
Abstract
Missing medications can negatively contribute to the financial and operational workflows of pharmacy departments and add medication safety challenges. The missing medication request (MMR) system at the study institution converted to entirely electronic in June 2018 from a hybrid electronic system. This study evaluated 4-week periods pre- and post-conversion. The objective of this study was to evaluate the impact of conversion to an electronic MMR system on the quantity of requests received at an academic medical center. The average daily number of MMR’s decreased from the pre-conversion group to the post-conversion group (1.77 (±0.16) vs 1.48 (±0.17), p < 0.001). During post-conversion, the median triage time was 8 min [3 min–19 min], pharmacists triaged 62.4% of requests, and 29.6% of requests were declined. Conversion to an electronic MMR system represents one solution to decreasing missing medications. Future studies are needed to evaluate the financial, operational, and medication safety impact of conversion.
Background
The timely and consistent administration of pharmaceutical products remains an important component of providing quality patient care. 1 After a medication is ordered for a patient by a provider, a pharmacist must provide a critical clinical review to ensure the safety and appropriateness of the order. The critical clinical review is conducted electronically through the electronic medical record software where the pharmacist evaluates the clinical status of the patient through the patient’s electronic chart and the clinical implications of the medication order for that specific patient. Once the pharmacist has reviewed and verified the order, the medication must then be obtained by nursing staff for administration. Due to the lack of standardization in on-hand inventory between hospital pharmacies, there are few protocols for medications regarding storage and dispensing. 2 Medications can be dispensed via automated dispensing cabinets, pharmacy technician deliveries, cart fill, pneumatic tube system, or individually handed to a specific practitioner. At the study institution, if a nurse did not have a specific medication, a request for the missing medication could be placed through the electronic medical record (EMR) via an old process. The request served as a notification via a printed medication label to the hospital pharmacy that the nursing staff had not received the medication that was required for a patient.
Missing medications present a true problem to both patients and staff in the hospital. Medication supply and storage challenges represent one major pathway that can contribute toward a medication administration error. 3 It is estimated that missing medication doses may make up to approximately 50% of all discrepancies for hospital-wide medications. 4 Additionally, the higher volume of requests increases the number of phone calls to the pharmacy and the number of distractions to the pharmacy staff. In one study, missing medication phone calls to an inpatient pharmacy accounted for approximately 10% of calls and contributed to distractions. 5 Approximately 45% of medications errors in hospitals and health-systems are due to distractions.3,6 Nursing staff is negatively impacted by missing medications as well, as they are taken away from direct patient care in an attempt to obtain a medication. The benefit of having less interruptions by all staff has benefit that has been shown in several studies.7,8
Solutions to address missing medications have been implemented at multiple institutions with varying results. One study institution implemented a thrice daily cartfill process to replace its once-daily process. This actually led to an increase in missing medication requests, although the authors suggest confounding variables (e.g. increase in nurse adherence to request protocol) may have contributed to the difference. 9 Another institution implemented bedside delivery by pharmacy technicians of medication doses to replace medication room and automated dispensing cabinet delivery, which resulted in a decrease of missing medication requests. 10 Several institutions implemented medication tracking and visibility to nursing staff as a means of addressing missing medication requests, and these programs demonstrated a reduction in missing medication requests that the pharmacy received.11,12 All of these mentioned processes require additional human or technological capital that may present a financial barrier to other institutions depending on their available resources.
Presence of an EMR system has demonstrated value in improving outcomes in previous evaluations. A review of implementation of EMR systems found that healthcare quality can be improved through increasing time efficiencies, increasing adherence to guidelines, and reducing medication errors and adverse drug events. 13 Electronic medical records have the ability to produce large amounts of data that needs validation before it can be accepted and acted upon. Implementing a process to assess data validity within an EMR has been demonstrated to identify corrective actions needed to increase the output quality. 14 Once data has been evaluated and corrected for quality, strategic management of the data is necessary to realize the full impact of the area evaluated. 15
This study institution utilized Cerner® for its EMR. Prior to June 27th, 2018, a missing medication request (MMR) placed by nursing staff resulted in a physical medication request being printed in the main pharmacy as a means of notifying pharmacy staff that the medication was unable to be located. Both pharmacists and pharmacy technicians were responsible for triaging the MMR’s that were printed in main pharmacy. However, since this was a purely paper process, information regarding who triaged the requests, the validity of the requests, and the action taken by the pharmacy staff member on the request was unable to be captured.
