
Abstract
Introduction: The introduction of information technology was one of the key priorities for policymakers in healthcare organisations over the last two decades, due to the potential benefits of this technology to improve healthcare services and quality. However, about 50% of those projects failed to achieve their intended aims. This was as a result of several factors and included the level of readiness to the new IT projects. Aim: The aim of the study was to assess the readiness of Saudi primary health care centres (PHCCs) readiness for the implementation of an electronic health record system (EHRS) from the project team perspective. Methods: Explanatory mixed methods design was used with both qualitative and quantitative methods. Thirty-one members of project team at the ministry of health (MOH) participated in the online-based questionnaire, while 13 participants from the same population took part in the semi-structure interviews. Eight different readiness scales were quantitatively examined. These scales include resources, Knowledge, process, management structure and administrative support, end user, technology and values and goals. Result: Although, very high level of readiness has been recorded at the process, management structure and administrative support levels, readiness was average at the end user, technology and values and goals levels. Moreover, the study findings revealed that primary health care centres readiness for an electronic health record system must be considered in the early stages of implementation (pre-implementation phase), particularly readiness at a technical level, such as preparedness of the infrastructure. A positive significant correlation has been recorded between all readiness scales with centralization of management system and financial resources. Conclusion: Overall, the level of primary health care centres readiness recorded to be high, which indicates that primary health care centres are ready for implementation of the electronic health record system, and in this context, management structure, organizational process, financial recourses and administrative support play significant roles to increase the project success rate.
Keywords
Introduction
The safety of patients and quality of care are two of the most studied and important topics in the area of health informatics (HI).
1
Due to rapid technological changes, researchers, academicians and practitioners see the value of enhancing the features of electronic health record systems via modification. These change simply the process of record-keeping so that patients can receive timely care.
2
The notion of an electronic health record system (EHRS) is not only established in developed countries but also in developing countries, which are now taking the initiative to implement such a system.
3
Most health care professionals have claimed that the quality of care and safety of patients have been improved through the implementation of the EHRS.
4
Errors and mistakes have been reduced by the EHRS.
5
The EHRS is still overlooked and demands the attention of policy-makers and practitioners. The reasons underlying this ignorance are several.
6
In health care organizations in Saudi Arabia, policy-makers’ first choice has been to implement an EHRS and derive benefits from such a system with respect to improving the performance of professionals and the safety and quality of care.
7
Although the importance of an EHRS is very high, developing economies are reluctant to implement such a system because of the huge costs, given the limited financial resources available to developing countries.
8
Health care organizations should assess their readiness before implementing an EHRS in their health systems. This process requires systematic planning. Past studies have suggested that an organization should prepare itself before implementing the EHRS. These organizations should be sufficiently flexible to accommodate such a change.9,10 Ross et al.
11
affirmed that readiness for EHRS execution is a significant aspect of this process. Readiness evaluation has been described by number of authors such as12–16 See in Figure 1 Steps for assessing readiness of PHCCs.
Various factors have been identified as affecting readiness for the implementation of the EHRS; individual factors; leadership; management; organizational culture; technical readiness; operational readiness: changes in management; training; and technical support13–15 (see Figure 2). The factors that must be investigated to assess the readiness level of an organization include the following: (a) current IT systems and infrastructure, (b) technological experience, (c) goals, motivations, requirements and attitudes, (d) potential constraints and issues, and (e) economic and manpower resources.
17
These factors, which are highlighted above, can help organizations add value while implementing a new EHRS.
17
Attributes/determinants and factors shoudl be consider durign evaluation of PHCCs readiness.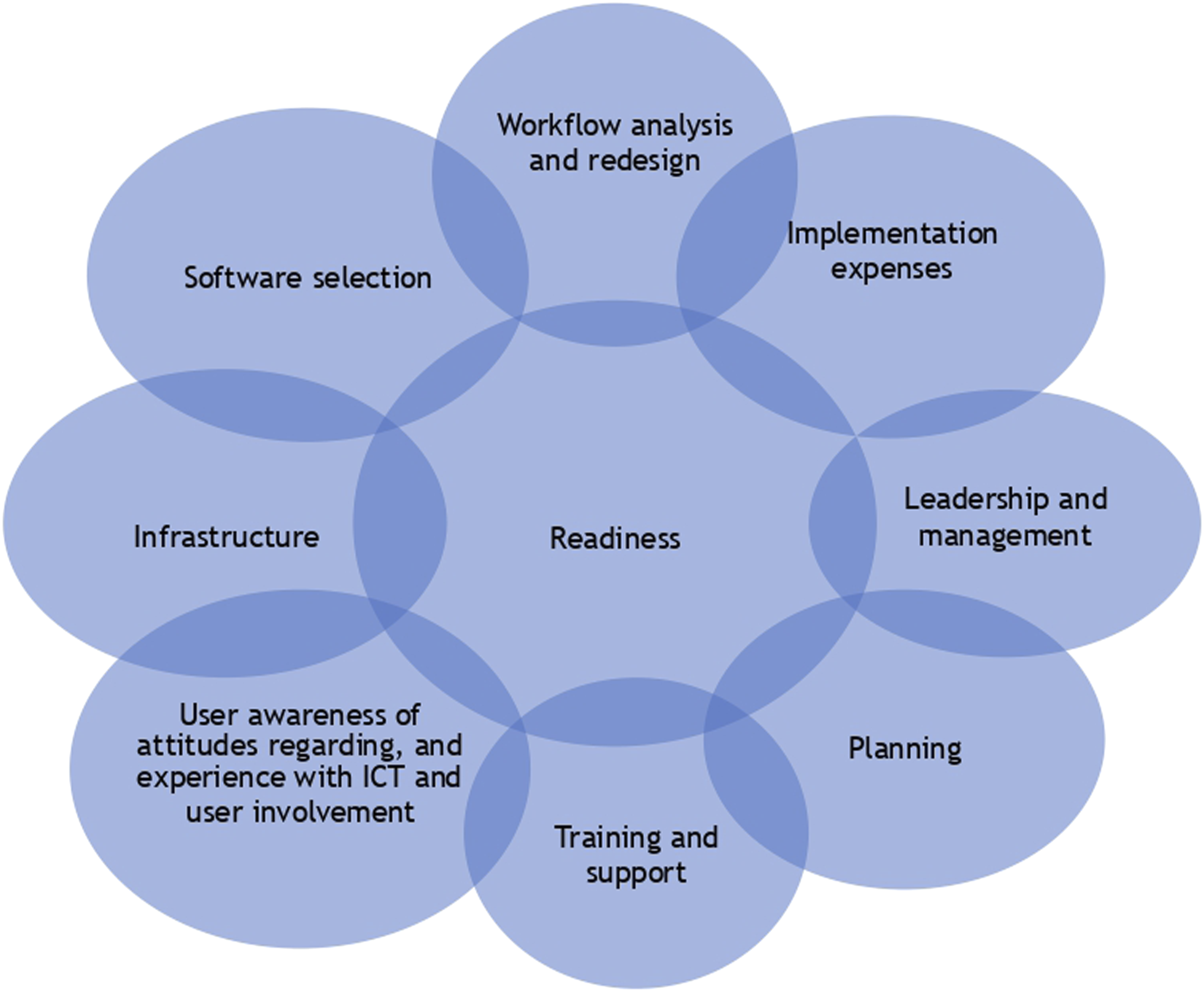
Before implementing the EHRS in organizations, an assessment of readiness can help organizations find enough time to select software and conduct planning so that no disruption occurs during working hours. 18 This fact is the reason why readiness prior to implementation is considered to be more important. 11 The issues and challenges faced by organizations implementing such a system include difficulties with resources, a reluctance to change and problems that occur during the process.9,19 Therefore, it is imperative for management of PHCCs to strive for readiness, to select project team members, and to formulate a process before the planning stage. The responsibility for readiness assessment falls on the project team and its members. The data collected can facilitate quality decision-making and an appropriate selection of software and proper training programs (see Figure 2). On the basis of the preceding discussion, the main objective of the current study is to investigate the readiness of primary health care centres with respect to the implementation of a large-scale electronic health record system in Saudi Arabia.
