
Abstract
Background
Supervised physical activity interventions can improve cancer survivor quality of life. However, they are resource intensive and may not support physical activity maintenance. Therefore, most cancer survivors remain inactive. Electronic health is a promising tool to support physical activity maintenance, yet technology-based physical activity interventions in oncology have shown mixed effectiveness. We surveyed cancer participants in the Alberta Cancer Exercise program to better understand their experience with technology.
Methods
Alberta Cancer Exercise participants were invited to complete a survey on technology literacy, usage, and perceived usefulness. Summary statistics were calculated for all variables. Multiple regression examined demographic prediction of technology usage and literacy.
Results
The response rate was 52.6% (n = 627/1191), with 93.3% survey completion (n = 585/627). Respondents were 60.6 ± 11.0 years old, 96.2% Caucasian, and of high socioeconomic status (83.3% with post-secondary education, 65.5% with income >$60,000). While electronic health literacy was low (mean 1.73 ± 0.73/4), computer (87.6%) and smartphone (87.5%) use was widespread, with 94.6% of smartphone users reporting daily use. One in two respondents used mobile applications or wearable trackers for physical activity, which were perceived as useful by >80% of users. Age and income were significant predictors of technology use and literacy.
Conclusions
Technology is part of the lives of cancer survivors who engaged in a physical activity program, with mobile devices perceived as useful to support physical activity. However, the present findings highlight a need to increase electronic health literacy via education and tailoring of digital tools. These survey findings are being used to build our patient-centered, technology-supported physical activity interventions.
Keywords
Introduction
Despite the evidence and the guidelines supporting the critical role of exercise for adult cancer survivors, most survivors remain insufficiently active.1–3 Many demographic (higher age, lower income) and cancer-related factors (type, stage) are associated with lower physical activity (PA).4,5 Cancer survivors face significant barriers to PA, including lack of time, lack of access to facilities, lack of motivation, insufficient social support, and low self-efficacy.6,7 Furthermore, supervised PA programs are resource intensive, requiring expert staff and full-feature fitness facilities, which are costly and unavailable in many settings, limiting scalability.7–9
The emergence of modern health technology (electronic health: eHealth), such as commercially available wearable activity trackers (WATs) and mobile health applications (a subset of eHealth called mHealth), may represent a key avenue to address PA barriers, support PA behavior change, and promote PA maintenance, while also increasing scalability of PA programs in oncology. Emerging technologies not only enable objective PA measurement (the primary use in studies to date), but also can provide real-time automated feedback, enhanced communication with exercise specialists, access to a wealth of personalized PA resources, and remote access to social support networks. These features may support PA behavior change and increases in PA levels. For example, WATs can enhance PA self-efficacy via PA reminders, goal setting, and personalized feedback, resulting in higher PA levels. 10
In 2015, development and evaluation of mHealth for PA promotion in cancer survivors was identified as a research priority by the National Cancer Institute, leading to an expansion in PA trials using mHealth. 11 Systematic reviews of eHealth and mHealth PA interventions in oncology have highlighted the growing evidence that a range of technologies can effectively increase PA levels and improve health outcomes for adults affected by cancer.12–16 However, the ability to draw conclusions is limited due to the heterogeneity across interventions and mixed impact on factors including patient-reported outcomes, quality of life, and PA levels.12–16 In addition, challenges concerning study adherence and continued engagement with mHealth may limit the effectiveness of mHealth PA interventions.17,18
According to the Technology Acceptance Model and the Unified Theory of Technology Use and Acceptance, perceived ease of use (effort expectancy), as influenced by technology literacy and previous use, and perceived usefulness (performance expectancy) are important drivers of engagement. 19 Tailoring of eHealth PA interventions to target these constructs has been associated with improved adherence to technology, mediating short- and long-term intervention effectiveness.17,20 Therefore, a key step to inform development and implementation of eHealth PA interventions for cancer survivors is to determine their technology literacy, use, and perceived usefulness. 21 While cancer survivors’ interest in technology-based interventions has been documented in the literature, little is known about their eHealth literacy and current usage, especially in relation to PA (i.e. within cancer survivors with a history of PA).22–24 Having this data then supports development of a patient-driven intervention design that aligns with the respective characteristics of the target population, potentiating enhanced intervention effectiveness. 25
Therefore, the purpose of this study was to assess technology literacy, use, and perceived usefulness to support PA behaviors, in cancer survivors with a history of PA. To our knowledge, this is the first large-scale survey of PA-related technology literacy and usage in a sample of participants from an exercise oncology program. This work provides preliminary insights that are being used to inform our participant-driven research in technology-supported PA behavior change for adults living with cancer (NCT04478851).