On June 27th, 2018, the study institution implemented a completely electronic missing medication system that allowed for previously non-existent data regarding the missing medication process to be collected and reported. Nursing staff were now able to place a MMR through the electronic medical record (EMR) that was able to be received and triaged electronically also in the EMR by pharmacy staff. The new completely electronic system also allowed for electronic communication back and forth through the EMR between pharmacy and nursing staff regarding missing medications. The system was upgraded specifically for MMR’s. Initial education was provided to both pharmacy and nursing staff regarding the process change.
The new technology expanded the information that was available to both pharmacy and nursing staff when placing and triaging the MMR’s. Before a MMR was placed, the nursing staff member would be able to see a history of prior MMR’s that had been placed by previous nursing staff, as well as see if a dose had already been dispensed. Nursing staff members would then need to select a reason why the MMR was placed and have an option to fill out a comment box for further explanation. Once a MMR had been placed, the pharmacy staff member would be able to see the reason why and the comment box. The pharmacy associate would then would select an action taken and have an option to fill out a comment box for further explanation. If a MMR was declined, the pharmacy staff member would be required to give a reason from a selected list or add a free text comment before the action would be deemed complete. A screenshot of a test patient can be seen in Figure 1 that provides an example of the electronic communication on a declined MMR.
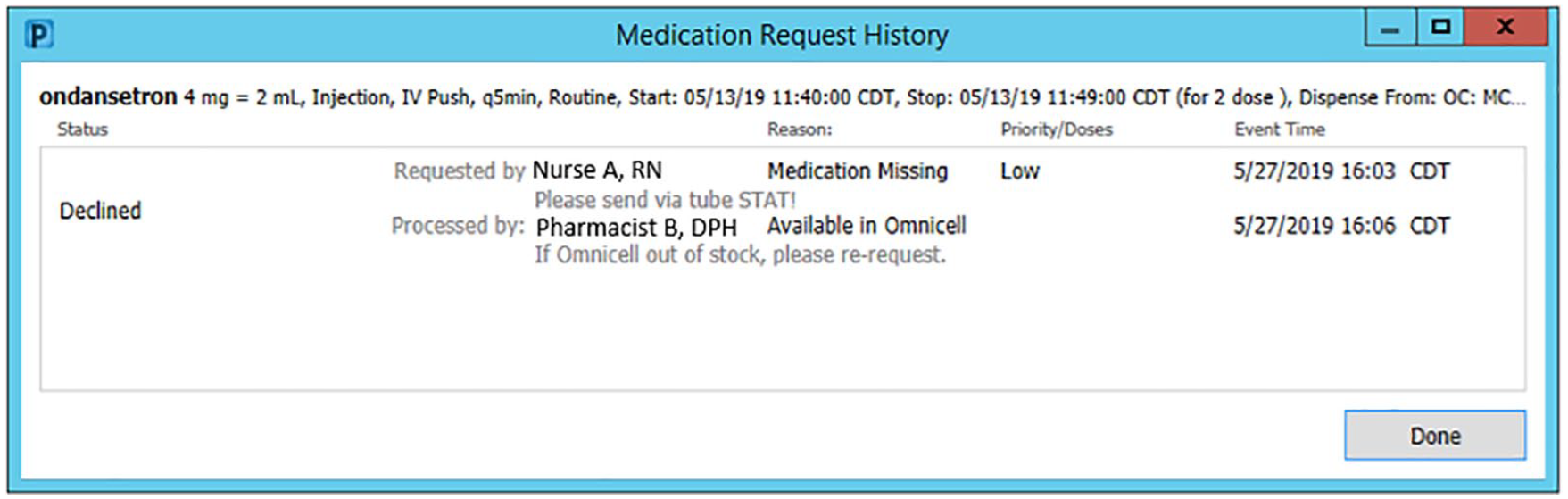
Electronic communication through Cerner®.
The available options for nurses as reasons to place a MMR included missing dose, barcode scanning issue, on-demand medication, Omnicell out of stock, patient emesis, refill bulk medication, wasted dose, and wrong medication received. The available options for action taken by a pharmacy staff member included accept, acknowledge, and decline. The reason for declining a MMR included available in Omnicell, duplicate request, on delivery run, order discontinued, order rejected, and patient takes own. MMR’s that were accepted communicated that a new label was generated for a dose, acknowledged meant that a dose was in progress but no new label was printed, and declined meant that no additional dose was to be expected by nursing staff.
