
Abstract
Objectives
Our study analyzed dental nurses’ use and use behavior determinants of electronic patient IS modules in telephone triage. The modules were implemented in public oral healthcare organizations’ patient ISs to digitalize the national waiting time monitoring system.
Methods
For the cross-sectional survey, we collected data from dental nurses using convenience sampling and applied a modified UTAUT as the theoretical framework.
Results
The results indicate that using the module for different purposes varied, and the nurses used it sparsely in recording data for monitoring national waiting times. Using the module was laborious, and triage work was busy.
Conclusion
Dental nurses’ low system usage resulted in poor-quality data for waiting time monitoring. As healthcare data is increasingly used for purposes other than clinical decision making, we must ensure that healthcare professionals performing clinical tasks perceive data recording for non-clinical purposes as meaningful and have time for proper data entry.
Introduction
In healthcare, decisions are made at national, organizational, and individual levels, and varied information is required for clinical, management, internal, and external purposes. 1 In many healthcare systems, waiting time information is essential in decision making, as the length of waiting times remains an issue across the world. Combining maximum waiting times stipulated in regulation and regular waiting time monitoring with different demand- and supply-side interventions has proved successful in addressing these issues. 2
For waiting time monitoring, high quality statistical data is required. The key aspects are relevance, availability, and accuracy. 3 There is no single high quality statistical waiting time data, but several. For example, national-level and the organizational-level decision making require differing statistical data to establish indicators. The concept of actionable indicators 4 emphasizes an indicator’s fitness for purpose.
Waiting time for primary care is defined as the amount of time to receive an appointment with a healthcare professional. 5 For waiting time monitoring of these appointments, the purpose-fitting indicator for national authorities is retrospective “completed waits”. 6 These refer to the realized waiting times of patients who already had an appointment, 7 e.g., the average waiting time to see a dentist was 68 days. Healthcare organizations often have internal indicators to assess patients’ waiting times. 8
The national authorities must acquire the data for waiting time monitoring from healthcare organizations. There has been speculation that self-reported information may be biased.9,10 Therefore, investments in information systems (IS) have been made to obtain data to control organizations’ behavior. 11 The supposition that data extracted automatically from electronic patient ISs guarantees the validity of waiting time information is false. Interviews in the Swedish healthcare system 12 showed that sending usage guidelines written by administrative managers via email was not a successful strategy for implementing a new waiting time reporting IS. Healthcare professionals did not adhere to the guidelines, as they did not perceive the system as useful.
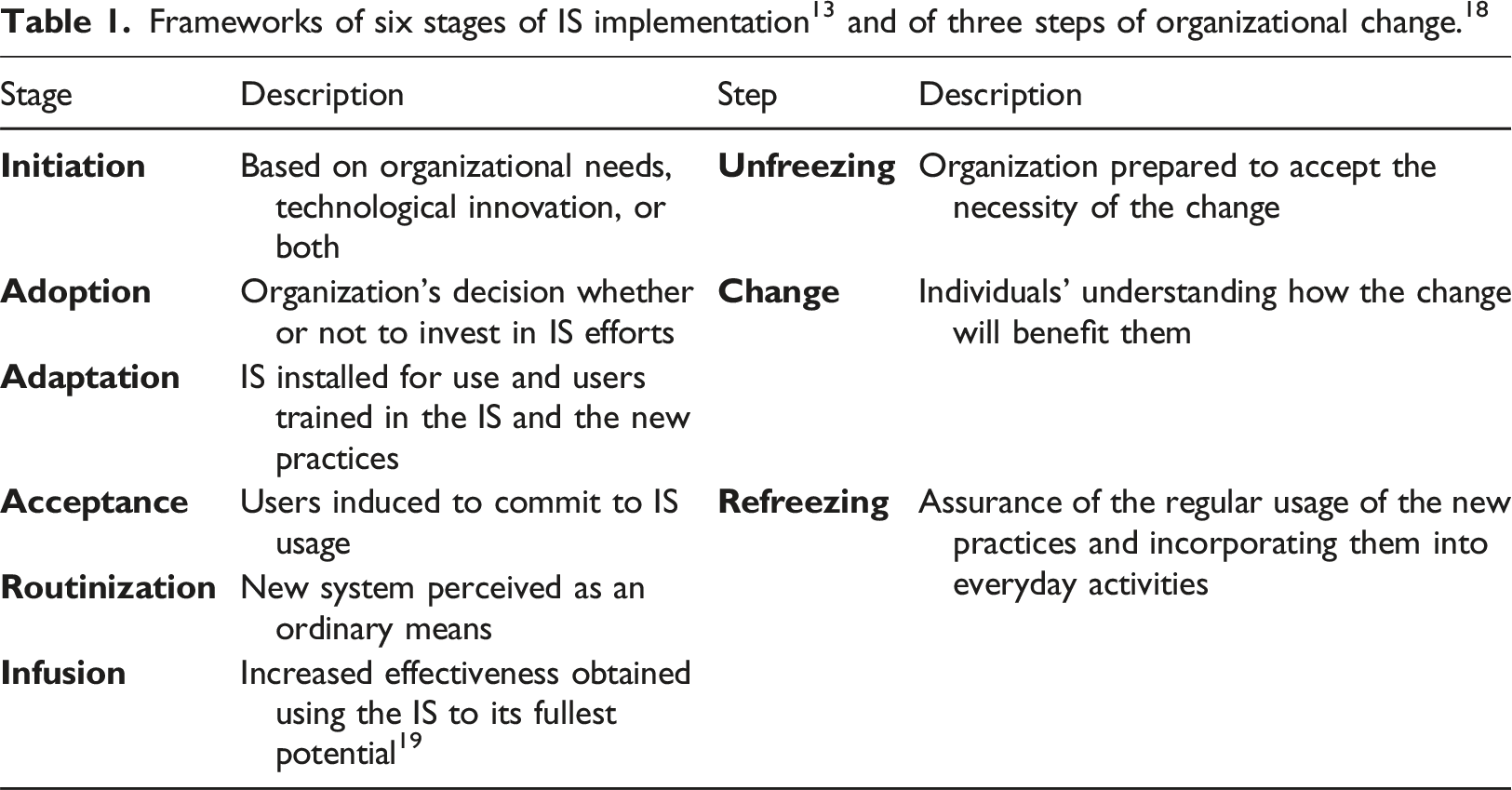
In Finland, the Healthcare Act 20 defines times for care guarantee, as well as maximum allowed waiting times for care in public primary oral healthcare. This waiting time is defined as the period from triage contact to an appointment to see a dentist. To monitor realized waiting times nationally, all public primary oral healthcare organizations must provide data to the Finnish Institute for Health and Welfare (hereafter the Institute).21,22 Since 2014, data has been submitted from electronic patient ISs to the Institute. 23 Before 2014, the data was gathered from oral healthcare managers through questionnaires twice a year. The electronic monitoring system meant that each organization had to implement a new module in its electronic patient IS. Altogether, there were six electronic patient ISs in public oral healthcare. During and after the implementation, the success of the national monitoring system was not rigorously evaluated.
