
Abstract
Introduction
Implementing large-scale health information systems (HIS) is undoubtedly a challenging task. Not only are old technologies replaced by new ones, but workflows and work practices must change accordingly. Large-scale HIS implementations therefore imply a profound sociotechnical change that may lead to changes in professionals’ roles, patterns of work and organisational culture.1–3 Furthermore, implementations go through phases, with prior phases influencing latter ones. Hertzum 3 describes three phases of implementation: preparations, which consist of planning the activities initiated by the decision to adopt the system; going live, which involves the initial planned change; and continuing design during use, which can be seen as a long, improvisational process in which users learn about the system and uncover new opportunities and changing work practices. Due to these complex, lengthy and unpredictable processes, large-scale implementations are difficult to carry out successfully. 4
Hospitals and municipalities in Central Norway are implementing a new cross-sectoral electronic health record (EHR), which is regarded as a realisation of the national policy ‘One Citizen, One Health Record’. 5 This policy aims to enable access to patient health information across specialist and municipal healthcare services, thereby facilitating more seamless treatment and care. The new EHR implies radical shifts in work practices, such as new workflows, real-time documentation and structured documentation. As such, it is a good example of a large sociotechnical change process, where the risk of failure is high.
To improve the chance of successful implementation, it is generally recommended that organisations and individuals prepare and ‘get ready’ for the new technology.6,7 Thus, this paper explores how hospital staff prepared for the new EHR and how expectations were met during initial use.
Preparing for change
Individuals’ and organisations’ expectations, preparations and readiness have been studied across different disciplines and from different perspectives. Implementation studies provide an overview of a broad range of factors that influence an implementation process, and several frameworks have been developed for capturing such processes.8–11 These frameworks typically diverge in terms of adopters (e.g., healthcare professionals), technology (e.g., an EHR system), organisations (including capacity to innovate and work needed to implement change), and contexts (e.g., socio-cultural, political, legal aspects).8,12 By investigating such factors and their relationship at various stages of the implementation process, such as during the stage of preparation or pre-implementation, go-live or implementation, and sustainability, 13 we can get a better understanding of each of these stages.
Some research has specifically focused on preparation processes or organisations’ readiness for change. Readiness for change is key to successful change. This is also the case in EHR implementations.9,14,15 Many organisations therefore invest in preparing themselves for change through readiness programmes.
Organisational readiness for change is a multifaceted and multilevel construct encompassing both individual and organisational aspects. 14 Broadly speaking, individuals’ readiness for change concerns their capacity and commitment for change. 16 More specifically, Austin et al. 7 discuss individual readiness based on five elements identified in the literature: discrepancy (perception of need for change), appropriateness (the proposed intervention is the adequate response to the need for change), valence (an individual’s assessment of whether the change is beneficial and, if so, worthwhile), self-efficacy (an individual’s confidence in their ability to participate in and implement the change successfully) and fairness (procedural fairness: how decisions on the change are made and whether those being affected had the opportunity to express their views; distributive fairness: an individual’s perceived equity in resource allocation). On an organisational level, readiness refers to the shared capacity and commitment to implement change. 17 Organisational readiness comprises elements such as available resources and expertise, as well as vison clarity, change appropriateness and organisational conflicts and politics.14,15
Furthermore, the sociology of expectations is relevant for understanding preparations for implementation, as it addresses future users’ expectations and how they shape the design and development of new technologies.18,19
Expectations have been shown to be ‘performative’ or ‘constitutive’ of the desire to purchase a product 20 and the actual use of it. 18 For example, in a study of Norwegian general practitioners (GPs) and their expectations toward a prospective electronic health record, the authors discuss experiences that shape the GPs’ expectations. These included satisfaction with their current systems, accounts of negative user experiences with the prospective system from other users, and uncertainty about the inclusion of GPs needs in the new system. In summary, these experiences led to skepticism about investing in and implementing the new EHR. Ensuring that users have realistic expectations is, therefore, key for those responsible for implementation. 20
Moreover, Bozan and Berger 21 show how clinician’s expectations of the information quality (e.g., completeness, accuracy, timeliness) impacts their satisfaction with a clinical information system. If the perceived quality is lower than the expected quality, they tend to develop work arounds, resulting in using the system in unattended ways.
