
Abstract
Within the anamnesis, medical information is frequently withheld, incomplete, or incorrect, potentially causing negative consequences for the patient. The use of conversational agents (CAs), computer-based systems using natural language to interact with humans, may mitigate this problem. The present research examines whether CAs differ from physicians in their ability to elicit truthful disclosure and discourage concealment of medical information. We conducted an online questionnaire with German participants (N = 148) to assess their willingness to reveal medical information. The results indicate that patients would rather disclose medical information to a physician than to a CA; there was no difference in the tendency to conceal information. This research offers a frame of reference for future research on applying CAs during the anamnesis to support physicians. From a practical view, physicians might gain better understanding of how the use of CAs can facilitate the anamnesis.
Introduction
The examination of patients usually begins with the anamnesis, the most important step in the process of medical care. This serves primarily to collect all relevant medical information, the completeness and accuracy of which are fundamental for further treatment. 1 The duration of the anamnesis mostly depends on the physician’s available time for each patient. However, not only time pressure may lead to incomplete and incorrect information 2 but also the behavior of patients. Recent research has shown that medical information is not always disclosed to physicians. 3 Scenarios in which patients withhold information may lead to dramatic consequences. If a patient conceals the use of freely available or even illegal substances, severe interactions can occur 3 ; for example, the effect of a prescribed medication can be augmented, diminished, or eliminated. Misrepresentation of medical information can lead to mismedication with negative consequences not only for the health of the patient but also for people in their immediate surroundings.2 –4
In contrast, collecting medical information through questionnaires without the presence of a physician can lead to more forthright interviewing behavior than in the presence of a real person. 5 However, a questionnaire is unable to guide the conversation, react to the patient’s statements, and motivate them to continue answering new, related questions over a longer period. 6 In this context, the application of a conversational agent (CA), a computer-based system capable of holding a conversation with a human being, 7 may prove beneficial. CAs are being increasingly applied for health-related purposes, 8 including to assist with the anamnesis. 1 They ask patients questions based on relevance, carrying out a detailed anamnesis for which a physician has no time, and motivate patients to answer the questions completely. 1 The fact that a CA is not a real person might positively influence the response behavior of patients. Previous research has focused on the problem of failure to disclose medical information in multiple instances and under different conditions, but not in relation to CAs used for the anamnesis. In this regard, the application of CAs seems reasonable, although it has not yet been investigated whether patients are generally willing to share information with a CA. Thus, this research aims to provide first insights into the application of CAs for the anamnesis and their ability to elicit further discussion. To formalize the goal of this study, we propose the following research question:
RQ: How do patients’ attitudes toward disclosing and concealing medical information differ when interacting with conversational agents or with physicians?
To answer this, an online survey with German participants was conducted. The respondents were divided into two groups, one of which was shown an example of an anamnesis with a CA and the other was not. Afterwards, participants were asked whether medical information would be readily disclosed or concealed in conversing with a CA or with a physician.
Theoretical background
There are various reasons why patients do not share medical information fully and truthfully, ranging from simple forgetfulness to the fear of being judged negatively. The following section explains these reasons in greater detail, why failure to disclose can have far-reaching consequences, and how CAs may be applied to overcome this behavior.
Disclosure and concealment of medical information
Self-disclosure describes to whom we disclose personal information and is influenced by the extent to which people trust their listener and whether there is mutual understanding. 9 The full disclosure of medical information, such as the patient’s history, symptoms, and health behavior, is mandatory for physicians to determine appropriate treatment processes, achieve the best possible medical care,1,3 and avoid short- or long-term consequences for the patient and others.2 –4 Relevant information is collected in the anamnesis, a conversation between the patient and the treating physician, 6 in which the current health condition and medical history are discussed to yield a correct diagnosis. However, there are various reasons why medical data are concealed and not exchanged with physicians.
