
Abstract
Objective
With the rise in public health awareness and the rapid development of digital healthcare services, users’ perceptions of platform corporate social responsibility (PCSR) have become an important factor influencing behavioral intention (BI) to use online healthcare platforms.
Methods
Drawing upon the technology acceptance model (TAM) and customer perceived value (CPV) theory, this study develops a moderated mediation model in which perceived ease of use (PEU) and perceived usefulness (PU) mediate the relationship between PCSR and BI, while privacy concerns (PCs) moderate this relationship. A mixed-methods approach is adopted, integrating structural equation modeling (SEM) with necessary condition analysis (NCA), to examine both the sufficiency and necessity of the proposed conditions.
Results
The SEM results indicate that PCSR positively affects BI both directly and indirectly via PEU and PU. In addition, PC significantly weakens the positive effect of PCSR on BI. The NCA results further reveal that PU and PCSR are necessary conditions for users’ intention to use online healthcare platforms.
Conclusion
This study advances the theoretical understanding of TAM in high-sensitivity service contexts, expands the application of PCSR in the domain of digital health, and provides actionable insights for online healthcare platforms seeking to enhance user engagement through socially responsible and privacy-aware strategies.
Keywords
Introduction
With the continuous advancement of internet technology and the growing structural imbalance in healthcare resources, online healthcare platforms have rapidly emerged as a vital supplement to traditional medical systems. 1 Various public health crises have further exposed the limitations of offline medical services. During the COVID-19 pandemic, visiting hospitals not only increased the risk of cross-infection among patients but also posed similar risks to healthcare professionals.2,3 These events have underscored the value of online healthcare services—which can maintain continuity of care while reducing physical contact. Platforms such as Haodf, Chunyu Doctor, and WeDoctor offer services like online consultation, telemedicine, and health management, which help overcome geographic and resource barriers. These platforms significantly improve the accessibility and efficiency of healthcare, addressing the increasing diversity of public health needs.4,5 However, as platform services expand, issues related to trust between users and platforms have become increasingly prominent. Problems such as insufficient user awareness, misinterpretation of data privacy laws, and a general lack of public trust have severely hindered the widespread adoption of online healthcare platforms,6,7 with many users adopting a cautious “coexistence of expectation and concern” attitude toward them. Due to the high sensitivity of personal health information and the irreversible nature of medical decisions, users tend to adopt a more cautious attitude toward online healthcare services. 8 Beyond technical capabilities and service quality,9,10 how platforms can strengthen user trust and promote behavioral intention (BI) through the fulfillment of corporate social responsibility (CSR) has become a pressing question.
Although prior studies in traditional consumer contexts have demonstrated that perceptions of CSR positively influence brand evaluation, 11 purchase intention,12,13 and customer loyalty,14–16 the mechanisms through which CSR affects user behavior in the context of online healthcare—characterized by high sensitivity, complexity, and perceived risk—remain underexplored. In recent years, studies have pointed out that online healthcare platforms often operate in complex scenarios involving health information processing and privacy data governance, giving rise to ethical, legal, and acceptance-related challenges that are more pronounced than those in conventional industries.17–19 The high sensitivity of medical data, along with the fact that medical decisions directly concern patients’ health and life safety, leads users to set higher trust thresholds and pay particular attention to the platform's fulfillment of responsibilities in areas such as transparent data management and patient well-being. 20 Therefore, perceived CSR (PCSR) may serve as an important psychological antecedent influencing users’ adoption behavior in this context. On the one hand, the online healthcare experience involves greater information asymmetry and decision risk, which may increase reliance on non-economic cues such as users’ perceptions of PCSR. On the other hand, empirical research remains limited on how PCSR translates into actual behavioral outcomes through perceived technological value, namely perceived usefulness (PU) and perceived ease of use (PEU). Furthermore, privacy concerns (PCs) have been shown to influence online behavior significantly 21 and may play a moderating role in this process.22,23 In contexts involving personal health data, users with higher PCs may respond differently to the same platform initiatives.
To address these research gaps, this study aims to systematically examine how users’ perceptions of PCSR influence BI to use online healthcare platforms. Specifically, PEU and PU are proposed as mediating variables, while PCs are incorporated as a moderator to capture users’ varying sensitivity to information disclosure. Technology acceptance model (TAM) is adopted because PU and PEU have consistently been validated as core predictors of user adoption intentions in healthcare technology contexts such as telemedicine, health IoT, and non-contact services.24,25 Introducing PCSR as an external variable helps extend the applicability boundaries of the TAM framework in high-sensitivity healthcare contexts and reveals its social value pathways. This study adopts a mixed-methods approach, integrating structural equation modeling (SEM) and necessary condition analysis (NCA). SEM is employed to identify causal relationships among variables and test the hypothesized model, while NCA is used to uncover necessary conditions and critical thresholds that constrain users’ behavioral outcomes. Unlike SEM, which reveals sufficiency, NCA helps identify whether any antecedent is indispensable for achieving high BI—thereby capturing the compensatory or conjunctural logic of user adoption in a more nuanced manner. By combining these two methods, this study offers a more comprehensive perspective on both the sufficiency and necessity of influencing factors. 26 The findings contribute to the literature by extending the boundary conditions of PCSR in sensitive digital service environments, enriching the explanatory framework of the TAM, and offering practical guidance for online healthcare platforms aiming to improve user adoption through responsible and privacy-conscious strategies.
Theoretical background
TAM
Davis 27 proposed based on the theory of reasoned action and incorporating elements from self-efficacy theory and expectancy theory, the TAM aims to explain the adoption of information technology within organizational contexts. 28 However, extensive research has demonstrated that, with appropriate extensions and modifications, TAM is equally applicable to user acceptance of new technologies or systems. The model is widely recognized for its strong predictive and explanatory capabilities, as well as its robustness and adaptability across diverse research scenarios. TAM posits that external factors influence users’ BI by shaping their PU and PEU of a system. Since the model does not specify the exact nature of “external factors,” scholars have subsequently explored various external antecedents, including demographic traits, usage environments, technological maturity, and temporal dynamics. 29 In the field of medical and health technologies, TAM has been widely applied to explain users’ BIs to adopt contactless healthcare services, 30 business intelligence, 24 health Internet of Things, 25 telemedicine 18 and big data analytics tools. 17 Research has shown that, in healthcare contexts, PU and PEU remain core factors in predicting users’ BIs to use digital health services, and that external contextual variables such as social influence, security, and privacy can affect the formation paths of PU and PEU. 31 In the present study, users’ perceptions of PCSR is introduced as a key external variable to further elucidate the formation mechanism of user adoption behavior within the TAM framework.
