
Abstract
Introduction
Health insurance and public health serve distinct roles within the healthcare ecosystem. Public health initiatives such as immunization programs and pollution control aim to enhance societal well-being by addressing collective health concerns. These initiatives are considered public goods—non-excludable and non-rivalrous—funded and implemented primarily by governments. 1 In contrast, health insurance is a market-based mechanism for mitigating individual health risks. It operates as a “club good,” providing financial protection and healthcare access to individuals who contribute through premiums or employment-linked memberships (i.e., it is excludable) while remaining non-rivalrous. This inherent exclusivity highlights significant differences in accessibility and equity between public health and health insurance systems.
Despite its critical role in providing financial security, traditional health insurance systems are fraught with inefficiencies, including fixed pricing structures, limited coverage, reliance on intermediaries, slow reimbursements, and opaque decision-making processes. These challenges contribute to inequities in coverage, erode stakeholder trust, and hinder the system’s ability to adapt to diverse and evolving needs. 2
The distinction between public health and health insurance underscores the need for innovative solutions that address the latter’s limitations while leveraging its potential to enhance individual health outcomes. Unlike public health, which relies on centralized government funding, health insurance has the flexibility to integrate market-based mechanisms and emerging technologies to improve efficiency, inclusivity, and transparency. This study proposes a blockchain-based health insurance framework as a transformative approach to bridge these gaps.
Blockchain technology, a decentralized digital ledger system, has transformed finance, supply chain management, healthcare, and insurance industries by ensuring transparency, security, and immutability without relying on a central authority. Transactions are recorded across multiple computers, with each new transaction linked to the previous one, forming a chain. Initially introduced in 2008 with Bitcoin, 3 blockchain has evolved through several generations. The second generation, marked by the introduction of smart contracts in 2014 through platforms like Ethereum, expanded blockchain’s application beyond digital currencies. 4 The third generation, emerging around 2017, introduced significant scalability, interoperability, and energy efficiency improvements, addressing major limitations of earlier blockchain models. These enhancements enable real-time data processing, lower transaction costs, and improved integration with advanced technologies such as machine learning (ML) and privacy-preserving mechanisms. 5 The current fourth generation integrates artificial intelligence to drive further innovation. 6
Blockchain and smart contracts offer significant potential to address inefficiencies in health insurance systems. Blockchain can improve efficiency and transparency by streamlining processes, reducing fraud, and eliminating intermediaries, while smart contracts allow for customizable insurance plans with faster settlements, enhancing system performance. 7
This study leverages third-generation blockchain technology for its enhanced transaction speed, cost efficiency, and integration capabilities with ML models and smart contracts. Unlike previous generations, third-generation blockchains introduce solutions like sharding and directed acyclic graphs to improve scalability, enabling faster and more efficient processing of health insurance transactions. Additionally, they facilitate interoperability between different blockchain networks, ensuring seamless communication with various healthcare platforms. Moreover, third-generation blockchains prioritize energy efficiency by adopting Proof of Stake (PoS) consensus mechanisms over the energy-intensive Proof of Work (PoW). These advancements are essential for developing a blockchain-based health insurance model that ensures transparency, fraud prevention, customization, and real-time decision-making, surpassing the limitations of earlier blockchain generations.
Literature review
Advancements in healthcare technology highlight the potential of integrating blockchain with emerging frameworks. The existing literature can be categorized into three main areas, as outlined below.
Blockchain in healthcare
Ghadi et al. emphasize the transformative role of the Internet of Medical Things and 5G-enabled Mobile Edge Computing systems in addressing latency, privacy, and computational inefficiencies within healthcare applications. 8 These technologies improve data handling and real-time analytics, while blockchain enables secure management of decentralized health records and transactions, facilitating seamless patient data integration. Similarly, Corte-Real et al. highlight blockchain’s potential for health data sharing, emphasizing its alignment with regulations like Health Insurance Portability and Accountability Act (HIPAA) and General Data Protection Regulation (GDRP). 9
Health data security and privacy
Ensuring patient data privacy is a major challenge in healthcare. Studies propose various blockchain-based solutions, such as hybrid architectures that balance on-chain transparency with off-chain data storage. 9 Nunes et al. explore the use of non-fungible tokens (NFTs) in medical records and pathology exams, demonstrating how decentralized trust models enhance security and efficiency. 10 Additionally, Agbo et al. analyze blockchain’s potential in drug supply chains and remote monitoring while identifying scalability and integration challenges. 11
Blockchain for health insurance
Blockchain has also been applied to health insurance to streamline claims processing and fraud detection. Bae and Yi discuss the eClaim system in South Korea, which automates claim verification using standardized healthcare data. 12 Ismail and Zeadally introduce the Block-HI framework, a blockchain-based fraud detection system that identifies fraudulent claims across multiple scenarios. 13
Beyond automation, emerging research integrates ML techniques and optimization algorithms into blockchain-based healthcare models. Khan et al. demonstrate how advanced neural networks enhance disease prediction, 14 while Shah et al. highlight the role of decentralized models in improving data security. 15
Together, these studies lay the foundation for blockchain’s role in modern healthcare. However, challenges such as scalability, regulatory compliance, and real-world implementation remain, which this study aims to address through a blockchain-based insurance model integrating QV and fraud prevention mechanisms.
Contribution to literature
The proposed blockchain framework builds on existing advancements by integrating blockchain technology with the QV technique and advanced validation mechanisms. By leveraging decentralized structures, smart contracts, and economic theories, the framework addresses key challenges in traditional health insurance, including inefficiencies, fraud, limited transparency, and lack of flexibility. This study contributes to the literature by proposing a blockchain-based model that combines economic principles with innovative technologies. Specifically, it: (1) Develops a blockchain-based health insurance system with smart contracts to offer personalized insurance plans. (2) Employs a decentralized architecture to enhance transparency, trust, and efficiency. (3) Uses QV mechanisms to make decision-making more democratic and ensure fair outcomes. (4) Incorporates KYC (Know Your Customer) processes and ML models to prevent fraud and maintain system security.
By bridging inherent gaps in traditional health insurance systems, the proposed framework delivers a scalable, equitable, and efficient alternative aligned with the health objectives of both individuals and society.
The rest of the paper is organized as follows: Section 2 describes the study’s methodology. Section 3 introduces the blockchain model developed for health insurance. Section 4 outlines a comprehensive evaluation plan for the proposed model. Section 5 discusses the findings, highlights the strengths and limitations of the proposed model, and offers recommendations for future research. Finally, Section 6 concludes the paper.
Methodology
This section outlines the theoretical framework and mathematical foundations of the proposed blockchain-based health insurance model.
Quadratic voting
Quadratic voting is a mechanism designed to enhance the efficiency of collective decision-making processes. Consider a scenario where a group of
In this decision-making process, the voter
Private value and voting cost
Following the model proposed by Posner and Weyl,
17
we consider a scenario involving independent symmetric private values with
Assuming the voting price (
Optimal voting pricing rule

