
Abstract
Introduction
In modern dentistry, digital photography has revolutionized diagnostic practices, offering unparalleled precision and efficiency in disease detection and treatment planning. As a key imaging modality, intraoral photography provides high-resolution visuals essential for detailed caries assessment, which demonstrate greater sensitivity than visual examination of extracted permanent teeth, although overall diagnostic performance does not differ significantly between the two methods.1,2 This versatile technology is indispensable across dental specialties, including orthodontics for tracking alignment progress, caries diagnosis for early lesion detection, periodontics for monitoring gingival health, and aesthetic dentistry for precise smile evaluations and restorative previews.
Digital dental photography is a valuable aid for dentists in daily clinical practice, as well as in education and knowledge sharing. Among available devices, Digital Single-Lens Reflex (DSLR) cameras have long been applied due to their superior image quality and have been clinically standardized by the American Academy of Cosmetic Dentistry (AACD) since 2013. 3 More recently, mirrorless cameras have demonstrated several advantages over DSLR cameras, including reduced weight and dimensions (enhancing intraoral maneuverability), silent operation (reducing patient discomfort), improved autofocus capabilities, advanced video functionality, focus-peaking aids for manual control, and high-resolution sensors that capture fine intraoral details. 4 Notwithstanding the ongoing technological paradigm shift toward mirrorless systems, their adoption in dentistry remains limited, predominantly due to high initial costs. 4 In contrast, DSLRs remain the cornerstone instruments in dental photography owing to their established familiarity and reliability. Nonetheless, the clinical implementation of DSLRs is challenged by several factors, including complex photographic techniques, cumbersome data storage and transfer, and significant equipment costs.
With advancements in mobile technology, smartphones equipped with high-resolution cameras have emerged as potential alternatives for dental imaging. Their advantages include ease of use, convenience in information dissemination, and the ability to produce images that meet clinical standards. In terms of feasibility, smartphones offer additional benefits over DSLR photography, such as cost-effectiveness, significantly lighter weight, and rapid information exchange. 5 Several studies have validated the effectiveness of smartphone use. For example, Kohara et al. 6 found that clinical images captured using smartphones were more effective for remote caries diagnosis than those obtained with DSLR cameras. Estai et al. 7 concluded that smartphone photographs could serve as diagnostic tools for occlusal caries detection, comparable to conventional clinical examination. Moreover, smartphone photography has been widely utilized in artificial intelligence (AI)-driven diagnostics, with studies confirming its high accuracy, sensitivity, and specificity in the early detection of various dental pathologies, including dental caries.8–11
Despite these promising findings, the objective evaluation of smartphone image quality and color accuracy in dental photography remains limited. Existing studies have primarily focused on the diagnostic feasibility of smartphone-captured images rather than their technical precision. For instance, Kohara et al. 6 investigated the use of smartphone images for remote caries diagnosis and reported inter-examiner reliability of approximately 0.7 for all devices in a laboratory setting, compared with around 0.9 for iPhone images captured in vivo. The authors concluded that diagnostic imaging using smartphone photographs is feasible and accurate for distinguishing between carious tooth surfaces and advanced carious lesions. However, their study did not explicitly analyze the color accuracy and overall image fidelity of smartphone photographs. Similarly, a previous study by Saincher et al. 12 compared the image quality and color accuracy of photographs taken with digital cameras and smartphones for intraoral imaging. They reported that smartphones demonstrated superior image quality compared with DSLR digital cameras, with average No-Reference Matrix BRISQUE (NRM) scores of 20.59/100 for smartphone images and 18.45/100 for digital camera images. Nevertheless, the color accuracy of DSLR cameras was found to be superior to that of smartphones. It is important to note that this study lacked clinical relevance, as the images were captured without flash, potentially influencing the results.
Moreover, numerous prior investigations neglected to implement standardized clinical protocols, including controlled lighting, auxiliary flash systems, and objective image quality assessments via the BRISQUE metric. Consequently, their results may not accurately mirror real clinical contexts. Accordingly, the present study aims to conduct a comprehensive evaluation of the color accuracy and image quality of intraoral photographs taken with smartphone cameras, compared to those captured with DSLR cameras, under clinically relevant conditions. The null hypothesis states that there are no statistically significant differences in image quality or color accuracy among photographs captured with DSLR cameras, smartphones, and smartphones equipped with auxiliary lighting.
