
Abstract
Introduction
Non-Communicable Diseases (NCDs) are long-lasting disorders that are not directly transmitted from one person to another, with the most common being heart disease, cancer, diabetes, and chronic respiratory diseases.1,2 NCDs are a major health crisis, causing over 41 million deaths annually, with a disproportionate impact on low- and middle-income countries (LMICs).3,4 A 2019 World Health Organization (WHO) report shows that LMICs account for 77% of all NCD-related deaths globally. 5 An estimated 23 million deaths per year are predicted to result from cardiovascular disease alone by 2030, with about 85% of those deaths occurring in LMICs. 6 80 percent of mortality in LMICs is related to diabetes mellitus and cardiovascular disease, and 90 percent is related to chronic obstructive pulmonary disease. 7 Like most of LMICs, NCDs account for high portion (44%) of all fatalities in Ethiopia. 8 In 2023, an estimated 554 per 100,000 people are affected, and an estimated 25 Ethiopians dying from NCDs every hour. Furthermore, NCDs are a major factor contributing to disability and DALYs (Disability-Adjusted Life Years), with millions of DALYs attributed to them in 2019.9,10 These estimates are comparable to those from the other low-income countries.11,12
The obesity pandemic, urbanization, aging populations, changing globalization-related cultural norms involving unhealthy lifestyles like smoking, and a decrease in physical activity are some of the factors contributing to the alarming rise in chronic illness and its widespread prevalence in developing countries.13,14 As part of the Sustainable Development Goals (SDGs), the United Nation (UN) has set a global goal to reduce the total premature mortality (among people aged 30-70) from NCDs by one-third by 2030 in an effort to slow down the fast-rising prevalence of the deaths. 15 However, no country is on track to achieve the global goal of a third fewer premature deaths from NCDs between 2015 and 2030. 16 Risk factor reduction, medication adherence, and counseling can largely prevent the morbidity and mortality associated with chronic diseases; nevertheless, their implementation might be difficult in nations with low resources. 17 In order for these to be affordable, widely available, and successful, especially for underprivileged populations, they need to be integrated into primary healthcare systems and tailored for low- and middle-income nations, which is difficult to accomplish. 18 To address this challenges the WHO acknowledges the potential use digital health technologies (DHTs) as distinct capabilities used to achieve health goals, particularly in the management of NCDs. 19
DHTs such as e-Health, telemedicine, mobile health, and wearable health devices are emerging as promising technologies to advance clinical care. 20 It comprise devices that serve as computing platforms, provide communication by creating networks, and serve as detectors and monitors for management of health and related problems. 21 It is a new and exciting approach that has the potential to improve health outcomes by strengthening medication adherence, disease prevention, diagnosis, treatment compliance, and clinic appointment remainder.22,23 DHTs integration into the healthcare delivery system for disease management programs will considerably save costs for patients and healthcare providers, as stated in a report by the Agency for Healthcare Research and Quality. 24 According to a 2015 overview study examining the use of telemedicine technology in the management of diseases, patients receiving telemedicine care for both infectious and non-infectious diseases report feeling more engaged and satisfied with their care. Additionally, patients said that using DHTs to attend remote appointments reduced travel time, saved them time, and decreased the number of missed workdays.25,26
The application of DHTs’ for preventative health initiatives and patient engagement that fill gaps in care for patients in vulnerable populations is receiving significant amounts of attention in several global health communities. 27 However, the report of WHO and other studies have highlighted the following barriers, which raise concerns regarding their impact and long-term viability, this includes a lack of financial support, lack of sound policy decision, lack of leadership abilities, connectivity, capacity building, lack of harmonized healthcare policy and governance models to support digital health initiatives, conflicting priorities in the field of medicine, unsustainable operating costs, an inability to consistently measure clinical and cost-effectiveness, a lack of information technology infrastructure to support digital health programs, patient literacy, privacy concerns, and cultural issues.28–30