Consider the vote pricing rules:

Combining equations (1) and (2), we get:

Maximizing the utility function gives:

If
Thus, QV balances dictatorship and majority rule. While acting with self-interest, voters unintentionally promote societal welfare. 20 The bottom line is that the quadratic pricing rule is the most optimal for voting.
Validation of health insurance claims
Validating health insurance claims is crucial for ensuring accuracy, transparency, and reliability in any insurance model, particularly a blockchain-based system. Claims data is a vital source of real-world evidence, informing risk assessment, premium calculations, and evidence-based decision-making. Accurate validation ensures computational models reflect real-world phenomena, supporting fairness and sustainability in health insurance systems. 21
In the insurance context, risk is often modeled as a random variable

Here,


Blockchain framework for secure and transparent health insurance
This section presents a blockchain-based health insurance solution, structured into six layers and eight stages. We also incorporate attacks and solutions specific to each blockchain layer to address potential security vulnerabilities. The system’s effectiveness is further enhanced through the integration of the QV mechanism.
Blockchain architecture
The proposed blockchain architecture for health insurance is developed in six layers: Application, Identity and Data Management, Consensus, Smart Contract, Ledger and Storage, and Network. Each layer plays a crucial role in ensuring the security and efficiency of the health insurance system. Figure 1 displays the six-layer architecture of the proposed blockchain model, highlighting the processes managed by each layer and the associated potential threats. A six-layer blockchain model for health insurance with potential threats. Arrowed lines represent the logical flow and interactions between blockchain layers and stages. Dashed lines indicate the threats associated with each blockchain layer and stage.
Summary of threats, relevant layers & stages, and countermeasures.