Objective
The new technology had the potential to impact workflow and the quantity of medication requests that were placed per patient. Given this information, the goals of this project were to evaluate the effects on workflow that occurred as a result of the implementation of the new technology as well as to qualitatively evaluate the new data that was now available. The workflow was evaluated to determine pharmacy staff role for triaging MMR’s, and the qualitative evaluation on the new data was conducted to identify further opportunities to optimize stocking and dispensing of medications.
The primary objective study was to compare the average daily MMR’s per patient per day between the pre-conversion group and the post-conversion group. Secondary objectives included descriptive reports about the time needed to triage the MMR, the pharmacy role of the individual who triaged the MMR, and the action taken as a result of triaging the MMR.
Methods
The study occurred over two 4 week periods with a 1 week washout between the timeframes evaluated. Four week time periods were used for the sample size of each group to encompass two biweekly pay periods at the study institution and capture a representative sample of both nursing staff and pharmacy staff users. The intent was to increase internal validity of the study by having the sample closely mirror the institution population. This was a single center study that was conducted at a 615 bed academic hospital in an urban metropolitan city. At the beginning of the washout period, the study institution made the conversion to an electronic MMR system. In the weeks preceding the change, education was provided to both pharmacy and nursing departments to detail the new process and to highlight any changes to workflow. This education was completed through live sessions for pharmacy personnel (pharmacists and pharmacy technicians) and was completed through online modules for nursing personnel. Educational documents were made available for both pharmacy and nursing departments for reference once the change was implemented. Nurses and pharmacy staff were not recruited for participation in this study, as the study was a retrospective review of a new process.
Reports about missing medications were developed by the health-system pharmacy information technology team to allow for data extraction. Data that were included in the report: specific medication that was missing, the time the request was placed, the personnel who placed the request, the patient location, the personnel who triaged the request, the time between request placement and triage, the action taken at triage, and the reason for the action taken at triage.
Data was obtained from Cerner Millennium® medical through generation of reports stored in the EMR. All data points originated directly from the information stored in the EMR. The data was exported into Microsoft® Excel. MMR’s were included if they were placed while the patient was at the study institution. MMR’s were excluded if they were placed while the patient was transferring from a different facility within the health-system. The admitted inpatient census for each day was used to for calculating the average requests per patient per day. Statistical analysis was done with SPSS® statistical program, version 20 (Chicago, IL). The Student’s t test was used for the primary objective, and a p value <0.05 was utilized to determine statistical significance. For parametric data, a mean ± standard deviation was used to report results. For non-parametric data, a median and interquartile range were used. This study was approved by the Institutional Review Board at the University of Tennessee.
Results
Over the course of the study, a total of 1379 different nurses placed at least one MMR. For pharmacy, the staff that triaged the requests included 168 different staff members, which included 73 pharmacists and 95 pharmacy technicians. Demographic and education data on nursing staff and pharmacy staff was not collected beyond the role (i.e. nurse, pharmacist, pharmacy technician).
There were 30,969 requests placed at the study institution over the study period. A total of 30,783 were included in this study for evaluation, with 16,797 MMR’s in the pre-conversion group and 13,986 in the post-conversion group. A total of 186 requests were excluded due to the patient transferring from another facility. There was no difference in the average daily admitted inpatient census between the pre-conversion and post-conversion groups (339.3 (±14.6) patients vs 338.8 (±13.8), p = 0.903).
The primary outcome (Table 1) of average quantity of MMR’s per patient per day demonstrated a decrease from the pre-conversion group to the post-conversion group (1.77 (±0.16) vs 1.48 (±0.17), p < 0.001). There was a decrease from the pre-conversion group to the post-conversion group in the average overall daily MMR’s at the study institution as well (599.9 (±58.2) vs 499.5 (±56.1), p < 0.001).
Quantity of missing medications requested.
