
Abstract
Several studies have investigated challenges that have marred success or even caused the failure of eHealth implementations in Uganda; however, none has focused on the risks and success factors of their sustainability. This study explored critical risk and success factors for the sustainability of an electronic health data capture, processing and dissemination platform for Uganda. A mixed-method research design was followed involving collecting empirical data from all four regions of Uganda. A purposive sampling strategy was used to select the study districts per region, health facilities per district, and respondents/participants per facility or district. Findings revealed several risks and success factors for sustainability, including; bad leadership, corruption, lack of sustainable maintenance programs, lack of suitable sustainability plans, lack of ICT infrastructure investment, poor management systems, funds, stakeholder buy-ins, data sharing and access rights. The success factors included reinvestments as a partial sustainability plan for ICT infrastructure. These factors can be leveraged to ensure the continued operation of eHealth implementations in Uganda. Every electronic health project aiming at success should always make due consideration/sustainability plan at the onset of project conceptualisation; as lack of such a plan has often resulted in failed projects after the initial funds have been withdrawn.
Introduction
eHealth became an essential component of the World Health Organisation (WHO) initiative to enable Universal Health Coverage. 1 Whereas in high-income countries, ICT is transitioning from solely supporting efficiency in recording and transferring health information between providers to near real-time surveillance for faster identification of public health problem 2 and sophisticated decision support in healthcare settings based on sophisticated artificial intelligence (AI) algorithms;3–8 low and middle-income countries continue to struggle even with an efficient recording of health data. Yet the UN document 9 highlights ICT as a key enabler of economic development and wellness globally, emphasising that the utility of health ICT is not just for high-income settings.
While most eHealth systems implementations have focused on patient flow, decision support and personalised medicine, it may also have significant application to population-level care and treatment, particularly in resource-limited settings requiring electronic capture and near real-time processing of health data. To achieve near real-time data capture and processing, nation-wide eHealth systems would require a minimum of; reliable ICT infrastructure to support security, data transfer, and automated analyses; workforce to support the ICT infrastructure; high-level of governmental, non-governmental organisation and service provider coordination and regulation; policies and procedures to support operation; community acceptance for health data usage; and front-line care provider engagement, training and cooperation in recording data. Nationally, Uganda has begun to advance their ICT capacity for health systems delivery.
The Uganda Ministry of Health (MoH) recognised the value of eHealth and implemented a strategy to realise a national vision of eHealth adoption. 10 Furthermore, to reap the benefits of eHealth, Uganda’s MoH has permitted several eHealth initiatives/interventions for data capture to be implemented. In fact, several different eHealth data capture systems within Uganda are predominately based on proof-of-concept pilot projects with partner organisations and capture data retrospectively.10,11 Most of them have been donor-funded, eventually dying off when the donor funds cease.
Only a few studies have looked at the cost of return of electronic health records (EHRs), but these primarily focus on financial recovery through billing, which does not reflect Uganda’s setting12,13 and not the broad concept of sustainability. Further, a body of Literature focuses on eHealth readiness and technology adoption.14–20 In addition, though few focus on the EHR adoption in low-income settings, 18 implementation success has been reported by contributing factors outside of theoretical frameworks in low and middle-income country (LMIC) settings. 21 Finally, studies that have investigated challenges that cause eHealth interventions’ failure to scale over have not focused on risks and success factors of sustainability.
Notwithstanding the definition22,23 sustainability focuses on resource flows with the aim of the project’s continued viability beyond the initial funding period and prevents burdening of the beneficiaries. However, any lack of sustainability of eHealth interventions implementations will prevent improvements in quality, efficiency, and equity outcomes, defeating potential benefits and the ultimate goal to improve care quality through information technology. 24
Literature presents five dimensions of sustainability; 25 several factors influence these dimensions in the healthcare domain, including poor infrastructure, inappropriate approach to systems development, inappropriate donor policies and strategies, uncoordinated donor efforts, and inadequate human resource capacity; some of which are risk factors that threaten the long-term viability of eHealth systems after the withdrawal of external support. 26 In fact, studies have shown that healthcare interventions in LMICs continue to face challenges, some of which have to do with a lack of sustainability; hence most eHealth interventions/projects close after the pilot stage. 27
To avert the trend in LMICs and particularly for Uganda, there is a need to know what can be a threat to and what is possible for the sustainability of an eHealth data capture and processing platform. Therefore, this study sought to understand the risk factors that would hinder the sustainability of an eHealth data capture and processing platform for Uganda and how to mitigate them in terms of critical success factors.
Methodology
Study design and population
We adopted a mixed-method (qualitative and quantitative) research design. The study was conducted across districts in four regions of Uganda, namely; Northern, Eastern, Western and Central. The study population included the general public and Community Health Workers/Village Health Teams (CHEWs/VHTs) for focus group discussions (FGDs); health Partners and NGO Partners, and government officials who work in a health-related capacity as well as representatives of commercial ICT for key informant interviews (KIIs); health researchers from Uganda universities and beyond, and healthcare providers across Uganda as informants.
