that occurs before nurses face high-acuity clinical situations.
Embedding digital competencies into continuous professional development frameworks helps maintain confidence and prevent skill decay. Additionally, fostering a psychologically safe environment where nurses can ask questions, experiment, and learn without fear of judgment accelerates adaptation and improves the quality of patient care. Organizations should recognize that adaptation is not a one-time achievement but requires ongoing support to maintain, particularly during system updates or periods of high workload pressure.
For nursing management
Managerial leadership plays a pivotal role in sustaining digital transformation. Leaders should allocate protected time for training within working hours—this investment is essential for several reasons. First, it demonstrates organizational commitment to digital competency as a valued professional skill. Second, it prevents the ethically problematic expectation that nurses learn complex systems during unpaid personal time. Third, it enables graduated practice that allows procedural automaticity to develop before nurses face high-complexity situations.
Specifically, organizations should consider the following: dedicated training time during orientation to new systems with reduced patient care assignments; protected time for practice and exploration beyond initial training sessions; scheduled refresher sessions when systems are updated; and recognition that digital competency development is part of professional paid work, not an additional activity that needs to be done during one’s free time.
Leaders should also provide accessible technical support, recognize staff achievements in digital competence to reinforce motivation, and ensure that system usability aligns with clinical needs. Incorporating principles from the Progressive Digital Adaptation model into change management strategies can help managers anticipate and address the cyclical nature of adaptation—acknowledging that progress may be disrupted by technical failures, workflow pressures, or staff changes. Management should establish feedback loops to address operational challenges quickly and prevent the erosion of expectancy-value beliefs that triggers regression.
For future research
This study highlights the need for further investigation into how contextual factors—such as educational background, gender dynamics, and healthcare infrastructure—influence the pace and depth of digital adaptation. Quantitative studies could examine causal pathways between adaptation stages, leadership behaviors, and patient outcomes. For example, research could test whether protected practice time (e.g., ≥2 hours/week) predicts faster resistance-to-learning transitions, or whether technical reliability thresholds (e.g., >95% system uptime) correlate with sustained integration.
Comparative cross-country studies would be valuable to explore how the Progressive Digital Adaptation model applies across different technological maturity levels and cultural contexts. Longitudinal research could assess sustainability of adaptation over time and the influence of evolving technologies on professional identity and clinical practice. Additionally, studies should examine factors differentiating sustained resistance from progressive adaptation, exploring whether alternative support mechanisms could facilitate adaptation for nurses currently excluded from the progressive trajectory.
Future research could be strengthened by integrating the Medical Research Council (MRC) Guidance for process evaluations of complex interventions, 59 which shares conceptual similarities with Progressive Digital Adaptation including attention to contextual factors, implementation mechanisms, and mechanisms of impact. Applying the MRC framework could support systematic validation of the theory through: investigation of dose-response relationships (e.g., sufficient protected time); identification of critical contextual moderators; and specification of implementation fidelity criteria. Additionally, intervention studies testing organizational strategies to facilitate stage transitions—and comparative research across different digital technologies (electronic health records, telehealth, clinical decision support systems)—would enhance both theoretical robustness and practical utility of the theory.
Footnotes
Acknowledgements
We extend our sincere gratitude to all the participants who contributed their time and insights to this study.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (2008). Ethical approval was obtained from the Ethics Research Committee of the Faculty of Nursing, Alexandria University (IRB approval No. [IRB00013620]). Prior to data collection, written informed consent was obtained from all participants, who were fully briefed on the study’s purpose, procedures, and their rights, including the right to withdraw at any point without any consequences.
Author contributions
All authors (Abou Hashish E, and Abdel Razek N) have substantial contributions to Conceptualization, Methodology, Software, Data curation, Writing- Original draft preparation Abou Hashish E: final manuscript draft and correspondence.
Contributing authors:
Study design: EA, NA,
Data collection: EA, NA.
Data analysis: EA, NA.
Study supervision: EA
Manuscript writing: EA, NA. Critical revisions for important intellectual content: EA, NA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is provided within the manuscript file.