
Abstract
This study examines the postures and activities of elders using activity-monitoring device or diary booklet. The research focuses on using the tracked data to assess sedentary behaviors, toss-and-turns, and sleep duration. Fifty seniors participated in the study for 14 days to obtain anecdotal evidence: half of them wore Sookjai, a motion-tracking device; the other half recorded their activities manually via a diary. The results show that they spent most of their time in the sit/stand posture; they tossed and turned during naps and sleep. Both groups showed a similar pattern of activities: the higher level of sedentary behavior is related to a longer sleep duration. Sedentary behavior and naps increased the number of toss-and-turns at night; toss-and-turns did not affect sleep duration. These independent living adults rated themselves healthy regardless of the extent of their sedentary behaviors or tossing and turning. Although the device did not meet all expectations, the seniors did indicate a positive intention to use wearables.
Keywords
Introduction
To cope with the aging society, the governments of developing countries, such as Thailand, must increase the healthcare budget for the elderly. Although government subsidies for health-related expenses have increased in recent years, the rising cost of healthcare for seniors living at home with their families still significantly burdens the government budget. Sasiwongsaroj and Burasit discussed the problem of the public healthcare management system in Thailand; they pointed out that a report from the Ministry of Public Health indicated that the Thai government increased its healthcare budget for medical technologies. 1 Like other developing countries, appropriate public healthcare policies combined with cyber healthcare procedures can address rising healthcare costs. 2 An alternative to costly healthcare services is to provide preventive medicine and health improvement plans that aid the elderly in maintaining good health and independent living for as long as possible. 3 Moreover, researchers in health promotion suggest further investigation on how to integrate activity trackers into community care as health monitoring devices for activity tracking could contribute towards health improvement and fall detection in the elderly. 4 However, it is challenging to determine the type of tracking devices for those living in a non-English speaking countries in addition to the equal distribution among the elderly in need.
Collecting health and activity data automatically with a self-tracking device enables the elderly to be aware of the sedentary behavior in their daily activities. For example, some seniors might sit and watch television all day long; others might walk and exercise a little bit in the morning then sit and nap during the rest of the day. The daily sedentary routines with a low energy expenditure physical activity have adverse effects on senior’s sleep behaviors, causing insomnia and restlessness at night. Moreover, older adults, especially in developing countries, might not recognize that prolonged hours of inactivity can jeopardize their long-term health and well-being.
Different research fields have examined the relationship between physical activity, sedentary behaviors, and sleep patterns. Nevertheless, recent research still reported mixed results between physical activity, sleep duration, and sleep quality.5-8 Moreover, there is a need to determine the relationship between physical activity, restlessness during daytime naps, nighttime sleep duration, and successful aging. 9 Thus, this study aims to determine whether sedentary behavior affects a senior’s sleep duration. The research also intends to provide empirical evidence to the scant studies exploring the effect of restlessness during lie-down postures, specifically the tossing and turning, on nocturnal sleep duration. Finally, the day-to-day usage feedback from the seniors in this study can provide insights into designing and developing a self-tracking device for a non-English speaking retirees living independently in a nursing home with a limited income.
Literature review and hypothesis development
Physical activity and associated postures
An appropriate physical activity (PA) level can yield several health benefits, especially for older adults living independently. Nevertheless, older people might not be aware of the intensity of daily activities, whether low, moderate, or vigorous. As a result, the elders might lose track of time in a given posture while performing an activity that affects their physical function in the long run. For example, if they spend several hours in sitting posture, they may face weakened muscle strength, cardiovascular health, and possible insomnia.
The Metabolic Equivalent Task (MET) is typically used to measure the levels of PA intensity: light, moderate, and vigorous. Many studies use the standard MET values in the Compendium of Physical Activities. 10 The Compendium provides a classification of activities with codes and MET values. For example, the home activity comprises 05041 washing dishes/standing with 1.8 MET, 05023 mopping/standing/light effort with 2.5 MET, and 05036 kitchen activity/cooking/cleaning/moderate effort with 3.3 MET. The self-care activity comprises 13030 eating/sitting with 1.5 MET, 13050 showering/standing with 2.0 MET. The transportation activity shall consist of 16015 riding in a car, bus, or train with 1.3 MET. Finally, inactivity includes 07010 lying quietly and watching television with 1.0 MET, 07026 sitting with 1.3 MET, 07041 standing with 1.8 MET, 07030 sleeping with 0.95 MET, and 07070 reclining with 1.3 MET.
The sedentary behavior of older adults has been widely studied. Prior research found older people spend up to 80% of their waking hours in sedentary positions.11-13 However, the Sedentary Behaviour Research Network proposed to journal editors a standard definition of “sedentary behavior” as any waking behavior that consumes an energy expenditure ≤1.5 METs while in the sitting or reclining posture. The Network also suggested the term “inactive” to describe the people who perform insufficient amounts of moderate and vigorous physical activity (MVPA). 14 Both sedentary behavior and PA intensity constructs use the MET value to measure activities from postures, such as taking a nap by lying down, sitting, standing, walking, and transporting. Using the above definition, an elder’s daily routines 15 can be grouped into three incremental extents of sedentary behaviors: naptime, sedentary time, and inactive time. The first extent includes naptime. The second extent adds the first extent to sitting/standing. Finally, the third extent incorporates transportation activity to the second.
Great research interest has focused on the impact of sedentary behavior and PA intensity level on health. Few researchers suggested that PA intensity level and sedentary behavior were independent predictors of health outcomes. 16 Regardless of the health condition of the elders in residential aged care facilities, prior research did not find a relationship between elderly functional performance and the proportion of time spent in sedentary behaviors and PA. However, healthcare professionals and health-related organizations still recommend PA in daily life. 17 Health promotors also suggest reducing the sedentary behaviors for the wellness and well-being of people in all age groups. 18
Health and PA monitoring wearables
Health wearables for the elderly are gaining momentum; two of the most valuable functions of these wearables are fall detection using Global Positioning System (GPS) and SOS or emergency code signaling for help. For example, the Dring Smartcane, which is not wearable but received the 2017 CES Innovation Awards, detects a fall using motion sensors, an accelerometer, and gyroscope technology. 19 Prior research found that the highest precision wearable to detect falls should be position in the middle of the torso, such as a belt. 20 In Thailand, fall-detection belts are available only in academic laboratories, such as the Chiang Mai University and the King Mongkut’s Institute of Technology Ladkrabang.
Many commercialized fall detection systems focus on elderly clientele, which include a pendant or a clip-on gadget that connects to a base station or a hub. Famous brands, such as Philips Lifeline, Medical Guardian, Medical Alert, Alert1, and LiveAlert, charge a monthly service fee with a 24/7 protection system for approximately one US dollar a day. While these commercialized wearables are promising in the western world, they are not suitable for many developing countries like Thailand. Owing to the language barrier and localized connections to Thailand medical centers and network operators, subscription to the mentioned services is not readily obtainable. Moreover, the living allowance for the Thai elderly is less than USD 30 per month. This amount is barely enough for the elderly living alone with no family support to cover the day-to-day living costs.
With a fall detection device in mind, one entrepreneur in Thailand 21 recognized the economic limitation of Thailand’s aging society as a market opportunity. He worked with researchers in various universities and developed a prototype pendant called Sookjai (meaning “happiness”). Sookjai is an intelligent aid for the elderly that won the IFIA Best Invention Medal in the 2018 International Invention and Innovation Show INTARG® in Poland. 22 It also won the 2018 National Innovation Award in Economic. 23 Sookjai is the most suitable system for Thai seniors as the language barrier is no longer a problem. Neither is for less-educated seniors. Also, Sookjai has gone beyond just fall detection. The hardware and its algorithm were improved to monitor subjects’ movements and analyze their activity patterns. The current design allows users to receive feedback via a mobile application instantaneously. A personalized activity pattern model can also be formulated if longitudinally tracked data are available. The model can be used to develop a customized health promotion program that would extend an elder’s independent living and a better quality of life. Thus, this research chose the locally grown activity tracking system, Sookjai, for the Red Cross-established nursing home study.
