
Abstract
Primary healthcare professionals face an increasing number of geriatrics patients, and patient care often involves different disciplines. eHealth offers opportunities to support interprofessional collaboration (IPC). This exploratory study aimed to gain insight in 1) IPC in community-based rehabilitation, 2) facilitators and barriers for technology-based IPC and 3) technological IPC solutions envisioned by the primary healthcare professionals An focus group with six primary healthcare professionals and a design thinking session with four participants were conducted. Data analysis was based upon an IPC model. Results indicate that facilitators and barriers for IPC can be clustered in three categories: human, organization and technology, and provide some requirements to develop suitable IPC technological solutions Primary healthcare professionals recognise the urgency of working collaboratively. Current barriers are understanding each other’s professional vocabulary, engaging the older adults, and using technology within the patient’s environment. Further research is needed to integrate IPC components in a technological solution
Introduction
The population worldwide is ageing, increasing the number of older adults with one or more geriatric syndromes, such as falls and osteoarthritis (World Health Organization [WHO], 2021. In the Netherlands, most older adults go straight home for community-based rehabilitation after being discharged from hospital. 1 This is partly due to the Dutch government policy that encourages “ageing in place”. 2 As a result of population changes and policies, primary care physical therapists will be confronted with more older adults (65+) who need to rehabilitate at home. 3
The increasing demand on primary care physical therapists for community-based rehabilitation for patients with complex health problems, also increases the need to collaborate with other professionals. 4 Research has shown that community-based rehabilitation is multifaceted, 5 and patient care involving geriatric syndromes often involves several primary healthcare professionals (e.g. General practitioners, physical therapist, occupational therapist, community nurse, social workers). 6 Together these professionals provide a combination of home care and therapy, taking into account the home situation of the older adults. Interprofessional collaboration (IPC) has become a necessity and can positively affect community care delivery for the older adult. 7 The WHO 8 defined IPC as ‘Collaborative practice happens when multiple health workers from different professional backgrounds work together with patients, families, carers and communities to deliver the highest quality of care across settings’. However, achieving IPC remains a challenge. For example, it involves client-centered care, professionals sharing a common purpose, recognise and respect each other’s body of knowledge, role and team-agreed responsibilities, and requires effective communication and organisation.9–14
eHealth offers opportunities to support IPC in community-based rehabilitation of older adults. eHealth is broadly defined as “the use of technology to improve health, well-being and healthcare”. 15 The term characterises not only a technical development, but also a new way of working, an attitude, and a commitment to improve healthcare. 16 Research also shows the added value of using eHealth in delivering care to older adults who need to deal with different primary healthcare professionals. 17 Several technologies are currently available for IPC in community-based rehabilitation, including communication technology such as telehealth, sensors, electronic or patient held records, wearables, remote communication apps and electronic platforms (e.g.).18,19 Although these technologies are available, technological solutions to support IPC between primary healthcare professionals for community-based rehabilitation is still uncertain.
The goals of this exploratory study were to gain insight in 1) the current state of IPC, 2) facilitators and the barriers that play a role in technology-based IPC and 3) possible technological solutions envisioned by the primary healthcare professionals to support IPC, with the aim to support the community-based rehabilitation of older adults in a Dutch primary care context.
Methods
Study design
The exploratory study was conducted using two qualitative methods: a focus group and a design thinking session. Participants were Dutch primary healthcare professionals in The Hague and the surrounding area delivering community-based rehabilitation to older adults. Focus groups were used to collect more in-depth information through interactions within the group. Also focus groups were an efficient way to collect data of several healthcare professionals at the same time. The focus group 20 provided a way to explore and discuss IPC between primary healthcare professionals and the use of technology in the context of community-based rehabilitation for older adults. Design thinking method was chosen to allow co-creation to occur and stimulate innovative ideas. Specifically, the design thinking 21 session provided a human-centred approach to generate creative ideas around technology-based IPC, anchored in understanding the needs of the primary healthcare professionals.
Recruitment
Focus group
Participants were recruited through two physical therapy practices with whom the universities of applied sciences closely collaborated and through an existing primary care network. Recruitment was aimed at diversity of the primary healthcare professionals’ disciplines. Inclusion criteria were: being a primary healthcare professional and having experience with home rehabilitation for older adults.
