
Abstract
Keywords
Introduction
In the case of a first-class infectious disease such as coronavirus disease 2019 (COVID-19), epidemiological investigations take much time and present difficulties. An epidemiological investigation is a difficult task for both epidemiologists and infected individuals. If an infectious disease is suspected, it is essential to conduct an epidemiological investigation. Individuals are expected to recall and report their contact route during the assumed infection period. 1 They should also provide their demographic and clinical characteristics to epidemiologists. While rapid epidemiological investigations are crucial, it is often challenging for subjects to remember details about their movement and infection during the disease’s incubation period. This epidemiological investigation has the disadvantage of relying only on data from infected people. Accordingly, it has limitations in terms of a lack of real-time data updates, misinformation, and manual data collection and analysis. Therefore, it is necessary to establish an environment where people can manage infectious diseases independently and actively participate in epidemiological investigations. 2
Since the outbreak of COVID-19, various digital contact tracing technologies have been developed to prevent and control the spread of existing infectious diseases.3–10 This technology verifies information regarding an infectious disease risk area and an infected individual, records the contaminated area data, tracks the location, and compares this location with the data on the infectious disease-contaminated area. When the location corresponds to an infectious disease-contaminated area, it is designed to receive the log record from a mobile terminal that sends the visitation log of the infectious disease-contaminated area. While these technologies may aid in epidemic control mechanisms, 11 they are limited by their inability to provide detailed accurate state information about the user. Additionally, there are difficulties in contact tracing and monitoring due to a lack of voluntary participation and misinformation. 12 Although it is possible to build extensive data sets corresponding to location, data related to state information may only be partially collected based on the selected state information. Therefore, challenges arise in constructing and generating comprehensive big data and maintaining accuracy regarding the status of infectious disease patients. Consequently, the effectiveness of these technologies is still controversial and needs more empirical studies.13,14
Therefore, we developed an epidemiological investigative support application based on an infectious disease self-management model. This study attempted to develop voluntary data collection application for the epidemiological investigation of infectious diseases through the donation of infected patient data. We aimed to develop and evaluate application to support epidemiological investigations by local governments using big data from infectious diseases.
Methods
Development environment
We used the Double Diamond design process to develop the application. The Double Diamond design process consists of four stages: Discovery, Define, Develop, and Deliver. 15
For the Discovery and Define stages, there was a need to find out which applications were most needed and what services were needed to overcome COVID-19. We conducted a pre-online survey on the most needed applications related to COVID-19 between November 11 and December 6, 2020. From the analysis of 1148 data, we found that applications designed for epidemiological investigations are the most crucial in preventing COVID-19 (61.8%).
16
Thus, we developed the KODARI application, an epidemiological investigation support system based on an infectious disease self-management model.
17
The KODARI application means “KOREA with a diary.” The KODARI application is a Korean version, and there is an English version, MEDARI application
17
(Figure 1). In the development stage, this study developed KODARI application, utilizing various software and systems. Initially, the server’s operating system was Ubuntu version 20.04, developed by Canonical Ltd In England. Subsequently, the application operated on the PHP 8.0 Laravel framework, developed by Zend Technologies Ltd In Cupertino, California, USA. Moreover, the database server utilized MariaDB 10.51, developed by the MariaDB Foundation. Lastly, the mobile applications were implemented on iOS/Android platforms. Architecture of the KODARI app.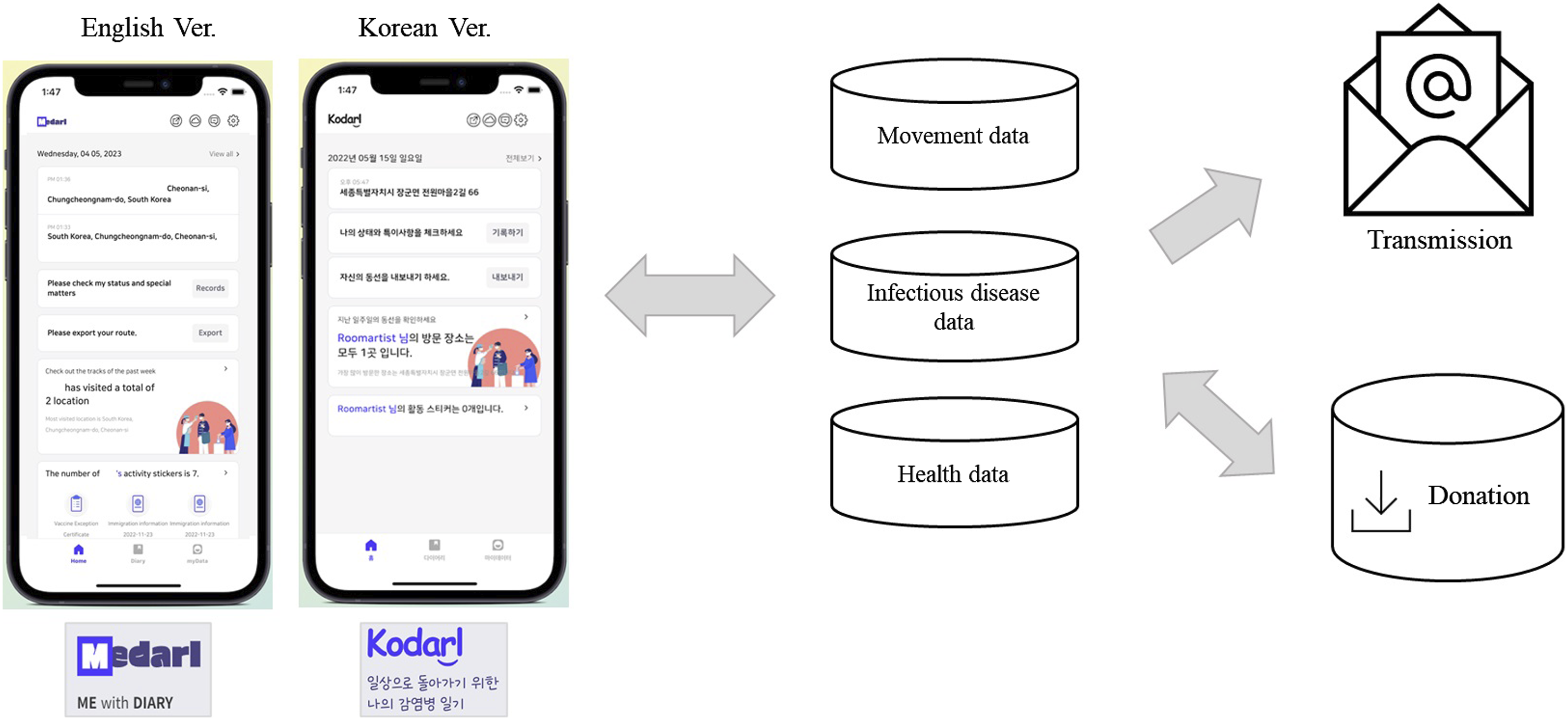
Application user collection items
Items of the KODARI based on the epidemiological investigation form for COVID-19(Ver. 6).