Customer perceived value (CPV) theory
CPV theory was initially defined as a trade-off between perceived benefits and perceived sacrifices made by the customer.32,33 Early models often adopted a unidimensional structure and overlooked experiential aspects of consumer behavior. Subsequently, Sheth et al. 34 developed the theory of consumption values, which incorporated multiple dimensions—including emotional, cognitive, functional, social, and conditional values. Holbrook and Schindler 35 later expanded this into eight consumption value dimensions. With the rise of e-commerce and mobile technologies, scholars have contextualized CPV theory across various digital settings. For instance, Mathwick et al. 36 proposed an experiential value model, and Overby et al. 37 differentiated between utilitarian and hedonic values. These adaptations highlight that the perceived value dimensions can vary significantly by platform context. CPV theory thus provides a multidimensional analytical framework for understanding consumer behavior in diverse scenarios and has been widely applied in emerging digital domains such as online healthcare and mobile payment services. 38
PCSR perception and BI
CSR refers to a company's voluntary commitment to economic, legal, ethical, and philanthropic responsibilities while pursuing business objectives. 39 This concept emphasizes that enterprises should look beyond shareholder value and consider a broad range of stakeholders, including employees, customers, communities, and governments.40,41 As public awareness of corporate responsibility grows, increasing attention has been paid to how users’ perceptions of CSR influence attitudes and behaviors. 42 Earlier studies primarily focused on a single dimension of CSR, such as environmental or philanthropic efforts, and failed to capture users’ holistic CSR perceptions.43,44 Later research introduced multidimensional CSR measurement frameworks—encompassing economic, legal, ethical, and philanthropic responsibilities—to better represent users’ evaluative structures. 45 Online healthcare platforms often involve complex scenarios such as health information processing and privacy data management, where the resulting ethical, privacy, legal, and technology acceptance issues are more pronounced than in other industries.17,46 Medical data are highly sensitive, and medical decisions are directly related to patients’ health and even life safety; therefore, users tend to have higher trust thresholds and safety expectations when evaluating such platforms. For example, in the context of medical artificial intelligence, users often exhibit a “coexistence of expectation and concern” mindset—on the one hand, acknowledging its potential to improve efficiency, 47 on the other hand, remaining cautious or even resistant due to risks of misjudgment and unclear ethical accountability.48,49 Existing studies have shown that, in research on contactless healthcare services and blockchain-based healthcare technologies, perceived platform responsibility is regarded as a key antecedent influencing users’ trust and willingness to adopt. 2 Although CSR has been extensively studied in traditional industries, related research within the emerging context of online healthcare platforms remains relatively limited. Given that these platforms operate in a context of high user dependency and sensitivity, users pay particular attention to the fulfillment of platform responsibilities in areas such as transparent data management and patient well-being. Accordingly, CSR practices in online healthcare platforms are not only relevant to corporate image but may also profoundly influence users’ trust in and willingness to use the platform. 20 Therefore, introducing PCSR into this emerging context helps decode its behavioral mechanism and provides a theoretical basis for building trustworthy platform–user relationships.
PCs
PCs refer to users’ apprehensions about the collection and use of their personal data by digital platforms. These concerns are shaped by cultural background, legal context, individual characteristics, and prior experiences. 21 Due to the conceptual complexity of privacy and its reliance on user perception rather than objective judgment, empirical studies often assess PC through cognitive, attitudinal, and perceptual dimensions. In recent years, PC has become a core variable in information systems research, frequently employed to measure user privacy attitudes. 50 In digital health scenarios such as contactless medical services and blockchain-based healthcare, privacy and security are widely recognized as critical barriers to users’ adoption intentions.31,51 Platforms may collect information through user interactions or even without user awareness. 52 Concerns that health data could be accessed without authorization, misused, or transferred across borders may reduce patients’ willingness to use such platforms, and the absence of transparent data usage policies can further intensify these PCs. 2 Empirical evidence indicates that, within healthcare contexts, privacy issues constitute the most significant predictors of users’ BIs. 53 In this study, PC is introduced as a moderating variable to capture the differential responses of users with varying levels of PC in the behavioral mechanism model.
Hypotheses development
PCSR and BI
PCSR is conceptualized as a second-order reflective construct consisting of four first-order dimensions 45 : (1) SCSR (social responsibility)—the platform's contribution to society; (2) CCSR (customer responsibility)—commitment to protecting customer rights and ensuring service quality; (3) BCSR (shareholder responsibility)—ethical governance and transparent disclosure toward shareholders; and (4) ECSR (employee responsibility)—fair treatment, training, and development opportunities for employees. According to CPV theory, users form overall value perceptions by evaluating the trade-off between perceived benefits and perceived costs, which in turn influence their BIs. In this context, users’ perceptions of PCSR serve as critical signals that shape both perceived benefits and perceived costs, thereby affecting users’ willingness to use online healthcare platforms.
On one hand, PCSR enhances users’ perceived benefits, leading to more favorable evaluations of platform value. In practice, CSR activities such as providing free health education or organizing charitable medical consultations can enhance both the functional and affective value perceived by users, thereby increasing the overall attractiveness of online healthcare platforms. From a cognitive perspective, CSR practices can increase user recognition and emotional identification with the platform, thereby strengthening their BI. Previous research has confirmed that a positive CSR image can improve consumers’ overall evaluation of a company and increase their purchase intentions. 54 A positive relationship has been observed between CSR and consumer attitudes and behaviors.55,56 From an affective perspective, CSR activities such as charitable health initiatives or public health education can evoke favorable sentiments and emotional attachment, thus reinforcing the emotional bond between users and the platform. Related studies have shown that fulfilling social responsibilities aligns with users’ moral expectations of companies57,58
On the other hand, PCSR can lower users’ perceived costs by alleviating the uncertainty in using online healthcare platforms. In practice, simplifying appointment and registration procedures or providing dedicated consultation channels can reduce perceived risks, learning costs, and operational complexity. Moreover, transparent information disclosure—a core component of CSR practices—can mitigate distrust. Event-based research has shown that the active disclosure of CSR-related information can positively influence investor behavior, 59 suggesting that CSR enhances transparency and trust, thereby increasing users’ BI. 60 Considering the inherent uncertainty associated with online healthcare platforms, users may prefer service providers with reputable CSR records to reduce perceived risk. Prior studies have revealed that consumers are more likely to choose products from socially responsible companies, 61 particularly when direct product experience is lacking. In such cases, CSR perceptions serve as heuristic cues to infer service quality, thereby shaping usage preference.
The mediating role of PU and PEU between PCSR and BI
To further clarify the mechanisms through which PCSR influences user behavior, this study introduces the TAM as a theoretical framework. TAM posits that PEU and PU are critical antecedents of BI. 62 PEU is defined as the degree to which a person believes that using a specific system would be effortless. 27 In this study, it refers to users’ perceptions of how easy it is to use the online healthcare platform. PU refers to users’ beliefs that using a system enhances their efficiency or performance. 27 Here, it is conceptualized as the extent to which users believe that the online healthcare platform improves service efficiency and reduces time and effort. To further explain the mechanisms through which PCSR influences PEU and PU, this study incorporates additional analysis based on the CPV theory. It posits that specific CSR practices undertaken by platform enterprises can improve users’ value assessments regarding the convenience and utility of using the platform, thereby shaping their subjective perceptions of ease of use and usefulness.
