
Abstract
Keywords
Introduction
The global population is progressively aging. It is projected that approximately 1.6 billion people worldwide will be older than 65 years, accounting for 16.7% of the global population of 9.4 billion. 1 Older adults are susceptible to injuries, with falls being the most common cause. 2 Approximately 30% of adults aged ≥65 years experienced falls at least once per year, and among them, 10.2% reported sustaining fall-related injuries. 3 Falling also contributes to injury-related fatalities. 4 Although most falls are non-fatal, some lead to serious injuries, including hip fractures. Approximately one-third of patients with femoral neck fractures experience declining health and die within a year. 5 A study estimates that by 2030, there will be 100,000 fatal falls among older adults annually, costing the United States $100 billion. 2 Numerous fall prevention interventions have been developed to improve the health and safety of older adults. A recent systematic review revealed that comprehensive multi-component programs, which include education, exercise, medication, mobility devices, vision, psychological management, and environmental modifications, 6 were found to be effective in preventing falls. 7
The need for non-face-to-face fall interventions has rapidly increased due to the advancement of digital health solutions and the threat posed by the coronavirus disease 2019 (COVID-19) pandemic. Subsequently, various information and communication technology (ICT) interventions for fall prevention have been developed. 8 ICT interventions can be classified into five categories: (a) telehealth, including exercises conducted in a non-face-to-face setting; (b) exergames that aim to improve physical well-being and leisure; (c) combined exercise and cognitive training; (d) computer feedback on balance control; and (e) smart home systems and fall detectors. Telehealth refers to communicating between healthcare providers and patients at home via phone or video calls. 9 Exergames are forms of physical activities combining exercises and games, which often use motion-sensing technologies to track a player’s motions. To evaluate the impact of non-face-to-face interventions on fall prevention, it is necessary to assess the effectiveness of each program.
Previous studies have investigated the effects of ICT interventions on fall prevention. However, most of these studies focused on partial ICT interventions, fall monitoring systems, or ICT combined with other interventions. Some studies have focused exclusively on equipment such as fall detection devices or sensors, rather than exploring the broader scope of digital healthcare.10–13 One review 14 focused on the technologies of fall monitoring systems and not comprehensive fall interventions. Another systematic review 15 examined psychometric properties, including the reliability and validity of balance and fall risk assessment tools. A systematic review 16 analyzed the effects of fall prevention interventions, however, no meta-analysis provided integrated quantitative results. While another recent systematic review 8 analyzed the effects of ICT interventions, it included non-ICT interventions, such as direct home visits 17 or telephone call. 18 Recently, a network meta-analysis 19 evaluated the effectiveness of technology-assisted rehabilitation on functional mobility, but their primary outcome of interest was not falls. To clarify their effects, it is necessary to analyze the outcome and effectiveness of ICT interventions for fall prevention. In this systematic review and meta-analysis, we aimed to analyze the effectiveness of different types of ICT interventions (e.g., telehealth, computerized balance training, exergaming, mobile application education, or virtual reality exercises) on fall prevention. The primary outcomes of interest were fall rates, proportion of fallers, balance, fall efficacy, and physical function. The secondary outcomes were quality of life, and cognitive function.
Method
This systematic review was conducted following the 2020 PRISMA statement 20 and the Cochrane guidelines.
Eligibility criteria
The inclusion criteria were as follows: (a) community-dwelling individuals aged ≥60 years; (b) experimental studies including fall prevention interventions using ICT; and (c) studies written in English. The interventions included telehealth, computerized balance training, exergaming, exercise with virtual reality, education through mobile applications, and cognitive-behavioral training. The outcomes included fall rates, proportion of fallers, balance, fall efficacy, quality of life, physical function, and cognitive function. The exclusion criteria were as follows: (a) posters, abstracts, studies on animals, non-English-language studies, duplicated studies; (b) studies with a mix of online and offline interventions; and (c) protocols and reviews.
Data sources
The selection of the search database was based on the COre, Standard, Ideal (COSI) model endorsed by the National Library of Medicine in the United States, following formal and established protocols. 21 We searched the following databases for published articles up until November 15, 2023: Ovid-MEDLINE, Ovid-EMBASE, Cochrane Library and Cumulative Index of Nursing and Allied Health Literature (CINAHL).
Search strategy
We placed no restrictions on the year of publication. Comprehensive search strategies for all searches and databases are included in the supplemental material (Appendix 1).
Selection and data collection processes
In the initial phase of the selection process, two researchers independently reviewed the titles and abstracts after removing duplicate studies. In the second phase, the two researchers further reviewed the full texts of the selected literature. In case of any disagreement, a third party was involved as an arbitrator, and a decision was reached by majority vote. Two independent reviewers collected the data separately and compared the extracted data for consistency. After the initial conversation, any discrepancies were resolved by a third person.
Data items
Two researchers independently extracted and verified the data using a predefined extraction form. We extracted data on the characteristics of the included studies, comprising the following: (a) country, first author, and year of publication; (b) participant numbers, average age, and gender; (c) intervention information data (duration, follow-up period, and control content); and (e) outcome measures. Additionally, the ICT interventions, including telehealth, computer feedback, smart home systems, exergames, and cognitive games were examined. Subsequently, the outcomes of the ICT interventions, including fall rates, the proportion of fallers, balance, fall efficacy, physical function, quality of life, and cognitive function, were evaluated.
Risk of bias
The researchers separately assessed potentially eligible studies for inclusion based on the complete text and addressed any disagreements through discussion. The quality of the included studies was evaluated using the Cochrane Risk of Bias tool (RoB) 22 designed for randomized controlled trials (RCTs). Additionally, the RoB for non-randomized studies was assessed using the Risk of Bias Assessment Tool for Non-randomized Studies (ROBANS). 23
Effect measures
Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for dichotomous data. For continuous data, we conducted a meta-analysis using the mean differences (MDs) with standard deviations (SDs) and 95% CIs. If more than one tool was used, the standard MDs were analyzed. The heterogeneity among the selected studies was evaluated using a chi-squared test with a significance level of p < .100 and I2 statistics, including meta-analyses. Data were analyzed using a fixed-effects model when I2 was less than 50%.