Methods
The reporting of this online cross-sectional cohort survey follows the checklist for reporting results of internet e-surveys (CHERRIES). 26
To gather information on technology use, perceived usefulness, as well as eHealth literacy in relation to PA behavior among cancer survivors, the current survey targeted Albertan cancer survivors who were past or current participants in the Alberta Cancer Exercise (ACE) program. 27 ACE includes (a) cancer survivor of any cancer type and (b) no more than 3 years post-treatment completion. Additional criteria for this survey were: (a) completed ACE 12-week study questionnaire, and (b) consented to receiving further questionnaires of sub-studies. ACE participants took part in a 12-week in-person exercise program, with no eHealth component as part of the intervention (see ACE protocol for further details 27 ). Convenience sampling of these ACE participants aligned with the purpose of understanding specific perspectives on technology use in cancer survivors with a history of PA, which has not been published in the literature to date. An invitation to the survey was emailed to eligible participants with information about its purpose and duration, as well as a link to complete the survey in REDCap.
Ethical approval was obtained by the Health Research Ethics Board of Alberta's Cancer Committee (HREBA-CC, ID 19-0489). All participants provided informed consent directly in the survey.
Development
Survey questions were developed by two authors (NCR, ME) and refined using feedback from experts in exercise oncology. Alongside general questions about technology access, current usage, and perceived usefulness to support PA behavior, the validated 35-item eHealth literacy questionnaire (eHLQ) was used to measure health technology literacy. 28 The eHLQ measures eHealth literacy in seven domains (five items per domain) according to the eHealth literacy framework: using technology to process health information; understanding of health concepts and language; ability to actively engage with digital services; feel safe and in control; motivated to engage with digital services; access to digital services that work; and digital services that suit individual needs. 28 A measure of health technology literacy was included as it is an important predictor of uptake and engagement with health technology.29,30
Readability, usability, and technical functionality of the survey were then optimized using two rounds of pre-testing. First, feedback was collected from 13 cancer survivors who voluntarily completed the first version of the survey, leading to improved definitions for some terms and removal of one question. The responses collected during this round were not included in the final sample. Secondary testing focused on technical functionality, assessed by two authors (NCR, ME) and additional exercise oncology professionals, via three additional rounds of edits that led to minor changes in wording and survey logic for the final version.
Health technology survey
The final survey contained 38 items and was delivered via REDCap, a secure platform for collection of clinical research data. The complete survey is available from the authors upon request. All participants were familiar with REDCap via their participation in ACE. Conditional formatting was used to reduce the number and complexity of required responses for the three questions on technology usage, frequency, and purpose/perceived usefulness. Specifically, after respondents indicated the technologies they used in question 1, options for questions 2 and 3 were limited based on this response. Due to the adaptive nature of the questions and the standard format of the eHLQ, randomization of survey items was not possible. An automatic check for completeness was done at the end of each page, requiring respondents to complete mandatory items before proceeding. At any point prior to survey submission, respondents were able to freely navigate between pages to review and change responses. All survey responses were automatically linked to respondent demographics including age, gender, and cancer diagnosis provided previously as part of the ACE program, via a unique ACE participant identifier in REDCap.
To access the survey, respondents were required to log-in using their email address, limiting responses to ACE participants and preventing multiple entries. Survey participation was voluntary, as highlighted in the invitation email and informed consent.
