
Abstract
SAFE is a mobile application co-created for and by people who have experienced self-harm, either themselves or as next of kin. This study intended to integrate SAFE into an Emergency Department (ED) to help patients share experiences of self-harm and to support professionals in conducting treatment as usual (TAU).
Introduction
Self-harm, which refers to any intentional self-poisoning or self-injury carried out by an individual irrespective of motivation, 1 is a major public health concern 2 with an average of at least 6400 cases a year in Norway. 3 This corresponds with the numbers in Denmark, 4 and the highest number of new cases of self-harm without suicidal intention is seen in the age Group 16–24 years for all genders.4,5 People who self-harm (PSH) experience significant health inequalities and have an increased risk of mortality. 6
Self-harm not only affects the individual; it also triggers feelings of powerlessness and suffering in others, including healthcare professionals (HCPs) who witness the psychological pain. 7 In addition, HCPs find the self-inflicted actions and the complexity of patients’ needs difficult to manage and understand because of their own feelings and moral beliefs, and they may react to patients with annoyance and rejection.8,9 According to Perboell et al., 10 such reactions may occur due to insecurity and lack of knowledge, and based on their investigation they argue that confidence and empathy depend on knowledge and experience; in spite of this, few HCPs receive education about self-harm. 10
General Emergency Departments (EDs) are typically the first point of contact for PSH when they need crisis care; however, their mental health history may overshadow their immediate needs. Often, HCPs meet them with judgment and stigma, 11 which increases the risk of inadequate care and treatment8,12,13 For example, human interaction is overlooked, and the go-to treatment of these patients is often short-term safety interventions, such as risk assessment and control, instead of sharing experiences where the HCPs are open and sensitive to the needs of the PSH.14,15
PSH often do not seek help from HCPs. 16 Rather, they seek to solve their problems via social media and in private virtual networks where they can share difficult thoughts and feelings. 17 However, these private networks can also motivate self-harm, and sharing self-harm experiences only with like-minded persons may worsen a critical process. 18
Digital technology is increasingly implemented within mental healthcare. 19 An increasing number of studies conclude that digital technology can lead to a decrease in acts of self-harm, e.g., by helping people handle stressful moments and learn long-term coping skills.17,18,20 However, employing technology to motivate patients to share experiences of self-harm and to support treatment as usual (TAU) can be challenging because HCPs, in addition to lacking knowledge about self-harm, must also familiarise themselves with such unfamiliar digital solutions. 21
Integrating a mobile application into the ED
The mobile application (app) SAFE 22 is targeted to PSH, relatives, and HCPs. Co-created for and by PSH, SAFE seeks to empower people to engage in decisions about their own lives. It supports interactions and dialogues between this population, their relatives and HCPs and thus allows them to share experiences. SAFE has three entrances where users can choose if they are: (1) a person who self-harm, (2) a relative or (3) a professional. The app is underpinned by the theoretical framework of Safewards 23 and Trauma Informed Care (TIC), 24 including the principles of empowerment and transparency, and the app is developed by people with lived experiences of self-harm. The app contains more than 30 Calm Down Methods (CDMs)23,25 to regulate emotions (see Supplemental File S1). Furthermore, SAFE allows HCPs to learn about self-harm and the needs behind patients’ behaviour. The app also offers professional suggestions for care and for supporting patients in sharing their experiences. In doing so, SAFE may strengthen knowledge, confidence and empathy in HCPs.
An ED was aware of their difficulties in coping with PSH and wanted to integrate SAFE. We therefore decided to utilise a Co-operative Inquiry research approach,
26
which is a method for conducting research with people with similar experiences who wish to engage in a joint examination of how they might extend and deepen their understanding of their situation, and who wish to learn how to improve their practices.
