
Abstract
A single-arm feasibility trial was conducted to explore rural-living young adult cancer survivors’ physical activity, fruit and vegetable consumption, and motivational processes underlying any behavior changes during a telehealth behavior change intervention grounded in self-determination theory. Participants (n = 7; 85.7% female; Mage = 33.9, range = 28–37) met with a health coach once a week for 60 min for 12 weeks. Participants completed pre- and post-intervention surveys that assessed their behaviors, basic psychological needs satisfaction, and behavioral regulations. Participants also completed a semi-structured interview post-intervention. Quantitative results indicate behavioral outcomes, basic psychological needs satisfaction, and behavioral regulations increased from pre- to post-intervention. Five themes provide context for the observed increases. Results provide preliminary evidence that motivation for physical activity and fruit and vegetable consumption may be facilitated by a one-on-one telehealth intervention among rural-living young adult cancer survivors. Large scale studies are needed to determine effectiveness of the intervention and identify mechanisms underpinning behavioral outcomes.
Introduction
Physical activity (PA) and fruit and vegetable (FV) consumption can reduce cancer-related sequalae, improve overall survival rates, promote physical and psychosocial health, and enhance quality of life among cancer survivors. 1 It is recommended that cancer survivors engage in aerobic PA at moderate-to-vigorous intensity for ≥90 min weekly 2 and consume ≥ five servings of FVs daily. 3 Among the 80% of young adult cancer survivors (YAs) who are expected to survive at least 5 years post-diagnosis, 4 approximately 10–30% meet PA guidelines and 20–30% meet FV consumption guidelines.5,6 Rates are even lower among rural-living cancer survivors. 7 Interventions promoting adherence to PA and FV consumption guidelines that work in urban areas may not work in rural areas.8,9 As rural-living persons struggle to access quality supportive care services, 10 ensuring their access to interventions promoting adherence to PA and FV consumption guidelines is critical to reduce observed health disparities.7,8
Interventions offering high accessibility and flexible scheduling are favored by rural-living cancer survivors and YAs in general.11,12 As such, telehealth interventions (i.e., interventions accessible remotely via teleconferencing or the Internet) are now considered an appropriate means of addressing access concerns for rural-living cancer survivors and incorporating YAs’ preferences.13,14 Moreover, based on qualitative studies with rural-living cancer survivors,15,16 synchronous interventions in which a facilitator interacts with participants in real-time are favored for their impact on participants’ motivation for engaging in lifestyle behaviors. Although preliminary evidence suggests interventions delivered remotely can lead to behavior change in adults,17,18 studies exploring the motivational processes underlying behavior change are rare, especially among rural-living individuals (including YAs).
Autonomous motivation (i.e., engaging in a behavior because it aligns with one’s intrinsic goals and emanates from the self) is a robust predictor of health behavior change.19,20 However, maintaining autonomous motivation for PA and FV consumption remains challenging.20,21 Based on self-determination theory (SDT), 22 increasing peoples’ autonomous motivation largely depends on the extent to which an intervention satisfies their basic psychological needs 23 —that is, their perceptions of autonomy (i.e., the sense that the individual is in control of their environment), competence (i.e., an individual’s perception of being able to complete a task or activity), and relatedness (e.g., the belief that an individual is being supported and feels connected to others). Indeed, basic psychological needs satisfaction has been associated with greater adoption and adherence to health-promoting behaviors. 24 Therefore, to promote autonomous motivation for PA and FV consumption among rural-living YAs, we developed a SDT-based 12-week telehealth behavior change intervention targeting these processes. We then sought to describe participants’ behaviors before and after the intervention and explore underlying motivational processes (i.e., SDT constructs) using qualitative and quantitative methods to identify possible mechanisms by which the intervention may exert its effects on PA and FV consumption. In turn, this information can be used to refine the intervention, and derive hypotheses to test during implementation and effectiveness testing.
Intervention studies incorporating qualitative and quantitative methods can furnish an in-depth understanding of the impact of a telehealth behavior change intervention on targeted processes and behavior change. Quantitative methods can help describe the magnitude of change in behaviors and SDT constructs, whereas qualitative methods enable participants to describe how their behaviors changed and the processes they saw as underlying their behavior change. Leveraging the strengths of both methods can guide the refinement and adaptation of the intervention to improve its effectiveness and guide implementation of a larger, ensuing hypothesis testing study. Therefore, the specific aims of this sub-study were to describe rural-living YAs’ PA and FV consumption before and after the intervention, and explore the motivational processes underlying any behavior change in the context of a single-arm, mixed-methods feasibility study.
Methods
Data analyzed and reported herein were collected as part of a single-arm feasibility trial designed to: (1) assess the feasibility of the intervention and study methods, (2) assess the acceptability of the intervention, and (3) explore motivational processes that may be associated with changes in PA and FV consumption in order to refine components of the intervention and/or study methods prior to proceeding to a larger, hypothesis testing study. The feasibility and acceptability outcomes are presented elsewhere. 25 The trial was registered in the ClinicalTrials.gov database (NCT03691545) and a detailed description of the protocol has been published. 26 The Template for Intervention Description and Replication 27 and the Standards for Reporting Qualitative Research 28 checklists were followed in the preparation of this manuscript to ensure complete reporting and transparency. A brief overview of the study design, intervention, and measures pertaining to this study are presented below.
A concurrent triangulation design was used for the single-arm, mixed-methods feasibility study, wherein quantitative and qualitative data were collected and analyzed concurrently. 29 This methodology was favored to comprehensively address the research objectives. 29 The quantitative data were used to describe participants’ behaviors and motivational process before and after the intervention, and the qualitative data provided insight into how changes (or lack thereof) may have occurred. Triangulation of quantitative and qualitative data enabled a better understanding of how SDT constructs may have contributed to changes in PA and FV consumption.
