
Abstract
Home telemonitoring is a promising approach in the management of patients with chronic diseases. However, no study has assessed its acceptability and possible service charge in Nigeria. Therefore, this study aimed to evaluate willingness to pay for pharmacist-provided telemonitoring among patients with chronic diseases and to explore its determinants. Hence, using the contingent valuation method, a cross-sectional study was conducted among eligible patients visiting 15 selected community pharmacies in Enugu metropolis, over a period of 3 months. Of the 335 patients who participated in the study, about 40 percent (i.e. 39.4%) were willing to pay an average monthly fee of ₦915.91 ± 485.49 (US$2.99 ± 1.59) for home telemonitoring services. Significant predictors of willingness to pay for home telemonitoring were perceived insufficient income (odds ratio = 0.20, 95% confidence interval = 0.07–0.60, p = 0.040) and health insurance status (odds ratio = 0.39, 95% confidence interval = 0.18–0.86, p = 0.019). Our findings suggest a promising potential for adopting home telemonitoring services among patients with chronic diseases in Enugu metropolis.
Introduction
Non-communicable diseases (NCDs) such as cardiovascular diseases, diabetes, cancer, and chronic respiratory diseases still remain the leading causes of mortality worldwide.1–3 In 2015, NCDs accounted for over 70 percent of death worldwide. Approximately 80 percent of these deaths occurred in low- and middle-income countries (LMICs) such as Nigeria.4,5 Even so, globally, the problem is expected to worsen in the near future as NCD-related deaths are estimated to increase by 15 percent in 2020, with the greatest casualty occurring in Africa, the Eastern Mediterranean, and Southeast Asia. 5 Significantly, NCDs are a source of huge global economic burden. For instance, in 2011, the World Economic Forum projected a cumulative economic output loss of US$47 trillion in 2030 due to NCDs. This loss represents about 75 percent global gross domestic product in 2010 (US$63 trillion). 6 LMICs alone are expected to suffer cumulative loss of US$7 trillion over the period of 2011–2025, an average of nearly US$500 billion annually. 7 Consequently, the 2030 agenda of Sustainable Development Goals (SDGs), adopted at the United Nations Summit on sustainable development in September 2015, identified chronic diseases as an important public health problem. Thus, the target was to reduce premature death due to NCDs by one-third while addressing the risk factors associated with it. 8
Home telemonitoring (HTM) is a promising approach for providing “case management services to patients with chronic conditions and lower access to care.” 9 HTM is a form of applied telehealth. Generally, it is the application of robust technology-driven communication systems for the transmission and collection of physiological data (e.g. vital signs, symptoms) and behavioral data (e.g. medication adherence, lifestyle changes) by the patients and healthcare professionals, respectively, for the purpose of patient monitoring, patient education, interpretation of data, and clinical decision making. 10 Telemonitoring involves the use of audios, video, or other telecommunication technologies to monitor patient status at a distance. 11 Thus, patients’ health information can be transmitted to respective healthcare settings such as the hospital, clinic, and community pharmacy right from the home through an automated process. The commonly used methods of telemonitoring communication include telephone calls, short messages, and video conferencing. 12 The practice of telemonitoring is well documented in developed countries such as the United States, the United Kingdom, Australia, Germany, and China.13–15 Evidently, telemonitoring practice “produces accurate and reliable data, empowers patients for self-care, influences patients’ attitudes and behaviors, and potentially improves their medical conditions.”13,16 Hence, some experts in the field of medical sciences suggest that telemonitoring will play a critical role in patient care in the future. For instance, Meystre 17 observed that long-term disease monitoring of patients at home was the most promising application of telemonitoring technology for delivering cost-effective quality care. Likewise, studies have demonstrated that telemonitoring practice improves clinical and economic outcomes in some but not all disease conditions. 18 For instance, it has been reported that telemonitoring reduces mortality, healthcare cost, and utilization among patients with chronic obstructive pulmonary disease.19–21 It has also been demonstrated to possess the potential to improve primary care management of cardiovascular diseases, even though further studies are required to ascertain the ways through which it improves health outcomes. 22 In addition, satisfactory results have been documented among diabetic patients. 23 However, some studies have reported little or no added benefits of telemonitoring among heart failure patients.24–27
In Nigeria, the proportion of patients to healthcare personnel is steadily increasing at an alarming rate, thus impeding access to adequate healthcare, especially in the hospital setting. 28 Consequently, community pharmacists currently have an additional responsibility as they are closer to the patients, and have the requisite skills and knowledge required for counseling, educating, and monitoring drug therapy for patients with chronic diseases. 29 Therefore, adopting HTM in community pharmacy practice in Nigeria may help ease the burden on its healthcare system. This may provide a suitable platform for achieving SDG’s target of reducing premature mortality owing to chronic diseases in 2030. However, to the best of our knowledge, there is no study in Nigeria that has assessed patients’ acceptability and possible service charge for HTM. Therefore, the purpose of this study was to use the contingent valuation technique in determining the willingness to pay (WTP) for pharmacists provided HTM among patients with chronic diseases in Enugu metropolis, Southeastern Nigeria, and to explore its determinants.