Sampling
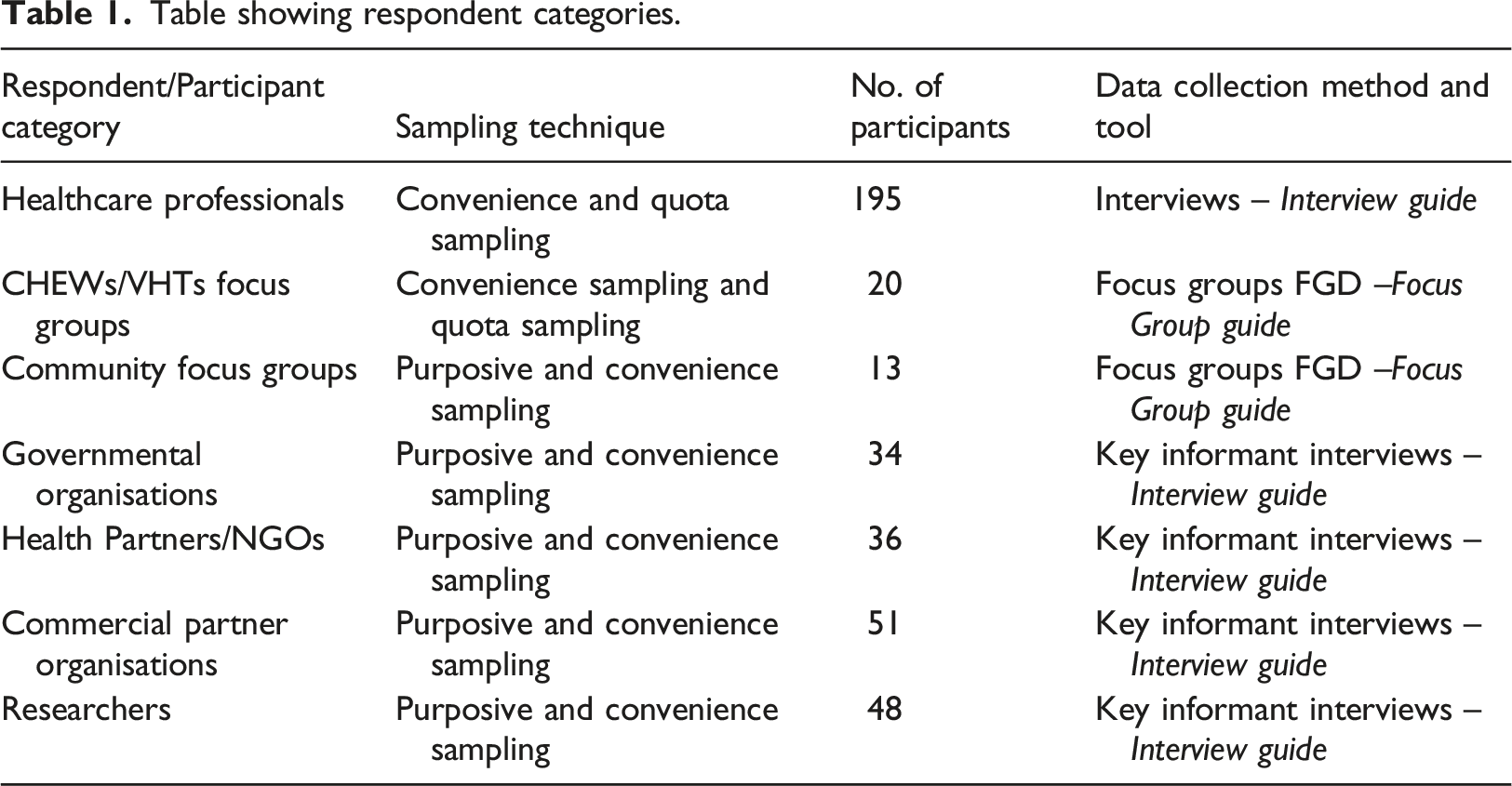
Table showing respondent categories.
Data collection
Data collection techniques involved interviews and focus group discussions using interview guides and FGD guides, respectively (see Table 1). 195 healthcare professionals from 200 different healthcare facilities attended qualitative interviews. Interviews were conducted until saturation. Semi-structured questions were used to allow for flexibility to elicit credible responses regarding risks and success factors for sustainability for a point-of-care platform. The construction of these questions was informed by three technology adoption theories, i.e., Technology-Organisation-Environment (TOE) Framework, 14 Diffusion of Innovation (DOI) Theory, 28 and Technology Acceptance Model (TAM). 29
20 Ad hoc FGDs were conducted with CHEWs/VHT members. For the general public, a total of 13 formal FGDs, each comprising 8–10 participants, were conducted, representing 01 FGD in each of the 13 districts identified. KIIs were held for participants drawn from governmental organisations (34), health partners/NGOs (36), commercial partner organisations (51), and health researchers (48).
Study investigators and research assistants collected the data. However, research assistants first undertook training on ethics in data collection and handling, and how to use the data collection instruments (interview guide and focus group guide). The recordings were uploaded on a shared google drive for transcription, as well as investigators to validate the transcriptions, a process where a member of the research team listens to a recording while reading the transcripts.
Data analysis and information synthesis
The study identified emerging issues by triangulating information from all the data sources and using the thematic analysis procedure. Thematic analysis was preferred because of its flexibility. 30 First, the transcripts were loaded into NVivo 12 and then coded to create the themes. We used NVivo because it facilitates researchers to code and synthesise 31 collaboratively. Coding of the transcripts supported members of the analysis team in identifying emerging themes, that eventually formed the main themes regarding risk and sustainability factors of an electronic health data capture, processing and dissemination platform for Uganda. Three research team members individually identified codes from a small data set. Then they discussed the codes to agree on a final set that was used to code the whole data set. Consensus was sought where they differed in coding a theme. The coded themes were revised to form high-level themes.
Ethical considerations
Permission to conduct the study was approved by Uganda National Council for Science and Technology. While this study held no personally sensitive information, confidentiality was considered important. Therefore, all participants completed an informed consent form before participating in the study. Additionally, participants were coded.