The survey was available over a 4-week period from 23 April to 21 May 2020, with reminder emails sent to eligible ACE participants who had not completed the survey after 7 and 14 days.
Statistical analysis
Recruitment rate was calculated as the number of ACE participants who provided informed consent divided by the total number of ACE participants who received the email invites. Completion rate was calculated as the number of respondents who completed the survey divided by the number of ACE participants who provided informed consent. Only submitted surveys were included in the analyses, as choosing to submit was considered the final step in participant consent.
Descriptive statistics were calculated for respondent demographics and all survey items. Statistics include means/standard deviations for continuous variables and raw numbers/percentages for categorical variables. Responses for the 35 items of the eHLQ were analyzed as recommended to yield scores for each of the eHLQ's seven domains of health technology literacy. To assess the representativeness of survey respondents relative to ACE program participants, demographics were compared between groups using independent t-tests with significance set at P < 0.05. Multiple regression was used to examine demographic characteristics in relation to technology use and eHLQ score, with standardized regression coefficients reported. All analyses were performed using SPSS for Windows, version 26 (IBM).
Results
Respondents
Of 1512 ACE participants, 1207 met the inclusion criteria for the survey. Sixteen emails could not be delivered, resulting in 1191 participants who were invited to complete the survey, and 627 who responded. The response rate was 52.6% (627/1191), with a completion rate of 93.3% (585/627). In total, N = 929 ACE participants did not complete the survey.
Table 1 summarizes demographics for the 585 respondents who completed the survey. The mean age of respondents was 60.6 ± 11.0 years (median 61, interquartile range 54–68), with 71.3% female and 28.7% male, and 85.3% having had at least some university/college education. A detailed breakdown of respondent age is presented in Supplemental Figure 1. Compared to the non-respondents and those that did not complete the survey from the ACE population (N = 929), survey respondents who completed the survey (N = 585) were significantly older, more likely to report a retired employment status, and were more likely to have a higher income (all P < 0.001). No other significant differences were observed between respondents and non-respondents.
Demographic characteristics of survey respondents.

Significant differences between survey respondents and non-respondents (P < 0.001).
Colon, rectal, pancreas, stomach, esophagus, liver, and anal.
Prostate, bladder, kidney, and testis.
Technology use
Type
The types of technology used by respondents are presented in Figure 1. Smartphone use included iPhone (67.3%, 348/517) and Android (32.9%, 170/517), with one respondent reporting using both. Common social media platforms were Facebook (93.4%, 338/362), Instagram (46.1%, 167/362), and Twitter (21.3%, 77/362). Roughly one-third of all respondents reported using PA/health-related applications (32.1%) and WATs (36.0%). The WATs respondents reported using were Fitbit (N = 134), Apple Watch (N = 37), Garmin (N = 32), and other (N = 17).

Technology usage by type (N = 585).
Frequency
Frequency of technology use was variable, as shown in Figure 2.