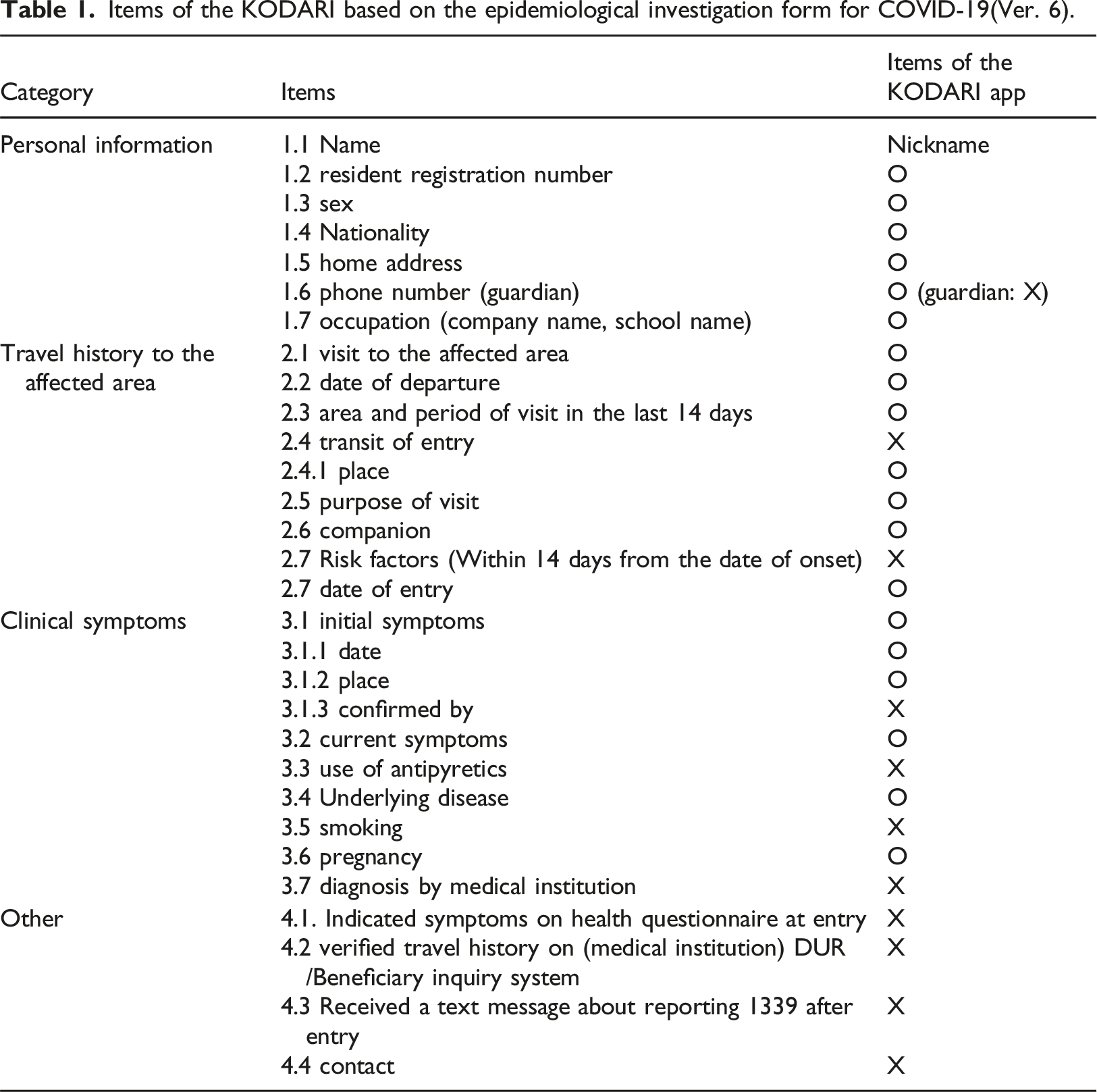
The extracted items are reflected in the Input and Update units of the KODARI application. The epidemiological investigation form for public health centers (version (6) is divided into four primary sections: (1) personal information (seven items), (2) travel history to the affected area (seven items), (3) clinical symptoms (six items), and (4) other (four items). Additionally, there are four specific items that the municipal epidemiological investigation team is required to enter directly. Several items from the epidemiological investigation form are incorporated into the application; consequently, we extracted these items. The extraction of the main user collection items from the KODARI application was conducted by four researchers, including two with doctoral-level qualifications, one with a master-level qualification, and one researcher. While we aimed to integrate as many items as possible into the KODARI application, not all items could be applied.