Design thinking session
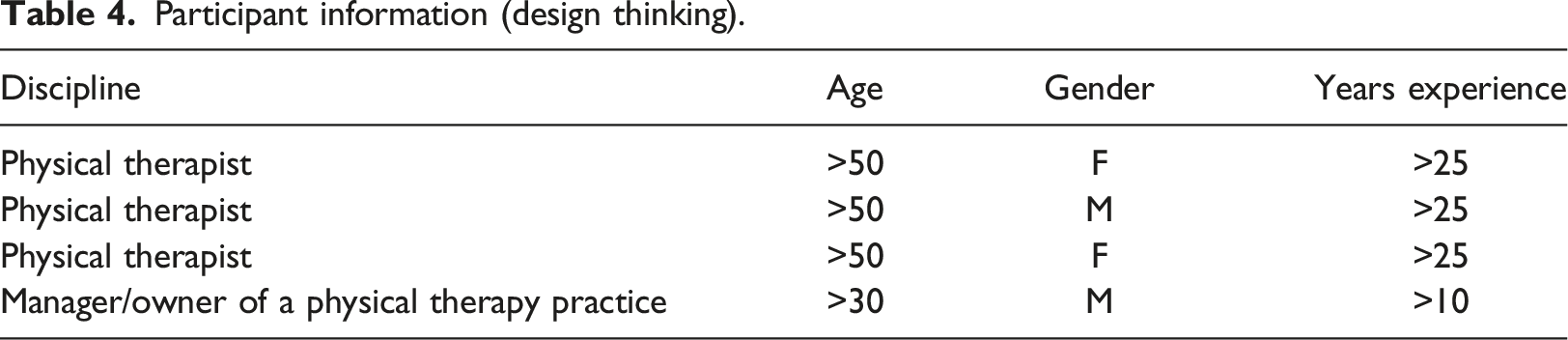
Participants were recruited from the same sources as the focus group. Only primary care physical therapist were recruited, since they often are the first point of contact to start home rehabilitation when the older adult has been discharged from hospital. Inclusion criteria were: being primary care physical therapist and having experience with community-based rehabilitation of older adults.
Setting and data collection
Focus group
Due the Covid pandemic, the 90 min focus group held its meeting online via Zoom in the spring of 2021. Informed consent was given by all the participants. The video and audio of the meeting were recorded and then transcribed. One researcher was assigned as the focus group leader, and three researchers from the project, assisted the focus group leader and took notes.
A manual was prepared beforehand and was reviewed by the research team as well the project advisory board. The manual outlined the structure of the focus group, the themes to be addressed and the types of questions. Themes aimed to explore the professionals opinions on IPC in home rehabilitation of older adults, and the use of eHealth in practice, specifically with regard to IPC. Attention was also given to the facilitators of and barriers to IPC.
Design thinking session
The design thinking session was held in the autumn of 2021 at the Inholland University of Applied Sciences (in The Hague). Participants were divided into two groups. Each group comprised of primary care physical therapists, a coach and a researcher (both members of the project). The session lasted 2 hours.
Similarly to the focus group, a manual was prepared beforehand outlining the structure of the session, and was reviewed by the project team as well the project advisory board. A separate document was prepared for the coaches to guide them through the various steps of the design thinking approach. Finally, a template was created for the participants to describe possible technological solutions. The template contained the problem the participants had to solve, which was defined as follows: Which technology could be used in order to optimise IPC for primary care professionals in the context of home rehabilitation by older adults? To answer this question, the participants had to complete the template by describing the possible solution, its effect, outcomes and impact for IPC. After the groups had completed the template, they gave a short presentation to the other group followed by a discussion of the findings.
Data analysis
Qualitative, theory-driven, data analyses were used to further our understanding of professionals’ perspectives on IPC and the use of technology in community-based primary care.
Framework
The IPC was analysed using the conceptual framework for interprofessional collaboration of. 14 This framework was selected since it is specifically adapted for the healthcare domain and in that regards the relevant core elements. This framework described eight core elements of IPC. These elements were used as initial themes for the analyses and to help understand how the professionals fleshed out the themes. The themes are: 1) client-centered care supporting self-management and engaging the client in decision-making; 2) focus on positive health i.e. on the clients’ ability to adapt and self-manage in the light of social, physical and emotional challenges in life; 3) role and responsibilities i.e. professionals’ know, value and acknowledge roles and responsibilities and have an agreed structure of coordinating care; 4) shared liability and responsibility i.e. professionals share the responsibility and liability for the whole process of treatment, guidance and support; 5) interdependency, i.e. professionals are aware that they mutually depend on each other in attaining the client’s goals; 6) clear communication i.e. taking cultural/professional differences and context into account; 7) sharing knowledge/collaborative learning/integrating knowledge and skills, 8) easy access and swift referrals such as knowing each other and swift communication and referrals. The IPC themes analysis was conducted deductively, allowing the possibility to explore relationships, core elements and concepts and to measure concepts quantitatively.
Focus group
The transcript was read in full and thereafter re-read and coded by one researcher using the elements of the conceptual framework. Within each element, key statements were grouped, and barriers and facilitators were elicited from these and coded. Findings were summarised and a quote was selected to illustrate the findings.