26
Professionals from the ED were involved in designing the study, which took place in 2021 – 2023 (Figure 1). The Co-operative Inquiry included four research steps.26,27 In the first step, preparation, the research design were agreed upon. In the second step, orientation, two workshops with ED nurses (2), managers (1), researchers (3) and service-users with lived experiences of self-harm (2) were carried out, a learning intervention was designed, and the implementation and evaluation were planned. In the third step, implementation, the workshop participants facilitated the learning intervention in the ED. The fourth step, evaluation, comprised an interview study, which is reported in this paper. Flow chart of co-creation process of the study.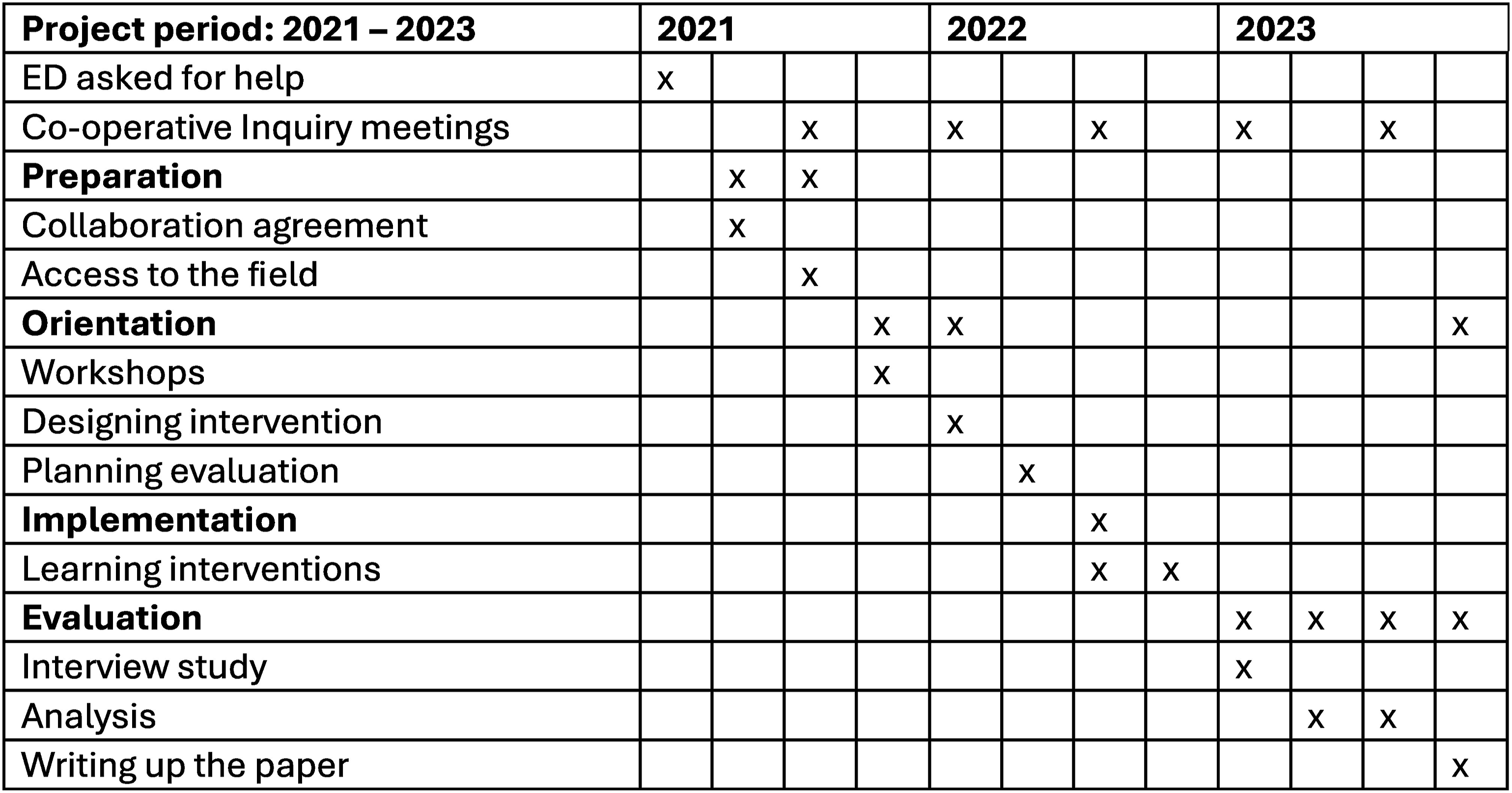
This process provided a possibility to investigate learning processes related to whether and how technology can influence TAU in EDs to PSH. The objective of this study is to continue the co-creation process by including knowledge from HCPs about how they believe technology can support TAU to PSH and thereby help understand this population and their needs. Specifically, we explored ED nurses’ reflections and learnings while integrating SAFE into their practice.