Participants
Research Ethics Board approval was granted from the University of Ottawa (file number: H-08–18-882). To participate in the single-arm, mixed-methods feasibility study, YAs had to: (1) be between 20 and 39 years of age, 30 (2) live in a rural community with fewer than 35,000 inhabitants,31,32 (3) self-report participating in <150 min of moderate-to-vigorous intensity PA weekly, 1 (4) self-report consuming < five servings of FVs daily, (5) have completed primary treatment for cancer, (6) have access to the Internet and an audio-visual device, (7) be able to read and speak English, (8) be able and willing to provide informed consent via an online form, and (9) be ambulatory. YAs who self-reported physical impairments precluding PA (e.g., symptomatic heart or vascular diseases, severe hypertension) were not eligible. 18 YAs expressed interest in the study; nine met inclusion criteria, though one dropped out before the first intervention session and one dropped out after the first session. Seven participants took part in the intervention and completed all assessments. Further details on exclusion are presented elsewhere. 25
Procedures
Recruitment was open for 12 months (September 2018–September 2019). Community-based recruitment methods were used (e.g., postings on social media, sharing of study details in community partner newsletters), and interested YAs were invited to contact the first author. YAs were screened for eligibility by telephone and provided detailed information about the study. Eligible YAs were emailed a link to a digital consent form. After providing informed consent digitally, they were directed to an online, pre-intervention questionnaire (T0). Once participants completed the questionnaire, they began the 12-week intervention, which consisted of weekly 60-min sessions one-on-one with the first author. Sessions were delivered using an online synchronous video platform of participants’ choosing (e.g., Skype). Post-intervention (T1), participants completed an online questionnaire within 1 week of completing the last intervention session and took part in an interview the following week.
Intervention
The 12-week intervention was a complex intervention consisting of relational and content components chosen based on previous literature33–35 and was delivered by the first author. The relational component focused on fostering participants’ perceptions of autonomy, competence, and relatedness, and facilitating autonomous forms of motivation (or self-determined behavioral regulations) using autonomy support and motivational interviewing techniques. To provide autonomy support,23,33 the first author actively supported participants’ capacity to be self-initiating and autonomous in their behavior change decisions and actions. She further facilitated autonomy support by employing motivational interviewing techniques, including:34,36 (1) resisting the righting reflex (i.e., resist giving suggestions to participants for their problems), (2) understanding and exploring participants’ motivations (i.e., be a curious listener and attempt to elicit underlying motivation for change), (3) listening empathically (i.e., listen with a patient-centered, empathic approach), and (4) empowering participants’ decision making (i.e., remind participants that they are in control of their actions, and that desired change requires they take steps toward that change).
Intervention schedule for the 12-week behavior change intervention.
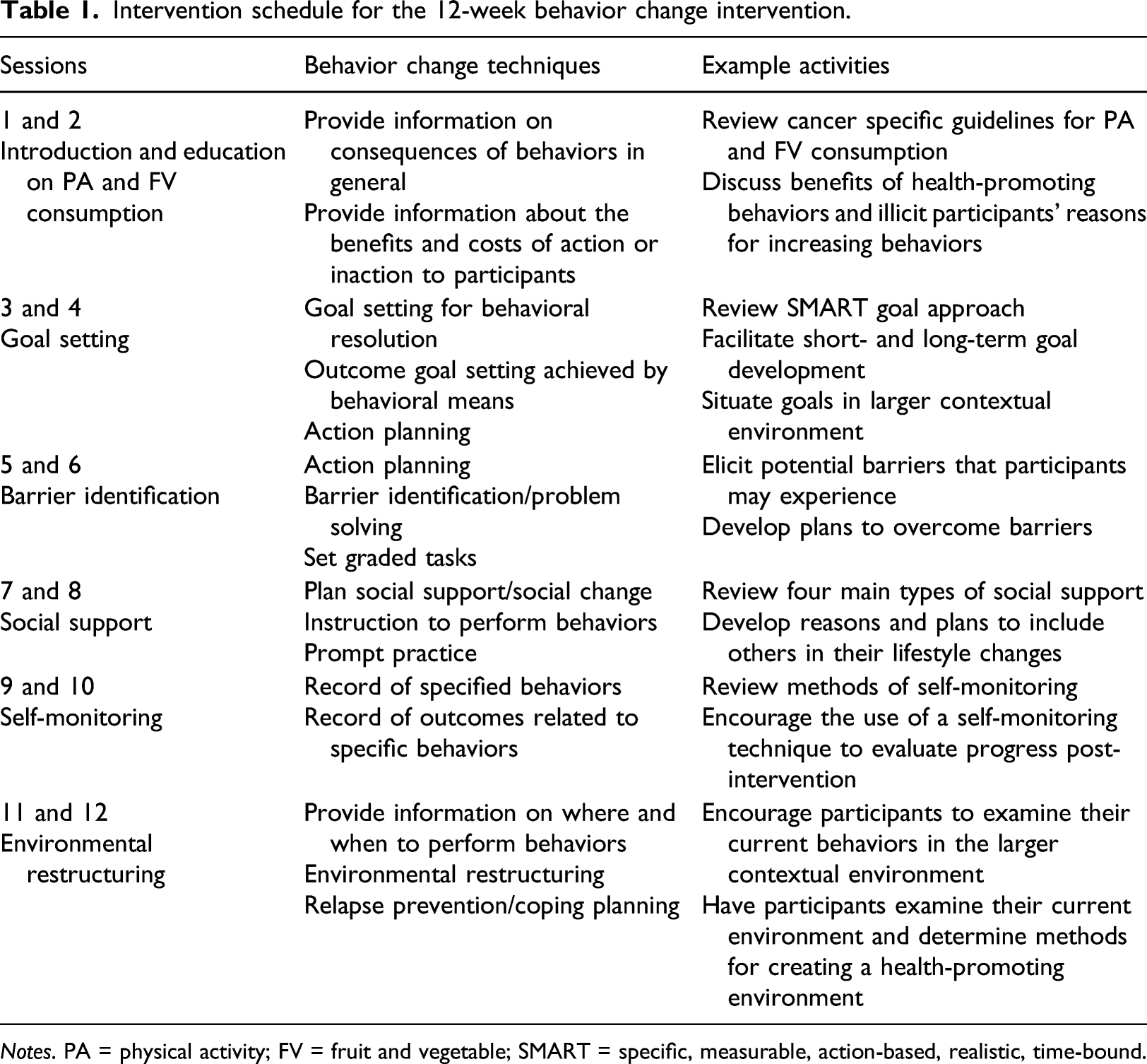
Notes. PA = physical activity; FV = fruit and vegetable; SMART = specific, measurable, action-based, realistic, time-bound.
