
Abstract
Symptoms of postpartum depression and anxiety in new mothers are prevalent and negatively impact maternal emotional wellbeing and infant development. Barriers to accessing treatment prevent women from receiving mental health care, a situation that has worsened due to the COVID-19 pandemic. mHealth interventions hold the potential to support women during the transition to parenthood despite these barriers and to promote the use of preventive interventions. This study uses a mixed methods design to assess the feasibility and preliminary effectiveness of a psychoeducational, guided mHealth intervention to prevent postpartum mental health difficulties in women who receive care in primary health centers in Chile. The study will contribute to evidence-based research on the effectiveness of mHealth interventions for new mothers from an understudied cultural background. The findings will also enable the development of a larger randomized controlled trial to assess the effectiveness of the intervention, which, if effective, could significantly contribute to the emotional wellbeing of women and their families.
Background
Maternal symptoms of depression and anxiety are prevalent during the perinatal period. Postnatal depression (PND) affects approximately 12% of women in high-income countries, and approximately 20% of new mothers in low- and middle-income countries. 1 Symptoms of maternal depression are often accompanied by comorbid symptoms of anxiety, which have a wide range of clinical presentations and affect 3%–43% of women in Western countries. 2
Chile has the highest PND prevalence rate among 56 countries 3 and this disorder affects 16–24% of women within the first 6 months after childbirth.4,5 Consistent with international studies, postnatal anxiety is estimated to impact 24%–41% of women in Chile. 6 Maternal mental health difficulties usually increase in high psychosocial risk contexts; which may be characterized by poverty, job insecurity, limited access to health care, and high levels of chronic stress.
Maternal mental health symptoms, if untreated, negatively impact mothers and infants. PND is usually related to low sensitivity to infant cues and reduced caregiving capability; which negatively affect child development 7 and entail a risk for the intergenerational transmission of depression.8,9 PND is also a risk factor for paternal depression. 10 With regard to anxiety, it intensifies maternal negative affect 11 and negatively impacts maternal sensitivity by contributing to higher intrusiveness during mother-infant interactions. 12
In Chile, although effective detection and treatment protocols are available for new mothers, only a minority (i.e., approximately 29%) of women who are at-risk of developing PND access treatment.5,13 Some of the barriers that prevent women to access or adhere to treatment in the country include negative beliefs about PND and the available interventions, stigma, and limited access to mental health care. With regard to health professionals, limited information about perinatal mental health, insufficient time during consultations, and lack of coordination between health providers are also described. 14 Characteristics of the health system that contribute to these barriers involve limited availability of mental health services, long waiting lists for mental health appointments, and difficulties to provide regular appointments to individuals undergoing treatment.14,15 Most of these characteristics are related to funding limitations. 16
The negative consequences of PND and anxiety for new mothers and their families, as well as the limited access and adherence to treatment, warrant evidence-based, easily accessible interventions to promote maternal wellbeing. In this context, preventive interventions are highlighted as an effective initiative that can significantly reduce the development of PND.17,18 These interventions are also cost-effective and reduce the burden that depression poses on health systems. 19
An effective, preventive intervention in this area is “What Were We Thinking” (WWWT). WWWT was developed in Australia, and it uses a psychoeducational and gender-informed approach to address risk factors for PND and postnatal anxiety that may be modified in first-time mothers. These include poor-quality partner relationship and unsettled infant behavior.20,21 Earlier studies indicate that WWWT effectively reduces the risk of developing PND up to 6 months after childbirth. 20 The original version of the intervention is delivered by a trained health professional to a group of up to 10 new mothers, their partners and new born infants in one single session. The intervention has been successfully adapted to be used in Chile. The main modifications involved including local metaphors and sayings, as well as including an explicit infant mental health approach. The Spanish version of WWWT holds the potential to significantly contribute to maternal, paternal and infant emotional wellbeing in the postpartum period. 22