The Saudi health system and the history of electronic health record system implementation
Saudi Arabia’s health system is divided into three levels. The first level is the primary level, which includes primary health care centres, followed by the secondary level, which consists of general hospitals, and finally the tertiary level, which includes specialist hospitals. Billions of riyals have been invested in the health sector by the Saudi government to improve the quality of health care services. For reasonable fees, insurance policies are also available to the general public for medical services. The majority of the health services budget is provided by the MOH, while other governmental bodies also contribute to the provision of health services, such as Aramco, the National Guard, the Ministry of Defence and the Interior Ministry, as well as universities, hospitals and aviation organizations. Due to variation among these health systems, there is also variation in the information-tracking systems used by these health organizations, and patient information is scattered, except in cases where patients habitually receive all treatment from the same health centre. Another disadvantage of these varied health care centres is that this situation leads to a waste of time, resources and effort. This situation calls for the implementation of the EHRS. Electronic health records have benefits for management, physicians and patients. Such systems increase performance quality, reduce time, effort, wellness and medication costs, and facilitate decision-making. 20
Saudi health care institutions currently rely largely on advanced information and communication technologies. Recently, the Saudi Data and Artificial Intelligence Authority (SDAIA) were established. The main aim of this authority is to promote digital health services throughout the kingdom. All health-related e-applications and digital health-related systems are regulated by the MOH. To provide quality services and accurate information, e-applications such as the Tawakalna, Tabuad, Sehati, and Mawid applications have been developed, and all these applications have been linked together. These applications facilitate services such as appointments, diagnosis, and medical assessment of patients. Health practitioners can also communicate with each other and with patients; moreover, national health information centres can exchange information among different health sectors.
Hypothesis development
Ajami et al. 21 reported a significant relationship between factors influencing readiness and EHRS. Similarly, Gatiti et al. 22 also reported significant relationships among different forms of readiness and asserted that such systems can help professionals in PHCCs improve patient safety and the quality of care. Moreover, Ayaad et al. 23 also confirmed that electronic health records not only have a significant impact on increasing the quality of care but also increase the performance of professionals and reduce errors and mistakes. Furthermore, Mayer et al. 24 and Patel 25 also reported that electronic medical records have a significant impact on quality, safety, related with criterion variables (i.e. centralization of management system & financial resources). Furthermore, Cheng et al. 26 remarked on the significance of readiness prior to implementing the EHRS and the impact of such readiness on quality, safety, and criterion variables. On the basis of the preceding discussion, the following hypotheses were developed:
System innovation readiness predictors are positively and significantly related to criterion variables, centralization and financial resources.
System innovation readiness has a significant influence on the criterion variables.
Materials and methods
Research design population and sampling
The current study was conducted in the MOH which is located in the capital city of Riyadh, Kingdom of Saudi Arabia. Mix methods were used in the existing study. As per Creswell 27 the best fit research design for this study was explanatory sequential research design. This design consisted of two phases. First phase included quantitative data collection and its analysis followed by semi-structured face to face interviews to support quantitative findings. The quantitative survey research design was adopted, and a structured questionnaire, the Organizational Information Technology/Systems Innovation Readiness Scale, was employed. These cross-sectional data were collected for the current study. The target population for this study was decision-makers and stakeholders who were directly involved in the implementation of the electronic health records system (EHRS) at primary health care centres (PHCCs). According to the statistical year book of Saudi Arabia, the number of employees in this sector was 430,096, but respondents were selected on the basis of their specialty, background, involvement in the decision-making process and knowledge of the implementation of the EHRS at PHCCs, which is why the population and sample used in the current study were low. Non-probability purposive/convenience sampling techniques were used in the current study. The population considered in the sample included all decision-makers and implementation project teams in the MOH (n = 53). The project team was responsible for leading and supervising the implementation process from the pre implementation phase until the live phase. Many significant decisions were made by the project team, such as decisions concerning the mode of implementation, software selection, champions and super user selection. In addition, the project team was responsible for designing the project plan and creating the Request For Proposal (RFP) document. Finally, the project team was responsible for providing financial and moral support to facilitate the success of the project.