Furthermore, this study encompassed data not captured in the initial epidemiological investigation form, incorporating additional collection items such as personal health information and vaccination history. Personal health information was meticulously selected after consulting with a physician, focusing on elements pertinent to COVID-19; this included underlying diseases, pregnancy status, history of cancer treatment, immunosuppressive conditions, confirmed infectious diseases, and side effects from vaccinations. Additionally, detailed vaccination records and exemption certificates were available. Users also had the option to manually log COVID-related assessments, including test results from medical facilities, self-diagnosed test records, and antibody testing outcomes.
KODARI application evaluation
We employed a set of 11 questions to assess the application (Appendix table 1): three questions were concerning the willingness to utilize the healthcare application related to infectious diseases; two questions were about the willingness to record movement; two questions evaluated satisfaction with the KODARI application; one question addressed the burden associated with using the KODARI application; one question gauged the intention to use the KODARI application; and two questions explored the value of the KODARI application.16,21–24
The survey period was from December 02 to December 14, 2022. Participation was only possible if informed consent was obtained prior to the survey. Furthermore, only users who donated data to the KODARI application participated in the online survey. Voucher coupons were provided to those who responded.
Inclusion/exclusion criteria
Before the Deliver stage, we conducted an online survey to evaluate satisfaction with the KODARI application. The inclusion criteria are those who have used KODARI application for more than 2 weeks after installing it. The target was Koreans in their 20s and 40s who own an Android smartphone. The target was a user who donated data in the app. Exclusion criteria are those who have only installed the application but have not used it for more than 2 weeks. The exclusion criteria are those who did not donate app data. Additionally, adults over 50 years of age were excluded.
Ethics statement
The study procedures were carried out in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Dankook University (2021-12-009). All participants provided written informed consent prior to enrolment in the study. Participants’ data were anonymized to ensure confidentiality.
Results
KODARI application
The KODARI application collects three types of information: user route information and related daily events, infectious disease-related information, and health-related information (Figure 1). The KODARI application has four units: input, update, big data, and transmission.
Input and update unit
The input and update unit features a self-tracing diary and infectious disease management functions (Figure 2). The units gather user status information based on the GPS-derived user location. Furthermore, users can update their daily information regarding changes in infectious disease status. Four units of the KODARI app.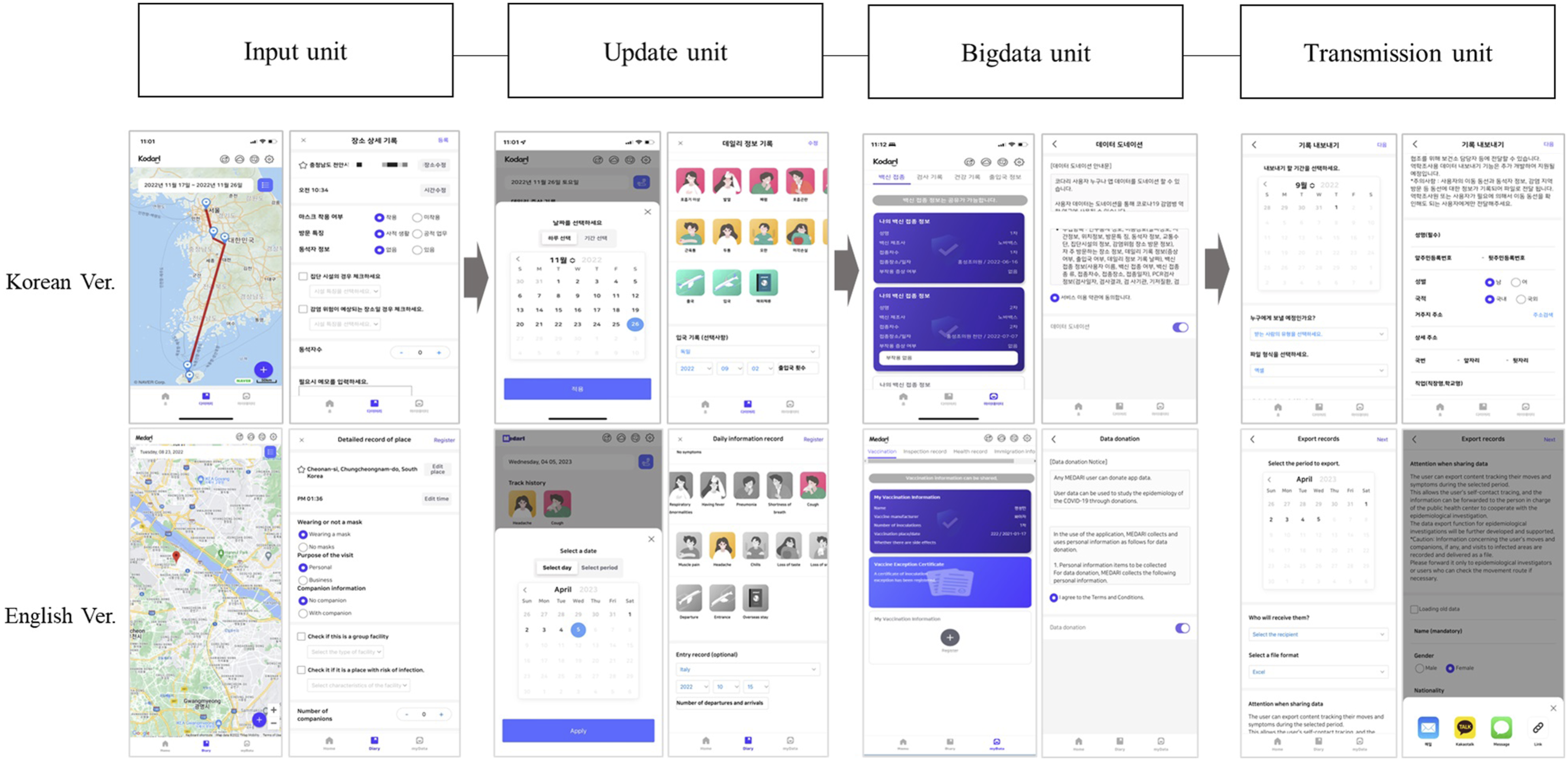
Initially, users may automatically or manually log their immigration records and movements they deem necessary to remember. Subsequently, users can manage their activity patterns, save companions, and note the characteristics of specific locations. On the detailed registration page for each place, it is possible to enter information such as mask-wearing requirements, visit characteristics, companion details, the presence of group facilities, facilities with infection risks, and the number of companions.