Measures
Personal and medical factors [T0]
Participants self-reported personal (i.e., age, self-identified sex [Male/Female/You do not have an option that applies to me. I identify as (please specify):], annual household income, education attainment, school/work status) and medical information (i.e., cancer diagnosis, treatment protocol, time since treatment, co-morbid conditions). These data were used to describe the sample.
Physical activity behavior [T0, T1]
Self-reported PA was assessed using the International Physical Activity Questionnaire-Short form. 37 It includes seven questions about participation in vigorous and moderate intensity PA, as well as participation in walking and sedentary behaviors. Weekly PA was determined by summing reported min of moderate-to-vigorous intensity PA.
Fruit and vegetable consumption [T0, T1]
Self-reported FV consumption was assessed using the Behavioral Risk Factor Surveillance System-FV questionnaire. 38 Daily FV consumption was determined by summing participants’ responses to six questions about the frequency of fruits, vegetables, and potatoes consumed daily (e.g., “Not including juices, how often did you eat fruit per day?”).
Psychological needs satisfaction for physical activity [T0, T1]
Perceptions of autonomy, competence, and relatedness in PA contexts were assessed using the 18-item Psychological Need Satisfaction in Exercise Scale. 39 The word “exercise” was replaced with “physical activity.” Each item was rated on a scale ranging from 1 = false to 6 = true. Scores were computed for each psychological need by summing scores for autonomy, competence, and relatedness, respectively, with higher scores representing higher needs satisfaction.
Psychological needs satisfaction for fruit and vegetable consumption [T0, T1]
The 21-item Psychological Need Satisfaction questionnaire40,41 was used to assess the degree to which participants’ basic psychological needs were satisfied in regards to their FV consumption. The questionnaire was modified by adding “fruit and vegetable” to the question stems. Each item was rated on a scale ranging from 1 = not at all true to 7 = very true. Scores were computed for each psychological need by summing scores for autonomy, competence, and relatedness, respectively, with higher scores representing higher needs satisfaction.
Behavioral regulations for physical activity [T0, T1]
Behavioral regulations for PA were assessed using the Exercise Treatment Self-Regulation Questionnaire. 42 It consists of four subscales reflecting controlled (i.e., external regulation, introjected regulation) and autonomous motivation (i.e., identified regulation, intrinsic motivation). The word “exercise” was replaced with “physical activity.” Each item was rated from 1 = not at all true to 7 = very true. Scores were calculated by summing scores for autonomous and controlled motivation subscales, respectively. Higher scores represent higher autonomous and controlled motivation.
Behavioral regulations for ruit and vegetable consumption [T0, T1]
Behavioral regulations for FV consumption were assessed using the Dietary Self-Regulation questionnaire. 43 It consists of three subscales that assess: autonomous motivation, controlled motivation, and amotivation. Each item was rated from 1 = not at all true to 7 = very true. Scores were calculated by summing scores for autonomous and controlled motivation, respectively. Higher scores represent higher autonomous and controlled motivation.
Participants’ perspectives—Interview [T1]
Topics covered and sample questions from the interview guide with rural-living young adult cancer survivors who completed a 12-week behavior change intervention.