Digitalizing the waiting time monitoring system was a national-level decision in Finland. Specific data was required, and IS offered a new method of data acquisition. In oral healthcare organizations, there was no need to initiate this IS investment. The solutions to the waiting time problem differ, such as improving the allocation of appointment slots and reducing no-shows for scheduled appointments. 24 As a result of the national decision, technical implementations were completed, but the internal justifications for any change were missing in organizations. There was no understanding of how a change requiring more documentation would benefit patients and healthcare professionals in the issue of waiting time. Based on the literature, “patient-oriented” nurses 25 generally experience documentation as a meaningless burden that is of no benefit to the patient, 26 and documentation remains insufficient when nurses work in a hurry. 27 Nurses’ attitudes are more negative toward administrative than clinical documentation. 28
Our study analyzes dental nurses’ use of the electronic patient IS module in telephone triage and the determinants of this usage. The theoretical framework for the study was adapted from the United Theory of Acceptance and Use of Technology (UTAUT). 29 Digitalizing the national waiting time monitoring system technically enabled new data for the decision making of triage dental nurses, dentists, and the national authorities. For high quality decision making, data must also be relevant and accurate. This cannot be realized if the systems are not defined and used appropriately. In this study, we focus on analyzing dental nurses’ use of the electronic patient IS module in telephone triage. For example, nurses’ system usage contributes to the quality of data in the system, and sparse data recording results in poor-quality waiting time data for decision making at the national level. The research questions are: 1) How do dental nurses use the electronic patient IS module in triage? 2) Which factors determine this usage?
Materials and methods
Survey participants
To study dental nurses’ usage of the patient IS module and use behavior determinants in telephone triage, we conducted a cross-sectional electronic survey in 2021 of public primary oral healthcare in Finland. The Ethics Committee for Human Sciences at the University of Turku approved the study proposal in February 2021 (Permit 7/2021). Each dental nurse was required to provide informed consent to participate in the study at the beginning of the electronic questionnaire. We also submitted applications for research permits to all 135 public primary healthcare organizations in Finland. Of these, 48% had a population base of more than 20,000. We obtained permits from 105 organizations.
The research design was originally a census study, including all Finnish-speaking triage dental nurses from all public primary oral healthcare organizations in Finland. Practically, all triage dental nurses speak Finnish, but 22% of the organizations did not approve the research permit. The census study turned into convenience sampling, including all Finnish-speaking triage dental nurses who worked in the 105 organizations. The number of Finnish-speaking triage dental nurses in these organizations in May 2021 was 915.
In Finland, a triage dental nurse assesses each patient’s dental care needs in telephone triage before they can access public primary oral care. With the new patient IS module, 23 nurses received the right to access patients’ dental histories to support their treatment-priority decision making in triage. Using the module was mandatory, but the module did not force users to utilize all of its functionalities. The data concerning the triage contact of a patient was recorded into an electronic patient IS either manually by nurses or automatically. However, nurses were required to make the entries required for booking appointments. The clinical data, such as patients’ symptoms and reasons for seeking treatment, could be recorded into the system and subsequently available for dentists. Recorded triage contact data, which may be incomplete, was automatically submitted to the Institute once a day, using pre-defined content. 30 The systems of the Institute processed the individual-level data, including the data of each triage contact, appointment, and cancellation 30 into aggregated summary reports of realized waiting times. The national authorities used these reports for monitoring the care guarantee. The Institute also published reports on its public website. 23
Survey data
The theoretical framework of our study (Figure 1) was based on the UTAUT,
29
which has been used to study the acceptance of various technologies in healthcare through different user groups.
31
However, its usage in analyzing the utilization of nursing information technology is minor.
32
Theoretical framework of this study adapted from the UTAUT.
29
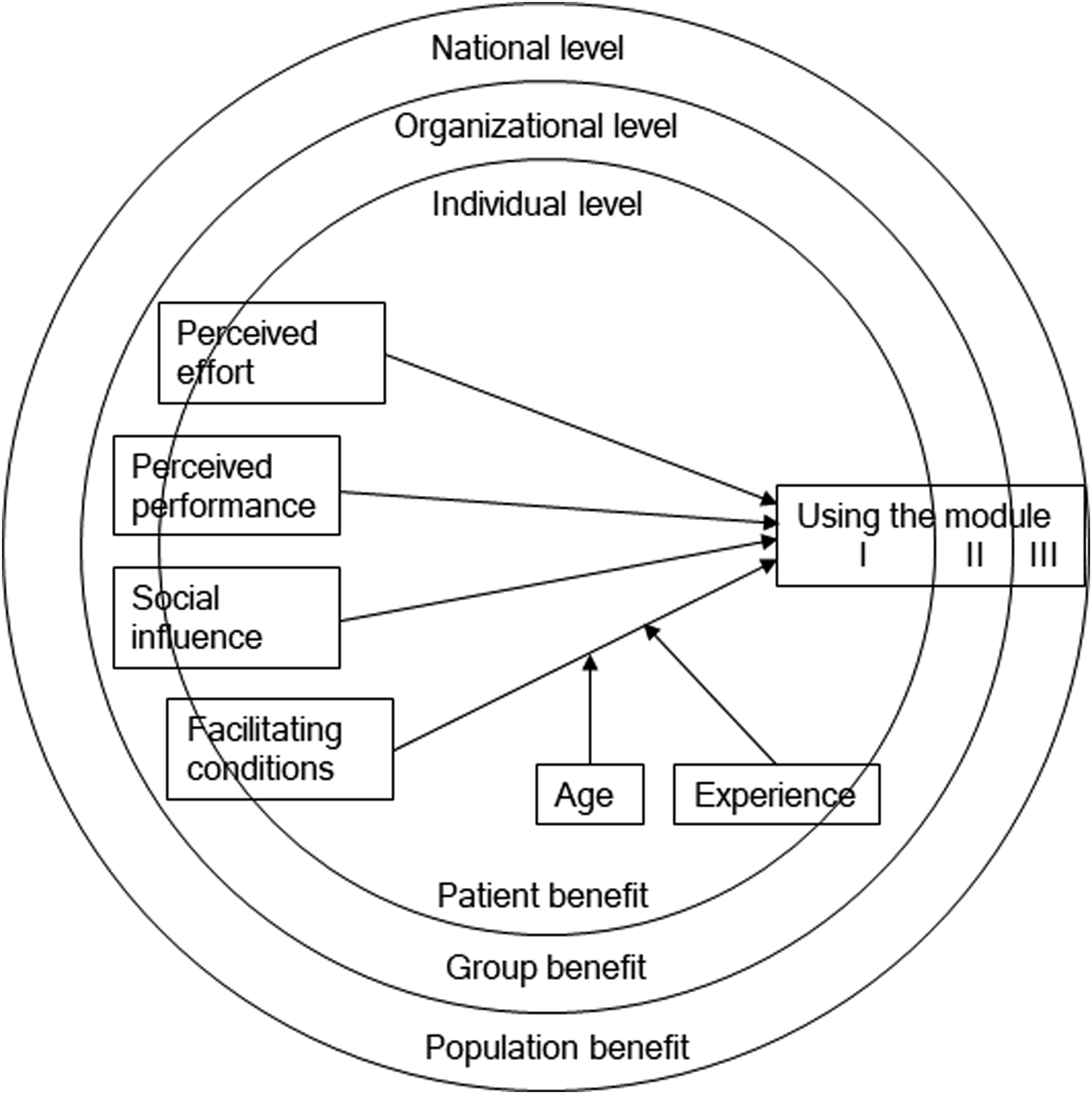
In the present study, we examined actual usage, as the investigated module had been in use for years. We were interested in dental nurses’ using the module for three purposes: I) Supporting decision making in triage, II) Recording data for dentists, and III) Recording data for the Institute. Using the module for the first purpose assisted triage nurses’ decision making (patient benefit), while using the module for the second and third purposes provided data for dentists’ decision making (patient and group benefit) and provided data for the national level to monitor realized waiting times (population benefit), respectively.
