
Abstract
Introduction
HosmartAI project is developing a common, open-source integration platform to streamline the incorporation and evaluation of digital technologies (including robotics and AI) within the healthcare system. This platform will be piloted across eight large-scale initiatives focused on enhancing medical diagnosis, surgical interventions, disease prevention, and treatment, as well as rehabilitation and long-term care support within diverse hospital and care settings. Notably, Pilot 5 specifically targets advancements in cardiovascular disease and thoracic disorder management in Slovenia.
In this study, we describe the co-creation steps towards to Pilot 5 study which were achieved before the actual testing in real world environment. Pilot 5 (Assistive Care in Hospital: Robotic Nurse) focuses on cardiovascular diseases and Thoracic Disorders and was carried out by the UKCM Hospital, Slovenia. Its goal is to evaluate a social assistive humanoid robotic system (SAHR) that supports nursing care and improves the quality of care. SAHR assumed communicative functions such as assistance (providing medical information, reminding patients to take medication, drinking behavior, etc.) and monitoring the patient’s objective (measuring blood pressure, temperature, hydration) and subjective state of health (emotions, pain, PROMs). The robot interconnects with the clinical data repository to support clinicians during a grand round.
In Pilot 5, the emphasis is on values-sensitive design and co-creation, highlighting the significance of incorporating ethical considerations and stakeholder input into the development process.1,2 This approach underscores the importance of ensuring that the design and implementation of solutions align with ethical principles, societal values, and user preferences. By engaging in co-creation with stakeholders, including end-users, researchers, and experts, Pilot 5 aims to foster a collaborative environment where diverse perspectives are considered, leading to more inclusive and user-centered solutions.
Values-sensitive design (VSD) is a crucial approach for developing socially assistive robots in hospitals. VSD emphasizes integrating human values throughout the design process. This ensures robots align with societal values and minimize harm while promoting positive outcomes. 3 In healthcare settings, VSD can address ethical challenges and prioritize patient care. 4 By incorporating VSD principles, developers can create robots that respect patient privacy, promote well-being, and ultimately improve the quality of care provided by hospital staff. 5
Pilot 5 heavily relied on Participatory Design (PD), a crucial approach for effective technology development. PD involves active stakeholder engagement, transforming them from passive recipients to co-designers. 6 This approach is linked to increased trust, user acceptance, and overall effectiveness of socially assistive robots. 7 By actively involving users, stakeholders, and caregivers, PD allows for addressing concerns, incorporating feedback, and tailoring the robot design to specific needs and preferences. The literature highlights various factors influencing user acceptance, including robot characteristics, 8 interaction dynamics, 9 user perceptions based on observed interactions, 10 self-efficacy, 11 and visual design. 12
The core position of co-creation (integrating co-design and co-production) as a strategy for social and health innovation is unquestionable.13,14 Public engagement in shaping research and innovation fosters a sense of ownership and empowerment, ensuring projects are truly “with” and “by” the people, not simply delivered on their behalf. Still, it is highly challenging and due to different limitations, barely implemented in the research, development, and innovation cycles. 15 Therefore, systematizing the introduction of a user-centered design culture is a challenge that requires a continuous and evolving effort to ensure that value is created ensuring users’ long-term engagement which was followed through in this study. In the healthcare field, the concept of the method of co-creation is based first on acknowledging a silo culture and then on the difficulties to work across silos. 16 From that point, co-creation has a built-in provision to sort immanent conflicts of interests and opinions upfront. It does so by having the participants in the process learn each other’s perspectives during the development of innovation.
Living Labs methodology is a user-centered approach to innovation that takes place in real-world settings. 17 It emphasizes co-creation, where stakeholders from various backgrounds work together throughout the entire innovation process. By bringing together stakeholders and testing ideas in a real-world setting, our living lab approach helped to increase the success rate of HosmartAI project pilots.
The levels of acceptance among stakeholders regarding the implementation of socially assistive humanoid robots (SAHRs) in nursing and care routines and, additionally, the factors that influence higher or lower acceptance within these groups, focusing on demographic variables, technology expectations, ethical considerations, and negative perceptions were recently examined by. 18 That study revealed that most patients and healthcare providers view SAHRs positively. Specifically, many participants were willing to be treated or work in a hospital where an SAHR collaborates with humans. The structural models of overall acceptance highlighted specific personal traits that lead to greater acceptance of SAHRs. In particular, patient acceptance was significantly influenced by realistic expectations of SAHR functionality, rather than unrealistic depictions portrayed in the entertainment industry.
This study employed a co-creation approach in Pilot 5, divided into two distinct phases: Sprint 1 and Sprint 2. During Sprint 1, ethical approval for patient interaction was pending. Consequently, data collection relied on a cross-sectional online survey (completed by 282 healthcare employees and 346 patients) and a face-to-face workshop (involving 24 participants from diverse stakeholder groups: researchers, nurses, and project coordinators). These activities aimed to gather initial insights and inform subsequent phases. In Sprint 2, the focus shifted towards co-creation through a series of face-to-face workshops (four in total, with 51 participants from diverse stakeholder groups). These workshops addressed key aspects of the robot’s development, including finalizing its real-world architecture and placement, defining the conceptual design for human-robot interaction, designing the care plan, identifying and scheduling digital interventions, and developing and deploying the first iteration of vision models on the robot. As a last step, a cross-sectional study was designed with 110 patients to evaluate the SAHR’s readiness for the clinical trials.
In the following sections, the co-creation activities of Pilot 5 which were completed before starting the actual studies within the project are explained within the living lab methodology. In the next sections, stakeholders’ engagement, participatory design, and deployment scenarios are explained according to the results of co-creation sessions with stakeholders.
Methodology
This section details the methodological approach employed in Pilot 5. This study has a mixed-method approach. Surveys, workshops, and interviews were used as data collection methods. Collected data was analyzed by basic statistical methods. We will delve into the implementation of the Living Lab approach, specifically focusing on the design of extended sprints tailored for Pilot 5. Additionally, we will explore the strategies undertaken for stakeholder community engagement. Furthermore, we will discuss the Pilot’s adherence and elaborate on the deployment scenarios envisioned for the Pilot’s outcomes.