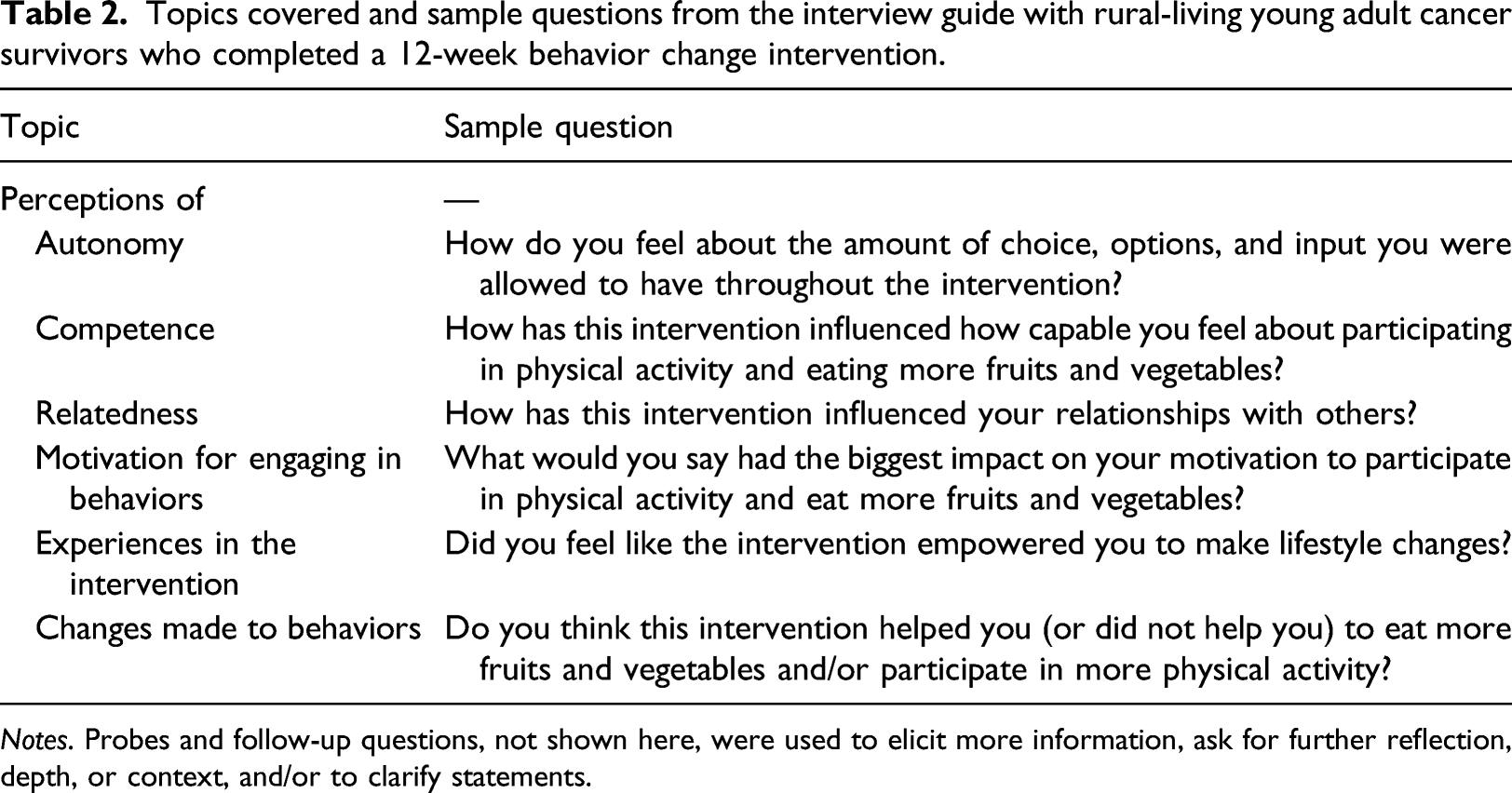
Notes. Probes and follow-up questions, not shown here, were used to elicit more information, ask for further reflection, depth, or context, and/or to clarify statements.
Sample Size
Given the feasibility design, sample size calculations were not performed.44,45 Rather, recruitment remained opened for 12 months and feasibility metrics were tracked. Nevertheless, it is worth noting that data saturation was achieved for the qualitative data as experiences relayed by participants began to recur, and additional interviewing failed to identify new insights.
Data analysis
Quantitative data were analyzed using SPSS (Version 26; SPSS Inc. Chicago, Illinois, USA). Descriptive statistics were used to describe and summarize the data (i.e., describe central tendencies [via medians] and dispersions of variables [via interquartile ranges] at T0 and T1), and non-parametric tests were used to examine trends between T0 and T1 because of the small sample size and non-normality of some of the data. Specifically, Wilcoxon matched-pairs signed-rank tests were conducted to describe the magnitude of differences in behaviors and SDT constructs between T0 and T1. As this study was not powered to detect statistically significant differences, correlational effect sizes (r) were computed using the following equation: r = z/√ (nT0 + nT1), with n T0 = n at pre-intervention and n T1 = n at post-intervention, and interpreted as: r = ± 0.1 indicates a small effect, r = ±0.3 indicates a medium effect, and r = ± 0.5 indicates a large effect. 46 Effect sizes, rather than p values which are related to the sample size, were interpreted to describe whether potential differences may exist between T0 and T1. Since the analyses were to meant to summarize the data that were collected, the analysis did not consider intention-to-treat analysis; dropouts were excluded from analysis (i.e., per-protocol analysis) given the early timing of dropouts. Qualitative data were thematically analyzed deductively to establish how participants’ accounts added to, or undermined, existing research on SDT and behavior change. A detailed semantic level analysis was conducted following six steps to explore common themes across interviews. 47 Descriptions were prepared and anonymized illustrative quotations were selected for reporting. Last, quantitative results were compared against the emergent themes from participants’ accounts to gain insight into similarities as well as nuances, discrepancies, and contradictions between the quantitative and qualitative data.
Study rigor
Throughout the single-arm, mixed-methods feasibility and this sub-study, several steps recommended in the literature were taken to enhance the quality and trustworthiness of data. 48 First, the researchers recruited a sample appropriate for the study objectives and collected data to inform meaningful and significant claims. Second, the research process is presented above to elucidate the depth and breadth of analysis, and to enhance transparency. Third, the first author developed a strong rapport with participants over the course of the intervention to help gain participants’ trust, which is essential for a constructive qualitative interview.49, 50 In addition, prolonged contact with the interviewer helped participants feel safe sharing their experiences during the interview and discuss ‘negative’ thoughts and experiences, as previously reported. 25 To this end, the interviewer informed participants that she was there to listen to them and framed the interview as an opportunity for participants to share any/all thoughts and experiences to contribute to the refinement or improvement of the intervention. Finally, the researchers acknowledged and reflected on their preconceptions, life experiences, and knowledge of the literature as they interpreted the results.