Many systematic research reviews in the fields such as technology, sport, and healthcare have increasingly used accelerometer devices to collect PA, especially for older adult cohorts.8,24–26 The signals that are tracked by these devices give an objective measure of different daily activity patterns and sedentary behavior. 27 Although researchers and practitioners tend to believe in the technical accuracy of accelerometer devices; the research method disparities make it difficult to compare the findings from one study to another. The differences include data collection and processing criteria, such as device placement, sampling frequency, non-wearing time, factors that constitute a valid day, PA intensity classification, and algorithms to estimate PA. 28 In a majority of the sedentary behavior studies, the older adults were asked to wear an accelerometer at the right hip for 7 days and found the largest portion of the total wear time as sedentary.11,29,30 Besides small numbers of wear days, ranging from 1 to 7 days, the research results were not generalizable because of the differences in the participant’s demographic, behavioral, and biological variables. 24
The accelerometer-based studies of older adults in the 2010s focused on assessing PA and fall detection in the USA, Canada, United Kingdom, and northern European countries. 30 In these studies, the participants were asked to attach the accelerometer wearables to different body parts, that is, waist, head, and hip/thigh. The wrist watches have become a popular wearable for activity tracking because of the convenience of wearing and size. However, the accuracy of fall detection and Activities of Daily Living (ADL) predictions from the online signals varied greatly, depending on the deep-learning models being used. Also, the models performed better overall on the offline smartwatch dataset than on the real-time experiments, which increased the need for research on older people in a natural living environment rather than on healthy adults in a laboratory setting. 31
Sedentary behavior and sleep duration of elderly people
The two frequent factors that influence senior’s health are PA and sleep characteristics. The reviews of previous research on the relationship between PA and the health and wellness of older adults indicate a positive relationship between healthy aging and different levels of PA. Older people tend to spend a significant amount of time performing light-intensity activities in their daily routine. Thus, the time in the postures associated with these activities, especially the sedentary behavior, is expected to affect older people’s health.32,33 However, the health conditions of elders also affect their sleep patterns and disorders. 34 Chronic diseases and multimorbidity, cognitive decline, and depressive symptoms also affect older people’s sleep, PA, and sedentary behavior.35–38 Older people with 7–8 h and 6–9 h duration of sleep differed in the frailty of their physical function. 39 Sedentary behavior hurts sleep quality; improved sleep quality increases physical, mental, and social well-being.6,8
Although previous research indicated that the baseline sleep duration, or sleep-time, was 7–8 h and too short or too long sleep duration might affect the health negatively, 40 the criteria for setting the sleep duration range were inconsistent in these studies. The sleep habit studies used ≤6 h for short sleep duration; 6.1–8.9 h, medium; and ≥9 h, long.41,42 The Guangdong cross-sectional study used <7 h, 7–9 h, and ≥9 for short, normative, and long sleepers. The presenteeism study of the Australian Health and Social Science Panel classified participants into <7 h, >7–8 h, and ≥8 h. 40 The chronic disease study in Ghana labeled <6 h for short sleepers; 6–8 h, medium; and >8 h, long. 43
The intertwined relationships among sleep duration, sedentary behavior, and health are complex. A study found that patients with Chronic Obstructive Pulmonary Disease with more than 9 h sleep per day had more sedentary behavior and physical inactivity. The inactive elders exhibited more frequent sleep bouts that affected their sleep quality during the night and negatively affected their health. 44 Nevertheless, no association was found between high activity levels and better sleep quality for independently living elders. These healthy people with the highest PA level per week had a sleep duration of ≥5 and <6 h. 5
To examine these complicated relationships and provide additional evidence on the seniors living independently in a Thai nursing home, we propose the following hypothesis:
Sedentary behaviors affect sleep duration, regardless of health condition.
Tossing and turning, sedentary behavior, naptime, and sleep duration of elderly people
According to the Cambridge Academic Content Dictionary, tossing and turning (T&T) is when a person moves around restlessly while sleeping or trying to sleep. Restlessness affects the sleep quality of older people. Previous studies indicate that PA affects sleep disturbances and psychological outcomes of retired elders.38,45 Older people who live in a nursing home tend to suffer more sleep disturbance than those who live at home. 46
Min et al. (2014) built an Android-based application to log in sensor inputs from a mobile phone to collect and relate the T&T data with a self-reported diary of the participant’s sleep quality. Among the 37 subjects that participated in the study, no person is older than 50 years. The authors did not report the number of T&T; instead, they represented T&T for a not-sleep stage or the sleep disturbance by deriving T&T time from sleep duration, bedtime, and waketime. 47 Although mobile phones are an easy and cheap technology for sleep quality study, recent studies used pressure sensors and developed an algorithm to detect in-sleep activities from the vibration data. 48 The number of T&T events was employed as one of the sleep parameters in the 1-year study of 37 Swiss seniors who live at home. A pressure sensor under the mattress detected body movements, duration in bed, out of bed, awakening, and so on. The researchers gathered perceived health status and health-relevant events weekly and found the total number of T&T events per night to be the strongest predictor of a senior’s health. The elders with more than 200 T&T events per night reported higher numbers of health-relevant incidents, such as heart failure, hypertension, abdominal tumor, seasonal flu, gastrointestinal problems, and urinary tract infection. 49
No concrete evidence has been reported about the elder’s use of an accelerometer to track the number of T&T on daytime naps. Even though previous research links sedentary behaviors and elderly naps with sleep quality, an explicit differentiation of naps from other sedentary behaviors would warrant a better insight into the effect of T&T on sleep quality and elderly health. The algorithms of the wearable device in the present research were designed to track a lie-down posture on a 24/7 basis, specifically Naptime, Sleep-time, number of T&T during nap (No.T&T-Nap), and during sleep (No.T&T-Sleep).
In a critical review of the nap paradox, the authors suggested that midday naps benefit health. However, frequent naps can lead to adverse health outcomes for older people. 50 The relationship between napping and nocturnal sleep was inconclusive in Taiwanese elders. Some indicated that if they took a nap for more than 1 h in the afternoon, they would toss and turn about 20–30 min before sleeping at night. Thus, more research is needed to determine whether daytime napping causes fragmented nocturnal sleep and affects the health of older people. The T&T events of afternoon naps and nightly sleep can provide a more comprehensive assessment of disturbances in sleep duration and quality. Moreover, as naptime is a part of sedentary behavior, we proposed the following hypotheses:
Sedentary behaviors affect T&Ts.
Nighttime T&Ts negatively affect sleep duration. This present study focuses on integrating behavioral theories and biophysical characteristics, mainly the relationships between sedentary behavior, in-sleep activity, and sleep duration, addressing a high-priority research issue. Only a few empirical studies were available on factors that influence the acceptance of health-related technology among the elderly; even fewer studies were found for developing countries, where retirement stipends barely cover the cost of living.51–53 Therefore, research evidence from the present study should add to the scarcity of research regarding the perception and use of wearables for tracking physical and in-sleep activities in older people’s everyday lives in Asian countries.
54
In addition, the study overcomes some limitations from previous studies on physical activity tracking, including using an interview battery or survey methods to assess the acceptance, card sorting exercise and focused group to determine monitoring needs, and fitness trackers for health monitoring in older people.55–58 Those studies provide retrospective insights on the attitude and perception of device acceptance factors; however, they fall short of accessing real daily usage experience by seniors. Furthermore, the findings can add to the literature of the effect of sedentary behavior on sleep characteristics and senior’s health,59,60 usability and adoption of mobile tracking technology,61,62 acceptance of in-home health monitoring for aging in place,
63
and data analysis model of a real-time personalized tracking experience.
