
Abstract
The prevalence of MCD (multiple chronic disease) is increasing due to increased life expectancies and aging populations. Individual and socioeconomic burdens of MCD are also increasing. To reduce these burdens, it is necessary to establish policies to prevent MCD; therefore, it is important to understand the characteristics of MCD in the current population. In this study, the combinations of MCD that affect hypertension, which has the highest prevalence, were examined according to different age groups. The combinations of diseases were identified utilizing association rules analysis, using the Community Health Survey as the raw data. Two association rules were determined in young adult group, 18 in the middle-aged group, and 30 in the senior group, showing that the number of rules increases with age. Association rules of this study mean that combined chronic diseases are highly associated with hypertension. Then logistic regression analysis was performed on the MCD combinations with highest lift value in each age group to identify relationships between health behavior and MCD combinations. Especially, alcohol consumption was found to be a common factor affecting MCD prevalence in three combinations. On the contrary, sleep habit did not have a statistically significant influence on any combination.
Keywords
Introduction
As of 2017, the prevalence of hypertension in Koreans 30 years of age is 31.2% and is higher in males (35.0%) than in females (27.6%), also the prevalence increases with age. 1 Furthermore, the cost of hypertensive treatment has increased by an average of approximately 4% per year from KRW 769.3 billion in 2012 to KRW 901 billion in 2016. 2 Globally, 40% of the adult population over the age of 25 is hypertensive as of 2008, and 9 million people die each year from complications of hypertension. 3 Hypertension is the most common and influential risk factor of cardiovascular disease, and the World Health Organization defines hypertension as a major threat for coronary artery disease and ischemic and hemorrhagic cerebrovascular diseases. 4
The National Health Insurance Review and Assessment Institute (HIRA) and the National Health Insurance Service survey 12 diseases including hypertension, diabetes, arthritis, and heart disease every year, showing a continuous increase in the number of patients and medical expenses. The number of patients was 18,891,000 as of 2019, an annual increase of 4% from 2015 and medical expenses increased by 10.3% per year over the same period. 5
Overall, the population is aging and the incidence of chronic disease is increasing6,7; however, there is an increasing incidence of multimorbidity, in which a single patient has multiple chronic diseases. 8 The term “multiple chronic disease” (MCD) describes a patient who has two or more chronic conditions simultaneously, regardless of the type of disease 9 ; however, MCD is distinct from comorbidity. 10 The prevalence of MCD increases sharply from age of 40 to 70, and a plot of MCD prevalence exhibits an S-shaped curve that reaches a plateau. 11 The tendency of MCD prevalence to increase with age means that older individuals have an increased burden of disease. 12 South Korea is seeing a rapid shift to an aging population. By 2025, South Korea is predicted to have an ultra-aging society; by 2065, 42.5% of the total population will be over 65. 13 Most elderly individuals in South Korea have chronic diseases; the average number of chronic diseases per patient is 4.1, and 70.9% of the elderly have MCD. 14 The Organization of Economic Co-operation and Development proposed that addressing MCD is a task that OCED countries will face in the coming decades. 15 This means that the significance of managing and preventing MCD is growing.
In recent years, the incidence of chronic diseases has increased significantly; chronic diseases now account for six of the top 10 causes of death in South Korea. 16 Consequently, chronic disease management has become a national issue. Therefore, the government continues to operate various pilot projects for preventing and managing chronic diseases based on the ‘Act on the Prevention and Management of Cardiovascular Diseases’. Since 2007, the government has implemented projects to manage chronic diseases, and recently, it has been pushing for a ‘Primary medical chronic disease management integrated pilot project’ by integrating the advantages of existing projects. 17 Also the government is conducting national surveys such as the National Health and Nutrition Survey and the Community Health Survey to identify the current status of chronic diseases. Although analyses of the current state and related factors of chronic diseases using data from these questionnaires are actively being conducted, our current understanding about MCD is incomplete.
Studies on MCD are increasing in response to these developments. In short, the number of domestic and foreign related studies under the keyword “multimorbidity” in “ScienceON” of Korea Institute of Science and Technology Information increased from 54 in 2010 to 412 in 2020. 18 Although previous studies focused on the number of chronic diseases in MCD patients, recent studies are focusing on combinations of MCD. 19 MCD can be manifested as a combination of various chronic diseases. In previous studies that identified combinations of MCD by comparisons between countries or systematic literature reviews, combinations involving cardiovascular diseases and metabolic diseases were the most frequent.19,20 One combination of diseases in MCD patients that has been reported in multiple studied consists of hypertension, diabetes, and hyperlipidemia.12,21,22 This high frequency combination of MCD means that patients with certain chronic diseases are more likely to suffer from other chronic diseases included in the combination. Identifying these probabilities can be used to predict and prevent other chronic diseases that will occur additionally in chronic patients.
Therefore, the combinations of MCD that influence hypertension, which has the highest prevalence among chronic diseases and is the disease that is most frequently included in MCD, are analyzed by age groups in this study. The intent of this study is to provide data to facilitate the management and prevention of MCD. Therefore, MCD cases were organized by association rules analysis. To verify the validity of the association rules, sensitivity and specificity values were used. In addition, the influence of health-related behavior factors on the MCD combinations were identified by logistic regression analysis.
Research method
Research subjects
The primary data analyzed in this study are sourced from the Community Health Survey conducted by the Korea Disease Control and Prevention Agency (KDCA) from 16 August 2016 to 31 October 2016. The survey was conducted as an electronic one-to-one questionnaire household survey, and adults aged 19 and over who were living in the sampled households at the time of the survey were selected as subjects. 23 The raw data consisted of 228,452 survey responses. In this study, data with missing values were excluded, and the final raw data consisted of 226,709 survey responses.
Operational definition of variables
Individual variation
In this study, gender, age, occupation, and education level were used as personal characteristics variables. Gender was categorized as male or female. Age was classified into a young adult group (19–44 years old), middle-aged group (45–64 years old), and senior group (≥65 years old). This grouping is the same as that used previously. 24 To classify middle-aged and senior groups, the standard of 45 years of age is used based on standards from the Longitudinal Study of Aging, and the standard of 65 years old is taken from the Elderly Welfare Act. Moreover, occupation responses were re-classified into four groups based on 10 classifications listed in the Korean Standard Occupational Classification. Managers, experts and related workers, and office workers were classified as “office workers”; service workers and sales workers were classified as “service and sales workers”; agricultural and forestry and fishery workers, skilled and related functions workers, equipment and machinery operation and assembly workers, and simple laborers were classified as “production and technical workers”; soldiers were classified as “soldiers.” Furthermore, a total of seven occupation groups were defined by adding housewife, student/re-trainee, and unemployment; these categories are available as responses in the Community Health Survey. Education level was classified into uneducated, elementary school, middle school, high school, 2-year/3-year university, 4-year university, and graduate school, according to the responses available in the Community Health Survey.