Synthesis methods
The combination of outcomes from separate studies was obtained based on the assessment of heterogeneity. When studies were determined to have sufficiently homogeneous study designs, a meta-analysis was conducted to determine statistical heterogeneity. Statistical analyses were performed using ORs and fixed-effect models, which were preferred. If significant heterogeneity was observed, we employed the random-effects model for our analysis. Additionally, because the physical functions of the two tools, Timed Up and Go (TUG) 24 and Short Physical Performance Battery (SPPB) 25 were opposed, the resultant value from one tool was multiplied using a negative (−) before being evaluated. The Cochrane’s Review Manager program (RevMan version 5.4.1) was used for statistical analysis.
Results
Study selection
We initially retrieved 6361 articles from four databases, including Ovid-MEDLINE, Ovid-EMBASE, Cochran Library and CINAHL. After excluding overlapping articles and reviewing the titles and abstracts, 209 of which were selected. After checking the full text, 31 articles were selected. In addition to the database searching, three articles were added by a citation searching. Ultimately, a total of 34 articles9,26–58 were selected. Among these, 33 studies9,26–36,38–58 were RCTs while one
37
was a quasi-experiment (Figure 1).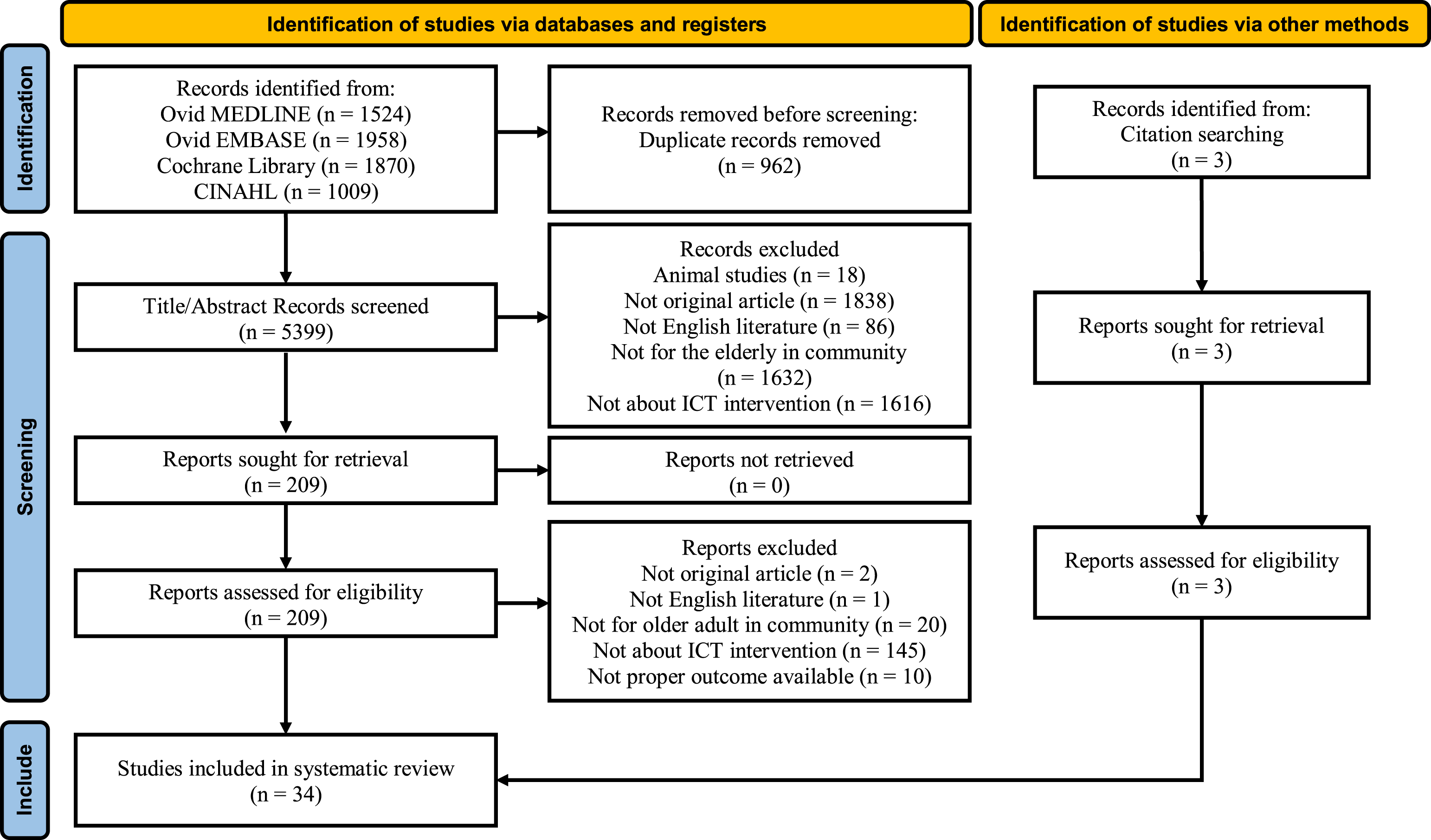
Study characteristics
Characteristics of the selected studies (n = 34).