The Countermeasures column outlines strategies to mitigate these risks, including input validation, ML-based anomaly detection, PoW, PoS, and sharding. These solutions are consistently applied across relevant layers and stages, enhancing the overall security and integrity of the system.
This framework highlights the dynamic interplay between the blockchain architecture layers, their functionalities, and the security mechanisms required to protect the health insurance system from potential threats.
Figure 2 provides a graphical representation of the designed blockchain for health insurance. It illustrates the interactions between key components, showing how blockchain and smart contracts automate processes, from application submission to claims processing, ensuring a streamlined and secure flow of information and transactions. A blockchain-based health insurance system: key components and process flow.
The following section delves into each stage of the blockchain development process, providing a detailed analysis of the identified threats and corresponding countermeasures.
Development stages of the blockchain-based health insurance system
The designed blockchain model for health insurance is structured in eight stages. The following sections provide a detailed overview of each stage.
Stage 1: Application submission
Customers submit an application requesting health insurance services. At this stage, the system may face some threats and require appropriate defenses. • •
Stage 2: Data verification
The insurance company collects and verifies KYC information, including basic identity details such as age and gender, along with additional data such as phone number, address, and social security number. This forms a streamlined electronic KYC (eKYC) system, reducing costs and addressing anti-money laundering concerns. 25
To ensure accuracy, the insurance company verifies the submitted information by connecting to external databases. For example, the Social Security Administration and Department of Motor Vehicles are used to verify identity details, and the USPS Address Verification System ensures the accuracy of the insured’s address.
With the customer’s consent, the insurance company may access medical records from sources like the Medical Information Bureau to mitigate risks such as adverse selection. This comprehensive verification process enables a thorough and accurate evaluation of applicants. • •
Stage 3: Data validation
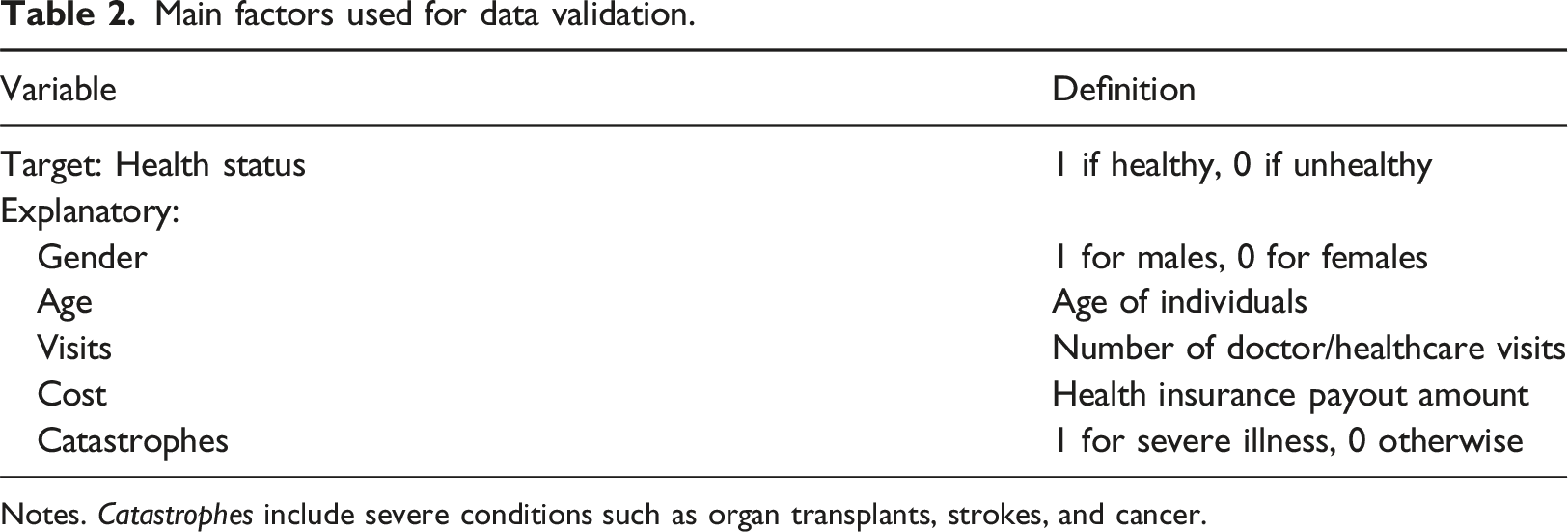
The data validation process involves several steps to ensure accurate health status prediction. First, the target and explanatory variables, as shown in Table 2, are identified. Then, the dataset is divided into training and testing sets in an 80/20 split, where the training set is used to build the model, and the testing set evaluates its accuracy. Subsequently, data normalization is applied to standardize variables like binary gender, numerical age, and monetary cost, enabling meaningful comparisons and effective model training. The multi-layer perceptron (MLP) algorithm is then implemented, defining characteristics and iterations, while weight training determines variable influence to enhance prediction accuracy. Finally, the model predicts health status (healthy or unhealthy) with minimal errors, and validation ensures precise classification to guide premium decisions. • • Main factors used for data validation. Notes. Catastrophes include severe conditions such as organ transplants, strokes, and cancer.
Stage 4: Insurance contract customization
After stage 3, the insurance company creates flexible and fixed-price contracts. The QV mechanism introduces
Table 3 outlines these plans. Columns (4)–(6) display the flexible-price plans, where • Potential Threat: Flooding attacks could impact this stage, where attackers overload the system to cause delays or crashes. • Recommended Solutions: Introduce PoW or rate-limiting techniques to mitigate system overloading. In addition, distributed denial-of-service (DDoS) protection services are to be employed.
29
A flexible insurance contract. Notes. This table presents the insurance coverage details, including maximum reimbursements and premiums under fixed- and flexible-price models.