Multiple chronic disease
The incidences of chronic diseases vary by country and study. In this study, the chronic diseases included in the 2016 Community Health Survey were used. In the survey, the status of the following chronic diseases was assessed: hypertension, diabetes, dyslipidemia, arthritis, stroke, myocardial infarction, and angina pectoris (heart disease). 23 In this study, the prevalence of a chronic disease was defined when a respondent had been diagnosed with two or more diseases.
Health-related behaviors
The health habits referred to as ‘‘Alameda 7” in numerous studies was chosen to investigate health behaviors in this study. Alameda 7 refers to seven health habits identified by large-scale epidemiological surveys conducted in Alameda County, California, USA in the mid-1960’s. The study listed seven health behaviors that were related to health status: smoking, alcohol consumption, weight control, physical activity, breakfast intake, snack intake, and sleep. These factors exhibit good correlation with disease occurrence and mortality. 25
Among the Alameda 7 categories, five categories (smoking, alcohol consumption, physical activity, breakfast intake, and sleep) are divided into two categories: healthy lifestyle and unhealthy lifestyles. Then classified according to the unhealthy lifestyles. In particular, smoking was classified into current smoking and current non-smoking. 26 Heavy drinking was classified according to the high-risk drinking standard suggested by the Korean Statistical Information Service (KOSIS). The high-risk alcohol consumption was defined as at least two drink events including seven or more standard drinks per event weekly in males and at least two drink events including five or more standard drinks per event weekly in females. 27 Physical activities were into physically active and inactive lifestyles as suggested by the KOSIS. Individuals are classified as having a physically active lifestyle if they engage in vigorous physical activity for more than 20 min a day for at least 3 days a week or moderate physical activity for more than 30 min a day for at least 5 days during the past week. 28 Breakfast intake was categorized according to the definition of skipping breakfasts provided by the KOSIS: having not eaten breakfast for more than 5 days in the last week. 29 Sleep was categorized into two groups, depending on whether the individual averaged 7–8 h per night. 30
Analysis method
Because the data from previous studies suggest that the morbidity of MCD increases with age, 31 the group was divided into young adult, middle-aged and senior groups. After the data processing, association rules and statistical analyses were performed using R (ver. 1.0.143), SPSS (ver. 25.0), and SAS (ver. 9.4). The raw data of the Community Health Survey were analyzed using stratification variables, cluster variables, and weight variables as composite sample data in the statistical analysis.
In association rules analysis, the combinations of MCD were analyzed by selecting chronic diseases that influence the outcome variable, hypertension, as conditional variances (i.e., diabetes, dyslipidemia, arthritis, stroke, heart disease). If the lift value between two items is greater than 1, it means that the two items have a positive correlation with each other. 32 Therefore, a chronic disease having a lift value greater than 1 with hypertension was defined as a significant combination.
By statistical analysis, the validity of the association rules was verified by identifying the distribution of personal characteristic variables for each age group and calculating the sensitivity and specificity values for the derived association rules
Association rules analysis
Association analysis reveals rules regarding the possibility that the simultaneous occurrence of a set of variables affects a specific outcome. 33 Utilizing various evaluation scales, association analysis derives a set of items with strong rules, and the relationship between these items is expressed as X→Y. 34 There are three evaluation scales that explain the relationship between X and Y: support, confidence, and lift. In this study, to establish the direction of the related rules while conducting the analysis, the prevalence of hypertension was set as a result clause, and the prevalence of diabetes, dyslipidemia, arthritis, stroke, or heart disease was set as a conditional clause.
“Support” in this study is defined as the “probability of patients having hypertension with certain chronic diseases among all subjects.” “Confidence” means the “probability of having hypertension among patients with certain chronic diseases.” “Lift” is defined as the “confidence value divided by the probability of having hypertension.” Because the most significant association rules are those that show a significant relationship between hypertension and other chronic disease, lift is the most important evaluation scale value in this study.
Validation of the association rules
Sensitivity and specificity values were calculated for each significant association rule to verify the validity
Furthermore, sensitivity is a criterion of how well those with the disease are identified when using a specific diagnostic method. 35 In this study, sensitivity refers to the ratio of the association rules that identify those who simultaneously present with hypertension and a specific chronic disease. Specificity is a criterion of how well those without the disease are identified when using any diagnostic method. 35 In this study, specificity refers to the ratio of the association rule that identifies those who do not exhibit either hypertension nor another chronic disease. Specificity has the more meaningful value in this study because it contributes substantially to knowing the prevalence of a specific combination of MCD in the study population.
Logistic regression analysis
Logistic regression analysis was conducted on combinations of MCD with the highest degree of lift value in each age group to determine lifestyle affecting the prevalence of MCD. The presence of chronic disease was selected as a dependent variable, and the behaviors of smoking, alcohol consumption, physical activity, breakfast intake, and sleep were selected as independent variables. This study’s dependent variable, chronic disease prevalence, is a categorical variable that appears in two ways: yes and no. These binary variables follow a binomial distribution and can be used to analyze the relationship between independent and dependent variables. 36 In this study, the groups corresponding to “yes” in each independent variable were analyzed by setting them as references. For example, smoking is a reference for a group that smokes and breakfast intake is a reference for a group that does not eat breakfast.