Methods
The research methods were explorative qualitative interviews 28 and reflexive thematic analysis. 29 The setting was a general ED in Denmark which by Danish standards had an average size and staffing consisting of 275 registered nurses and other cross-functional healthcare staff. The ED receives more than 70,000 patients annually and provides critical care to PSH, among other things.
Learning intervention
In addition to achieving the specific research aim, a Co-operative Inquiry approach also ensures that the research intervention is co-produced and relevant to practice. There were different underlying expectations related to the different stakeholders
30
: (1) Nurses were supposed to reflect upon and learn to use the app alongside engaging with PSH in TAU. (2) Managers were supposed to ensure competencies among staff members. (3) Researchers wanted to gain knowledge about the target group and about how SAFE could be integrated into care procedures. (4) PSH wanted to be met as human beings and to teach staff how they wanted to be treated. These expectations were transparent and were aligned during the process. The learning intervention was designed as an interactive workshop, inspired by the participatory paradigms’ four interconnected ways of gaining knowledge, which influence each other.
31
We presumed that the dynamic interaction between experiences, presentations, theory and practical training could strengthen knowledge, confidence and empathy in ED nurses, who would simultaneously gain familiarity with technological solutions. Figure 2 illustrates the learning intervention. It shows the didactic process that involved a collaboration between the different types of teachers. Altogether, 19 nurses participated in the learning intervention. The teachers facilitated the SAFE implementation by putting up informative posters, delivering folders and having interactive dialogues about SAFE and its potentials. Also, pictograms and tools to support CDMs
25
were widely provided in the ED. Description of the learning intervention.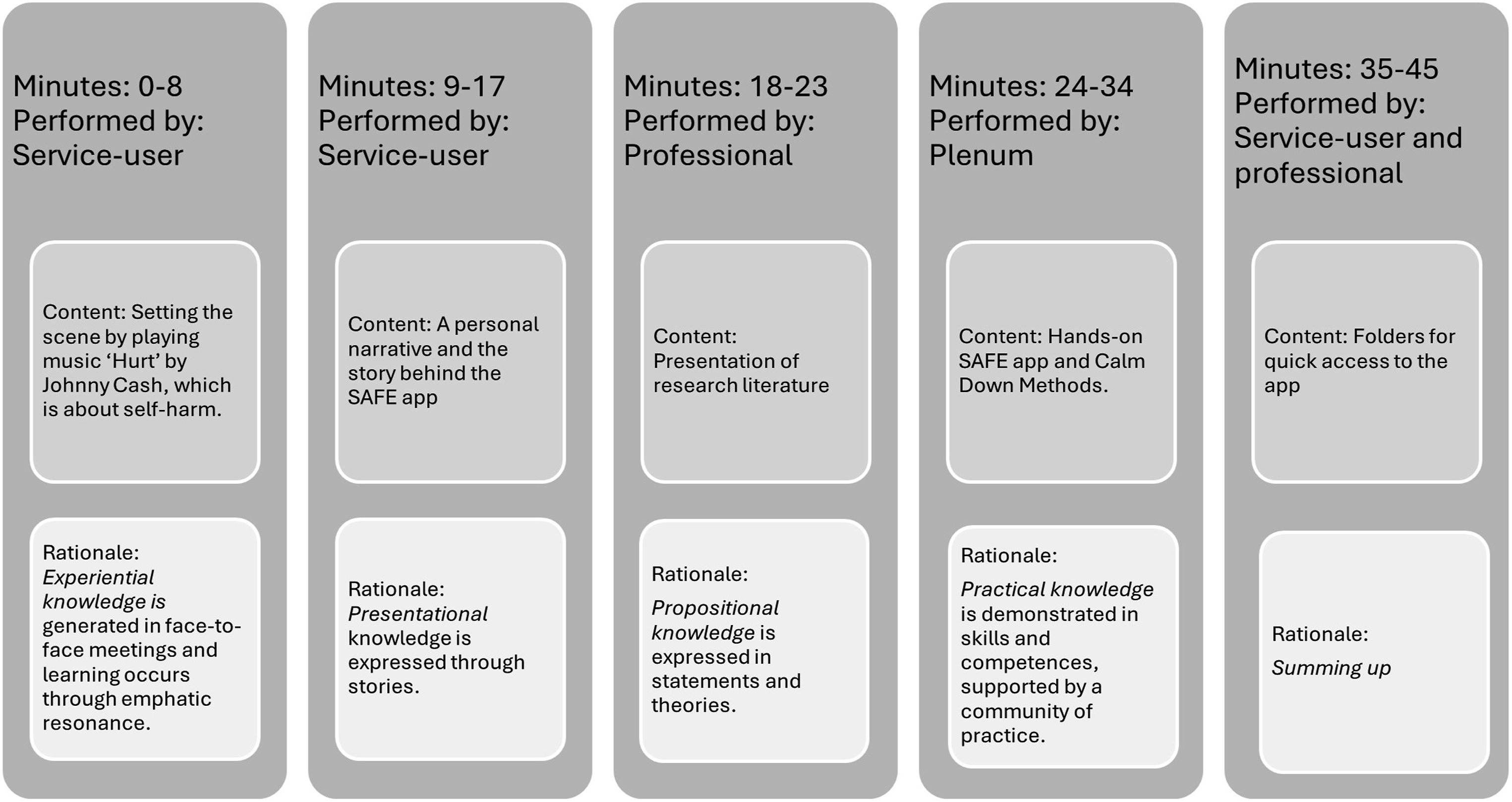
The interview study
The 19 nurses, aged 24–64 years (mean 40.5 years), who attended the learning intervention, were invited to participate in an individual interview 28 approximately 6 weeks after the learning intervention. However, six were not able to due to a lack of resources in the ED. The remaining 13 informants received an email providing information about the interview. All informants had previously met the interviewers, who were nurses (LBØ, LMC, AJ), at the learning intervention (see Figure 2). Three informants had experience in psychiatry, but only one had knowledge about self-harm. Out of the 10 informants without psychiatric experience, six knew of self-harm. None of the 13 informants had formal education on the subject.