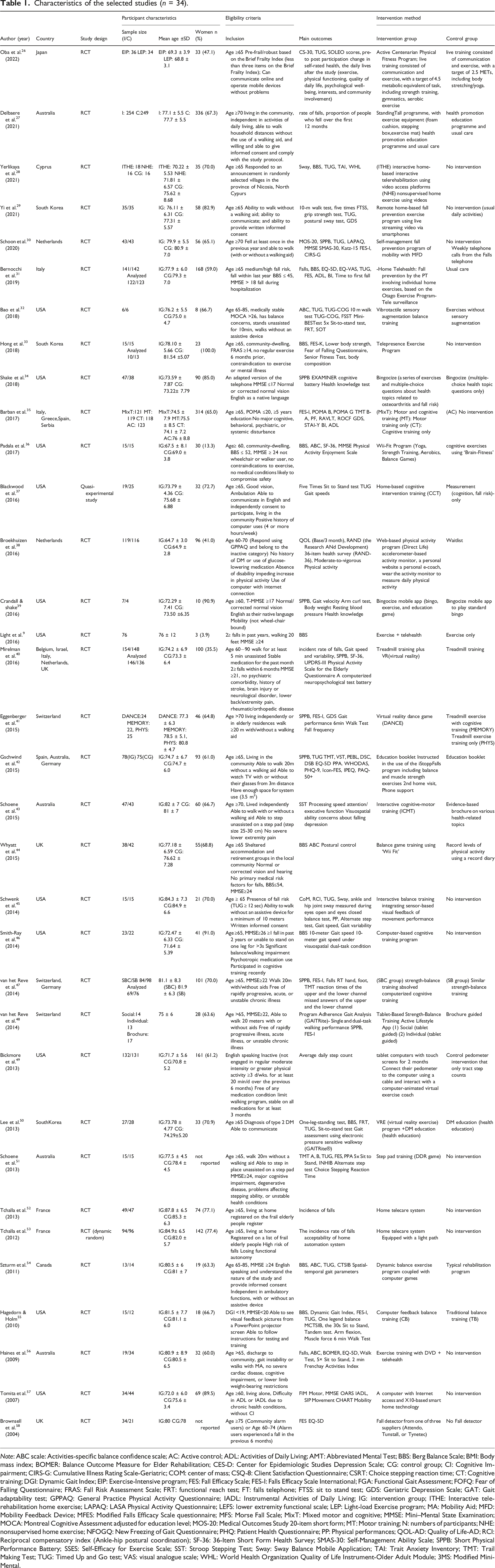
Note: ABC scale: Activities-specific balance confidence scale; AC: Active control; ADL: Activities of Daily Living; AMT: Abbreviated Mental Test; BBS: Berg Balance Scale; BMI: Body mass index; BOMER: Balance Outcome Measure for Elder Rehabilitation; CES-D: Center for Epidemiologic Studies Depression Scale; CG: control group; CI: Cognitive Impairment; CIRS-G: Cumulative Illness Rating Scale-Geriatric; COM: center of mass; CSQ-8: Client Satisfaction Questionnaire; CSRT: Choice stepping reaction time; CT: Cognitive training; DGI: Dynamic Gait Index; EIP: Exercise-Intensive program; FES: Fall Efficacy Scale; FES-I: Falls Efficacy Scale International; FGA: Functional Gait Assessment; FOFQ: Fear of Falling Questionnaire; FRAS: Fall Risk Assessment Scale; FRT: functional reach test; FT: falls telephone; FTSS: sit to stand test; GDS: Geriatric Depression Scale; GAT: Gait adaptability test; GPPAQ: General Practice Physical Activity Questionnaire; IADL: Instrumental Activities of Daily Living; IG: intervention group; ITHE: Interactive telerehabilitation home exercise; LAPAQ: LASA Physical Activity Questionnaire; LEFS: lower extremity functional scale; LEP: Light-load Exercise program; MA: Mobility Aid; MFD: Mobility Feedback Device; MFES: Modified Falls Efficacy Scale questionnaire; MFS: Morse Fall Scale; MixT: Mixed motor and cognitive; MMSE: Mini–Mental State Examination; MOCA: Montreal Cognitive Assessment adjusted for education level; MOS-20: Medical Outcomes Study 20-item short form; MT: Motor training; N: numbers of participants; NHE: nonsupervised home exercise; NFOGQ: New Freezing of Gait Questionnaire; PHQ: Patient Health Questionnaire; PP: Physical performances; QOL-AD: Quality of Life-AD; RCI: Reciprocal compensatory index (Ankle-hip postural coordination); SF-36: 36-Item Short Form Health Survey; SMAS-30: Self-Management Ability Scale; SPPB: Short Physical Performance Battery; SSES: Self-Efficacy for Exercise Scale; SST: Stroop Stepping Test; Sway: Sway Balance Mobile Application; TAI: Trait Anxiety Inventory; TMT: Trail Making Test; TUG: Timed Up and Go test; VAS: visual analogue scale; WHL: World Health Organization Quality of Life Instrument-Older Adult Module; 3MS: Modified Mini-Mental.
ICT components of home-based fall prevention interventions (n = 34).

Note: FIM: Functional Independence Measures; IADL: Instrumental Activities of Daily Living; ITHE: Interactive telerehabilitation home exercise; MFD: the Mobility Feedback Device; MMSE: Mini-Mental State Examination; NHE: nonsupervised home exercise; PPA: Physiological fall risk; QOL: Quality of life; VR: virtual reality.