Agile schema
The agile methodology was applied during the whole task and several sprints were conducted to optimize the technologies within this study. Following the guidelines provided by the hybrid methodology, an adaptation of the CAPTAIN 2020 project methodology was carried out to adjust the sprint approach into our study’s framework.19,20
Inclusion/exclusion criteria
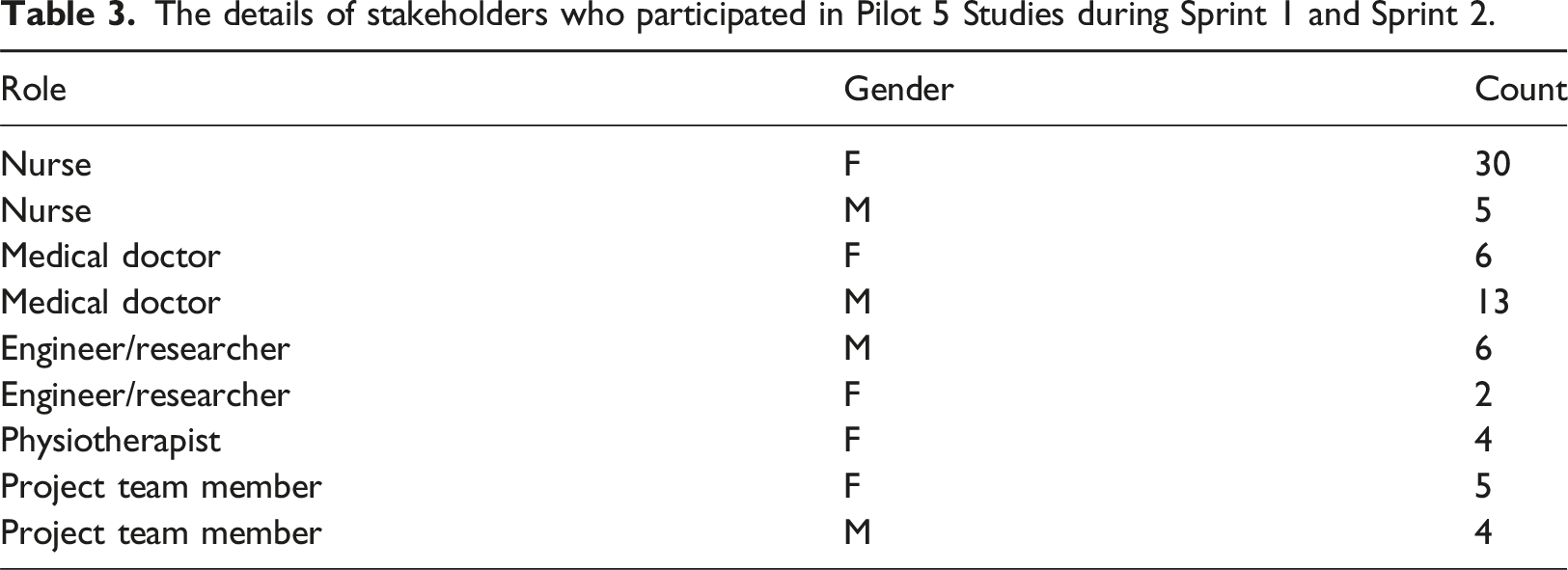
This study recruited participants from various stakeholder groups (Table 3). The clinician and nurse sample included clinicians who regularly participate in grand rounds within the vascular surgery or thoracic surgery ward. Engineers/researchers and project team members were selected from those actively involved in the project.
Implementation of living lab approach: Design of sprints for pilot 5
Planned HosmartAI sprints.
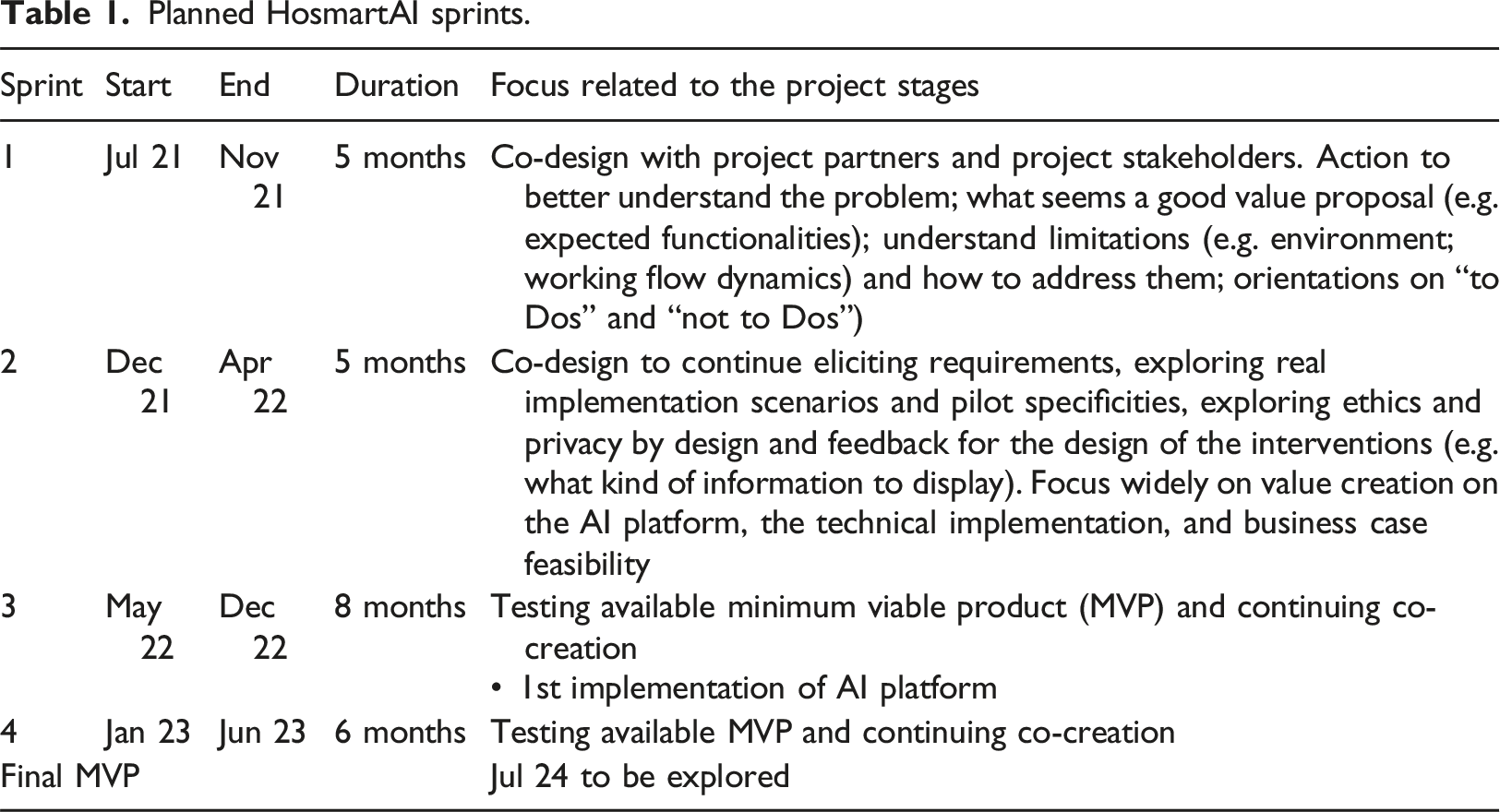
In Sprint 1, common co-creation activities were discussed in groups with the participants regarding the concept to be explored. Conclusions were extracted from this discussion as to where and when possible, the robotic nurse would be utilized in co-creation. Interaction with patients could be facilitated only after ethics approval has been obtained. Thus 1st co-creation is being carried out as a cross-sectional survey and can also include health professionals participating in a workshop.