Results
Quantitative
Participants’ sociodemographic and medical characteristics (N = 7).
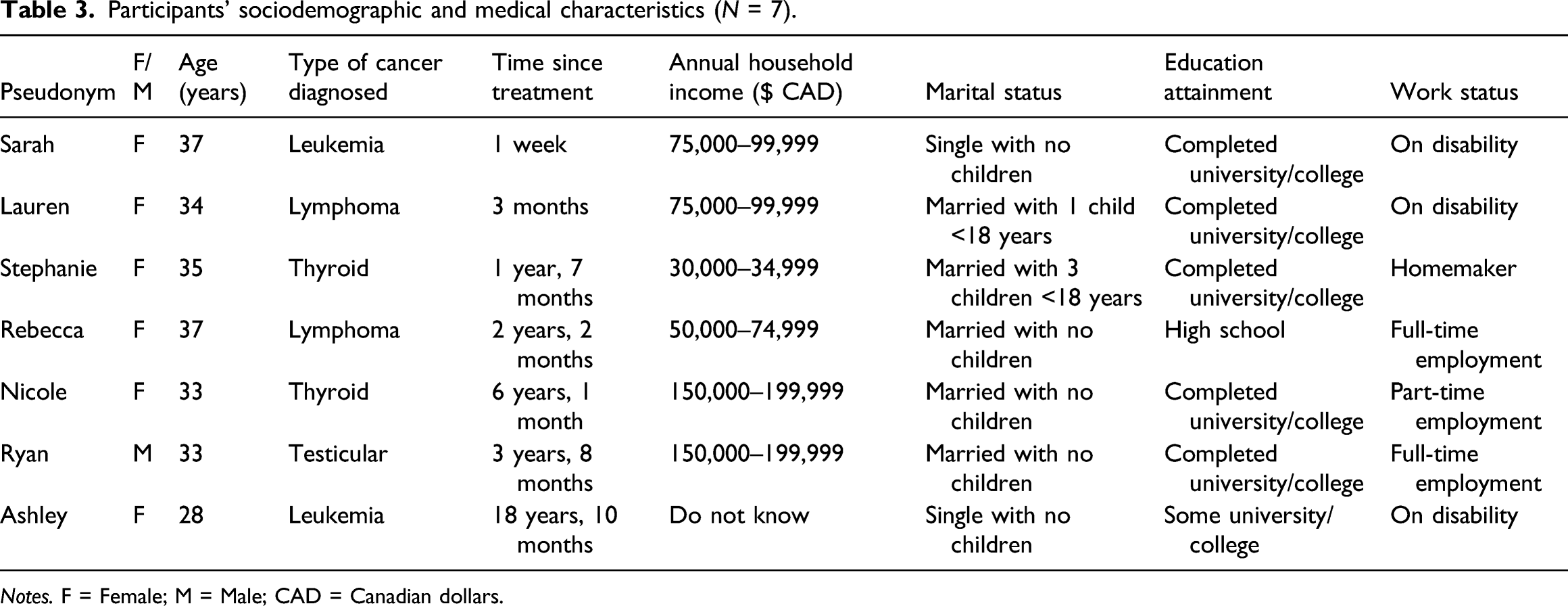
Notes. F = Female; M = Male; CAD = Canadian dollars.
Wilcoxon matched-pairs signed-rank tests of differences between pre (T0) and post-intervention (T1) PA, FV consumption, and SDT constructs (N = 7).
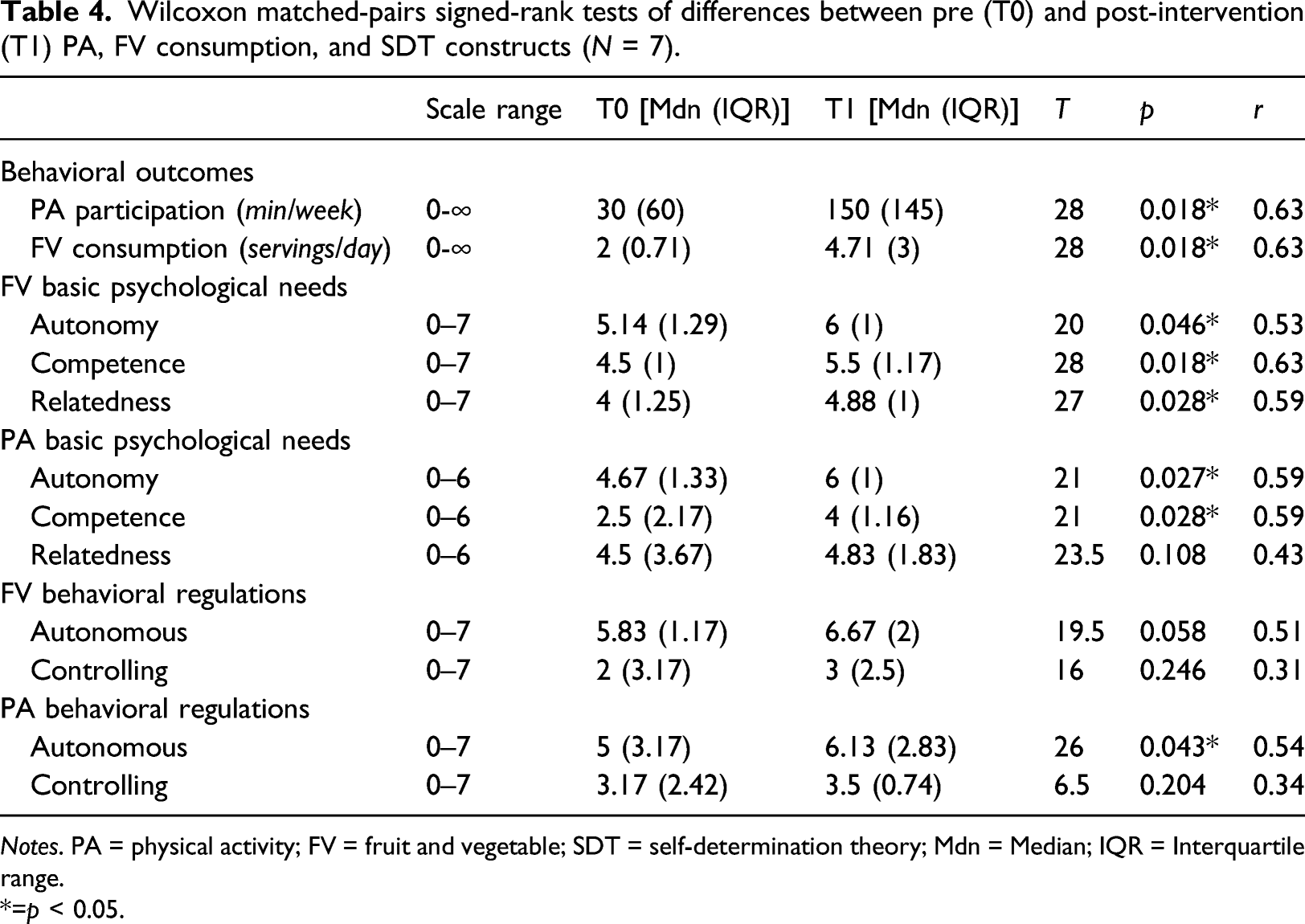