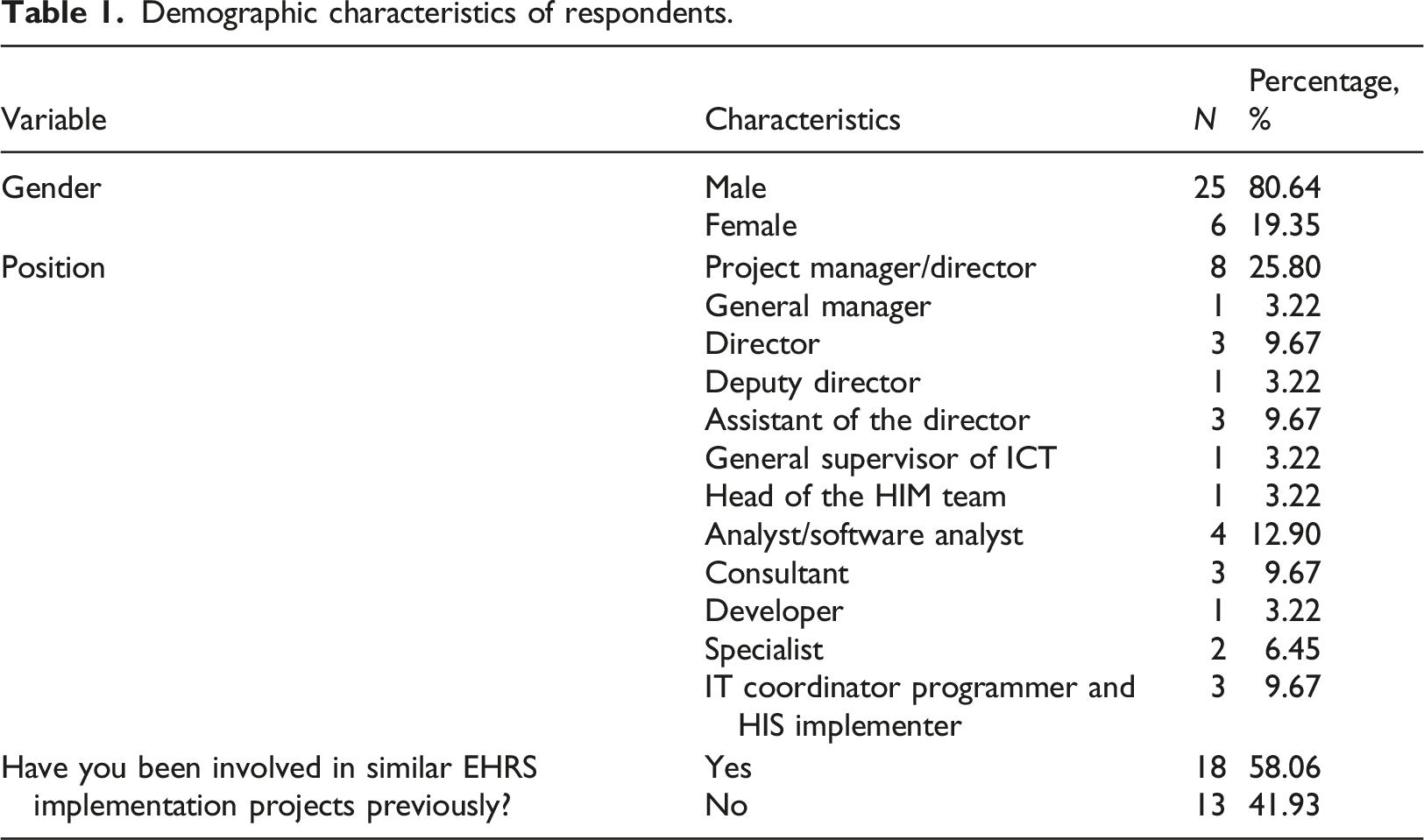
A total of 31 completely completed and valid questionnaires were returned and used in the analysis for a response rate of 58.49%. The information communication technology office of the MOH was approached to determine the population for this study, and the relevant authority provided the names, positions and contact details of all decision-makers and project team members who were directly involved in the EHRS implementation project for PHCCs. Face-to-face semi-structured interviews were also conducted to obtain an in-depth understanding of the subject matter. Therefore, permission was requested for respondents to participate in the interview, and 13 respondents agreed and participated in the interview sessions.
Assumptions of sample size and partial least squares structural equation modeling
According to Kay-Wong, 28 PLS-SEM should be used when the sample size is small, i.e., less than 100. Wong 29 claimed that when a researcher has a limited number of respondents, PLS-SEM is useful. As per Kay-Wong, 28 determining an accurate and precise sample size is always a problem for researchers. The sample size guidelines for PLS-SEM were developed by Hair et al. 30 who discussed the “maximum number of arrows pointing at latent variables, significance level, and R2 values”. If the number of arrows pointing at latent variable is 2, then the required sample size is 52; if the number of such arrows is 3, then the required sample size is 59; similarly, if the number of arrows is 4, then the required sample size is 65; and if the number of arrows pointing at latent variables is 10, then the required sample size is 91. In the current study, the number of arrows pointing at the latent variable was 1, so a smaller sample size was used for this analysis.
Measures and instruments
Demographic characteristics of respondents.
Description of constructs.
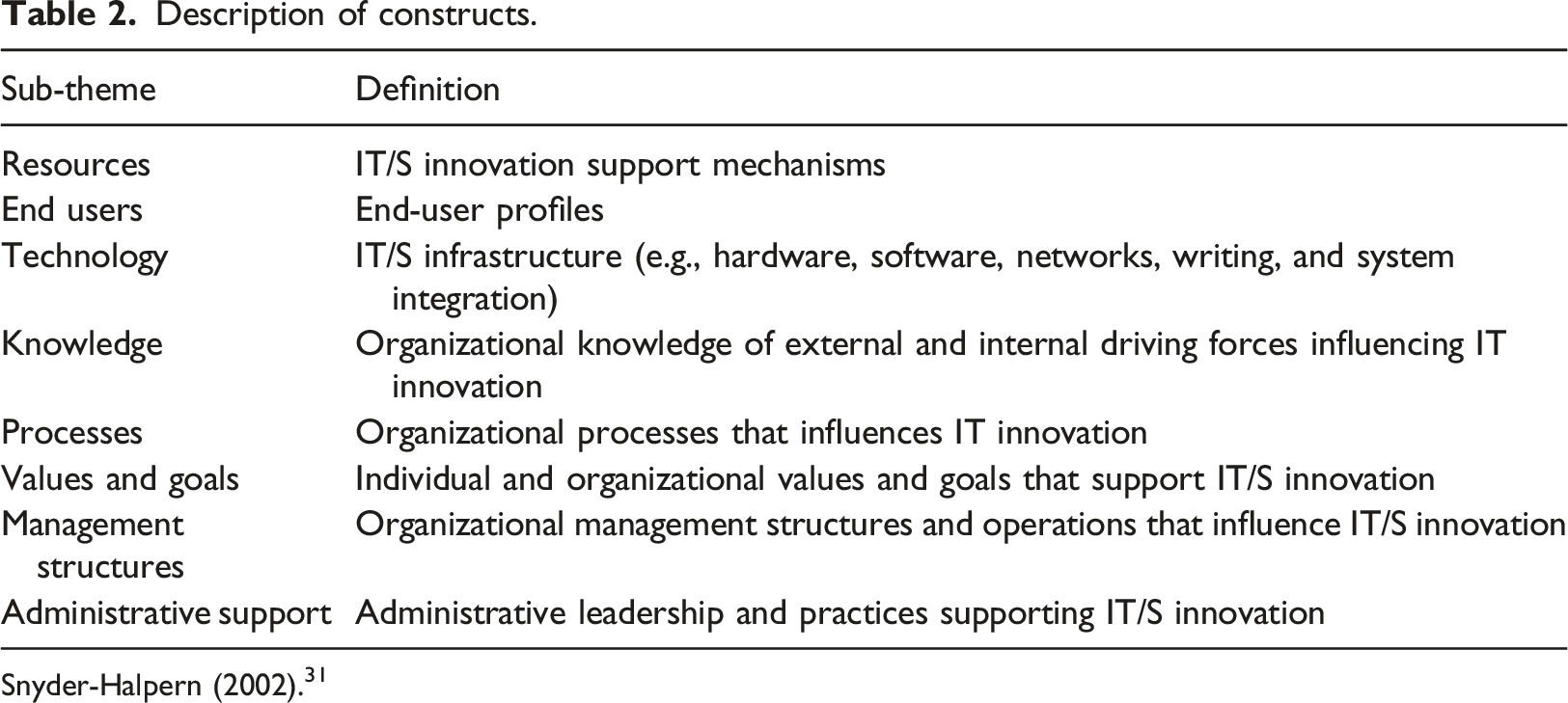
Snyder-Halpern (2002). 31
Measurement and structural models
In measurement models, two validities need to be established, namely, convergent validity (average variance extracted, AVE, and construct reliability, CR)and discriminant validity, i.e., the Fornell-Larcker criterion established by taking the square root of the AVE values. The aim of convergent validity is to investigate whether the items used in the instrument measure the same concept, while discriminant validity is used to examine whether items can differ among constructs. Once the measurement modelling stage is completed, the researcher proceeds to the next stage, i.e., the structural modelling stage, in which researchers test the hypotheses by using inferential statistics such as correlation and regression.