The development of a technology involves a dynamic between promises and requirements. When users learn about promises, they expect something like what has been promised. However, disappointment seems to be built into the way expectations operate in science and technology. 18 Moreover, expectations, including the future uncertainty of the technology, vary between different groups, such as developers and end-users. This may be related to the differences in end-users’ and developers’ level of knowledge or the possibility of influencing technological development (or process). 18
In sum, organisations’ and users’ preparations for implementation influence the implementation process. Simultaneously, expectations may contribute to investments in preparation activities and in perceptions of the developed technology.
Setting
Our study took place in Central Norway, where, in 2019, the regional health trust signed a NOK 2.7 billion (EUR 270 million) contract with the Epic Systems Corporation to implement the Epic EHR suite. The choice of Epic was a result of a tendering process; a formal procedure where bids on a new EHR from external suppliers were invited. The tendering process was driven by the implementation of the national policy ‘One Citizen, One Health Record’ 5 which mandated the adoption of an EHR system capable of being utilised across hospitals and municipal healthcare services. Nine hospitals and the largest municipality in the region were the first entities to sign up for the new EHR. Other municipalities in the region can opt to implement the system. Currently, 28 municipalities have implemented the system, while an additional 34 municipalities are expected to do so in the near future. Municipalities are responsible for primary healthcare, such as nursing homes and home care services, and the new EHR enables the sharing of information across municipalities and hospitals within the same EHR. General practitioners are currently not offered the system – a version better adapted to their requirements is pending.
Epic is a relatively self-contained EHR system providing most of the functionality needed by health personnel – either in ready-to-use form or through configuration – to meet various health professionals’ needs. 22 The system has been extensively configured, but researchers have questioned the representativeness of health professionals’ involvement in the configuration. 23
Main preparation activities relevant for hospital staff, including organisational readiness activities and training.

Training on the new EHR system was a central component of the readiness program for end-users, organized by the Health Platform organization. As summarized in Table 1, end-users were invited to 2-day classroom courses tailored to their professional roles, such as ‘mental health: nurses and healthcare workers,’ ‘surgery – orthopaedics: physicians,’ and ‘internal medicine: clerical staff.’ Typically, 8–12 participants attended each course. The training was delivered by health professionals with backgrounds similar to those of the attendees, with a super user assisting the instructor. The courses followed a traditional classroom format, where the instructor presented the EHR system, its functionalities, and the most common workflows step-by-step. Participants then worked through tasks in the system based on case cards. These courses were designed to provide a basic understanding of the system. In addition to the classroom sessions, e-learning courses—covering various workflows—were mandatory and available both before and after the classroom training. It was up to the managers in the different hospital departments to determine how to facilitate staff access to e-learning and ensure completion of the training.
In the period before and after the go-live, the EHR system was frequently discussed in the local newspaper. The majority of the comments were critical of the decision to purchase the Epic EHR system, with previously reported negative experiences with the system in Denmark cited as a key reason (see e.g., 24 ).
Materials and methods
This paper draws on data collected in the ongoing project ‘Realising the shared electronic health record: a multi-site study of a region-wide implementation’, which analyses the implementation of the Epic EHR in Central Norway. This paper focuses on expectations and organisational readiness and uses insights from semi-structured interviews.
Interviews are a suitable method for capturing people’s experiences, beliefs and attitudes. We adopted a semi-structured approach because it allows for flexibility and provides study participants with the opportunity to address topics they deem relevant. 25 We developed one interview guide for clinicians and one for the members of the implementation team. The clinician interview guide contained questions about preparations, training, experiences with using the system, their general impression of the implementation process, and their expectations for the future use of the system. The implementation team interview guide contained questions about their work tasks, collaboration partners, stakeholder involvement, conditions that they considered affected the implementation (internal and external), and what they so far had learned from the implementation process. The interview guides were developed based on insight from the literature, in particular from implementation research,9,26 and both guides cover elements that are considered central in implementation processes. All authors contributed to the development of the interview guides. The interview guides are available in the Supplemental Material.