In the UTAUT, 29 the constructs effort expectancy, performance expectancy, and social influence are used to determine the construct of intention to use, which, in addition to the construct of facilitating conditions determines the construct of usage behavior. As the IS module studied had been employed for years, we did not utilize intention to use as a determinant. We rather used the four other constructs to determine directly the module usage. Each determinant was characterized by its equivalent determinant in the UTAUT. Perceived effort was defined as the degree of ease in learning and using the system, and perceived performance referred to the degree to which the system helped improve job performance. Social influence was defined as the degree to which people important to the individual communicated the individual should use the system, while facilitating conditions referred to the degree to which infrastructure existed to support using the system.
In literature, performance expectancy has been the clearest determinant of healthcare professionals’ behavioral intention.33–37 Effort expectancy has been demonstrated as both a clear determinant of behavioral intention33–38 and not.39,40 Social influence has had positive effects on users’ behavior in healthcare.38,39,41,42 Healthcare professionals may feel more social influence from peers than from top managers, 34 and facilitating conditions have been significant predictors of usage.36,39,41,42
As moderators on facilitating conditions, we included age and experience in the same manner as in the UTAUT. 29 We defined experience as dental nurses’ proficiency in telephone triage, as studies in other healthcare areas have emphasized that the telephone as a service medium requires special skills.43–45 Significant learning occurs while working on these tasks,43,45 though sufficient time is also essential. 44 We supposed that these results may also prove valid in telephone triage tasks in oral healthcare, and this experience might affect the use behavior. To measure experience, we used a 5-point ordinal scale (daily or almost daily = 1, weekly or almost weekly = 2, monthly or almost monthly = 3, occasionally, e.g., during holiday seasons = 4, and very rarely or never = 5).
In the survey, we investigated each determinant construct with three items (Supplemental Appendix A) adapted from Venkatesh et al.29,p.460 using a 5-point Likert scale (strongly disagree = 1, disagree = 2, neither agree nor disagree = 3, agree = 4, and strongly agree = 5). We chose three items in each determinant and a 5-point Likert scale to increase the response rate. For the usage behavior, we included one item for providing data for dentists, one for providing data for the Institute, and three for supporting decision making in triage. These three items were for the module usage in analyzing a patient’s health problem, improving the effectiveness of treatment assessment decisions, and enabling individualized care. We measured the usage behavior with a 5-point ordinal rating scale (not at all = 1, a little = 2, somewhat = 3, much = 4, and a great deal = 5). The questionnaire also included queries on backgrounds and for other studies. At the beginning of the questionnaire, we asked each respondent to provide informed consent to participate in the study.
We pre-tested the Finnish questionnaire to ensure its clarity and comprehensiveness. We sent the pre-survey to ten dental nurses in three organizations, and all answered. Based on the comments, we made minor changes to improve clarity. In the pre-test phase, no statistical analysis was conducted. To gather data, we used the software Webropol Survey & Reporting, Version 3.0, and an open Internet link to allow anonymous responses. We sent the Internet link to the contact persons of the oral healthcare organizations at the beginning of May 2021. The persons were named for this task in the approved research permits. Reminders for answering were sent at the end of May 2021, and the questionnaire remained available until 11th June 2021.
Statistical analysis
We used the software IBM SPSS Statistics for Windows, Version 28.0.0.0 for our statistical analyses. The data gathered with ordinal and 5-point Likert scales was handled as interval-level data.
46
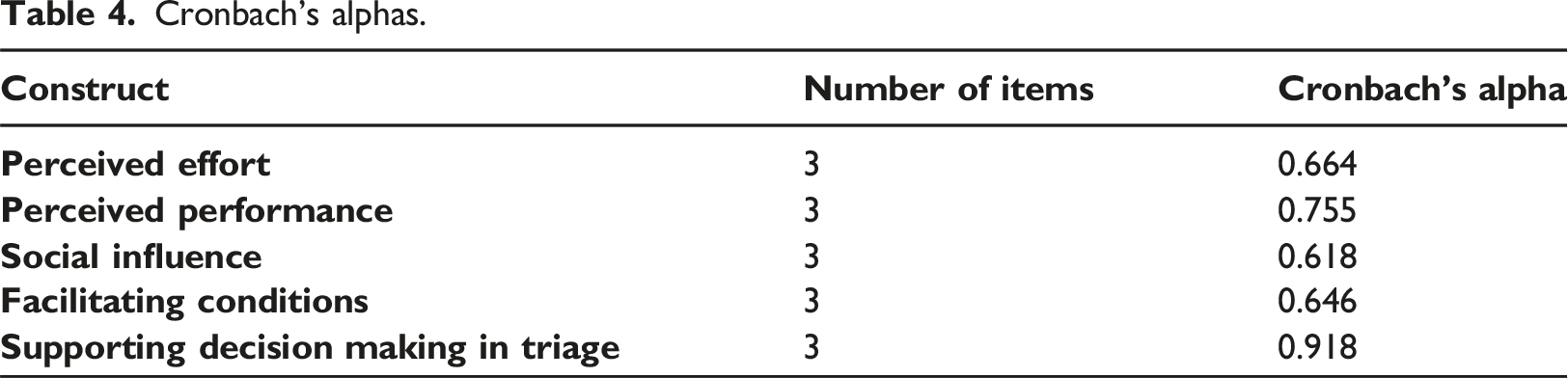
Any missing data was handled using listwise deletion. To describe the background data of dental nurses and the determinant items of the IS use behavior, we calculated measures of central tendency and variability. The distribution of the actual use behavior variables was illustrated using box plots. We compared the means of two dental nurse group variables using two-tailed Student’s t-tests assuming unequal variances. The chi-squared test of independence was employed for the categorical variables. The four use behavior determinant variables and one actual use behavior variable were summated from their three-item variables. To assess the internal consistency of the sum variables, we used Cronbach’s alpha, with a threshold of 0.6 considered acceptable.