Results
Demographics
The study participants represented views from the health facilities, government, and healthcare organisations. In all, 195 valid responses were received on the questionnaires, 33 in FGDs, and 169 in the interviews. Most of the participants were healthcare professionals from health facilities who responded to the questionnaires (49%). Additionally, 5% were CHEWs/VHTs FGDs, 3% were community FGDs, 9% were government organisations, 9% were Health Partners/NGOs, 13% were Commercial Partner organisations, and 12% were researchers (Figure 1). Respondents distributed by Health Facility, Government or Organization.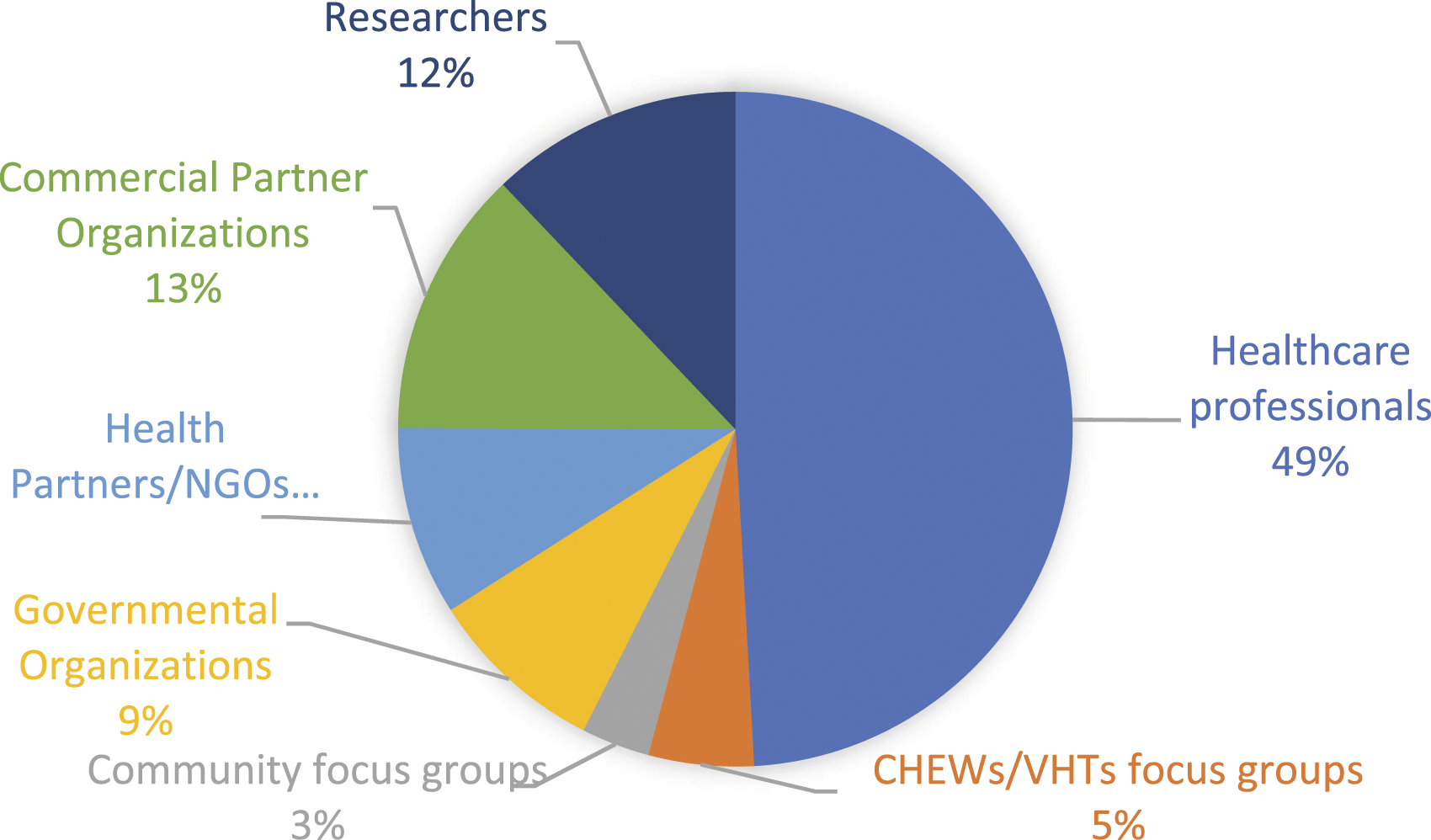
Risk and success factors for sustainability of an eHealth data capture and processing platform
This study focused on exploring the technological, financial, institutional, and environmental factors of sustainability that relate to implementing and maintaining an eHealth data capture and processing platform for Uganda. Study participants’ views of sustainability included … “extending beyond project implementation to include how the platform will remain functional and require resources” (GC_04, Health Partner/NGOs); “Sustainability depends on people managing the system and the structure being set because not every system being developed has a future of running” (GC_02, Health Partner/NGOs).
Risk factors to sustainability
Risk factors for the sustainability of an eHealth data capture, processing and dissemination platform for Uganda.