Quality assessment
Figure 2 depicts the quality assessment results. The Cochrane RoB tool was used to evaluate the 33 RCTs.9,26–36,38–58 The results revealed that seventeen studies9,26–30,32–34,38,40–43,49,51,56 had a low RoB for performance bias. Twenty-six studies9,26–35,38–43,45,47–49,51–54,56 had a low RoB for detection bias. Twenty-four studies26–32,35,36,38,40–43,45,47–50,52–54,56,58 were rated as having a low RoB for attrition bias. Twenty-two studies26–31,33,34,36,38,40,42,43,45,47–51,54,56,57 were rated as having a low RoB for reporting bias. Regarding selection bias, random sequence generation was low in 28 selected studies,9,26–36,38–43,45,47–51,54,55,57,58 and allocation concealment was low in 19 selected studies.26–31,33–36,38–41,43,45,51,54,56 One non-RCT
37
was assessed based on the ROBANS tool, the following risks were low: participant selection, confounding variable, measurement, blinding, incomplete outcome data, and selective outcome reporting. A summary of the results of quality assessment. (A) Risk of bias summary (B) Risk of bias graph.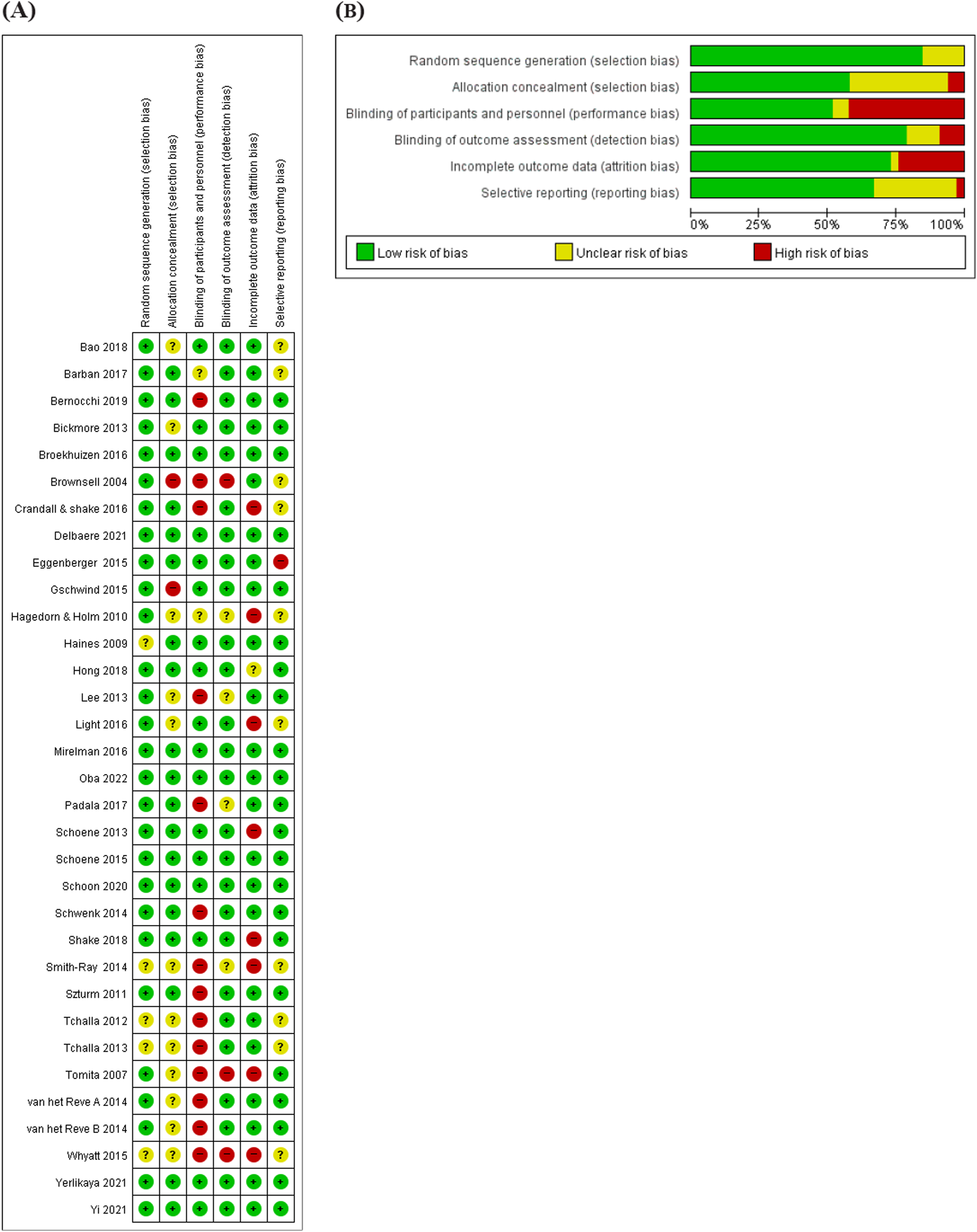
Effect of ICT interventions on fall rates
A summary of the effectiveness of ICT interventions on fall rates.
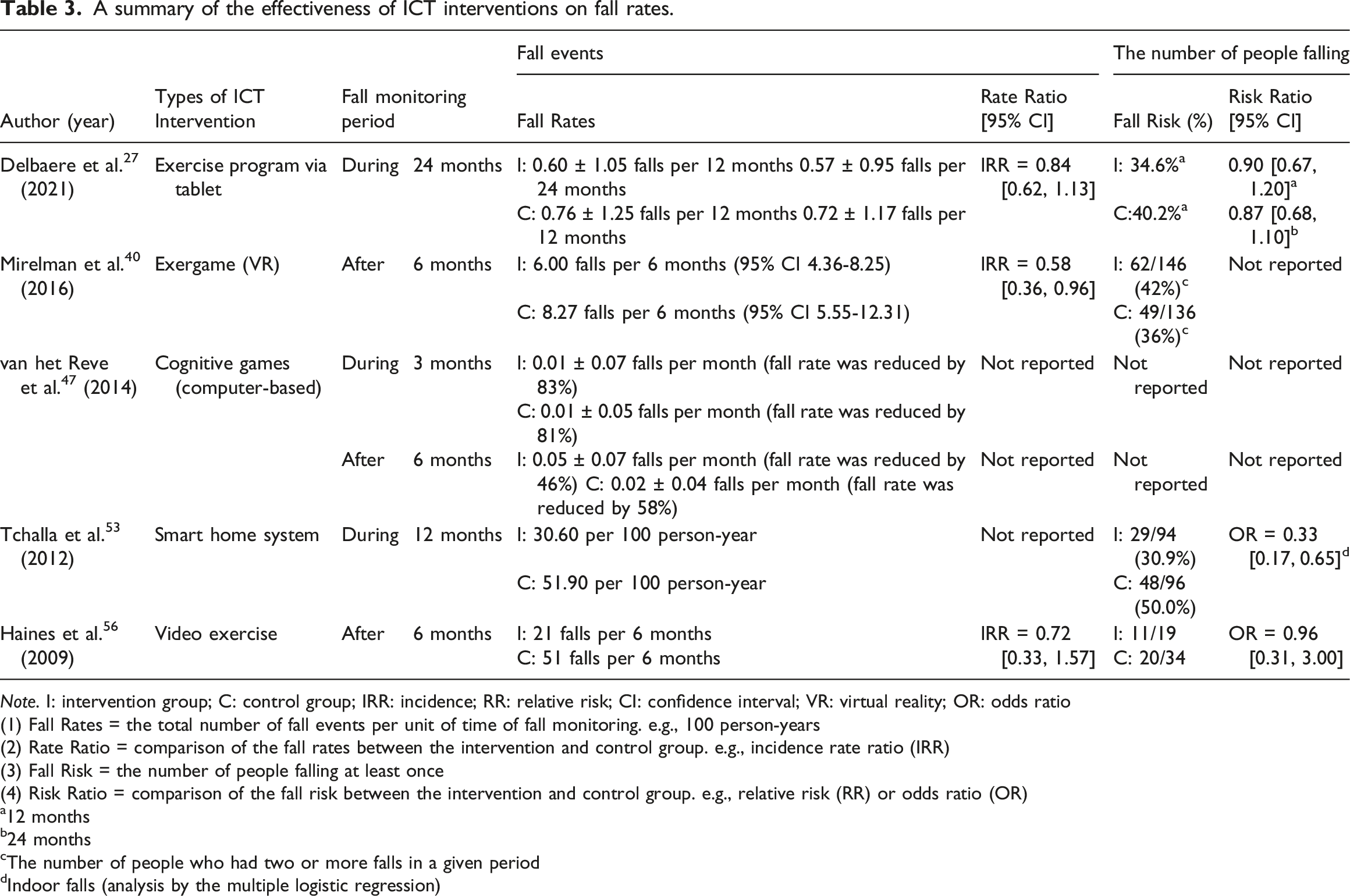
Note. I: intervention group; C: control group; IRR: incidence; RR: relative risk; CI: confidence interval; VR: virtual reality; OR: odds ratio
(1) Fall Rates = the total number of fall events per unit of time of fall monitoring. e.g., 100 person-years
(2) Rate Ratio = comparison of the fall rates between the intervention and control group. e.g., incidence rate ratio (IRR)
(3) Fall Risk = the number of people falling at least once