On the one hand, PCSR can ease users’ operational burden by enhancing platform functionality and user interface friendliness. Prior studies have shown that social support—such as informational and emotional support—can significantly lower usage barriers and enhance user experience.63,64 Prior research has indicated that positive user experience with system usability promotes favorable attitudes, which subsequently influence behavioral outcomes. 65 For example, Haodf.com offers disease consultation, online diagnosis, and health information exchange services. 66 Through user-friendly design and rich health information resources, such platforms reduce access difficulty and facilitate appointment booking and consultation for elderly users. These measures lower learning costs, minimize operational errors, and improve interface perceptions, thereby enhancing users’ overall evaluation of the platform's ease of use.
On the other hand, PCSR can strengthen perceptions of platform professionalism and service effectiveness, leading users to believe that the platform offers clear advantages in improving medical efficiency and reducing diagnostic costs. Research has shown that both cognitive and affective trust are key drivers of users’ continued adoption of online healthcare platforms, 67 and that providing authoritative, reliable health information significantly reduces uncertainty about platform performance, thereby increasing PU. 68 Moreover, a fair, transparent, and ethical environment can further enhance users’ trust and reinforce platform credibility. 69 For example, CSR initiatives such as partnering with top-tier hospital doctors, launching rare disease education columns, and enabling remote diagnostic services not only convey the platform's public value but also raise users’ expectations of its diagnostic efficiency, thereby boosting PU.
Furthermore, CSR initiatives that promote public health literacy and enhance patient experience can strengthen users’ perceptions of PU and PEU. Specifically, positive CSR practices boost trust in platform friendliness and service quality,70,71 thereby lowering perceived barriers. Additionally, CSR actions that address social concerns help form positive user impressions, 72 which can enhance evaluations of usefulness. Therefore, PCSR is expected to not only directly influence BI but also exert indirect effects via the mediators of PU and PEU.
The moderating role of PCs
PCs examine the extent to which users are concerned about how their personal information is collected and utilized by the platform in an online healthcare context. Prior studies on online services have shown that PC is significantly and negatively associated with online transaction intention. 73 Alzaidi and Agag 30 found that users with high PC are less likely to adopt location-based mobile commerce services. In the case of online healthcare, users with high PC may question the underlying motives of the platform's CSR initiatives, suspecting that such efforts are veiled attempts to harvest sensitive personal and health data. This increases the perceived risk of privacy violations. 71 Therefore, for users with high PC, the positive effect of PCSR on BI may be attenuated or even neutralized due to heightened concerns about data misuse.
The conceptual model is shown in Figure 1.
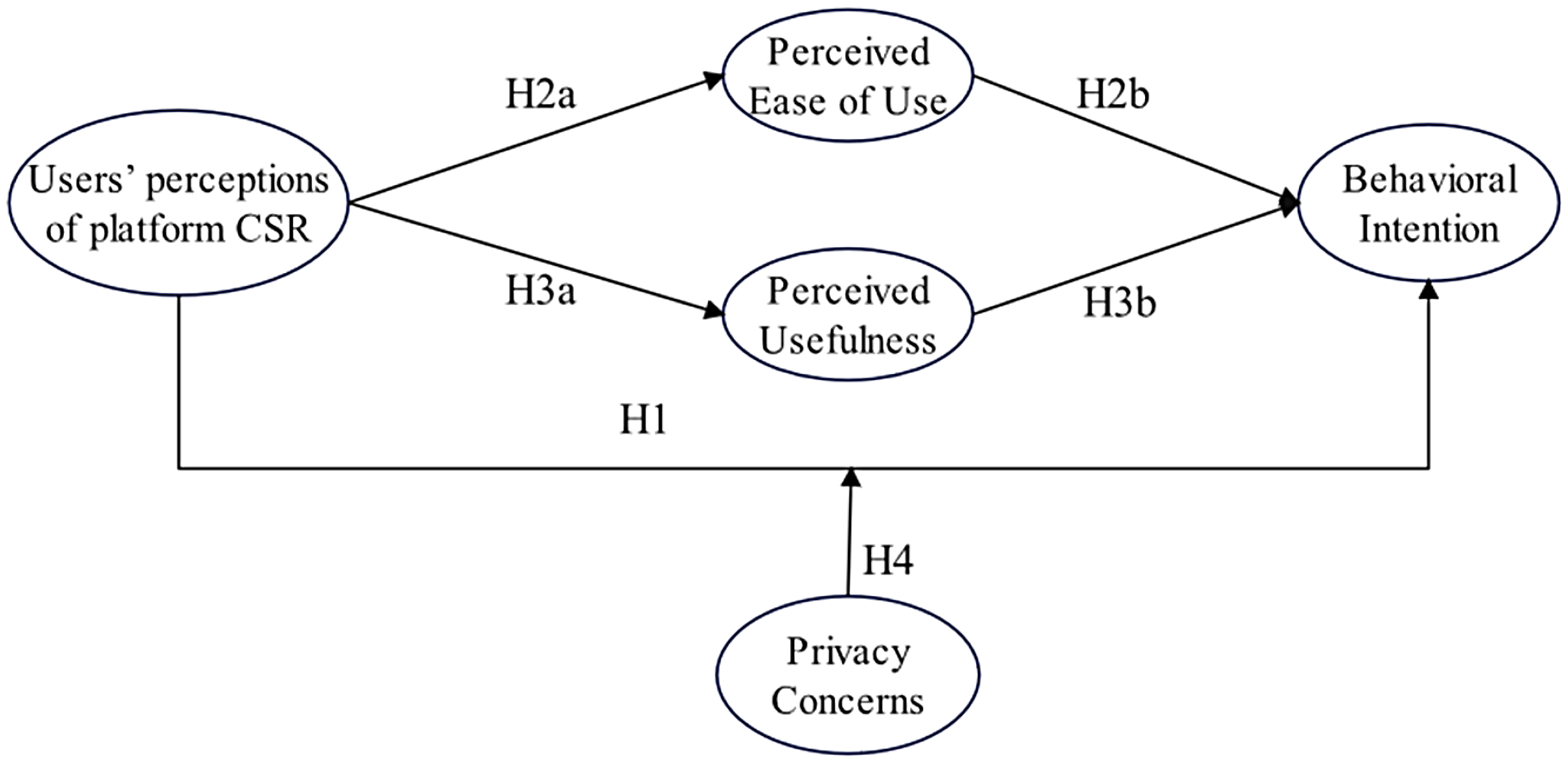
Conceptual model.