Methods
Study design
This study was a cross-sectional survey conducted among patients with chronic diseases visiting selected community pharmacies in Enugu metropolis.
Study setting and participants
Enugu metropolis is the capital city of Enugu State, located in the Southeastern region of Nigeria. The state is bordered by five other states which include Abia, Imo, Anambra, Benue, and Kogi. The state is densely populated, with a population estimate of over 3.2 million from 2006 National Census. 30 There are about 120 community pharmacies presently registered with the Pharmacists Council of Nigeria (PCN) in Enugu State. Hence, with the aid of an online sample calculator, a minimum of 15 community pharmacies were required for the study. 31 Using convenience sampling techniques, the 15 community pharmacies were selected based on proximity and ease of data collection. To ensure fair representation, five community pharmacies were selected from each of the three local government areas (LGAs) that constitute Enugu metropolis, namely, Enugu North, Enugu South, and Enugu East. All participants enrolled in this study met the following criteria: (1) patients visiting any of the selected community pharmacy for the purpose of filling and/or refilling prescriptions within the study period, (2) adults (⩾18 years), (3) patients with confirmed self-reported diagnosis of one or more chronic diseases such as diabetes, hypertension, asthma, and heart failure, and (4) those who are willing to participate in the study. However, patients with cognitive impairment or unable to complete the survey questions in English language were excluded from the study.
Study instrument
Respondents’ WTP for community pharmacists provided HTM services was elicited using a self-administered questionnaire developed based on contingent valuation principles. 32 The first section of the questionnaire contained patient’s sociodemographic data such as gender, age of respondents, marital status, level of education, occupation, and monthly income. The second section contained a hypothetical description of the concept and benefits of HTM services to patients with chronic diseases. The respondents were then asked “would you like to pay for HTM services?” If “yes,” given the below-listed prices, how much were you willing to pay as monthly charges for HTM services? And finally, what is the exact amount you are willing to pay as monthly charges for HTM services? However, if a “no” response was given to the first question, the patient was then asked, “what is the reason for your unwillingness to pay for HTM services?” The content and face validity of the instrument was assessed by three experts in the field of Pharmacoeconomics and Pharmacy Practice in the University of Nigeria, Nsukka. Pre-test was conducted among conveniently selected 20 patients visiting two community pharmacies in Nsukka district, Enugu State. Afterwards, ambiguous words were reworded where necessary to enhance clarity and understanding of the survey instrument. See Supplemental Material for more information on the study instrument used.
Survey administration
The survey instruments were distributed to eligible patients through six independent research assistants who were trained on the protocols of the study. Subsequently, the self-administered questionnaires were retrieved immediately after completion in the community pharmacies. Where necessary, the research assistants provided clarification to the respondents while completing the questions. On average, it took the respondents about 15 minutes to complete the questionnaire. The data collection lasted for a period of 3 months, between 1 May and 31 July 2017.