(4) Risk Ratio = comparison of the fall risk between the intervention and control group. e.g., relative risk (RR) or odds ratio (OR)
a12 months
b24 months
cThe number of people who had two or more falls in a given period
dIndoor falls (analysis by the multiple logistic regression)
Effect of ICT interventions on the proportion of fallers
A meta-analysis was conducted on six studies31,40,47,52,53,56 that examined the proportion of fallers, and a total of 1059 patients were included. A subgroup analysis was conducted to investigate the effect of fall prevention intervention using ICT on the proportion of fallers. In terms of reducing fall risks, ICT interventions reduce the risk of falls (Figure 3(A)). Telehealth (RR = 0.62, 95% CI [0.45, 0.84]), smart home systems (RR = 0.58, 95% CI [0.44, 0.77]), exergames (RR = 0.58, 95% CI [0.36, 0.95]) have also been shown to reduce fall risks. Moreover, a subgroup analysis was conducted according to the performance bias for the proportion of fallers; the performance bias was categorized into high-risk (n = 4)31,47,52,53 and low-risk groups (n = 2),40,56 and the results revealed no unclear risk. There was no significant subgroup difference in RR (Chi2 = 0.35, p = .56). In the group with a high risk of performance bias, the RR was 0.62 (95% CI [0.51, 0.74]), and the RR in the low-risk performance bias group was 0.70 (95% CI [0.47, 1.00]). The RR for the overall proportion of fallers is 0.63 (95% CI [0.54, 0.75]). Meta-analysis of the effects of information and communication technology interventions (A) Proportion of fallers, (B) Balance.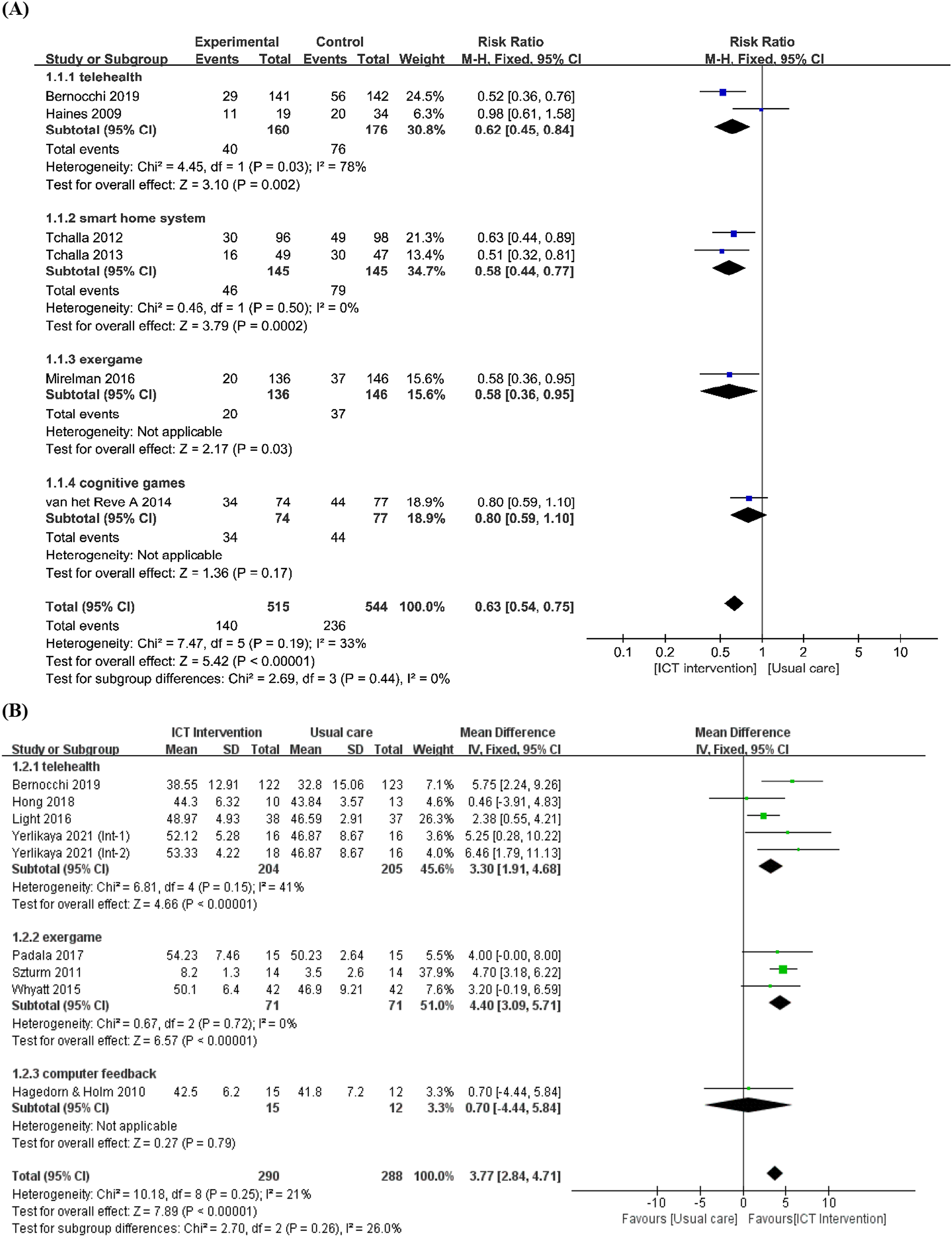
Effect of ICT interventions on balance