The implementation of DHTs is made possible by several factors, including good knowledge of health technology, favorable attitudes towards electronic health (e-Health), and perceptions of stakeholders, trained and qualified staff, good perception of healthcare providers (HCPs) and their willingness to use the system, having national DHTs policy and governance models and adequate infrastructure.30–32 There is a great need for adequate digital infrastructural resources as well as enabling policies that favor digital health initiatives that are attuned to the sociocultural and cognitive needs of the population in the Sub-Saharan African (SSA) context. 33 The adoption and effective use of digital health technology in the management of chronic medical conditions in SSA can only be of value to the population if there is an enabling environment.34,35
To deliver rapid, evidence-based, high-quality healthcare services, the Ethiopian Ministry of Health is currently working with other stakeholders to computerize the healthcare system. 36 The information revolution, the biggest efforts in health information and communication technology is one of Ethiopia’s four agenda’s for the health sector transformation plan and a national digital health strategy for the adoption of DHTs in NCDs management is also the greatest moves in digitization of the health system. 37 This indicates the government’s strong determination to a paradigm shift towards the application of DHTs in healthcare delivery systems. 38 Although Ethiopia’s healthcare delivery system has seen tremendous advancements and initiatives in the use of DHTs, particularly in the prevention and management of chronic diseases, no major changes have been made, and no systematic research has been conducted to date to evaluate the barriers to the use of DHTs in this regard. Therefore this review aims to assess the barriers and facilitators to digital health technology intervention for chronic disease management in Ethiopia.
Review questions
The PICOS (participants, interventions, comparisons, outcomes, and study design) approach was used to develop a review question to guide the search strategies and it’s structured as follows: (1) What evidence exists on the use of digital health technology for chronic disease management in Ethiopia? (2) What are the key barriers and facilitators of digital health technology interventions for chronic disease management in Ethiopia?
Methodology
A team comprising of experts from the relevant disciplines (NCDs management, health informatics and digital health expert, and systematic review methodology) was designed, conduct and report the systematic review. The process of the review was followed the methods described in the Cochrane Handbook for Systematic Reviews. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) reporting standard was used in this systematic review final report writing. 39 The review was registered on PROSPERO with the registration number of CRD42024582359 and the full protocol was not prepared or published.
Search strategies
A bibliographic database of CINAHL Database, MEDLINE (PubMed), Cochrane library, and other gray literatures was searched between March 2024 and June 2024 in order to find studies that had been conducted in English and published in peer-reviewed journals between January 2010 and June 2024 concerning digital health technology, mainly wearable health devices, e-Health, mobile health, and telemedicine and their barriers and facilitators for the management of chronic diseases like cancer, diabetes, cardiovascular disease, lung diseases, and mental disorders.
Medical Subject Headings (MeSH) for database searching and Boolean terms (AND/OR) were used to separate our keywords. The search term for this review was developed by review of previously conducted reviews on this area13,33,40–42 and it’s organized as follows: “Barriers”, “facilitators”, “digital health”, “digital health technology”, “wearable health devices”, “telemedicine”, “Tele care”, “digital-care”, “e-Health”, “e-health”, “electronic health”, “mobile health”, “mobile health applications”, “utilizations”, “implementation”, “chronic”, “non-communicable”, “NCD”, “disease”, “diabetes“, “DM”, “cancer”, “cardiovascular disease”, “CVD”, “lung disease”, “management” and “Ethiopia”. Additional relevant articles were identified by searching the reference lists of full-text articles studies published from conception to the last searched date of June, 2024, were included.
Inclusion and exclusion strategies
This review examined the implementations, barriers, and facilitators of wearable health devices, e-Health, mobile health, and telemedicine for the management of cancer, diabetes, cardiovascular disease, lung diseases, and mental disorders in Ethiopia. This study included both quantitative and qualitative research that was published in peer-reviewed journals in the English language. Scoping reviews, systematic reviews/meta-analyses, case studies, single views or “perspective” articles, preprint publications, abstracts that only described the technology without identifying study participants, and articles that were not exclusively focused on NCDs were all excluded from the review.