Data analysis tools and techniques
SPSS version 25 and PLS-SEM 3 software were used for data analysis in the current study. Descriptive and inferential statistics were used for data analysis. In descriptive statistics, the mean standard deviation and respondent information were used alongside exploratory factor analysis for validity and Cronbach’s alpha for reliability. On the other hand, inferential statistics were used to test hypotheses. Bivariate correlation and Pearson correlation analysis were conducted to test the strength and direction of the relationship between variables. The structural model investigates the influence of predictors on criterion variables.
Regression equation
Regression equation 1:
αo and
ε = unexplained variable or error term. (Figure 3). Framework of the study in which left side variables are predictors and right side are criterion variables.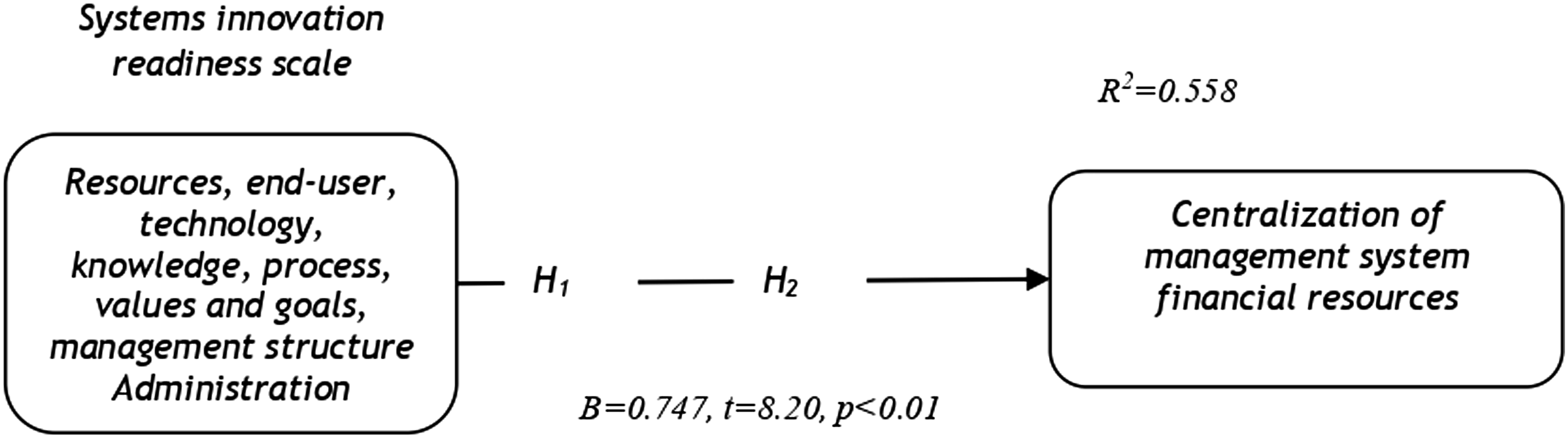
Quantitative results
Measurement model organizational information technology/systems innovation readiness scale.
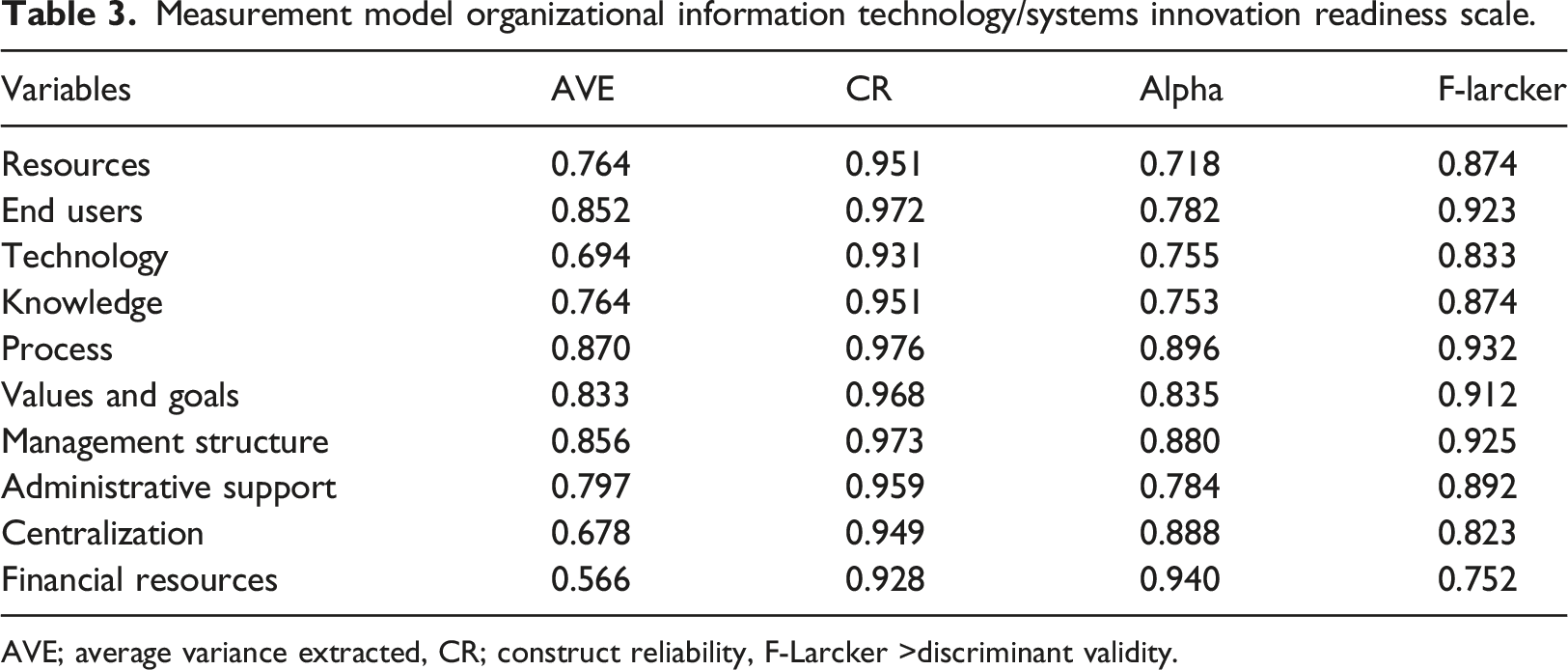
AVE; average variance extracted, CR; construct reliability, F-Larcker >discriminant validity.