47
We used binary logistic regression to study the associations between the use behavior determinant variables and the actual use behavior variables. The independent variables were used as continuous variables when there was a linear relationship between any continuous independent variables and the logit transformation of the outcome variable
Results
Of the 915 potential respondents, 294 answered the questionnaire, a response rate of 32%. Two respondents did not provide informed consent to participate in the study. The number of dental nurses included in the analysis was 292. There was also minor data loss because not all nurses answered every question. The number of respondents answering the different questions varied from 274 to 292. The number of valid responses (n) is separately reported for each question.
Background information
Descriptive statistics of the respondents.
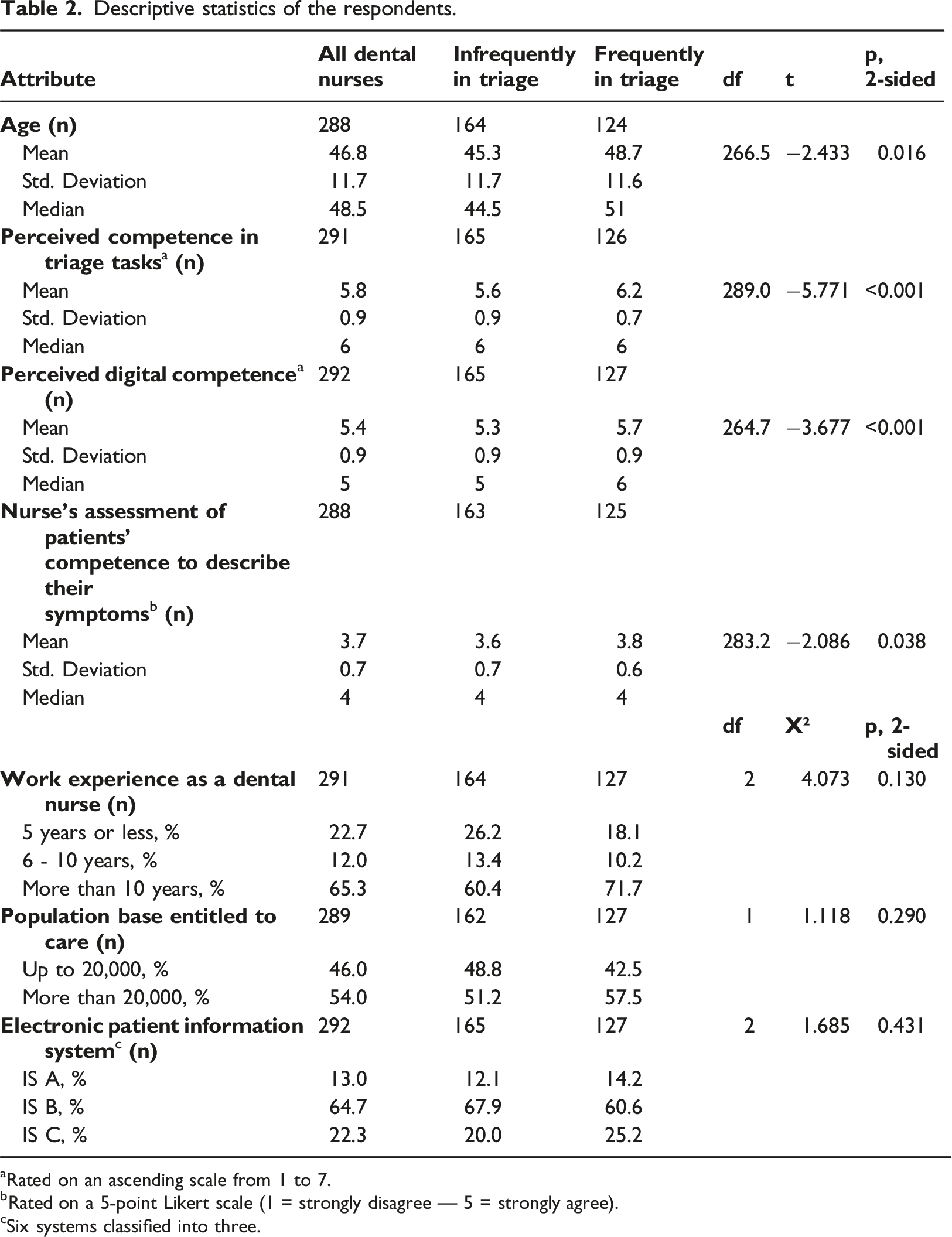
aRated on an ascending scale from 1 to 7.
bRated on a 5-point Likert scale (1 = strongly disagree — 5 = strongly agree).
cSix systems classified into three.