With the aid of a semi-structured interview guide, 28 informants were asked about their experience with treatment for PSH, see questions in Supplemental File S2. The guide was informed by literature, the workshops and reflections upon the learning intervention. The interviews took place in the ED and lasted 28–58 min (38.5 m on average). Richness in the data set provided data adequacy.29,32
Analysis
Audio-recorded interviews were transcribed verbatim (143 pages/78,922 words) and analysed using the framework of reflexive thematic analysis (RTA).29,33 This approach ensured that data were analysed in a manner that respected and expressed the nurses’ first-person accounts while also acknowledging the reflexive impact of interpretations 29 within the research team that consisted of nurses with various experiences within lived experience in self-harm, mental healthcare and qualitative research. The six-phase analytical process began with familiarisation, in which all transcripts were read several times and initial ideas for coding were identified. In the second phase, the entire dataset was coded by the second author, and the third phase consisted of repeated iterations of coding and an initial generation of themes within the whole research group. In phase four, potential themes and sub-themes were reviewed in consistency with the coding and the final themes were defined. Also, each theme was further refined, and illustrative quotes were selected in phase five. Phase six, the reporting, is presented in the section on findings.
Ethics
We followed formal ethical rules for medical research. 34 The use of SAFE was voluntary. All participants were informed about anonymity, they gave written consent, which they could withdraw at any time, and data were kept confidential. As the nurses were engaged actively in the study, there was a specific obligation to share knowledge and reflections about the research during the process. The study was approved by the Danish Data Agency.
Findings
We identified two main themes and five sub-themes in the data of ED nurses’ reflections on providing care to PSH and their learnings while integrating SAFE into practice (Supplemental File S3). The first main theme, ‘Increased awareness to the potential of person-centred technology’, included understandings and expectations that nurses generated regarding the app. The second main theme, ‘A hesitant approach to the adoption of person-centred technology’, involved nurses’ attitudes and anticipated barriers to integrating SAFE into their practice.