Methods
Necessary conditions refer to those antecedents without which the outcome cannot occur. NCA quantitatively assesses the minimum level of a given antecedent required for a particular level of the outcome to be achieved. Therefore, a mixed-methods approach—combining SEM and NCA—is employed in this study to simultaneously uncover both sufficient and necessary causal mechanisms, thus offering a more complete explanation of user behavior in the online healthcare context. SEM is used to validate causal paths and assess sufficiency logic, while NCA identifies threshold conditions and constraints, thereby addressing the limitations of traditional modeling techniques.
Sample selection and data collection
This study received ethical approval from the Institutional Review Board of the School of Management, Zhejiang University of Finance and Economics. The Board reviewed the research program, which involved an online questionnaire survey distributed through platforms such as Wenjuanxing. It confirmed that participants were fully informed of the study's purpose before participation and that submission of the questionnaire was regarded as informed consent, with the option to withdraw at any time. The Board further noted that the study posed no harm or risk to participants, did not involve sensitive personal data, and was based on voluntary participation and protection of participants’ rights and privacy. For the 29 participants under the age of 18, their participation was deemed to have been conducted with the implied consent of their legal guardians. The Institutional Review Board concluded that the research design and protocol were scientifically sound, fair, and ethically compliant, and therefore approved the project to proceed as planned.
This cross-sectional empirical study employs a mixed quantitative approach integrating structural equation modeling (SEM) and necessary condition analysis (NCA) to systematically explore key factors influencing users’ adoption of online healthcare platforms. Data were collected through an anonymous online questionnaire survey from March to April 2025 across mainland China. The survey was distributed via Wenjuanxing, a widely used online survey platform, targeting users with actual experience using online healthcare platforms. The questionnaire consisted of three sections: The first section introduced the research purpose and included a screening question to exclude respondents who had never used online healthcare platforms, thereby enhancing data relevance and reliability. The “Methods” section collected basic demographic information, including gender, age, income, internet usage experience, occupation, and frequency of using online healthcare services. The third section measured the constructs of interest, such as PCSR, BI, PU, PEU, and PC.
A non-probability purposive sampling method was employed to recruit respondents with actual experience using online healthcare platforms. This approach ensured that the collected data were relevant to the research context. To justify the sample size, we referred to established SEM guidelines recommending at least 10 cases per observed variable. Our SEM model contains 33 observed variables, indicating a minimum required sample size of ∼330. The valid sample size of 553 thus substantially exceeded this threshold, providing robust statistical power for model estimation and hypothesis testing.
A total of 636 questionnaires were distributed. After removing 83 invalid responses (e.g. too short response times, uniform selections, and logically contradictory answers), 553 valid questionnaires were retained, yielding an effective response rate of 86.94%.
Measurements
Drawing upon established CSR literature, 74 PCSR was conceptualized as a second-order reflective construct comprising four distinct first-order dimensions: SCSR, CCSR, BCSR, and ECSR. The measurement model was assessed in two stages: (1) first-order CFA to evaluate each dimension's reliability and validity; (2) second-order CFA treating the four validated dimensions as reflective indicators of PCSR. Since the hypotheses were formulated at the aggregate PCSR level, SEM analysis used PCSR as a single latent construct, while NCA was conducted for the four individual dimensions.
This study measured the following constructs: users’ perceptions of PCSR—including social (SCSR), customer (CCSR), shareholder (BCSR), and employee (ECSR) dimensions, BI, PEU, PU, and PCs. All measurement items were adapted from well-established scales and revised to suit the context of online healthcare platforms. To ensure semantic accuracy and contextual equivalence of the translated items, a standard Brislin back-translation procedure was employed. All items were measured using a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The full list of adapted items—along with their original Chinese phrasing and English back-translation—is provided in Appendix A for full transparency and replicability.
Specifically, the PCSR scale (20 items) was adapted from Pérez et al. 45 and Kim and co-authors, 75 encompassing four dimensions. BI was measured using a 3-item scale adapted from Davis. 27 PEU and PU were measured using three items each, adapted from Davis, 27 Wixom and Todd, 76 respectively. PCs were assessed with four items derived from Kim et al. 21 In addition, based on previous literature, 77 demographic characteristics, including gender, age, education, and occupation, were included as control variables in the analysis.
Results
Demographic characteristics
Among the valid sample, 49% were male and 51% female. In terms of age, users aged 19–30 and 31–45 made up the majority (41% and 35%, respectively). Regarding education level, undergraduate degrees accounted for the highest proportion (37%), followed by associate degrees (33%). Most respondents were enterprise employees (59%). Monthly disposable income was mostly concentrated in the 3000–5000 CNY range (43%). Regarding internet usage, 92% had more than 10 years of online experience, indicating substantial familiarity with digital environments. As for usage frequency, 298 respondents (54%) had used online healthcare platforms 1–3 times in the past year. In terms of health status, 64% of respondents reported not having any chronic illness (see Table 1).
Demographic information (n = 553).

Source: Author's data analysis.
Note: SD: standard deviation.
Common method bias test
To mitigate the impact of common method bias on the results, both procedural and statistical remedies were applied. At the ex-ante stage, respondents were informed that the survey was anonymous and confidential, and that their responses would be used solely for academic research purposes. These precautions aimed to reduce social desirability and evaluation apprehension. At the ex-post stage, Harman's single-factor test was employed. An exploratory factor analysis was conducted using all measurement items. The Kaiser–Meyer–Olkin (KMO) value was 0.933, and Bartlett's test of sphericity was significant at p < 0.001. The variance explained by the first unrotated factor was well below the critical threshold of 40%, indicating that common method bias was not a serious concern in this study and that the data were suitable for further analysis.
Reliability and validity assessment
This study employed SPSS 27.0 to conduct reliability analysis for all constructs in the model. Internal consistency was evaluated using Cronbach's alpha (α) and corrected item–total correlation (CITC). As shown in Table 2, all CITC values were above the threshold of 0.5, and the deletion of any item did not result in a substantial increase in the corresponding α value; thus, all items were retained. The composite reliability (CR) for each construct exceeded the commonly accepted cutoff of 0.7, and Cronbach's α values were all above 0.8, indicating that the scales demonstrated high internal consistency and reliability.
Reliability and validity.

Source: Author's data analysis.
Note: PCSR: users’ perceptions of platform corporate social responsibility; SCSR: users’ perceptions of PCSR (society); CCSR: users’ perceptions of PCSR (customer); BCSR: users’ perceptions of PCSR (shareholders and supervisory boards); ECSR: users’ perceptions of PCSR (employee); BI: behavioral intention; PEU: perceived ease of use; PU: perceived usefulness; PCs: privacy concerns; CICT: corrected item-total correlation; CAID: corrected average inter-item correlation; α: Cronbach's α; FL: factor loadings; AVE: average variance extracted; CR: composite reliability. ∗∗∗ p < 0.001.