Correlation matrix, mean and standard deviation values.
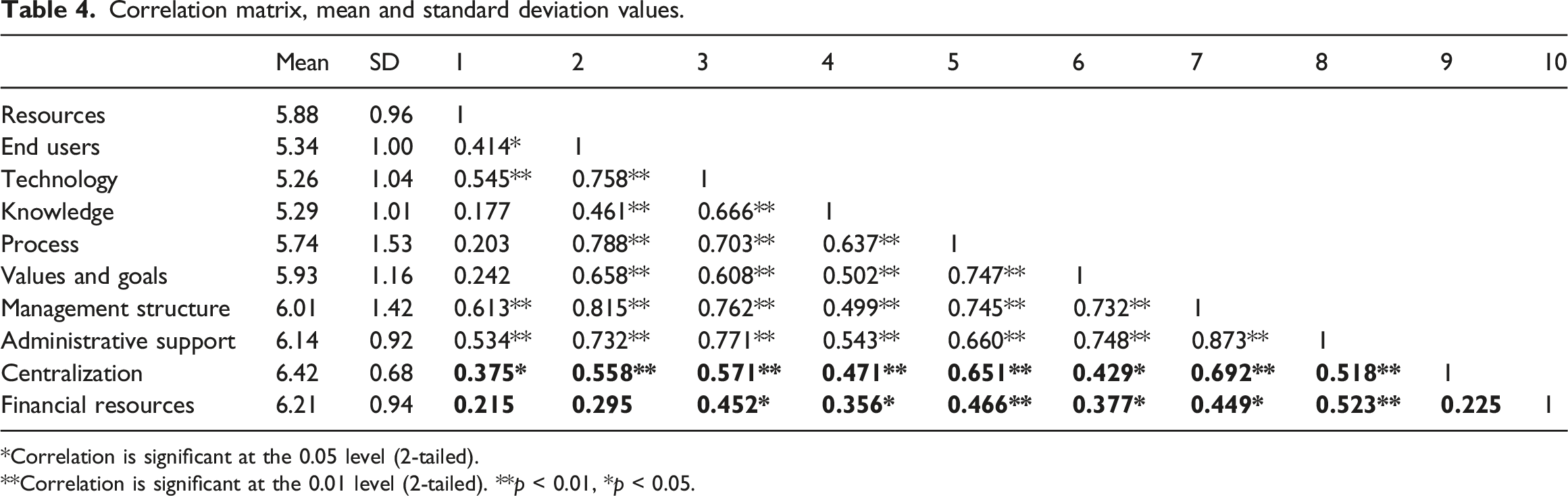
*Correlation is significant at the 0.05 level (2-tailed).
**Correlation is significant at the 0.01 level (2-tailed). **p < 0.01, *p < 0.05.
To develop a structural model, smart PLS-SEM software was used to test Hypothesis 2. See Figures 4 and 5. Figure 4 represents the structural model with t-statistics; the threshold value for t-statistics is 1.96 as per Hair et al.