Results
Participant characteristics
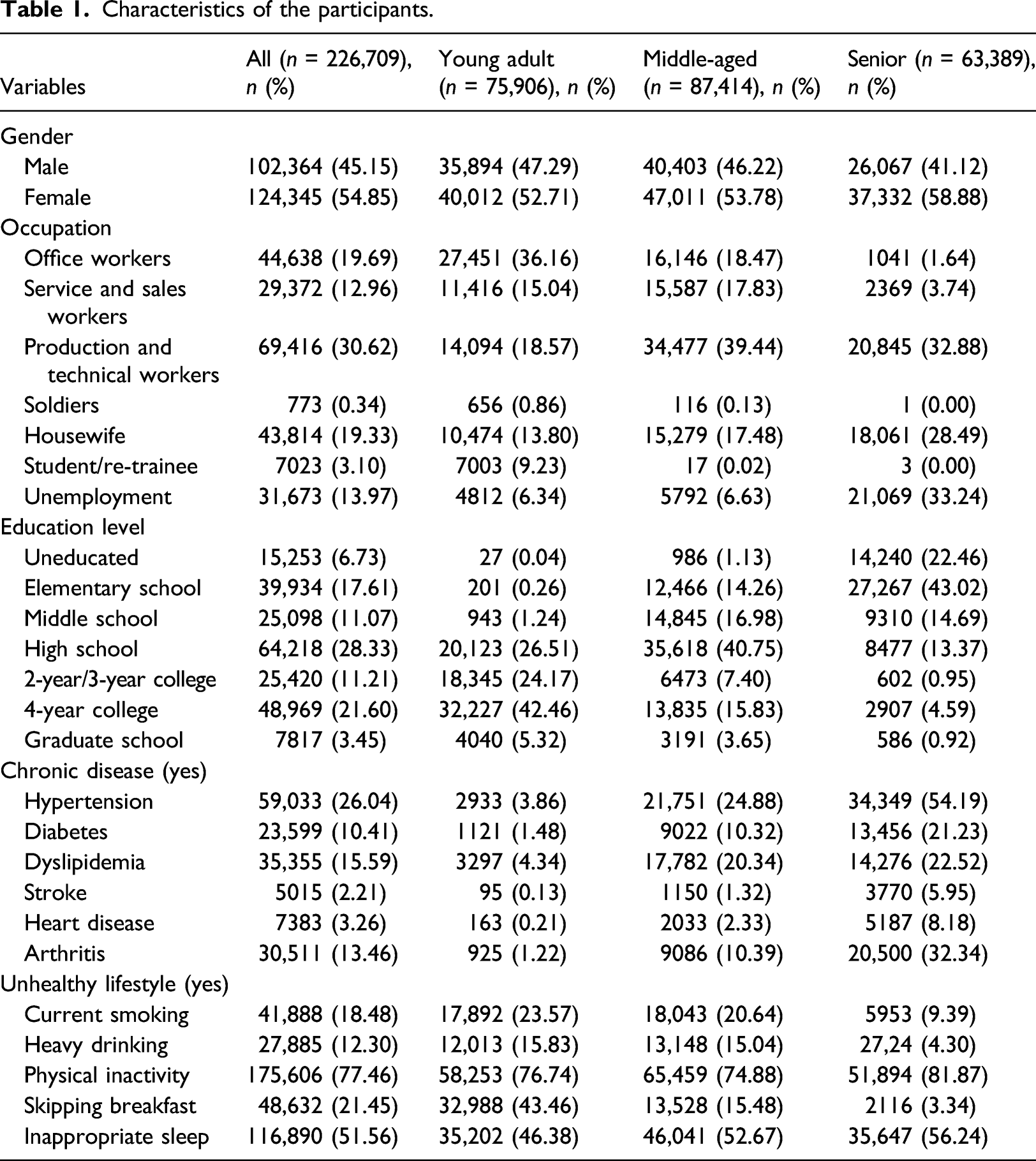
The average ages of the 75,906 (33.5%) young adults, 87,414 (38.6%) middle-aged people, and 63,389 (28%) seniors are 33, 54.4, and 74.2, respectively. There are more females than males in all age groups; occupation and education levels also differed among age groups. In the young adult group, the highest proportion (36.16%) are office workers, and production and technical workers are the highest proportion in the middle-aged (39.44%) and the senior (32.88%) groups. The highest proportion of education levels is 4-year college education level in the young adult group (42.46%), high school in the middle-aged group (40.75%), and elementary school in the senior group (43.02%).
Chronic disease prevalence increased significantly with age. Based on all participants, the prevalence of hypertension was highest at 26.04%, followed by dyslipidemia (15.59%), arthritis (13.46%), diabetes (10.41%), heart disease (3.26%), and stroke (2.21%).
Characteristics of the participants.
Association rules analysis and validation
Among patients with chronic diseases, MCD combinations satisfying a minimum confidence of 30%, and a lift value greater than 1 are identified as significant association rules in this study. In addition, considering the number of patients with chronic diseases in this study, we set the minimum support at 0.1% to the minimum level at which the association rules can be representative. All the identified association rules are verified as having a statistically confidence level of 95%. The validity of the association rules is then compared to obtain the sensitivity and specificity values for each combination of MCD.
Young adult group
Young adult group’s significant association rules.

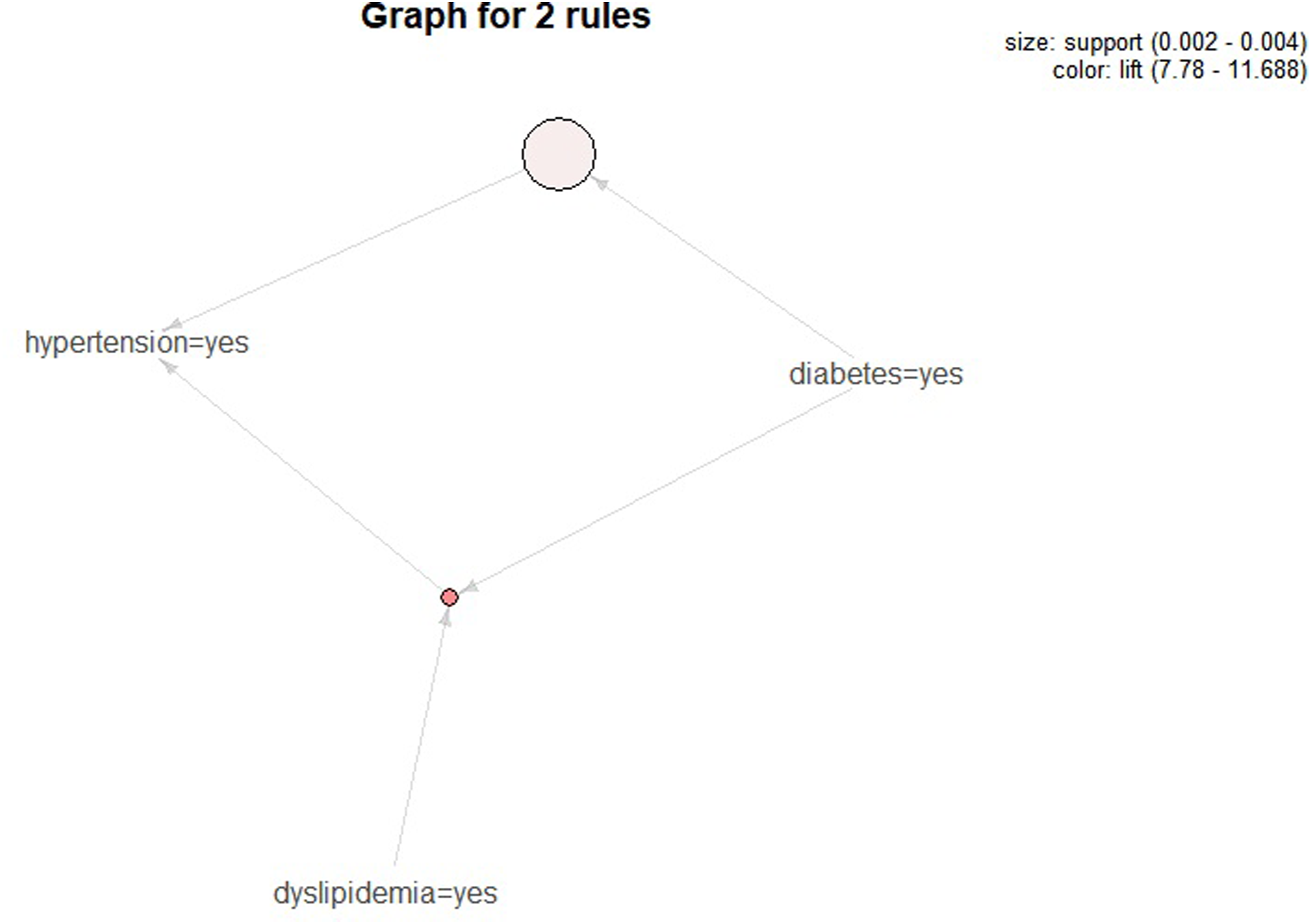
Young adult group’s multiple chronic disease combination graph.