Confirmatory factor analysis (CFA) was performed using AMOS 23.0 to assess construct validity. The model demonstrated a good fit to the data, with key fit indices reported as follows: χ²/df = 1.497, RMSEA = 0.030, GFI = 0.931, and AGFI above acceptable thresholds. Convergent validity was supported by standardized factor loadings above 0.7 for all items, AVE values exceeding 0.5, and CR values above 0.7. Discriminant validity was verified by comparing the square root of each construct's AVE to its correlations with other constructs, which confirmed that each construct was distinct from the others (see Table 3).
Discriminant validity.

Source: Author's data analysis.
Note: PCSR: users’ perceptions of platform corporate social responsibility; SCSR: users’ perceptions of PCSR (society); CCSR: users’ perceptions of PCSR (customer); BCSR: users’ perceptions of PCSR (shareholders and supervisory boards); ECSR: users’ perceptions of PCSR (employee); BI: behavioral intention; PEU: perceived ease of use; PU: perceived usefulness; PCs: privacy concerns. The diagonal elements represent the square root of the average variance extracted (AVE) for each construct.
Hypothesis testing
The SEM model used PCSR as a second-order latent construct to align with the theoretical hypotheses. The four first-order CSR dimensions were validated in the measurement model and used in the NCA but were not included as separate predictors in the structural model.
To test the sufficiency of antecedent variables, SEM was conducted using AMOS 23.0. The results of the direct effects among variables are presented in Figure 2. After controlling for demographic variables, users’ perceptions of PCSR had a significant positive effect on BI (β = 0.322, p < 0.05), thus supporting H1. PCSR also significantly predicted PEU (β = 0.646, p < 0.001) and PU (β = 0.653, p < 0.001), confirming H2a and H3a. In turn, PEU (β = 0.205, p < 0.05) and PU (β = 0.248, p < 0.001) significantly influenced BI, thereby supporting H2b and H3b.

The structural model. The results of structural model testing. Source: Author's data analysis. Note: PCSR: users’ perceptions of platform corporate social responsibility; SCSR: users’ perceptions of PCSR (society); CCSR: users’ perceptions of PCSR (customer); BCSR: users’ perceptions of PCSR (shareholders and supervisory boards); ECSR: users’ perceptions of PCSR (employee). ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
For the NCA, we examined the four first-order CSR dimensions to identify whether specific dimensions represent necessary conditions for the outcome. To assess the necessity of antecedent variables, this study employed the NCA package in R. The analysis first evaluated the effect size of each antecedent variable. NCA includes two techniques: ceiling regression-free disposal hull (CR-FDH) for continuous variables and ceiling envelopment-free disposal hull (CE-FDH) for discrete ones. Given the characteristics of this study, CR-FDH was used to construct the ceiling line, while CE-FDH was also reported to test robustness. According to the threshold proposed by Dul et al. (2020), an effect size (d) > 0.1 with statistical significance (p < 0.05) is required to determine a necessary condition. As shown in Table 4, none of the antecedent variables met the criteria to be considered necessary conditions for influencing BI.
NCA necessary conditions analysis results.

Source: Author's data analysis.
Note: PCSR: users’ perceptions of platform corporate social responsibility; SCSR: users’ perceptions of PCSR (society); CCSR: users’ perceptions of PCSR (customer); BCSR: users’ perceptions of PCSR (shareholders and supervisory boards); ECSR: users’ perceptions of PCSR (employee); BI: behavioral intention; PEU: perceived ease of use; PU: perceived usefulness; PCs: privacy concerns. Effect size (d): 0.0 ≤ d < 0.1 = “low”; 0.1 ≤ d < 0.3 = “medium.” p-values were calculated via permutation tests (resampling = 10,000).
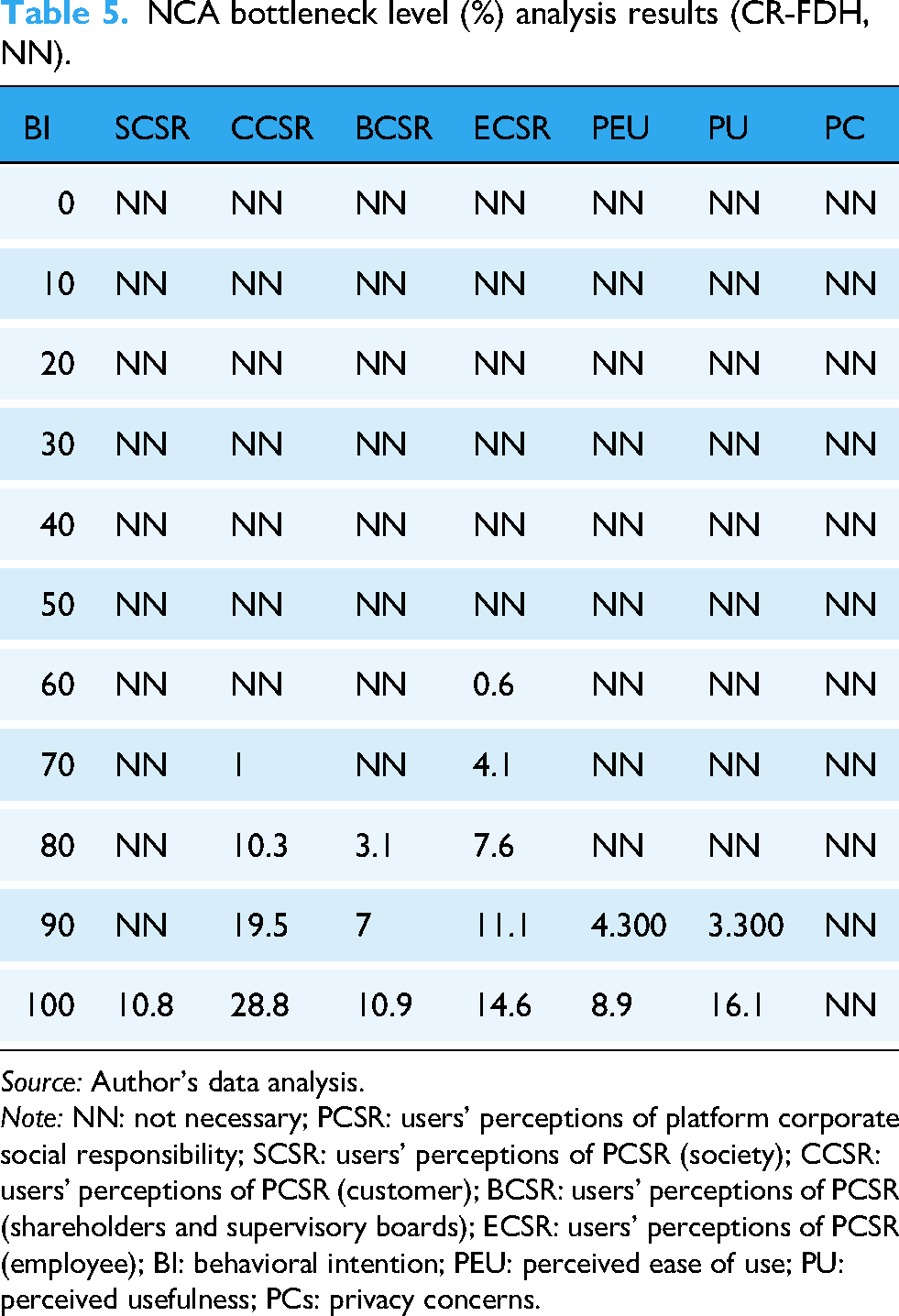
A bottleneck level analysis was also conducted to determine the minimum level of each condition required to achieve specific outcomes. As shown in Table 5, to reach 70% of BI, 1% of CCSR, and 4.1% of ECSR are required. Notably, PEU and PU only exhibit bottlenecks at the 90% level of BI, while PCs do not present any bottleneck threshold at any level.