Despite the effectiveness of perinatal preventive interventions, low attendance is a challenge that remains to be effectively addressed. This has become increasingly relevant due to the COVID-19 crisis, which has been associated with restrictions to visit health centers and allocation of most health professionals to assist COVID-19 patients. In this context, online interventions targeting mental health are promising, especially considering the significant evidence supporting their acceptability and effectiveness.23,24 These interventions, usually referred to as “digital mental health” use digital technologies to provide a wide range of services, such as screening, prevention, and treatment, among others. 25 They can be guided (i.e., include support from a facilitator or professional) or unguided (i.e., automated and self-administered). Studies suggest that guided interventions may improve effectiveness, 26 adherence and treatment satisfaction. 27
Within the existing types of digital-mental health interventions, those which rely on the use of mobile communication technologies to provide health care services are labelled as mobile health (mHealth). 28 The development and implementation of mHealth interventions have significantly raised during the past years. This is probably associated with the increasing use of mobile phones and widespread access to web-based text message services, particularly in Chile, 29 and the multiple benefits offered by mHealth, such as increasing patient interactivity and encouraging treatment adherence. 30
Pregnant women and new mothers have been reported to have a positive predisposition toward mHealth interventions31,32 and a significant number of perinatal women use online sources, including websites and Apps 33 to obtain information about pregnancy, childbirth, and infant care; as well as to receive advice and support.34,35 Interestingly, first-time mothers are more willing to use health and parenting related mobile applications (apps) than experienced mothers. 36 mHealth interventions targeting perinatal women address a wide range of issues, such as gestational weight gain, 37 smoking cessation, 38 breastfeeding,39,40 and infant care. 41 In particular, mHealth interventions oriented to promote perinatal mental health are promising in low and middle-income countries, 42 as they effectively increase the contact and communication between women and health providers during the perinatal period.
Studies on mHealth interventions that use web-based text messaging show that this is an effective, relatively low-cost tool, which has been used to successfully treat and prevent diverse mental health problems. 43 Also, text messaging offers the opportunity to adjust the level of participants’ interactivity (one-way vs two-way) and to use either standardized or personalized contents, depending on the availability of a facilitator and the guided or unguided nature of the intervention. 43 However, the great variety in terms of message content and frequency add to the complexity of the assessment of these interventions’ effectiveness. 41 Assessing the feasibility and use of mHealth interventions is especially relevant when considering the evidence available regarding their limited use by patients, either due to treatment drop-out or low adherence.44–47
The prevalence and impact of symptoms of depression and anxiety on new mothers and their families highlight an urgent need to develop and adapt effective and easily accessible strategies to promote maternal emotional wellbeing. mHealth strategies hold the potential to reach large groups of women who present with limitations to access interventions and health services, partly due to the sanitary crisis. Thus, they may offer an effective response to the current emotional needs of perinatal women. 48
In this context, the aim of our protocol is to evaluate the feasibility, acceptability, and preliminary effectiveness of the Spanish version of WWWT adapted as a mHealth intervention (m-WWWT) to prevent maternal postpartum depression and anxiety. This will contribute to the development of preventive initiatives to promote emotional wellbeing for new mothers and their families in Chile.
Aims and objectives
The aim of this protocol is to evaluate the feasibility, acceptability and preliminary effectiveness of m-WWWT, a psychoeducational intervention -delivered remotely via communication technologies (i.e., WhatsApp)- to prevent symptoms of depression and anxiety in new mothers during the postpartum period.
Methods
Intervention
“What Were We Thinking” (WWWT) is a psychoeducational, preventive intervention targeting risk factors for the development of PND and anxiety in new mothers.
49
The intervention, including participants’ materials and facilitator´s manual have been adapted to be used with Chilean populations.