Eight studies reported balance measured by the Berg Balance Scale (BBS). 59 The ICT interventions for fall prevention improved BBS scores in the intervention groups (mean difference [MD] = 3.77, 95% CI [2.84, 4,71]). To investigate the effects of ICT interventions on balance by type, a subgroup analysis was performed (Figure 3 (B)) which included telehealth (n = 4),9,28,31,33 exergame (n = 3),36,44,54 and computer feedback (n = 1). 55 Telehealth and exergame improved the balance (MD = 3.30, 95% CI [1.91, 4.68], MD = 4.40, 95% CI [3.09, 5.71], respectively) while computer feedback did not (MD = 0.70, 95% CI [-4.44, 5.84]).
Effect of ICT interventions on physical function
Physical function was assessed using the TUG and SPPB tests. ICT interventions were effective in improving physical function (SMD = 0.37, 95% CI [0.10, 0.64]) (Figure 4(A)). Unlike SPPB scores, higher TUG scores indicated worse physical performance. Thus, a negative value was calculated for the TUG test value to confirm physical function. Meta-analysis of the effects of information and communication technology interventions (A) Physical function, (B) Fall efficacy.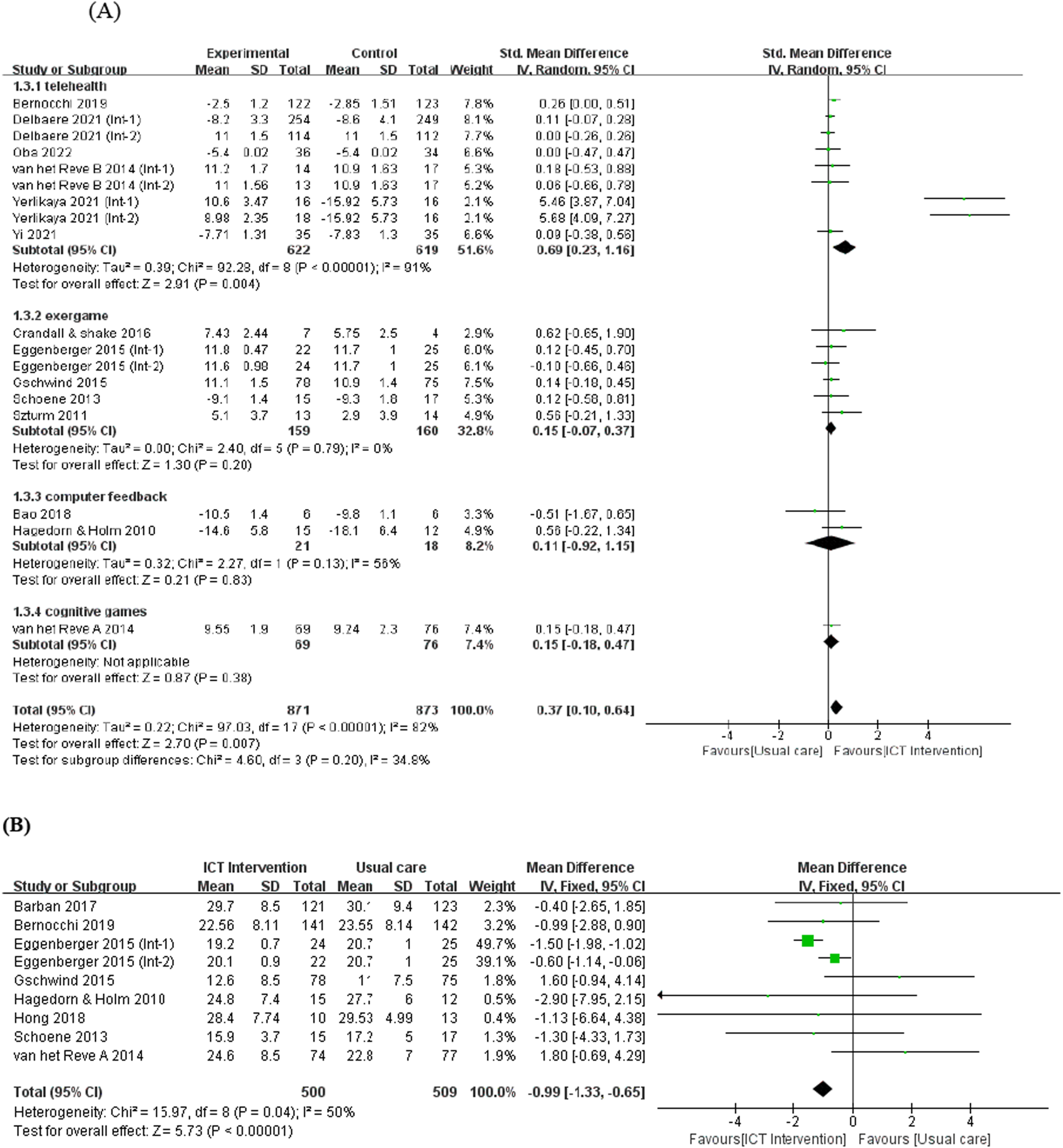
Effect of ICT interventions on fall efficacy
Eight studies used the Fall Efficacy Scale (FES) 60 to determine fall effectiveness. This meta-analysis included 1009 participants (Figure 4(B)). ICT interventions in older adults have shown positive effects on fall prevention (MD = −0.99, 95% CI [−1.33, −0.65]). A higher FES score indicates a stronger fear of falling, 60 suggesting that reducing the FES score in the intervention group was effective in enhancing their confidence in preventing falls.