NCA bottleneck level (%) analysis results (CR-FDH, NN).
Source: Author's data analysis.
Note: NN: not necessary; PCSR: users’ perceptions of platform corporate social responsibility; SCSR: users’ perceptions of PCSR (society); CCSR: users’ perceptions of PCSR (customer); BCSR: users’ perceptions of PCSR (shareholders and supervisory boards); ECSR: users’ perceptions of PCSR (employee); BI: behavioral intention; PEU: perceived ease of use; PU: perceived usefulness; PCs: privacy concerns.
Mediation analysis
To test the mediating effects, the bootstrapping method with 5000 resamples and a 95% confidence interval was applied, using custom Visual Basic code. As shown in Table 6, the total standardized effect of PCSR on BI was significant (β = 0.576, p < 0.001). The total indirect effect via PEU and PU was also significant (β = 0.295, p < 0.001), indicating partial mediation.
Bootstrapping results showing the mediating effects.

Source: Author's data analysis.
Note: PCSR: users’ perceptions of platform corporate social responsibility; BI: behavioral intention; PEU: perceived ease of use; PU: perceived usefulness.
Specifically, the indirect effect of PCSR → PEU → BI was significant (β = 0.133, p = 0.007), as was the indirect effect of PCSR → PU → BI (β = 0.162, p = 0.002). The direct effect of PCSR on BI remained significant after accounting for these mediators (β = 0.282, p < 0.001). Additionally, the 95% bootstrap confidence intervals for both indirect effects did not include zero, further supporting the significance of these mediations. These findings support hypotheses H2 and H3, confirming that PEU and PU partially mediate the relationship between PCSR and BI.
Moderation analysis
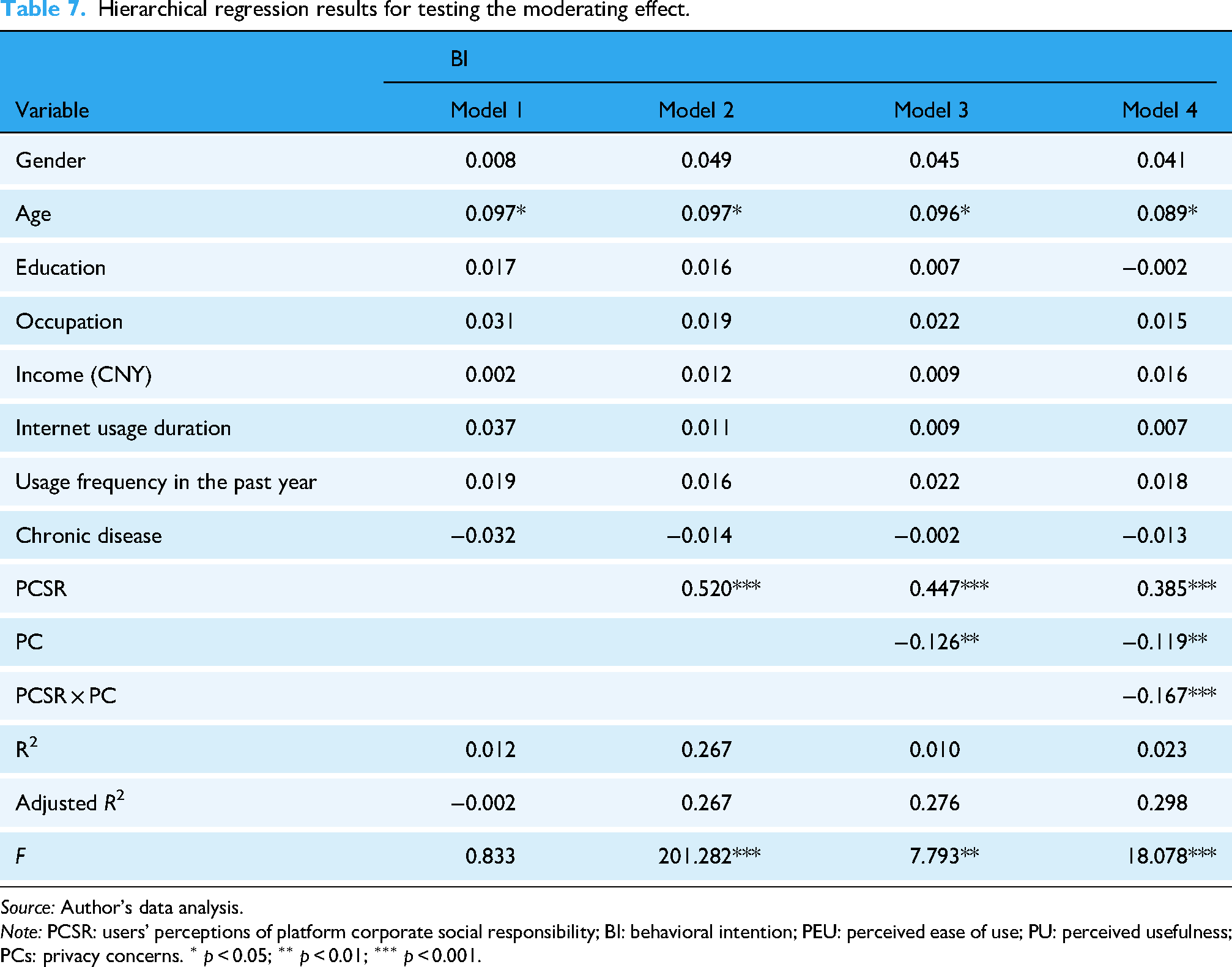
As shown in Model 4 of Table 7, the interaction term between PCSR and PCs had a significant negative effect on BI (β = –0.167, p < 0.01), and the corresponding F-value was significant, indicating a significant moderating effect. This suggests that PCs weaken the positive effect of PCSR on users’ BI, thus supporting H4. To further interpret the moderation effect, a simple slope analysis was conducted. As shown in Figure 3, when PC was low (–1 SD), PCSR had a strong positive effect on BI (β = 0.472, p < 0.001). At the mean level of PC, the effect remained positive and significant but weaker (β = 0.310, p < 0.001). However, when PC was high (+1 SD), the effect of PCSR on BI dropped substantially and became statistically nonsignificant (β = 0.148, p = 0.116). This pattern suggests that the positive influence of PCSR on users’ BI diminishes as PCs increase, ultimately disappearing when concerns are high. This again confirms the negative moderating effect of PCs, providing additional support for H4.