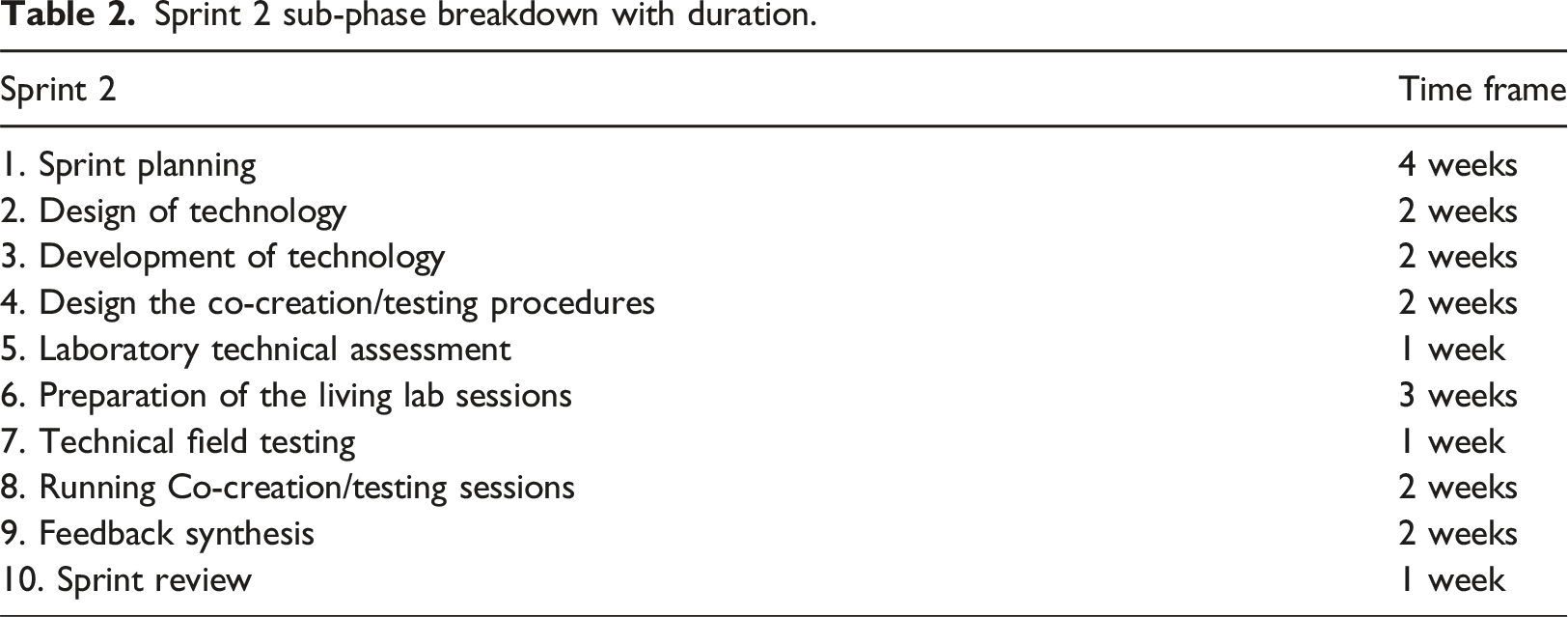
Sprint 2 sub-phase breakdown with duration.
Stakeholders’ community engagement: Strategy
The initial custom-made feedback questions and focus group studies were used as a strategy to establish the local stakeholders’ groups.
Those questions consisted of a phase where the objective was to have a first understanding and gather a general idea of stakeholders’ preferences for technical, pilot, and business partners, their backgrounds on the methodology adopted by HosmartAI project, the barriers foreseen, the mitigation strategies, etc.
The details of stakeholders who participated in Pilot 5 Studies during Sprint 1 and Sprint 2.
Participatory design: Sprints of pilot 5
As stated in the methodology, this co-creation study involves only the first two sprints. The details of the workshops during those sprints are given in the following text.
Sprint 1
Details of the workshop of Sprint 1.

Sprint 2
During workshop 1, researchers (healthcare professionals) from the Department of Thoracic Surgery expressed interest in the presented scenarios. One area for future exploration is the potential impact of surgical robots on workload, as identified by the participants. The workshop resulted in the following key outcomes: Established goals for upcoming workshops and developed a clear action plan for the forthcoming period.
Sprint 2’s initial workshops addressed two crucial aspects: exploring integration possibilities and identifying implementation challenges. Researchers presented five potential scenarios for robot-assisted workflows in thoracic surgery, fostering discussion and exploration.
In workshop 3, the project aimed to achieve three main objectives: introducing the robot “Frida” to participants, evaluating its core functionalities, and collaboratively defining its role within the clinical setting. Participants first encountered Frida at the University of Maribor facilities. To determine the appropriate complexity for the robot’s future training content, researchers assessed its basic functions such as speech recognition, gestural communication, movement capabilities, and object manipulation.
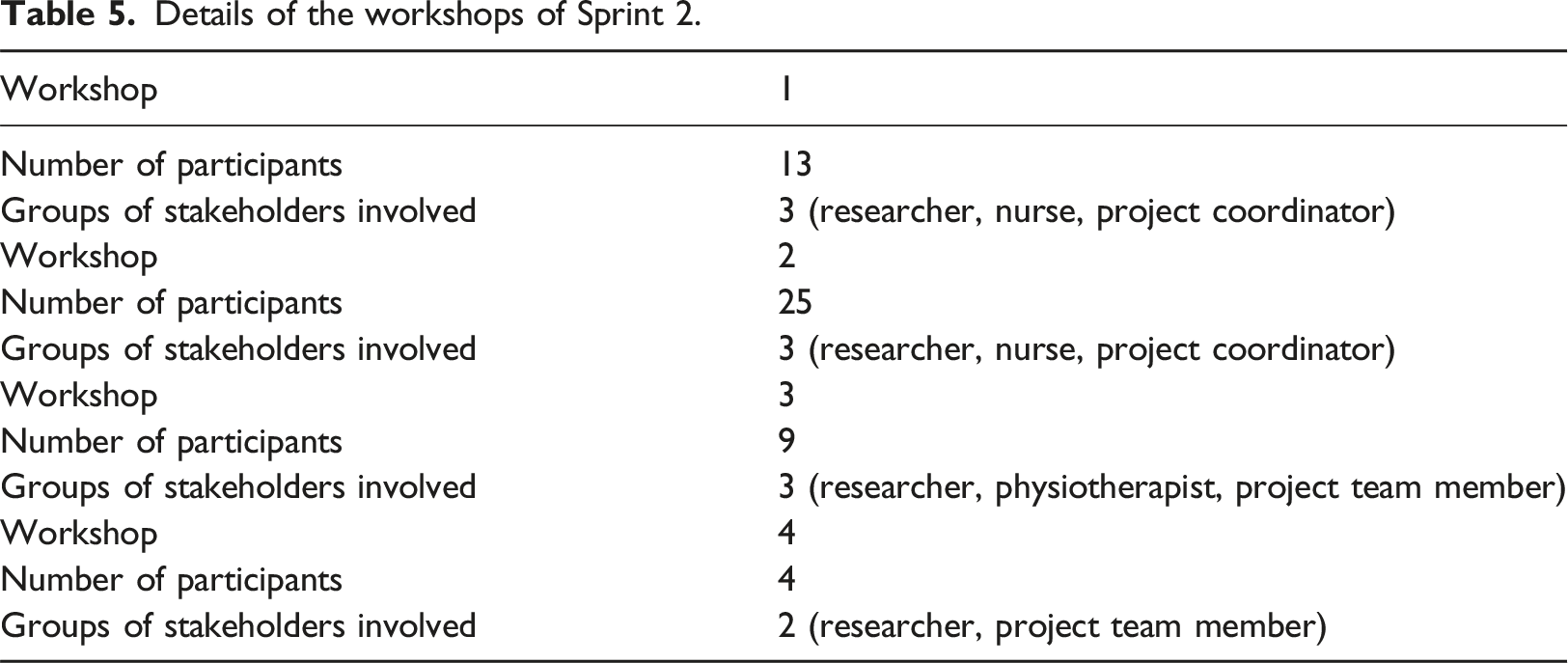
Details of the workshops of Sprint 2.