Notes. PA = physical activity; FV = fruit and vegetable; SDT = self-determination theory; Mdn = Median; IQR = Interquartile range.
*=p < 0.05.
Qualitative
Direct quotations from rural-living young adult cancer survivors (N = 7) who completed the 12-week behavior change intervention.
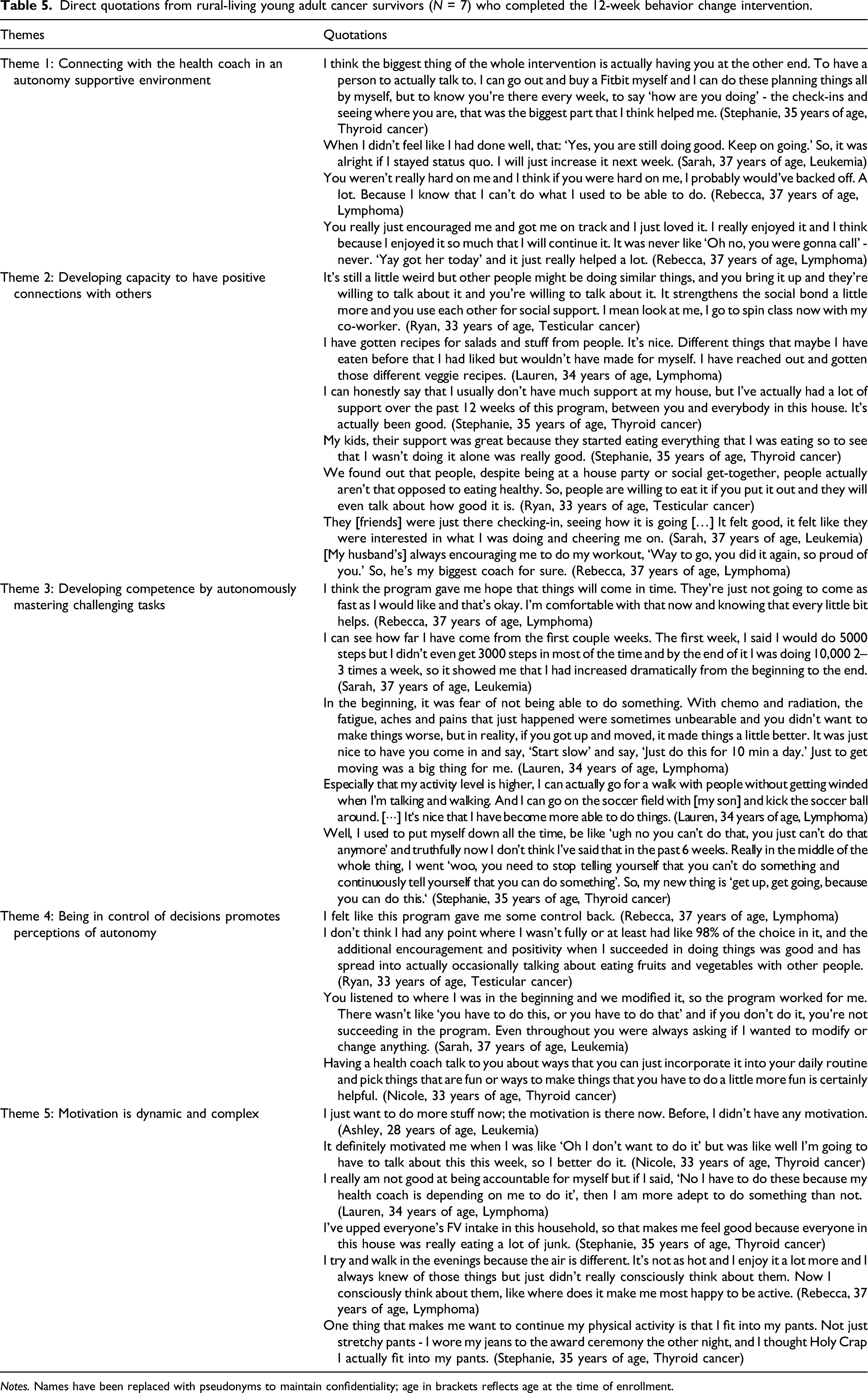
Notes. Names have been replaced with pseudonyms to maintain confidentiality; age in brackets reflects age at the time of enrollment.