Using the electronic patient IS module in triage
Figure 2 presents triage dental nurses’ actual use of the electronic patient IS module for supporting their decision making in triage, recording data for dentists, and recording data for the Institute. The differences in the use between the dental nurses working infrequently in triage and those working frequently were statistically significant for the purposes Supporting decision making in triage (Pearson Chi-Square 11.891; df3; 0.008 two-sided) and Recording data for the Institute (Pearson Chi-Square 16.500; df3; <0.001 two-sided). The difference between the nurse groups using the module for Recording data for dentists was not statistically significant (Pearson Chi-Square 3.834; df3; 0.280 two-sided). Dental nurses’ use of the electronic patient IS module for three purposes in telephone triage using Questionnaire score: 1 = not at all, 2 = a little, 3 = somewhat, 4 = much, and 5 = a great deal.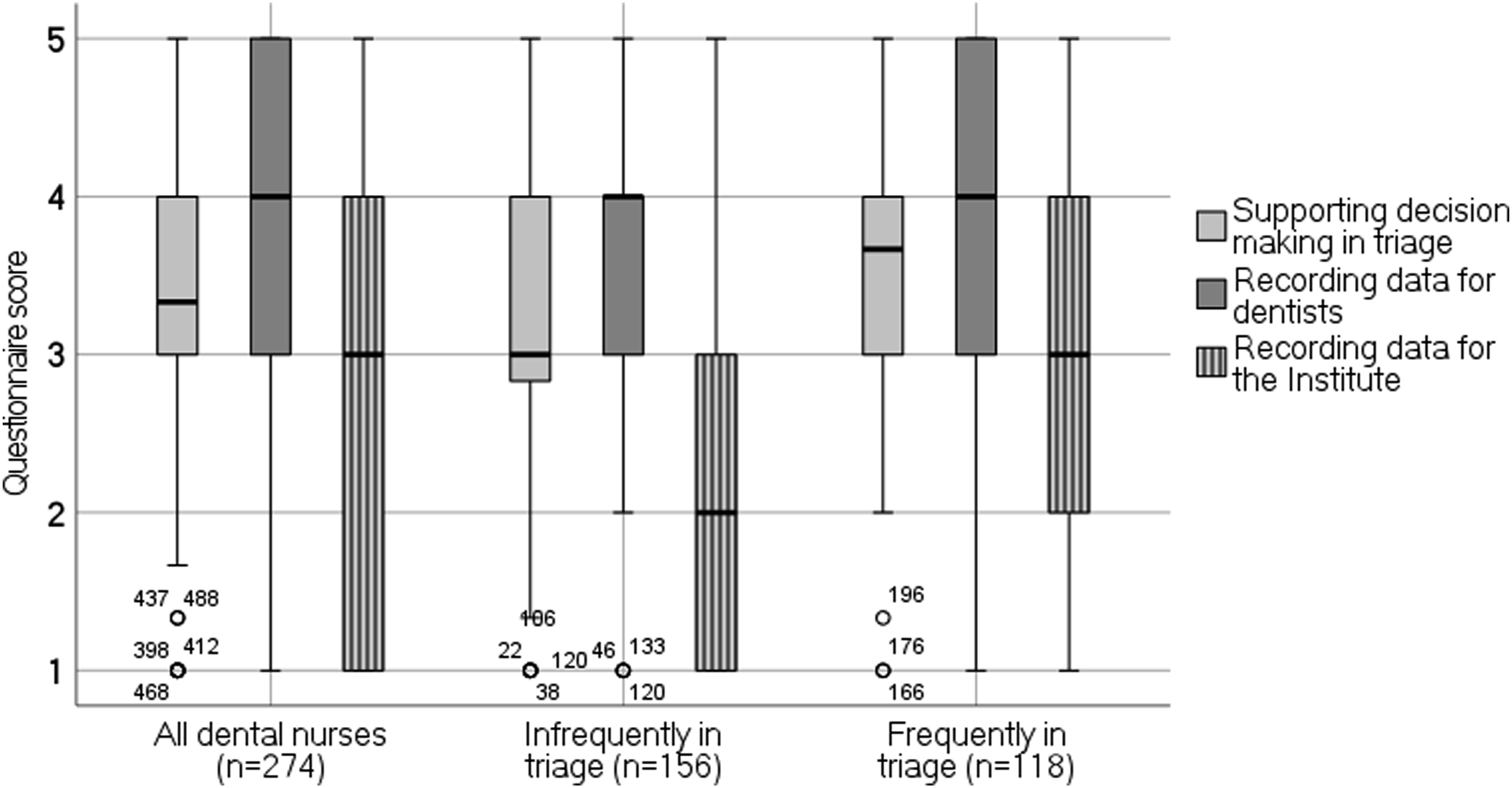
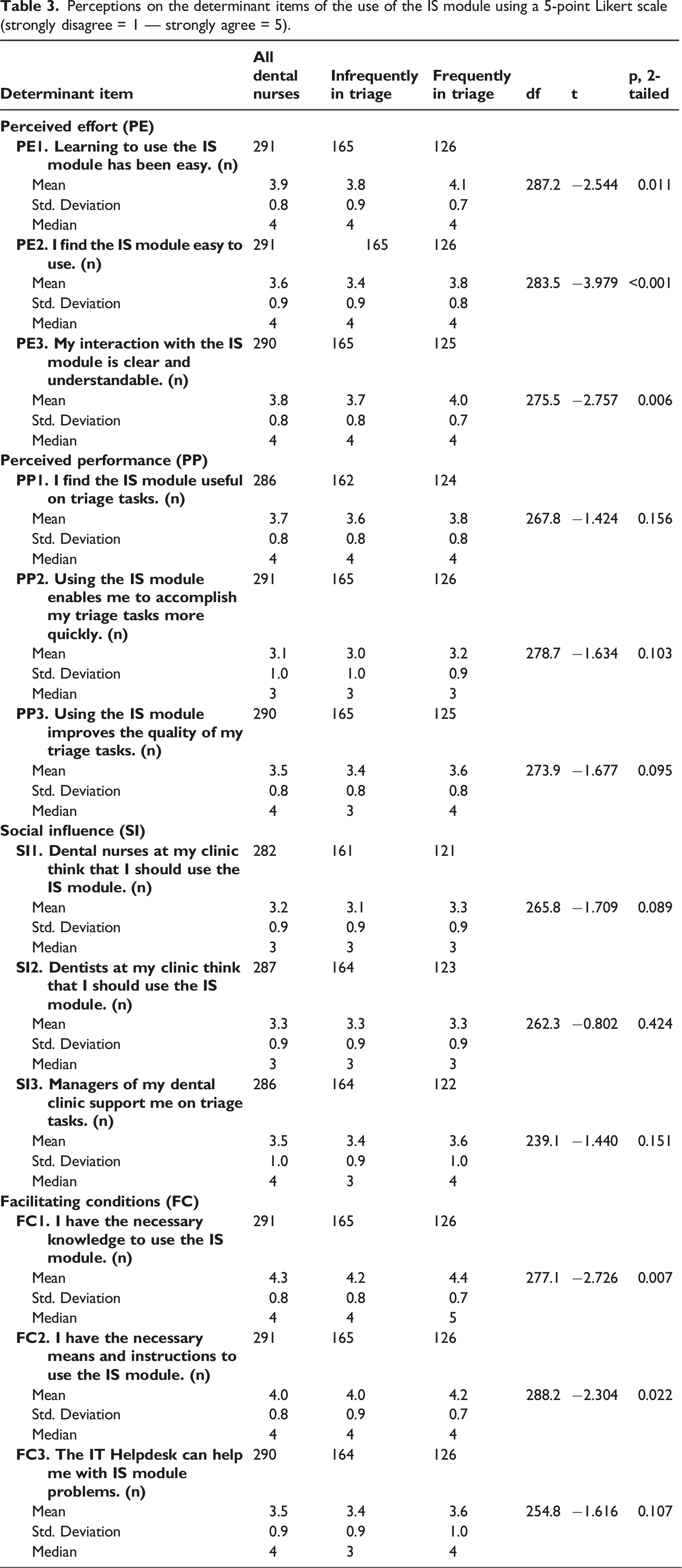
Determinant items of using the module in triage
Perceptions on the determinant items of the use of the IS module using a 5-point Likert scale (strongly disagree = 1 — strongly agree = 5).