Increased awareness to the potential of person-centred technology
This main theme accounted for nurses’ reflections on how they could translate their new understandings and basic experience with the app into TAU. The two sub-themes were: ‘Pros and cons in anticipated usefulness’ and ‘SAFE as a potential digital game changer.’
Pros and cons in anticipated usefulness
Due to the short period after the learning intervention was held, most of the nurses found limited opportunity to gain further familiarity with SAFE, since the learning intervention. However, the opportunity to support their dialogue with patients by using the app was mainly encountered with interest. Nurses’ attitudes to digital technology differed, but the fact that SAFE was co-produced and introduced by PSH aroused their curiosity. For example, the smart user interface with different entrances to patients, relatives and HCPs was mentioned as making SAFE attractive to explore further. A young nurse stated: It’s easy to navigate and it’s appetising and makes you want to check it out (I-9).
This quote reflected its appealing nature and as such, most of the nurses presumed that the app would be useful to a broad range of people in contact with the ED. However, some also foresaw a diversity of challenges, which was expressed in a more general concern for excluding patients with low readiness to access a mobile application. Issues such as age, digital and cognitive capabilities, and the type and severity of symptoms must be taken into account to ensure that SAFE would be an appropriate tool for the individual patient.
SAFE as a potential digital game changer
Some of the nurses explained how SAFE forced them to change their view on TAU, in which patients’ safety and treatment of the acute injury were in focus. A majority of the nurses found it challenging to engage in dialogues with patients about self-harm. However, one seasoned psychiatric nurse mentioned that SAFE could build a bridge between patients and HCPs (I-12). Another trained ED nurse, with no experience in psychiatry, explained: We want to solve their problem and fix it. We don’t have to do that, we just have to be with them without having to fix a problem others might have tried for months (I-6).
This nurse exemplified the game changing from ‘just fixing’ towards a new understanding of adapting a reflective listening approach without needing to fix underlying causes of self-harm. This belief in being able to promote safe and equal relationships indicated a hopeful attitude in the nurse. The app seemed meaningful to integrate into the ED context, and the nurses deemed it likely that they would choose these methods in future care, thus showing a certain willingness to develop TAU.
A hesitant approach to the adoption of person-centred technology
In this main theme, the nurses demonstrated a hesitant approach, which implied reflections on how they could integrate SAFE into TAU. Despite the increased interest, nurses described an uncertainty, which is unfolded in three sub-themes: ‘Foreseen contextual challenges,’ ‘Worries about the added value,’ and ‘Uncertainty about own skills.’
Foreseen contextual challenges
The hesitance towards SAFE was explained by a diversity of challenges linked to the ED setting and culture. Some nurses reported a lack of opportunity to test the app because they had not met PSH on their duty. Other barriers reported included limited resources and lack of practical access to mobile devices. In addition, most nurses doubted how much the app would support them in their brief encounters with patients. I don’t know how much it [the app] will help us, because they [patients] stay here for a short time… it’s kind of a pit stop (I-11).
Describing the ED as a pit stop in which an app was of no use underestimates the importance of the nurses themselves in crisis care. The above quote exemplified how a large flow of patients, heavy workload and time constraints were contextual factors not seen to provide optimal conditions for care to PSH in general, nor for the adoption of person-centred technology. When it came to critically affected patients in need of crisis care, the idea of using the app was difficult to grasp, as the nurses believed that patients were unable to engage with the device.
Worries about the added value
Nurses’ worries about the value of using SAFE in the interaction with patients contributed to their hesitance regarding the app. The difficulty of anticipating patients’ reactions was a dominant concern, centring on critical reflections on how an app featuring CDMs would be received. One trained ED nurse expressed this concern: Will it cause a distance when you ask, ‘Have you tried this [SAFE]?’ or, on the contrary, cause a better relationship? (I-2).
This quote shows an uncertainty about whether integrating the app into care would work as intended. The risk of creating a distance led to a fear of doing more harm than good. For example, one of the young nurses imagined how patients might respond to an app that originated in a psychiatric context: When I say: ‘You have to download this app and [patients] will ask why?’ Then I’ll answer: ‘I think you’ll benefit from it [SAFE] and if they [patients] are not known in the psychiatric field, it can be a bit judgmental’ (I-7).