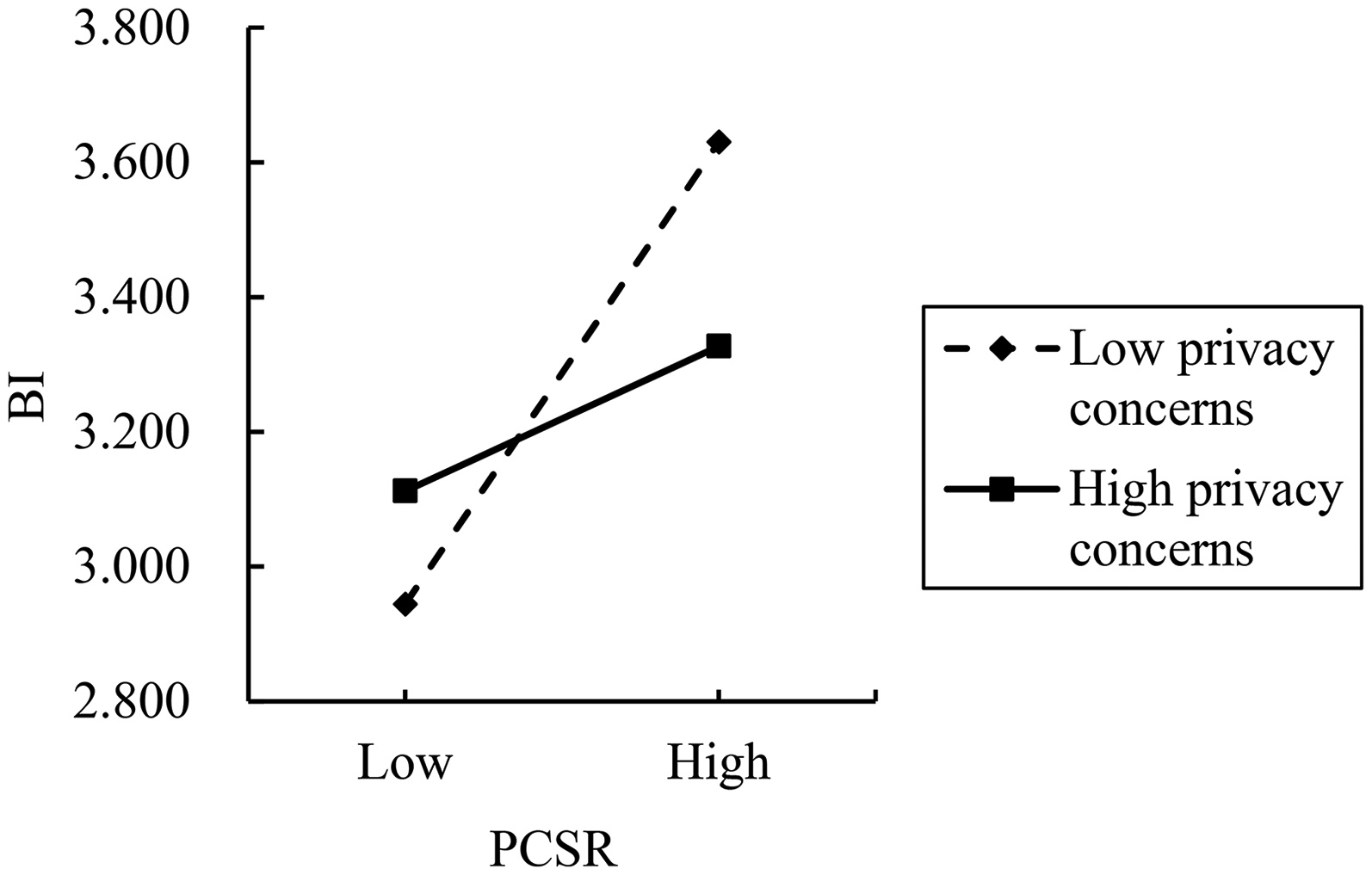
Moderating effect of privacy concerns. Source: Author's data analysis. Note: BI: behavioral intention.
Hierarchical regression results for testing the moderating effect.
Source: Author's data analysis.
Note: PCSR: users’ perceptions of platform corporate social responsibility; BI: behavioral intention; PEU: perceived ease of use; PU: perceived usefulness; PCs: privacy concerns. ∗ p < 0.05; ∗∗ p < 0.01; ∗∗∗ p < 0.001.
Discussion
The findings of this study provide robust empirical support for the hypothesized model, offering insights into how PCSR influences users’ BI to use online healthcare platforms. Drawing upon the TAM and CPV theory, this study validates the proposed mechanisms of direct, indirect, and moderated effects.
The results supported the positive direct effect of PCSR on users’ BI (β = 0.322, p < 0.05), confirming H1. This indicates that when users perceive online healthcare platforms as fulfilling social responsibilities—such as offering public health education, protecting consumer rights, and disclosing information ethically—they are more likely to intend to use the platform. According to CPV theory, such CSR practices enhance both cognitive and emotional evaluations, improving perceived benefits and reducing perceived risks. Prior studies have similarly found that CSR activities foster user trust, satisfaction, and ultimately greater acceptance of digital health services.55,56
PCSR significantly predicted users’ PEU (β = 0.646, p < 0.001) and PU (β = 0.653, p < 0.001), thus supporting H2a and H3a. Further analysis revealed that both PEU and PU partially mediated the relationship between PCSR and BI, supporting H2 and H3. The indirect effect of PCSR via PEU (β = 0.133, p = 0.007) and via PU (β = 0.162, p = 0.002) was statistically significant. This indicates that users’ perceptions of the platform's ease of use and usefulness are important mechanisms through which CSR perceptions translate into BI. As suggested by TAM, PEU facilitates user acceptance by reducing cognitive effort, 65 and CSR practices that simplify platform design or provide support services reinforce this ease. Similarly, PU reflects users’ beliefs in the platform's efficiency in delivering healthcare, which is strengthened by CSR initiatives such as partnerships with reputable hospitals or free expert consultations. 66 These results support earlier findings that CSR actions not only build ethical impressions but also tangibly enhance functional service perception, leading to increased usage intention.70,71
The moderating role of PC was also validated. The interaction effect between PCSR and PC on BI was negative and significant (β = –0.167, p < 0.01), supporting H4. This suggests that users with higher PCs are less responsive to CSR initiatives in forming BIs. Even if a platform is perceived as socially responsible, users who are skeptical about how their personal or health data will be handled may hesitate to engage with the service. This finding is consistent with previous studies indicating that PCs inhibit trust and reduce intention to use digital services, especially in sensitive domains like healthcare.30,73 The simple slope analysis further showed that under conditions of high PC, the positive effect of PCSR on BI was substantially weakened. This finding indicates that PC significantly conditions the influence of CSR on users’ BI, with its positive effect weakening and even disappearing when PC is high.