Stage 5: Insurance plan selection
A sample of recommended insurance coverage and benefits.

For a nonparticipant individual 
Each vote incurs a cost, with the total voting cost (
The total fees collected from all voters are then redistributed equally, giving each voter a share (
It is important to acknowledge that the plan selection stage of the blockchain is susceptible to certain risks: • •
Stage 6: Customer information and contract review
The insurance company reviews the customers’ eKYC information, medical history (obtained in stage 2), and their selected draft contract (specified in stage 5). •
Stage 7: Smart contract integration
The insurance company defines smart contract policies and encodes customer data obtained in stage 6. • •
Stage 8: Smart contract implementation
Smart contracts containing finalized data from stages 6 and 7 are reviewed, approved, and deployed on the Ethereum platform. Ethereum is offered for its role as a leading platform for smart contracts, offering a customizable blockchain architecture that supports decentralized applications. Known for its extensive developer support, well-established ecosystem, and robust security infrastructure, Ethereum provides the necessary functionality to automate health insurance processes. These smart contracts enable secure, seamless, and automated interactions between customers and service providers, enhancing operational efficiency and fostering trust.
1
• •
Evaluation plan
To assess the feasibility and effectiveness of the blockchain-based health insurance model, we propose a multi-stage evaluation strategy. This approach includes a simulation-based evaluation, a real-world feasibility study, and a comparative analysis.
Simulation-based evaluation
The performance of the blockchain system can be evaluated through simulations using synthetic and real-world insurance datasets, where smart contracts could be deployed on Ethereum test networks (e.g., Rinkeby or Goerli) to assess transaction efficiency and scalability. Simulated participants with predefined risk profiles and claim histories will help analyze system behavior under various scenarios.
Moreover, the ML models like XGBoost (Extreme Gradient Boosting) 31 can be integrated to improve fraud detection and cost efficiency (e.g., see Srivastava et al.). 32 Recently, a novel ensemble technique combining Random Forest (RF), XGBoost, and Support Vector Machine (SVM) was introduced to further improve fraud detection accuracy in the Ethereum blockchain, achieving a score of over 98% across key classification metrics, including accuracy, precision, recall, and F1-score. 33
Key performance metrics of the health insurance blockchain model.