64
Research ethics
All participants were informed about the study objective and signed consent forms. Project number 154.2/62 received ethical approval (CAO No. 103/2563) by the Research Ethics Review Committee for Research Involving Human Research Participants, Group 1, Chulalongkorn University.
Methods
This study collected data from three sources: the automated signals from a local activity monitoring device, the manual records of daily activities in a diary, and a self-administered questionnaire. Participants were drawn from the survey respondents in related research examining three factors influencing the intention to use health monitoring wearables: acceptance of personal health data collection, acceptance of technology, and acceptance of a health monitoring device. 65 The research design divided participants into the device user group and diary recorder group.
Sampling and setting
The sampling frame consists of the elderly living in a Thai nursing home; the facility comprises eight buildings with apartments for seniors having medical personnel available on-site 24/7. Most of the subjects are independently living single female retirees who are using their pensions for their living expenses. In a related study that entails pre-post surveys examining factors influencing the intention to use the wearable devices, 108 seniors answered the pre-questionnaire, and 60 answered the post-questionnaire. The sample selection used stratified random sampling on three different age groups (the 60 s, 70 s, and 80 s) to select 60 out of the 108 seniors who answered the pre-questionnaire: 30 of them were to wear the device, and the other 30 were to record activities with a diary manually. The researchers sent out the invitation letter explaining the study’s objectives. 26 out of 30 (86.67%) volunteered to use the wearable device called Sookjai; 28 out of 30 (93.33%) to record their activities in a diary manually. The seniors who wore the Sookjai device will henceforth be called the “Sookjai group,” the diary recorders, the “Diary group.”
Each participant is assigned an anonymous identification: “s#” is for those participants who use the wearable device; “d#” for the participants who use a diary booklet to record movement and activities. After 14 days of data collection, only 50 out of 54 respondents completed the task. One of the participants in the Sookjai group passed away during the data collection period; his incomplete signal data (s23) was excluded. Thus, only 25 participants were counted for the Sookjai group. Two diary records from the Diary group were unusable (d21, d26), and 80% of the data from another participant were missing (d19). Thus, only 25 participants were counted for the Diary group. The final response rate was 83.3%.
Profile of participants.
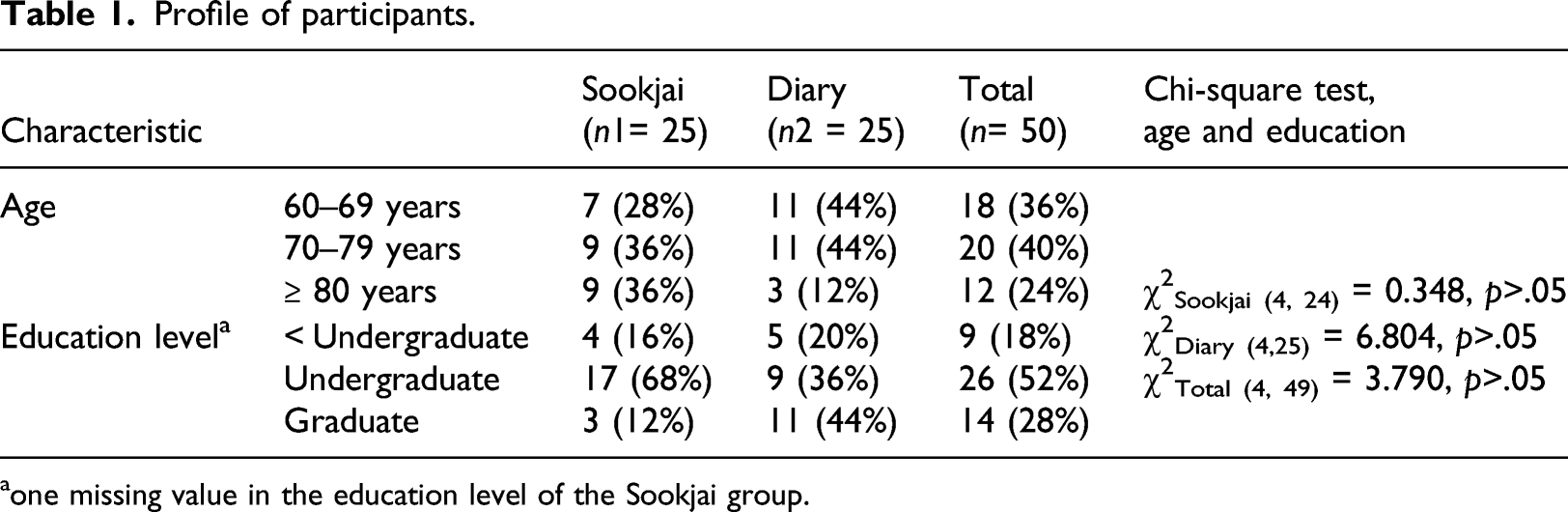
aone missing value in the education level of the Sookjai group.
Data collection
Automatic posture/activity tracking with the Sookjai wearable
Supplemental Material A provides a snapshot of the device and brief technical details. Subjects wearing the Sookjai pendant send motion signals via the Internet using the mobile phone that links to a centralized server. The server processes the signals and translates them into different postures or activities. The application on the mobile phone displays the amount of time the user was in different postures. Daily, weekly, and monthly posture times are also displayed as sections of a circle. If a falling posture is detected, the device will sound and send an alert signal to the server that automatically connects to caregivers or relatives listed in the database.
The Sookjai group was required to wear the device for 14 days. Prior to data collection, the researcher spent 2 h explaining the research objective, training the participants on charging the wearable’s battery, pairing the device with the mobile phone, working with the application, understanding its display, among other things. Replacement of the device was made easy with the on-site coordinator, who helped answer simple questions and monitored the situation to ensure few signal transmission interruptions.
Activity/posture tracking with the diary booklet
The diary format passed the test of two experts who commented on the layout and ease of use through 2 hours of in-depth interviews. After adjusting the font, layout, size, and method to fill the diary, the final version of the booklet was printed on color paper (A4 size), folded in half, and packed in a light handbag with an erasable pen. Example booklet layout is provided in Supplemental Material B. The diary recording process was designed to ensure mobility and ease of handling by the elderly. Then, six elderly individuals tested the recording in the diary for 7 days; they did not find any difficulty recording their daily activities and corresponding postures.
Like the training for the elderly wearing the Sookjai device, the researchers spent 2 h explaining the objective, obtaining a signed consent form, distributing the diary booklet, explained and had the participants try filling out activities and associate postures in the diary. Seniors were asked to record their activities in the diary for 14 consecutive days as well.
Participant’s support and feedback
Two well-trained coordinators were designated to provide any assistance required by the participants. One person was the caregiver at the nursing home, and the other was the research associate who was on-call 24/7. Both coordinators monitored the device signals on a tablet that shows the status of all Sookjai users simultaneously. They also assisted the Diary group with any questions that arose from the manual recording participation. The device developer company also appointed one technician at the training session to serve as a helpdesk at the nursing home 4 times during the 14 days of data collection on the last 2 weeks of January 2020. A post-questionnaire survey was sent to all seniors in the nursing home in April 2020. Only 54 of them responded because many left the nursing home and went to stay with their relatives during the first wave of COVID-19 in Thailand. The nursing home did not allow any visitors for 3 months. In the middle of June 2020, the researchers had permission to organize the focus group and obtain the results. The seniors, on-site caretakers, and the nursing home staff participated in two group discussion sessions. The focused group discussions with nine to ten participants per group were carried out to obtain feedback and verify the study results.
Measurements
The constructs identified in the study hypotheses are sleep duration, sedentary behavior, and T&T. This section explains data sources, scales, and the equations used for measurement calculation.