Deployment scenarios
In Sprint 1 and Sprint 2, the Pilot 5 study defined the following deployment scenarios (test cases) to be delivered. Wizard of Oz (WoZ) experiments are a valuable tool for researchers to gain early insights into user needs and preferences for new technologies. They help bridge the gap between theoretical concepts and real-world user experiences. Thus, for the experiments with the robot, we designed from scratch and applied WoZ experiments within the project after the face-to-face workshop with stakeholders.
Scenario 1: Robot in data collection mode
Within this test case, the socially assistive robotic unit acted as a tool to collect patient data and store the data in the FHIR (Fast Healthcare Interoperability Resources) based patient record. The robotic unit navigates to the patient’s room, scans the QR code to identify the patient, reports its location and activity to the blockchain, and executes the activity (or multiple activities in a sequence). The activities were scheduled using FHIR CareWorkflow (version 3). The following UML outlines the test case.
Figure 1 depicts the SAHR undergoing a data collection test. The right side of the figure illustrates data flow from the human user. It shows a patient interacting with the system, possibly through a physical interface labeled «Human». The left side of the figure depicts how the system responds to the user. The Multimodal Sensing module gathers health data like temperature or blood pressure. The Converse module enables communication between the user and the robot, through a Frida interface. SAHR in data collection mode test case.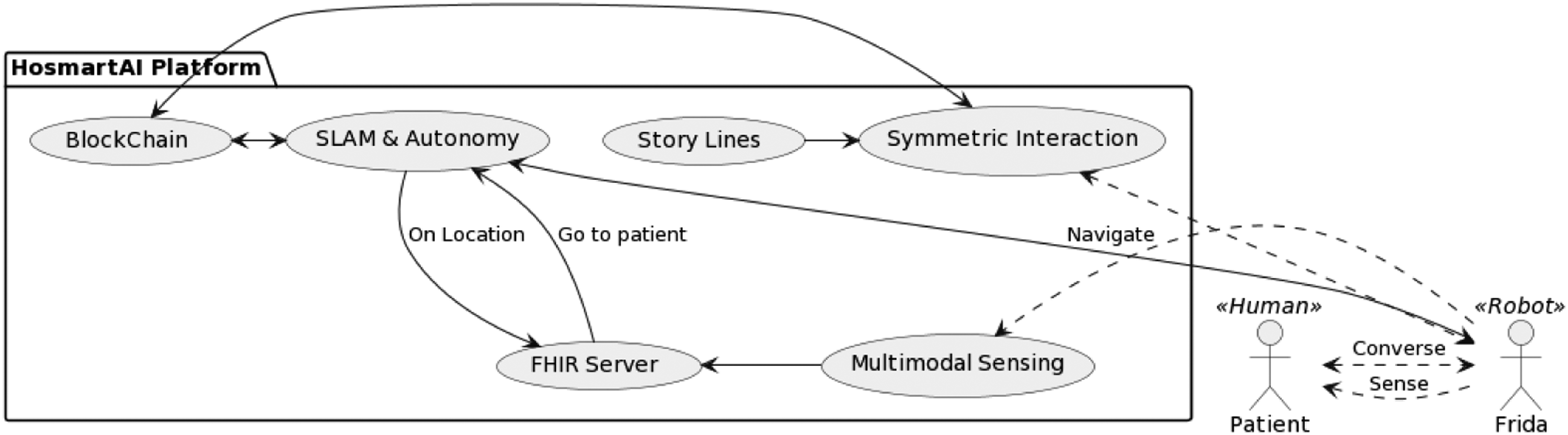
Scenario 2: Robot in the group activity
Within this test case, the socially assistive robotic unit acted as a tool to motivate patients to carry out physical activities and assess the correctness of exercise execution. In this test, case the physiotherapist explained the exercises to the patient and trained them in the first session (with the presence of the robot). Using the FHIR CareWorkflow (version 3) resource, the exercises were scheduled and the robot navigated to the room and tried to engage with patients to carry out the activities. The robot helped patients with breathing exercises in a WoZ experiment. The following UML outlines the test case.