Design thinking session
The design thinking templates were used as the basis for a three-step analysis. In the first step, each group of researchers separately reviewed the two templates and, for each template, filled the relevant elements into the themes which had been identified in the focus group. During the second step, the elements were scrutinised for similarities and differences. In the final step, a thematic clustering was made. Elements of IPC were analysed in the same way as for the focus group.
Ethical considerations
The study adheres to ethical standards. All the participants were informed and gave verbal informed consent and the data were anonymously analysed. Audiotapes were destroyed after transcription.
Results
Results from the focus group
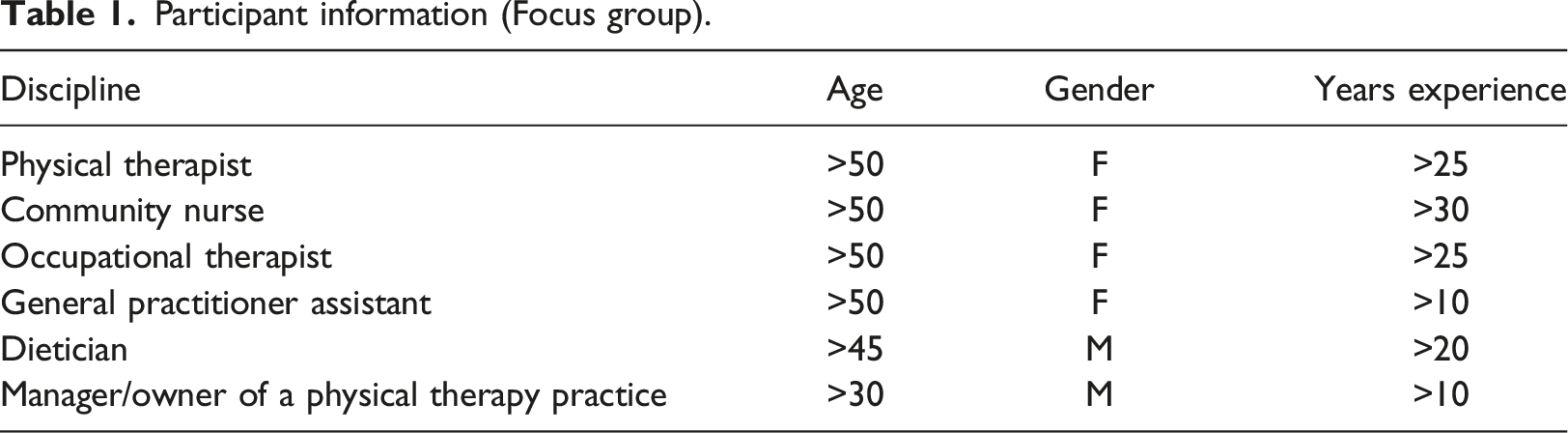
Participants
Participant information (Focus group).
Interprofessional collaboration
Current collaboration
All the participants collaborate with one or more other disciplines. The physical therapist and the occupational therapist often work together and have regular contact with the community nurse. When needed, both professionals seek contact with the general practitioner or the general practitioner assistant. The occupational therapist also has contact with podotherapists and increasingly with alternative practitioners. In addition, a collaboration with the client and his informal caregiver was mentioned by all the participants. Dieticians are rarely included in the current IPC. However, the participants mentioned that nutrition is considered to be important during the entire rehabilitation process of the older adult. Collaboration with social workers was reported to be absent. Contact with the pharmacy was mentioned in relation to drug prescriptions. Primary healthcare professionals make use of their specialised network, for example, when the older adult in home rehabilitation has a specific health problem, such as early dementia. Primary healthcare professionals also have contact with other non-primary healthcare professionals. For instance, after discharge from hospital, there is sometimes contact with the hospital or with the specialised nurse.
Current use of technology
Several ICT-based applications were reported, mainly aimed at interprofessional communication (with GPs and clients) and at reporting patient information. Software applications, such KIS, 1 Zorgdomein 2 and Siilo, 3 are often used to exchange information via secure networks.
Professionals’ understanding of interprofessional collaboration
Summary of themes of interprofessional collaboration addressed in the focus group.