Selection of studies and quality appraisal
Four authors (JBA, AAA, SMD and ADW) were searched and evaluated the quality of the studies included in the review. Screening of titles, abstracts, and full texts was conducted independently by two review authors (JBA and AAA). A disagreement regarding the decision against the inclusion of articles between the two reviewers was resolved by consensus or the third reviewer (DNM). A second reviewer (SDK) was blinded to the primary reviewer’s (JBA) decision for checking articles selection and data extraction. Any differences of opinion were discussed; otherwise, a third reviewer (DNM) was available to arbitrate any issues that remained unresolved. The Joanna Briggs Institute (JBI) framework was employed for assessing the study quality. 43 A quality assessment criteria with categories of low (<49%), medium (50–79%), and high (80–100%) study quality were developed for assessing the quality of studies included in the final report. Studies were not excluded based on their quality; however, this information guided the narrative synthesis and discussion.
Data extraction and processing
Data extraction and result comparisons were carried out by three authors (JBA, AAA, and SMD). Decisions were made by the third reviewer (SDK) or through discussion to settle disagreements. To gather, analyses, and summarize data from studies, a standardized data extraction form in Microsoft Excel was utilized. Comprehensive data was extracted from the included studies using the following three key headings: (1) the study description, which included the authors, study setting (region), and the years of publications; (2) the methodology, which included the study characteristics, such as the study design, participants, mean or median age of the participants and sample size; (3) the results, which included types of digital health technology under consideration, the outcomes of interest, and the barriers and facilitators of digital health technology for the management of cancer, diabetes, cardiovascular disease, lung diseases, and mental disorders in Ethiopia; and (4) the quality of each studies which is grouped as high, medium and low quality based on JBI quality assessment criteria.
Due to the heterogeneity of studies, a narrative synthesis approach was used to collect, synthesize, and map the literature. 44 The following categories were used to synthesize the studies: (1) available evidence on use of wearable health devices, e-Health, mobile health and telemedicine for the management of cancer, diabetes, cardiovascular disease, lung diseases, and mental disorders in Ethiopia; (2) barriers and facilitators to the implementations of wearable health devices, e-Health, mobile health, and telemedicine in the management of cancer, diabetes, cardiovascular disease, lung diseases, and mental disorders in Ethiopia.
Data synthesis and analysis
Result synthesis was conducted using the information reported in the studies characteristics. A descriptive thematic analysis was employed to provide more complete picture of the evidence by identify and categorize the various findings in the included studies. This helps to map the range of strategies employed to prevent barriers in the use of DHTs for the management of cancer, diabetes, cardiovascular disease, lung diseases, and mental disorders in Ethiopia. The findings were presented through tables and diagrams in a narrative format, summarizing the key themes and providing a comprehensive overview of the current evidence.
Ethics consideration
Since the data were collected from publicly available materials, this study does not require ethical approval.