As seen in Figure 2, the initial deployment (v1.0) of scenario 2 aimed to assess the robot’s effectiveness as a physical therapy coach, specifically for breathing exercises. SLAM ensured navigation and blockchain securely stored robot location and activity data. While a multi-modal sensing component observed patients’ exercise execution, a one-way communication module only demonstrated and guided exercises without unrelated conversation unless an emergency arose. SAHR in group activity test case.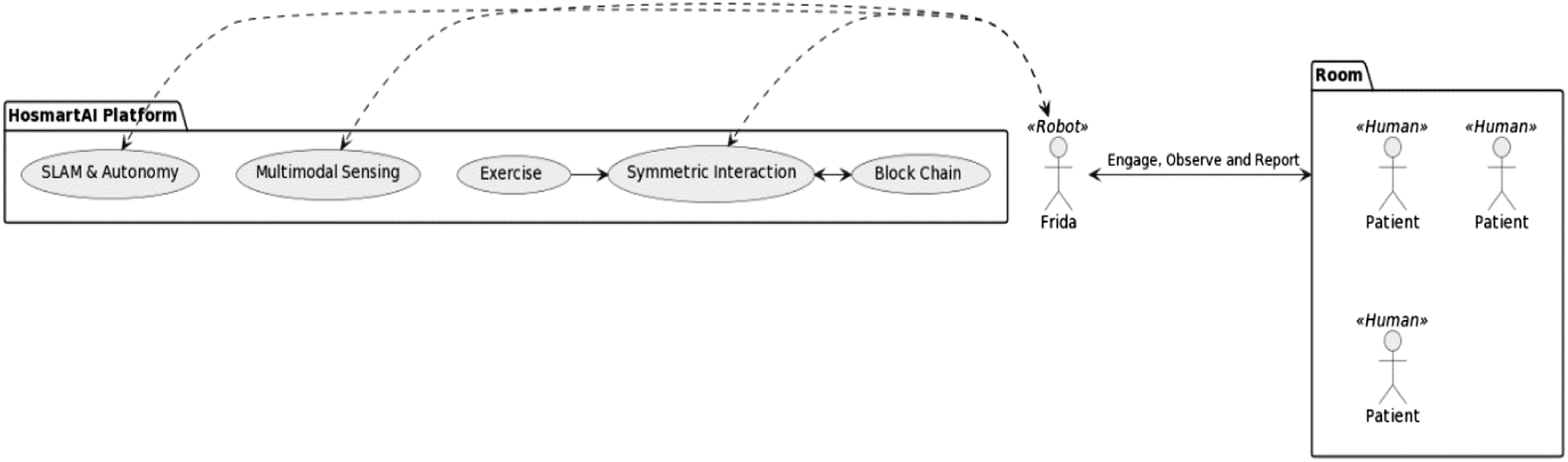
Scenario 3: Robots during grand round routine
Within this test case, the socially assistive robotic unit acted as a tool to enable the clinicians’ intelligible and real-time access to patient sources, such as diagnostic reports, laboratory results, radiology images, etc. The robotic units follow the clinician, scan the QR codes, and load patient resources. Speech recognition and natural language understanding was used to formulate queries and a tablet was used to display the data. In the first deployment, a series of WoZ Experiments were planned, where the operator navigated the robot to simulate follow functionality and also re-interpreted queries in natural language to compensate for possible recognition failures due to the real-life environment. The following UML outlines the test case:
Test Case 3 builds upon the foundation of test Case 1 by significantly enhancing the FHIR interface (Figure 3). This upgraded interface boasts two key features: a clinician’s interface specifically designed for data visualization, and a RESTful interface that seamlessly connects with the hospital’s existing digital system and database. SAHR in grand round routine.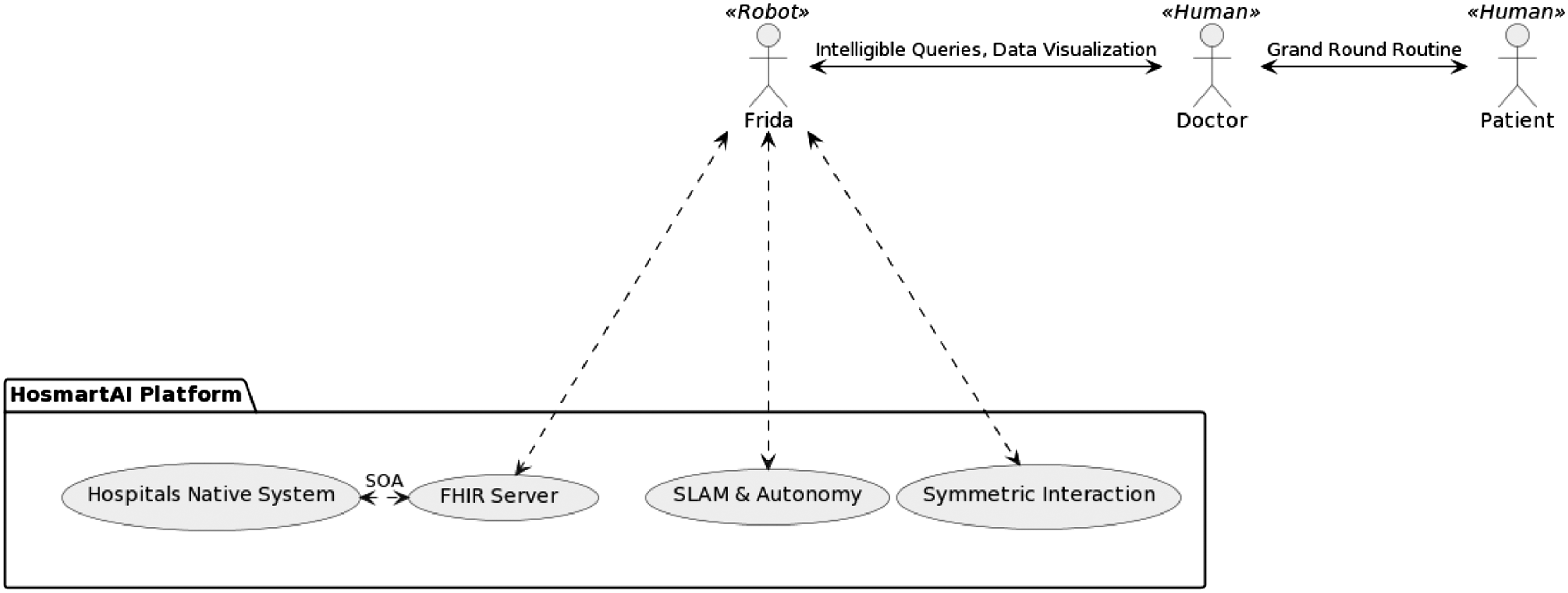
Satisfaction survey
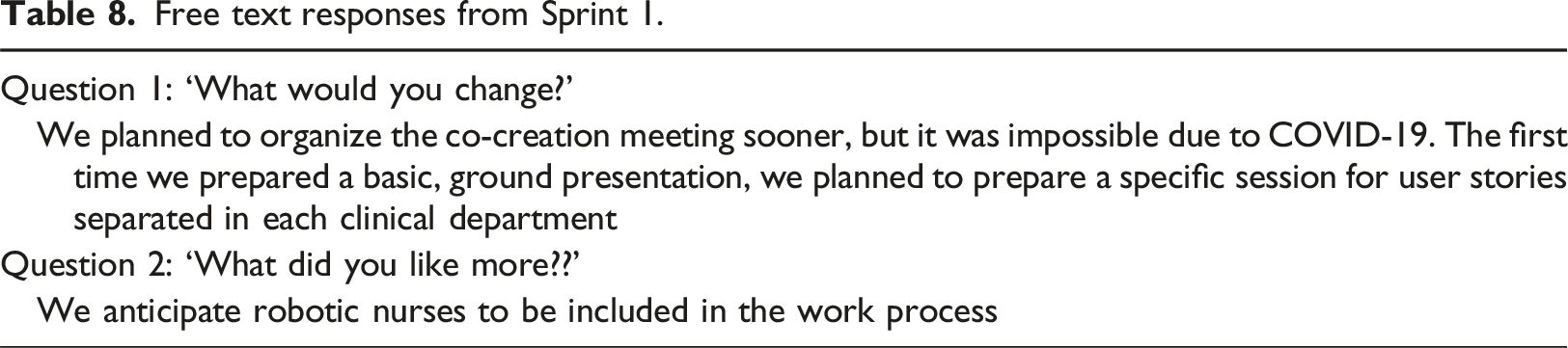
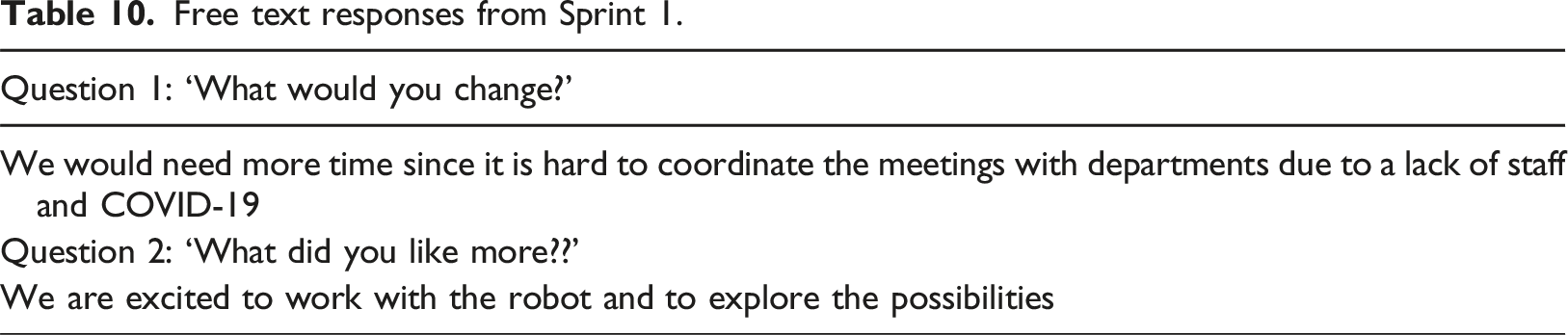
A satisfaction custom-made questionnaire was prepared and filled by the facilitators’ team. The aim is to understand possible problems in the procedure, the communication, and the assigned work and improve it in the next sprint. It includes 3 questions with Likert 5 responses (Tables 7 and 9) and two questions with free-text responses (Tables 8 and 10). Custom-made questionnaires are often used to study the job satisfaction of hospital staff. 21 In general, custom-made inventories to examine the job satisfaction of nurses seem to be constructed with practical purposes in mind 22 instead of focussing on the theoretical and methodological adequacy of the instruments.