Sleep duration has been used as a dependent variable in numerous wearable tracker studies.66 In this study, the Sookjai device automatically collected the older adults’ duration of nighttime sleep, interchangeably called sleep-time. The analysis used each participant’s average sleep-time calculated from the collectible data during the 14 days of data collection. The number of hours of the nighttime sleep duration of the Diary group was extracted from the wake-up time and bedtime recorded in the diaries. The duration of daytime nap hours of the two groups was collected from the same sources.
Sedentary behaviors are based on the definition used in the Compendium of PA.
10
In this research, we combined sitting and standing into Sit/stand posture because the transition time from sitting to standing and vice versa was negligible.
67
Moreover, the elders live in a small room of approximately 15–20 sq m, with a countertop kitchen, a small living space, and a bathroom. The nursing home has all recreation facilities and sells ready-to-eat food on the ground floor, thus requiring minimum walking activity. Thus, sedentary time includes the time in sit/stand and nap postures because the elders are likely to be in reclining or lie-down posture while taking a nap, consuming 0.95–1.3 of the MET values.
10
The sedentary behaviors in the present research can be observed in three incremental extents: Naptime, Sedentary time, and Inactive time. The time was operationalized by the average number of hours per day and the percentage of awake time of those three sedentary extents. Thus, the measurements and their notations (in italic) of sedentary behaviors were calculated from the participant’s data as follows: Total awake time = Total data collectible hours – sleep hours (Sleep-time) Naptime = The time in Nap posture %Nap = (Naptime/Total awake time)*100 Sedentary time = The time in Sit/stand posture + Naptime %Sedentary = (Sedentary time/Total awake time)*100 Inactive time = Naptime + Sedentary time + time in Transport posture %Inactive = (Inactive time/Total wake time)*100
T&T, tossing and turning, an in-sleep activity during both daytime naps and nighttime sleep was tracked automatically by Sookjai. Thus, the analysis and tests of hypothetical relationships would cover only the device wearer group. The device detected the number of T&T and the length of time when the elders were in a lie-down posture. Therefore, two T&T metrics include the number of tosses and turns during daytime naps (No.T&T-Nap) and nighttime sleep (No.T&T-Sleep). Two per hour metrics, T&T/h-Nap and T&T/h-Sleep, were calculated and used for analyses.
Health-related data was used as a control variable in elderly behavior studies, such as physical activity, sedentary time, sleep quality, and sleep duration.6,8,40 The present study considered the health-related items in the self-administered questionnaire of a related research project. 65 This construct addresses the physical, cognitive, and mental problems of older people. 68 Physical problems embrace the risk of falling caused by the aging of posture and balance functions that might lessen the independent style of living of the elderly. The PHSES measures fundamental sensory receptor problems (P), including hearing (H), seeing (S), and eating (E).69,70 Problem with sleeping (S) that affects health is also included as part of this combined measure.43,71 Cognitive health was the self-perception of the elders about their health. Health 6 m enquired from the elders whether they had health problems in the past 6 months and Chronic Disease whether they have any chronic medical conditions. Mental health employs the validated depression scale, Depress 9Q, which consists of 9 questions developed by the Department of Mental Health, the Ministry of Public Health in Thailand. PHSES, Health 6 m, and Depress 9Q used the 5-points rating scale (1–5). Fall 2 year asked whether the elder had a fall experience in the past 2 years. Both Chronic Disease and Fall 2 year use a no/yes answer (0, 1).
Data analysis
The activity data of the Sookjai and Diary groups were compared by the average per hour of each posture for every person and then by three age groups. These averages per hour were cross-checked with the data collected from a short open-ended questionnaire answered before the 2-week data collection. The questionnaire asked the subjects’ wake-up time and sleep time, daily routine activities (such as cooking, exercises, rest, and hobbies), the approximate number of hours spent on each activity, and whether there was a difference in these routines for weekdays and weekends.
The data were analyzed using IBM SPSS StatisticsTM 22; the significance was set at two tailed p < .05. The descriptive analyses of all variables were presented with a t-test or Chi-square test to compare the Sookjai and the Diary groups. Spearman rank-order correlation (ρ) and Pearson correlation (r) were used to determine the association among variables in groups separately and in combination. The differences in sedentary behaviors according to age groups were analyzed using ANOVA. Regression analysis was used to test the hypotheses for the two participant groups.
Descriptive anecdotal evidence from the focused group is provided on the experiences the seniors had during the data collection period, the problems and obstacles they encountered, and factors that would encourage them to use the activity tracking device.
Results
This section organizes the analyses into three subsections: Descriptive analysis of measurements, comparing the two groups, Sookjai and Diary; Hypothesis testing results of the relationships between the sedentary behavior, tossing and turning, and sleep duration with health data as a control variable; and Result verification and participant’s feedback.
Descriptive analyses of participants
Compare Sookjai and Diary groups on postures, sedentary behavior, T&T, and health data.
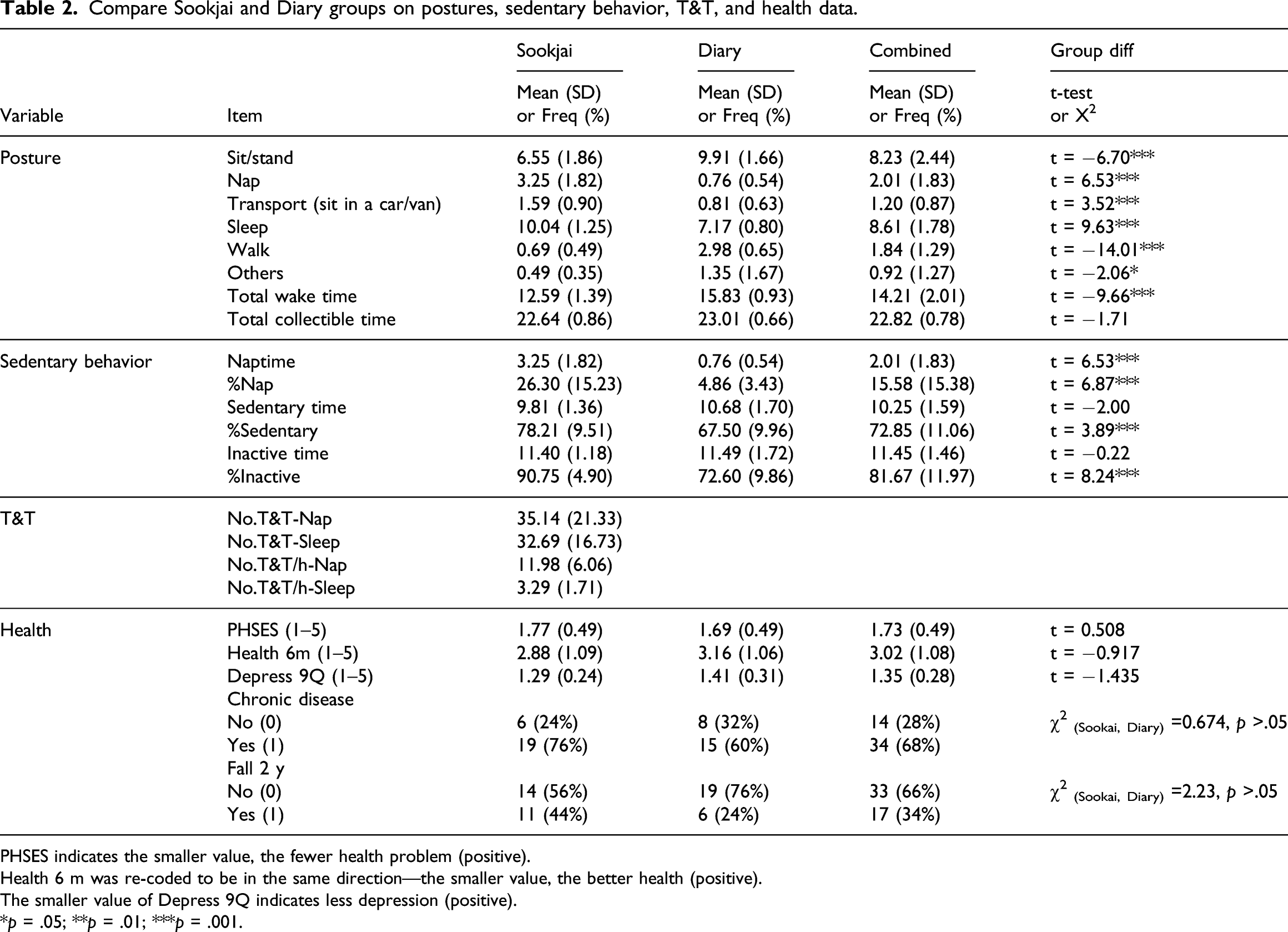
PHSES indicates the smaller value, the fewer health problem (positive).