The clinician participants were recruited from three different clinical domains: mental health, surgery and emergency medicine. These domains were selected to capture variations, but the study did not aim to compare them. We asked the department leaders, who were our main contacts, to invite a diverse sample of staff, ensuring representation from various professional groups and individuals with different levels of engagement with the new EHR. All the participants were recruited through their leaders, and none of the researchers knew any of the participants. The researchers contacted the participants via email and arranged the time and place for the interviews. In total, 19 healthcare professionals were included in the study. Four physicians, six nurses (two of whom worked as leaders) and eight therapists (of various disciplines) were interviewed.
The members of the implementation team were recruited through our contact person in the implementation organisation. They were invited based on their central roles in the process. Two implementation team members participated. Even though we used an interview guide, they were also encouraged to talk freely about their work and how the implementation was organised.
Around half of the interviews were conducted face-to-face in a suitable location at the participants’ workplace, while the other half were conducted via Microsoft Teams. The interviews were conducted by the first and second authors, both senior scientists holding PhDs; by one other researcher from the project team, also a senior scientist with a PhD; and by two master’s students, all of whom are female. All participants were informed about the purpose of the study and the possibility of opting out of the study at any time. All participants provided their written or verbal informed consent, depending on whether the interview was conducted face-to-face or via Teams. The study was approved by the Norwegian Agency for Shared Services in Education and Research, the national body for data protection in the knowledge sector and where health services research is registered. Verbal consent is approved if documented on audio tape.
The interviews were conducted in the spring of 2023, about 4 months after going live. They lasted between 30 and 60 min. At the end of the data collection period, we found that no new themes emerged in the interviews. All interviews were audiotaped and transcribed. Data were organised in Excel spreadsheets and analysed from an inductive standpoint. We were inspired by a thematic analysis described by Braun and Clarke 24 and Naeem et al.27,28 The first author was responsible for the initial coding of the data.
To illustrate the development of the analysis and coding process, instances of both broad codes (e.g., ‘experiences with the implementation process in general’) and overlapping codes (e.g., four codes related to the use of the system) were identified. The authors discussed these codes and related them to the phases of the implementation process (ref. 3) as a way of organising them. The codes were subsequently reorganised to build themes aligned with the respective phases.
Results.
Results
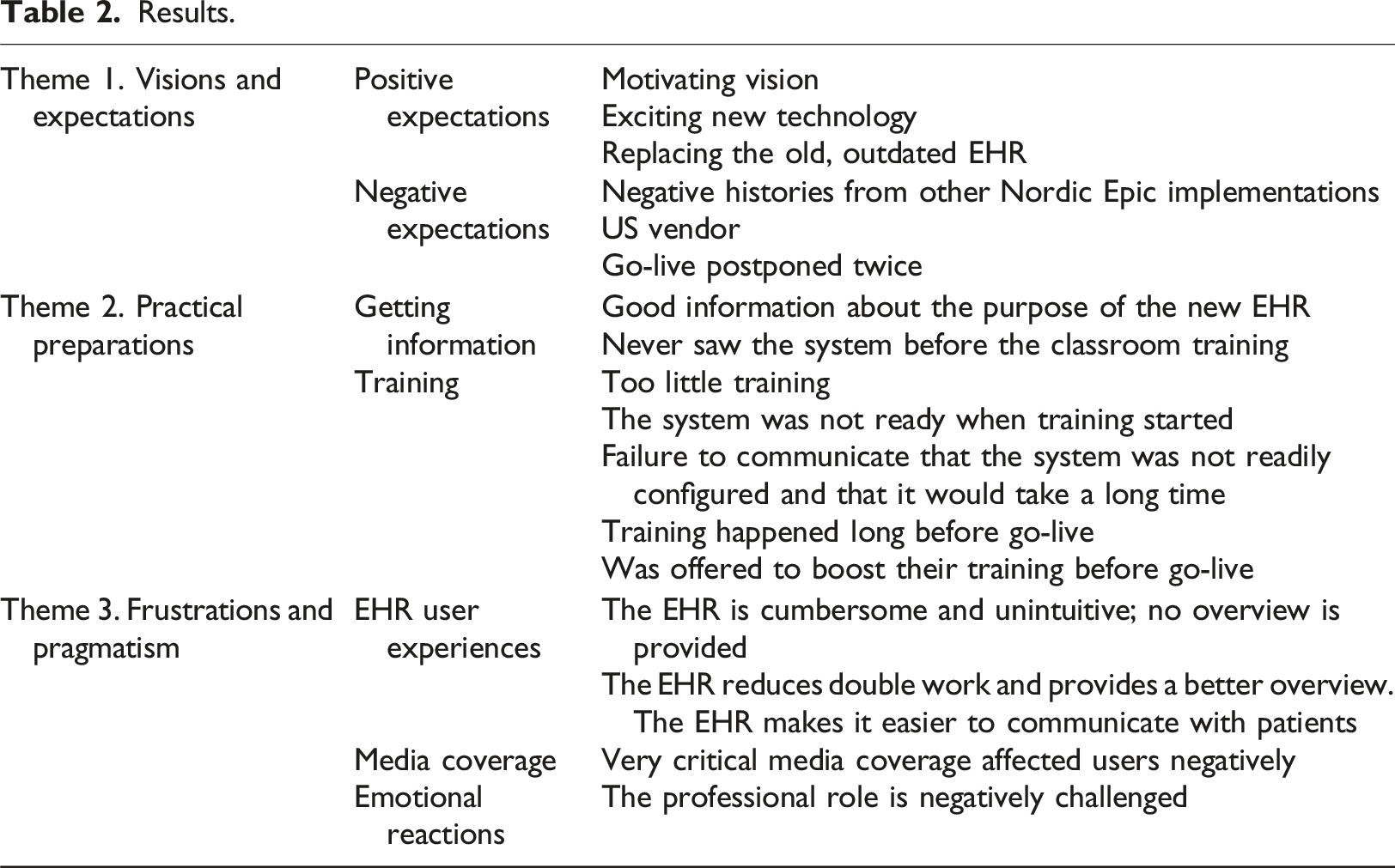
In the following section, we present the study’s three main themes and provide examples from the interviews.
Getting ready: Visions and expectations
Ambitions for the system were publicly communicated (e.g., to local media and in meetings with staff) by managers in the health trust and in the Health Platform organisation long before the formal readiness programme started. Healthcare providers’ expectations, therefore, began to take shape well in advance of the system’s formal implementation.