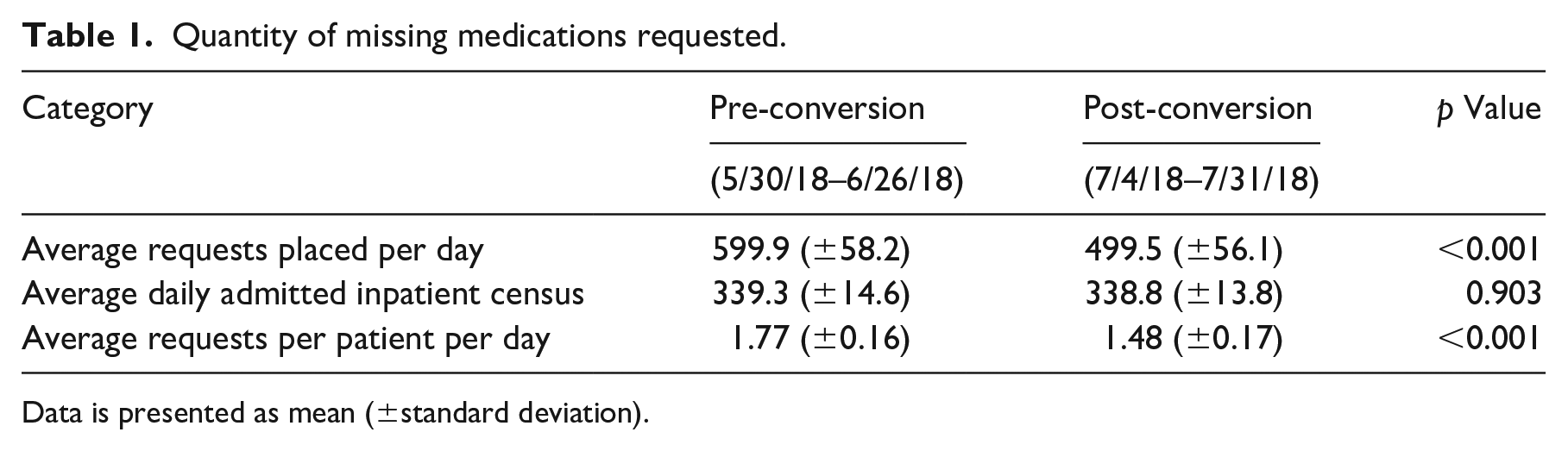
Data is presented as mean (±standard deviation).
The secondary outcome of evaluating the time to triage for the MMR was only able to be evaluated in the post-conversion group. This data point represented the time elapsed from when a nursing staff member places an initial MMR to when the pharmacy staff member triaged the MMR. The data for triage time was non-parametric. The median triage time was 8 min [3 min–19 min]. This information can be seen on Table 2.
Secondary outcomes post-conversion.
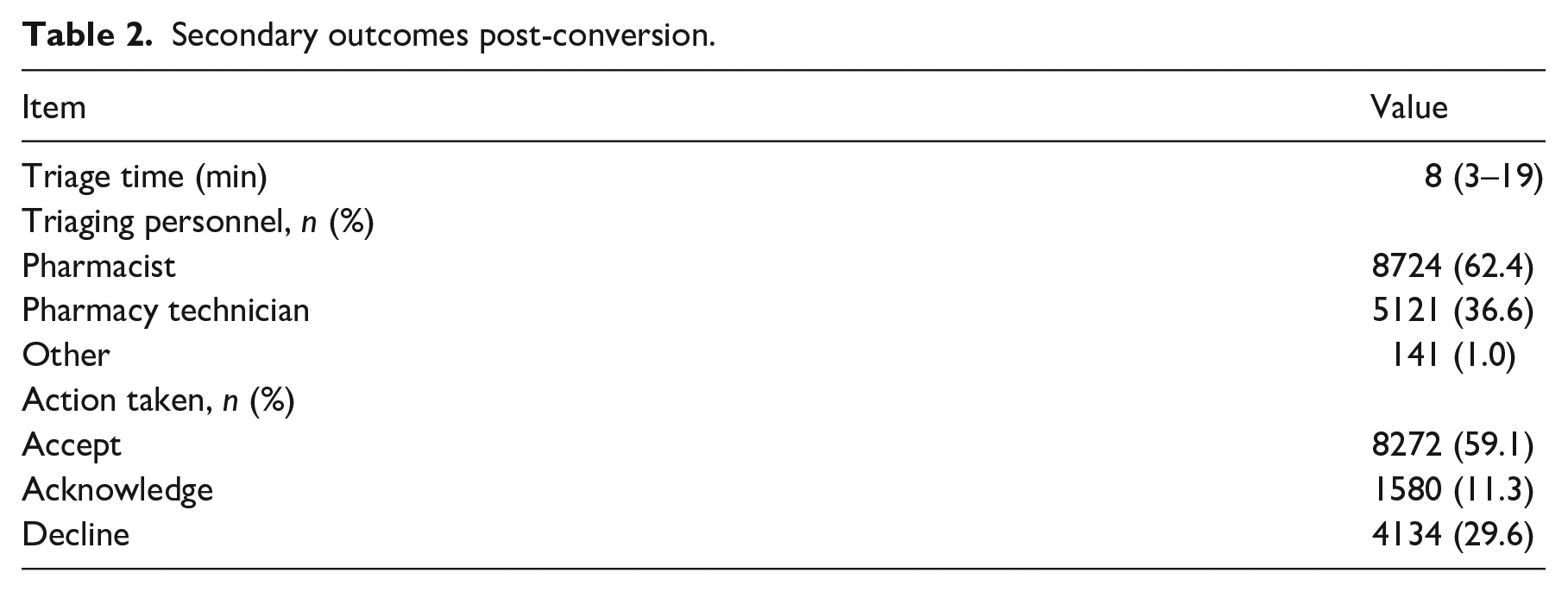
The secondary outcome of triaging personnel was only able to be evaluated in the post-conversion group. The most common role to triage MMR’s was a pharmacist (62.4%), followed by pharmacy technicians (36.6%). The remaining 1% of MMR’s were triaged by a miscellaneous group of other individuals, which included nursing staff updating a previously placed request with additional comments. This outcome provides insight into the impact on pharmacy workflow, and this information can be seen on Table 2.