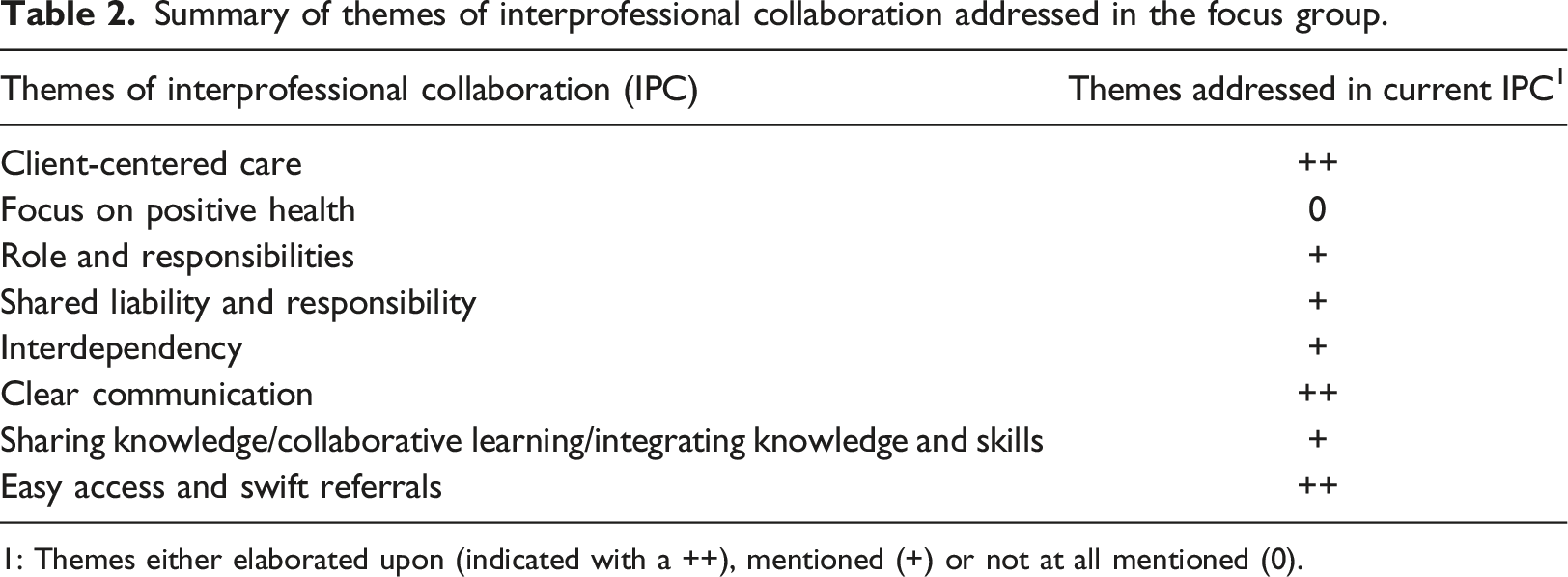
1: Themes either elaborated upon (indicated with a ++), mentioned (+) or not at all mentioned (0).
Clear communication was elaborated on in terms of the need for the right amount of communication and the type of language, in view of the goal of the communication. A better match leads to easier collaboration and technology can play an important role in creating the right match. Professionals related the right type of language to the degree that patients are involved. A shared language is thought to be important among professionals from different backgrounds. “In treatment, it is very important to me that we speak the same language. It takes a while before you realise what they are talking about” (dietician). In addition, the type of communication (face-to-face, telephone, written, etc.) will influence the communication itself. In general, personal contact is considered to be important for both the professional-patient relationship and professional-professional interactions.
Easy access and swift referrals were related to information and relationship. Easy access to information (through technology) was mentioned as a way to be well informed. Easy access to other professionals was mentioned to be beneficial ‘It is easier to line up if you know each other and know how to get in touch easily’ (occupational therapist). Knowing the other professionals was considered to be also important for the client ‘It gives the patient confidence in the care if I know, for example, who their dietician is' (GP assistant).
Themes which were mentioned but not much elaborated upon were: roles and responsibilities, shared liability and responsibility, interdependency, and sharing knowledge/collaborative learning/integrating knowledge and skills. Interdependency was discussed as being a risk. ‘Working with a big home care organisation is nice because they can provide many different services besides care, but working with just one such organisation is a risk. If you hear that they struggle getting enough staff, you worry: is it going to be okay? (Practice Nurse GP)'. Collaborating with just one organisation or GP brings benefits, but a risk for the continuity of care. Also, working closely together with a technology company involves the risk of being dependent of the company’s continued existence, its choices and priorities. Finally, focus on positive health was not mentioned at all.
Barriers and facilitators for technology-based IPC
Summary of facilitators and barriers from the three perspectives.