Moreover, users can store and manage personal health information and vaccination histories by registering vaccination details and exemption certificates. Personal health information includes underlying diseases, pregnancy status, cancer treatment history, immunosuppressed status, confirmed infectious disease status, and vaccine side effects. Additionally, users can manually document COVID-related inspections, such as medical institution test records, self-diagnosis test results, and antibody test findings.
Bigdata unit
Users can modify their records at any time and delete them freely at any time if they do not want to save them. Therefore, it is possible to reduce concerns about the accumulation of records for storing and managing records related to infectious diseases. In-application records were automatically deleted after four or more weeks. Through donations, users can contribute to constructing big data on infectious diseases.
The application has a function to approve donations from constructed epidemiological data, and donations have been developed to be withdrawn at any time. When a user cancels a data donation, the user's data is not visible and cannot be used even on the admin page.
Transmission unit
Users can send their activities' records in an Excel file by email or text message at any time. The recipient of the data was the user or epidemiological investigator. Users can export records up to 4 weeks before the date of transmission. The KODARI application was developed to store and transmit user information for up to 4 weeks. It can be sent by, for instance, email, KakaoTalk as a messenger service, and text messages. KakaoTalk refers to a global free mobile messaging service provided by Korea’s Kakao Co., Ltd. Users can also copy and send the links. This finding is useful for epidemiological investigation.
User’s evaluation of the KODARI application
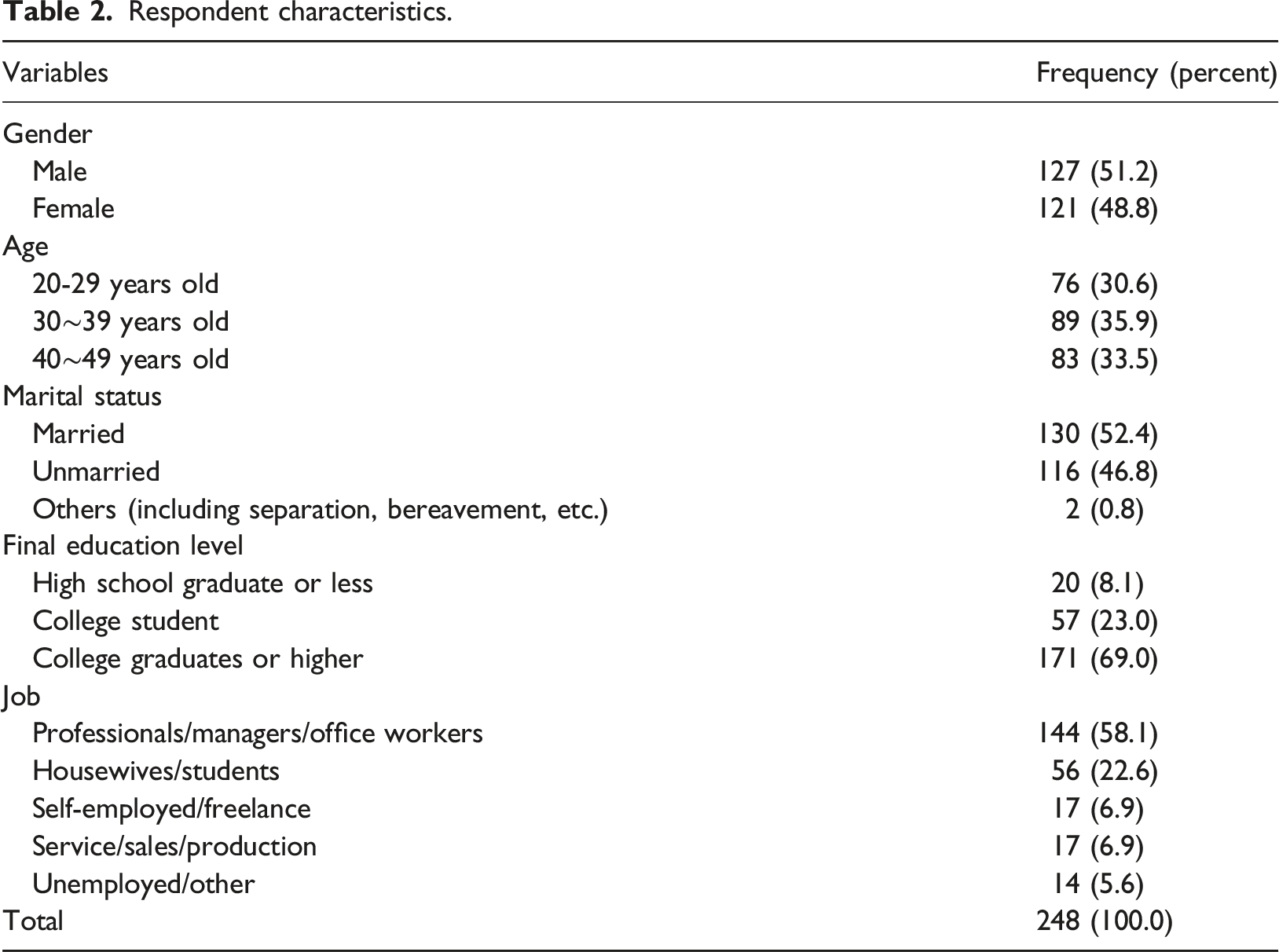
Respondent characteristics.