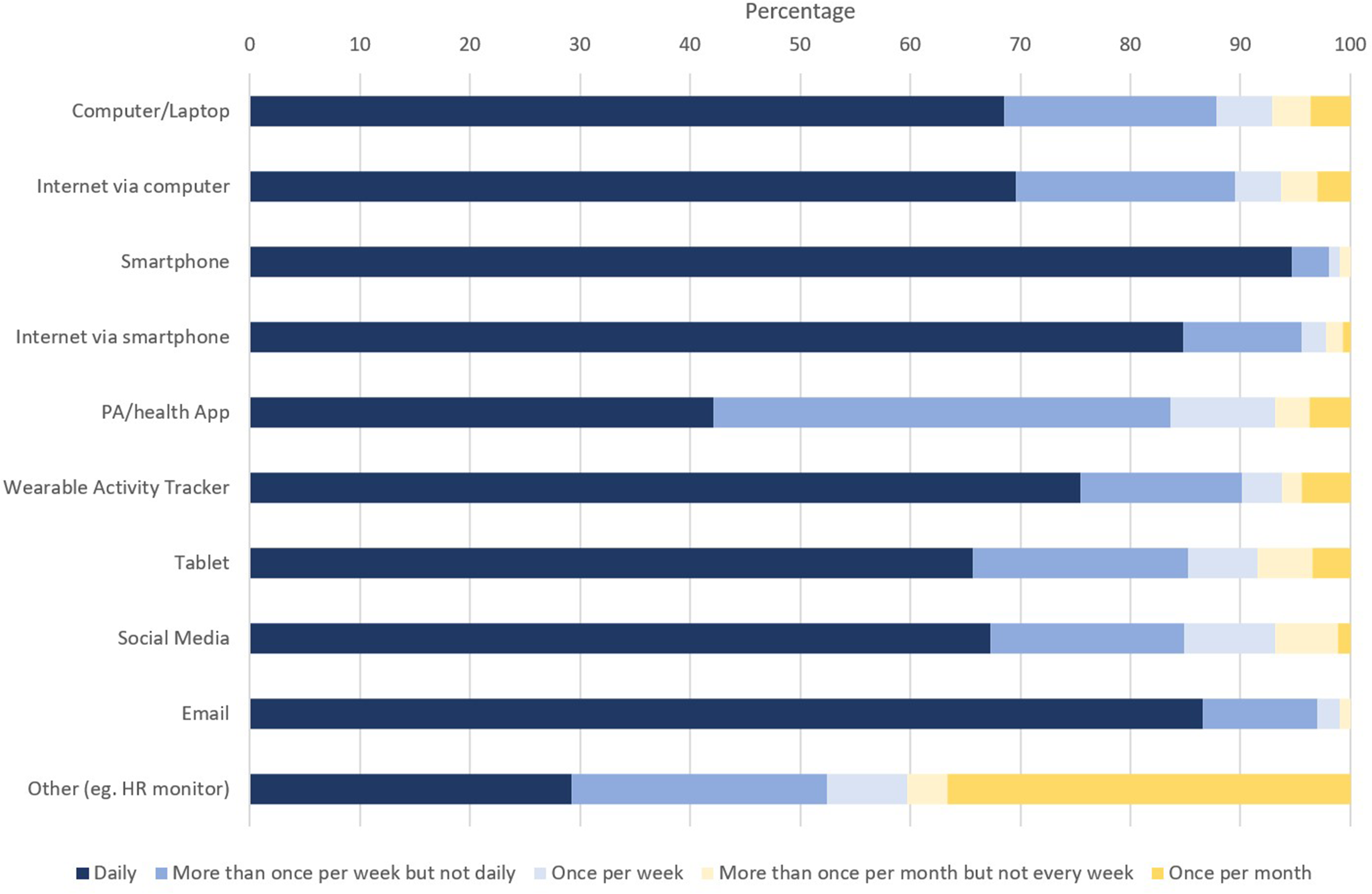
Frequency of technology usage by type (N = 585).
Perceived usefulness to support PA/health behavior
Figure 3 presents respondent perceptions on usefulness of technology to support healthy lifestyle behaviors. Perceived usefulness was the highest for WAT (83.9% rated as useful or very useful) and PA/health apps (80.5% rated as useful or very useful).