Results
This section presents the findings of Pilot 5 during Sprint 1 and Sprint 2. We will begin by detailing the process of establishing stakeholder groups, a crucial step in the Living Lab approach. Subsequently, we will delve into the participatory design process employed during Pilot 5’s extended sprints. This will be followed by an overview of the specific actions carried out within the Pilot’s co-creation phases. Finally, we will present a retrospective analysis of the Pilot’s sprints, alongside a cross-sectional study conducted with participating patients. This combined approach will provide a comprehensive understanding of the Pilot’s outcomes.
Building the stakeholders’ groups
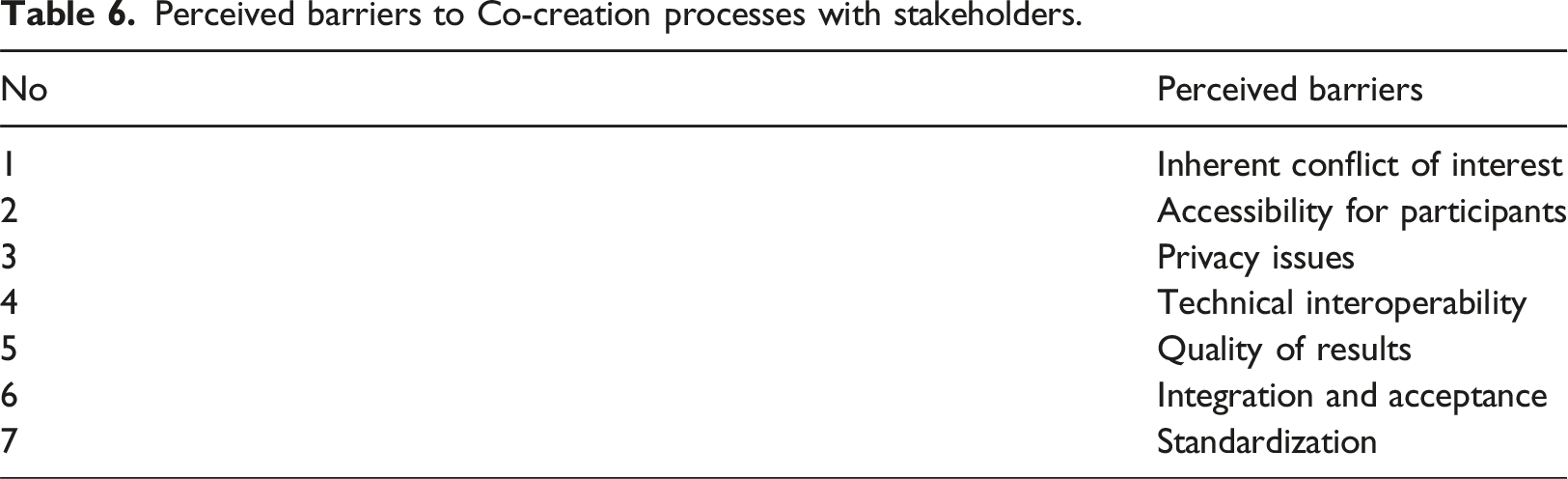
Perceived barriers to Co-creation processes with stakeholders.
Outputs and satisfaction results of participatory design
In sprint 1, the study mainly relied on technical partners for detailing and discussing technical components and conducted co-creation sessions with healthcare professionals and patients. The team defined six personas from the results of a cross-sectional survey, optimizing them based on new information, and prioritizing unmet needs.
In sprint 2, work was carried out to finalize the architecture and placement of the robot in the real environment, conceptualize robot interaction, and design care plans, and storylines/exercises. Moreover, the team worked on identifying the blockchain deployment scenario, validating the user interface, creating the first version of the vision models, and deploying them on the robot.
Sprint 1
During the discussion, medical doctors shared their perspectives on how the robot could be integrated into surgical patient care. Nurses identified potential tasks the robot could handle. All participants collaboratively discussed potential challenges and limitations the robot might face in a hospital setting. Based on these discussions, we developed a preliminary plan for the initial interaction between staff and the robot within the hospital environment. Overall, the participants were engaged and enthusiastic about the next steps in piloting the robot technology.
Team’s satisfaction after sprint 1 (likert 5).

Free text responses from Sprint 1.