Willingness to use healthcare applications related to infectious diseases
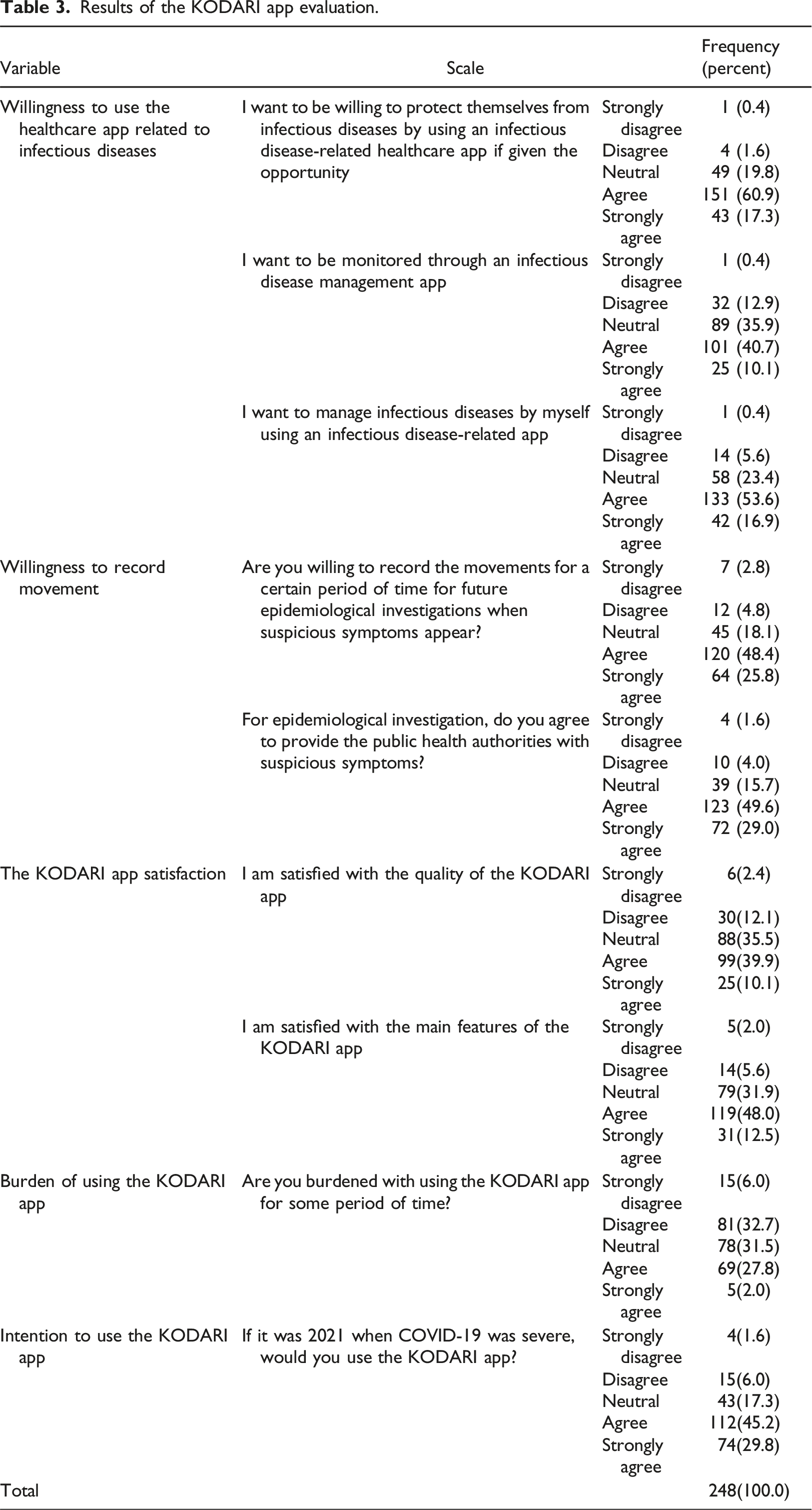
Results of the KODARI app evaluation.
Willingness to record movement
The results of the two questions about the willingness to record movement are as follows (Table 3). First, 184 out of 248 respondents (74.2%) responded positively to the question, “Are you willing to record your movements for a certain period of time for future epidemiological investigations when suspicious symptoms appear?” Second, 195 (83.9%) of the total 248 respondents responded positively to the question, “Do you agree to provide the public health authorities with suspicious symptoms for epidemiological investigation?”