The joint interpretation of SEM and NCA offers richer insights than either method alone. SEM results show that PCSR, PEU, PU, and PC are sufficient to increase BI, indicating that enhancing these factors can promote adoption. In contrast, NCA reveals that no single factor is necessary (d < 0.1), suggesting that users’ adoption decisions follow a compensatory logic rather than being dependent on any single prerequisite. This dual perspective highlights both convergence and divergence between the two methods. For example, PU exerts a strong effect in SEM, yet NCA indicates that users may still adopt platforms even with low PU, provided CSR perception, ease of use, or privacy assurances are strong. Theoretically, this combination reveals that adoption is shaped by multiple interacting drivers rather than strict preconditions. Practically, it means platform managers should pursue holistic improvement strategies—simultaneously strengthening CSR perception, platform usability, and privacy protection—rather than narrowly optimizing one domain in isolation.
Theoretical implications
This study makes several theoretical contributions. Firstly, it extends the application of PCSR into a new domain. While prior research has extensively examined CSR's effects in traditional consumer contexts, empirical investigation within high-risk, high-sensitivity service environments—such as online healthcare—remains limited. By introducing PCSR into this context, the study offers a novel perspective on how CSR operates in digital health settings.
Secondly, by integrating TAM with CPV theory, the study provides a more nuanced explanation of how CSR perceptions shape usage behavior. Specifically, it identifies a dual-path mediation mechanism through PEU and PU, which connects external CSR cues to users’ internal cognitive evaluations. Additionally, by incorporating PCs as a moderator, the model captures individual-level differences in how CSR perceptions translate into BI. This responds to growing scholarly interest in the interplay between CSR and digital privacy, and enriches the role of PCs in online decision-making.
Thirdly, the study responds to the call for methodological pluralism in behavioral research. As Johnson et al. 78 have advocated, understanding complex behavioral phenomena requires a combinatory approach. By integrating SEM and NCA, this study not only tests the sufficiency of causal paths but also examines whether variables constitute necessary conditions. In doing so, it addresses a common shortcoming in prior CSR-intention research, which often lacks necessity analysis.
Managerial implications
The results also offer actionable guidance for platform operators and healthcare technology firms. Firstly, organizations should actively engage in socially responsible initiatives to enhance user trust. Beyond technical competence and service quality, platforms should focus on transparent communication, public health outreach, and user education, all of which contribute to a more trustworthy image and stronger emotional bonds with users.
Secondly, platform design should emphasize usability and practical value. Simplifying the interface, streamlining workflows, and enhancing efficiency can strengthen users’ perceptions of ease and utility—two cognitive channels through which CSR effects are amplified.
Thirdly, firms must take user privacy seriously. This includes improving transparency around data handling, clearly articulating the purposes and safeguards for personal data, and offering customizable privacy settings. For example, Doxy.me adopts a zero-retention model to reduce data exposure, while PatientsLikeMe allows users to control data sharing and explains how de-identified data is used. These practices help mitigate PCs, especially for sensitive users, and translate trust into continued usage.
Limitations and suggestions for future research
Despite its contributions, this study has several limitations that offer avenues for future inquiry. Firstly, this study was conducted in the context of online healthcare platforms in China. While the findings offer useful insights, their generalizability may be limited by cross-national differences in privacy regulations, healthcare infrastructures, and public attitudes toward CSR. These contextual factors may shape how users perceive and respond to PCSR efforts. Therefore, future research is encouraged to conduct cross-cultural or multi-country studies to test the applicability of our model in diverse institutional settings.
Secondly, the data were collected via self-reported questionnaires, and the sample was concentrated among specific user groups. Notably, participants with higher digital literacy were more likely to complete the online survey, potentially introducing selection bias and limiting the generalizability of the findings to less digitally literate populations. While the study employed controls to ensure quality, broader and more diverse samples are needed to enhance the robustness and external validity of the conclusions. Moreover, although both procedural and statistical remedies were applied to mitigate common method bias, the possibility of residual bias cannot be fully excluded. In addition, the cross-sectional design constrains causal inference: while the mediation analyses suggest potential mechanisms, the results should be interpreted as indicative associations rather than definitive causal pathways. Future studies could address this issue by incorporating multi-source or longitudinal data.
Thirdly, the study focused solely on PCs as a moderating factor. Other relevant individual differences—such as trust propensity, risk aversion, or past platform experience—may also influence how CSR shapes user behavior. Future research should consider incorporating these factors to develop a more comprehensive model of CSR perception and user intention.
Conclusion
Drawing upon the TAM and CPV theory, this study developed a conceptual framework that positions PCSR as the antecedent variable, with PEU and PU as mediators, and PC as a moderator. The model was employed to explore the underlying mechanisms driving users’ intention to use online healthcare platforms.
The findings yield several key insights. Firstly, PCSR was found to significantly enhance users’ willingness to engage with online healthcare services. Rather than exerting a vague influence on user trust or emotional attachment, CSR initiatives shape concrete perceptions of platform utility and usability—improving users’ evaluation of both functional value (PU) and ease of interaction (PEU)—which in turn encourage usage. Secondly, PEU and PU both mediated the effect of PCSR on BI, underscoring the dual perceptual pathways through which CSR initiatives indirectly reinforce users’ willingness to adopt digital healthcare services. Thirdly, PCs negatively moderated the relationship between PCSR and usage intention, indicating that strong CSR alone is insufficient—platforms must also address users’ data security and privacy expectations, especially in high-sensitivity contexts like digital healthcare. Importantly, beyond the SEM results, the NCA findings provide a distinct theoretical contribution: none of the predictors were identified as necessary conditions for BI. This highlights the multi-causal nature of user decision-making, suggesting that different combinations of antecedents may drive adoption rather than a single indispensable factor. Such evidence enriches our understanding of the complexity underlying technology acceptance in healthcare contexts.
These findings highlight the multifaceted role of PCSR in shaping user adoption of online healthcare platforms—not only by influencing users’ perceptions of usefulness and ease of use, but also through its interaction with contextual risks such as PCs. Future research may explore whether these mechanisms hold across different user populations, regulatory settings, or healthcare technologies.
Footnotes
Acknowledgements
We appreciate the strategic discipline group on digital innovation and management of Zhejiang University of Finance & Economics. This study is supported by the National Natural Science Foundation of China (grant number 72002188). We are grateful to all participants who contributed their time to this study.
Ethical approval
This study received ethical approval from the School of Management, Zhejiang University of Finance and Economics in February 2025.
Contributorship
Jinjiang He: conceptualization, manuscript revision, and supervision. Bingqian Wang: data collection, data analysis, and draft writing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is partially supported by the National Social Science Foundation of China (grant number 72002188).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Appendix A
Full Measurement Items in English and Chinese.