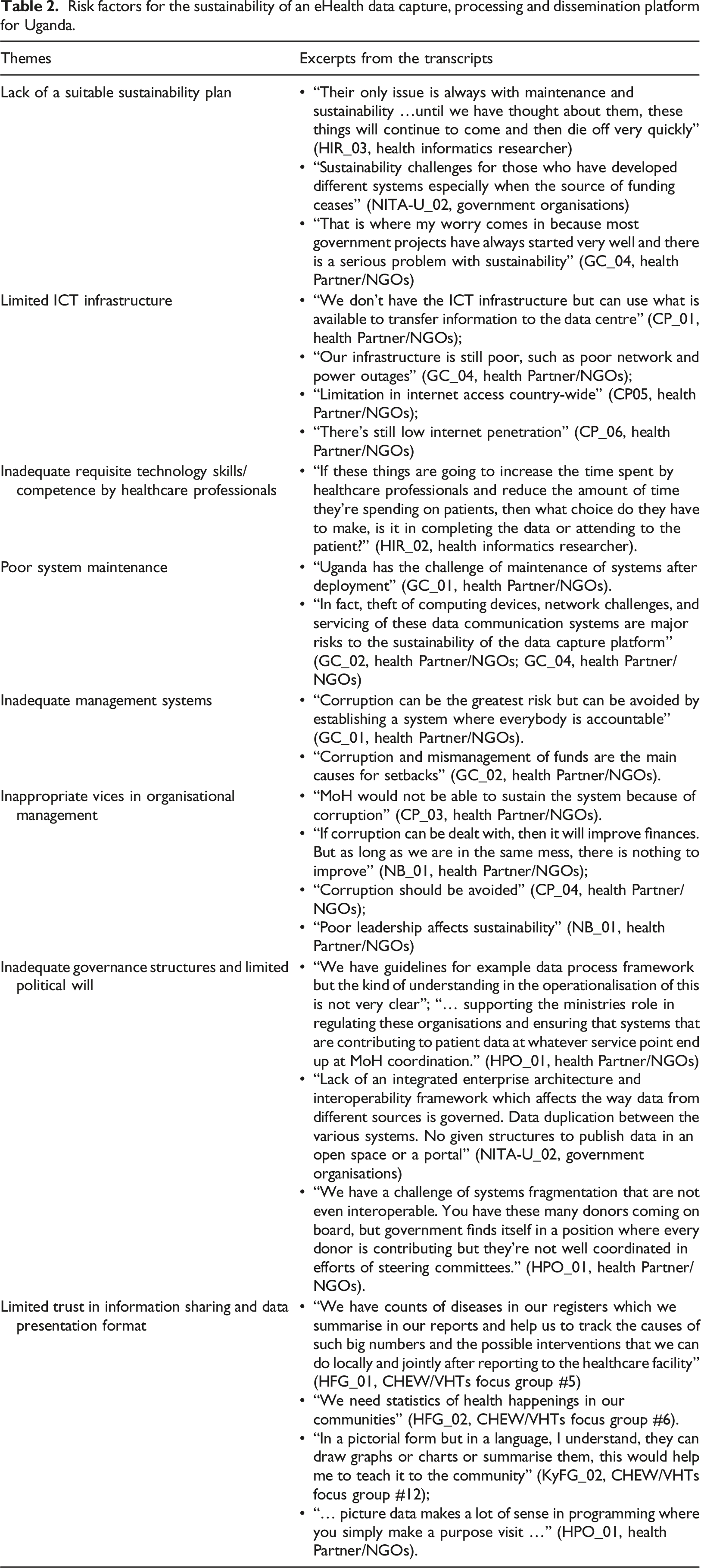
The lack of a sustainability plan affects the smooth transition from the Implementing Partners who initially support such healthcare interventions to facility governance and/or continued system financing. The challenges have caused slowing down of systems performance and eventual closure after funding is withdrawn/stopped. Its effects are evident when funding ceases (NITA-U_02, Government Organisations), showing off in poor maintenance of existing system components, limited to no addition of ICT devices, network/connectivity failures, and failed use. A participant recommended a sustainability plan to include training of health personnel on how to use the system, strict laws/policies/SOPs on use, and sensitisation of stakeholders on the values of the system (GC_04, Health Partner/NGOs).
Concerning the ICT infrastructure, limitation of the infrastructure components such as intermittent Internet connectivity and slow end-user devices would decrease the feasibility of implementing such a platform in Uganda. Availability of the Internet will affect how readily the collected data is uploaded to the shared platform, and hence a factor of near real-time that the system intends to achieve. Several respondents alluded to the fact that there is a considerable lack of ICT infrastructure to support electronic data capture, processing and presentation (CP_01, Health Partner/NGOs; GC_04, Health Partner/NGOs; CP_06, Health Partner/NGOs). Despite improvements in ICT infrastructure like the extension of the internet backbone, the Internet remains a challenge in hard-to-reach health facilities in rural areas (GC_05, Health Partner/NGOs).
Healthcare professionals, the main users of such eHealth data capture and dissemination platform, often have to decide whether to spend more time serving patients/clients or meet the eHealth system’s requirements. The inadequate technology use and skills/competence among health care professionals present them with such unusual choices, causing them to decide between spending time in health data capture and serving the patient (HIR_02, Health Informatics Researcher). To avert the human resources limitations, participants suggested training of staff on ICT and use of such platforms should continue, more healthcare professionals with required ICT skills be recruited, and employment of ICT knowledge persons, maintain and manage the system (KTC_02, Health Partner/NGOs), and create in them positive attitudes towards ICT projects for health (GC_05, Health Partner/NGOs).
When management of an eHealth implementation switches from the implementing partners and funder support to facility level/government management, even the system maintenance deteriorates. Several focus groups indicated that Uganda has a challenge in maintaining eHealth systems often evidenced by loss of computing devices, poor servicing, downtime of the communication networks among others (GC_02, Health Partner/NGOs; GC_04, Health Partner/NGOs). Part of the maintenance challenges is a case of inadequate management systems. The lack of inbuilt checks and balances for the long-term impact and sustainability of the electronic data capture and dissemination platform for Uganda.
Negative organisational/managerial vices often hamper Uganda’s deployment, use, and maintenance of ICT interventions. For example, some participants mentioned corruption as a vice that may hamper Uganda’s implementation and proper maintenance of the eHealth data capture platform (CP_03, Health Partner/NGOs). However, some believe that finding a solution to corrupt tendencies in system implementation and leadership problems will facilitate the success and sustainability of the platform in Uganda (NB_01, Health Partner/NGOs; CP_04, Health Partner/NGOs).