The secondary outcome of action taken by pharmacy staff members was only able to be evaluated in the post-conversion group. The most common action taken in response to a MMR was accept (59.1%), followed by decline (29.6%) and acknowledge (11.3%). This information provides insight into the validity of the MMR placed by nursing staff and can be seen on Table 2. The reason for declining MMR’s was selected from the available drop down menu on 2547 requests. The reason of “med on delivery run” was the most common reason (n = 962), followed by “duplicate request” (n = 938), and “available in Omnicell” (n = 598). The remaining reasons combined occurred on 49 MMR’s. A breakdown of the reasons for declined MMR’s can be seen in Figure 2. This data was utilized as a tool for future education to nursing staff regarding proper usage of the electronic MMR system.
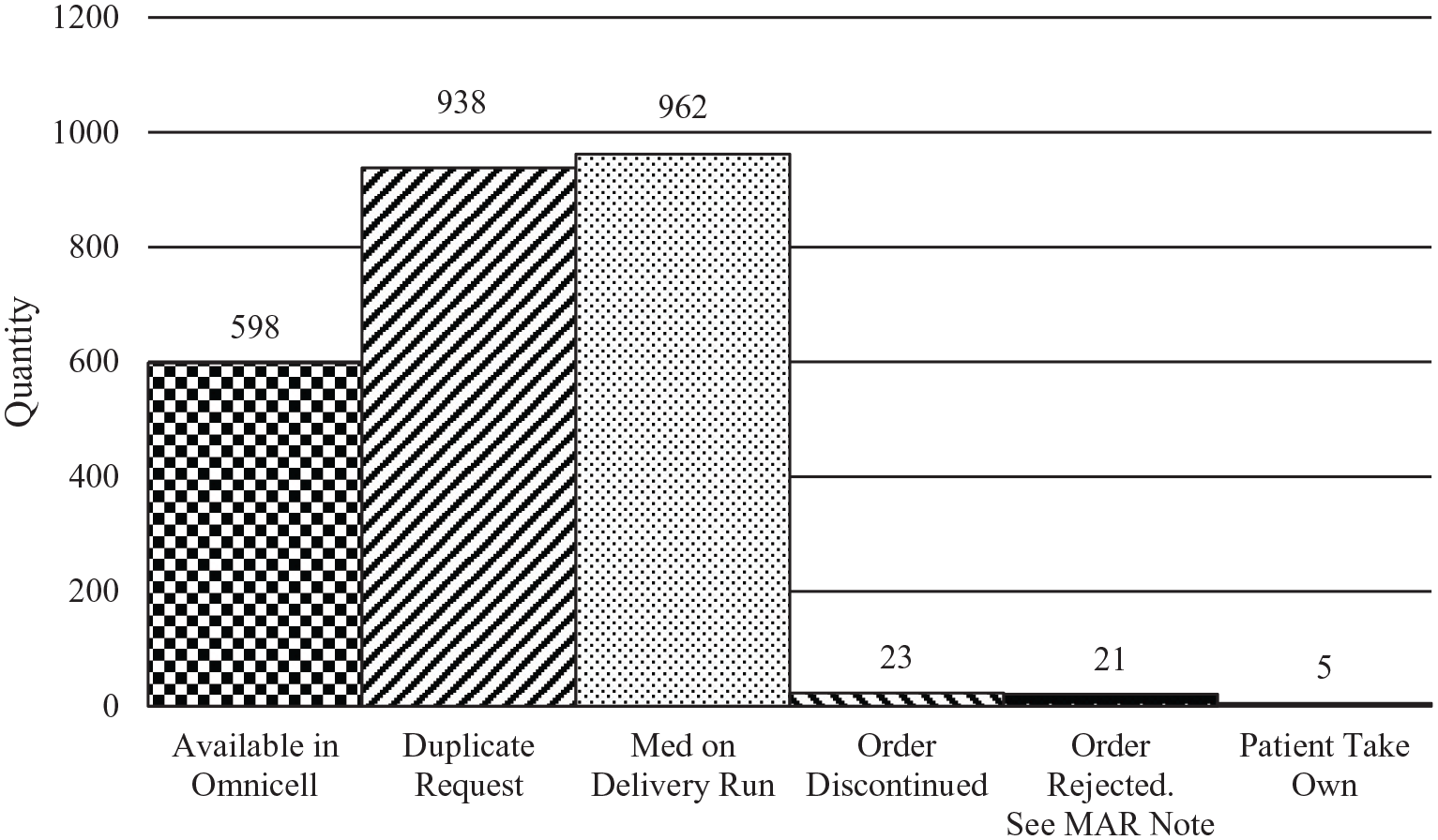
Reasons for declined missing medication requests post-conversion.
Conclusions
Based on the significant findings of our study, the conversion to an electronic MMR process represents one solution that exists within health-systems. In light of other current literature that is available to address missing medications, this represents one possibility to address that may not require as great of a financial or human capital investment. The technology is available within certain EMR vendors already and requires education and implementation. The conversion has a potential financial impact through reduced lost or wasted medications as well as through decreasing the work burden or staffing requirement used to triage the MMR’s, although a quantification of these figures is beyond the scope of this study. Additionally, the study has potential to positively influence medication safety through fewer delayed or omitted doses of medication and can decrease distractions to healthcare professionals.
There are several proposed reasons why the volume of MMR’s may have decreased. First, this enhancement brought visibility, transparency, and real-time electronic communication for the status on MMR’s. Prior to this study, when a MMR was placed, there was no follow-up or information available, unless external communication was made to pharmacy, until the medication arrived on the nursing unit. Additionally, the initial education around the new electronic MMR system provided additional information around the medication distribution processes occurred at the study institution, so nursing staff was reminded of when certain medications should be expected to be delivered.