Notes. The control group includes customers under the traditional health insurance system.
Real-world feasibility study design
A pilot study could test the model in a real-world setting using data from a mid- or large-sized company. Smart contracts would automate policy selection and claims processing, while quadratic voting would allow employees to prioritize coverage options.
ML models can be used for fraud detection, customer validation, and premium adjustments (i.e., step 3 of the blockchain model). For example, Shouri used health insurance claims data from 29,785 employees of the East Oil Company of Iran, analyzing 148,925 records in 2023. 34 The study used the XGBoost technique to classify individuals as healthy or unhealthy and found that 1.78% of policyholders were classified as unhealthy but accounted for 17.48% of total claims. The model achieved an accuracy of 99.98%, highlighting its effectiveness in identifying high-risk individuals and enabling risk-based premium adjustments.
The pilot study design consists of four main steps: Planning, Data Collection, Evaluation and Analysis, and Finalization and Reporting. Figure 3 represents a hierarchical flowchart of the study design, following a logical grouping of steps and their subsets. Study design for evaluating the efficiency of the blockchain model for health insurance. Solid arrowed lines represent the logical flow between study phases and their interactions with key tasks. Dashed lines indicate study elements, including data points, processes, and actions.
Below, we provide an overview of the main phases of the study design.
Planning
To ensure a robust study, the pilot should begin with well-defined objectives, such as evaluating operational feasibility, user adoption, efficiency improvements, cost-effectiveness, and regulatory compliance. Employees from diverse departments, age groups, and health conditions should be included to ensure broad representation. A clear participant recruitment plan must be established, selection criteria must be defined, enrollment procedures must be established, and informed consent must be obtained.
Data collection
Data collection will involve both quantitative and qualitative methods. Surveys and questionnaires will measure key metrics such as adoption rates, user satisfaction, trust in the system, and efficiency gains, while in-depth interviews and focus groups will provide richer insights into user perceptions, challenges, and preferences. Both baseline and follow-up measurements will track the impact of blockchain adoption over time. Additionally, a control group using traditional insurance methods will allow direct performance comparisons by analyzing differences in claim processing time, administrative costs, and fraud detection rates.
For example, data can be collected electronically via questionnaires to analyze the effectiveness of the QV model. Similarly, surveys can assess whether policyholders feel that quadratic voting results in fair and customized coverage options. Additionally, historical data could be used to validate health insurance customers. Finally, ML-based risk assessment models can also be integrated to analyze premium calculations and enhance fraud detection by identifying patterns in fraudulent claims.
Evaluation and analysis
The evaluation will also incorporate expanded metrics such as adoption rates, efficiency improvements, user experience scores, cost savings, and regulatory compliance. To refine the system before full-scale deployment, feedback should be collected at multiple stages. A risk management plan will identify potential challenges, including technical issues, data privacy concerns, user resistance, and mitigation strategies.
Evaluation factors for assessing the blockchain-based health insurance model.

Finalization, reporting, and documentation
Comprehensive reporting and documentation will be essential, covering study design, data collection instruments, analysis methods, and ethical considerations such as participant confidentiality and compliance with healthcare regulations. Additionally, scalability and integration testing will assess the system’s ability to handle increased users and its compatibility with existing health insurance providers and hospital systems.
Comparative analysis
Comparative analysis of blockchain-based and traditional health insurance models.