The tendency to self-conceal is defined as the active and conscious hiding of personal information which an individual considers negative or embarrassing. 10 Within the anamnesis, patients may consider certain circumstances to be irrelevant, 3 or are unable to remember them due to a pre-existing disease. 4 Excessive administrative burdens, such as gathering various documents from several physicians, and the limited duration of the anamnesis may lead to simply forgetting some information.2,4 Importantly, some patients do not want to share certain information, presenting it differently or incorrectly and even withholding or lying about relevant facts.3,4
According to Tourangeau and Yan, 11 willingness to share information depends on three factors: the sensitivity of the information, the interviewee, and the interviewer. In terms of the anamnesis, the factors that determine whether health-related information is shared with the treating healthcare professional are the sensitivity of the medical information itself, the affected patient, and the treating physician. Sensitive information is described as obtrusive, dealing with topics that are considered inappropriate in everyday conversations, 11 or that affect privacy excessively. 5 Patients are particularly dishonest regarding information perceived as unethical 12 or socially undesirable and unacceptable, 11 even more so if the answer entails legal or social consequences. 5 Research has ascertained that patients are frequently embarrassed to express certain information as they want to be liked by healthcare professionals. 12 Also, patients do not want to be judged as ignorant or awkward thus are more likely to ignore harmful behavior. 3
The disclosure of information to physicians is likely to be avoided 3 and represents a major problem for effective healthcare, however, the application of CAs appears to be a suitable alternative.
Conversational agents in healthcare
Communicating with CAs has several advantages, such as increased willingness to disclose information and the promotion of honest communication. 13 Research has reached no consensus on a consistent definition for the term CA but explains it from different perspectives. 14 CAs differ in their primary mode of communication, in other words, how users interact with CAs, such as text- or speech-based input. They also differ in their purpose, such as whether they are narrowed to one function or can be used in a more general context. In this study and in the context of health-related purposes, the definition of Abdul-Kader and Woods 7 seems most suitable: “A computer program that has the ability to hold a conversation with a human using natural language speech”.
CAs have been applied successfully in health-related tasks, for example, to monitor patients’ health condition 15 or to support diabetes patients in their daily routines. 16 There are even initial approaches to managing health-related information provided by patients. “Ana,” a mobile self-anamnesis application with a conversational user interface, was developed to gather medical information in preparation for therapy. 1 However, there are no CAs yet that are integrated into the entire medical treatment process, 1 but can guide patients through the anamnesis and obtain all relevant medical information to assist physicians in achieving the best possible medical care.
Unlike many physicians, CAs are not limited in their time, so patients may no longer feel pressured and they may thus be less likely to forget to disclose relevant medical information. CAs remain factual, which may remove the perception of being judged negatively and trigger patients to share socially undesirable actions. Despite all the possible positive advantages, research has not yet investigated whether patients are generally more willing to share information with CAs. Therefore, the focus of this study is on disclosure and concealment of medical information; other clearly important aspects, such as acceptance, trust, security, and privacy, are not considered; further research should take these into account. This study is intended to provide initial insights into the topic.
Method
Sensitive information is often misrepresented or held back to a certain extent. 5 A wide variety of instruments have already been used to carry out anamnesis to change this behavior in order to collect all health-related information from patients. The aim of this study is to determine how patients’ attitudes toward disclosure and concealment of medical information differ when interacting with CAs or with physicians.
Procedure
To explore the differences between CAs and physicians in receiving disclosure or concealment of medical information, respondents to the German survey were divided into two groups—one group was asked if they would share information with a CA and the control group were asked if they would reveal their information to a doctor. In both groups, the validity of medical confidentiality was pointed out. The survey was carried out with LimeSurvey, and statistical analyses were conducted using SPSS Statistics software (Version 25) and Jamovi (Version 1.0.7). We used an alpha level of 0.05 for all statistical tests.