32
and bootstrapping with 1000 resampling was performed in order to obtain beta values, t-statistics, significance levels, and bootstrapping confidence interval upper and lower limits (i.e., BCIUL & BCILL).Common method bias and multicollinearity were also investigated via VIF. It is evident that β = 0.747, SE = 0.091, t = 8.22, p <0.01, BCIUL = 0.875, and BCILL = 0.471. The fact that the variance inflation factor, i.e. VIF = 1.000 demonstrates that all the values met the threshold level recommended by Hair et al.32, and there no zero is included between BCIUL and BCILL. Hence, Hypothesis 2 is substantiated and verified. It can be concluded that system innovation readiness has a significant impact on the centralization of the management structure and financial resources. Moreover, the effect of each variable was also investigated, and the influence of resources on centralization and financial resources was found to be positive and significant (β = 0.358, t = 2.062, p < .05, which means that a one-unit increase or decrease in resources could entail a change of 35.8% in centralization and financial resources). Further analyses of the results revealed that the end users factor has an effect of β = 0.514, t = 3.224, p < .05, which implies that a 51.4% change is possible in centralization and financial resources due to end users. Likewise, technology also has a positive and significant impact on the criterion variables, β = 0.636, t = 4.438, p < .05, i.e., a63.6% change is possible in centralization and financial resources due to a one-unit change in technology. Similarly, organizational knowledge also has a positive and significant impact on the criterion variables, i.e., β = 0.512, t = 3.212, p < .05, and soa one percent change in organizational knowledge could entail a 51.2% change in the criterion variables. Furthermore, organizational processes also have a significant and positive effect on centralization and financial resources, i.e., β = 0.689, t = 5.12, p < .05, such that a one percent change in organizational process could cause a68.9% change in the criterion variables. Similarly, values and goals also entail a50.5% change in the criterion variables, β = 0.505, t = 3.149, p < .05. Management structure explained 69.9% of the change in criterion variables, i.e. β = 0.699, t = 5.259, p < .05, and support from administration explained 66% of the significant and positive change in centralization and financial resources, β = 0.660, t = 4.733, p < .05. The most dominant factors in the current study as determined by beta values, i.e., the factors that explained more positive change in the criterion variables, were management structure and organizational process, followed by administrative support. This is structural model developed in PLS-SEM for testing hypotheses. Shows path coefficients during bootstrapping.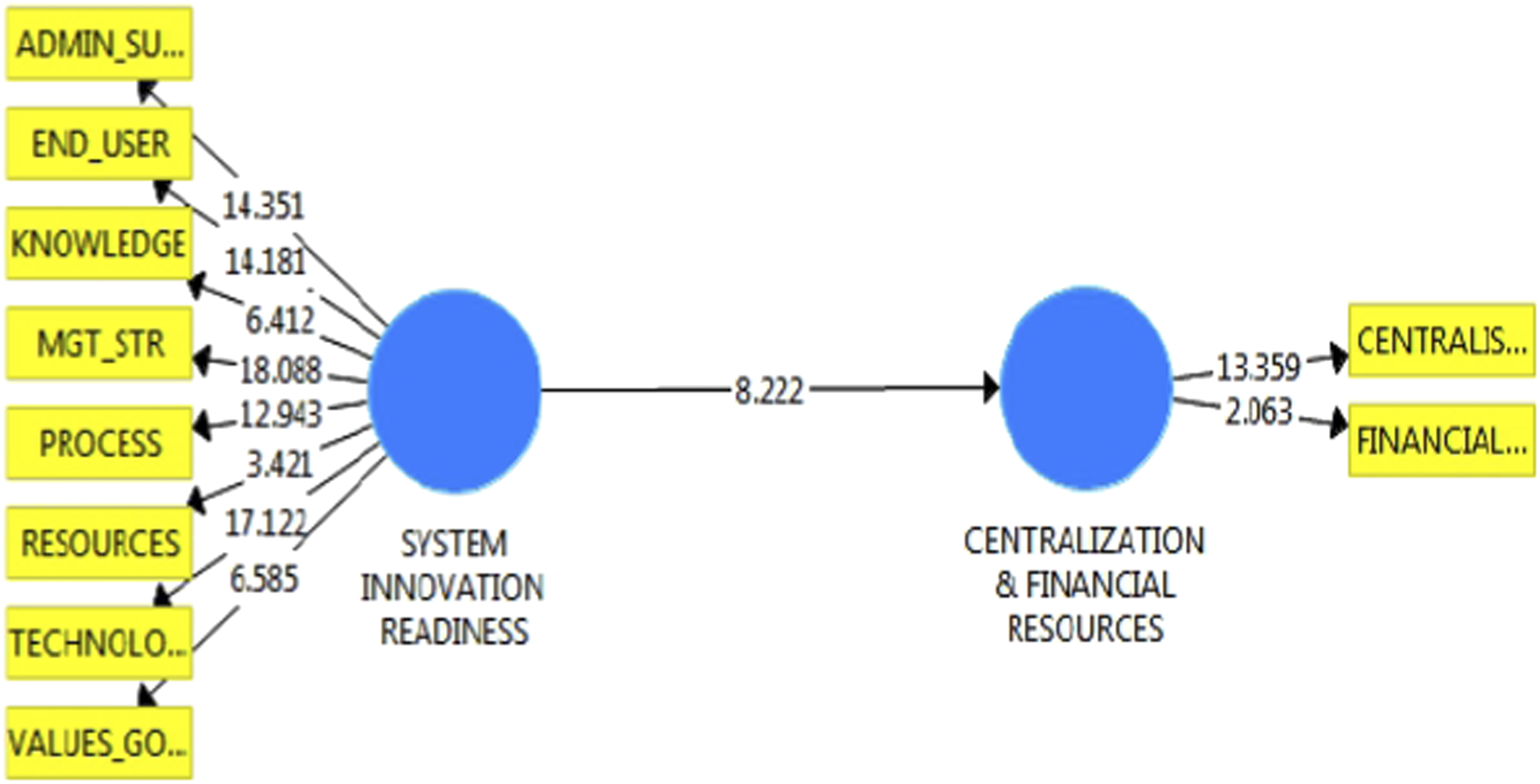
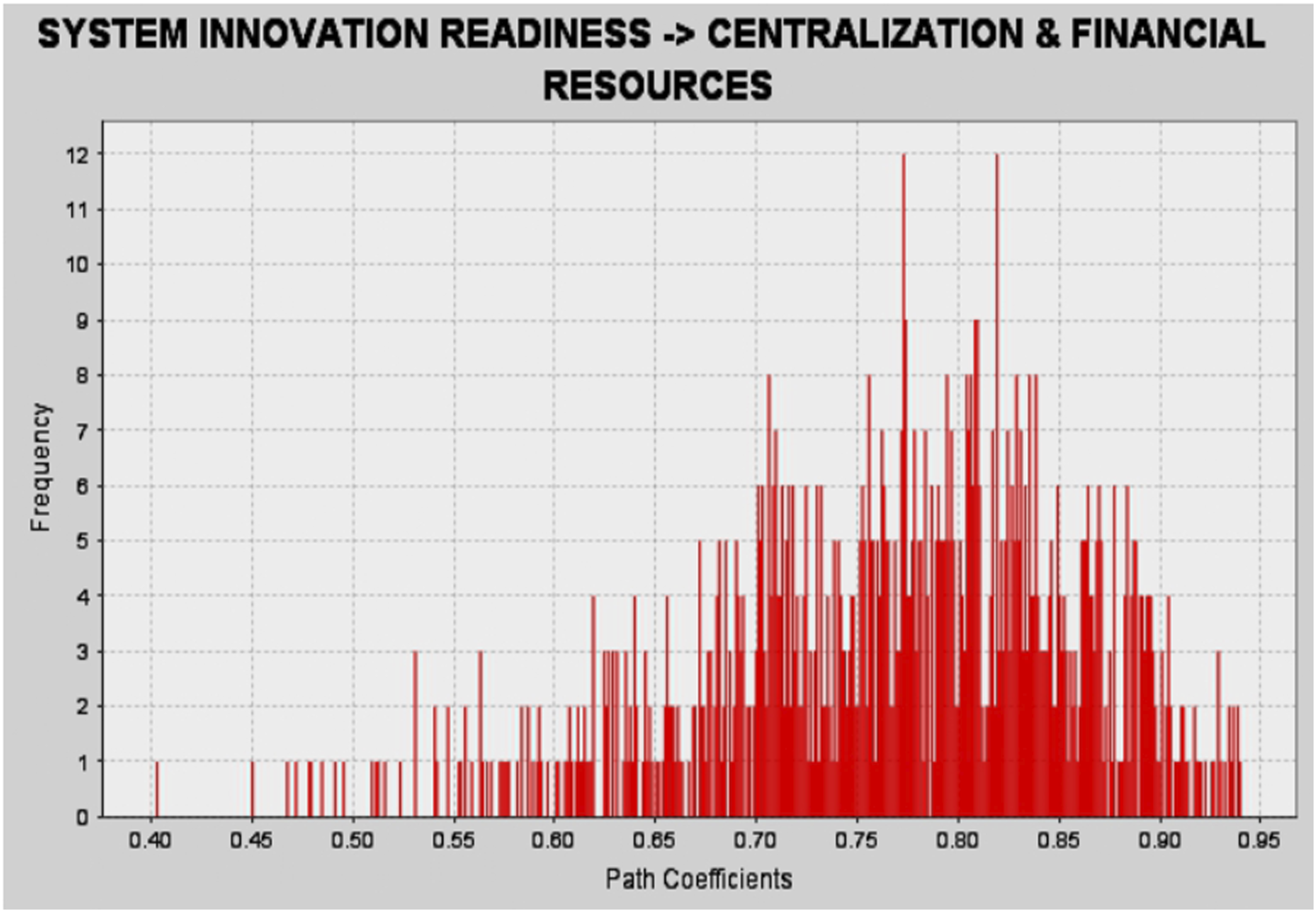
Figure 4 is produced by PLS-SEM and shows the graphical form of the structural model. The values shown in Figure 4 represent the t-statistics cut-off level for t values of 1.966. Figure 4 shows that all values are >1.966 and thus demonstrate the significant impact of predictors on the criterion variables.