Diabetes has the highest sensitivity (11.49%), and the highest specificity (99.74%) is seen with the diabetes-dyslipidemia combination. Using diabetes as an example, the description of its sensitivity and specificity in this study is as follows: The probability that the association rule determines that young adults with hypertension have diabetes is 11.49%, and 98.93% do not exhibit either the hypertension nor the chronic diseases (Table 2).
Middle-aged group
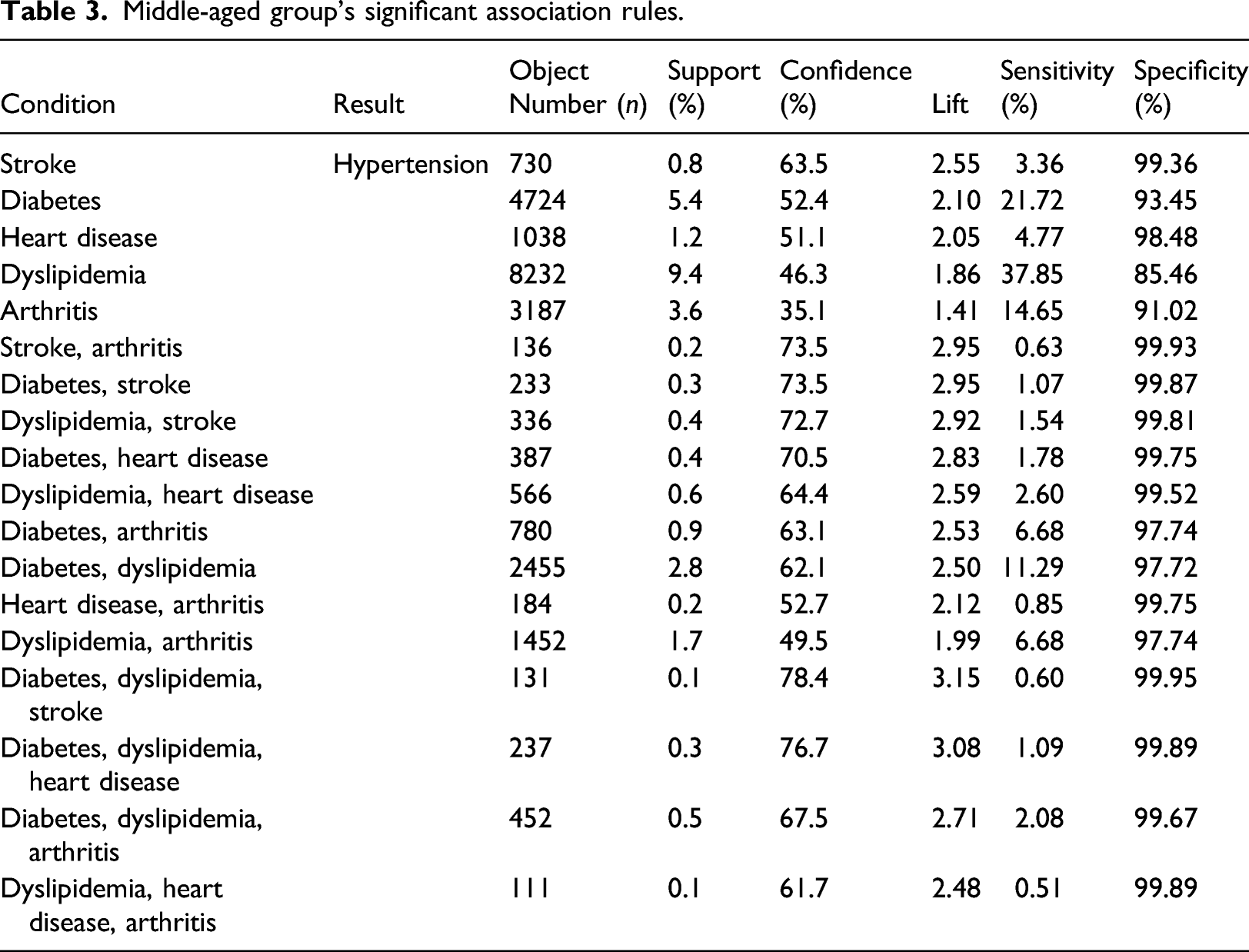
Middle-aged group’s significant association rules.