To provide participants a realistic picture of an interaction with a CA during the anamnesis, we showed them a sample conversation as illustrated in Figure 1. To ensure that this example is as similar as possible to a typical conversation between a patient and a doctor, the dialogue was validated by an independent physician and confirmed as realistic and authentic. The design—in its language as well as the human attributes—is based on the research of Denecke et al. 1 who developed a mobile self-anamnesis application with a conversational user interface for capturing medical information. In addition, the goal of the CA was explained to the patients and the application scenario was described. In the group with the doctor, the information was simply presented via text since it can be assumed that all participants are familiar with the role of the patient and have been or are currently undergoing treatment. Following the respective explanations, participants were asked about disclosure 17 and concealment 10 of medical information. The questions were further supported with examples of matters considered sensitive in prior research that are regularly asked in anamnesis.3,5
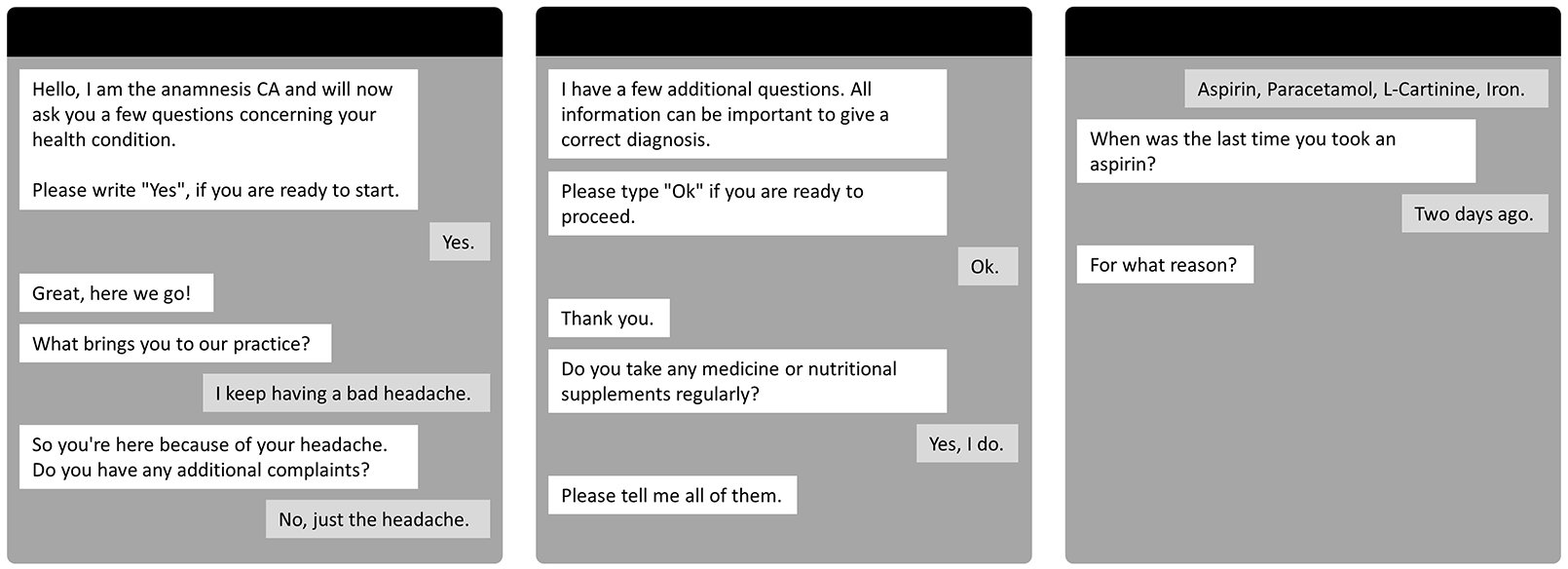
Exemplary anamnesis with a CA.
Materials
To measure the differences between CAs and physicians, two scales for the disclosure and concealment of medical information were used 10 as outlined in the Appendix. Both instruments represent processes that influence the revelation of personal medical information. 9
Self-disclosure
The Self-Disclosure Index according to Miller et al. 17 was adapted to determine the willingness to disclose medical information. Participants were asked to answer eight questions all starting with “To what extent would you discuss the following information with a [CA/physician]?” Examples of the items are: “Information about my alcohol and tobacco consumption” and “Information about my eating habits (e.g. diets, sugar consumption, supplements)”. Following the original version, willingness to disclose information was measured using a 5-point Likert scale ranging from 0 (not discuss at all) to 4 (discuss fully and completely). The translation is based on Reinecke and Trepte. 18
Self-concealment
Cramer and Barry 19 proved empirically the internal consistency and reliability of the secrecy scale developed by Larson and Chastain. 10 The scale uses a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Participants were asked to answer seven questions, again all starting with “To what extent would you discuss the following information with a [CA/physician]?” Examples of the items are “I have an important secret that I’ve never revealed to anyone” and “If I told all my secrets to my friends, they would not like me as much”. The German translation was validated for reliable internal consistency with Cronbach’s alpha values between 0.81 and 0.93. 20
Participants
For recruiting participants, the questionnaire was distributed within a circle of acquaintances and via internal mailing lists in various organizations. A total of 212 people participated in the study, of which 164 completed the survey (77.4%); 16 (9.7%) of the completed response sets could not be included in the analysis due to extreme outliers—values that were more than three standard deviations away from the mean. The participants were randomly assigned into two groups resulting in a sample of 60 (40.5%) in the group with the CA and 88 (59.5%) in the physician group. The baseline descriptives are described in Table 1.