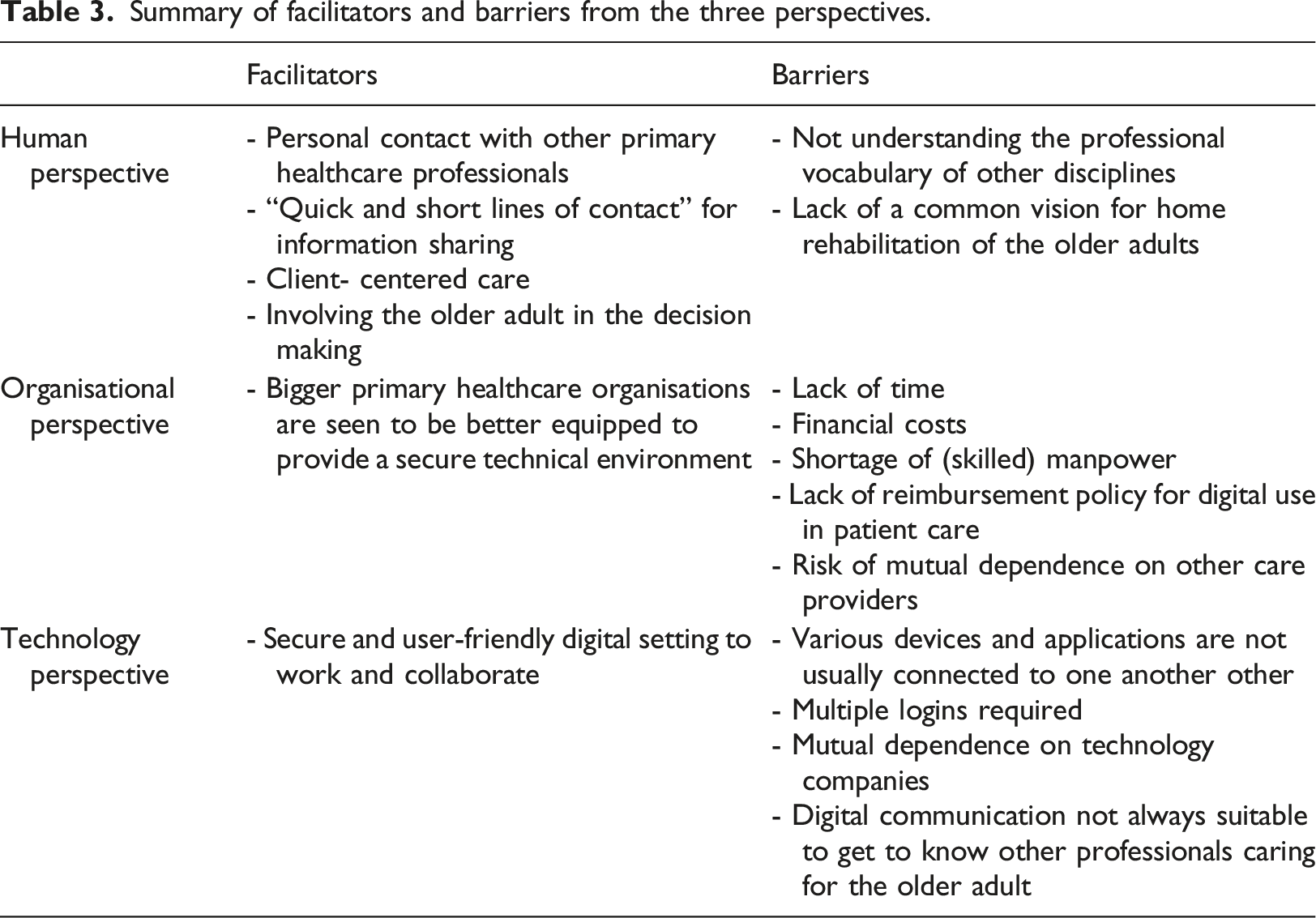
Human perspective
Personal contact with other primary healthcare professionals is seen as a facilitator: it makes IPC easier and allows parties to get to know one another. In addition, quick and short lines of contact” facilitate the sharing of (digital) information quickly. In the relational sense, it means professionals can be “on the same page”. For the client, it provides confidence in the care provided given that his or her primary healthcare professionals know each other. Involving the client in decision making without being overburdened is desirable. While there is a need for a CCC approach, not enough attention is given to it in practice. With respect to the barriers, not understanding the other professional’s vocabulary and ways of working restricts adequate knowledge and information sharing. Furthermore, a lack of a common vision hinders an interprofessional home rehabilitation of older adults.
Organisational perspective
A lack of time, financial costs, shortage of (skilled) manpower, lack of reimbursement policy for digital use in patient care are seen as barriers IPC. In addition, mutual dependence is seen as risk when the organisation only works with one other organisation.
Technological perspective
The potential of technology for IPC is acknowledged. However, there are barriers relating to: 1) the access and usability of devices and applications; 2) the way digital information is communicated. In the current situation, primary healthcare professionals use various applications which are not usually connected to one another, each requiring separate logins. Having a secure and user-friendly digital environment to work and collaborate in is viewed as a facilitator. Bigger organisations where primary healthcare professionals work are seen to be better equipped to provide this secure environment. In this context, mutual dependence is mentioned as a risk when one organisation relies too much on the companies providing the technology. In addition, digital communication differs from real-life conversation. Face to face contact remains important for collaboration between the professionals but also between the professional and the client.