Materials and methods
Study design
A cross-sectional study was conducted on intraoral images of 40 participants aged 18 to 24 years, who exhibited no significant dental restorations, severe malocclusion, or visible oral lesions. Exclusion criteria included individuals with dental prosthetics, orthodontic appliances, severe gingivitis, or any condition affecting intraoral photography quality (e.g., excessive salivation or facial asymmetry). Written informed consent was obtained from all participants before study initiation.
The minimum sample size was calculated using the formula for estimating mean differences between two groups, based on the study by Saincher et al., which compared image quality between DSLR cameras and smartphone devices.
12

Reported mean BRISQUE scores were 19.39 (SD = 3.69) for DSLR and 20.44 (SD = 2.65) for smartphone images. Assuming α = 0.05, β = 0.2 (power = 80%), and K = 1, the calculated minimum sample size was 147 images per group. In the present study, this requirement was exceeded, as 200 images were obtained for each device (600 images in total), ensuring sufficient statistical power for analysis.
All photographs were captured in a standardized clinical environment with controlled patient positioning to promote methodological consistency across devices. Specifically, participants were positioned in an upright posture with the head aligned to the midline, and a standardized camera-to-tooth distance and angle were maintained. Lighting conditions were calibrated to emulate daylight-balanced illumination, incorporating a color temperature of approximately 5500 K,
13
a Color Rendering Index (CRI) of ≥90,
14
and ambient illuminance levels ranging from 1000 to 3000 lux, as measured at the dental chair.
15
Variability from supplementary operatory lighting was minimized, while all cameras were configured with invariant parameters for ISO sensitivity, aperture, shutter speed, and white balance. Uniform intraoral field exposure was further ensured through the application of standardized cheek retractors and mirrors. Three devices were selected for the study: a DSLR camera (Canon 6D Mark II, Canon Macro Lens EF 100 mm, Twin flash lighting) - Device A, a smartphone (Apple iPhone 12 mini, USA) with an auxiliary lighting device - Device B, and a smartphone using its built-in flash - Device C (see Figure 1). Photographic Devices: A. DSLR camera with Twin Flash; B. Auxiliary lighting device; C. Apple iPhone 12 mini.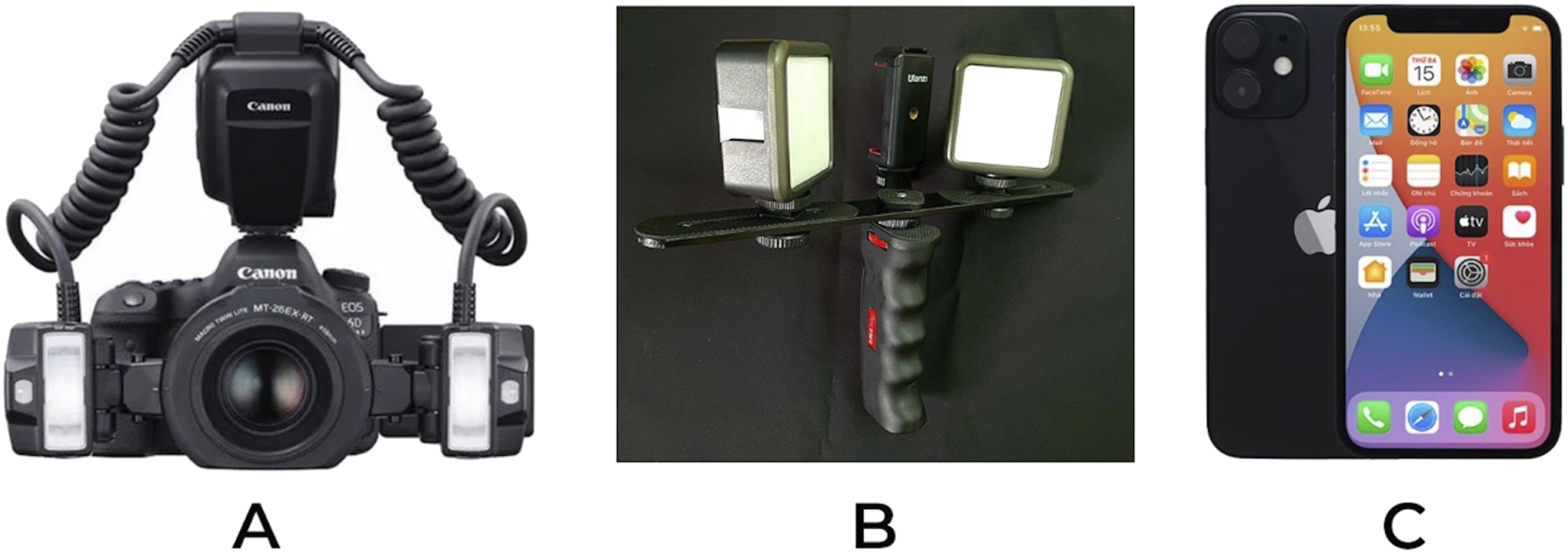