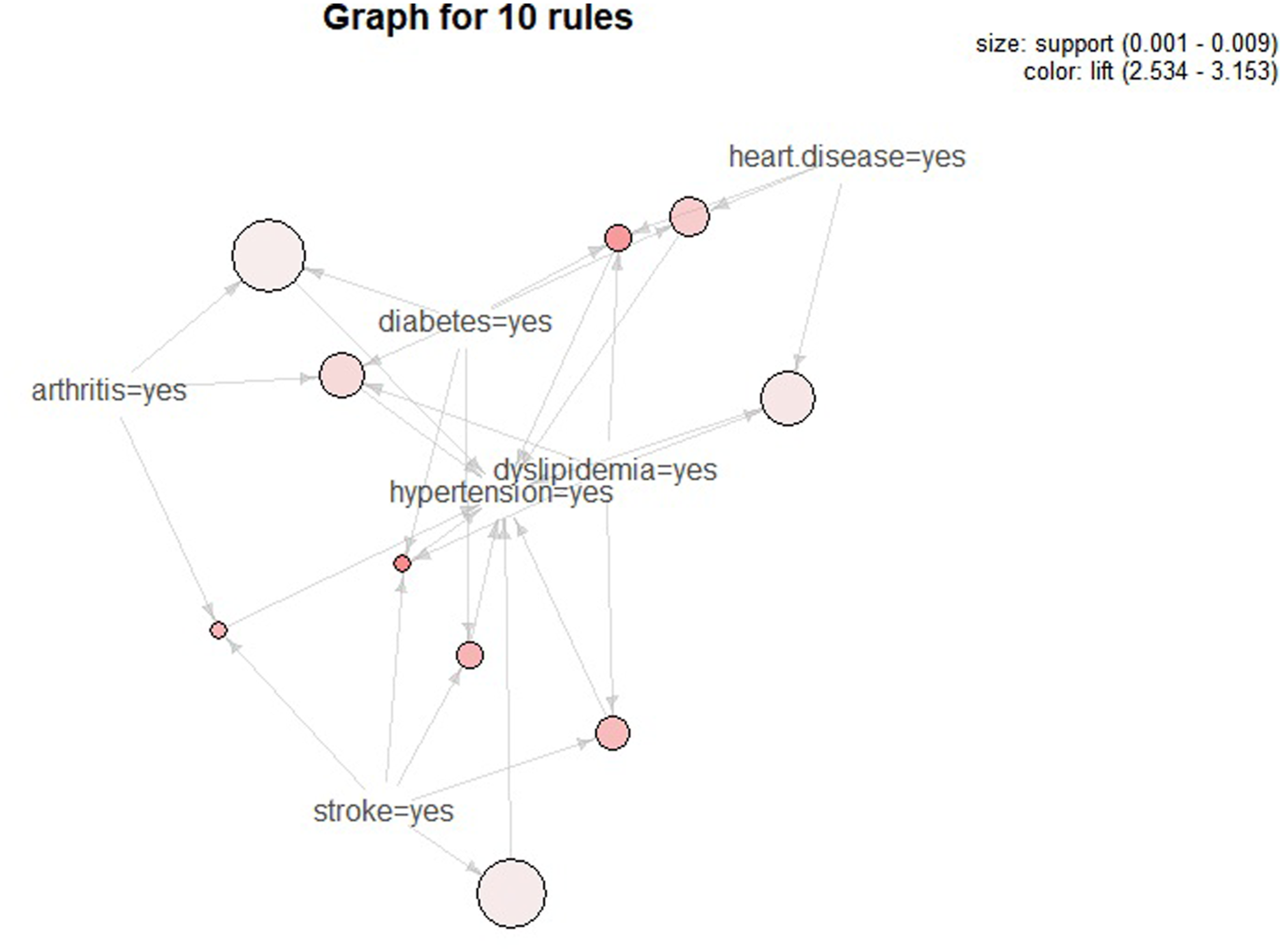
Middle-aged group’s top 10 multiple chronic disease combination graph.
Dyslipidemia exhibits the highest sensitivity (37.85%), and the diabetes-dyslipidemia-stroke combination had the highest specificity (99.95%). The sensitivities of diabetes (21.72%), arthritis (14.65%), and diabetes-dyslipidemia (11.29%) are 10% or higher; these values are significantly higher than the other combinations (Table 3).
Senior group
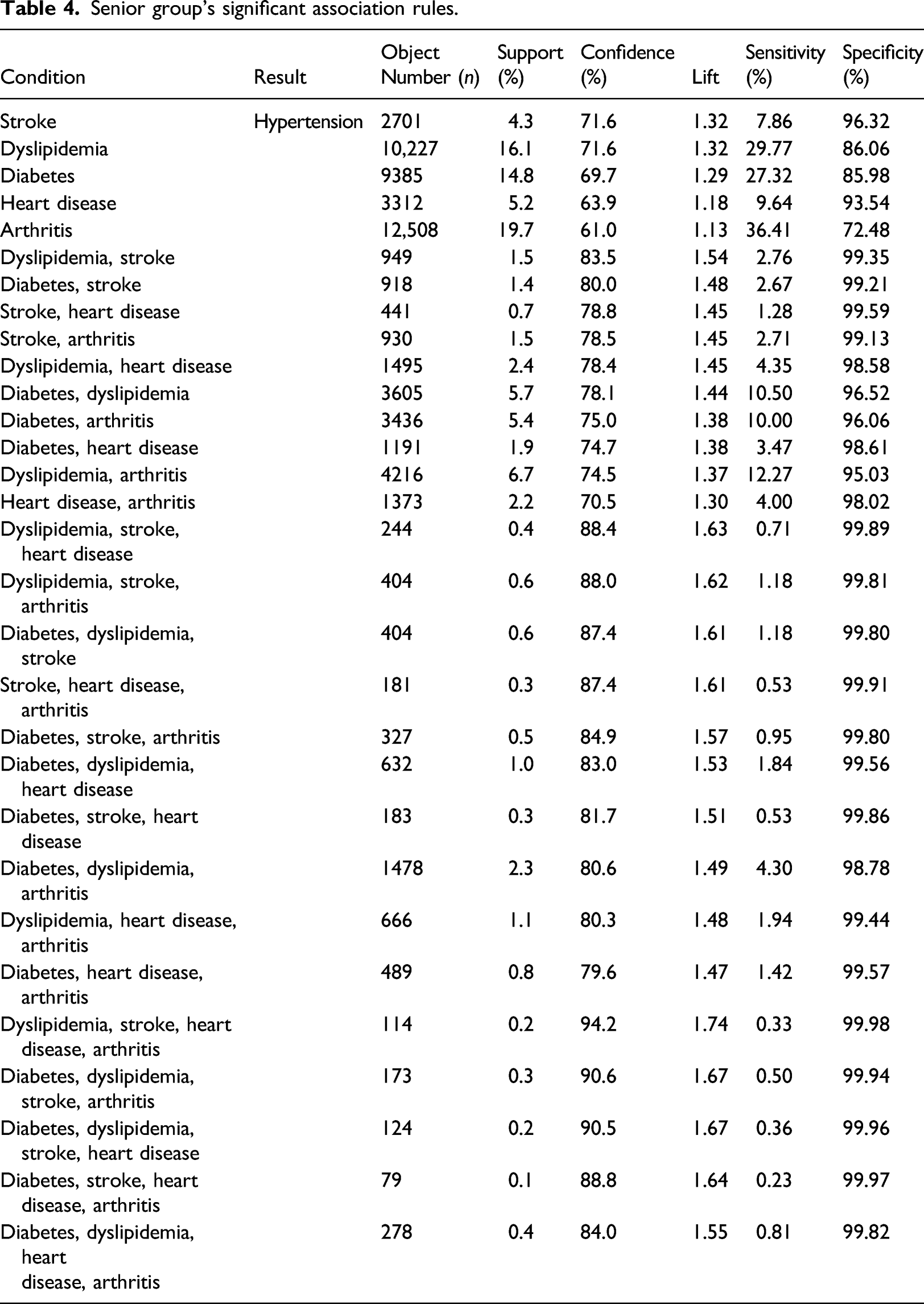
Senior group’s significant association rules.