Effect of ICT interventions on quality of life
Four studies with 954 participants reported post-intervention quality of life measured by the EuroQol-5 Dimension (EQ-5D) or EuroQol Visual Analog Scale (EQ-VAS). 61 The ICT interventions on quality of life, measured by EQ-5D have been shown to be ineffective (MD = 0.03, 95% CI [-0.03, 0.09]) while ICT intervention measured through EQ-VAS have been shown effective (MD = 5.84, 95% CI [1.32, 10.37]). (Appendixes 2A and B).
Effect of ICT interventions on cognitive function
Three studies27,42,47 identified the effects of ICT interventions on cognitive function using Trail Making Tests (TMT) A and B. 62 The TMT evaluates visual search, scanning, processing speed, mental flexibility, and executive skills. 63 Cognitive function assessed using either TMT A or TMA B was not shown to be effective (MD = −4.56, 95% CI [−14.49, 5.36], MD = 2.70, 95% CI [−5.62, 11.02], respectively) (Appendix 3).
Discussion
To assess the effectiveness of fall prevention interventions for older adults in the community using ICT, we focused more on fall prevention interventions using the most recent types of ICT (e.g., telehealth, computerized balance training, exergaming, mobile application education, or virtual reality exercises) and excluded studies where interventions were conducted simply by telephone interviews or home visits. This study found that ICT interventions, including telehealth or smart home systems, can be effective in reducing the proportion of fallers and improving balance, while the effect of cognitive games and computer feedback on balance remains unclear. In addition, board-type exergames can be effective in reducing falls among the various types of exergames. Finally, community-based non-face-to-face fall prevention interventions improved physical functions and reduced the fear of falling in older adults.
Effects on fall risk and balance by intervention types
Our review found that telehealth interventions for older adults significantly reduced the number of fallers and improved their balance. Consistent with our study, a recent systematic review in community-dwelling adults with neurological conditions found that telehealth interventions significantly improved balance outcomes. 64 A systematic review 8 found that combined intervention including telehealth and balance-related exercises reduced the proportion of fallers. When considering intervention adherence, telehealth might have disadvantages as intervention adherence rates tend to decrease over time. 64 However, ICT interventions, which enhance intervention adherence, can mitigate the disadvantages of telehealth as a non-face-to-face intervention. Thus, in older adults, incorporating balance exercises into ICT interventions is crucial to prevent falls and achieve positive outcomes in the future.
Smart home devices lowered the number of falls among older persons in our review. The combination of a light path and teleassistance decreased falls at home in the frail senior group. Consistent with our findings, a systematic review 65 demonstrated that smart homes and health monitoring systems provide clinical advantages by 66.66% over no intervention or alternative forms of intervention. By using automated assistance, smart home systems can enhance the comfort of older adults without disrupting their usual way of life. 66 Other studies have also demonstrated that smart home systems play a crucial role in promoting the safety and well-being of older individuals, enabling them to spend more time in familiar environments.67,68 Therefore, the appropriate use of smart home systems, in conjunction with exercise, can be one intervention option for fall prevention in older adults.
Our study found that fall prevention interventions using exergames reduced the number of fallers and improved their balance. Consistent with our findings, other systematic reviews also indicate that exergame-assisted rehabilitation was effective in reducing the incidence of falls, 69 and improving functional balance in older adults. 70 Contrastingly, one study 71 demonstrated statistically nonsignificant improvement in the balance following a 3-week exergame intervention. Furthermore, another systematic review 8 reported that exergames exhibited no significant effect, while telehealth and exercise interventions led to improvements in balance. This inconsistency can be explained that among various types of exergames, board-based exercises were effective in reducing falls in our review. Balance exercises (e.g., balance training, resistance, and aerobic exercises) and board training (e.g., Wii Fit training) have been proven to be effective in increasing the balance ability of older adults. 72 As the adherence of older adults to conventional physical exercise programs is poor, interventions using exergame technology have been developing rapidly. 73 Although the positive effects of exercise are well known, only 30% of older adults exercise regularly. 74 Therefore, we suggest that exergames can be a good option for ICT fall prevention interventions in older adults. This approach is not only clinically important for achieving positive outcomes, but it is also helpful in promoting exercise adherence. Moreover, since most exergames are targeted towards younger generations, developing older adult-friendly exergames that enhance usability for older adults 75 may be beneficial for promoting older adults’ health.