Baseline descriptives in the groups with conversational agent and physician.
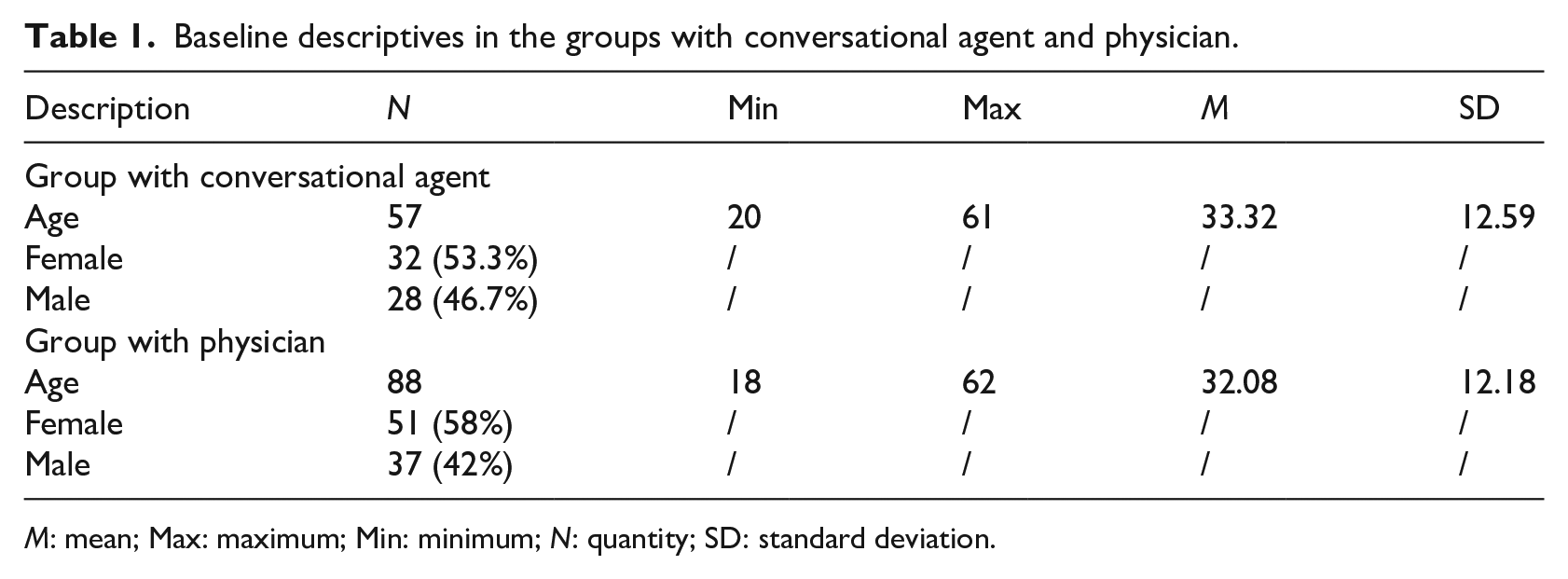
M: mean; Max: maximum; Min: minimum; N: quantity; SD: standard deviation.
Results
Statistical data were calculated for the Self-Disclosure Index and the Self-Concealment Scale (see Table 2). All variables were checked for normal distribution (self-concealment with physician, p = 0.444, from a Kolmogorov-Smirnov test; self-concealment with CA, p = 0.331 and self-disclosure with CA, p = 0.050 from Shapiro-Wilk tests). The scales were further assessed for reliability using Cronbach’s alpha with values around α = 0.7 rated as acceptable. The Self-Disclosure Index had high reliability with α = 0.906 (group with CA) and α = 0.911 (group with physician). The Self-Concealment Scale could be confirmed as sufficiently reliable in the group with the CA (α = 0.705) and in the group with the physician (α = 0.719).
Variables and results in the groups with conversational agent and physician.