Sprint 2
Open dialogue with nurses and doctors revealed interest in these scenarios, alongside concerns about potential workload increases. This emphasizes the need for proactive mitigation strategies to ensure a seamless integration process. In workshop 3, Open discussions were then held with nurses and medical doctors to identify potential challenges associated with Frida’s integration and collaboratively determine suitable tasks for it to perform. Finally, all participants were encouraged to interact with Frida, fostering a sense of familiarity and gauging its potential appeal to patients. This positive reception towards robot interaction served as a promising indicator for future exploration. Discussions in workshop 4 highlighted the need for improved video quality (technical support) and future protocol refinement.
Team’s satisfaction after sprint 2 (likert 5).

Free text responses from Sprint 1.
Retrospective analysis of Sprint1 and Sprint 2
The Retrospective Analysis marks the culmination of each Sprint loop, offering invaluable insights into the team’s dynamics and developmental progress. A thorough analysis of feedback from all partners reveals a positive trend of improvement across all sprints. As the project progressed, the team honed their collaborative skills and problem-solving capabilities, thus demonstrating growing adeptness within their roles.
One of the keys to success is balancing the technical and clinical aspects of the project, making sure that all stakeholders are involved, and considering the varied schedules and commitments of the partners. The continuous improvements seen during Sprint 1 and Sprint 2 demonstrate the team’s commitment to learning and adapting, pointing to a successful project overall.
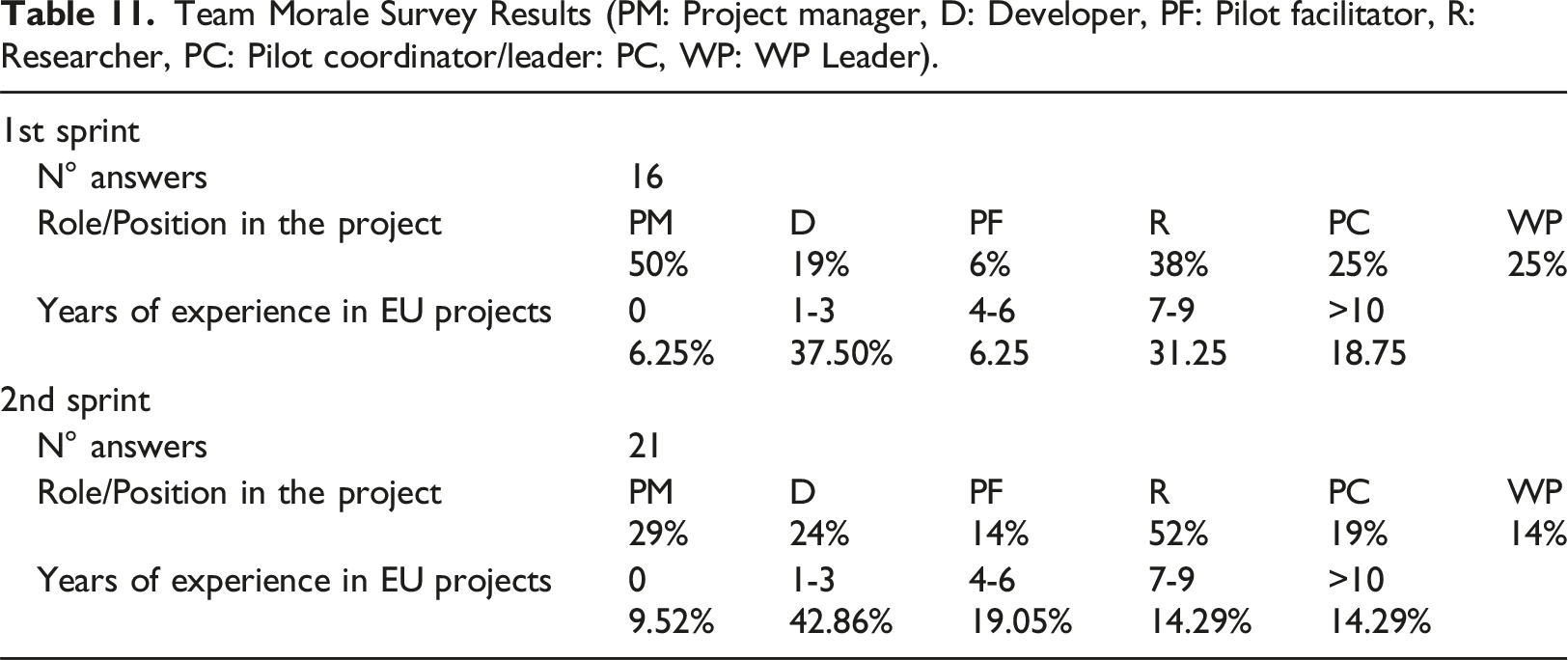
Team Morale Survey Results (PM: Project manager, D: Developer, PF: Pilot facilitator, R: Researcher, PC: Pilot coordinator/leader: PC, WP: WP Leader).
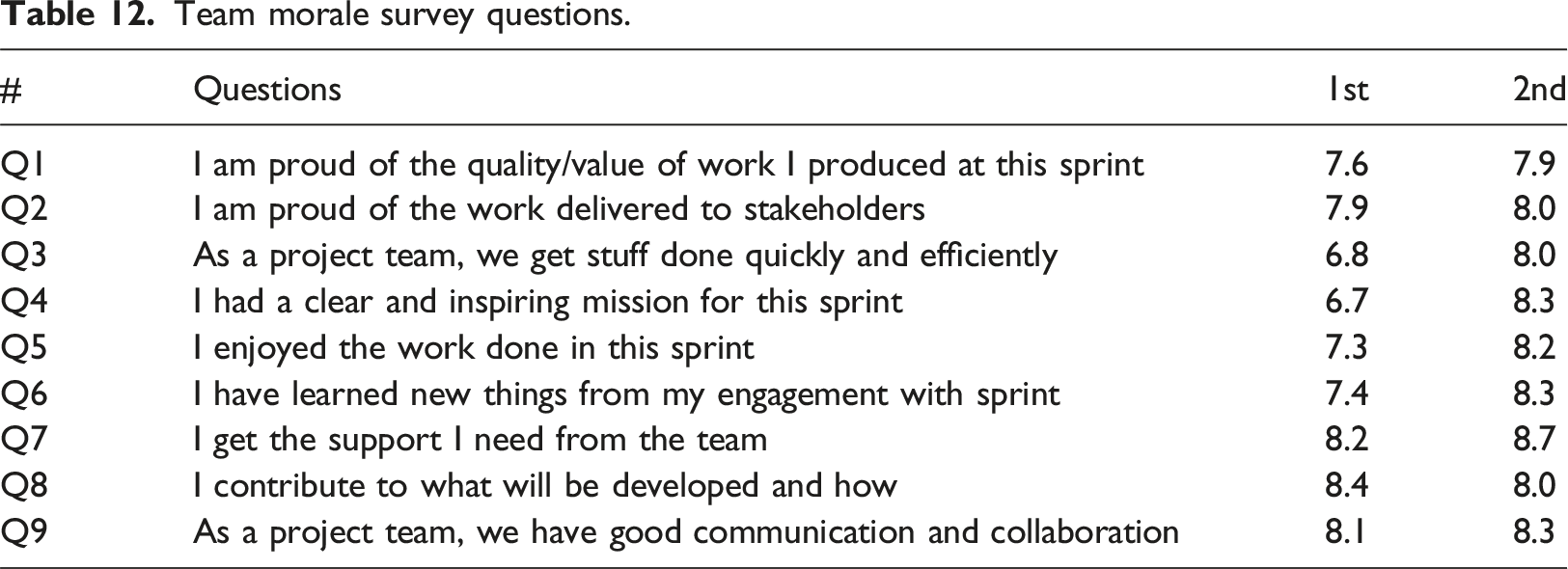
Team morale survey questions.