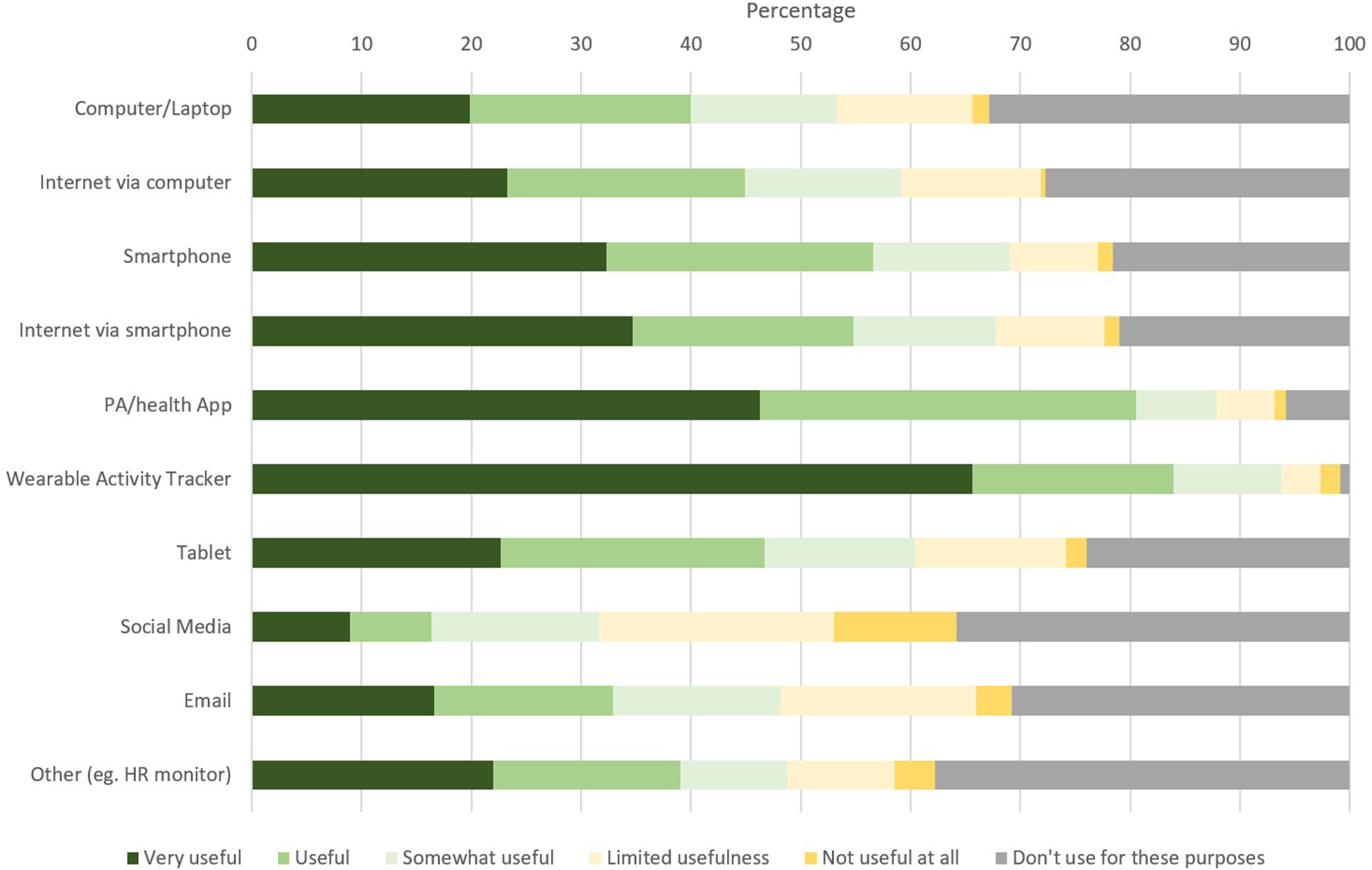
Perceived usefulness of technologies to support PA/health behavior (N = 585).
eHealth literacy
Respondent eHealth literacy scores across the seven eHLQ domains are presented in Table 2. The average score across all domains was 1.73 ± 0.73 out of 4, with no domains above 2, indicating low overall health technology literacy in this population. Significant correlations were found between mean scores on all domains (R2 = 0.383–0.809, P < 0.001).
Electronic health literacy questionnaire (eHLQ) scores across seven domains.