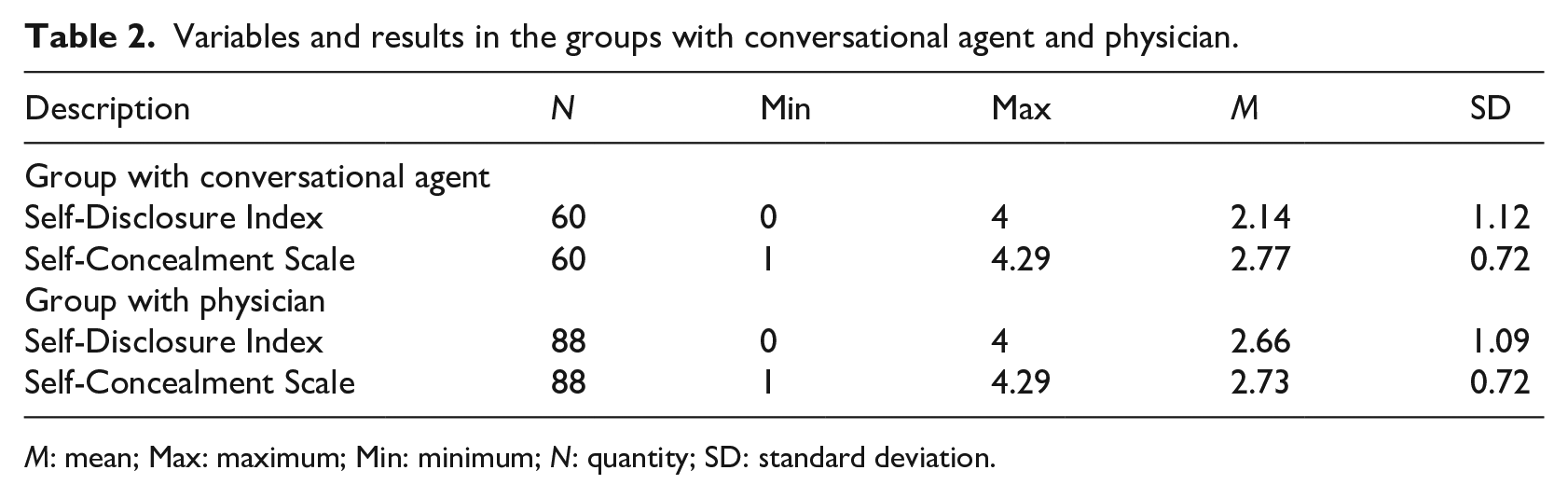
M: mean; Max: maximum; Min: minimum; N: quantity; SD: standard deviation.
For comparing willingness to disclose and tendency to conceal medical information with a CA compared to a physician, a t-test was performed for unpaired samples. The Levene’s test for homoscedasticity of variance showed that equality is given for both constructs between the groups. Overall, on average, participants of the physician group (M = 2.66, SD = 1.09) would rather disclose information than participants of the CA group (M = 2.14, SD = 1.12). This difference was significant t(146) = −2.81, p = 0.006 and represents a moderate effect (d = −0.47). This indicates that patients tend to disclose more information with a physician than with a CA. Further, the results show no overall significant difference between patients concealing information from a CA (M = 2.77, SD = 0.72) or a physician (M = 2.73, SD = 0.72), t(146) = 0.35, p = 0.725 and d = 0.05. This indicates that there are no differences in the concealment of information from a CA or from a physician.
To take a closer look at individual self-disclosure items between the CA and physician groups, we conducted a Fisher’s one-way ANOVA (cf. Table 3). The willingness to provide information about illegal drug use (F(1,146) = 10.034, p = 0.002), sexual behavior (F(1,146) = 12.499, p < 0.001), illegal use of prescription drugs (F(1,146) = 9.636, p = 0.002), and intake of publicly available medicine (F(1,146) = 5.179, p = 0.024), was significantly lower in the group with the CA than in the group with the physician. The mean values of the information on alcohol and tobacco consumption (F(1,146) = 1.245, p = 0.266), physical activity (F(1,146) = 0.776, p = 0.380), eating habits (F(1,146) = 2.388, p = 0.124), and taking medication which was not prescribed (F(1,146) = 2.969, p = 0.087) do not differ significantly between the groups.
Group descriptives of Fisher’s one-way ANOVA.