For each participant, five standardized images were captured per device: frontal, left lateral, and right lateral views with teeth in maximum intercuspation, plus occlusal views of the upper and lower arches, following the standards of the American Academy of Cosmetic Dentistry (AACD) and the guidelines of Irfan Ahmad.3,16 All images were saved under coded filenames that matched their identification numbers for digital record-keeping and subsequently transferred to secure storage. The final dataset comprised a total of 600 images, with 200 images captured using each device. (see Figure 2). Example of Photographs taken by 3 devices on the same object (frontal view): A1a. Photographs taken by DSLR camera; B1a. Photographs were taken by smartphone with an auxiliary lighting device; C1a. Photographs taken by a smartphone using its built-in flash.
Image assessment
All captured images were processed using the OpenCV software package
17
to extract the average L, a, and b values based on the CIE Lab color space; meanwhile, image quality assessment was performed concurrently using the No-Reference Blind/Reference-less Image Spatial Quality Evaluator (BRISQUE) algorithm, incorporating its No-Reference Matrix (NRM) variant. A ΔE threshold of >2.3 was employed to signify perceptible color differences, in accordance with prevailing standards.18,19 The resulting data were analyzed to compare image quality among devices and to calculate the color difference (ΔE) using the standard formula:

On the other hand, the images obtained from the three devices were evaluated by five dentists for their suitability in five clinical applications: diagnosing dental caries, classifying Angle’s malocclusion, storing orthodontic records, images for presentations, and exchanging tooth color information. Evaluations were conducted independently under blinded conditions, with all images anonymized and randomized by device. Using a standardized survey instrument featuring predefined response options, each evaluator selected the most appropriate image for each application. After selecting a digital record, each dentist visually reviewed images and commented on predefined assessments to distinguish differences in evaluation. This procedure would be repeated until an inter-examiner agreement is reached >80%, which was made following discussion. A Kappa value of at least 0.8 was required to ensure consistency and reliability among evaluators. 20
Statistical analysis
Numerical data, including NRM score, ΔE, L, a, and b values of all the obtained images, were processed using STATA software version 14 (Stata Corp. LP, College Station, United States of America). Data were normally distributed, and variances were homogeneous. Therefore, one-way analysis of variance (ANOVA) was applied to compare devices, followed by Tukey’s post-hoc test for pairwise comparisons. A significance level of p < .05 was considered statistically significant.
Results
Color accuracy analysis
Mean ΔE values between 3 devices.

ANOVA test for ΔE.

Note. p-value <0.05 are indicated
Lightness and chromaticity analysis
ANOVA test for the L values of images obtained from three devices.

Note. p-value <0.05 are indicated
ANOVA test for the a values of images obtained from three devices.