Health 6 m was re-coded to be in the same direction—the smaller value, the better health (positive).
The smaller value of Depress 9Q indicates less depression (positive).
*p = .05; **p = .01; ***p = .001.
Although the total collectible time of the two groups did not differ much, the wake time did at .001 level of significance (twaketime=−9.66, p = .000), and the Sookjai group had a lesser wake time than the diary. The minimum, maximum, and average hours of wake time were Min.= 9.99 h, Max.= 17.90 h, Mean (SD)= 14.21 (2.01) for all study participants. The Sookjai group took longer naps than the Diary group. The two groups differed statistically at .001 for both naptime (tNap = 6.53, p = .000) and %Nap (t%Nap = 6.87, p = .000). Although sedentary time and inactive time of Sookjai and Diary did not differ, %Sedentary differed at .001 level of significance (Mean (SD) for Sookjai and Diary = 78.21 (9.51) and 67.50 (9.96) with t%Sedentary = 3.89, p =.000). Likewise, the %Inactive for Sookjai was 90.75 (4.90) and Diary 72.60 (9.86) with t%Inactive = 8.24, p =.000.
Because only the Sookjai group can track the T&T of participants, the Means (SD) of T&T during daytime nap and nocturnal sleep are 35.15 (21.33) and 32.69 (16.73). It appears that elders in the present study had an average of more than 30 T&T times during both day and night. However, the spread between minimum and maximum numbers of T&T was vast, 9.33–77.60 for daytime and 8.85–70.36 for nighttime. Also, the per hour of T&T during nap was about four times greater than sleep (11.98 vs 3.29). The min-max hours were 2.68–31.01 and 0.88–7.69, respectively. There was no statistical difference in the health data provided by seniors in Sookjai and Diary groups. However, more participants in the study had experienced falls in the past 2 years. The two groups saw themselves having a minor hearing, seeing, eating, and sleeping problem (PHSES). They scored moderately well on their health in the past 6 months (Health 6 m). Their average scores of depression (Depress9Q) were low.
ANOVA of sedentary behavior and T&T by age groups.
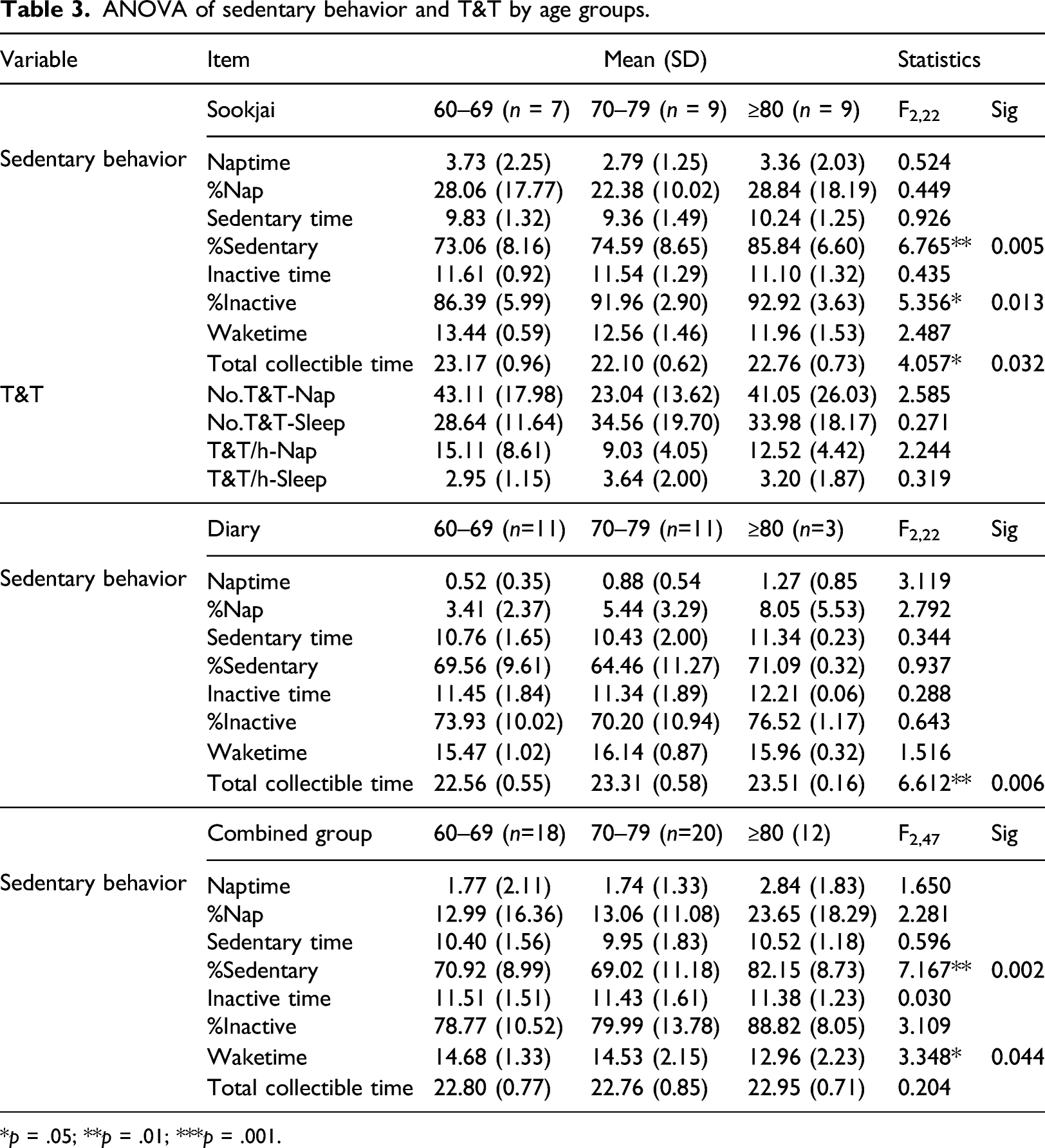
*p = .05; **p = .01; ***p = .001.
Hypothesis testing
Sedentary behavior and sleep duration
Effect of sedentary behavior on sleep duration.