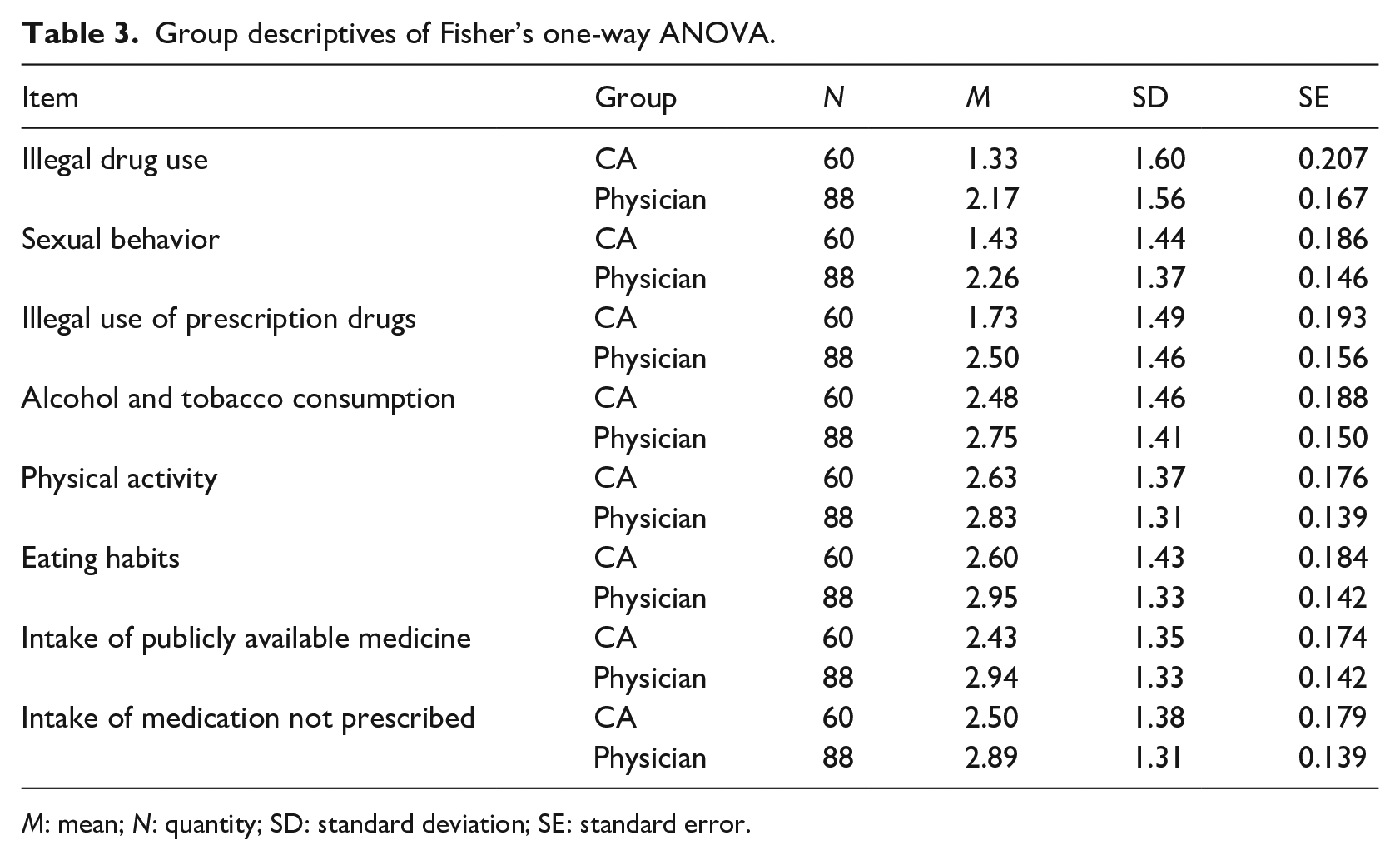
M: mean; N: quantity; SD: standard deviation; SE: standard error.
Discussion
The results of the study indicate that patients prefer to disclose medical information to a physician rather than a CA, and that there are no differences in concealment of information from a CA compared to a physician. Nevertheless, the results show that disclosure with either the CA or the physician is insufficient, underscoring the ongoing problem of medical information frequently being entirely withheld, incomplete, or incorrect. A comprehensive disclosure of all medically relevant information is not achieved in either situation.