Comparison of results from the team morale web survey
The study team morale web survey has demonstrated an overall positive trend across the sprints. There was a gradual increase in pride regarding the quality of work produced (Q1) and delivered to stakeholders (Q2). The team’s efficiency (Q3) and clarity of mission (Q4) significantly improved from the first to the second sprint. Satisfaction from work (Q5) and learning opportunities (Q6) consistently increased over time. Team support (Q7) maintained high scores throughout, reflecting a strong sense of camaraderie. Contribution to development (Q8) remained relatively high. Finally, team communication and collaboration (Q9) showed a steady improvement over time, indicative of a healthy team dynamic. In summary, the data points to a progressive enhancement in team morale and unity over the sprints, with pride in work, enjoyment, and mutual support emerging as key strengths.
Discussion
This study employed a Living Lab methodology with iterative sprints (5-8 months) to facilitate continuous improvement through co-creation with all stakeholders. Retrospectives conducted after each sprint proved instrumental in this process. By analyzing user feedback, the project team was able to dynamically adapt and refine strategies throughout the project lifecycle.
Key takeaways from this co-creation experience highlight the importance of comprehensive stakeholder involvement, encompassing clinicians, technical teams, and end-users. This inclusive approach fostered nuanced discussions and ensured that developed solutions catered to everyone’s needs. Stakeholder perceptions significantly influenced project success; a positive outlook towards challenges and potential solutions from all parties expedited the development process.
The agile development model required flexibility to accommodate the varying schedules of clinicians and project teams, ensuring optimal participation. Proper timing for stakeholder engagement increased their participation and commitment, while also facilitating the smooth execution of tasks and sprints. Clear, concise, and regular communication across all stakeholders emerged as essential for project success. This included clarifying expectations, sharing progress updates, and fostering open discussions about potential challenges.
Close collaboration between technical and non-technical partners fostered a unified problem-solving approach and ensured the effective execution of tasks. Active participation from end-users throughout all project phases proved vital for its success. A well-organized approach to sprints and tasks, coupled with readily available resources, streamlined project operations.
Finally, the findings revealed positive user acceptance of SAHRs during patient admission. This suggests SAHRs have the potential to alleviate nurses’ workload and enhance patient satisfaction within this specific healthcare context.
Limitations
The study encountered several limitations. Firstly, participation was contingent upon a favorable attitude towards technology and robotics. This inherently limited the age range of participants, typically skewing younger. Additionally, co-creation can be a time-consuming process for both patients and healthcare staff, especially in busy clinical settings. This can restrict the number of participants willing or able to dedicate the required time. Finally, demonstrating the concrete benefits of co-creation initiatives proved challenging. While we measured factors like satisfaction and team morale, different aspects of co-creation likely require different evaluation metrics. In this study, we used custom-made questionnaires to get the initial feedback from employees and measure their satisfaction according to the requirements of the project. However, this approach raises concerns about whether it accurately measures the intended constructs. Those custom questionnaires were specifically designed for this project study within the hospital. This limits the generalizability of the findings to other settings or patient populations.
Future work
This study served as the culmination of a value-sensitive design process of Pilot 5, evaluating the readiness of a proposed socially assistive humanoid robot (SAHR) for inclusion in clinical trials assessing the effects of interactive digital patient assistance (HosmartAI Pilot 5 Trials). As a next step in the project, in Sprint 3 and Sprint 4, a single-session case study involving 110 patients (average age: 59.66 years, 56.4% male) explored patient perceptions of the SAHR. Following informed consent, participants engaged in a face-to-face interaction with the robot, including a question-and-answer session mimicking a patient admission process. Post-interaction, participants provided feedback using the e-acceptability scale and a behavioral intention questionnaire. Results indicated generally positive attitudes towards the SAHR in a patient admission scenario, suggesting high user acceptance. Patients reported favorable evaluations of the robot’s social capabilities, ease of use, and overall experience. Detailed findings will be presented in a forthcoming publication as a future work.
Conclusion
Pilot 5 of the [details omitted] project successfully demonstrated the value of a co-creation approach in developing a Socially Assistive Humanoid Robot (SAHR) for supporting nursing care within a hospital setting. This study employed a Living Lab methodology with iterative sprints, fostering continuous improvement through active participation from all stakeholders, including clinicians, technical teams, and patients.
The co-creation process, divided into two distinct phases (Sprints 1 and 2), leveraged various methods for data collection and stakeholder engagement. Initial insights were gathered through online surveys and face-to-face workshops, informing subsequent co-creation activities in Sprint 2. These activities, consisting of a series of workshops, addressed key aspects of the robot’s development, including design, functionality, and implementation within the real-world hospital environment.
The project benefitted significantly from the diverse perspectives brought forth by stakeholders. A positive outlook towards challenges and solutions from all parties expedited the development process, while clear and consistent communication ensured alignment throughout. Close collaboration between technical and non-technical partners fostered a unified problem-solving approach, further contributing to the project’s success.
This study contributes to the growing body of knowledge around co-creation and its effectiveness in developing user-centered healthcare technologies. Future research can explore the long-term impact of SAHRs on nursing staff and patient outcomes, while further refining co-creation methodologies for optimal stakeholder engagement in healthcare innovation projects.
Footnotes
Acknowledgements
We extend our deepest gratitude to the dedicated nurses, clinicians, and patients who are considering or participating in this study. Their invaluable contributions were instrumental in advancing knowledge in understanding the role of socially assistive robotic nurses in hospitals.
Author contributions
U.A., B.B, I.M, N.P., I.R.R., V.S. devised the project, the main conceptual ideas and proof outline. B.B, I.M, N.P., S.U., I.R.R., R.S., V.S. conceived and planned the experiments. B.B, I.M, S.U., I.R.R., V.S. carried out the experiments. U.A., B.B, I.M, N.P., S.U., I.R.R., R.S., V.S. contributed to the interpretation of the results. U.A. wrote the manuscript with support from I.M, V.S. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was carried out under the Horzion H2020 funded project HosmartAI (Grant no. 101016834) and the ARIS research and infrastructure programme (Grant no. P2-0069) The funding source had no impact on the decision to carry out the study or in its design. The funding source had no impact on the decision to publish this research. The content of this paper does not reflect the official opinion of the European Union or any other institution. Responsibility for the information and views expressed therein lies entirely with the authors.