22
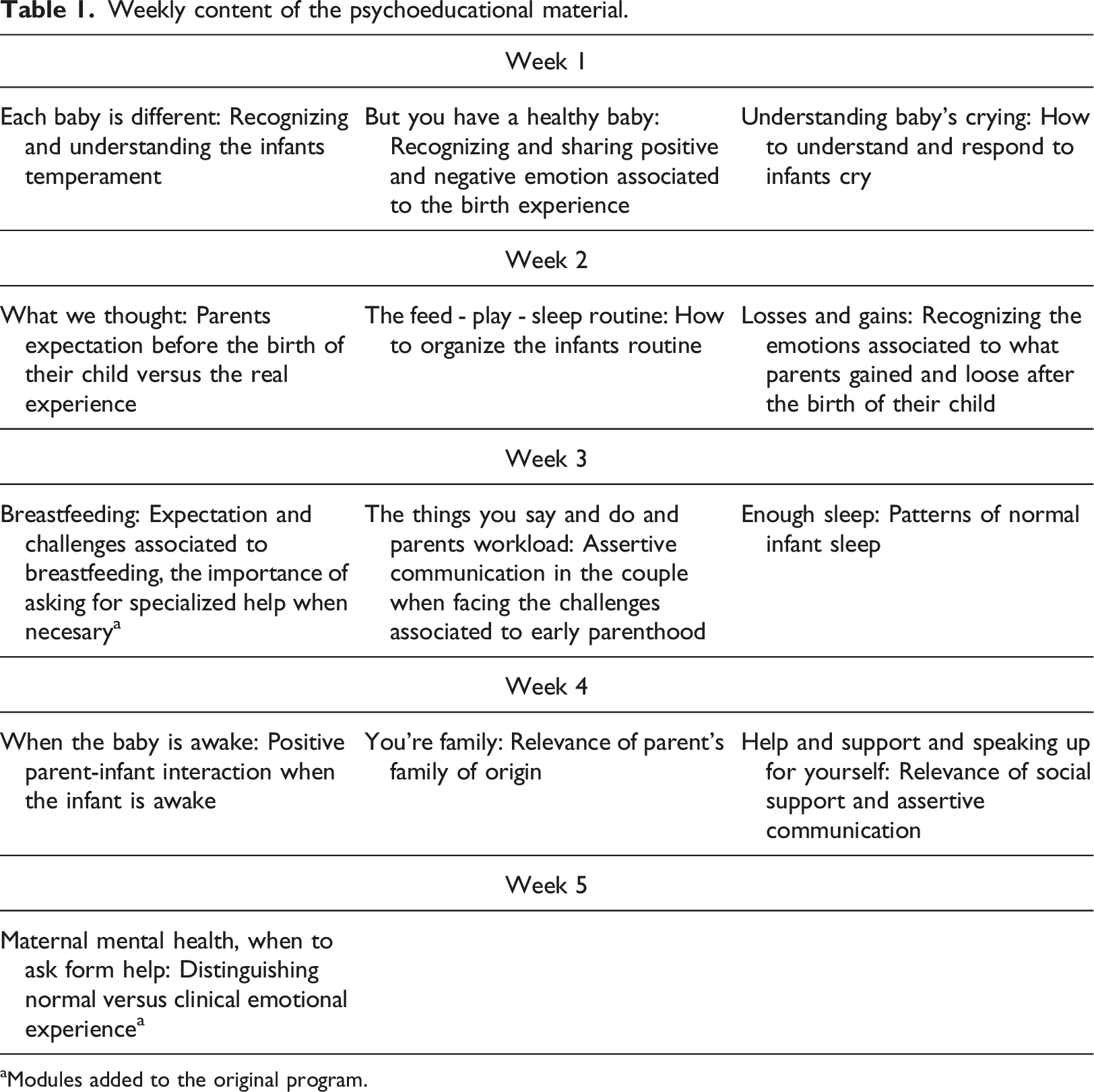
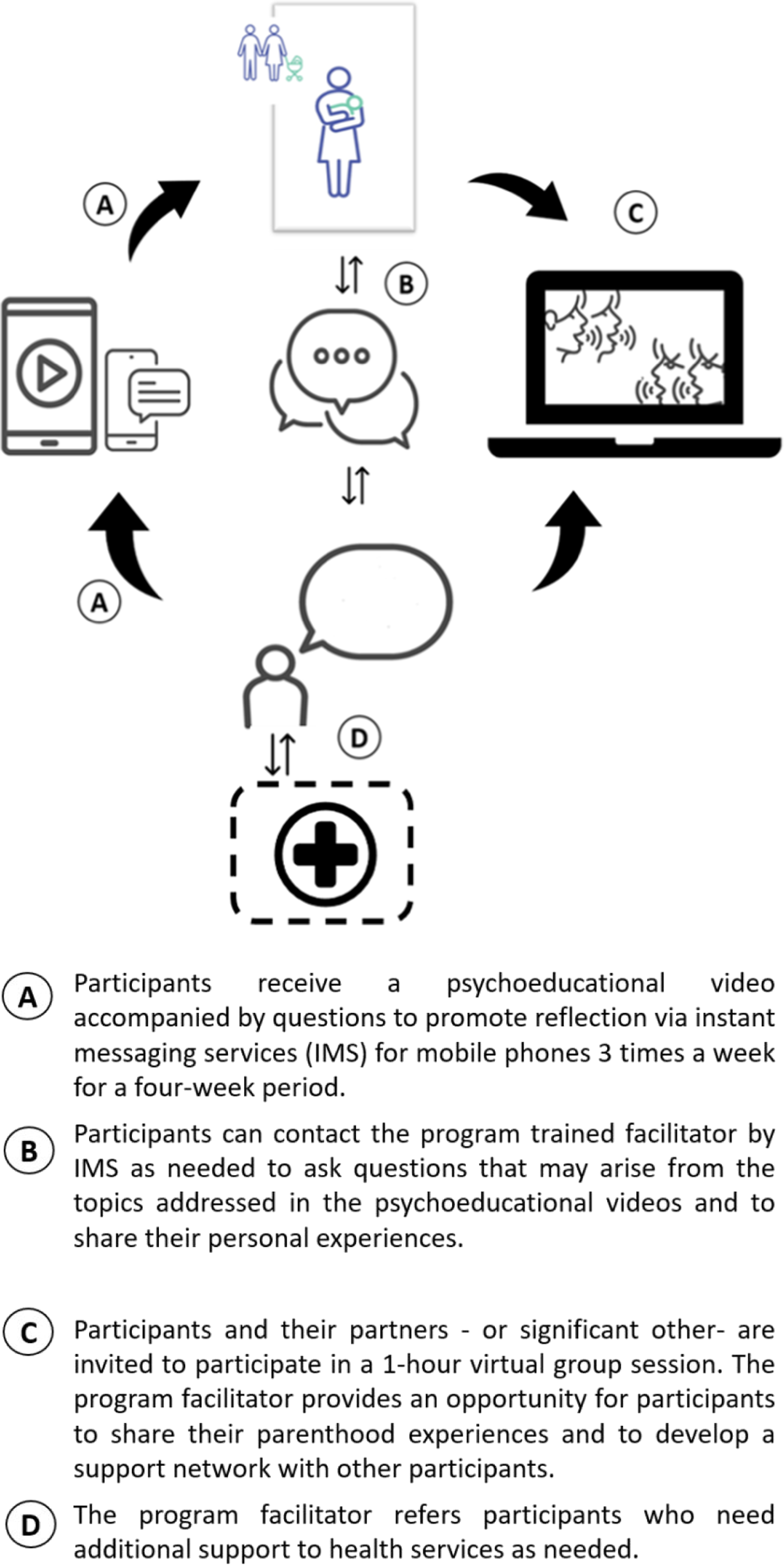
The m-WWWT program includes (see Figure 1): (a) Psychoeducational information on infant behavior and changes in interpersonal dynamics associated with parenting. Modules aimed at understanding and managing infant behavior include information on infant temperament; how to understand and respond to infant crying; soothing strategies; patterns of infant sleep and how to establish positive sleep habits; the use of settling strategies, infant feeding; and issues about the development of healthy daily care routines. Modules on matters related to interpersonal dynamics associated with parenting include reflections about the losses and gains associated with parenthood for mothers and fathers, identifying and effectively communicating emotional needs, managing emotions associated with adverse birth experiences, and practical skills that partners may use to address the needs and expectations experienced in the postpartum period in a non-confrontational manner. This information will be delivered individually to each participant through instant messaging services for mobile phones (i.e., WhatsApp) 3 times a week for a four-week period. Each module will include a 3-to-5-minute video offering information regarding a specific topic, a suggestion to engage in a personal exercise, and the invitation to assess the perceived usefulness of the information received. For example, in the section regarding infant routine, the proposed personal exercise is “We invite you to talk with your partner or the person who supports you in parenting your child, about the following questions: Do we have a feeding-game-rest routine? If we do, is it useful? Would you incorporate something else based on what you saw in the video? If you don’t have a routine, do you think it would be useful to establish one? Why?”. Some modules include links to external, complementary information from the Chilean Infancy Policy. Although only mothers will receive the intervention videos, they are encouraged to share them with their partners or support person. For information on the 14 modules see Table 1. (b) Individual contact with the program trained facilitator. It will allow mothers to individually ask questions that arise from the topics addressed in the psychoeducational videos and share their personal experiences. The facilitator responses will focus on promoting the understanding and elaboration of