Demographic predictors
The results of the multiple regression analyses show that a model using demographics (age, gender, income, educational status, marital status, employment, and cancer type) was a significant predictor of the number of technologies used (F(7,519) = 5.52, P < 0.001, R2 = 0.069) and mean eHLQ scores (F(7,519) = 5.51, P < 0.001, R2 = 0.069) of respondents. Each model explained 6.9% of the variance in technology use and eHLQ score. Age (B = −0.022, P = 0.007), education (B = 0.189, P = 0.007), and income (B = 0.155, P = 0.01) added significantly to the prediction of technology use. For the predictive model of eHLQ score, age (B = −0.006, P = 0.001), gender (B = 0.098, P = 0.024), and income (B = 0.045, P < 0.001) contributed significantly.
Discussion
Principal findings
The purpose of the current survey was to provide novel insights into the technology landscape among cancer survivors with a history of PA, especially with regards to PA-specific eHealth technology. Understanding the relationship between technology literacy, use, and usefulness in cancer survivors with a history of PA is essential to inform our ongoing work, designing a technology-supported intervention that will positively impact PA levels and quality of life for participants. Our results indicate that use of technology was high, with most respondents reporting more than weekly use of computers, smartphones, and the internet via these devices. Survey results align with trends toward rapidly growing technology usage in cancer survivors over the past decade, and suggest that technology adoption may even be higher in this unique subset of cancer survivors who engaged in a PA program.31–33 The pervasive use of internet-connected computers and smartphones in this sample of physically active adults living with cancer confirms that such technologies may be useful tools to support PA. For example, a mHealth app may be a viable tool to support PA behavior change in subgroups of the population who use smartphones. Furthermore, the high frequency of use speaks to technology's potential to support development of PA habits in the target population, with devices already integrated into daily life.
Adoption of technology to support active lifestyles was common, with one in two respondents using a PA/health app and/or a WAT, slightly higher than the 40% in a survey of 279 breast cancer survivors. 22 In addition, mHealth (smartphones, PA/health apps, or WATs) was perceived as the most useful for supporting healthy lifestyle behaviors, rendering mHealth as a primary candidate to support PA behavior change and not just “track” PA behavior. Even in cancer survivors who engage in an exercise program, such as ACE, overall exercise adherence levels remain low in the long term. 8 As such, using technology to support key behavior change techniques linked to exercise maintenance, such as goal setting or planning implementation, is required.
Despite varied and frequent use of technology, respondents demonstrated relatively low eHealth literacy. The eHLQ results indicate that cancer survivors in Alberta may lack digital services that work and suit individual needs (Domains 6 and 7), which may contribute to decreased motivation and use of eHealth technology (Domains 1 and 5). Significant correlations between domains point toward the need for a cohesive development of overall eHealth literacy. For example, improved cancer-specific digital services (Domains 6 and 7) could improve eHealth use and motivation (Domains 1 and 5) and thereby enhance user understanding, ability, and feelings of safety and control (Domains 2–4). However, the causality and directionality of these inferences remains unclear. An eHealth literacy survey in 305 Danish cancer survivors with a comparable demographic profile measured much higher average eHLQ domain scores, between 2.5 and 3.0. 34 Additional research is required to better understand the underlying factors contributing to this variability in eHealth literacy, and low eHealth literacy must be addressed to improve technology engagement and ultimately support PA behavior change and maintenance.29,30
The low eHealth literacy among respondents indicates that technology-based tools within PA interventions for this population must carefully consider and address the seven domains of eHealth literacy, as personalization and tailoring of eHealth is known to reduce technology abandonment and enhance intervention effects. 35 Findings from a mixed methods study emphasize that technology used within cancer-specific PA interventions must be easy to use and tailored to unique cancer survivor populations (age, race, cancer type, and other demographics), with individualized solutions needed due to variability in preferences.36,37 The importance of individualized solutions is further emphasized by our findings that age, education, gender, and income predict technology use and/or eHealth literacy in cancer survivors who participated in a PA intervention. Similar trends have been noted in both cancer survivor and older adult populations.34,38 As the present models only explained 7% of the variance in technology use and eHealth literacy, additional work is required to determine other predictive factors. For example, some factors associated with lower health technology literacy among cancer survivors in previous studies include living alone and having additional chronic conditions. 34 Assessment of demographic or health-related factors, as well as past experiences with eHealth, may thus enhance our understanding of technology use and eHealth literacy, informing improved tailoring of eHealth PA behavior change interventions for the target population.