Theme 1: Connecting with the health coach in an autonomy supportive environment
Communicating in real-time with a health coach allowed participants to give updates on their progress and celebrate that progress. Participants felt the health coach’s supportive actions and words communicated investment, acceptance, warmth, and affection, and this encouraged them to be honest about their goal progress. For example, participants were determined to keep trying to reach their goals in the face of challenges and setbacks because the health coach conveyed to them that behavior change is a process. Participants believed the health coach interacted with them in a manner that conveyed patience, respect, and understanding, which helped them to feel comfortable during the intervention. Participants described that receiving emotional support during the sessions and having enjoyable interactions with the health coach enhanced their behavioral goals’ value and intensified their motivation for PA and FV consumption.
Theme 2: Developing capacity to have positive connections with others
Participants talked about the benefits of learning how to build social support networks with existing and new sources. It helped them reach their behavioral goals because it increased opportunities to engage in PA with others (e.g., family, friends, co-workers) and knowledge of how to consume more FVs. Receiving support from family and friends was a new and good thing for some. Observing that others were open to changing their behaviors enthused participants. Having others to check-in with and give updates on their progress made them feel good. Moreover, receiving praise for success motivated them to continue.
Theme 3: Developing competence by autonomously mastering challenging tasks
Participants explained that the intervention taught them the value of making progress and that progress is not “all or nothing.” At the start of the intervention, they set targets and they wanted to achieve them right away, but over time, they realized that seeing improvements (however small) kept them going and helped them believe they could achieve their goals. They appreciated that the health coach provided feedback and encouragement that conveyed confidence in their ability to make changes and overcome barriers. This, coupled with making goal progress, encouraged participants to seek out opportunities to engage in PA with others and was inexplicably linked to feeling empowered and worthy.
Theme 4: Being in control of decisions promotes perceptions of autonomy
Participants stressed that cancer made them feel like they had lost control of everything, including their bodies. However, they felt that the intervention gave them back some control. They explained that having choice played an important role in helping them to step outside their comfort zones and involve others to reach their goals. Participants felt the constant communication with the health coach who listened to them and helped them create their own goals motivated them to remain in the intervention and continue working towards their goals. Participants appreciated the flexibility of the intervention and the open-mindedness of the health coach because both allowed them to have input over what was covered during the sessions. Participants became more motivated because they had someone to talk to about their own ideas for how to reach their goals.
Theme 5: Motivation for behavior change is dynamic and complex
When asked to reflect on their motivation throughout the intervention, participants described a fluidity to their reasons for engaging in PA and consuming FVs. Participants had primarily extrinsic reasons at the start of the intervention that began to shift to internalized reasons by the end of the intervention. Initially, they adopted a more controlled orientation towards engaging in PA and consuming FVs. The reasons mentioned included social recognition and avoidance of feelings of shame and/or guilt. With time, participants’ motivation became more internalized, and they no longer engaged in the behaviors to “please” the health coach or “avoid feelings of guilt.” Rather, participants engaged in PA and consumed FVs because it made them feel good, which fed their inner drive to keep up with these behaviors. Participants also looked forward to engaging in PA and consuming FVs because they learned that there were different things that they enjoyed and focused on those. Nevertheless, improvements in body composition continued to drive their PA and FV consumption as well post-intervention.
Triangulation
In support of the quantitative data, the qualitative data suggest the intervention facilitated autonomous motivation and behavioral persistence. Indeed, the large effects (r = 0.51–0.53) observed for changes in autonomous motivation likely suggests that participants developed an inner drive for PA and FV consumption, which is supported by participants’ accounts that they developed intrinsic reasons to participate in PA and consume FVs over the course of the intervention. However, the medium effects (r = 0.31–0.34) for controlled motivation suggests that participants continued to have external reasons for PA and FV consumption, and the qualitative data points to weight loss as a reason to stay active and eat FVs.
Moreover, the quantitative and qualitative data suggest the intervention may have facilitated satisfaction of participants’ perceptions of competence, autonomy, and relatedness. Considering the large effects observed and participants’ accounts during the interviews, the environment created by the health coach, along with the use of BCTs, may have helped to enhance participants’ perceptions of competence in making behavioral changes, helped them feel supported and connected to others, and allowed them to decide when and how to take steps to reach their target goals. In addition, the qualitative data helps illustrate how the basic psychological needs possibly relate to each other. For instance, competence and relatedness seem connected because as participants felt optimally challenged and capable of achieving their PA goals and desired outcomes, they also felt more connected to and engaged in PA with others. Participants also highlighted that the provision of choice and freedom to set their behavior goals and pace to meet their goals facilitated feelings of acceptance and connectedness with the health coach, which in turn motivated them to stay in the intervention and continue working towards their behavior goals. These instances of connections between SDT constructs illustrate their potential interrelationship.
Discussion
Framed within SDT, 22 a single-arm feasibility trial was conducted to explore rural-living young adult cancer survivors’ PA, FV consumption, and the motivational processes underlying any behavior changes during a telehealth behavior change intervention. The quantitative and qualitative data were generally aligned and provide some indication that this intervention may help to promote perceptions of relatedness, competence, and autonomy in relation to PA and FV consumption, and facilitate internalization of motivation for these behaviors. Although derived from a small sample, quantitative estimates suggest that changes in SDT constructs and behavioral outcomes from T0 to T1 were generally large, except for controlling motivation for PA and FV consumption. Overall, these estimates, coupled with the qualitative findings, support the notion that a behavior change intervention delivered via synchronous videoconferencing sessions may help to assist rural-living YAs in making positive lifestyle behavior change by enhancing basic psychological needs satisfaction and autonomous motivation for PA and FV consumption. This information can be used to justify a large-scale study to determine the effectiveness of the intervention and identify mechanisms by which the intervention exerts its effects on behavioral outcomes.