Results from the design thinking session
Participants
Participant information (design thinking).
Generated solutions
Group 1 chose the case study of an older adult in need of a hip replacement. The group focused on a solution providing fast, up-to-date and efficient insight into the medical report and other related health information, making it easy for the primary healthcare professionals to be involved when needed, supporting clear communication and providing unambiguous advice to the patient.
Group 2 chose the case study of an older adult with co-morbidity (78+). The group advocated a solution focused on an “intelligent” patient record, each discipline having its own “box” to be shared with other disciplines and also allowing collegial consultation.
Even though the chosen case study of the older adult was slightly different in each group, both groups came up with similar aspects related to human, organisation, and technology. Differences occurred during the analysis when some phrasing was put in a different category by the team of researchers. Consensus and discordance were reached through discussions and going back to the template to ensure context clarity.
Use of interprofessional collaboration themes in ICT solutions
Summary of themes of interprofessional collaboration addressed in the design thinking session.
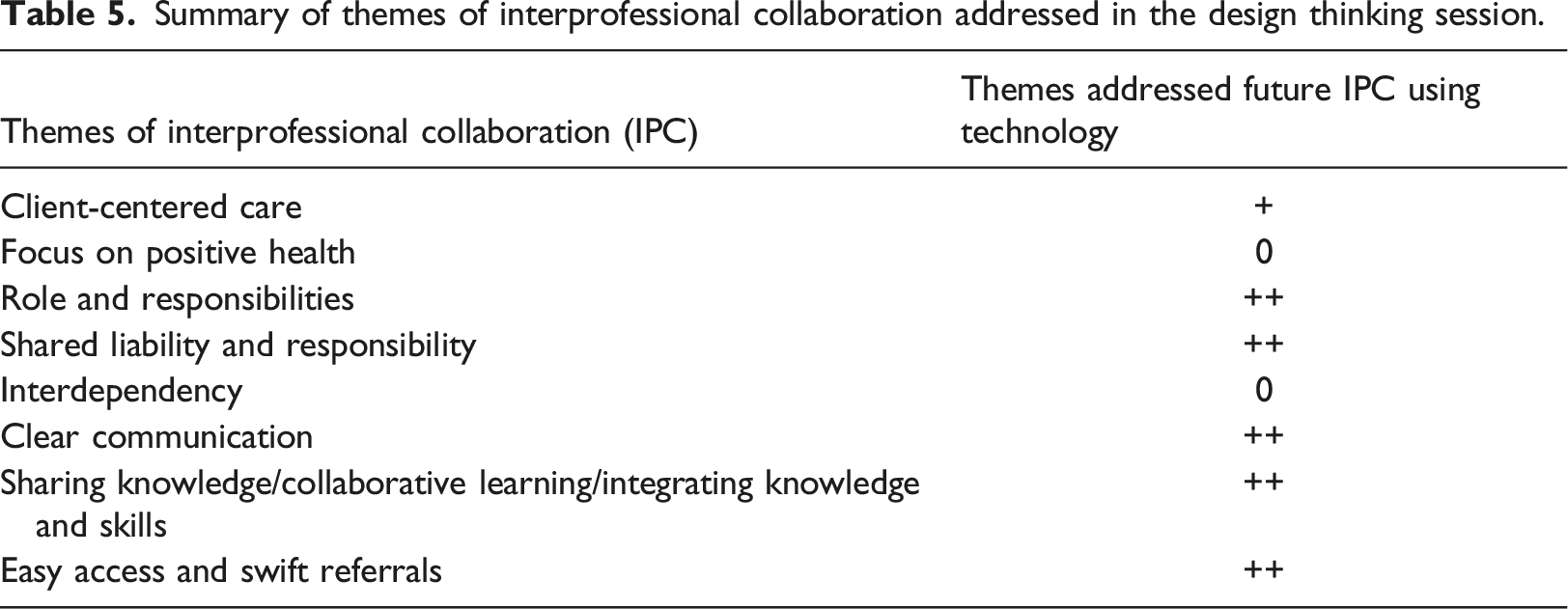
When thinking about technological solutions to facilitate IPC, clear communication, sharing knowledge and collaborative learning, and easy access are mentioned. Clear communication is mentioned in terms of efficiency, for example, clients not having to repeat themselves with each new professional. Professionals being able to learn from each other and learn how to use the ICT application are examples of sharing knowledge and collaborative learning. Easy access is mentioned in terms of better access for professionals to patient information. This can increase efficiency, by saving time, lowering costs and reducing administrative tasks. Easy access is also mentioned in terms of coupling existing applications and devices used by professionals clients.