Result
The primary search strategy was yielded potentially 2224 articles from PubMed, Cochrane library, through HINARI search and gray literatures like Google scholar. After duplicates were removed, 798 articles were remained. Of these, 694 articles were excluded after review of their titles and abstracts. The remaining 104 articles were assessed for inclusion criteria and 92 articles were excluded, primarily because the study was conducted in another country or because the outcome was not reported or not solely focused on NDs. Overall, 12 were included in the final review (Figure 1). Flow chart of study selection.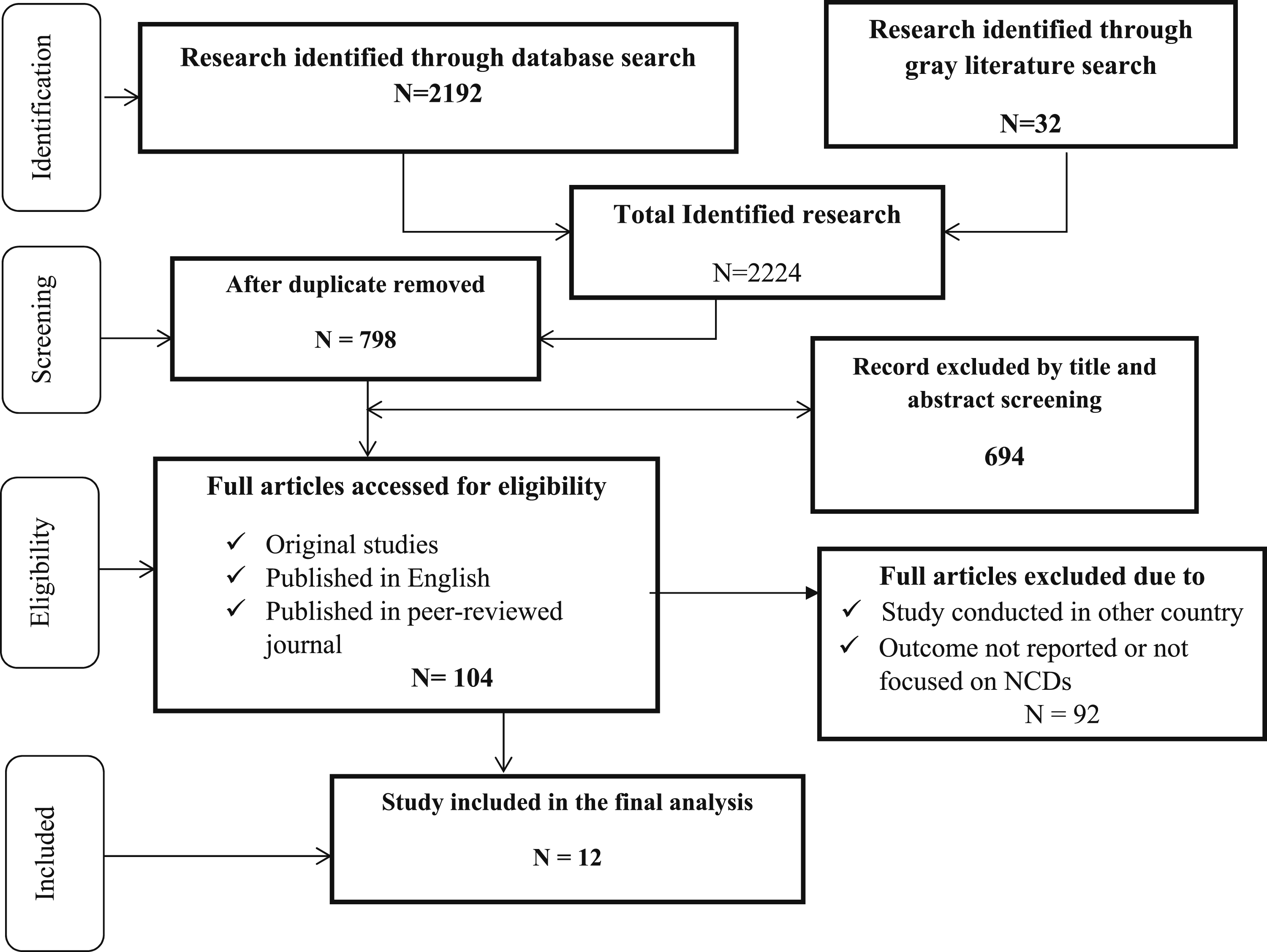
Characteristics of reviewed studies
This review included studies with publication years ranged from 2019 to 2023; with an overall increase in articles published more recently. None of the studies published before 2019 met our inclusion criteria. Twelve (12) studies were included in the final review fulfilling the inclusion criteria. There was heterogeneity in the studies in terms of the study region, study design, outcome of interest and study participants In terms of study area, majority 6 (37.5%) was conducted in Amhara region45–49 and Addis Ababa.34,35 In terms of study design, all of the included studies were cross-sectional34,35,45–54 of this one was conducted using mixed method. 52
Studies included in the systematic review of barriers and facilitators of DHTs intervention for management of chronic disease in Ethiopia.