Determinants predicting the module usage in triage
Cronbach’s alphas.
Supporting decision making in triage
Model summary for the binary logistic regression model for Supporting decision making in triage.
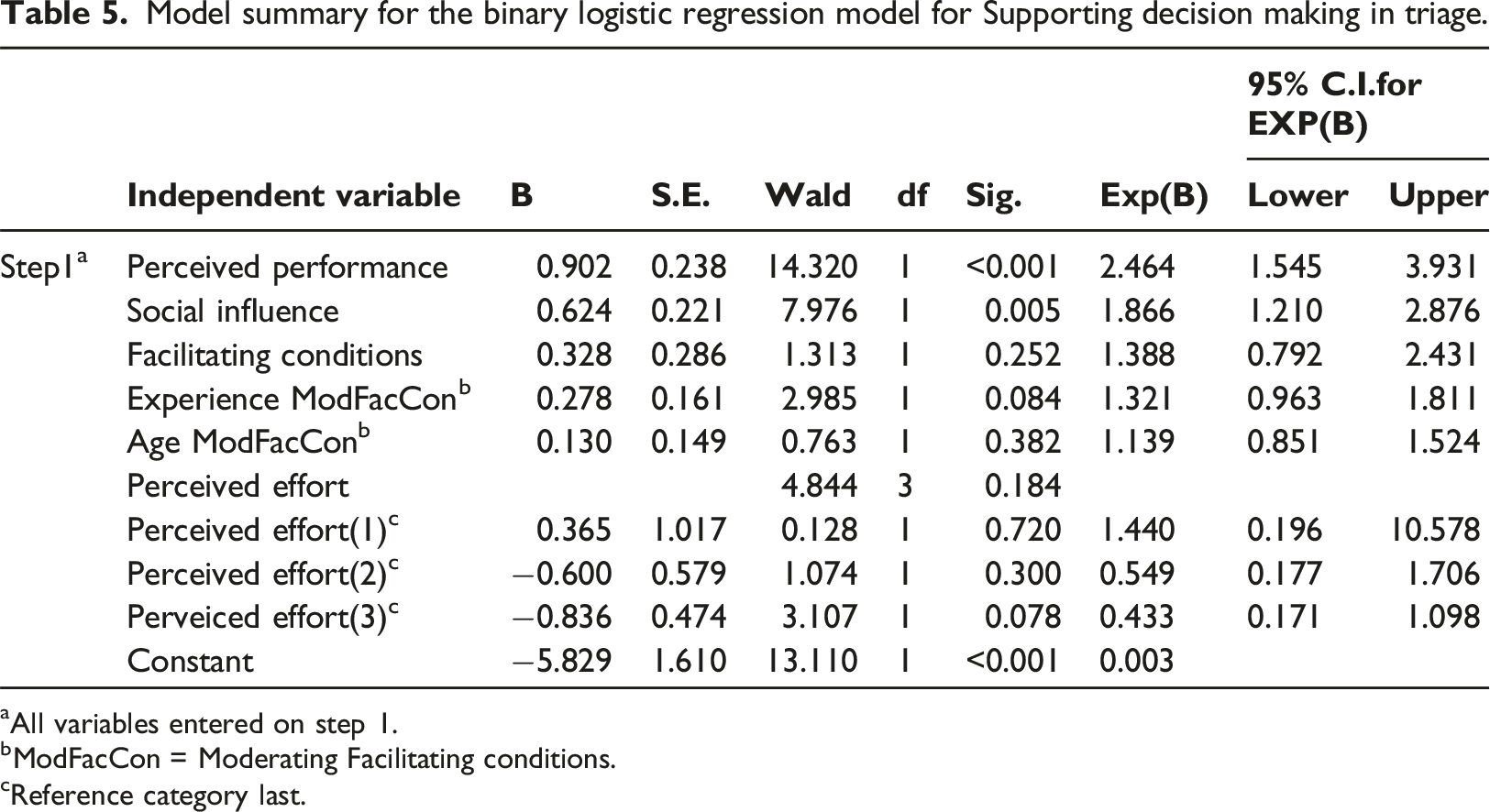
aAll variables entered on step 1.
bModFacCon = Moderating Facilitating conditions.
cReference category last.
Recording data for dentists
Model summary for the binary logistic regression model for Recording data for dentists.