Willingness to disclose medical information differs between the groups, but the two are similar in their tendencies to disclose individual medical information—willingness to disclose information concerning illegal drug use, sexual behavior, and illegal use of medication is significantly lower than willingness to disclose other information. The fact that other information is more likely to be shared, such as information on physical activities or tobacco and alcohol consumption, may be explained by the fact that this information is not closely related to taboo topics. 11 Humans are fearful of being rejected or condemned based on certain personal information and secretive about their deviations from accepted norms of society. 21 However, details about tobacco and alcohol consumption may seem more socially acceptable, causing patients to be more likely to disclose that information.
The results of this study show that CAs are generally an appropriate technology to assist healthcare professionals with the anamnesis. Non-critical medical information is disclosed with CAs to the same degree as with physicians. However, the findings also indicate that CAs, in their current form, are not suitable for eliciting medical information assessed as taboo. Thus, CAs can be used for a simple, casual anamnesis, but physicians cannot be replaced by this technology and continue to play a superior role.
This study has certain limitations. No direct interactions with a CA took place. Despite concrete representation and assessment by an independent physician, the topics may have formed different notions from those of an actual interaction with a CA. Participants may have felt that the CA is not an equal conversation partner and did not build a feeling of belonging or social bonding. It might be assumed that a CA does not fully understand and is therefore judged to be useless in establishing a correct diagnosis and proper treatment. In addition, further factors that could be of interest in the context of anamnesis were not considered. Medical confidentiality was pointed out in both groups; anonymity, privacy concerns, the security of the information, and trust in the CA were not explored as influencing factors. Patients may tend to conceal information if they feel that data may be misused or accessible by third parties. Furthermore, this study assessed baseline differences according to the participants demographics, further variables such as specific pre-existing conditions were not considered.
Further research should develop a prototype of a CA for the anamnesis and validate it in real-life scenarios. Studies have shown that CAs are capable of assisting in the execution of work-related tasks and are able to accelerate internal processes.22,23 However, in the health-related context, CAs are not yet widely used, resulting in patients viewing them unfavorably. In addition, the validation of the prototype should further examine additional factors that have not been considered in this study. Alongside other influencing factors, privacy and security aspects should also be taken into account. Exploration of the complete topic requires further investigations to verify whether these aspects may impact in patients’ answers, and taking them into account may lead to CAs achieving better results.
Conclusions
This research provides first insights into the application of CAs for the anamnesis. We have presented results on how CAs differ from physicians in patients’ attitudes toward both disclosure and concealment of medical information by carrying out a study with 148 participants divided into two groups and using the Self-Disclosure Index and the Self-Concealment Scale. The results show that willingness to disclose medical information to a CA is lower than to a physician, particularly for taboo topics. The attitude toward concealing information from a CA does not differ compared to a physician. As practical implications resulting from the findings in this work, physicians gain new insights into patients’ attitudes toward conversations with a CA compared to a physician, and how they differ by topic. Therefore, these findings establish the extent to which CAs might be applicable to facilitate the anamnesis. From a theoretical point of view, this research serves as a first foundation related to self-disclosure and self-concealment in the context of CAs’ usefulness in conducting an anamnesis.