Statistical analysis
The data collected were sorted and coded in Microsoft Excel spreadsheet. It was cleaned for correctness and appropriateness. It was transferred to SPSS (Statistical Product and Service Solution) for further analysis. Descriptive statistics (frequency, percentage, mean, and standard deviation) were used to present respondents’ sociodemographic and WTP characteristics as well as their reasons for unwillingness to pay. Furthermore, multiple binary logistic regressions were performed to determine independent predictors of respondents’ WTP employing the Enter method. The WTP (yes = 1, no = 0) for HTM services was used as the dependent variable, while the independent variables were respondents’ sociodemographic characteristics (gender, age, marital status, educational status, occupation, monthly income, income description, place of residence, size of household, health status, history of hospitalization, and health insurance). All analyses were performed using IBM SPSS for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). The level of statistical significance (α) was set at p ⩽ 0.05.
Ethical considerations
The study protocol was approved by the National Health Research Ethics Committee (NHREC) of the University of Nigeria Teaching Hospital (UNTH), Ituku-Ozalla, Enugu State, Nigeria. The ethical clearance had the approval no. NHREC/05/01/2008B-FWA0000245B-1RB00002323. A written consent was sought from eligible respondents before their inclusion in the study. The responses provided by the patients were treated with strict confidentiality during the study period.