Note. SD means Standard Division, IQR means interquartile range, SNNP means Southern Nations, Nationalities and Peoples.
Barriers and facilitators to digital health technology intervention for management of chronic disease in Ethiopia
Poor socioeconomic and income conditions,52,54 female gender, age (older) and increase in work experience,
46
were among the socio-demographic barriers to DHTs intervention in chronic disease management. Poor knowledge34,48,52 and attitude towards digital health technology,34,35,46,53 subjective norm, poor habit to use e-Health technology,
53
lack of trust in technology, resistance to accept new services,
52
poor interest of using digital health applications,
50
lack of experience in supporting patients through digital tools,
47
lack of computer-related training,
47
poor computer literacy,34,48 and poor awareness about the availability and importance of online health resources48,50,52,53 were among personal or behavioral factors frequently reported to affect DHTs interventions in chronic disease management in Ethiopia. Lack of access to necessary hardware and software technology and technology inequality,34,35 poor internet access,50,52 poor access to electricity, network, smart phone and computer were also the most frequently reported organizational and technological barriers to DHTs interventions in chronic disease management50,52,53 (Figure 2). Barriers to DHTs interventions in chronic disease management.
Lower age group,52,53 male gender,
46
higher income level,
48
an increase in educational level,45,48,52 being a government employee
48
and urban residence48,53 were among the socio-demographic facilitators of DHTs intervention for chronic disease management in Ethiopia. Perceived usefulness and ease of use,51,53 perceived innovativeness,46,47 performance expectancy, effort expectancy, access to health care facility,
52
good knowledge about digital health services,34,52 having computer, telemedicine applications and e-Health technology related training,34,35,46 having positive attitude toward online medical resources, e-Health technologies and telemedicine,34,35,47–49 current use of mobile phone for appointment remainder and adherence support,
45