the contents based on prototypical responses, which will be tailored to the women´s particular circumstances. This will be done through instant messaging service for mobile phones (i.e., WhatsApp). The women in the study will initiate contact with the facilitator according to their own experiences and needs. We expect that some mothers will contact the facilitator more often than others. In the present study, the facilitator will be a mental health professional of the research team, who was involved in the development of m-WWWT. Standard training for facilitators involves two half-day theoretical and practical sessions about the program content and delivery. (c) Group virtual meeting. One 1-hour virtual group meeting will take place with mothers and their partners (or significant others) and the program facilitator. The group meeting offers an opportunity for new mothers and fathers to share their parenthood experiences and the changes it has involved in their daily lives, as well as providing the opportunity for developing a support network between them. The group meeting will be conducted online, 10-15 mothers and their partners or support person will be invited to attend. Weekly content of the psychoeducational material. aModules added to the original program. Components of m-WWWT.
The experimental group will receive the previously mentioned components of the intervention in addition to treatment as usual (TAU).
Treatment as usual
TAU involves infant routine health checks conducted by a nurse every month from 0 to 4 months of age, and at 6, 8 and 12 months of age. The purpose of routine health checks is to monitor the child’s development and growth, guide parents and/or caregivers regarding child development, health, and upbringing. Nurses also promote exclusive breastfeeding, healthy mother/child bonding and encourage paternal participation in the child´s care and upbringing. During the infant health check-ups at 2 and 6 months postpartum maternal symptoms of depression are screened for with the Edinburgh Postpartum Depression Scale (EPDS). Women who score above the EPDS cut-off score (i.e., 10) will be considered at risk and will be referred for mental health assessment and care.
Trial design