Roles and responsibilities and shared liability and responsibility are also frequently mentioned when thinking about ICT solutions. This can be at the professional level (e.g. having the right ICT skills) and at the organisational level (e.g. providing the financial means). In term of shared liability and responsibility, compliance with governmental regulations, authorisation of access and coordination of task are mentioned. CCC and interdependency were rarely mentioned. Positive health was not mentioned.
Thematic clustering of solutions using three perspectives
Thematic clustering of solutions from the design thinking session.
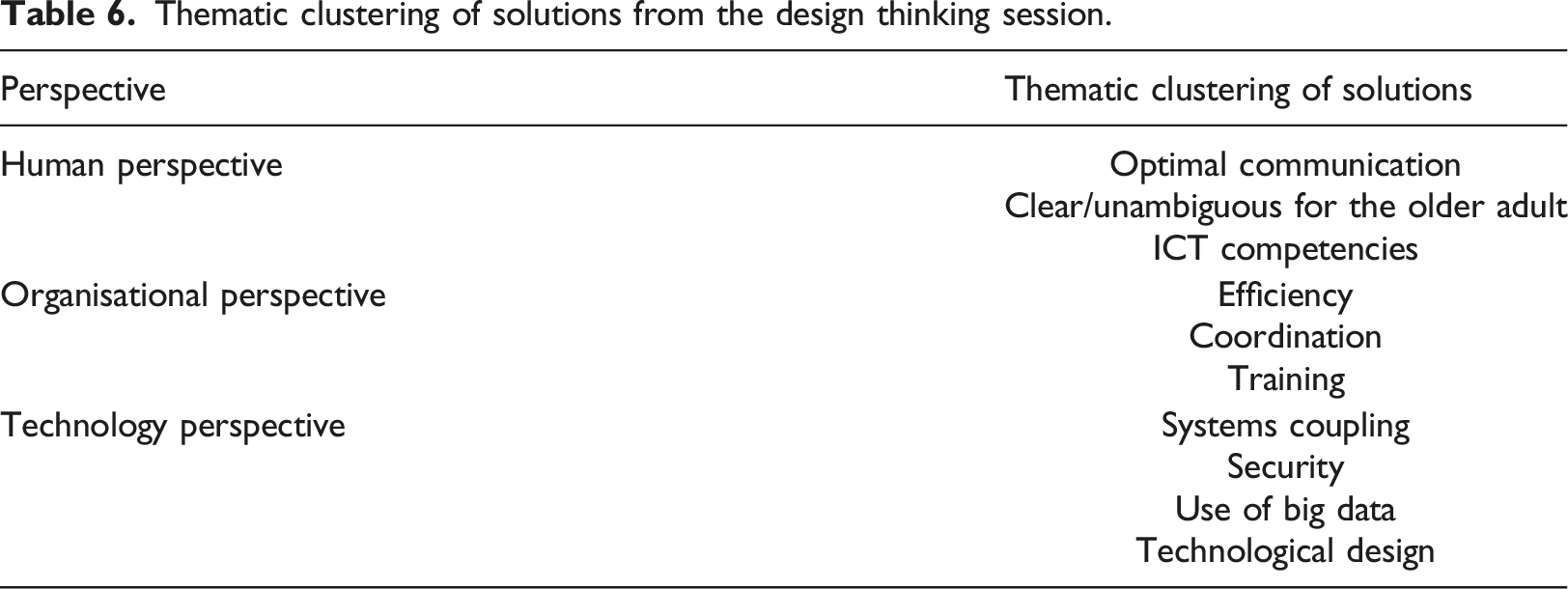
Human perspective: solutions should support optimal communication amongst primary healthcare professionals. In this way, the healthcare professionals learn from each other and get to know one another better. Optimal communication means clear communication with the older adult. In addition, this means that the older adult does not have to constantly repeat the same information to each primary healthcare professional. Using a technology-based solution also implies that the primary healthcare professionals should have the necessary ICT skills to use it.
Organisational perspective: the solutions should provide efficiency in terms of time savings, lower costs and reduced administrative tasks, better treatments for the older adults and access to patient information. The solutions allow the organisation to authorise the sharing of information to primary healthcare professionals and support the division of tasks. In this context, the solution could facilitate the coordination of health-related tasks and access to digital information. In addition, the organisation should ensure training for the professionals to use the technology solution and provide funding to develop and implement the solution within national regulations (such as data privacy).