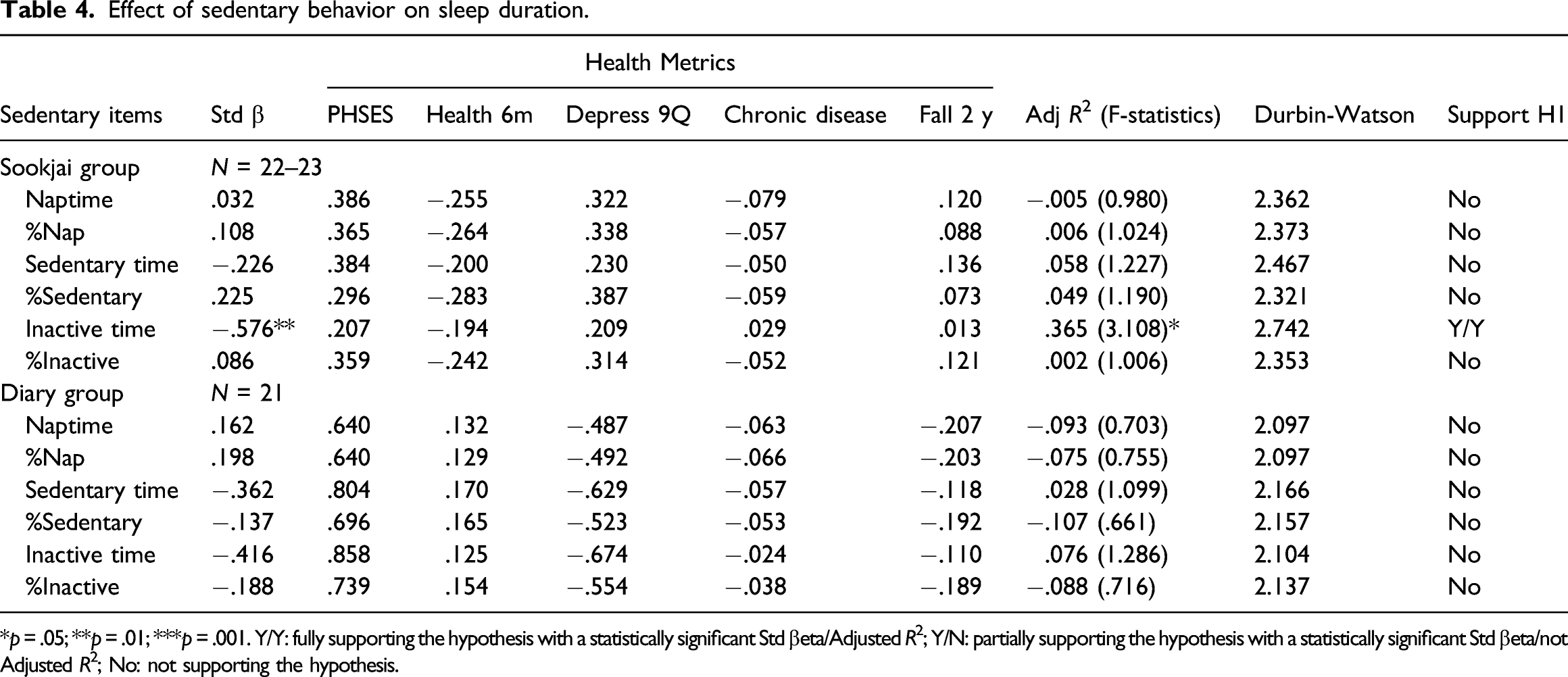
*p = .05; **p = .01; ***p = .001. Y/Y: fully supporting the hypothesis with a statistically significant Std βeta/Adjusted R2; Y/N: partially supporting the hypothesis with a statistically significant Std βeta/not Adjusted R2; No: not supporting the hypothesis.
Sedentary behavior and nighttime T&T
Controlling the health data, %Sedentary was the only sedentary behaviors explaining the number of T&Ts at night (F = 2.878, p = .043), accounting for 33.9% with the Std β coefficient 0.631, p = .005 (Table 5). This result supported H2, the effect of sedentary behaviors on nocturnal T&Ts; specifically, the higher the percentage of sedentary time, the higher is number of tosses and turns at night. Although the Std β coefficient of Sedentary time was statistically significant (0.473, p = .032), the regression equation accounting for 18.4% was not (F = 1.827, p > .05), indicating a positive relationship between sedentary behaviors and nighttime sleep interruption. Similar results were found between the number of T&T per hour and sedentary time and %Sedentary, the Std β coefficients were .510 and .580, p < .05, but the regression results were not significant.
Effect of sedentary behavior on nighttime T&T.
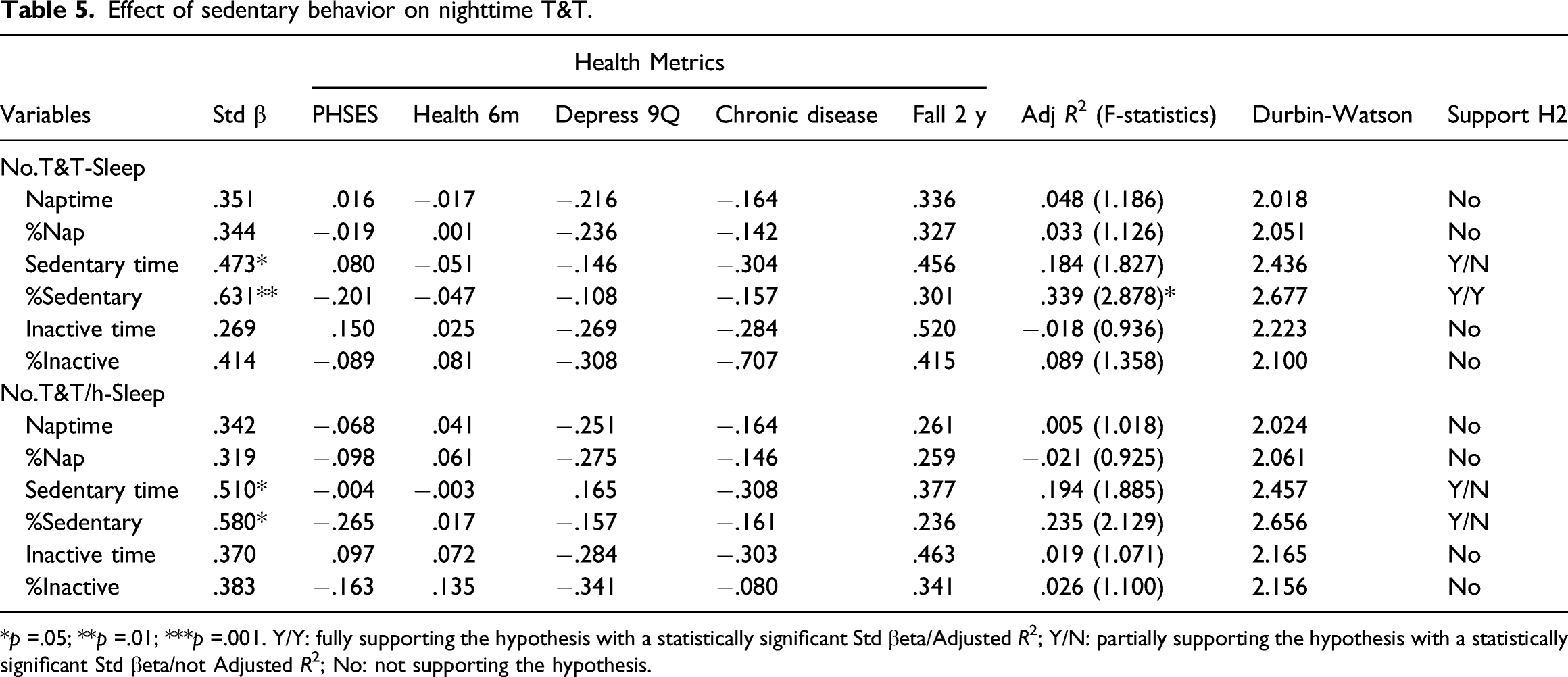
*p =.05; **p =.01; ***p =.001. Y/Y: fully supporting the hypothesis with a statistically significant Std βeta/Adjusted R2; Y/N: partially supporting the hypothesis with a statistically significant Std βeta/not Adjusted R2; No: not supporting the hypothesis.
Nighttime T&T and sleep duration
Effect of nighttime T&T on sleep duration.