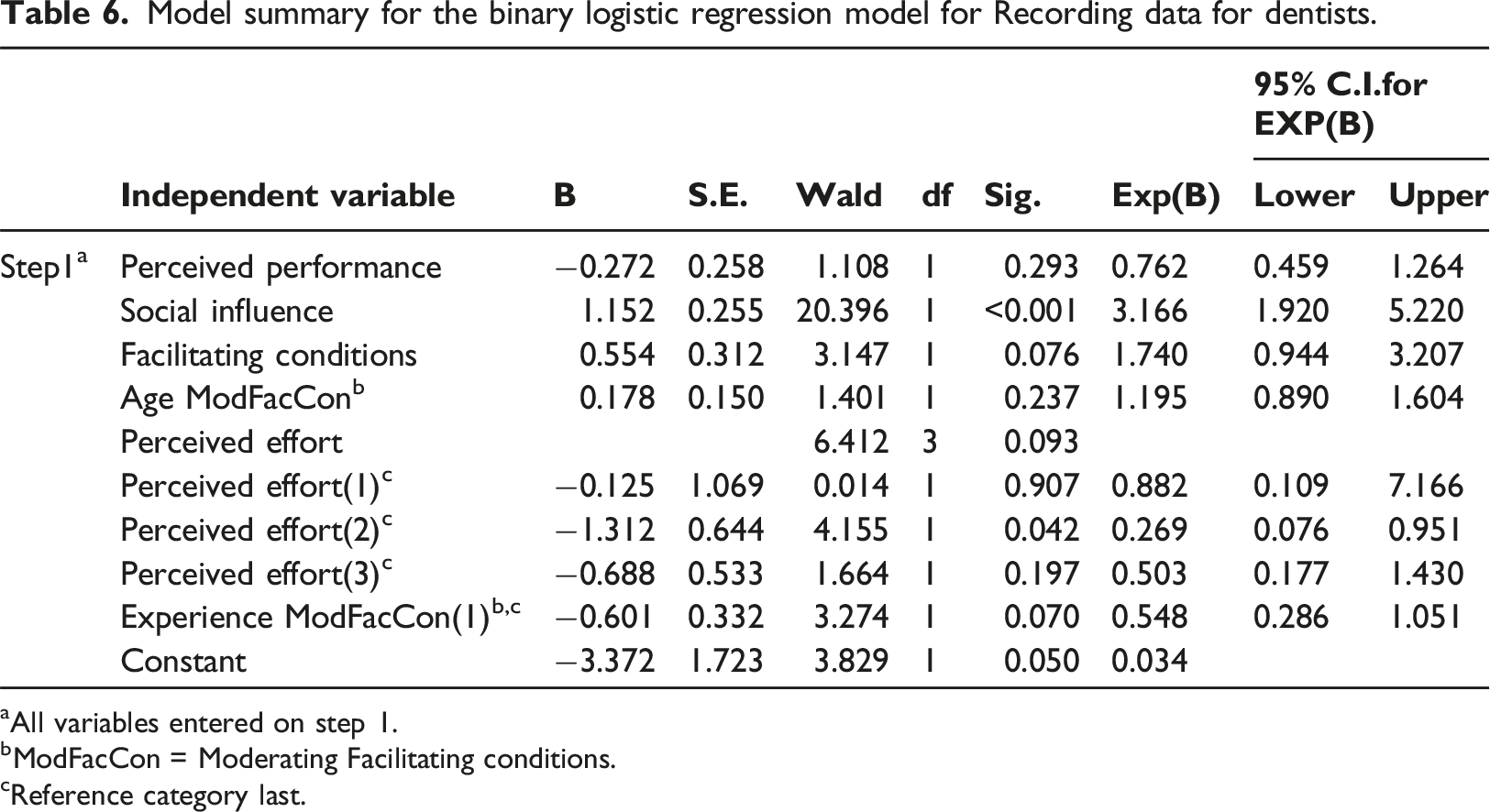
aAll variables entered on step 1.
bModFacCon = Moderating Facilitating conditions.
cReference category last.
Recording data for the institute
Model summary for the binary logistic regression model for Recording data for the Institute.
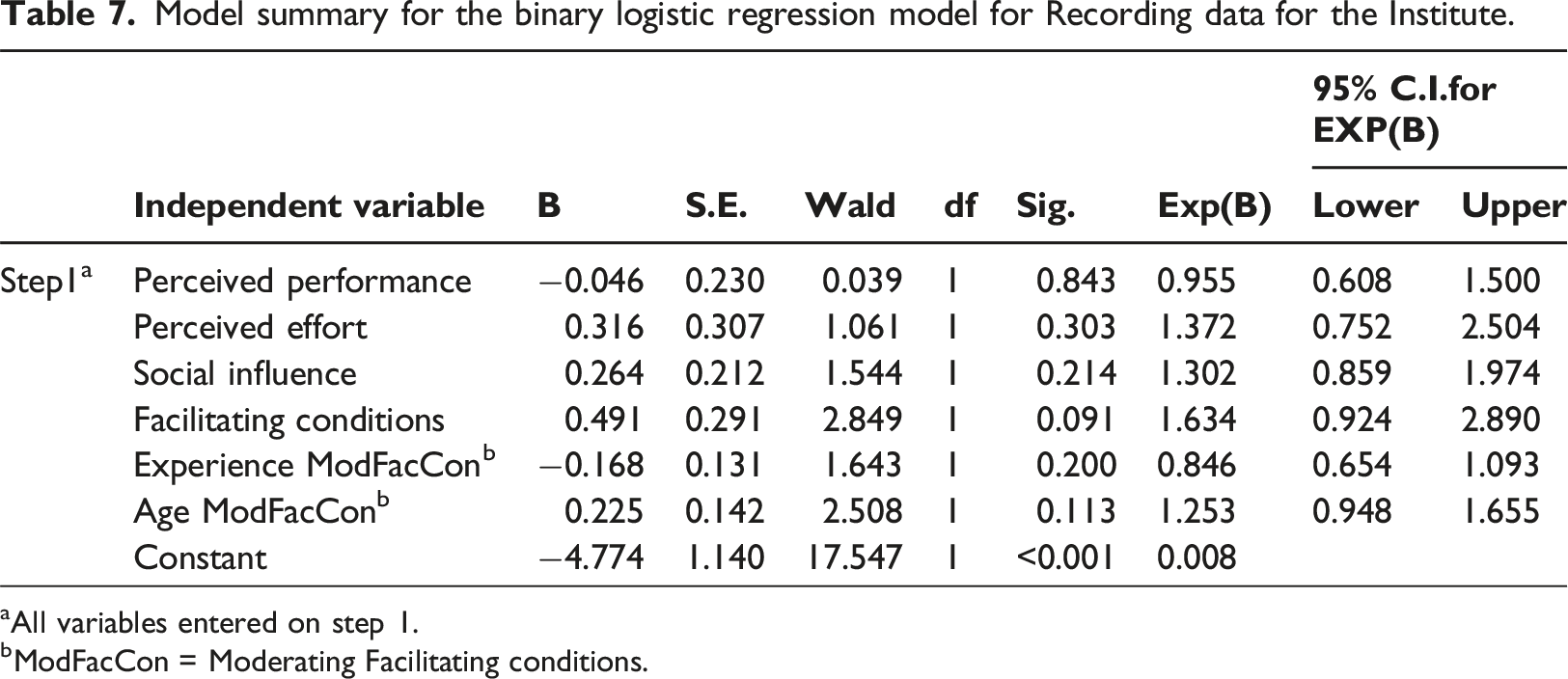
aAll variables entered on step 1.
bModFacCon = Moderating Facilitating conditions.
Discussion
This cross-sectional study analyzed how dental nurses used the electronic patient IS module in telephone triage and which factors determined this usage. The modules were implemented in oral healthcare organizations’ electronic patient ISs to nationally monitor patient waiting times for public oral care in Finland. In the study, an electronic questionnaire based on a modified UTAUT model 29 was used. The results indicate that the dental nurses’ use of the module was positively associated with the frequency of triage work. All nurse groups used the module least for recording data for national-level purposes. Perceived performance and social influence predicted using the module for supporting nurses’ decision making in triage, and social influence also predicted using the module for recording data for dentists.