This nurse explained how she was afraid of stigmatising and creating distance. Many of the nurses furthermore worried that the app might be belittling and inappropriate for, say, agitated patients. A risk that the interaction with patients would be negatively affected made nurses distrust the app and held them back from choosing it as a supplement to TAU.
Uncertainty about own skills
The hesitant approach was also linked to nurses’ previous experiences of feeling incompetent in terms of how to interact with PSH. They described how they tried to avoid the care of psychiatric patients, which they ascribed widely to patients’ unpredictable and unintended reactions to their communication. Furthermore, a lack of confidence in being able to introduce the app made some nurses feel unequipped to utilise it. One trained nurse wondered whether presentation of SAFE ought to be a part of her work: If they [patients] knew about it [SAFE] in advance, it would be fine, but we don’t know how to introduce it. If you have a good idea of how we could introduce it, we might do it (I-7).
This reflection illustrates a certain openness towards wanting to learn more about how to engage with the app together with patients. In their request for clear instructions to follow, the nurses nevertheless gave the impression of feeling like unskilled novices. At the same time, a community of learning practices was missing, and the collegial support was poor, as they did not see their colleagues using the app. As suggested by one trained nurse, attention to the app should be ‘verbalised repeatedly during the daily morning meeting’ (I-3). Such reminders and encouragement could stimulate learning in practice and support nurses in building new skills in taking a digital approach to care.
Discussion
This study shows nurses’ nuanced reflections and learnings while integrating SAFE into care in the ED. As EDs might not be a first-choice place to treat people in acute episodes of severe distress such as self-harm, 35 and as the treatment should be informed by peer support and TIC, 24 the study illuminated how nurses became encouraged to understand their regular methods of care in new ways. Nevertheless, they were hesitant towards using the app, as they foresaw multiple challenges, such as the risk of stigmatising, which held them back from engaging with the technology in practice. TIC 24 is not integrated into Danish Health Care, but several principles of TIC, 24 such as empowerment and transparency, are integrated in SAFE and in addition the app is developed by PSH. 36
The potential game changer of integrating SAFE into care constituted a significant change in the care usually provided. Before the learning intervention, the nurses in our study usually sought to ‘fix’ all underlying problems of self-harm; but the learning intervention and using SAFE made them aware that patients wanted presence and attention to their immediate suffering while being in a crisis. In the same way, HCPs in the study by O’Keeffe et al. 14 underestimated the significance of the interaction, while patients considered a ‘human’ connection with a focus on hope as a therapeutic intervention in its own right. With SAFE, nurses in the current study discovered a new promising tool to support a hopeful dialogue with patients about CDMs, 25 which forced them to engage with patients as partners, rather than only resorting to risk assessment and control. 14 This approach may support personal recovery 37 as it creates hope and empowerment when patients choose solutions themselves to solve their problems. Thus, nurses are required to step away from their expert role and become professional partners with patients and learn from them, as the literature highlights that some PSH know how to use digital technology to regulate their emotions.17,20
The hesitant approach among ED nurses in this study was due to several reasons, including both difficulty and uncertainty in adopting digital approaches. This is noteworthy since several studies indicate that PSH appreciate digital solutions,17,18,20 which corresponds to the stance of the users who participated in developing SAFE. If nurses distrust the solution and presume that they are stigmatising or distancing themselves from patients, the latter continue to engage with the technology on their own. Distrusting the technology, as our findings show, might be due to a more general inability to connect with PSH, which is in line with O’Keeffe et al., 14 who found that HCPs’ approach to care and the environment of the ED posed limitations for building up a therapeutic connection with patients. As requested by the nurses in our study, SAFE was introduced as a solution to meet such challenges in a person-centred way. However, they still hesitated to include it in interactions, e.g. with agitated patients, even though the CDMs 25 in the app targeted this patient group. CDMs 25 adapted from Safewards 23 are important to mitigate agitated behaviour and can be used to help patients de-escalate, particularly when nurses help patients process their experience afterwards by reflectively listening to patients about what brought them to this situation. 38
This study showed that a biomedical approach, a heavy workload, a lack of mobile devices and a lack of daily attention to the app were perceived as challenges by the nurses, making it hard to see how to apply achieved knowledge to an ED context. Konttila et al. 39 highlight how organisational support to ensure sufficient resources, time and equipment, and collegial teamwork are essential factors to enable HCPs to improve skills in digitalisation. Hence, the contextual challenges pointed out in this study may affect the opportunity to build up experience with the use of digital technology. Even though a previous study of patients’ experiences of SAFE in the same ED context showed how access to SAFE could make the waiting hours in the ED more humane for PSH 31 the nurses nevertheless described the ED as a pit stop, with no time to use an app.