In fact, improper management of eHealth systems and negative organisational attitudes can be attributed to the problem of inadequate governance structures and limited political will to develop, implement and manage a common eHealth data capture platform for Uganda. MoH does not have approved and documented operating procedures to govern eHealth data access. Existing frameworks, like the data access framework, are not clear enough to be operationalised (HPO_01, Health Partner/NGOs). There seems to be a political gap where fewer resources are allocated to MoH who should regulate eHealth operations in Uganda including development partners leading to uncoordinated donor support. Besides, there is lack of an integrated enterprise architecture and interoperability framework affecting the way data from different sources is governed (NITA-U_02, Government Organisations). The uncoordinated efforts have caused lack of interoperability between the multiple eHealth implementations in Uganda (HPO_01, Health Partner/NGOs).
Finally, there is limited trust in information sharing and data presentation format among eHealth users. Participants, especially VHTs raised concerns on utility of collected data to them and patients, i.e., there was only an upward flow of information. Views from FGDs and KIIs emphasise the need for the lower-level health system stakeholders to get feedback from health managers regards aggregated data that is vertically shared with them (HFG_01, CHEW/VHTs Focus Group #5; HFG_02, CHEW/VHTs Focus Group #6). Stakeholders at all health system levels need to appreciate and trust the usefulness of the data collected to continue using/supporting such an eHealth system. Dissatisfaction with data usefulness will often lead to its discontinuation. Additionally, participants were not satisfied with the presentation format and details that are availed whenever such information is shared. They indicated their preference for pictorial formats, pie charts, and simple and concise words (KyFG_02, CHEW/VHTs Focus Group #12; HPO_01, Health Partner/NGOs).
Critical success factors for sustainability
This study’s consideration of the critical success factors for implementing an eHealth data capture, processing and dissemination platform for Uganda was constructed on the premise that meeting them would result into meaningful value and positive outcomes for the country. Critical success factors are of two dimensions; what needs to be, and what already exists to facilitate such implementation.
Critical success factors for sustainability of eHealth data capture, processing and dissemination platform for Uganda.
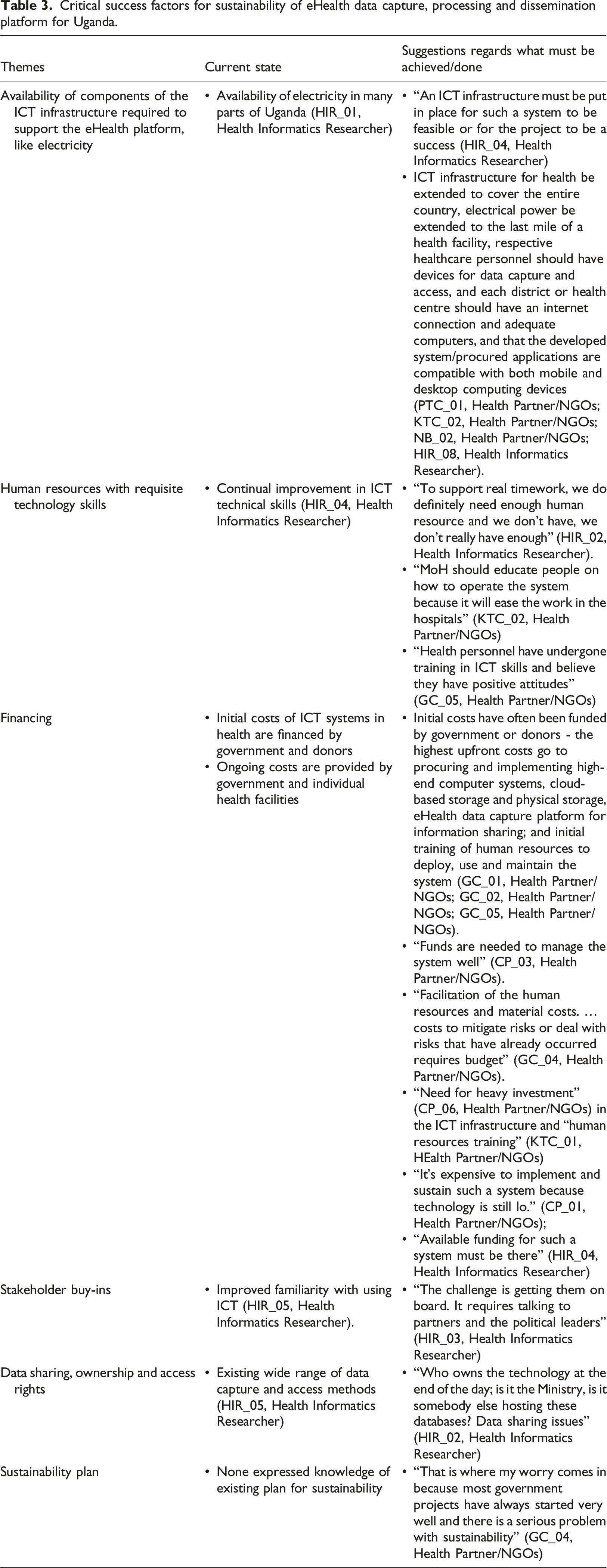
Participants suggested that ICT infrastructure for health be extended to cover the entire country, electrical power be extended to the last mile of a health facility, respective healthcare personnel should have devices for data capture and access, and each district or health centre should have an internet connection and adequate computers, and that the developed system/procured applications are compatible with both mobile and desktop computing devices (PTC_01, KTC_02, Health Partner/NGOs; NB_02, Health Partner/NGOs; HIR_08, Health Informatics Researcher). If these infrastructural recommendations are operationalised in addition to a well-laid plan for continued improvement and maintenance, these will ensure sustainable eHealth data capture platform implementation for Uganda.
Of course, the existence of a robust ICT infrastructure alone without requite human resources is inadequate. There is a need for the necessary workforce to develop, implement, use and maintain the system (HIR_02, Health Informatics Researcher). Additionally, there is a need to train people who will manage and use the eHealth data capture platform (HIR_08, Health Informatics Researcher). The availability of skilled human resources is an enabler of successful health data capture platform implementation.