Qualitative results
Readiness assessments
The readiness of health care organizations to implement a new EHRS has been found to be influential with respect to the success of such a project therefore, the Saudi MOH examines several readiness measurements to ensure successful EHRS implementation. “Some of the requirements have been considered, such as the readiness of PHCCs to successfully implement new technology.” (GM 1)
Numerous studies have been conducted to identify all the obstacles and facilitators directly associated with the success or failure of EHRS implementation projects. In addition, the MOH conducted research to determine the strengths and weaknesses that may influence EHRS implementation in PHCCs in SA. “First, we did so many studies prior to the implementation to know the strengths and weaknesses of the challenge.”(DHD 1) “We conducted a number of studies and research before the beginning of any EHRS implementation to learn strengths and weaknesses as well as to determine the challenges and causes of failure and to identify risks.” (HD 3) “The Ministry conducted research to avoid any problems and ensure the successful implementation of the EHRS.” (GM 3)
At a technological level, the MOH is currently engaged in the task of assessing the readiness of PHCCs in light of connectivity infrastructure to accommodate the EHRS implementation project and identify any relevant obstacles and challenges. “We discussed the readiness of hospitals and PHCCs in terms of infrastructure compatibility with the change, especially for PHCCs.” (HD 3) “We are currently conducting a situation analysis of PHCCs, including an assessment of PHCCs’ readiness in terms of connectivity.” (GM 3)
However, some participants believed that all PHCCs are currently ready for EHRS implementation. “PHCCs are currently ready to implement the EHRS.” (DHD1) “I think they are almost ready to use a new EHRS.”(HD 3)
Other participants, in contrast, thought that PHCCs are not yet ready to implement the EHRS. “I think some of the PHCCs are still not ready for this project, compared with hospitals.” (SD 1) “Some of the PHCCs need to be prepared for the new implementation - they are not ready yet.” (GM1)
In the pre implementation phase, the MOH plans to restructure the workflow of PHCCs to comply with the changes introduced by EHRS implementation. This plan confirms that the MOH intends to restructure the workflow of certain centres that use EHRS. Although three different vendors implement EHRS in Saudi PHCCs, the MOH assumes the responsibility of redesigning a unified workflow. According to one participant, this workflow redesign is not affected by the fact that the Ministry intends to select three different vendors. “Another thing that we could take into consideration is to redesign the PHCCs workflow; even if we do have three vendors, we will ask them to design one workflow for all PHCCS.” (HD1) “If you go to the PHCCs that have the EHRS and other centres, you will see that they have been redesigned to comply with new IT projects.” (GM1)
Main results
Mix methods were used in which first quantitative data was collected, analyzed followed by semi-structured interviews to support quantitative results. It was revealed from the findings that centralized decision making and financial resources are crucial to implement EHRS in PHCCs. Furthermore, it was also found that government should provide all necessary resources to PHCCs also administrative support and structure of management are found important for successful readiness and implementation of EHRS. There was significant relationship found among attributes of EHRS readiness, centralization, and financial resources. Moreover system innovation had significantly predicted centralization and financial resources. Semi-structured interviews taken from general managers, head of departments, system developers, had revealed that PHCCs were ready to implement new technology except two respondents they raised their concerns for few PHCCs. Overall it was concluded from the findings that PHCCs in Saudi Arabia are ready to implement EHRS in whole country.