Bucci et al. 19 highlight that co-production and collaboration with users are critical to successfully improving HCPs’ response to digital approaches in mental healthcare. The participatory study design is consistent with this point of view; nevertheless, nurses in the study showed considerable uncertainty and asked for further training. Despite the potential of SAFE to promote empowerment in patients, the nurses may fear to stigmatize patients by insinuating that they might have a psychiatric disease. This would distance them from patients and create health inequalities. 11
The learning intervention included several means for gaining knowledge and evoke empathy and compassion, such as when one of the teachers told her personal story of living with self-harm, and how she was met in the ED. The nurses appreciated this story; however, it did not motivate them to use the app. Achieving confidentiality and new learning requires continual processes of reflection on practice. It cannot be created through theoretical explanations alone.38,40 Therefore, it is essential to create a learning environment in which it is possible to connect the four ways of knowing (Figure 2). SAFE includes several ways of learning to cope with self-harm, including video-clips of personal experiences. However, the readiness to trust technology and incorporate dialogues about the use of digital tools in this target group needs further investigation. Although HCPs may believe they cannot be replaced by technology, PSH use this technology already.17,18,20 HCPs must be able to understand the needs behind the self-inflicted injury and SAFE has the potential to provide this new understanding – however, nurses must step away from their position as experts and become partners with the patients. SAFE has shown the ability to create such space for partnerships. 36 Through this partnership, nurses can build a collaborative relationship with persons who mostly suffer alone. In a future with digital technology, it is furthermore important that clinicians take a critical view of the devices and know how to combine their own knowledge with digital knowledge to customise the solution directly to patients.
Strengths and limitations
This study details novel insight into how digital technologies developed to support PSH, relatives, and HCPs can be used within a general ED hospital setting. It elucidates plausible resistance foci, such as not using the app due to worries about stigmatisation. While only 13 nurses’ reflections were analysed, these voices are helpful when decision-makers must decide how to integrate digital solutions into healthcare settings. A key strength in our study is that stakeholder involvement shaped the research. For instance, the learning intervention was co-produced with important stakeholders from the field. Our findings were limited to one hospital setting, but we believe that the insight they provide into HCPs’ reluctance to combine digital technology with TAU is important in future health care.
Conclusion
Digital technology grounded in the lived experience of PSH can be rewarding for nurses and has the potential to develop innovative practical skills and changes within a partnership approach. To integrate digital technology into TAU can be a game changer and it is necessary to ensure continuous, reflective learning processes in hospital departments. Future research on HCPs’ perceptions of digital technology must focus on how trust can be established. Trust may occur when the solution helps nurses understand PSH’s distress, which enables them to become open and sensitive to their needs.
Supplemental Material
Supplemental Material - Emergency department nurses’ learning and evolving perspectives in interacting with patients who self-harm. An explorative interview study of the use of a mobile application
Supplemental Material for Emergency department nurses’ learning and evolving perspectives in interacting with patients who self-harm. An explorative interview study of the use of a mobile application by Lene Lauge Berring, Ingrid C Andersen, Lise Bachmann Østergaard, Cecilie Borges Bygum, Line Marie Christensen, Ditte Høgsgaard, Anja Rebien Johannesen and Charlotte Simonÿ in Health Informatics Journal.
Footnotes
Acknowledgements
The authors would like to acknowledge the nurses and managers who generously gave of their time and insights while reflecting on the use of SAFE app. They participated from Emergency Department, Naestved, Slagelse, and Ringsted Hospitals. We would also like to thank SDU communication for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Slagelse Foundation [grant number SLA-2021-1].
Ethical statement
Data availability statement
The data set is available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.