Strengths and limitations
The current survey has several key strengths. The large sample size and high completion rate enhance the generalizability and confidence in the findings on the topic of technology use, usefulness, and literacy in a sample of cancer survivors with a history of PA. Given the current respondents’ PA program participation, they may be more motivated for PA, and thus their level of technology use for PA/health-related purposes and perceived usefulness of technology to support PA behaviors may be higher than in inactive cancer survivors. However, recruitment of respondents who were physically active was necessary to understand specific perspectives on technology use related to being physically active. Importantly, this information will be used to inform our upcoming eHealth implementation in exercise oncology program participants. Specifically, investigating the technology–PA relationship to understand what technologies are used and perceived as useful in this context will lead to patient-informed implementation of technology-supported interventions that support adoption and maintenance of PA habits.
The voluntary nature of this survey resulted in a respondent population that was older, more likely to be retired, and wealthier than the pool of ACE participants from which they were drawn, impacting generalizability to both the physically active cancer population, as well as the larger population of all individuals living with cancer. While all respondents were current or previous participants in ACE, there was diversity across age (25–92 years) and cancer types, enhancing the generalizability of the results to the broader cancer population. However, there is a lack of diversity based on ethnicity (96% White), high education levels (85% attending at least some university/college), and high income (50% having an annual family income greater than $80,000). Unfortunately, the demographic biases seen herein are commonly reported in exercise oncology research. 39 Funding agencies and researchers must work together with communities to improve equity, diversity, and inclusivity, reaching underserved cancer populations who often experience worse health outcomes and may have different perspectives on technology than the present sample. 40
Future directions
To address limitations and remaining gaps in the literature, future surveys should target underrepresented populations across a range of demographics to increase the representativeness of findings. Furthermore, to develop a deeper understanding of the technology landscape in oncology and inform effective use of technology for supportive cancer care, qualitative research using individual interviews or focus groups may be informative. An important question that remains to be answered is the temporal relationship between PA-related mHealth use and PA habit formation (i.e. does mHealth use prompt habit formation or do PA habits prompt mHealth use?). Lastly, demographic predictors of technology use and eHealth literacy (e.g. age and income) highlight the need for increased personalization of technology-based PA interventions to meet the unique needs of participants.
Conclusions
The present results provide an overview of the technology landscape within exercise oncology program participants, indicating pervasive use of internet-connected computers and smartphones, while mHealth was perceived as most useful to support PA behavior and eHealth literacy remained low. These findings speak to the potential for integration of mHealth technologies within cancer survivor PA habits, informing ongoing patient-oriented research to enhance the engagement with and effectiveness of mHealth PA interventions. However, in light of the sampling bias toward physically active, wealthy, educated, Caucasian cancer survivors, more work is needed to extend the current findings to other survivor populations (e.g. diverse ethnic backgrounds and lower income populations).
Footnotes
Acknowledgments
The authors thank Dr Christopher Sellar and members of the ACE study staff for assistance with survey distribution and data analyses, as well as ACE participants for taking the time to complete the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
ME, MHM, MM, and SNCR conceived the study. ME and SNCR developed the protocol and obtained ethical approval. MM assisted with patient recruitment and study coordination. ME and MM completed the data analysis. ME and SNCR wrote the first draft of the manuscript. All authors reviewed, edited, and approved the final version of the manuscript.
Ethical approval
Ethical approval was obtained by the Health Research Ethics Board of Alberta's Cancer Committee (HREBA-CC, ID 19-0489).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Guarantor
SNCR.
Peer review
This manuscript was reviewed by reviewers. The authors have elected these individuals to remain anonymous.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.