The time needed for pharmacy to triage MMR’s was valuable information to share with both nursing leadership and front-line nurses to discourage the practice of placing duplicate MMR’s. The pharmacy triaging personnel gave insight on how the current pharmacy operational workflow was addressing MMR’s. Both pharmacists and technicians were trained and capable of triaging the MMR’s, and further discussion about primary responsibility for triaging MMR’s can shift workload to a less expensive resource where the health-system would emphasize decreasing the proportion of MMR’s triaged by pharmacists. Data regarding declined MMR’s provided information that can be shared with nursing staff members to allow further education about the optimal way to place MMR’s that are valid.
There were several limitations to this study. First, there was not a medication tracking mechanism for orders once they left the pharmacy at the study institution, so the decision for the pharmacy staff member to select “med on delivery run” was based on anticipated location of the medication, not actual. Additionally, a confounding variable that was not evaluated in this study was other mechanisms by which nursing staff members request medications, which include phone calls to main pharmacy, requesting medications at the pharmacy pick-up window, and asking decentralized pharmacists on nursing units for the missing medications. The lack of data surrounding actions taken and reasons for those actions in the pre-conversion group prevents a comparison on these data points between the groups. Also, qualitative feedback given by nursing and pharmacy staff was not recorded in the scope of this study from end-users. A record of changes made to support the intervention implementation (e.g. technical issues encountered, changes in EMR functionality) was not recorded for the scope of this study. Finally, potential observer bias may exist to justify the implementation of the new system that could have overstated the impact on reduction of MMR’s.
Overall, the conversion to an electronic MMR system could prove valuable to many health-systems by simply improving communication and transparency when evaluating MMR’s. Knowing different solutions implemented at other institutions and potential limitations for this study previously discussed, this may represent a solution at other healthcare systems and holds moderate external validity. At this study institution, additional education to both pharmacy and nursing staff members could prove beneficial to demonstrate a greater magnitude in the decrease of MMR’s placed. Future studies should include an evaluation on the medication safety events related to missing medications as well as estimate the financial impact of decreasing missing medications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.