This is a data-analyst blind, superiority, pilot study that uses a mixed method design. The quantitative component will consist of a 2-arm randomized parallel group of 90 mothers of infants aged 4–8 weeks, who receive health care in two primary health centers in Santiago, Chile. Mothers will be randomized into the experimental (EG) or control groups (CG) in a rate of 1:1. using a computer-generated randomization schedule (Sealed Envelope Ltd.) with permuted blocks of random sizes (i.e., 2, 4, and 6). Group assignment is requested and sent to the research assistant at the moment of recruitment once the woman has accepted to take part of the study. In our study design, the data analyst will be blinded, however, the participants and facilitator of the intervention won’t be.
Both EG and CG will receive TAU provided by primary health centers, and only the EG will receive m-WWWT. Women in the control group will receive m-WWWT once the data collection for the study has been completed. Also, a qualitative component will be conducted, which involves 12 semi-structured interviews to evaluate the acceptability and satisfaction with the intervention from the perspective of EG mothers.
Setting and participants
Enrollment will take place at two public health centers in the suburb of Peñalolén, in Santiago, Chile, which primarily has a middle- and low-middle class population. These centers provide primary healthcare to the suburb population, including maternal antenatal checkups and health checkups for infants and children, as described in the previous TAU section.
Participant’s inclusion criteria are: (1) being adult (18–50 years old), (2) first time mothers, (3) having a healthy infant who is 4–10 weeks old, (4) receiving medical care at primary health centers, (5) having access to a mobile phone with instant messaging services (i.e., WhatsApp), and (6) being fluent in Spanish. Exclusion criteria are: (1) severe mental health problem (i.e., schizophrenia, mood disorder with suicidal ideation), (2) cognitive disability, (3) actual substance abuse, and (4) severe psychosocial problem (i.e., domestic violence). At the moment of recruitment, the women will be asked if they are receiving mental health treatment, in case they are, thew will not be randomized into the study. The qualitative component will have a purposive sample. We will identify women who are representative of the population according to diverse criteria, such as degree of interaction with the facilitator, sociodemographic variables (single v/s partnered mothers) and emotional well-being (absence vs. mild depressive symptoms). An initial sample of 12 women is proposed, this will be increased if saturation is not reached.