practice of supporting patient by electronic and frequency of searching health-related information online were also the most important personal/behavioral facilitators
46
and improved access to internet, computer and digital health tools47,50 and necessary technological resources,
35
computer access at work,
46
and technological and operational resource readiness, were the most widely reported organizational and technological facilitators of DHTs intervention for management of chronic disease in Ethiopia (Figure 3). Facilitators to DHTs interventions in chronic disease management.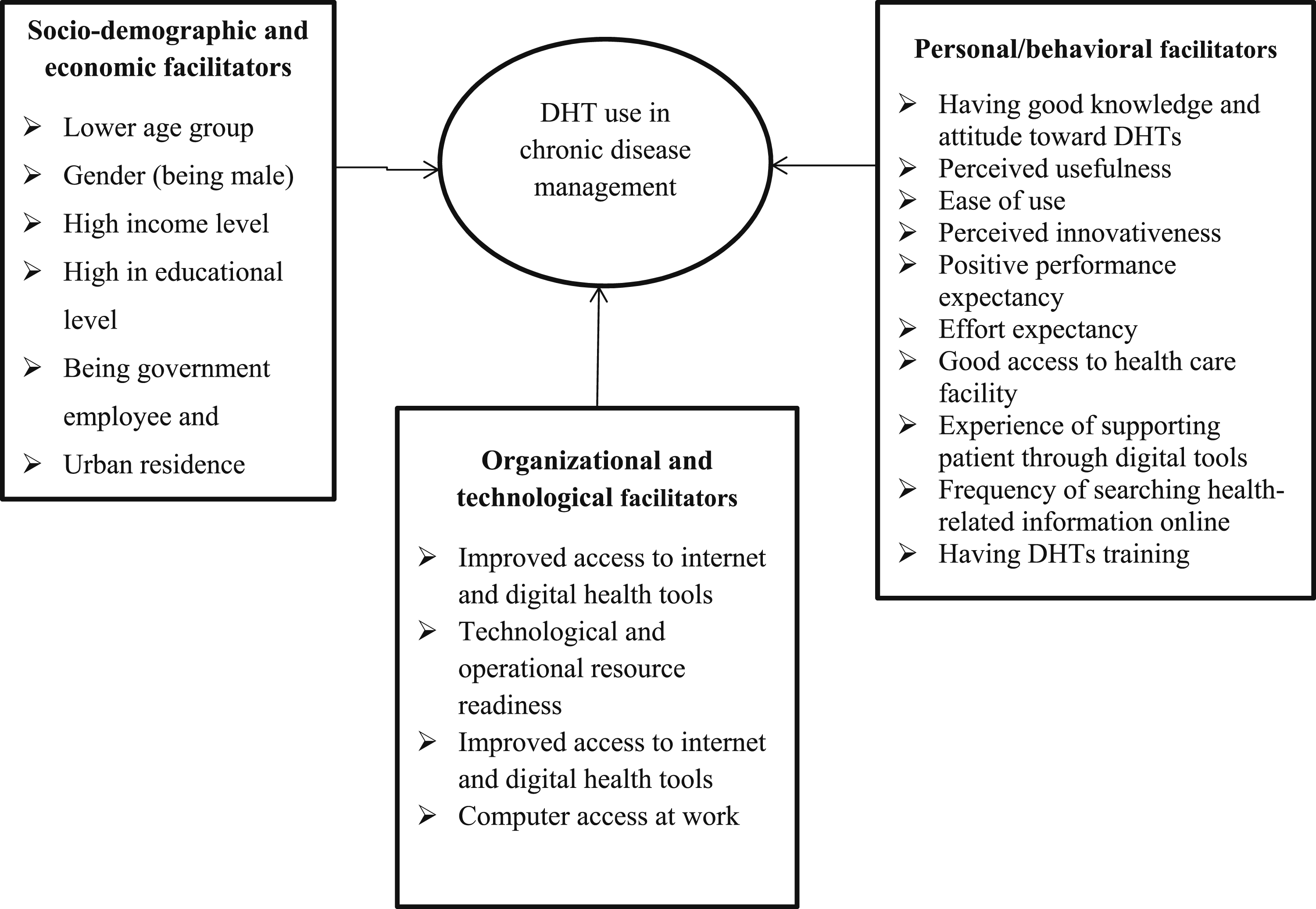
Based on the types of the digital health technology, poor knowledge and negative attitude towards mobile and e-Health technologies, subjective norm, performance, and effort expectancy, lack of trust in technology,51,53 poor access to internet, electricity and mobile phone, resistance to accept new services, poor awareness about DHTs, lack of satisfaction toward mobile phone services and poor habit of digital technology use49,51,52 were the most widely reported barriers of mHealth and e-Health technology intervention for chronic management in Ethiopia. Similarly, poor access to internet and necessary hardware and software technology, poor technology literacy, poor knowledge and attitude towards telemedicine, lack of training on telepsychiatry and poor interest of using health technologies34,35,46,50 were the most frequently reported barriers to telemedicine, telemonitoring and telepsychiatry intervention for chronic disease management in Ethiopia.
Perceived usefulness and ease of use,51,53 good computer and internet access, 51 good knowledge, attitude and intention about e-Health services, and having training on digital health technologies45,49,52 were the most widely reported facilitators of mHealth intervention for chronic management. Similarly, perceived innovativeness, good knowledge and attitude toward digital health service, access to necessary technological resources and computer use at work, having training and positive perception towards DHTs34,35,46,50 were the most frequently reported facilitators to telemedicine, telemonitoring and telepsychiatry intervention for chronic disease management in Ethiopia.