Results
Table 1 shows respondents’ sociodemographic and WTP characteristics. In total, 382 eligible patients were identified and approached for the study. In total, 335 participated and completed the questionnaire, giving a response rate of 87.7 percent. Out of the 335 patients, over half were male (54.3%) and between the ages of 45 and 60 years (55.8%). The majority of the patients were married (74.0%) and had a tertiary education (65.7%). Greater than 70 percent of the respondents had a monthly income between ₦18,000 (US$58.82) and ₦100,000 (US$326.80). More than 60 percent had perceived insufficient income and family size greater than four members. Overall, less than half of the patients (39.4%) were willing to pay an average of ₦915.91 ± 485.49 (US$2.99 ± 1.59) to obtain the service.
Respondents’ sociodemographic and WTP characteristics (N = 335).
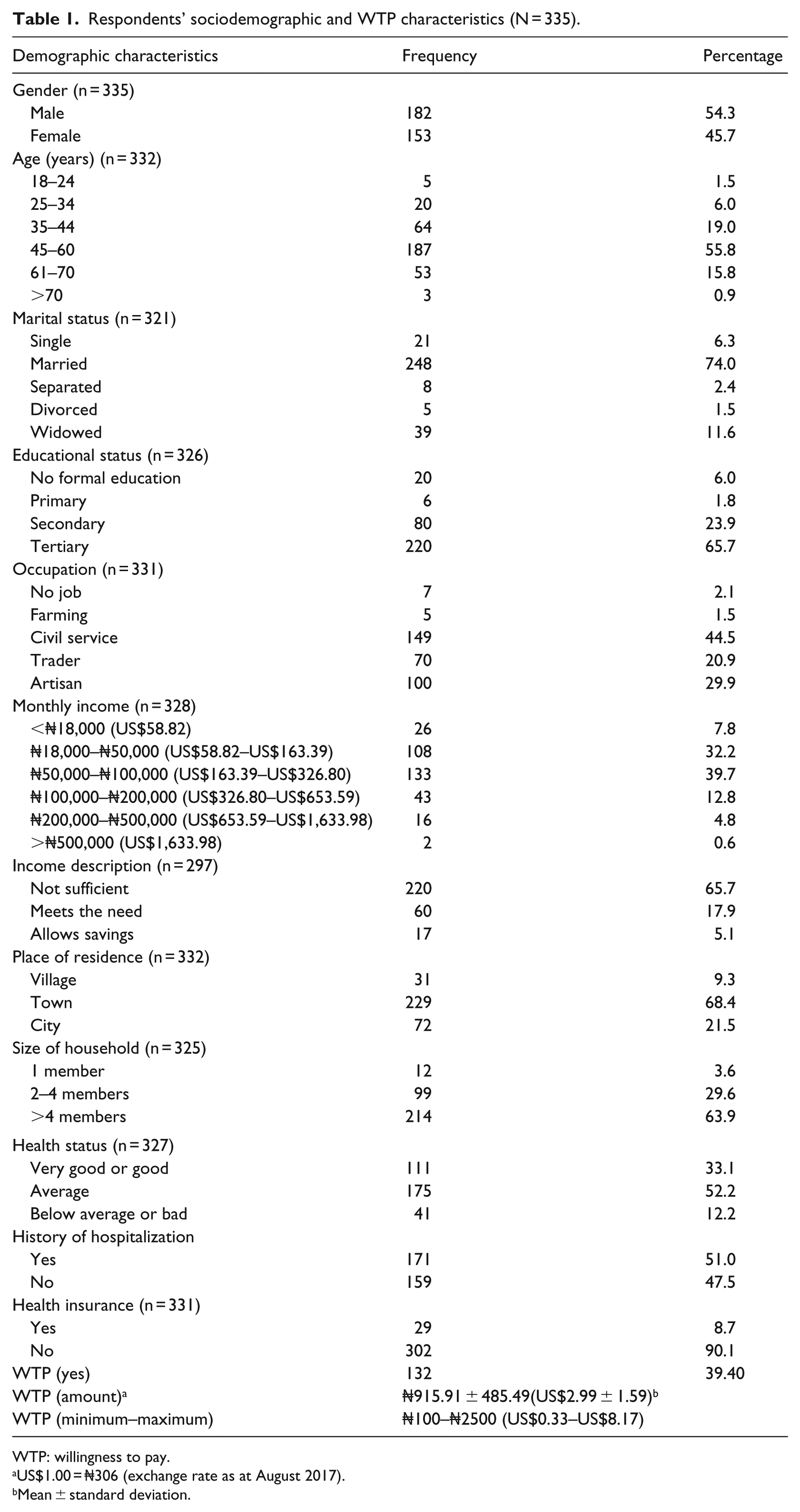
WTP: willingness to pay.
US$1.00 = ₦306 (exchange rate as at August 2017).
Mean ± standard deviation.
Table 2 shows multiple binary logistic regressions of respondents’ sociodemographic variables and WTP for HTM. The results demonstrated that income description and health insurance status were significant predictors of respondents’ WTP for HTM services. Specifically, respondents with perceived insufficient income had five times lower WTP probability for HTM services compared to those whose income allows savings (odds ratio (OR) = 0.20, 95% confidence interval (CI) = 0.07–0.60, p = 0.040). Similarly, patients who were insured had 14 to 82 percent lower WTP odds for HTM services (OR = 0.39, 95% CI = 0.18–0.86, p = 0.019). In addition, no significant associations were observed between WTP for HTM services and other sociodemographic variables (such as gender, age, marital status, educational status, occupation, place of residence, size of household, and health status).
Multiple binary logistic regression of respondents’ demographic characteristics and willingness to pay (WTP).
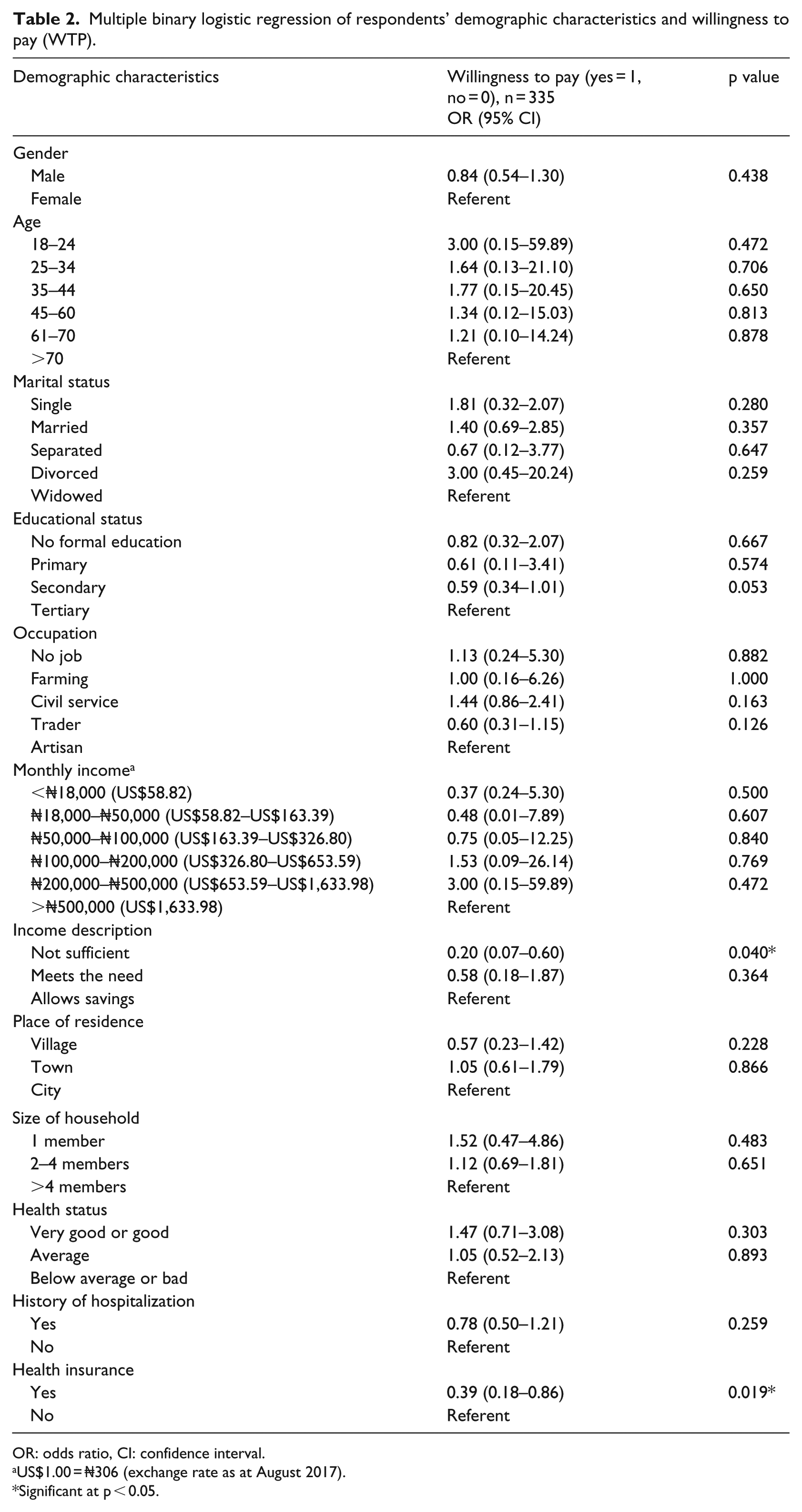
OR: odds ratio, CI: confidence interval.
US$1.00 = ₦306 (exchange rate as at August 2017).
Significant at p < 0.05.
Figure 1 presents respondents’ reasons for their unwillingness to pay. The figure shows that about a quarter of the patients (25.3%) were unable to pay for the pharmacist-provided HTM services. However, less than 10 percent either objected or were against paying for such health services.
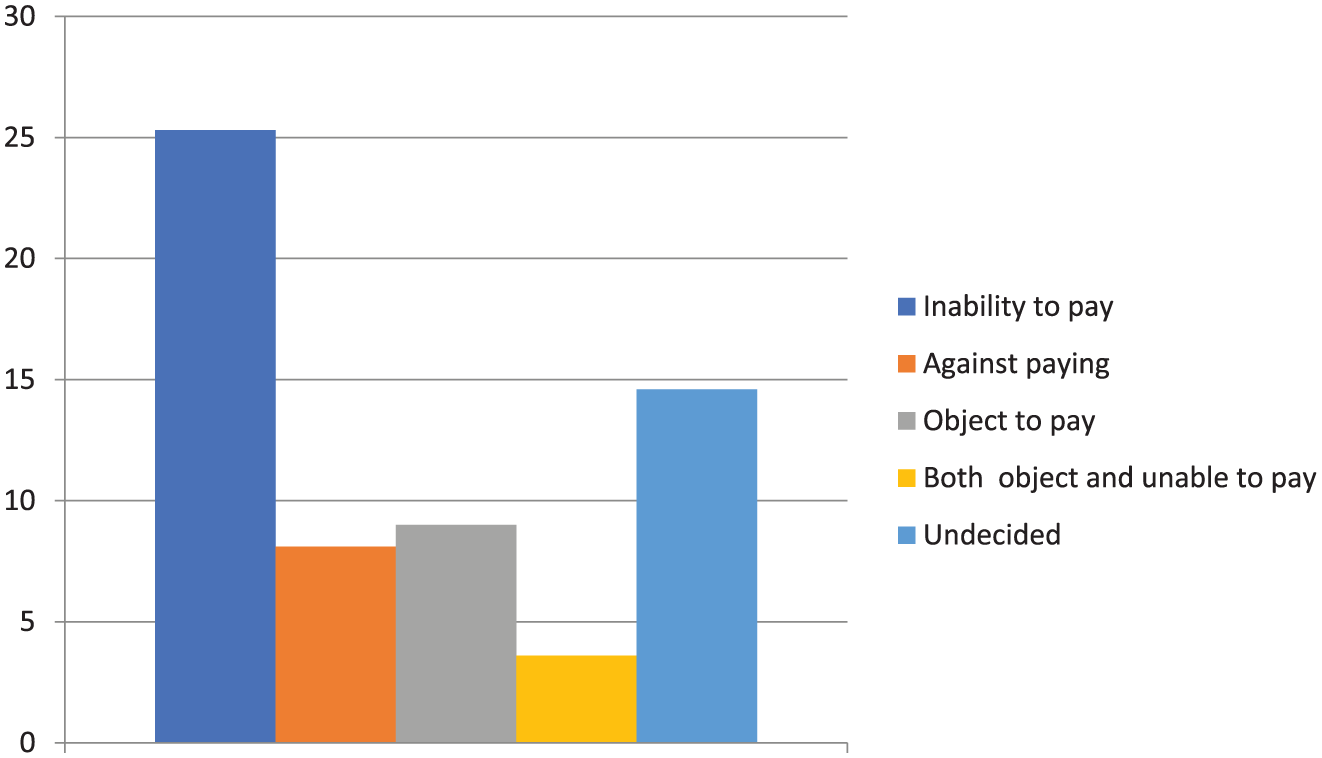
Reasons for patients’ unwillingness to pay (in percent).
Discussion
In this study, we sought to evaluate the WTP for HTM services among patients with chronic diseases in Enugu metropolis, Southeastern Nigeria and to explore its sociodemographic determinants. Our key findings showed that less than half of the patients were willing to pay an average [minimum–maximum] monthly fee of US$2.99 ± 1.59 (US$0.33–US$8.17) to access the services. Income description and health insurance status were significant predictors of WTP odds for HTM services. Respondents who have seemingly insufficient income were less likely to pay for HTM services compared to those whose income allows savings. Likewise, respondents who were insured had lower WTP odds for HTM services relative those without any form of health insurance. However, among patients who were unwilling to pay for HTM services, the most frequently reported reason was an inability to pay.
Our result demonstrates that less than half of the patients were willing to pay an average [minimum–maximum] of US$2.99 ± 1.59 (US$0.33–US$8.17) for HTM services. This proportion of patients probably indicates the extent of patients’ acceptance of pharmacist-provided HTM services. Our finding implies a promising potential of patient charges for telemonitoring services in Nigeria. In addition to the patient-expressed WTP amount, other factors such as the demand for and availability of telemonitoring services may probably play a significant role in determining its socioeconomic value. 33 Similarly, community pharmacy practice regulatory bodies, such as PCN and Association of Community Pharmacists in Nigeria, and other stakeholders could influence a decision regarding possible service charges of HTM practice if adopted. These charges will cover the cost of providing HTM services as well as remuneration for the pharmacists. Nonetheless, the future mode of payment should be such that it will be convenient for patients to pay with relative ease. This is necessary as the present system of out-of-pocket payment for medical bills in Nigeria limit utilization of healthcare services.34,35 Therefore, for patients to fully benefit from HTM services, the government may perhaps incorporate potential service charges as taxes or in health insurance schemes.