Overall, the participants were optimistic about the new EHR as they learned about it. These optimistic attitudes and positive expectations could be related to the perceived benefits of the new system and the desire to do away with the drawbacks of the old system. The participants agreed on the system’s overall aim for hospitals and municipal healthcare services to have easier access to each other’s information. This would improve collaboration across organisations. One participant felt that the communicated vision was highly motivating: The ambition with the new EHR – it feels significant (…) perhaps specialist and municipal health services will collaborate better. It was very meaningful and absorbing. (P3)
Another participant emphasised the value of having a modernised EHR and expected better plans and overviews of her work. I was expecting to have a modernised EHR system (…) that would give me a better overview of what is done, what the plan is, what we are working on and why we are doing it. That was my positive expectation. (P10)
Other reasons for looking forward to the new EHR had more to do with dissatisfaction with the old system and work practices than with the new system itself. The old system was typically referred to as a ‘digitalised paper record’, and many participants were discontented with the old system’s functionalities and the possibility of communicating with actors outside of the hospital. I actually thought it was exciting, this new system, so I hoped it would be good. Our old system was pretty old-fashioned, so I had quite positive expectations. (P7) We had talked about the Health Platform for years. No changes were made to our old EHR system because we would get the Health Platform. So, we have had very high expectations of the Health Platform, and we have waited for it for many years. We have been looking forward to it [not having to use the outdated old system]. (P18)
However, not all study participants were equally optimistic. Some explained that their initial optimism gradually turned into pessimism as time passed due to stories from other Nordic countries about challenging implementation processes, poor experiences with the system and reduced productivity in the hospital: After we got more and more information, I lost a little hope because it seemed like the Health Platform might not be so good after all. Then, I heard about the experiences from other countries, such as Denmark and Finland, and how poorly it had worked out there. I also got to test it a bit on my own, and it seemed like a cumbersome system. So, I didn’t have high hopes anymore as the implementation approached. (P2)
In addition, the fact that Epic was developed in the US was considered negative. Several questioned whether a US system would fit the Norwegian healthcare context. One participant said that he was negative towards the system and wondered why hospitals in Central Norway Health Trust had chosen a different system from hospitals in other Norwegian regions that use an EHR system from a Norwegian vendor. This view was shared by many participants. One nurse said: To me, it seems like the implementation was forced by higher management because there have been many protests against it. So, I wonder why they didn’t choose another EHR system when the other works so well. I wonder. (P17)
In general, the participants felt that management was positive and supportive of staff in the process up to go-live, particularly up to the first planned go-live. Several participants talked about how they were expectant and had mobilised energy for go-live. However, on short notice, go-live was postponed. Postponing go-live twice made some staff feel insecure and caused them to lose their motivation: When it was postponed… then, obviously, the air went out of the balloon a bit. And it was postponement after postponement. So, at one point in time, I thought, I don’t believe in the Health Platform until I see it. (P15)
Another said, ‘It was chaos in many areas, and it did not feel well. It was a period of time with much uncertainty.’ Yet another stated that the long implementation process had affected her more than she realised, which manifested in headaches and unrest about whether she liked her job less than she did previously. She both dreaded and was excited about the implementation.
In summary, the participants’ stories show that initial positive expectations began to fade.
Towards go-live: Practical preparations
Feeling competent and adequately informed could positively affect expectations. 29 Preparations included obtaining information and learning the system’s functionalities and the required changes in workflow. Training was organised as a separate sub-project in the overall implementation project and consisted of classroom training organised by the Health Platform and individual and small group training facilitated locally by the hospital. It was also possible for individuals to train at home after working hours and to be compensated for it.
Overall, when the study participants talked about how they felt prepared (in terms of being able to use the system and understand the new workflows), they seemed to agree that they were not sufficiently ready. One participant explained that she initially thought they received very good information about the aims of the new system, but she called for more information about the module for her clinical speciality. Another participant thought that it was unfortunate that they had never seen the system until they had received the classroom training. Information about the system was first presented to staff through short films and presentations: We had the system presented, and then we started with training. Among other things, we saw some information videos. Nothing of the system itself was actually shown. It was just said that ‘this and that will come’. I feel this was a waste of time. (P17)
While all participants received training, they questioned the usefulness of the classroom training and the amount of training.
We were very poorly prepared. Despite that, go-live was postponed… we did have 1 day of classroom training. We should have had much more training – particularly now after implementation. (P4) I think the training was pretty minimal. It was also carried out very early, so the system was not finished when we had our training. I was a bit like: ‘OMG, how will this be…’ (P13) I could have been better prepared. I guess I thought that I could just start using the system and that it would work out fine. I think that we should have been better prepared for the fact that the system is less finished than we thought and that it will take a long time before it is adapted to us. That could perhaps have been communicated earlier to us. (P6)
According to one participant, it was not communicated that the system was not as ready as originally planned and that it would take a while before it was properly configured. Some of the same experiences related to an unfinished system were also mentioned with regard to the training videos. While some thought they were good, others were more critical, primarily expressing concern about the system not being finished and the videos failing to show what this final version would look like.