Discussion
A systematic review can aggregate a significant amount of literature on a specific topic, guide future research, and provide a solid basis for medical decision-making and policy development by using objective methods to gather and analyze data from primary studies. 56 In this context, this review evaluated 12 articles that met the inclusion criteria to compile evidence on the barriers and facilitators of implementing digital health technology for managing chronic diseases in Ethiopia. To our knowledge, this is the first systematic review to collect, cluster, and synthesize quantitative, qualitative, and mixed methods literature on barriers and facilitators to the intervention of digital health technologies by patients and healthcare professionals at all levels of care. Studies under consideration were conducted among healthcare providers and patients focusing on mobile health (mHealth), telemental-health/telepsychiatry, telemonitoring, wearable health device and telemedicine utilizations for chronic health condition management in Ethiopia.
The result of this review indicates that, the use of digital health technologies for the management of chronic disease is associated with socio-demographic factors like, low income status, and poor socioeconomic condition, older age, rural residence and increase in work experience.48,52,53 This finding is consistent with the result of systematic reviews conducted elsewhere57,58 which revealed a substantial connection between use DHT for patient management and socioeconomic status, work experience, and age. Therefore, focusing on these demographic factors should be given attention in the process of digital health technologies implementation for chronic disease management in middle and low income countries. 59
Similarly, factors such as lack of access to necessary hardware and software technology and technology inequity, poor internet, electricity, smartphone and computer access34,35,50,52 were the most frequently reported organizational barriers to DHTs interventions in chronic disease management.50,52,53 These findings are consistent with previous research, 60 which revealed that telecommunication infrastructure is critical for the sustainability of DHTs intervention programs. Another study found a similar outcome. 61 The authors highlighted that the availability of sufficient infrastructure to support the use of DHTs should be investigated. 61 Technological barriers made DHTs impossible to operate and they ended prematurely. 62 As a result, DHTs cannot be sustained in these circumstances, necessitating continued learning and problem-solving, ongoing adaptation of interventions with a primary focus on the fit between interventions and multi-level contexts, and expectations for ongoing improvement rather than diminishing outcomes over time. 63
The review found that personal factors such as poor knowledge and attitude towards digital health technologies, poor habits with e-Health technologies, lack of technology trust, resistance to accepting new services, and a lack of training on digital tools were frequently related to the use of DHTs in managing chronic diseases in Ethiopia.34,35,46–48,50,52,53 Consistent with our findings, a systematic review of 101 studies assessed factors influencing the uptake of DHT by clinicians across multiple diseases 64 indicated that the most common challenges for healthcare providers were inadequate reimbursement and inadequate technology for DHTs adoption. In similar vein, other reviews suggested that the limiting factors for the broad use of digital health technologies are associated with users’ concerns about increased workload and altered workflow, which could hinder the sustainability of the digital health technologies. 65 Furthermore, perceptions of these newly introduced technologies would require implementation, training, access, adaptation, and establishing stages were revealed to be key variables. 66
The most commonly reported personal/behavioral facilitators of DHTs intervention for the management of chronic diseases were perceived usefulness, ease of use, innovativeness, effort, and performance expectations, the use of computers at work, experience of digital health support to patients and good knowledge and attitude toward e-Health technologies and telemedicine.34,35,45–49,51–53 Consistent with our findings, the study 64 discovered that the most common facilitating factor for healthcare providers was the perceived usefulness and ease of use of DHT. A comprehensive scoping analysis of 36 trials was also examined the parameters associated with DHT use for hypertension control. 67 In-line with our findings, this research discovered that effort and performance expectancy, easy-to-use technology and improved patient-clinician contact were facilitators of DHT uptake in patients.
Moreover, e-Health technology related training, improved access to the internet and digital health tools, readiness to use technology and digital resources and good access to health care facilities were among the most important organizational facilitators of DHTs use for chronic disease management.19,35,46,47,50,52 A recent literature review analyzed conceptual models and discovered commonalities between the constructs used to explain DHTs adoption and use. 68 Our thematic analysis results aligned with many of the common constructs. For example, facilitating conditions such as digital technology related training, internet availability and technological support were shared by all frameworks, 68 all of which we identified as facilitating variables for DHTs adoption and its long-term sustainability. The similarities between our findings and pre-existing frameworks indicate that there may be common barriers and facilitators to DHTs implementation. Thus, concerted initiatives to address these variables may increase DHTs utilization in NCDs management in low and middle income countries.