Discussion
Blockchain technology has transformative potential in health insurance, where traditional fixed-coverage contracts limit customer choices. By incorporating QV techniques, this study introduces a democratic approach that offers flexible contracts with customizable coverage and pricing options.
An eight-stage blockchain system was developed to enhance the health insurance system. The MLP neural network validates customer information in stage 3, while stages 4 and 5 implement the QV model. These stages empower customers to vote on preferred coverage-price combinations, optimizing medical reimbursement and introducing a dynamic pricing model. Additionally, voting is crucial in identifying optimal contracts and enhancing reimbursements. Finally, blockchain strengthens fraud prevention through KYC validation, eliminates intermediaries, and enables instant settlement of treatment costs, enhancing trust and efficiency.
To assess the effectiveness of the designed blockchain, we offered a comprehensive evaluation plan, including simulation-based assessments for transaction efficiency and scalability, a real-world pilot study to test user adoption, and a comparative analysis with traditional models to measure improvements in fraud detection, cost efficiency, and user control.
Strengths of the proposed model
The blockchain-based health insurance model presents several advantages over traditional systems. Blockchain technology enhances transparency and trust, as all transactions are recorded on an immutable ledger, ensuring auditability and fraud resistance. The integration of QV empowers customers to actively participate in the plan selection process, creating a more democratic and inclusive system. This model also strengthens fraud prevention by utilizing KYC processes and ML models to detect and mitigate fraudulent activities. Additionally, smart contracts automate administrative tasks, eliminating intermediaries, reducing operational costs, and ultimately improving efficiency.
Comparison with recent studies
The study’s proposed blockchain-based health insurance model advances beyond recent studies by seamlessly integrating multiple innovative features into a unified and comprehensive framework. Prior research primarily focuses on automating claims, enhancing transparency, or addressing fraud.12,13,26 However, our model combines these aspects with a user-centric approach. Specifically, it incorporates ML models with decentralized KYC validation for robust fraud prevention and introduces QV to enable customer-driven customization of insurance plans. This holistic integration addresses system inefficiencies and fosters inclusivity, delivering broader applicability and functionality compared to earlier models.
Limitations of the proposed model
Despite its advantages, the model faces several challenges to implementation. Integrating blockchain into healthcare systems requires technical expertise, resources, and organizational changes, which could slow adoption. High implementation costs may be a barrier for smaller entities, and regional regulatory compliance introduces complexity. While blockchain provides a secure framework, continuous monitoring is necessary to protect data privacy, particularly during the KYC process. The lack of real-world testing further underscores the need for pilot programs to assess its practical application. Lastly, the implementation of QV and blockchain may not be readily generalizable, necessitating further research to evaluate its broader applicability.
Recommendations for future research
Future research should focus on evaluating the framework using real-world data. Conducting pilot programs across diverse healthcare systems and expanding the model to national, public, and private settings will provide insights into its performance and help assess its broader applicability. Integrating the framework with existing insurance platforms is crucial to address interoperability challenges. Additionally, exploring cryptographic methods such as zero-knowledge proofs will be key to ensuring data protection and regulatory compliance.
Conclusion
This study demonstrates the transformative potential of blockchain technology in health insurance by addressing long-standing inefficiencies and limitations of traditional systems. The proposed model incorporates an eight-stage blockchain framework and integrates QV techniques, enabling customers to access customizable contracts and dynamic pricing. This design fosters a more inclusive and democratic insurance process.
Additionally, integrating ML techniques for fraud prevention and decentralized KYC validation strengthens trust and improves operational efficiency. Smart contracts reduce administrative overhead and expedite reimbursements, marking a significant advancement over traditional models.
As blockchain technology evolves, this framework underscores the value of combining technological innovation with economic principles to create scalable, equitable, and efficient systems. Although challenges in adoption and implementation remain, this work provides a foundation for future interdisciplinary research and real-world applications, with the potential to modernize health insurance and inspire similar transformations across various industries.
Footnotes
Acknowledgments
The authors extend their gratitude to the two anonymous reviewers for their insightful comments and constructive feedback, which significantly enhanced the quality of this paper. We are also grateful to the editors for their guidance and support throughout the review process. Special thanks to Glen Cooper for his assistance in proofreading and improving the clarity of the manuscript.
Ethical statement
Author contributions
Saeed Shouri led the development of the blockchain framework and authored the discussion and conclusion sections. Rasoul Ramezani contributed to the development of the introduction and methodology sections and played a key role in designing the blockchain architecture. He also prepared both the original and revised versions of the manuscript. Both authors collaborated on designing the evaluation plan and thoroughly reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.