The program facilitator will meet the following inclusion criteria: (1) being a health professional (i.e., psychologist, nurse), (2) having professional experience with mothers and infants, and (3) completing the intervention training for facilitators.
Power calculation
Considering this is a feasibility study, we will not test any hypotheses; therefore, a power calculation is not needed.50,51 Each of the two health centers involved in the study receives approximately 15 first-time mothers per month. In view of this information and its implications for recruitment, our goal is to have 90 participants; this sample size will enable us to achieve the objectives of the study.
Procedures
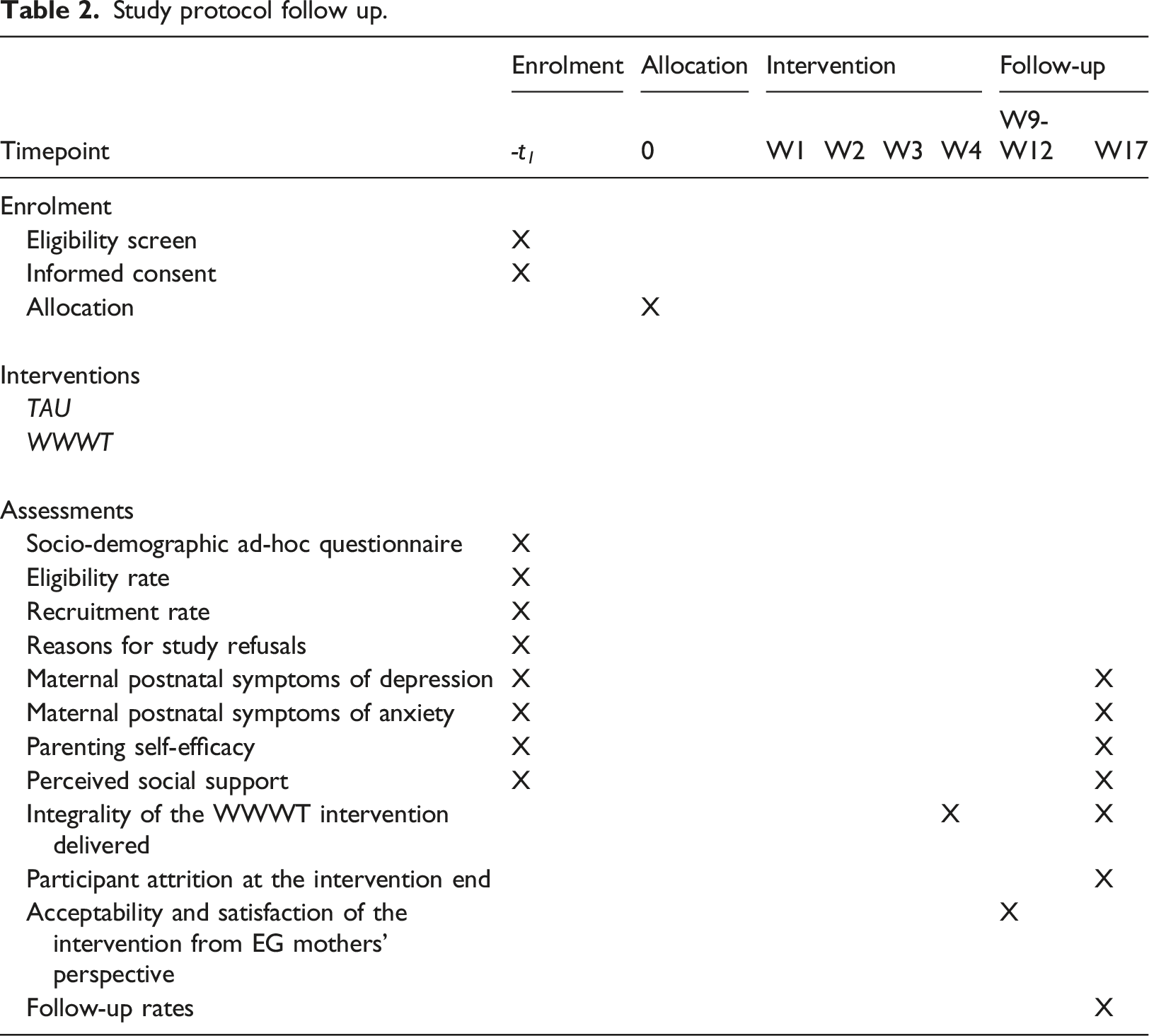
Study protocol follow up.