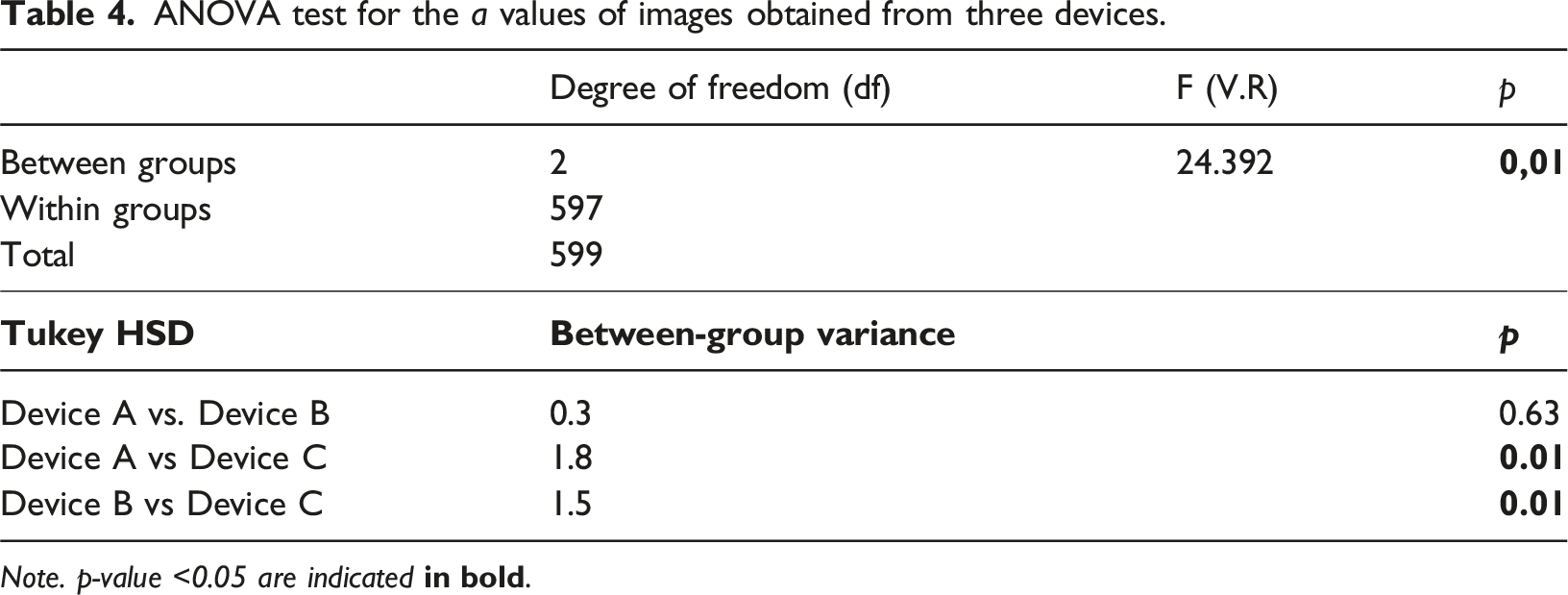
Note. p-value <0.05 are indicated
ANOVA test for the b values of images obtained from three devices.

Note. p-value <0.05 are indicated
Image quality assessment
The average NRM score of the three devices.

ANOVA test for the NRM score of images obtained from the three devices.

Note. p-value <.05 are indicated
Tukey HSD post-hoc tests confirmed significant differences between Device A and Device C (p = .00) and between Device B and Device C (p = .01), but not between Device A and Device B (p = .34) (see Table 7).
Expert evaluation
Expert evaluations highlighted significant differences in the perceived effectiveness of the devices for clinical applications (see Chart 1). Notably, the smartphone without auxiliary lighting (Device C) was deemed unsuitable for any clinical application by the evaluators. For caries diagnosis and presentation purposes, the DSLR camera was preferred in 96.67% of cases, with the smartphone with auxiliary lighting (Device B) chosen in only 3.33%. For Angle’s malocclusion classification, orthodontic record storage, and tooth color communication, Device A was selected in 60% of cases, while Device B was chosen in approximately 40%. Expert opinions.
Discussion
This study’s null hypothesis stated no statistically significant differences in image quality or color accuracy among images captured by DSLR camera, smartphones, and smartphones with auxiliary lighting. The results partially rejected this hypothesis, demonstrating that DSLR cameras and smartphones equipped with auxiliary lighting produced comparable image quality, whereas smartphones without auxiliary lighting performed significantly worse. The ANOVA analysis of No-Reference Matrix BRISQUE (NRM) scores revealed that images captured by the DSLR camera (Device A) exhibited significantly superior quality compared to those taken with a smartphone using its built-in flash (Device C) (Table 7), with average NRM scores of 45.32 and 53.14, respectively. This result demonstrates that images captured by DSLR camera have substantially fewer distortions compared to those of regular smartphones, highlighting the superiority of digital cameras in intraoral photography.