Discussion and conclusions
A substantial increase in the adoption of electronic health record systems by health care organizations has been noted due to the significance and importance of such systems. Professionals require medical information that can assist them in providing medical services to patients. In this context, quality decision-making and its results depend on the information supplied by the EHRS. 33 Overcrowding and short timeframes are issues faced by professionals in health care organizations. In this regard, professionals depend on the information supplied by the EHRS to make decisions. The current study attempts to provide further insight into the field of medical informatics. The EHRS facilitates decision-making with regard to admissions and diagnosis. There is limited evidence available concerning the effectiveness of the medical technologies available to professionals, physicians and clinicians. 34 Despite a gradual increase in the availability of medical technologies, the effectiveness of such technologies has been overlooked in the literature. The EHRS provides access to testing, imaging, and medical history in a professional, computerized format. Such systems also help medical professionals make decisions quickly in difficult situations. The EHRS helps reduce costs by reducing unnecessary and redundant tests, improving performance, providing financial returns on investment and reducing the percentage of mistakes and medical errors. 35 Physicians do not have access to certain pieces of information during communication with patients, but the EHRS provides physicians with access to such information (X-rays, laboratory tests, images, etc.). The main purpose of the present study is to add value and extend the body of scientific knowledge concerning the effectiveness of electronic health record systems and readiness assessments with respect to such systems in the context of primary health care centres. The main aim of this study is to highlight the significance of readiness assessments of PHCCs with respect to a large-scale EHRS implementation in Saudi Arabia. To ensure PHCCs’ readiness for this large-scale EHRS implementation, financial resources, human resources, technology, knowledge, processes, administrative support, appropriate management and centralized decision-making are needed. The findings of this study revealed that there is a significant association between predictors and centralization at the p <0.05 level. These findings are consistent with those of past studies by Häyarinen, Saranto and Nykänen. 36 Moreover, the findings of this study are also in agreement with those of Makam, Lanham, Batchelor. 37 Likewise, the findings of the current study are compatible with the findings of Snyder-Halpern. 27 The current study replicated the results of a previous study of the Snyder-Halpern 20 scale, which was developed from a Western perspective. This scale needed validation from a Saudi perspective. It can be concluded that the innovation readiness scale is reliable and valid from the Saudi perspective. As Holt and Daspit 38 explained, innovation provides a path towards competitive advantage and sustainable performance for organizations. These authors further argued that innovation also creates value for firms. In this context, innovation resources (such as financial and nonfinancial resources and human and nonhuman resources) play a crucial role. Human resources are assets of organizations, such as financial resources, that help organizations attain a competitive advantage and maintain sustainable performance. Health organizations are complex organizations that engage in formal and informal processes and include both medical and nonmedical staff as well as various management structures. Hence, leaders and policy-makers working for health care organizations in Saudi Arabia may improve their innovation capabilities by focusing on innovation readiness; innovation readiness may require an understanding of the centralization of the management structure and financial resources to support the innovation process. To attain a high level of innovation readiness, it is necessary for health organizations to ensure that their staffs are highly and professionally trained to support the implementation of electronic health records. These staff should be sufficiently educated to use such a system. In addition, research and development activities should be conducted at regular time intervals to allow for an understanding of current market trends; implementing this suggestion can help the health care sector remain aware of current trends and survive in the marketplace. Health organizations should be equipped with the latest technology and advanced equipment.
Health care managers and health services managers as well as hospital directors must involve their employees in the decision-making process. Such involvement can motivate health care professionals; in such a state, they feel valued by members of their organizations and are able to provide their own input. The process of implementing an EHRS must be sufficiently fair and adequate. All legal formalities must be followed, and there this process should include the participation of experts and individuals who have knowledge, experience and expertise regarding the implementation of the EHRS in health care organizations. Moreover, the IT division must continuously manage the EHRS databases. Hospital staff must be motivated to support implementation of the EHRS. Support from administrators, such as those working in IT divisions, hospital board members, and senior executives, as well as adequate financial support for the EHRS system are essential for the successful implementation of the system. From Hypothesis 1, it is evident that the innovation readiness scale is positively and significantly related to the centralization of management, i.e., the provision of adequate resources, knowledge, processes, values and goals and support from management and the administration are crucial for the success of electronic health record systems. Furthermore, resources and end users were not significantly related to financial resources and the centralization of the management structure. These results are in line with those of Nieto et al. 39 Thus, we can say that H1 is substantiated and verified. A second hypothesis was developed to test the impact of the innovation readiness scale on the centralization of the management structure and financial resources. To examine this hypothesis, smart PLS-SEM partial least square structural equation modelling was used. Bootstrapping featuring2000 resampling was conducted, and beta values, t-statistics, significance values, i.e., p values, the upper and lower limits of bootstrap confidence intervals, and multicollinearity were investigated. It was found that the innovation readiness scale has a positive and significant impact on the centralization of management and financial resources. According to Hair et al. 32 the VIF value must be less than 5. The researchers concluded that there were no co linearity issues in the structural model. A one-unit change and variation in innovation and readiness could account for a 74.7% change in the centralization of management structure and financial resources. The second hypothesis was also substantiated. Therefore, it can be concluded from the above discussion that PHCCs are ready for implementation of the EHRS, and in this context, management structure, organizational process, and administrative support play important roles.
Practical implications
The results and findings of this study are helpful and beneficial for practitioners and scholars. On a practical level, practitioners can discover which aspects are more important and which factors are relevant to the task of assessing PHCCs’ readiness for large-scale electronic health record systems, which may affect their properly synchronized implementation. The application of EHRS is beneficial for PHCCs. Practitioners must focus on the structure of management, organizational processes and administrative support to assess the readiness of PHCCs for the EHRS. In addition, financial resources and centralization also play important roles in implementing the EHRS. Factors such as resources, end users, organizational knowledge, technology and values and goals cannot be ignored. The qualitative findings provide support to the quantitative findings, and the majority of respondents claimed that PHCCs in Saudi Arabia are ready to implement the EHRS. Respondents highlighted factors such as technology, strengths and weaknesses, and challenges. The most important and substantial effects were determined to be caused by management structure, organizational process and administrative support. The second implication for managers, administration, professionals and decision- and policy-makers is that communication and coordination can be improved in the context of clinical care, which may produce more sophisticated results. Third, through the implementation of electronic health records, better health services may be provided at low cost and more quickly. This process can reduce financial burdens and help health care organizations save financial resources, better manage their resources and attain competitive advantages and sustainability.
Limitations and future research directions
The current study makes several contributions but also faces certain limitations. The data were collected from policy- and decision-makers in Riyadh, so the findings of the current study can be generalized to the Saudi perspective as a whole and to the context of Saudi health care organizations, but these results cannot be generalized to other sectors, such as the education and manufacturing sectors. This study used cross-sectional data drawn from a single source, which may cause bias. It is recommended that future studies collect qualitative data alongside quantitative data to support these findings, and additional longitudinal and multi group data might help future researchers better understand the topic at hand. The sample size of this study was sufficiently small that normality issues may have been a factor; it is better recommended that future studies reference a larger sample size. The sampling technique used may also limit the generalization of the findings, and so it is recommended that different sampling techniques may be used in the future to help researchers better understand the topic at hand. A potential moderating factor that can be examined by future studies could be user involvement.
Supplemental Material
Supplemental Material - Assessing primary health care readiness for large-scale electronic health record system implementation: Project team perspective
Supplemental Material for Assessing primary health care readiness for large-scale electronic health record system implementation: Project team perspective by Haitham Alzghaibi, Yasir H Mughal and Ali H Alharbi, Mohammed H Alwheeb, and Adel S Alhlayl in Health Informatics Journal
Footnotes
Acknowledgements
The authors extend their appreciation to the deputyship for Research & Innovation, Ministry of Education and Qassim University, Saudi Arabia for funding this research work through the project number (QU-IF-2-2-3-26937). Researchers would like to thank the Deanship of Scientific Research, Qassim University for the support of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the deputyship for Research & Innovation, Ministry of Education and Qassim University, Saudi Arabia for funding this research work through the project number (QU-IF-2-2-3-26937)"
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.