In line with SDT propositions, 23 participants felt the supportive environment created by the health coach helped satisfy their need for autonomy, competence, and relatedness, and this enhanced their autonomous motivation for PA and FV consumption. Further, several BCTs were featured in the intervention to provide participants with tangible strategies to self-manage their behavior. Whilst their detailing in this manuscript enables other researchers to replicate components of the intervention, 35 Hagger and Hardcastle 51 suggest the interpersonal style of the person delivering the intervention may influence participants’ uptake of BCTs. For this reason, it is unclear whether the success of the current intervention was due to the content or the way the first author delivered the intervention and communicated with participants. Furthermore, as with many interventions,52, 53 the aggregation of intervention components was done to create as potent an intervention as possible based on theory and literature. 54 Although the results suggest that each component of the intervention may have contributed to participants’ motivation and subsequent behavior change, it will be important to investigate if all components equally contributed to the outcomes. Thus, while testing whether the intervention is effective will be in important, investigation of the key ingredients that lead to the observed changes in SDT constructs and behaviors will help to optimize the intervention and inform future SDT-based telehealth interventions.
The qualitative results suggest that the satisfaction of one basic psychological need may help to promote satisfaction of another need, highlighting possible connections between the three needs, which has support in the literature. 55 Therefore, it may be prudent to explore how to best capture this connection, whilst maintaining and still capturing the unique presentation of each need. Although they have been conceptualized and operationalized as distinct constructs, in practice, it is hard to target and measure a single need without considering other needs. 56 Intervention strategies that promote perceived competence may also promote perceptions of relatedness and autonomy (and vice versa). Accordingly, it may be beneficial to investigate how each need is impacted by an intervention generally and by its specific components.
Cancer provokes a range of emotional responses, 57 close scrutiny of survivors’ lifestyles, 58 threats to people’s social and personal identity, 59 and the need to construct a new identity. 60 It is therefore not surprising that participants’ motivation for change was externally driven initially. However, the current results are consistent with the assertion that motivation is dynamic rather than static, 23 as participants described during the interviews changes in their motivation and experiencing autonomous and controlled motivation concurrently by the end of the intervention. Moreover, although definitive conclusions cannot be made based on the quantitative descriptive analyses, these also suggest that motivation may change. Experiencing both controlled and autonomous motivation is common among populations seeking behavior change due to health reasons. In a qualitative study exploring motivational experiences of people newly diagnosed with diabetes, Sebire and colleagues 61 found that participants described several types of motivation and those further along in their behavior change journey expressed more autonomous reasons for engaging in PA and consuming a nutritious diet.
Notwithstanding the implications of this study, there are limitations that must be considered. First, the quantitative results should be interpreted with caution because of the small sample size and absence of a comparison group. Whilst the results can serve as the foundation for generating hypotheses surrounding possible causal mechanisms, to make definitive conclusions and valid causal inferences, a larger randomized controlled trial employing inferential statistics (e.g., causal mediation analysis) is needed to compare the differences between the intervention group and a comparison group (e.g., usual care, alternative intervention) and draw conclusions about the causal mechanisms. Second, the majority of participants enrolled self-identified as White and female, and they were between 28 and 37 years of age. Including the perspectives of a more diverse sample may have provided a more varied response to the intervention. Additionally, participants were at different stages along the cancer continuum. Although this helped to provide maximal variance within a homogenous sample, it is possible that treatment status and time since treatment completion affected participants’ perspectives and experiences. Fourth, the first author delivered the intervention and conducted the interviews. Although this could have helped to develop rapport with participants, the inherent power imbalance between the first author and participants could have made participants reticent to share negative perspectives, and thus lead them to filter their answers. Last, PA and FV consumption are complex behaviors that may not have been fully captured using the current measures. More comprehensive assessment of PA and FV consumption in future studies is necessary to capture the effects of the intervention on different parameters (e.g., frequency, duration, context of PA; quantity and quality of FV consumption).
Conclusion
Although definitive conclusions cannot be made based on the quantitative descriptive analyses, collectively, the quantitative and qualitative findings suggest that this synchronous one-on-one telehealth behavior change intervention is a potentially promising intervention that may help to support autonomous motivation for PA and FV behavior possibly by satisfying rural-living YAs’ basic psychological needs. Further, findings point to the importance of having a positive attitude, developing resilience to barriers, persistence, and having a health coach who encourages gradual change in order to facilitate autonomous motivation. Hence, these are potentially important targets for future studies seeking to develop new interventions or refine existing interventions aiming to promote motivation for behavior change among those living in rural areas who may be at greater risk of health problems due to limited access to quality supportive care services. However, a larger, hypothesis testing study including an adequate comparison group is needed to determine the effectiveness of this intervention and identify the mechanisms by which it exerts its effect.
Footnotes
Acknowledgements
The authors would like to thank participants for their involvement in this study. This work was conducted while the first author (JP) was supported by a Queen Elizabeth II Graduate Scholarship in Science & Technology. The second author (JB) holds a Canada Research Chair Tier II in Physical Activity Promotion for Cancer Prevention and Survivorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Note
1. Inclusion criteria were based on PA guidelines in use at study conception (Schmitz et al., 2010).