The qualitative component of the study will be conducted to assess users’ acceptability and satisfaction. The 12 semi-structured interviews to members of the EG group interviews will be conducted by phone. The maximum variation sampling strategy will be used according to the completion and use of the intervention.
Outcomes
The feasibility of m- WWWT will be assesses using the following indicators: eligibility and recruitment rates, reasons for study refusals, integrity of the intervention delivered, participant attrition, and follow-up rates according to treatment condition. Acceptability considers participant intervention completion and a qualitative assessment of the users’ acceptability and satisfaction. Preliminary effectiveness will be assessed as secondary outcomes.
Primary outcomes
Eligibility rate: Proportion of women who meet inclusion criteria compared with the total number of new mothers registered during the recruitment period in the primary health centers involved in the study.
Recruitment rate: Proportion of women who accept the invitation to join the study with respect to those who meet eligibility criteria.
Integrity of the intervention delivered: Percentage of EG participants who receive the 14 psychoeducational modules, attend the virtual meeting, and establish contact with the program facilitator at least once.
Participant attrition: Percentage of participants receiving the intervention who fail to finish it by group.
Follow-up rates: Percentage of participants receiving the intervention who are retained at follow-up measurement by group.
Secondary outcomes
These include changes in maternal postnatal symptoms of depression and anxiety, self-efficacy, and perceived social support in both groups. These outcomes will be measured with the EPDS,52,53 Perinatal Anxiety Screening Scale,54,55 Parental Evaluation Scale 56 and the Multidimensional Perceived Social Support Scale, 57 respectively.
Other outcomes
Reasons for study refusals: A list will be made containing the different reasons given by women who refuse to participate, the results will be aggregated in terms of percentages.
Acceptability and satisfaction of the intervention from EG mothers’ perspective: EG mothers’ acceptability and satisfaction with the intervention, assessed using qualitative semi-structured interviews.
Instrument description
The EPDS will be used to examine symptoms of maternal depression. The EPDS is a 10-item, self-report instrument that screens for current maternal symptoms of depression using a 4-point scale, total score ranges from 0 to 30 points. 52 This instrument has been validated in Chilean populations. 53 Maternal anxiety symptoms will be assessed using the Perinatal Anxiety Screening Scale (PASS). This 31-item, self-report instrument assesses maternal perinatal anxiety over the past month in pregnant and postnatal women. Items use a 4-point Likert scale (0=Never – 3= almost always”).54,55 The total score results from the sum of scores on each item, with higher scores indicating more anxiety. The PASS has been validated for Chilean mothers, it includes 27 items, corresponding to four subscales: general worry and specific fears (4 items); perfectionism and control (5 items); social anxiety (5 items); and acute anxiety, adjustment difficulties and trauma (15 items). The Spanish version of the PASS has good psychometric properties. 58
The Parental Evaluation Scale (PEE) will be used to assess motherhood-related satisfaction and self-efficacy. Each of the 10 items is rated on a 11-point scale (0 = strongly disagree; 10 = strongly agree), the total score results from the sum of single item scores divided by 10. 56 Finally, the Multidimensional perceived social support scale (MSPSS) will be used to assess perceived social support. This is a 12-item, self-report instrument that includes three subscales on perceived social support in three areas: family, friends, and significant others. Items are rated on a 7-point Likert-scale (1 = very strongly disagree; 7 = very strongly agree). Three subscales' scores (range 4–28) and a total score (range 12–84) are estimated by the sum of item scores. The MSPSS has been adapted for its use in Chile. 59
Regarding the qualitative component, the interviews have the purpose to explore the participants ‘experience during the intervention, specifically acceptability (i.e., how frequently they accessed the intervention components and how easy/difficult this was). Additional areas of assessment include the general perception of the intervention (i.e., images, language, and usefulness of the videos), the relationship with the facilitator (i.e., contact frequency, communication quality, emotional attunement) and the group session (i.e., participation and perceived usefulness).