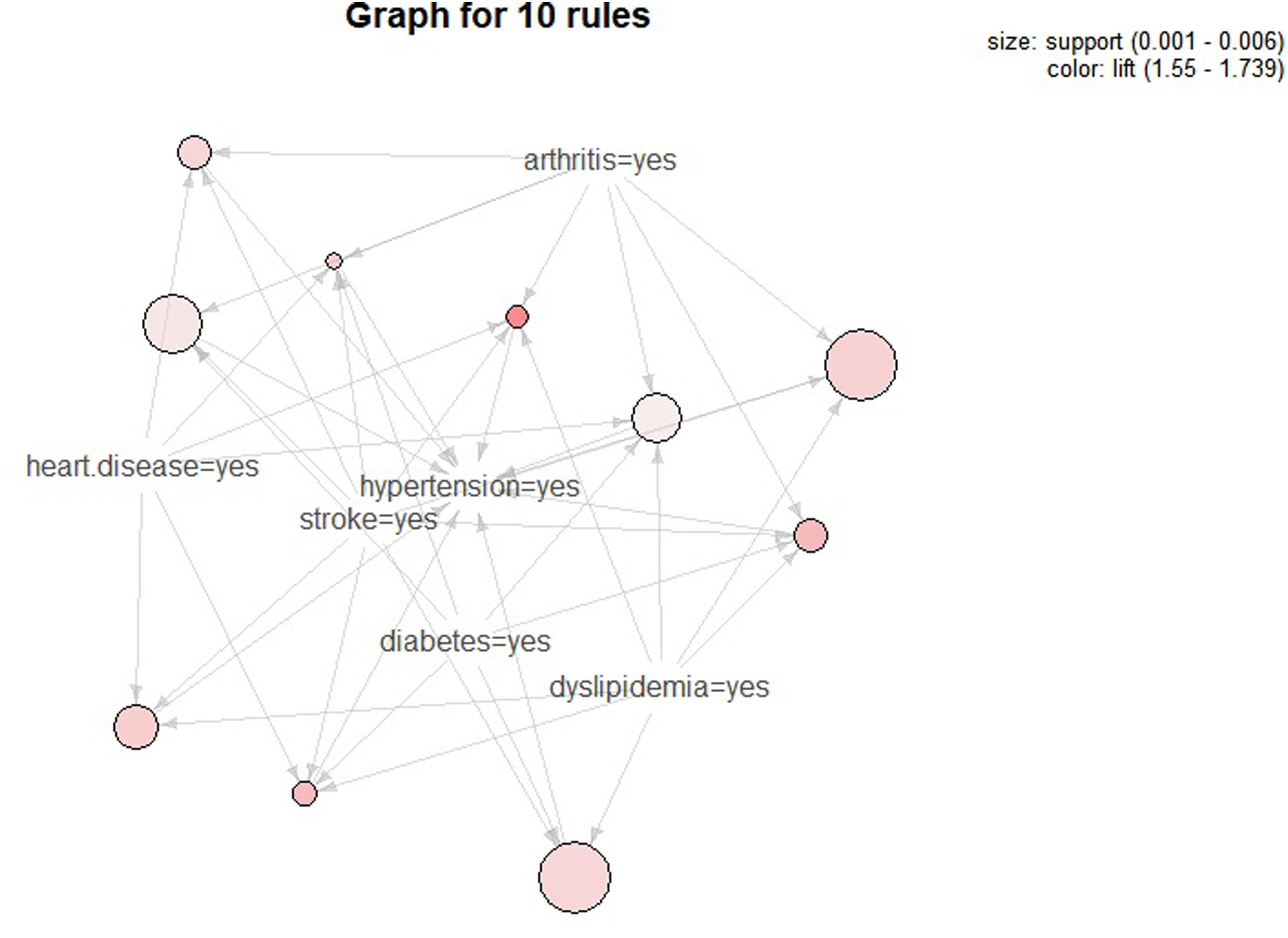
Senior group’s top 10 multiple chronic disease combination graph.
Arthritis exhibits the highest sensitivity (36.41%), and the combination of dyslipidemia–stroke–heart disease–arthritis has the highest specificity (99.98%). Other combinations having high sensitivities (≥10%) include dyslipidemia (29.77%), diabetes (27.32%), dyslipidemia–arthritis (12.27%), diabetes–dyslipidemia (10.50%), and diabetes–arthritis (10%) (Table 4).
Health behavior factors that affect multiple chronic disease combinations
Logistic regression analysis was performed to identify the influence of health behaviors on MCD combination, using the MCD combinations with the highest lift values in each age group. These combinations are diabetes–dyslipidemia in the young adult group, diabetes–dyslipidemia–stroke in the middle-aged group, and dyslipidemia-stroke-heart disease-arthritis in the senior group.
Logistic regression results of representative multiple chronic disease combinations.