Strength and limitations
Regardless of the comprehensive results obtained, this study has certain limitations. First, the search technique used in this systematic review excluded certain publications (such as dissertations, conference proceedings, and so on). Second, the analysis only considers articles published in English-language, potentially excluding additional empirical evidence. Third, our review did not cover all papers published before 2010. It is difficult to pinpoint the precise historical time when various digital health tools first became widely available. In addition, the study’s cross-sectional nature and limited number of included studies may limit its generalizability. Finally, the inclusion of research on patients and healthcare professionals that focuses on different digital health technologies may mask important distinctions in the ways that each group experiences digital health interventions, as well as the main barriers and enablers for each group. Despite these limitations, the included studies were enabled us to undertake an updated review of recent literature and identify characteristics influencing the usage of DHTs in chronic disease management in Ethiopia and developing countries.
Conclusion and recommendations
This review aims to systematically analyze the barriers and facilitators affecting the use of DHTs in managing chronic diseases. It also provides an overview of current digital health interventions for chronic disease management in low- and middle-income countries. The findings indicate that socio-demographic factors such as poor socioeconomic and low income, older age, rural residency, and extended work experience influence the implementation of DHTs for chronic disease management in Ethiopia. Personal or behavioral factors, including a lack of understanding and negative attitudes toward digital health technology, subjective norms, poor e-Health usage habits, and mistrust in technology, were significant barriers. Additionally, organizational and technological barriers such as insufficient access to necessary hardware and software, technological disparities, inadequate internet connectivity, and limited access to electrical power, the internet, smartphones, and computers were the most commonly reported barriers to DHT interventions for chronic disease management.
In this review facilitators for the use of DHTs in managing chronic diseases include several personal and organizational factors. On the personal side, important aspects are the perceived usefulness and ease of use of the technology, its perceived innovativeness, effort expectancy, a positive attitude towards online medical resources, e-Health technologies, and telemedicine, as well as having good knowledge and experience with mHealth services. Performance expectancy, access to a computer, and training in telemedicine applications and e-Health technology also play a role. Organizational and technological facilitators include improved internet access, availability of digital health tools, readiness of technological and operational resources, good access to healthcare facilities, availability of computers and necessary technological resources, and the practice of supporting patients through electronic tools. The result of this review demonstrated that, in developing nations like Ethiopia, where there is a scarcity of healthcare providers in rural and remote areas, the use of digital health technologies for the management of chronic diseases is feasible. Additionally, the integration of DHTs into the health care system has the potential to strengthen the weak health care delivery systems and promote universal health coverage.
This systematic review offers several recommendations, emphasizing the need to address potential barriers and facilitators throughout different phases of DHTs initiatives. Factors such as perceived usefulness and ease of use, good knowledge and positive attitudes toward DHTs and online medical resources, access to digital health tools, training, and technological resources are essential. Addressing technological disparities, inadequate internet connectivity, and limited access to electronic resources is crucial for enhancing the design, implementation, scaling, and sustainability of DHTs. Therefore, promoting the identified facilitators for sustainability and swiftly addressing barriers with targeted strategies is crucial. This approach will enhance the design, implementation, scaling, and sustainability of DHTs. Considering these factors, developing strategies to boost future effectiveness while focusing on the sustainability of DHTs is essential. Additionally, further study is necessary to determine the barriers and facilitators of particular digital health technologies from the perspectives of particular stakeholders, including patients, caregivers, and policymakers.
Footnotes
Acknowledgments
We would like to thank all the authors of the studies included in this systematic review.
Authors’ contributions
JBA developed the protocol, established the search strategy, and was involved in designing, selecting study data, analyzing and developing the initial manuscript drafts. ADW, SMD, DNM, and SDK were involved in the selection of studies, data extraction, and quality assessment. JBA prepared the subsequent drafts and prepared the final draft of the manuscript. All authors have read and approved the final draft of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.