Overall, CP_06 (Health Partner) argued for heavy investment in the ICT infrastructure to support sustainable implementation and maintenance of the eHealth data capture platform. On the other hand, KTC_01 (Health Partner) encourages training and development of requisite human resources to use the system.
Finance is key in every project and cannot be isolated (GC_03, Health Partner/NGOs; GC_04, Health Partner/NGOs). Mobilising adequate funds to sustain the project can be a challenge that may require lobbying for financial support from donors to supplement government resources (GC_05, Health Partner/NGOs). Figure 2 shows the number of respondents from commercial organisations who indicated cost implications for the eHealth data capture platform. Cost Implications for the eHealth Data Capture and Processing Platform.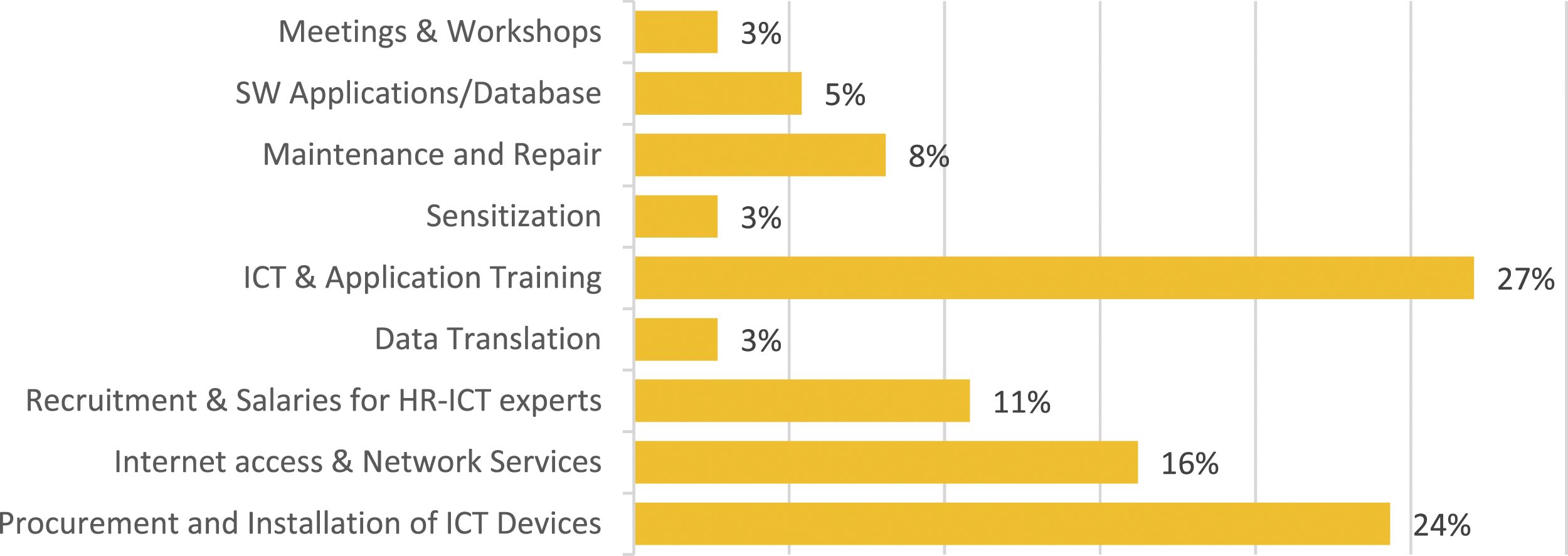
From Figure 2, 27% and 24% of project costs go to healthcare professionals' training to use ICT, procurement and installation of ICT devices; followed by internet access and network services costs (16%), recruitment and salaries for ICT human resources cost (11%), maintenance and repair of the computing devices and network cost (8%), software applications (5%), and data translation, sensitisation and meetings/workshops costs (each 3%). These costs are grouped into initial/upfront and ongoing/maintenance costs;
Initial/Upfront costs
The highest upfront costs go to procuring and implementing high-end computer systems, cloud-based storage and physical storage, eHealth data capture platform for information sharing; and initial training of human resources to deploy, use and maintain the system (GC_01, Health Partner/NGOs; GC_02, Health Partner/NGOs, GC_05, Health Partner/NGOs).
Ongoing costs
Several ongoing costs include; network servicing, ICT staff salaries, ongoing training, maintenance and repair, software updates, and meetings/workshops. Additional running costs include the cost of maintaining human resources to man the system, cost of consumable ICT materials (subscription like Internet service, printing materials, etc), costs to mitigate risks or deal with risks to ICT (GC_04, Health Partner/NGOs).
It should be acknowledged that it is expensive to implement and maintain an eHealth system (CP_01, Health Partner/NGOs); therefore, funding must be available to ensure its continuity (HIR_04, Health Informatics Researcher). However, limited funds decrease the feasibility of system implementation. Actually, funding is on top of the list of factors that facilitate the sustainable implementation of the eHealth data capture platform (HIR_02, Health Informatics researcher). eHealth system implementers like the government require finances to run the project (GC_02, Health Partner/NGOs). Generally, achieving realistic costs for implementing and continued platform sustainability is based on proper planning and execution of the plans (GC_01, Health Partner/NGOs; GC_03, Health Partner/NGOs).
Besides soliciting funds, eHealth system implementers should ensure that there is stakeholder buy-in. Usually, it isn’t easy to get stakeholders to adopt a new system. Adoption is often characterised by a slow process of buy-ins followed by adoption ... “the challenge is getting them on board. It requires talking to partners and the political leaders” (HIR_03, Health Informatics Researcher). Moreover, stakeholders have to be convinced about the importance of the system and often require training on how to use the system. Improved stakeholder engagement/involvement in the system design process enables them to understand the system better and appreciate its relevance in supporting healthcare. Finally, wide stakeholder buy-in will guarantee management’s willingness to fund the system and the user’s acceptance to continue using it.