KODARI application satisfaction
The results of the two questions concerning satisfaction with the KODARI application are presented in Table 3. In response to the question, “I am satisfied with the quality of the KODARI application,” 50% of participants indicated agreement or strong agreement. Concerning the main features’ satisfaction of the KODARI application, 60.5% of respondents indicated agreement or strong agreement.
Burden of using the KODARI and intention to use the KODARI application
When queried about feeling burdened by using the KODARI application over a certain period, 38.7% of participants reported feeling not at all or minimally burdened (Table 3). Moreover, 31.5% described their burden as normal, suggesting that the overall burden of use was manageable. We also inquired whether participants would be willing to use the KODARI application in 2021, during the peak of COVID-19. Of the total respondents, 186 (75%) provided positive feedback, agreeing or strongly agreeing.
Value of the KODARI application
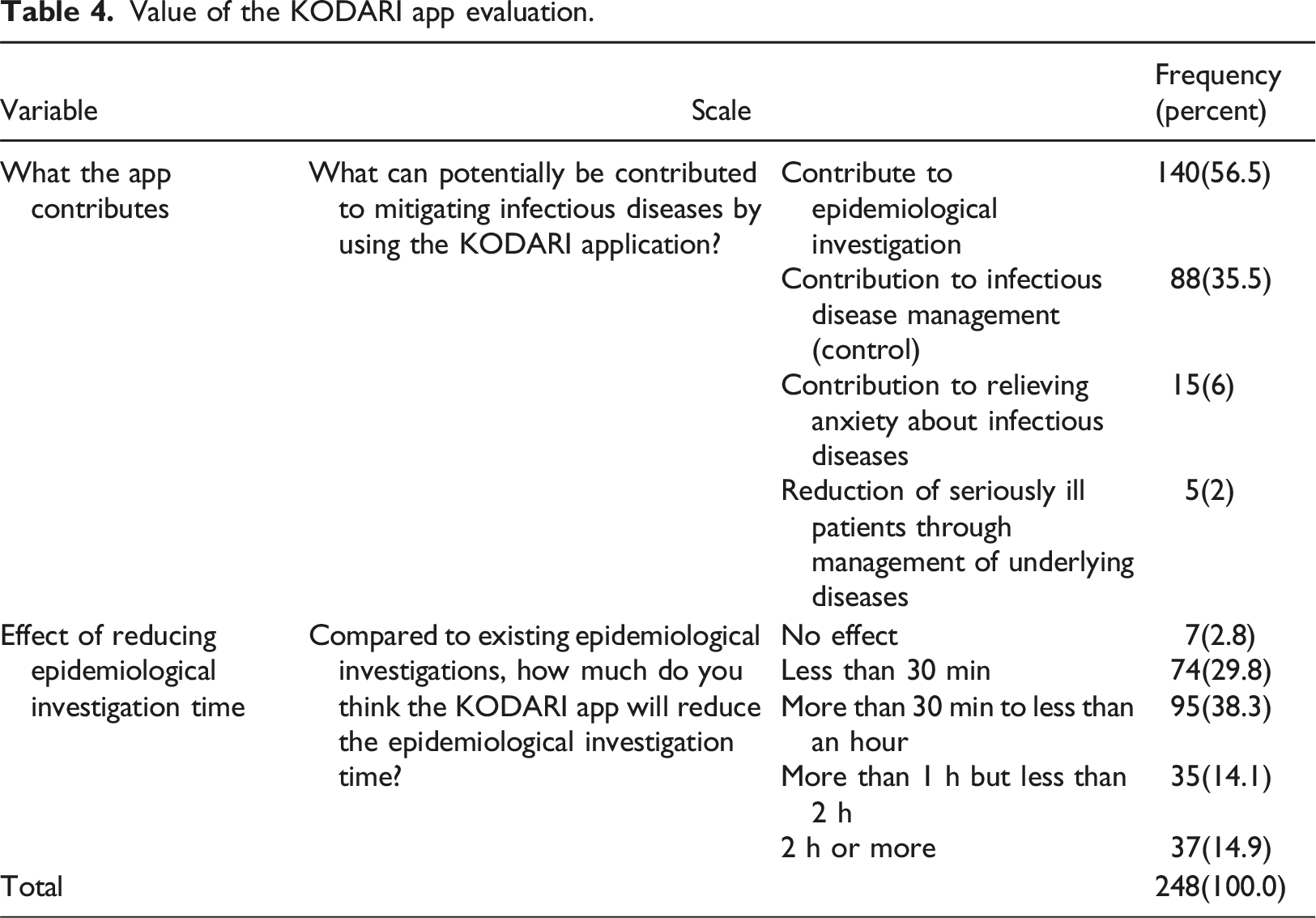
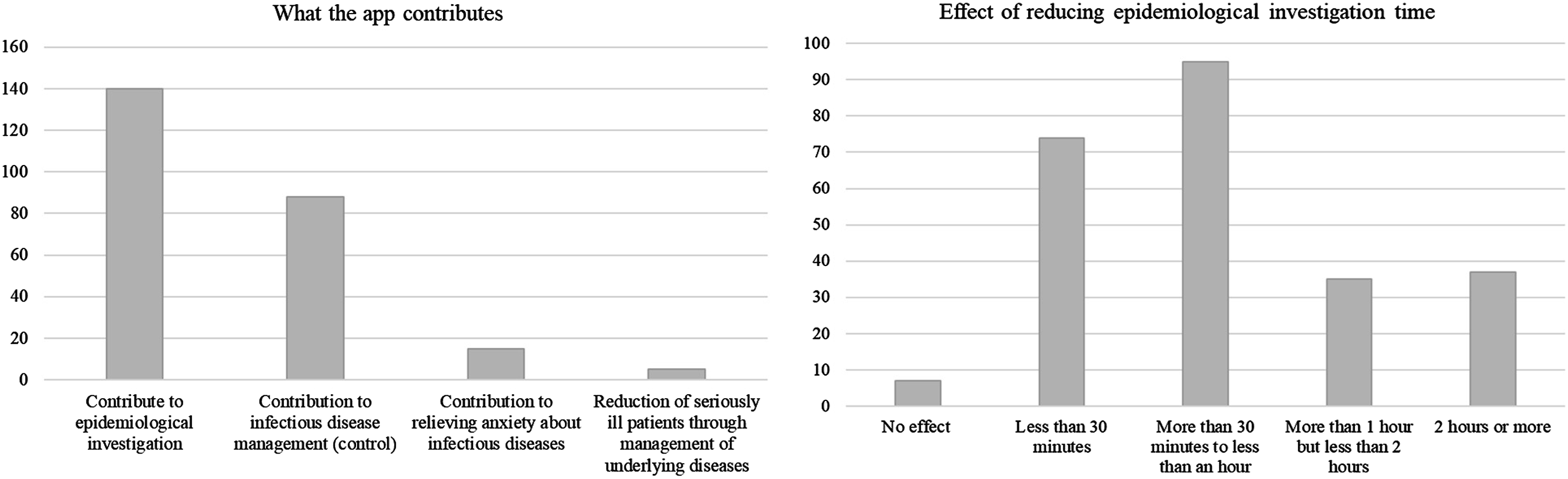
Value of the KODARI app evaluation.
Value of the KODARI app.
We inquired about the perceived reduction in time in epidemiological investigations when using the KODARI app compared to traditional methods (Table 4, Figure 3). A total of 38.3% of respondents believed that the investigation time could be reduced from 30 min to less than an hour. Additionally, 29.8% thought that using the app could decrease the time spent on an epidemiological investigation by less than 30 min. Only 2.8% felt there would be no reduction in investigation time.
Discussion
We developed an application to support the epidemiological investigations of governments in the endemic era: the KODARI application. The KODARI application has several advantages.
First, the KODARI application has the advantage of solving personal information issues and automatically collecting epidemiological investigation information. GPS-based route self-management is possible. As in Singapore, a confirmed case of COVID-19 must be interviewed by an epidemiologist. 1 Epidemiological investigation subjects should provide epidemiological investigators with information on demographic characteristics, clinical symptoms, and activities from 14 days before the onset of COVID-19 symptoms to isolation. Epidemiologists also perform contact tracing to identify close contacts and other contacts that interact with confirmed cases. During an epidemiological investigation, it is difficult to remember one’s movements and specific details. Thus, the KODARI application automatically collects movements based on GPS. However, it is also possible to collect movement only using the application. In addition, the user can store location and state information they want to remember. The stored information could be deleted at any time. Considering concerns about personal information exposure, it can be deleted at any time, and the deleted information cannot be recovered. The stored data were automatically deleted after 4 weeks. Even in the case of digital contact tracing, perceived security, privacy, and technology trust have been reported as major factors affecting user satisfaction. 25 Privacy concerns are predictors of resistance to digital contact tracing applications.16,26–29 Therefore, we made it possible for users to use the application to delete and edit their movement records as freely as possible so as not to worry about privacy and security.