Our results demonstrated that patients with perceived insufficient income had lower WTP odds for HTM services. Similarly, previous studies that utilized contingent valuation method in assessing the economic value of certain health services have reported a positive relationship between income level and respondents’ WTP for such services. For instance, Danyliv et al. 36 in their study of WTP for physician services at a primary contact in Ukraine found that lower income was significantly associated with an inability of patients to pay for the services. A similar result was reported in a study aimed at evaluating WTP for nursing consultation. 37 However, Yasunaga et al. 38 found no association between income and the ability to pay for hypertension treatment services. Generally, consumer’s demand for necessary goods and services rises as real income increases. 39 Delayed and erratic payment of salaries for public servants and unstable businesses in most states in Nigeria may have contributed to this finding, as the country is still recovering from an economic recession. In addition, patients with chronic diseases have to deal with other challenges of everyday life such as rising cost of food, housing, transport, and education.
We also found that being insured was associated with lower WTP odds for HTM services. Nevertheless, about 5.4 percent of insured patients in this study were willing to pay for HTM services. Our finding was similar to previously published studies on WTP for healthcare services.36,40 Tsao et al. found that approximately 8 percent of the respondents agreed that they would use medication management (MM) services provided by pharmacists if they had to pay 100 percent out of pocket. Moreover, about 81 percent of the respondents indicated that they would use MM services if an insurance company would cover all the cost. 40 Likewise, Danyliv et al. found a significant difference in WTP for physician services between insured and uninsured respondents. In their study, they reported that respondents who had voluntary health insurance were approximately two times less likely to pay for physician services compared to patients who had no health insurance. 36 Possible explanation for the reluctance to pay for HTM services among insured patients could be because such patients assume that it is the responsibility of insurance companies to cover the cost of healthcare services they utilize including HTM.
Furthermore, our results also showed that inability to pay was the most frequently reported reason for unwillingness to pay for HTM services. The possible implication of this finding is that many more patients could be willing to pay for HTM services at lower prices than was stated on the payment levels. Nonetheless, in real-life situation, such responses may not always be the case.
Finally, the strengths and limitations of this study are worth considering as it will guide the interpretation of its findings. First, our application of the convenience sampling technique in the selection of the community pharmacies used for the study may affect its generalization to other populations, particularly those with different socioeconomic status. However, our selection of an equal number of pharmacies in the three LGAs constituting Enugu metropolis could have ensured a fair representation as different cadres of pharmacies were selected. Second, in order to reduce non-responses, we adopted closed-ended questions and payment levels in eliciting respondents’ WTP for HTM services. In addition, it also mimics real or actual market and its WTP estimates are closer to the real value of the service under evaluation relative to open-ended questions which are fraught with gross outliers.41,42 There was also the possibility of hypothetical bias due to a disparity in survey description and the real market situation may affect respondents’ valuations. Despite that, we limited “yeah-saying” responses, that is, responding “yes” to a question without seriously thinking before giving the answer. Hence, we added follow-up questions to confirm respondents’ choice of value in the design of the instrument. 43 Future investigations among rural dwellers will further enhance the understanding of the pattern of patients’ acceptability and WTP for HTM services.
Conclusion
In conclusion, our findings showed a potential for HTM services in Enugu metropolis, as a substantial proportion of patients were willing to pay for the services. On average, respondents were willing to pay a monthly fee of (US$) ₦2.99 ± 1.59 to benefit from pharmacist-provided HTM services. However, the major contributors of positive WTP among patients were perceived higher income level as well as non-enrolment in health insurance premium. Conversely, inability to pay was the most frequently stated reason for unwillingness to pay for the service. Therefore, health policymakers, in deciding the future charges for HTM services in Nigeria, should be guided by the pattern of patients’ reasons for unwillingness to pay as it supports exemption criteria or special considerations for individuals with little means of livelihood.
Footnotes
Acknowledgements
The authors are grateful to all the community pharmacies in Enugu metropolis that granted permission for the conduct of the study in their facility. They also appreciate the efforts of Pharm. Ikechukwu Cynthia, Pharm. Asogwa Solomon, Pharm. Ugwu Chigozie, Mr Anosike Courage Chisom, and Pharm. Ezeobiora Chijioke, who assisted in the process of data collection.
Author contributions
C.A. and M.O.A. designed and analyzed the work. C.A., O.B.U.-K., and A.I. interpreted the data. C.A. drafted the article. All the authors revised and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.