Although unintentional, the timing of the training was poor. Originally, the staff were to receive training in the months leading up to go-live. However, because of a late decision regarding the postponement of go-live, most of the hospital’s staff members had already completed their training, which meant that all had received training about 6 months before the actual go-live. All staff were, however, offered a short brushing-up session right before the new go-live.
The examples shown were shared among many participants. People were more engaged and positive towards the overall vision of the system and less content with the practical training and information about the system. The interviews clearly show that motivation was decreasing in this phase of the implementation.
Using the system: Frustrations and pragmatism
After the system went live, participants’ expectations met the reality of everyday use. The experiences made in this phase indicate what participants were prepared for – or rather, what they were not prepared for.
The participants held varying opinions about the system. Some were highly critical, while others were more positive. The critics emphasised that the system is ‘not intuitive at all’, ‘cumbersome’ and ‘does not give an overview’. They also expressed concern that many new words and concepts have replaced old, familiar terms. Furthermore, some participants were uncertain whether electronic messages sent to collaborating partners outside the hospital had been received, which led to mistrust of the system. Conversely, some emphasised that the new system simplified work by reducing double work, providing a better overview and containing all information in one programme on one screen. In addition, communicating with patients was considered easier. All participants agreed, however, that the system was challenging to use: That’s probably one of the weaknesses of the system. It’s not intuitive. And that means that you must learn all steps by heart. You cannot understand it; you just have to learn it. (P19)
The interviews indicated that the level of difficulty was not something users were adequately prepared for. In addition, the system was frequently changed and reconfigured, which made preparations significantly more difficult.
In parallel with the implementation in the hospital, the media coverage of the project was wide-ranging and predominantly critical. This affected some of the participants negatively. Those who had positive experiences with the system found it frustrating that the media was constantly acting as a mouthpiece for the negative clinicians and never focused on the positive effects of the system. In this tense situation, broken expectations were manifested in two main ways, one of which was just to make the best out of it. People who were more positive about the system were also critical of much of the system’s usability; however, they argued that the system was there to stay: It doesn’t get better by going around whining about how bad we think it is because it just spreads to our colleagues and creates a bad atmosphere. I think we need to be positive. We just have to sit down, take a deep breath, and figure it out, you know. (P13)
Others reacted in a deeply emotional way, feeling that the core of their professionalism was challenged. These participants claimed that they felt helpless, resigned and indifferent, and that the system stole energy they should be using on patients, not on the system: It’s a very clumsy system. OK, it might get better, but what is clear is that it takes a lot of energy (…) it means that I don’t have the same amount of energy to spend on the patients (…) so I am not as good a doctor anymore. (P16)
The early-use phase was characterised by broken expectations and clinicians being unprepared for the amount of negative media coverage and the amount of training and energy needed to master the system. Many participants felt that their professional roles were challenged, and they felt less competent as a result.
Discussion
The implementation of the Health Platform is the largest HIS implementation in Norway. In this paper, we have tried to show how clinicians were prepared, what they expected and what their experiences with the system were some months after go-live, thereby addressing three central phases in an implementation process: preparation, go-live and (early) use. 3
In this snapshot of a complex and lengthy process, we focused on clinician users. From an implementation perspective, getting system adopters on board is crucial.9,10 In this case, much preparation was made on the parts of both the Health Platform organisation and the local hospital implementation team to prepare the hospital staff for the new EHR. The interviews show that the readiness programme was thoroughly considered, built on Epic’s standard methods and adapted to the Norwegian context, acknowledging that the implementation context is important.8,10 The overall vision of the system seems to have been clearly communicated and welcomed by the users during the preparation stage. All agreed that improved communication across hospitals and municipalities is desirable and that a new EHR may be a means to this end. However, the choice of Epic and the work needed to utilise the Health Platform seems to have been less clearly communicated – or at least less understood. The research literature on implementation of HIS addresses a myriad of factors that facilitate a successful implementation. The most common facilitated factor in the human domain is the perception of the benefits of the innovation. 9 Our study lends support to this, in the way that future users support the overall aim with the new EHR. However, many of them questioned the means to the aim.