Second, the KODARI application has advantages such as improved data accuracy through accurate information collection, improved contact tracing capabilities, and the ability to provide timely and targeted interventions. When an infectious disease is confirmed, it is possible to manage daily symptoms and write a symptom diary. It is also possible to manage the self-symptoms one wants to remember daily. This could provide clues to revive memories of the symptoms necessary for epidemiological investigations. The [My Data] menu in the KODARI application facilitates the self-management of infectious diseases by enabling users to record and store their vaccination and examination histories, as well as daily health records. This feature is particularly valuable when it is essential to document various infectious-disease-related information. Previous studies have demonstrated that self-reported symptom tracking is effective in predicting potential COVID-19 infections. 30 Self-reported symptoms, such as loss of sense of smell and taste, are included in the screening criteria. Moreover, following an infectious disease episode like COVID-19, individuals are keen to manage their condition promptly. This functionality proves beneficial during an endemic period.
In South Korea, the Epidemic Investigation Support System (EISS) is employed to track epidemics. This system features capabilities for mapping the movement data of confirmed cases and forecasting regions at risk of infection. 31 The EISS mitigates the spread of infectious diseases by monitoring confirmed cases, leveraging data from public transportation, mobile network base stations, healthcare facility visits, and international travel records. Nonetheless, it faces challenges in gathering and utilizing detailed individual symptom data and self-reported infectious disease information. Consequently, the KODARI application’s key benefit is enabling individuals to self-manage infectious diseases during endemic periods, exemplifying the characteristics of an ideal digital tracking application.2,32,33
Third, the data were used to build big epidemiological data through donations. It is possible to build big data based on the status of patients with infectious diseases. Infectious disease-related data collected by users are useful in epidemiological studies of infectious diseases. 34 In South Korea, many efforts are being made to induce users to donate data in COVID-19-related applications, such as SHINE (Study of Health Information for Next Epidemic). 35 Government-driven COVID-19-related big data exist, but user-driven data are also essential. This is because user-centric data include specific records and specifics of the time in which it was collected. Even in the COVID-19-related application evaluation framework, user control and self-determination are crucial from epidemiological and legal perspectives. 11
Fourth, it can transmit self-management information data to epidemiologist terminals or users in real time. Users can export records for up to 4 weeks prior to the transmission date. When an infected individual partakes in an epidemiological investigation, the investigator collects data on the individual’s movements and peculiarities during a specific period. However, it is challenging for individuals to recall all details pertinent to the estimated infection period. Users can now access and utilize the data stored in the KODARI application. An environment that facilitates independent management of infectious diseases and active participation in epidemiological investigations can be established. COVID-related applications serve various purposes, including monitoring the epidemic, tracing and tracking movements, and assessing exposure risks. 11 However, no service allows users to utilize recorded user information for epidemiological investigations. This can be said to be the most significant feature of the KODARI application.