Data collection
The participants in both groups will be assessed a week before they begin the intervention (baseline) and 3 months after its completion, to capture the mid-term impact of the intervention on maternal mental health. Qualitative interviews will be performed 4–8 weeks after finalizing the intervention. This timeframe is recommended to allow women some time to elaborate and assimilate their experience during the intervention, as suggested by earlier qualitative studies.60,61 Also, women´s experience during m-WWWT may be less vivid during the follow-up assessment 3 months after finishing the intervention. Online questionnaires will be used to assess all variables. There is a small economic compensation for participants, to cover the costs of internet use.
Safety monitoring and criteria for discontinuation
Negative effects associated with participation in the study are not expected. If participants responses to questionnaires indicate that they are presenting mental health symptoms that require further professional assessment and treatment, they will be referred to their health center. These participants will be excluded from the study if they begin psychological and/or psychiatric treatment after being referred. However, they will keep receiving the videos and messages from the intervention.
Data analyses
Participant characteristics at baseline, as well as intervention feasibility and acceptability outcomes will be assessed with descriptive statistics, including mean with standard deviation, median with interquartile range, frequency, and percentage (depending on data distribution). Mixed-ANOVA analysis will be used to examine possible differences in the secondary outcomes between EG and CG, whilst subjecting participants to repeated measures. Considering that this is a pilot study, our results will be judged as preliminary. Possible patterns of missingness will be studied in missing data and, if appropriate, multiple imputation (intention-to-treat) will be used. Open code of grounded theory will be used to analyze qualitative data.
Discussion and conclusion
Maternal symptoms of depression and anxiety are prevalent in the postpartum period and have negative consequences for women and infants. Despite the availability of mental health interventions, women have several barriers to access treatment, a situation that has worsened during the Covid-19 crisis. In this context, mHealth interventions hold the potential to promote maternal mental health during the transition to motherhood. This study will make a relevant contribution by evaluating the feasibility and preliminary effectiveness of m-WWWT; an intervention which promotes maternal emotional wellbeing by targeting modifiable risk factors for the onset of symptoms of depression and anxiety in new mothers.
This feasibility study will contribute to the larger body of research oriented to assess the potential contribution of mHealth interventions to support new mothers and enhance their -and their families-emotional wellbeing. We also expect this protocol study will inform similar initiatives in the wider scientific community to develop and assess mHealth interventions in diverse populations, which will help to overcome some of the diverse barriers that individuals face to access treatment for mental health difficulties. We hope the results from this study will enable the development of a larger randomized controlled trial to assess the effectiveness of m-WWWT.
Footnotes
Author contributions
CP, SC and MIG intellectually designed the study. CP obtained funding for the project. SC and MIG adapted the WWWT to mHealth intervention. SC and MIG will deliver the intervention. CP, SC, PF, MO, DA, OF, NA, FP wrote the manuscript. JF and HR developed the original English version of the intervention, supervised its adaptation, and contributed to the final manuscript. All co-authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the ANID Millennium Science Initiative/Millennium Institute for Research on Depression and Personality-MIDAP ICS13_005. Funding source had no role in data collection, analysis and interpretation of the results. PF received funding from ANID BECAS/DOCTORADO NACIONAL/2019–21190745.
Ethical approval
Ethics approval was obtained from the Ethics Committee of the Eastern Metropolitan Health Service, Santiago. A modification to the original protocol was approved to collect qualitative data.
Informed consent
All the participants are asked to provide informed consent before joining the study. Data will only be accessible to the research team, individual information about participants and potential participants will be confidential and only de-identified data will be available for analyses. Publication of the study results will not include any identifiable information about participants.
Data availability
The de-identified datasets generated from this study will be available from the corresponding author upon reasonable request.
Trial registration
NCT04847076. Registered on 15 April 2021