Trust in the data shared, owned and right to access it. Fears of data sharing and ownership and access control rights decrease the system’s adoption and implementation feasibility. The study participants expressed concerns about ownership of the technology that holds data and data sharing issues (HIR_02, Health Informatics Researcher). Health data ownership, access and use in Uganda should be stipulated to avert these fears.
Reinvestments as a partial sustainability plan for ICT Infrastructure.
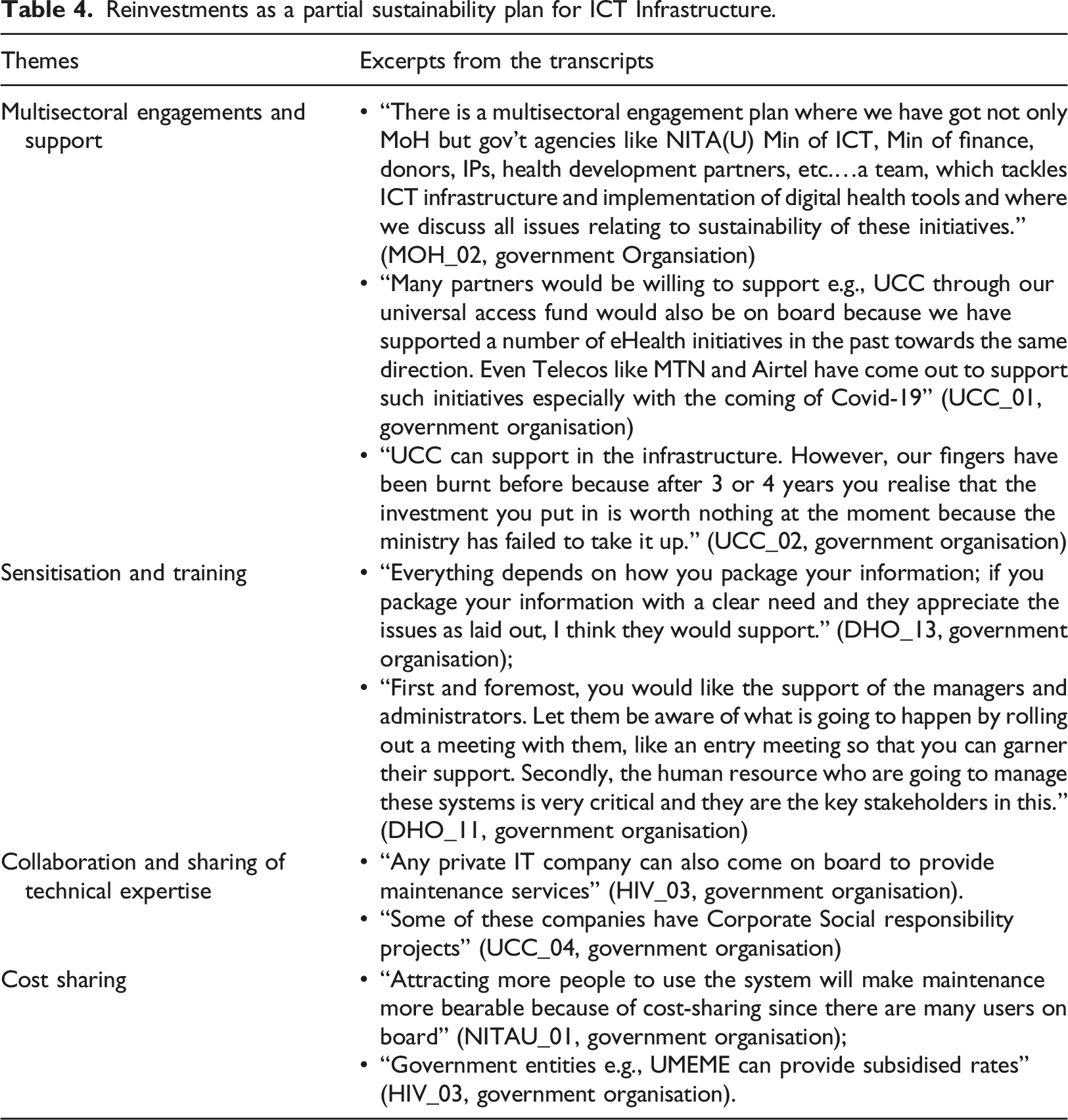
Participants suggested different government ministries, departments and authorities to engage with each other to ensure each plays their roles in supporting a sustainable eHealth data capture platform implementation for Uganda (MOH_02, Government Organisation; UCC_01, Government Organisation). However, there were participants who expressed views on failure of some of the sectors to take responsibility, which in turn affect willingness of other sectors to continue providing support (UCC_02, Government Organisation).
Participants also claim that the platform’s sustainability will also depend on the healthcare workforce’s appreciation and use of knowledge. Investments led by knowledgeable personnel who appreciate the project may receive the best effort and attention that may maintain it for the planned period of investment (DHO_13, Government Organisation; DHO_11, Government Organisation). In addition, existing training programmes for health professionals, IT service providers, and software suppliers have provisions for the training of users that can be leveraged to equip potential users of such an eHealth platform in Uganda.
Furthermore, collaboration and sharing of technical expertise between the government, system developers, ICT service providers, and users can facilitate sharing of ICT expertise in implementing, repairing and maintaining the equipment and systems. The country has created a conducive environment for this to happen, as exemplified in IT companies that are providing IT services to the different sectors of government (HIV_03, Government Organisation). Some of the companies have Corporate Social Responsibility projects that, when approached, can be explored to benefit the eHealth programs in the country (UCC_04, Government Organisation).