Several previous studies have investigated the feasibility of smartphone-based dental photography. For instance, Kohara et al. 6 reported that smartphone photographs could be reliably used for remote caries diagnosis, showing inter-examiner reliability comparable to DSLR under in vivo conditions. Nonetheless, their analysis did not include objective evaluations of color fidelity or standardized image-quality assessments. The present study extends these findings by revealing that, although DSLRs maintain superior color accuracy, smartphones augmented with auxiliary lighting yield clinically viable results.
Corroborating prior observations, Estai et al. concluded that smartphone-captured images could substitute for conventional clinical examinations in detecting occlusal caries. 7 In alignment with these findings, our expert evaluations indicated that smartphones with auxiliary lighting were deemed acceptable for orthodontic records and tooth color communication, although the DSLR camera retained preference for caries diagnosis and presentation images.
Saincher et al. 12 compared images captured using DSLR cameras and smartphones, reporting inferior image quality and color accuracy for smartphone images. However, the absence of standardized flash protocols in their methodology may have amplified these disparities. In contrast, the present study demonstrated that incorporating auxiliary lighting markedly enhanced smartphone image fidelity, thereby highlighting the critical role of uniform illumination standards in dental photography. Certain investigations have yielded divergent outcomes relative to our results. For instance, Moussa et al. 21 and Saincher et al. 12 observed no difference in image quality between DSLR cameras and smartphones; yet, both employed digital cameras in full auto mode without specialized dental flash lighting, which likely diminished DSLR camera performance. Analogously, Grigollo Patussi et al. 22 also demonstrated that DSLR cameras with dedicated flash systems produce higher-quality images, whereas those lacking specialized lighting performed worse than smartphones.
In the present study, the DSLR camera was standardized according to the American Academy of Cosmetic Dentistry (AACD) specifications 3 and utilized twin flash lighting, which may explain the disparity in results between our findings and those of other studies. The ability to precisely control camera settings and utilize specialized dental flashes ensures higher image fidelity in DSLR photography, further supporting its role as the gold standard in professional dental imaging despite cost and usability limitations.
Nevertheless, our study reveals some noteworthy findings. When combined with auxiliary lighting, the smartphone (Device B) captured images with quality nearly comparable to the DSLR camera (Device A), with no significant difference (47.62 vs. 45.32). This result underscores the considerable potential of smartphones with auxiliary lighting for intraoral photography. These devices retain all the advantages of smartphones, such as portability and ease of use, while producing images with quality comparable to DSLR cameras.
Regarding color accuracy, our results demonstrated significant color difference between DSLR cameras and smartphones with and without auxiliary lighting (mean ΔE = 18.98 ± 4.50 and 17.46 ± 5.30, respectively) (see Table 1). Specifically, the mean ΔE values between devices with overall values ranging from 17.4 to 19.3—far exceeding the clinically perceptible threshold of ΔE > 2.3,18,19 indicating that the color differences were readily visible to the human eye. Similarly, Giorgettti et al. 23 also reported nearly equivalent results when comparing the color accuracy of lesion photos captured by smartphones and digital cameras.
ANOVA analysis of CIE Lab color parameters showed that the L value of the images recorded from DSLR camera was significantly lower than that of smartphones (with/without auxiliary lighting), with differences of 18.7 and 16.9, respectively. This suggests that smartphones tend to capture brighter images compared to a DSLR camera. To improve the color accuracy of smartphone-captured images, photographers should consider lowering the L value, potentially by adjusting the intensity of all light sources (e.g., flash, auxiliary, and ambient lighting). Conversely, analysis of a (red-green) and b (yellow-blue) values showed no significant differences among the three devices. This finding indicates that smartphones can accurately reproduce certain color components, supporting previous studies by Yung et al., 24 which demonstrated that smartphones with external lighting systems yielded acceptable ΔE values for intraoral photography. However, further research is warranted to explore calibration techniques for mobile devices to enhance overall color accuracy.
The study by Saincher et al. 12 also identified a significant L-value difference between digital camera and smartphone images. However, their study reported a significant difference in b values, which was not observed in our study. This variation may be attributed to advancements in smartphone camera technology. The Apple iPhone 12 (2020) used in our study features improved lens quality, sensor calibration, and flash systems, whereas the Apple iPhone 6 (2014) used in the prior study lacked these optimizations.