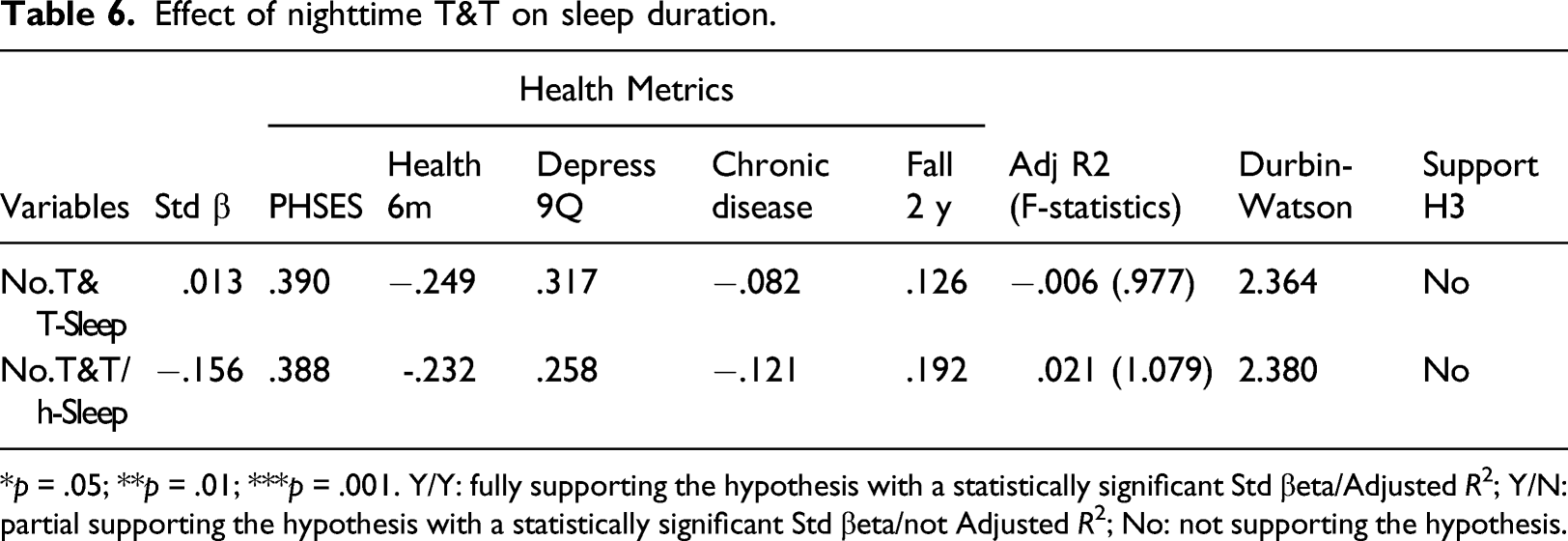
*p = .05; **p = .01; ***p = .001. Y/Y: fully supporting the hypothesis with a statistically significant Std βeta/Adjusted R2; Y/N: partial supporting the hypothesis with a statistically significant Std βeta/not Adjusted R2; No: not supporting the hypothesis.
Based on previous literature, sedentary behavior was separated from T&T in determining sleep duration. As shown in Table 4, the sedentary behavior that affected sleep duration the most, the Inactive time, was included in the multiple regression, along with the No.T&T-Sleep and the health metrics as control variables. The regression model (Durbin-Watson = 2.687) shown in the equation below was statistically significant (F-statistic = 2.765, p = .047); both independent variables explained 36.0% (Adjusted R2) of Sleep Duration. The Std β of Inactive time was significant at .05 level (−.626, t=−3.185, p = .006); No.T&T-Sleep was not significant (.184, t=.930, p = .367). None of the Std β of any health measure was statistically significant at .05 level. Thus, sleep duration associated negatively with sedentary behavior. Long sleepers had less sedentary time; sleep bouts did not affect sleep time.
Sleep time = –.626 Inactive time +.184 No.T&T-Sleep + .179 PHSES – .199 Health 6m + .259 Depress 9Q +.081 Chronic Disease –.083 Fall 2y
Result verification and participant’s feedback
The sleep hours from the short open-ended, self-reported verification questions were summarized and found to be consistent with the automatic and manual diary data. According to the questionnaire, the Sookjai group slept more than the Diary group: 7.72 h/day compared to 6.35 h/day. However, device and diary data showed longer hours of sleep than the open-ended verification questions. The discrepancy might come from the elderly’s estimation of their habitual sleep routine (i.e., go to bed at 10.00 p.m., get up at 5.00 a.m.). The open-ended data, combining those of both groups, show that one-third of the elderly reported that they cook often, do not play sports, and regularly do exercises, such as walking, Tai chi, yoga, and cycling. Moreover, these seniors’ relaxation activities include watching television, listening to music, napping, reading books, and using social media. Finally, approximately 75% indicated no difference between their weekday and weekend activities.
Seven device users and six diary recorders were in the focused groups. The discussion centered on the experiences that the seniors had had during the 2 weeks of data collection, the problems and obstacles they encountered from using the device, suggestions on the appearance of the device, factors that would encourage them to use the device, and services that they might want from the device platform.
The device users indicated that they were stressed because they were conscious about wearing the device. Notwithstanding the fact that the pendant was big and robust, the elders had an impression that they had to be careful
Some participants preferred a device that is not noticeable while wearing it. They also indicated that they did not want to be stressed by the faulty sensors (S10/fs6), that a brooch might be better
To motivate the independent living elderly further, the price of the device matters: renting is perhaps better than buying because one would get services from the platform owner
Furthermore, they preferred personal tracking services to remind them of the distance they are away from home or provide directions to prevent getting lost. In other words, they would like a service that automatically signals caregivers or condominium staff to come and rescue them when they lose their way (
Both the device users and diary recorders would like games to reduce the possibility of getting Alzheimer’s disease
The award-winning activity tracking device, Sookjai, is a relatively large pendant made from lightweight materials and straps with two clipped magnets for easy attachment and removal. However, when being used daily, the attachment falls off, and the long leash sways while walking. The strap’s rubbery nature causes the pendant to send standing signals online unintentionally because it is vertical. Sookjai, thus, does not present an altogether pleasant experience to the elderly because it was set up to be oversensitive in fall detection. The false positive for fall detection is intentional, and the device did detect actual fall incidents during the data collection period.
Pairing a wearable with a mobile phone becomes a de-facto standard of the health-related devices industry. The activity tracking device used in the present study also has a mobile application to display the real-time signals using easy-to-understand visualizations. The ability to see one’s movement instantaneously has its pros and cons. The advantages were that seniors were eager to use the devices, cooperate with the research, and feel confident about possible fall detection. However, the problem is that the device’s wearers were worried and kept comparing the instantaneous posture with what they saw on the mobile screen; if they were not the same, they felt agitated. For example, if the screen shows that they are sleeping while sitting, they question the device’s accuracy. The constant checking of each motion activity was stressful for them. Moreover, as the wearing of the device lasted only 2 weeks, some elders appeared to feel the effect of participating in the study and might not have acted naturally; they knew and were informed of being tracked by the device automatically. Thus, the Hawthorne effect might have come into play.
Discussion
The integration of behavioral and biophysical characteristics of older adults is in different research disciplines. In sports science and related PA research, the focus is on exercises, physical fitness, and health for all walks of life. In this line of research, sedentary behavior and lifestyle are linked to older adults’ physical and emotional health. Similar research inquiries are examined in healthcare and health promotion disciplines with increasing health-related issues and specific disease populations. Nevertheless, the operational definition and measurement of what is considered to be sedentary behavior and its associated postures still need more empirical evidence to narrow down the aging community research result disparities.