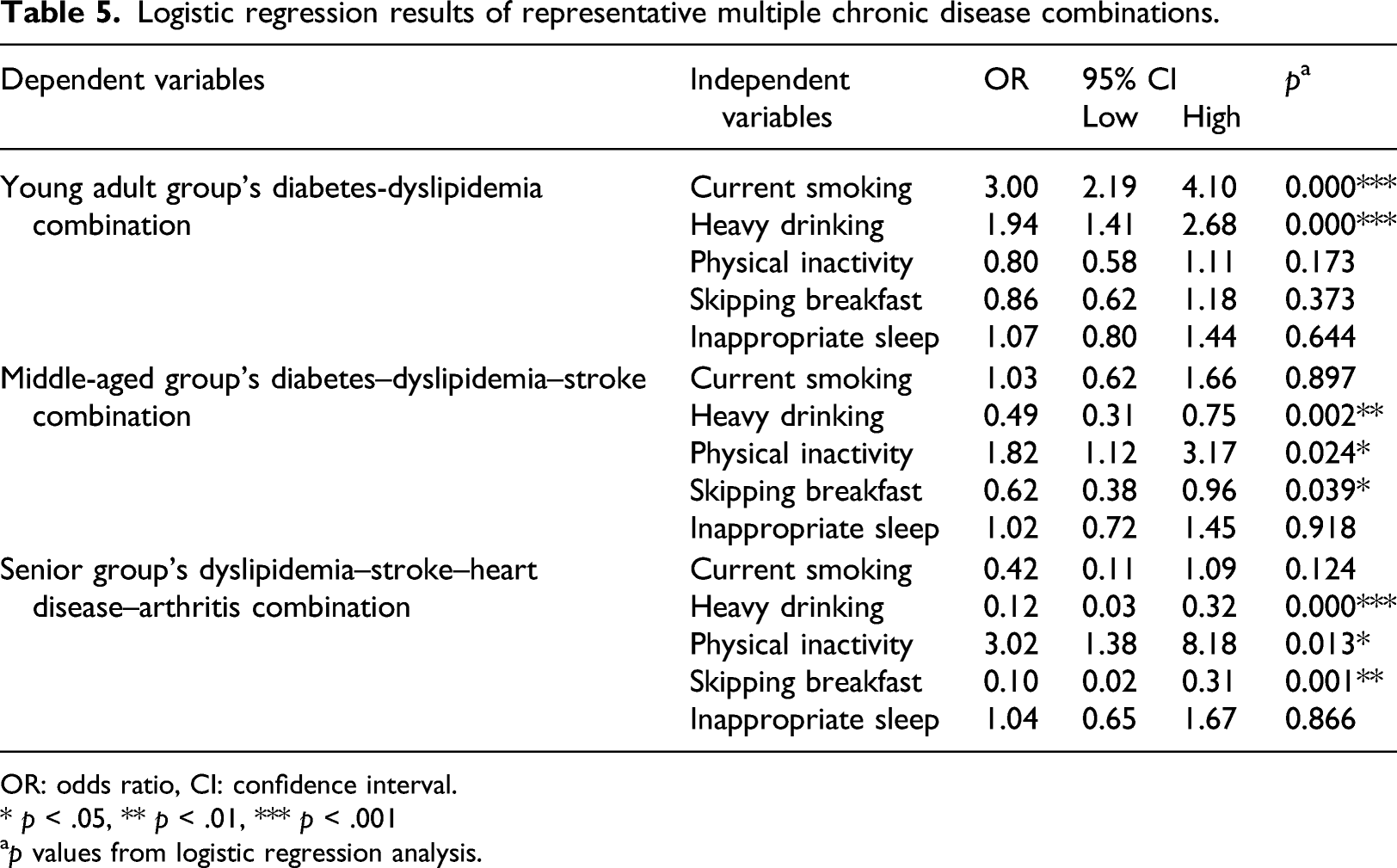
OR: odds ratio, CI: confidence interval.
* p < .05, ** p < .01, *** p < .001
ap values from logistic regression analysis.
For the diabetes-dyslipidemia-stroke combination in the middle-aged group, prevalence is 1.82 times higher in those who are not physically active, 0.49 times lower in those with heavy alcohol consumption, and 0.62 times lower in those who skip breakfast. Smoking and sleep do not exhibit statistically significant effects (Table 5).
For the dyslipidemia-stroke-heart disease-arthritis combination in the senior group, the results are similar to those seen in the middle-aged group. The prevalence of the combination is 3.02 times higher in those who are not physically active, 0.12 times lower in those with heavy alcohol consumption, and 0.10 times lower in those who skip breakfast. Smoking and sleep do not exhibit statistically significant effects (Table 5).
Discussion and conclusions
The prevalence of chronic diseases and MCD is increasing due to increased life expectancies and aging populations. MCD results in increased mortality,37,38 poorer quality of life, 39 and higher medical costs 40 compared to those who present with a single chronic disease. Considering that the proportion of the population who are aged in South Korea is rapidly increasing, individual and socioeconomic burdens of MCD are also expected to increase. To reduce these burdens, it is necessary to establish policies to prevent MCD; therefore, it is important to understand the characteristics of MCD in the current population. In this study, the combinations of MCD that affect hypertension, which has the highest prevalence worldwide, were examined according to different age groups: young adults, middle aged, and senior. The combinations of diseases were identified utilizing association rules analysis, using Korean health care big data from the Community Health Survey as the raw data.
Two association rules were determined in young adult group, 18 in the middle-aged group, and 30 in the senior group, showing that the number of rules increases with age. This is consistent with the results of a previous study reporting on the age-related morbidity of MCD. 31
Overall, the combinations of diabetes and diabetes-dyslipidemia were common to all three age groups. Diabetes and dyslipidemia are highly associated with hypertension, and this combination of chronic diseases has been frequently studied.21,22 In a study of veterans in the United States, the prevalence of the diabetes-hyperlipidemia-hypertension combination in young adult and senior groups was 24.4% and 29.1%, respectively, and was included in frequent combinations. 22 Likewise, in a Korean medical panel data study, the MCD combination of hypertension-diabetes-hyperlipidemia was the most prevalent (26.1%). 41 Hypertension, diabetes, and dyslipidemia are also important risk factors in patients with advanced cardiovascular disease with a high prevalence. 42
As the age of the groups increased, more MCD combinations were observed, along with an increasing number of chronic diseases in MCD combinations. In the young adult group, the number of diseases in MCD combinations was a maximum of two, but in the middle-aged group, that number increased to three, and in the senior group, it increased to four. These results suggest that as the prevalence of chronic diseases increases, more significant association rules can be drawn, and in general, as age increases, the number of chronic diseases and MCD combinations increases. 14
According to the results of age group analysis, the lift value of the association rules was very high in the young adult group compared to the other age groups. In particular, the lift value of the diabetes-dyslipidemia combination was 11.69, indicating a very high influence on the prevalence of hypertension. In fact, the prevalence of hypertension among the young adults presenting with diabetes and dyslipidemia was 45.2%. According to chronic disease health statistics, the prevalence of Hypertension in men aged 30–39 increased from 12.6% in 2010 to 17.1% in 2018, and the prevalence of women increased from 1.6% to 5.8%. 43 Also, the prevalence of hypercholesterinemia in men aged 30–39 increased from 8.9% in 2010 to 15.1% in 2018, and the prevalence of women increased from 3.1% to 9.2%. 43 Because a major cause of death in individuals between 20 and 30 years of age in South Korea is cardiovascular disease, this finding suggests that younger people in their 20s and 30s are exposed to risk factors for cardiovascular disease.16,44 In the association rules of young adult group in this study, a strong association of diabetes, dyslipidemia, and hypertension, which are precursors to cardiovascular disease, was identified, supporting this fact. Therefore, action is required to prevent cardiovascular disease in young adults.