The responsibility for the preparation activities was divided between the Health Platform organisation and the hospital. This division of labour and responsibilities was not much discussed among our participants, but it has been criticised elsewhere for being unclear and complex. 30 In general, our study participants spoke positively about their direct supervisors and agreed that they had been supportive, which is seen as important for promoting readiness.6,7 However, at the same time, many felt that they existed in a state of uncertainty and chaos. The hospital had only recently normalised operations after the Covid-19 pandemic – this involved increased preparedness levels and was followed by a high sick leave rate among staff. Simultaneously, the media published critical stories that frequently pointed out negative experiences with Epic in Denmark and Finland. The agreed-upon need for a change in the EHR system was therefore met with questions about the appropriateness of the chosen solution and the timing of the implementation. The circumstances can also have affected the hospital staff’s ability to invest time and energy in the implementation, thereby lowering their self-efficacy. These are all central components of organisational and individual readiness.6,7,14,15
The experienced value of a technology will influence adoption3,9,12 The technology being implemented in this case – the EHR system – was met with much critique among the participants. The system’s usability was at the core of this critique, but access control (too much or too little) and distrust in some functionalities were also addressed. In addition, the new EHR required new ways of working and changed workflows across the organisation. Many of the participants felt unprepared for using the new EHR. They explained that they had not seen the system, nor had it been demonstrated before they had received classroom training. One factor that has been shown to promote the successful implementation of HIS is involving users in the design phases and allowing them to test prototypes.9,31,32 In the case of the implementation in Central Norway, regular clinician users were not invited to trial the new system prior to go-live, which contradicts recommendations in the literature. While clinician users were involved in configuring the system, none of the study participants had such a role. Allowing clinicians to view and test the new EHR for clinicians prior to go-live could have facilitated a smoother transition to the new system.
Training is a well-established factor that promotes readiness for change and adoption of HIS.6,7,9,14,31 However, in our case, training was hampered by the fact that the system was still being configured to meet hospital users’ requirements. Staff members were therefore trained in something they knew would change later on. This was unfortunate, and it was recognised from the Health Platform implementation team’s perspective as well. The unfinished configuration was also one of the contributing factors to the postponement of going live.
Our study shows that staff members did not feel sufficiently prepared after classroom training to start using the system, and some even felt less confident than they did prior to training, as they realised that the system is not intuitive and must be learned by heart. It is important to mention that the Health Platform implementation team was clear in interviews that training prior to go-live would only cover a part of the competence and skills required to utilise the system and that the hospital was responsible for organising in-house training. As shown in Table 1, the hospital had arranged for such training, but our data do not indicate why participants did not train or did not find it satisfactory. Furthermore, the research underscores that much learning and tinkering happens when the system is in use. 3 Such perspectives on learning were not addressed among participants, which may suggest that they had little awareness of it. Future developments in AI may positively contribute to training, both before and after the system is fully configured. For example, AI-driven tutors may provide adaptive learning and personalised guidance to users. When the system is in use, AI may be used for creating realistic patient cases and facilitate scenario-based training. 33
Another issue frequently raised among the participants was why Epic’s EHR system was chosen and not a system from a Norwegian vendor. Epic was the only vendor that complied with the health region’s requirements; furthermore, the one Norwegian vendor that participated in the tender was not seen as qualified. Such processes may be invisible to end users. This lack of knowledge can lead to wrong expectations and to disappointment. 18 Background information on the choice of vendor and the details concerning the chosen solution (e.g., structured documentation vs free text) can be seen as examples of contextual factors. To our knowledge, neither the readiness programme nor the other training material addressed such topics. The coverage of the implementation in mass media and engagement in social media was also wide-ranging and predominantly negative. This can be regarded as another contextual factor affecting the implementation climate 6 that the readiness programme did not address sufficiently. Additional information and clarifications about possibilities and limitations of the EHR and the rationale behind the choice could have been useful for empowering users and aligning their expectations with what can realistically be achieved.