Footnotes
Appendix
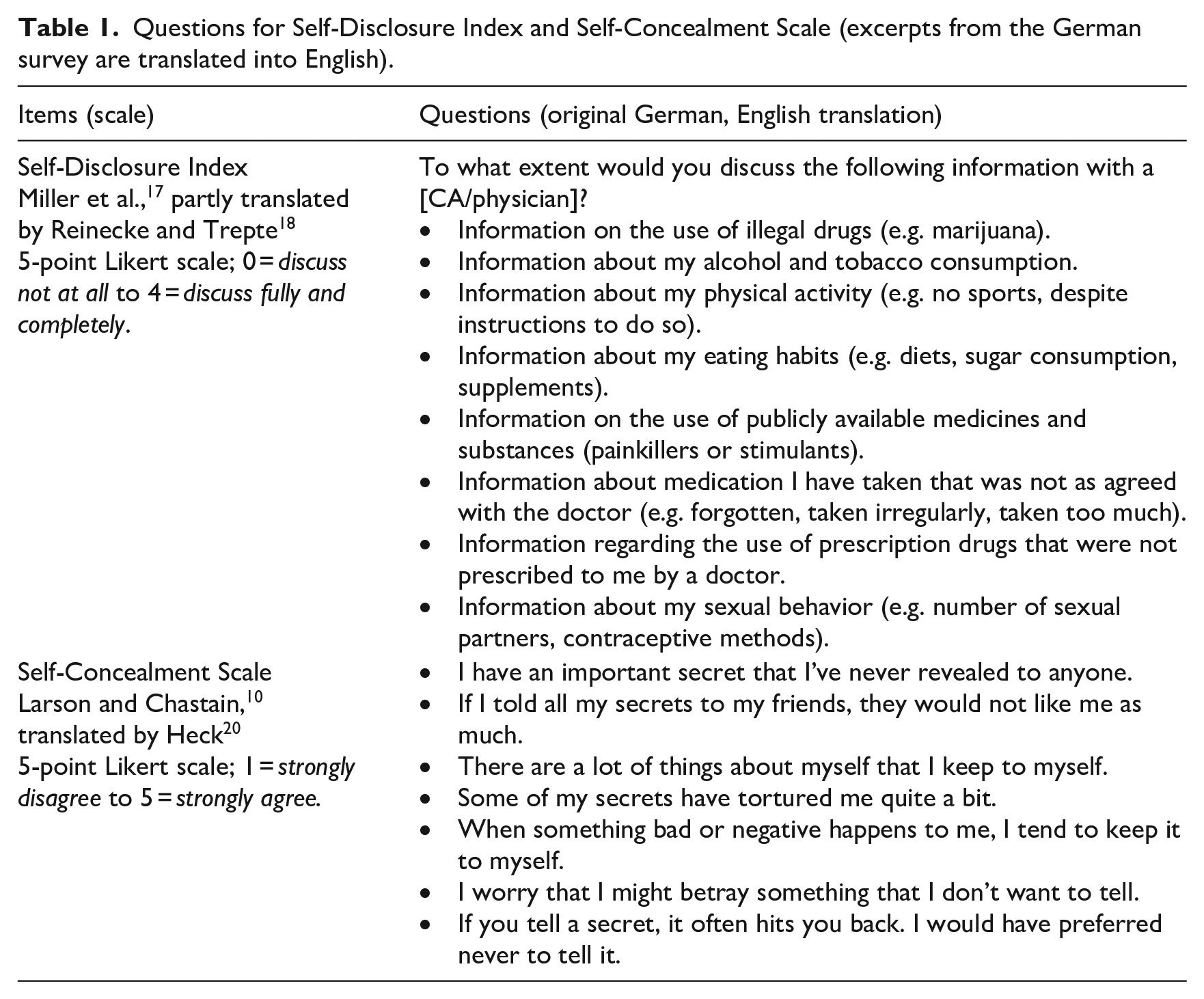
Questions for Self-Disclosure Index and Self-Concealment Scale (excerpts from the German survey are translated into English).
| Items (scale) | Questions (original German, English translation) |
|---|---|
| Self-Disclosure Index Miller et al., 17 partly translated by Reinecke and Trepte 18 5-point Likert scale; 0 = discuss not at all to 4 = discuss fully and completely. |
To what extent would you discuss the following information with a [CA/physician]? • Information on the use of illegal drugs (e.g. marijuana). • Information about my alcohol and tobacco consumption. • Information about my physical activity (e.g. no sports, despite instructions to do so). • Information about my eating habits (e.g. diets, sugar consumption, supplements). • Information on the use of publicly available medicines and substances (painkillers or stimulants). • Information about medication I have taken that was not as agreed with the doctor (e.g. forgotten, taken irregularly, taken too much). • Information regarding the use of prescription drugs that were not prescribed to me by a doctor. • Information about my sexual behavior (e.g. number of sexual partners, contraceptive methods). |
| Self-Concealment Scale Larson and Chastain, 10 translated by Heck 20 5-point Likert scale; 1 = strongly disagree to 5 = strongly agree. |
• I have an important secret that I’ve never revealed to anyone. • If I told all my secrets to my friends, they would not like me as much. • There are a lot of things about myself that I keep to myself. • Some of my secrets have tortured me quite a bit. • When something bad or negative happens to me, I tend to keep it to myself. • I worry that I might betray something that I don’t want to tell. • If you tell a secret, it often hits you back. I would have preferred never to tell it. |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge support by the Open Access Publication Fund of the University of Duisburg-Essen.