The UTAUT has been used in healthcare to study the determinants of behavioral intention. 31 In our study, we used the model adapted from the UTAUT to analyze nurses’ actual use behavior, which has been less studied. 32 Our model fitted the data. The changes in the module usage that could be accounted for by the four predictors were not high. In the binary logistic regression models, the values of Nagelkerke’s R2 were 8.3, 24.0, and 24.3. The value was the lowest in predicting the usage behavior of recording data for national-level purposes.
Performance expectancy has been the clearest determinant of healthcare professionals’ behavioral intention in earlier studies.33–37 In our study, perceived performance only determined nurses using the module for supporting their decision making in triage. The items of the determinant perceived performance may explain this. The nurses perceived that module usage increased the quality of their work in triage to assess patients’ dental care needs and to make decisions on treatment priority. On the other hand, recording data for administrative purposes for the national level might have been sparse as nurses perceived that using the module took time. Based on the literature, documentation remains insufficient when nurses work in a hurry, 27 and their attitude is more negative toward administrative than clinical documentation. 28
Social influence has demonstrated impacts on behavioral intention in earlier research.38,39,41,42 In our study, social influence determined using the module for recording data for dentists and supporting nurses’ decision making in triage. These usages impact the functioning of the dental clinic for group benefit and the quality of care for patient benefit. Dental nurses working frequently in triage perceived that the dental clinic managers supported them more than other dental nurses and dentists. This finding is in dissonance with earlier study results. 34
Digitalizing the national waiting time monitoring system did not guarantee accurate data for national decision making, corresponding to the results found in the Swedish healthcare system. 12 Triage nurses used the module for recording data for national-level purposes sparsely. Insufficient data in the system did not deliver the Institute a trustworthy picture of realized waiting times. The relevance of realized waiting time data in decision making at the national, organizational, and individual levels differs. Oral healthcare managers need waiting time data to manage patient waiting times in their organizations, but most organizations have internal indicators for this purpose. 8 Neither is the retrospective “completed wait” 6 the indicator that fits for decision making to manage current situations. For dental nurses and dentists, the purpose-fitting data for decision making concerns individual patients’ dental histories and reasons for seeking treatment.
As there was next to no need for realized waiting time data in oral healthcare organizations, little incentive existed to invest in a new IS and to prepare for organizational changes. Dental nurses were not convinced that digitalizing the monitoring system, which meant more documentation to them, is critical to making decisions on waiting times at the national level. Without understanding this importance and without sufficient guidance to institutionalize usage, dental nurses’ data recording for the population-level purpose was not appropriate in the busy telephone triage work. In dental clinics, communication should be improved to understand changes and motivate behavior. However, dental nurses and dentists consider shortening waiting times crucial for care quality and patient satisfaction.
Practical implications
The IS requirements might be more successful if the national and organizational level actors define them together. Both groups need data on waiting times for decision making, but the purpose-fitting indicators differ. The national system was designed to analyze realized waiting times. The gathered data would have also enabled processing waiting time indicators for decision making on current situations. Participatory system design might have aroused interest among oral healthcare managers in digitalizing the system and introducing simultaneous organizational changes.
The evaluation of the progress of the implementation was neglected. At the time of our study, seven years had passed since the technical implementation, and the system was still not used to its fullest potential. 19 The goals of an IS implementation can be achieved only by using the system appropriately, and assurance of the usage of the new practices is critical.
The dental nurses working frequently in triage perceived their desk- and patient-oriented competencies to be better than other nurses. Either their characteristics differed from the beginning, or their competencies developed while performing these tasks,43,45 or both. It would be wise to organize shifts in triage so that the number of dental nurses working infrequently on these tasks is low.
Limitations and further research
Our study is not without limitations. Our research was cross-sectional, which means we cannot establish causality. We found that the data recorded for monitoring purposes was not comprehensive, leading to poor-quality data for national-level decision making. However, we cannot confirm whether poor data recording has continued since 2014.
The use of convenience sampling reduced the validity and credibility of our results. 49 Originally, the research design was a census study, but we did not receive research permits from one-fifth of the oral healthcare organizations. The triage dental nurses who responded to our study questionnaire represented all public primary oral healthcare organizations with different population bases quite well, but their responses may have been influenced by extremely positive or negative views. While we used probability sampling, the possibilities to generalize the study results are limited due to differences in healthcare practices and social and cultural aspects among countries.
The study questionnaire was not validated. The questionnaire items were adapted from analogous questions from Venkatesh et al. 29 that were translated into Finnish. The Finnish questionnaire clarity was pre-tested. Measurement errors may have arisen, as we investigated the actual usage of the IS module through nurses’ self-evaluation instead of using logs. The use behavior determinants were surveyed with three commonly used items, but the internal consistency of the determinants was not very high. In general, including more items in each construct improves Cronbach’s alphas but may decrease the response rate. In the spring of 2021, the coronavirus pandemic continued to cause challenges in the public oral healthcare system, which may have lowered the response rate.
We believe that the UTAUT needs further development to better explain and predict IS usage behavior in healthcare. In our opinion, the UTAUT would work better if it included determinants associated with population-level environmental issues. The healthcare system aims at the common good rather than just the individual good. The Theoretical Domains Framework 50 could help understand behavior changes in IS implementation. The framework is used for implementation in evidence-based healthcare practices, and includes several domains, such as environmental context and resources, and beliefs about consequences, that are suitable as determinants of IS usage behavior in healthcare.
Conclusion
The study results indicate that investments in IS do not necessarily guarantee the achievement of the goals set. The national authority assumed digitalizing the national monitoring system would result in accurate data to monitor waiting times. Nurses, however, did not use the system properly, as they did not understand the importance of recording data for national-level decision making for population benefit when focusing on individual patient benefit. The low system usage resulted in poor-quality data for waiting time monitoring. Healthcare data is increasingly required for national-level decision making, therefore we must ensure that healthcare professionals completing clinical tasks understand the importance of data for population benefit. They must perceive data recording for population-level purposes as meaningful and have sufficient time for data entry.
Supplemental Material
Supplemental material - National waiting time monitoring in oral healthcare – The role of triage dental nurses
Supplemental Material for National waiting time monitoring in oral healthcare – The role of triage dental nurses by Riitta Söderlund in Health Informatics Journal
Footnotes
Acknowledgements
The authors thank the Finnish public primary healthcare organizers for enabling the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability
According to the privacy policy, the researcher can process the survey data for the time required for her thesis. During this time, the data will not be transferred outside the University of Turku. After that, the data without the credentials is disclosed to the Finnish Social Science Data Archive without conditions for the use of the disclosed materials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.