From a clinical standpoint, expert evaluations revealed that images captured using smartphones without auxiliary lighting (Device C) were deemed unsuitable for clinical applications (see Chart 1). In contrast, the DSLR camera (Device A) was the preferred device for tasks requiring high image quality, such as dental caries diagnosis and presentation images. These findings align with prior research, including studies by Kohara et al., 6 Priyank et al., 25 Qari et al., 26 and Estai et al.,7,27 which demonstrated that smartphone-based intraoral images can be as effective as conventional clinical examinations in detecting caries. However, the continued preference for DSLR cameras in caries diagnosis may be influenced more by perception than by empirical evidence, as clinicians may assume that higher-end equipment is inherently superior for complex tasks. On the other hand, smartphones with auxiliary lighting can effectively support routine applications, such as Angle’s classification of malocclusion and orthodontic records storage. Notably, in tooth color matching, expert evaluations showed that smartphone images with auxiliary lighting had acceptable accuracy, with 42.67% of experts preferring smartphone images versus 58.33% favoring DSLR. These results suggest that smartphones with appropriate lighting enhancements can serve as viable alternatives for various dental imaging tasks. However, further expert consensus studies with larger sample sizes are recommended to establish standardized clinical guidelines for smartphone-based dental photography.
This study has several limitations. First, the modest sample size of 40 participants may limit the generalizability of the findings. Second, the evaluation was confined to a single DSLR model (Canon EOS 6D Mark II equipped with a macro lens and twin flash) and one smartphone model (iPhone 12 mini), thereby precluding extrapolation to other devices or emergent technologies. Additionally, the absence of a color calibration card necessitated reliance on relative, rather than absolute, color metrics, potentially introducing variability in interpretive accuracy.
To mitigate these constraints, future investigations should encompass larger cohorts, a diverse array of smartphone iterations and camera systems—including mirrorless variants—and rigorous standardization of procedural variables such as illumination and chromatic calibration. Such endeavors could further delineate applications in tele-dentistry, longitudinal treatment surveillance, and the synergistic integration of artificial intelligence for augmented clinical decision-making. It should also be noted that mirrorless cameras are progressively replacing DSLRs in clinical dental workflows. Despite similar requirements for auxiliary equipment and operator skill, future comparative studies should focus on mirrorless systems to refine the current evidence base.
Conclusions
In conclusion, this study demonstrates that smartphone-based dental photography, when performed with auxiliary lighting and appropriate color calibration, yields images of quality and colorimetric accuracy comparable to those captured with DSLR cameras. Although smartphones have not yet matched the diagnostic precision of DSLRs in demanding clinical scenarios, images obtained using smartphones with auxiliary lighting were deemed clinically acceptable by experienced practitioners for orthodontic documentation and shade matching. These findings support the adoption of properly optimized smartphone photography as a reliable, cost-effective, and portable alternative to conventional DSLR systems in routine dental practice, particularly in resource-limited settings where professional camera equipment is impractical or unavailable.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the School of Dentistry, Hanoi Medical University, for supporting the implementation of this study. Special thanks are extended to the participating students and staff for their cooperation during data collection. We also acknowledge the contribution of the dental experts who participated in the evaluation process. This study would not have been possible without their valuable insights and dedication.
Ethical considerations
This study was approved by the Hanoi Medical University Institutional Ethical Review Board (Ref. No.: HMUIRB1943, Date: May 23rd, 2025).
Consent to participate
Informed consent was obtained from all participants prior to the commencement of the study.
Author contributions
Conceptualization, Van Tuong Luu, Duc Long Duong; Methodology, Van Tuong Luu, Duc Long Duong;
Software, Van Tuong Luu, Huu Vi Hoang, Anh Dung Ho and Duc Phu Do;
Investigation, Van Tuong Luu, Huu Vi Hoang, Anh Dung Ho, Duc Phu Do and Manh Tuan Vu;
Data Curation, Van Tuong Luu, Huu Vi Hoang, Anh Dung Ho and Manh Tuan Vu;
Formal analysis, Huu Vi Hoang, Anh Dung Ho, Duc Phu Do and Manh Tuan Vu;
Writing – Original Draft, Van Tuong Luu, Duc Long Duong;
Writing – Reviewing and Editing, Van Tuong Luu, Duc Long Duong, Huu Vi Hoang and Manh Tuan Vu;
Visualization, Van Tuong Luu;
Supervision, Duc Long Duong.
All authors discussed the results, reviewed, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.