In this study, we used the recommended standard definition of PA and PA intensity to differentiate between the extent of different sedentary behaviors, by using activity time, to examine the effects on sleep duration of independently living seniors.10,14,72 For the sedentary time that includes naps, sit/stand, and slow-walk, we found that Thai older adults had 72.85% sedentary behavior, which is lower than 75% in the Islandic elders but higher than 66% in Norwegian and 60.2% in Swedish elders. However, when counting all ≤1.5 MET activities as Inactive time, 82% sedentary behavior from Thai older adults is closer to the 80% sedentary behavior referred by different studies.11,29,30
Although the seniors in both Sookjai and Diary groups were demographically similar, the device-measured and self-reported data might not measure the same activity precisely. The differences might also come from the present research design that did not have the same individual as both the device-wearer and diary-reporter. Similar to previous studies, self-report diary participants in the present study estimated the low-intensity PA more than accelerometry.11,60 However, the composition of postures regarding sedentary differed; the device wearers had less sit/stand posture and more reclining (nap) than the diary recorders and vice versa. If future research would use the same subject to wear the device and write the diary in parallel, the researcher must carefully design the data collection procedure to ensure that reliable data can be collected without an inadvertent replication of manual from the auto-collected data.
Although the general profile of device wearers and diary-reporters are similar, they showed different sedentary behaviors. The relationship between sleep and unhealthy aging was inconclusive. Similar to Ortola et al. (2021), the long-sleepers (Sookjai) had less sedentary behavior because the correlations were negative. 60 The opposite was not true for the short sleepers. The shorter sleepers (Diary) also had negative associations between sedentary and sleep time, though not statistically significant. The beta coefficients of all health metrics were not statistically significant in any regression models. One possible explanation is that the elders are well-taken care of by the Red Cross-affiliated health professionals. The physicians, physical therapists, dentists, and public health officers from renowned hospitals would regularly do routine checkups and offer the latest knowledge and self-care tips. They perceived their health to be good regardless of how they behaved sedentarily.
Our findings agree with previous research in sleep quality. Both the T&T during daytime naps and nocturnal sleep relate to the sleep time of the elderly.44,47 We found elders who had more nap hours to have more T&T during daytime naps and nocturnal sleep. While researchers still debate the benefit of napping on health, they seem to agree more on the negative effect of T&T on health.38,73 Similar to the hypothesis testing between sedentary behavior and health, we did not find any significant relationship between T&Ts and seniors' health in our study. The same possible reason discussed early applies here. A large number of seniors in the nursing home are single females who were self-sufficient all their life. Thus, being healthy is one of their utmost priorities.
Although the wearable in this research had passed the interface design test by local people, the device configuration on the signal transmission can be quite challenging. Seniors were sensitive to the device’s stability and the signal processing algorithm directly linked to the mobile application. The current study points out the problems with the prototype device used in this study. The algorithm developer had set the Sookjai wearable to shake and make noises every time a possible fall was detected; this playing-it-save principle was disturbing to some people. However, during the study period, the device did send correct fall signals to the research associate’s tablet. The on-site helper contacted the elder right away and was informed of falls. Thus, the prototype wearable does live up to its reputation of being an excellent fall detection device.
The participants were also susceptible to the mismatch between the mobile display and the instant motion. This finding shows a similar result to a study on fitness band accuracy. 74 The prototype device did not detect the movement of older people accurately. Independently living seniors are perhaps more sensitive than others; they are aware of the need to be self-sufficient all the time. Thus, a potential topic for future research is developing a personalized false-positive algorithm that caters to individual people. The signal processing with this type of algorithm would gain more acceptance than a one-size-fits-all algorithm. The combination of data science and user experience research that accounts for individual differences will promote continued engagement and long-term benefits. 75
As suggested by Bourbonnais et al., studies on the need for technologies in a nursing home setting are relatively scarce. A few studies emphasized the administration and leadership of nursing homes’ technological implementation.76,77 In contrast, the present study focused on the nursing home’s residents. The findings of this study support previous literature findings stating that demographic and health data influence seniors’ self-care behaviors. Those anxious about self-care activities are likely to be more educated.78,79 Health-conscious people tend to seek information from the Internet and adopt health-related technology.79,80
Designers of wearable devices are often technologically driven. However, an efficient and useful device requires collaboration between designers and users.64,81 For example, home-use medical devices and activity tracking wearables can have both a positive and a negative psychosocial impact on the users. 82 It should be noted that although the device tracks motion in real-time, a hypothetical bias may occur because the participants might do things differently from what they would do daily during the study. 83
Conclusion
Similar to previous research, this study found that the device wearers want to evaluate their ability to live independently 84 ; aging-in-place seniors want to live in their own home, even if it means living alone. They want to be independent for as long as possible and are interested in using the device for fall prevention. The activity data tracked by the device can be readily available to caretakers and healthcare professionals to monitor health-related habits and suggest preventive medicines or personalized health improvement programs.85,86 The automatic signals and other vital signs are input to developing a personalized, predictive model of older adults' activity patterns that the local government can use to deploy an effective health promotion policy. Besides, by creating awareness about the actual time spent in certain activities, the older adults would perhaps change behaviors to ascertain their healthy aging. 87 For public health policymakers, accurate measures of older people’s daily physical activity patterns are essential for an effective intervention program to save healthcare costs.
The sedentary behavior and long sleep time in bed, accompanied by long daytime naps, were associated with more tossing and turning at night by the nursing home participants in this study. However, a lack of relationship between perceived health and sedentary behavior and in-sleep activity warrants further investigation. A possible explanation could be the unique setting of the study site, an exceptional group of individuals, or the imperceptive measurements that influence the seniors to rate their health highly. The future inquiries might investigate whether the residents are self-selected to this nursing home, compare elders living at home with those in the nursing home, determine factors affecting their health perception, and use alternative objective measures for health data.
The present study has limitations due to a short intervention study duration from a single site and an imperfect tracking device. Since in-sleep activities can only be collected from the device wearers (half of the research participants), this small sample size might affect the lack of relationship found between toss-and-turns and sleep duration. The limitation includes using 24 h in calculating sedentary behaviors and sleep duration measurements. A larger number of participants and a longer data collection period could help to achieve more accurate statistical results.
Although the study used the older adults from an Asian country, no comparison has been made regarding monitoring activities with the independently living seniors from any western country. A possible underestimate or overestimation of posture times found in this study may exist, and further investigations of seniors’ behaviors from eastern and western regions would be useful for contributing to the literature in this field. 72 Future research should overcome these limitations to attain better data to develop a more accurate activity model that can cater to each senior’s individual needs, thus eventually yielding personalized health promotions schemes and a better quality of life.
Supplemental Material
sj-pptx-1-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-pptx-1-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-pdf-2-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-pdf-2-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-jpg-3-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-jpg-3-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-jpg-4-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-jpg-4-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-jpg-5-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-jpg-5-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-jpg-6-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-jpg-6-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-jpg-7-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-jpg-7-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Supplemental Material
sj-jpg-8-jhi-10.1177_14604582211070214 – Supplemental Material for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors
Supplemental Material, sj-jpg-8-jhi-10.1177_14604582211070214 for Use of daily posture and activity tracking to assess sedentary behavior, toss-and-turns, and sleep duration of independently living Thai seniors by Uthai Tanlamai, Aim-Orn Jaikengkit, Trirat Jarutach, Surasvadee Rajkulchai, and Thanachart Ritbumroong in Health Informatics Journal
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research: This research is part of the research project, “An Analytical Study of Activity Patterns for Healthcare Promotion and Monitoring of Thai Elderly,” supported by the research grant #RGU6280011 from Thailand Science Research and Innovation (TSRI).
Ethical approval
All participants were informed about the study objective and signed consent forms. Project number 154.2/62 received ethical approval (CAO No. 103/2563) by the Research Ethics Review Committee for Research Involving Human Research Participants, Group 1, Chulalongkorn University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.