Technological perspective: the solutions should ensure the coupling with the existing applications used by the primary healthcare professionals and by the older adults such as wearables. “The tools are there, they just need to be linked. Work digital if possible, live when necessary” (physical therapist). Furthermore, the technology solutions should handle issues such as data security and manage big data of similar groups of older adults. The technical design of the solution should be aligned with users’ needs. Some user requirements have already been mentioned, including user-friendliness and ease of use, a virtual room per discipline, visible to the other disciplines and a shortcut for contacting a specific discipline. At the same time, the involvement of the older adult in developing the innovation should be given consideration.
Discussion
The three themes which emerged from the focus groups and the design thinking session are intertwined. To start with, a topic mentioned in both sessions was the importance of having personal professional contact with other disciplines to ensure efficient communication and to engage patients providing a CCC approach for IPC. This could help in understanding each other’s professional vocabulary and developing a shared vision for home rehabilitation of older adults. In order to do so, Schot, Tummers and Noordegraaf 22 advocate bridging professional social, physical and task-related gaps by negotiating overlaps in roles and tasks, and by creating spaces to do this.
The research reported here provides empirical evidence of the need for IPC for community-based rehabilitation of the elderly. This corroborates with other studies (e.g. ), 23 recognising the value and importance of IPC when caring for older adults. IPC can be seen as “the gatekeeper to breaking down “siloed” thinking in healthcare and enabling a culture of care that remains inclusive, comprehensive, and holistic for the care of seniors”. 24 The research reported here does not clearly identify “siloed” thinking amongst the primary healthcare professionals but may indicate an underlying contributing factor, such as a lack of understanding of each other’s professional vocabulary.
In the context of IPC, CCC is reported as being an important aspect. 25 This is in line with the results from the focus group indicating the need for a CCC approach in the home rehabilitation of older adults.
It is acknowledged that technology can play an important part in bringing innovation to IPC. However, “until IPC becomes an accepted strategy for change, significant conflicts will remain. ICT applications may provide new and effective tools to promote information gathering and communication”. 26 The study reported here provides initial steps that could be taken towards a strategic change by developing a common vision for community-based rehabilitation of the elderly and by ensuring the coupling of ICT applications used by primary healthcare professionals. While primary healthcare professionals do use ICT applications, these are often not connected to one another, making digital-based collaboration difficult. Both primary healthcare professionals and older adults should be involved in the design of a technology-based solution that supports IPC. Furthermore, such solution should provide a user-friendly digital environment in which to work and collaborate. In this context, the organisation plays an important role in ensuring that primary healthcare professionals can be trained to use the technology.
Results from this study may prove useful towards achieving these objectives. Similarly, our findings relating to the technology – e.g. facilitating and hindering factors – will help the development of future technological solutions. While this exploratory study has been carried out with a limited number of participants, it has provided a foundation for further work. To start with, there is a need to study how the aforementioned barriers should be addressed and solved in practice. In addressing these barriers, further research should take into account how community-based rehabilitation of older adults can be best organised amongst the allied healthcare professions in order to provide an interdisciplinary home rehabilitation. In future research general practitioners should also be involved since they coordinate the overall management of the medical and community-based rehabilitation care. Finally, the participation of the older adults should not be forgotten and should be at the forefront of further research in order to understand the wishes and needs of the older adults in relation to personalised and client-centred rehabilitation at home.
The limitations of the study include the small number of participants and the length of the study (12 months). In addition, the selection of the participants was confined to one district, and as such some of participants knew each other. While it may be seen as a bias, it also may have been an added value to stimulate the discussion.
Conclusions
Primary healthcare professionals who participated in this exploratory study recognise the urgency of working collaboratively, having a better understanding of each other’s professional vocabulary, engaging the older adults, and using technology under certain conditions to support this process within the community environment of the patients. While primary healthcare professionals do use ICT applications, there is a feeling that these technologies are not connected, restricting efficient IPC. The components of IPC need to be further researched in order to integrate them into a technological solution.
Footnotes
Author note
We would like to thank all participants of the focus group and design thinking session for their time and valuable input they provided. This study was financed by the Centre of Expertise Prevention in Healthcare and Wellbeing of the Inholland University of Applied Sciences and the Dutch Vitale Delta Research Program.
Ethical statement
This manuscript reports on an exploratory study. The participation to the focus groups and design thinking sessions was voluntary and the participant was allowed to quit at any time. The ethical approval was not required in the Netherlands, however the research was conducted in line with the Helsinki Declaration. Participants were informed of the study en verbal consent was given by all the participants. Details regarding this have been included in the manuscript. The study was financed by our institution/department and as such ethical aspect of the study was taken into consideration during the review process of the study proposal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by internal funding from the Centre of Expertise Prevention in Healthcare and Wellbeing of the Inholland University of Applied Sciences and the Dutch Vitale Delta Research Program.