The effect of computer feedback on balance was unclear in our meta-analysis. However, the analysis was based on only one study. While the group that received computer feedback balance training showed better balance improvement than that of the group that received traditional balance training, the differences were not statistically significant, highlighting the need for further research. Utilizing virtual reality or machine-based approaches for balance training offers a more diverse and engaging exercise experience compared to that associated with conventional balance training. Further research is needed to validate their effectiveness in improving balance ability.
We found that cognitive games did not significantly reduce the proportion of falls or improve balance. Nevertheless, interactive cognitive-motor interventions can help older adults enhance physical and cognitive functions. 76 As the causes of falls are multidimensional, including both physical and cognitive factors, cognitive interventions are necessary to prevent falls. Cognitively impaired older adults have a significantly increased risk of falling, at least twice that associated with their cognitively normal counterparts. 76 Although the exact mechanisms by which people with cognitive impairment are more likely to fall are not fully understood, reduced cognitive function may result in decreased attentional resource allocation while walking. 77 A meta-analysis 8 that included a study 46 that used the Posit Science program, which is a balance-related cognitive game, reported no significant effect on balance. However, the included study 77 identified a positive effect on small sample size, suggesting low statistical power. Therefore, future studies, such as large-scale RCTs including cognitive game interventions for fall prevention, are warranted.
Effects on physical function
In our meta-analysis, individual studies used different instruments (i.e., TUG and SPPB) to evaluate physical function. Videoconferencing exercise is reportedly effective in improving physical function among patients with chronic diseases. 78 A review study 75 also revealed that Wii exergames had a positive impact on physical function improvement. However, another meta-analysis 70 found that the use of Wii Fit exercise did not show significant improvement in muscle strength. We suggest further large-scale studies to examine the effectiveness of ICT fall prevention interventions on physical function.
Effect on fall efficacy
Our review indicates that ICT interventions for fall prevention among older adults in the community may have a positive impact on fall efficacy, or in reducing concerns about falling. This finding is consistent with the results of the most recent systematic review. 8 The FES-I evaluates concern on falling. 79 One of the most significant consequences of the fear of falling is avoiding activities that can severely influence physical ability over time. 80 Sedentary behavior in older adults results in decreased mobility and balance, which might lead to a tendency to fall or fear of falling. 81 Fear of falling may increase one’s chance of falling, and apprehensive older adults commonly avoid mobility tasks, such as reaching and walking. 80
Effect on quality of life
In our review, ICT fall prevention interventions showed improved quality of life outcomes when measured with EQ-VAS; however, when measured with EQ-5D, they did not show an improvement in the overall quality of life. Consistent with our study, a systematic review 66 in older adults with chronic conditions found that telemonitoring did not confer significant improvement on their quality of life. Future studies should consider health-related quality of life needs as an outcome measure because it includes multiple aspects of a healthy life measuring functionality and well-being in physical, psychological, and social domains.82,83
Limitations
Our study was an updated meta-analysis that assesses the effectiveness of ICT interventions (e.g., telehealth, computerized balance training, exergaming, mobile application education, or virtual reality exercises). Moreover, we performed a subgroup analysis according to the type of intervention to identify the best interventions. However, our study had several limitations. First, the included studies had small sample sizes. Further studies with larger sample sizes are required to enhance the level of evidence. Second, conducting a meta-analysis of falls was challenging as the intervention contents could not be easily standardized. Third, due to the variety of study types and the number of samples, comparative analysis according to intervention type was also difficult. Finally, studies that include the assessment of intervention duration and session time are required to confirm the effectiveness of fall prevention interventions using ICT for older adults. Most studies included the motivational benefits of ICT in encouraging older adults to exercise. Compliance may be increased by using interventions that entertain and motivate. However, such novel ICT interventions often tend to decrease motivation effects with time. Thus, one has to be cautious when generalizing the results of the short-term ICT intervention.
Clinical implications
Fall prevention interventions using ICT is critical for the health and well-being of older adults and helps in decreasing the social and economic burden. In the midst of COVID-19 pandemic, to prevent falls of community-dwelling older adults, ICT interventions are preferred more considering social factors, increasing access to healthcare and reducing costs to prevent falls. Providing a safe environment with a smart home system can be an important factor in preventing falls in older people. Since improving balance function is an important factor in reducing falls in older adults, it is important to increase interest by using telehealth or exergames to encourage older people to improve their balance and exercise independently. The completion of non-face-to-face interventions decreases over time. Therefore, using telehealth is necessary to increase the implementation of non-face-to-face fall prevention measures in older people. The assessment of fall prevention interventions utilizing ICT may facilitate the development and implementation of fall prevention strategies.
Conclusions
ICT fall prevention interventions, including telehealth or smart home systems, have a positive effect in reducing the risk of falls and improving balance. Moreover, exergames may be used to reduce falls among community-dwelling older adults and be a way for older people to exercise and stay active in an interesting way. Additionally, ICT fall prevention interventions have a positive effect on improving fall efficacy. It is meaningful that ICT interventions have potential applicability during pandemics or in situations where face-to-face interventions are difficult to implement. The most optimal ICT interventions for fall prevention should be used. However, they did not improve individuals’ quality of life and cognitive functions. Future investigations on telehealth, smart home systems, or exergames are needed to motivate older adults to exercise, prevent falls, and improve their quality of life.
Supplemental Material
Supplemental Material - Effects of community-based fall prevention interventions for older adults using information and communication technology: A systematic review and meta-analysis
Supplemental Material for Effects of community-based fall prevention interventions for older adults using information and communication technology: A systematic review and meta-analysis by Kayoung Lee, Jungeun Yi, and Seon Heui Lee in Health Informatics Journal.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financed in part by a grant from the Korea Health Technology R & D Project, administered by the Korea Health Industry Development Institute (KHIDI), and funded by the Republic of Korea’s Ministry of Health and Welfare (grant number: HI21C0575).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.