Lastly, we want to highlight the deep emotional reactions to the new EHR by some participants. All participants were concerned about patient care and patient safety, thus situating the benefits – or drawbacks – of the system outside themselves, cf. valence as a component of individual readiness. 7 The participants were concerned that the new EHR would jeopardise patient safety. Some expressed more personal concerns related to their struggle to use the system. They felt that the system took away valuable time from patient work and that it made them less effective as professionals. Some even wanted to quit their jobs because the working conditions imposed by the EHR system conflicted with what they thought good healthcare provision should be. Such reactions can be related to the literature on moral distress or moral injury, denoting the experiences healthcare workers may have when working under pressure and not fulfilling their non-negotiable moral and professional principles. 34 We did not find that such (unintended) consequences were addressed during the readiness programme.
In summary, numerous studies have explored both the preparation of future users for new technologies9,14,15 and the barriers and facilitators of successful implementations.9,31,32 However, to the best of our knowledge, one aspect that has not been sufficiently addressed—particularly in detail—is how user expectations for large-scale HIS are shaped, how they influence use, and how these expectations should be managed throughout the implementation process. In this study, we examined clinicians’ expectations of a new EHR system and analyzed how these expectations were met during the early use phase. Our findings highlight the need for even stronger emphasis on expectation management during the preparation phase to ensure that users develop realistic expectations of the new system.
Strengths and limitations
The study used a semi-structured interview guide, allowing participants to address topics they found important. This approach is effective for capturing what truly matters to the participants. However, such flexibility might have resulted in some topics not being sufficiently addressed in all interviews. A more structured interview could have yielded more detailed information on certain topics. The interview guides were not pilot tested, which may be another limitation. Nonetheless, the guides were developed by experienced researchers on the basis of insights from the literature. By the end of the data collection, no new main topics emerged, which can be considered a sign of saturation. However, increasing the number of interviews would likely have revealed more nuances in staff experiences. In future work, we will expand the number of settings and include participants with an even broader range of backgrounds.
Conclusion
How can clinicians be prepared to use a new, complex EHR system that also requires changes in work practices? Implementing readiness programmes can be one step in this preparation. Our study has shown that while clinician users were enthusiastic about the bright visions for the new EHR, dark clouds soon appeared on the sky, and many clinicians became frustrated and discouraged. Large-scale implementations are unpredictable, no matter how carefully planned they are, as they are influenced by a wide range of factors, including contextual ones. Preparations should take this into account. We suggest that readiness activities should be made even stronger to prepare users for change and learning. These activities should give users confidence and not only train them to use ready-made products. ‘Ready’ in this respect does not mean fully qualified; being ready means having the motivation and confidence to take a leap into the uncertain.
Supplemental Material
Supplemental Material - Bright visions, shady days: Exploring hospital staff expectations and early experiences with a new EHR system in Norway
Supplemental Material for Bright visions, shady days: Exploring hospital staff expectations and early experiences with a new EHR system in Norway by Line Melby, Kirsti Sarheim Anthun and Pieter Toussaint in Health Informatics Journal
Footnotes
Acknowledgements
The authors would like to thank the study participants for sharing their experiences with the project team. Thank you also to master students Nora Lian Aarrestad and Ann Kristine Halvorsen and senior researcher Kari Sand who took part in the data collection.
Ethical statement
Author contributions
Conceptualisation: LM, PT, KSA. Methodology: LM, PT, KSA. Data collection: LM, KSA. Analysis: LM, PT, KSA. Writing – Original draft: LM. Writing – Review and editing: LM, PT, KSA.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Norwegian Research Council [grant number: 326744].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.