The number of association rules in the middle-aged group increased by 16 relative to the young adult group, with a maximum of three additional diseases included in MCD combinations. In combinations with three chronic diseases, diabetes and dyslipidemia appeared (as they did in the young adult group); however, heart diseases and arthritis were also seen. These additional diseases agree with findings of previous studies, implying that the prevalence of disease increases rapidly with age. According to a report by the Korea Health Insurance Review and Assessment Service (HIRA) that included data from 2016, the proportion of patients with degenerative arthritis and rheumatoid arthritis was 27.5% for those in their 50s, which is a significant increase compared to the young adult group. 2 In the same data, angina and myocardial infarction also showed a sharp increase for those in their 50s. 2 In addition, the rates of hypertension, diabetes, and degenerative arthritis, which were reported to have higher rates of morbidity in individuals in their 50s compared to those in their 40s, were high: 126.5%, 121.4%, and 184.4%, respectively. 2
In the senior group, the number of association rules increased by 12 compared to the middle-aged group, and the number of diseases included in the MCD combinations increased to a maximum of four. The association rules analysis of the seniors revealed that the lift and confidence values increase as the number of chronic diseases in MCD combinations increases. This means that MCD has affects the prevalence of hypertension to a greater extent than a single chronic disease. Among MCD combinations of four diseases, the confidence value indicated a very high percentage (>90%) in dyslipidemia–stroke–heart disease–arthritis, diabetes–dyslipidemia–stroke–arthritis, and diabetes–dyslipidemia–stroke–heart disease. In other words, more than 90% of the patients with these combinations have hypertension, indicating that seniors present with more chronic diseases compared to other groups. Seniors over 65 years old have an average of 4.1 chronic diseases in a previous study. 14 Another study revealed that patients in their 60s have an average of three chronic diseases, and those in their 70s have an average of 3.5 chronic diseases. 45 Consequently, it is expected that the numbers of chronic diseases will continue to increase in seniors, and preventative measures are required. In particular, it is necessary to establish a long-term preventive strategy starting in young adulthood to address the long period to associated with the onset of chronic diseases.
Logistic regression analysis was performed on the MCD combinations with highest lift value in each age group to identify relationships between health behavior and MCD combinations. Alcohol consumption was found to be a common factor affecting MCD prevalence in three combinations. In the young adult group, heavy alcohol consumption resulted in a 1.94-fold higher risk for the MCD combination with the highest lift value, compared to 0.49, and 0.12-fold lower risks in the middle-aged and senior groups, respectively. The correlations of heavy alcohol consumption and chronic disease has yielded different results in various studies. After a thorough literature review, the effects of alcohol consumption can be summarized into three categories: heavy alcohol consumption increases the incidence of chronic disease; light alcohol consumption lowers the likelihood of developing chronic disease; and there is no relationship between alcohol consumption and chronic disease. 46
On the contrary, sleep did not have a statistically significant influence on any combination. In general, less sleep is believed to increase the risks of obesity, diabetes, hypertension, and coronary disease.47,48 Furthermore, getting less or more sleep than that which is deemed adequate is considered a risk factor for cardiovascular diseases and diabetes. 49 However, unlike the previous studies, sleep was not found to influence the risk of chronic disease in this study.
Furthermore, smoking was observed to have a significant effect on the prevalence of chronic disease only in the diabetes-dyslipidemia combination in young adults. Smoking is closely related to chronic disease because the odds ratio of subjects who smoke was 3.0. Smoking is a significant factor that adversely affects the prevalence of many diseases and causes coronary and respiratory diseases, malignant tumors, and cerebrovascular diseases. 50 A study that analyzed data from an American cohort also revealed a significant association between smoking and chronic diseases such as renal failure, ischemic bowel diseases, hypertension, respiratory diseases, breast cancer, and prostate cancer. 51
Moreover, physical activity and breakfast intake showed the same relationship with chronic disease prevalence in the diabetes-dyslipidemia-stroke combination in the middle-aged group and the dyslipidemia-stroke-heart diseases-arthritis combination in the senior group. The odds ratio of a physically inactive lifestyle was 1.82 in the middle-aged group and 3.02 in the senior group, showing that consistent exercise can prevent chronic diseases. According to a physical activity guidelines report from the U.S. Department of Health and Human Services, medium–high intensity physical activity reduces the risk of chronic conditions such as obesity, metabolic syndrome, hypertension, diabetes, and cardiovascular disease. 52 Moreover, the odds ratios of skipping breakfast in the middle-aged and senior group were 0.62 and 0.10, respectively, which implies that skipping breakfast lowers the risk of chronic disease. This result is contrary to previous studies, which report high correlations between skipping breakfast and cardiovascular risk factors such as hypercholesteremia and hypertension 53 or being diagnosed with diabetes. 54
Influences between chronic diseases in MCD become more significant with age, and the number of patients with MCD increases. Furthermore, the influence of healthy behaviors, which is the main cause of chronic disease, differs by age group, and the diseases constituting specific MCD combinations also vary. Currently, chronic disease management addresses single diseases; however, approaches to manage MCD are necessary to prevent chronic disease. When treating MCD patients, either prevention or treatment should be prioritized due to time and resource constraints. 55 When prioritizing, the characteristics of MCD data provided in this study may provide helpful guidance.
However, this study is limited because it uses cross-sectional study data in which the characteristics were assessed at one point in time. Therefore, this study does not reflect temporal factors. Furthermore, this study utilized big data of approximately 220,000 people in health care; therefore the study has some representativeness. However different association rules may be revealed depending on the year researched or target subjects of the survey. Additionally, all of the variables used in this study were collected through self-response questionnaires; consequently, questionnaires and limitation exist resulting from relaying on the subjectivity of respondents. Furthermore, it was not possible to reflect the cases of those who are currently sick, but were undiagnosed because the responses were based on the diagnostic experience of the respondents.
Despite its limitations, the results of this study suggested that applying association rules to big health care data yields meaningful results. The analysis method applied in this study can apply specific categories such as year, region, and chronic disease. If additional data is accumulated or the survey scope is expanded in the future, then applying this analysis method is not only possible but would also be expected to yield more accurate and reliable MCD management model.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This study utilized secondary data from the Ministry of Health and Welfare and was approved as exempt from IRB deliberation by the Kyung Hee University Institutional Review Board (KHSIRB-19-323).