Fifth, following experiences with COVID-19, analyses indicated that people are now more inclined to protect themselves from infectious diseases and utilize related applications. Moreover, there was a high level of self-management willingness regarding infectious diseases. Participants also consented to record their movements for epidemiological purposes. Furthermore, there were positive evaluations of the KODARI application, accompanied by a strong willingness to use it. The burden associated with using the KODARI application was also found to be relatively low. For COVID-19-related applications, such as contact tracing apps, to be effective, they must be adopted and utilized by the public. 36 However, prior studies have highlighted low adoption rates among the population.36–38 If a COVID-19-related application encourages voluntary participation, it is likely that users will actively engage with it, even if it involves collecting location data. Looking ahead, there is potential for expanding the KODARI application to manage other infectious diseases.
Sixth, this study demonstrated that the KODARI application can enhance epidemiological investigations and diminish the duration of existing epidemiological investigation processes. A majority of respondents (56.5%) assessed the KODARI application as beneficial for epidemiological investigations. This benefit distinguishes it from other existing contact tracing applications. Moreover, it was observed that using the KODARI application could reduce the epidemiological investigation time by more than 30 min compared to the conventional epidemiological investigation duration (97.2%). Merely 2.8% of participants indicated that there would be no reduction in investigation time.
Limitations and future research
Despite these advantages, this study had several limitations. First, we developed the KODARI application, which enables users to transmit epidemiologically relevant information to epidemiologists. Thus, it is necessary to develop a dedicated application for epidemiologists in the future. Second, a survey study on the effectiveness of the KODARI application is essential for epidemiological investigations. Therefore, focusing on individuals who have undergone such investigations is crucial. Third, we developed a Korean version of the KODARI application. It is imperative to create versions in various languages for national use. Fourth, we developed the application by extracting data items from an epidemiological investigation form for COVID-19 (Version 6, for public health centers) 17. As of December 2022, the 13th edition of the Response Guidelines was published. The epidemiological investigation form for COVID-19 evolves based on the COVID-19 response level, which cannot all be reflected. We aimed to include as many items as possible in the application, but some were not implemented. We plan to incorporate all items in future upgrades of the application. Fifth, the KODARI application anonymizes user data, ensuring there are no security issues. However, the implementation of security technologies, such as blockchain, is necessary. Sixth, we surveyed the KODARI application users and ultimately used data from 248 users for analysis. According to existing literature, when there are less than 12 variables, the number of samples is suggested to be 200. This study used 11 variables to assess the application. We determined that 248 data sets were appropriate for this study. Future studies need to calculate and justification of the sample size to choose for the study.
Conclusions
The KODARI application stands out as it introduces a service model predicated on voluntary participation. In the context of COVID-19-related applications, most were orchestrated by governments and centrally managed. Moreover, concerns about personal information exposure have made users hesitant to engage with these applications. Although COVID-19-related applications are acknowledged as providing theoretical evidence for new public health interventions, the global adoption of digital contact-tracing applications remains limited. Therefore, it is necessary to allow users to manage infectious disease-related information or track it on their own. Infectious diseases that threaten people’s lives worldwide are expected to continue to appear in the future. Therefore, the world requires a non-centralized and autonomous service that can protect itself when an infectious disease is confirmed, such as the KODARI application. Ultimately, collecting and utilizing epidemiological survey data through voluntary participation have the potential to improve the efficiency and effectiveness of disease surveillance and control efforts.
Finally, the KODARI application is valuable as a technology that supports epidemiological investigations based on collected big data. The KODARI application would be useful in cooperation with epidemiological investigations of infectious diseases in future pandemics.
Supplemental Material
Supplemental Material - Epidemiological investigation support application and user evaluation based on infectious disease self-management model in the endemic era
Supplemental Material for Epidemiological investigation support application and user evaluation based on infectious disease self-management model in the endemic era by Jihwan Park and Mi Jung Rho in Health Informatics Journal.
Footnotes
Author contributions
Conceptualization: Jihwan Park and Mi Jung Rho. Data curation: Mi Jung Rho. Formal analysis: Mi Jung Rho. Funding acquisition: Mi Jung Rho. Methodology: Jihwan Park and Mi Jung Rho. Project administration: Mi Jung Rho. Writing – original draft: Jihwan Park and Mi Jung Rho. Review & editing: Jihwan Park and Mi Jung Rho. App planning& app development: Jihwan Park and Mi Jung Rho.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The corresponding author and the first author are a married couple. They participated in this project at the time of the study. There are no competing financial interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2020R1I1A1A01072400). In addition, this research also was supported by Australia-Korea Joint Call for Joint Research Projects through the NRF (NRF-2021K1A3A1A17102523).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.