On cost-sharing, several stakeholders expressed willingness to support eHealth initiatives in Uganda. Besides, once developed, attracting more people to use such a system will lower the maintenance cost since many users will be on board (NITAU_01, Government Organisation). Also, aspects of expenses in operating the eHealth for example data sharing, can be shared by service providers such as providers of the electric power required to run the systems, internet services through the telecommunication data services providers, etc. All these readily available services can be provided at subsidised rates (HIV_03, Government Organisation).
Discussion
Walugembe et al. 23 argued that a focus on sustainability requires consideration of the potential loss of investments for organisations and people if interventions with perceived or actual benefits are not sustained. This study identified several risk and success factors for the sustainability of an eHealth data capture and processing platform for Uganda. Apart from the following risks factors including; limited ICT infrastructure, poor system maintenance, inadequate requisite technology skills/competence by healthcare professionals, inadequate governance structures and limited political will, as well as limited trust in information sharing and data presentation formats as identified in other studies; it emerged from this study that lack of a sustainability plan, inadequate management systems, and inappropriate vices in organisational management are risks to the success of implementing an eHealth platform in Uganda. Just like other ICT for health intervention studies, we found that the problem of financial resources/funds to support continued maintenance, staffing and use of the system remains.23,24 The system eventually collapses when the key funders of eHealth interventions in Uganda pull out. 27 We also found that there is lack of technical personnel to support the repair, maintenance and use of ICT devices and systems in health. Participants argued that obtaining technical support from the government is challenging, often resulting in prolonged system downtime.
Furthermore, skill competency limitations by healthcare professionals to use eHealth technologies identified in this study has been reported by several other authors, requiring training.32–34 Similarly, the gap in governance structure and or political will had been identified by other authors as challenges experienced in attaining success in any healthcare intervention, including eHealth implementations. 35 To support the sustainable implementation of an eHealth data capture platform for Uganda, both health workers and patients need to put more trust in the health data and information that they share. Besides, such data/information should be in formats and presented in a manner that all levels of the workforce can make sense of. Lastly, a sustainability plan was lacking to ensure smooth transition from Implementing Partners/Donors’ support to facility governance and/or continued system financing.
Nonetheless, several critical success factors of sustainability were identified. Particularly, it emerged from the study that multisectoral engagements and inter-ministry/department/agency support, the will to collaborate and share technical expertise/costs, and progressive development of health healthcare workers’ ICT skills are successes that Uganda can leverage in implementing an eHealth data capture, processing and dissemination platform. Of course, these four success factors add to those previously identified by other authors to exist in Uganda, including rapid development in ICT and its use in many of the public sectors in Uganda, progress towards an eHealth strategy and policy framework, existing infrastructure (electric power and telecommunication network connectivity).11,36 Literature identifies the availability of ICT infrastructure and widespread internet connectivity, ICT literate human resources especially digital healthcare professionals who are graduating for medical, availability of funds, stakeholder buy-ins, alleviation of fears of data sharing, ownership, and access rights to increase the system’s adoption and implementation feasibility; adequate organisational management; and availability of a sustainability plan as necessary success criteria for implementations of eHealth systems in low-resource countries like Uganda. 21 Some of the critical success factors are missing in Uganda’s context; and rather do exist as risk factors signifying that the country needs to make more effort to address them.
On the issue of reinvestments as a partial sustainability plan, it should be noted that several eHealth interventions implementations require substantial investment in terms of human, fiscal and technical resources and any form of inadequate attention to such investments could be considered careless and inefficacious. 23 The need to maximise limited resources continues to be a cross-cutting discussion of system sustainability. 23 It is impossible to make progress without resources, including financial, competent human and ICT infrastructural resources. 37 Whereas finances are needed to pay for the initial or upfront cost of the investment, sustainability would require additional finances to fund the cost of running the system, training and facilitating competent human resources which use the system and maintain ICT infrastructure. Despite funds availability, sustaining system implementations over time may still be difficult without a proper sustainability plan, management and maintenance plan. A good sustainability plan could include aspects of reinvestment.
Finally, regarding the cost implications of developing and deploying a successful eHealth data capture and processing platform for Uganda, we observed initial costs for investment and ongoing costs incurred to ensure that the system remains operational and viable. These costs are kin to the findings of other earlier studies for example, start-up costs, maintenance costs, and those costs related to loss of revenue and potential savings. 38 Others, are induced costs that relate to temporary productivity loss as a consequence of using the system.
Conclusion
The study investigated risk factors that negatively affect the sustainability of Uganda’s eHealth data capture and processing platform. The risk factors broadly rest on the lack of a suitable sustainability plan that has resulted in poor system maintenance and inadequate management systems, bad leadership, corruption and lack of sustainable maintenance programs. However, there are potential success factors that can be leveraged to ensure a sustainable eHealth data capture and processing platform implementation for Uganda, including the availability of ICT infrastructure, human resources, funds, stakeholder buy-ins, a framework on data sharing, ownership and access rights, multisectoral engagements and inter-ministry/department/agency support, the will to collaborate and share technical expertise/costs, as well as progressive development of health healthcare workers’ ICT skills. In their present form, these success factors could facilitate immediate operationalisation of Uganda’s eHealth data capture, processing and dissemination platform. But to achieve success, Uganda’s MoH can mitigate these risks through strengthening the legal framework for eHealth, providing guidelines for developing, implementing and using eHealth systems, as well as strengthening existing health governance frameworks to improve on eHealth leadership and governance that eliminate corrupt tendencies, and properties for planning for sustainable eHealth implementations in Uganda. Future works could explore alternative ways to plan and implement sustainability of eHealth systems, as well as investigate the balance of success and risk factors capable of eliciting meaningful value and positive outcomes for the country.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the MRC/UKRI (MR/S013164/1).