
Abstract
Surgical training in civilian hospitals may not be sufficient for managing complex trauma in a setting where such care is not commonly practiced. Understanding the challenges that civilian teams face when moving to austere environments can inform the competencies that need to be trained. The aim of this study was to explore the competencies required in austere environments for teams managing complex trauma, and how they can be trained with simulation technologies. Ethnographic field observations were conducted, and field notes were synthesized. The field notes were structured with the elements of Activity Theory to generate the teams’ competencies that need to be trained. A literature review was conducted to verify the results and identify examples of relevant simulation modalities. The analysis resulted in a structured list of competencies for civilian teams to manage complex trauma in an austere environment and recommendations which simulation technologies could be used in training of those competencies based on published studies. Our study contributes to understanding the challenges that civilian teams face when operating in an austere environment. A systematized list of competencies with suggested simulation technologies directs future research to improve quality of complex trauma training in civilian and military collaboration.
Background
The increase of emergency incidents in the civilian environment is raising concerns and especially in the context of the Nordic countries, where there is a lack of experience of how to handle such incidents. 1 As a matter of fact, many European countries have been struggling with managing the increased emergency incidents during the COVID-19 pandemic. 2
Particular lack of experience lies in the context of complex trauma care, where trauma professionals may work in both civilian and military settings. Trauma injuries are considered ‘‘simple’’ if only one body system is involved, and ‘‘complex’’ when there is injury to more than one body system, such as orthopedic, vascular, gastrointestinal, and/or urogenital injury. Complex trauma requires advanced techniques to sustain the functions of the human body and must be applied to avoid the potential loss of life. 1 Civilian and military collaboration is considered important 3 ; however, there are a number of challenges arising from the integrated collaboration related to different working routines, ethics, or cultures of the civilians collaborating with military personnel, where the need of learning opportunities focusing on collaboration is highlighted. 4
Complex civilian and military trauma care is characterized by time pressure that can affect clinical decision-making; involvement of various stakeholders that demand a multidisciplinary management; unpredictable workflows; and non-replicable conditions. 5 Appropriate management and treatment in complex trauma settings can provide survival benefits, and therefore, the ability of the trauma professionals to make timely and effective decisions is essential in order to reduce medical errors, improve professionals' performance, and ultimately optimize patient outcomes.6,7
Complex trauma management requires a combination of technical and non-technical skills; non-technical skills are considered as ‘‘the cognitive, social and personal resource skills that complement technical skills and contribute to safe and efficient task performance.” 8 Non-technical skills, also described often in literature as soft skills, include leadership, teamwork, decision-making, and situation awareness. 9 Leadership is an essential component in trauma management, where team leaders are usually senior surgeons with extensive experience.
The trauma team is a complex organization which has to work efficiently in complex trauma situations, whereas the trauma team set-up varies across countries. Operating rooms have been studied before with emphasis on the leadership, communication, and teamwork, due to concerns regarding the impact of human factors on patient safety in the surgical contexts. The impact of inadequate communication on quality and efficiency of surgical procedures and how attitudes concerning medical errors and teamwork may influence the quality and efficiency of surgical procedures have been of particular interest.10–12 Future research should build on and integrate research in team cognition, learning, and decision-making to maximize the potential of the teams’ collective cognitive capabilities. 13
As healthcare personnel are not exposed to complex trauma patients on a regular basis, they will not accumulate sufficient experience to develop their competence in the area. An often postulated training method in such cases is to use simulation. 14 Simulation may refer to various technologies, from virtual reality required extensive equipment to simple mannequins; different technologies are used to train different competencies. 15
General principles about designing educational material to train interprofessional teams suggest contextualizing the training into the characteristics of the setting where the team operates. A recent literature review 16 attempted to understand the unique characteristics and factors that shape a successful military medical team, while exploring whether contextualizing training could benefit educational interventions for military medical teams.
There is a lack of research about the challenges that civilian teams face when moving to austere environments; understanding these challenges is crucial for designing training that addresses the appropriate competencies. The aim of this study was to explore the competencies required in austere environments for teams managing complex trauma, and how they can be trained with simulation technologies.
Methods
Study Design
Ethnographic field observations 17 were conducted in two different contexts, and field notes were synthesized. A qualitative directed content analysis was performed: the elements of Activity Theory (AT) were used to code and structure the field notes.18,19 The analysis resulted in a structured list of competencies for teams managing civilian and military complex trauma that need to be trained. A literature review was conducted and examples of simulation technologies that have the potential to train the competencies were identified.
Data collection and analysis
Ethnographic field observations
Ethnographic field observations of complex trauma team training were performed in two different contexts, during the course “Definitive Surgical Trauma Care” (DSTC™), 20 which took place at the Sahlgrenska Academy, University of Gothenburg, during February 2019, and during the multinational exercise ‘‘Vigorous Warrior 2019’’ (VW19) 21 which took place in Romania, organized by NATO, Centre of Excellence for Military Medicine in April 2019—a multinational military organization working for and accredited by NATO. In both contexts, the observations focused on capturing challenges of teams, trained in a civilian setting, operating in a simulated military environment, which can inform technology-enhanced learning.
Definitive surgical trauma care is a high-end international course offering education in decision-making and training of surgical skills required for the management of complex trauma patients. The DSTC is designed to teach qualified surgeons and anesthetists in strategic thinking and decision-making in the management of the severely injured patients and provide them with practical surgical skills to manage major organ injuries. One of the authors NS participated as an observer and interacted with team members in a “marginal participant role” 17 that allowed for informal discussions with team members. Field notes in the form of jottings and direct quotes were transcribed.
The Vigorous Warrior 2019 (VW19) exercise was the biggest high scale multinational live simulation exercise for practicing military medicine. Observations were, in particular, performed at ROLE2 hospitals. ROLE2 can provide triage and resuscitation, treatment and holding of patients, and emergency dental treatment. Certain operations may require their augmentation with the possibility to perform emergency surgery and essential post-operative management. 22 To preserve accuracy and detail of the observations NS documented significant events and actions using field notes and photos; noteworthy events and impressions were captured in key words and phrases. 23 The notes were later analyzed by NS and KK and the results were shaped by the discussions with LS and KB.
Activity Theory as a framework to structure trauma team competencies
Activity Theory (AT) presents a conceptual framework within the field of human–computer interaction and interaction design used for the purpose of understanding and designing technology in the context of purposeful, meaningful activities, which is a central concern of human–computer interaction research and practice. 18
Activity Theory focuses on the interaction of human activity within its relevant environmental context, and it has been used as a methodological and analytical framework to structure information practices in the context of emergency management, focusing on how humans interact with each other in a community setting and with and through various kinds of tools in an environment toward certain objectives. 24 Activity Theory has been used before in order to support the designing of learning environments in a constructivist approach 25 and to structure learning activities in Massive Open Online Courses. 26
Activity Theory is viewed as an appropriate organizing framework for integrating the individual cognitive and social constructivist dimensions of learning, 27 and for that reason, it was selected as a method to analyze and structure the challenges of a complex trauma team as the first step toward informing the content of technology-enhanced interventions as authentic learning tasks.
In particular, the AT framework suggested by Engeström 28 includes the following six elements: subject, objective, tools, community, rules, and division of labor, interacting toward an outcome. This variant of the AT framework reflects the process of social transformation and incorporates the structure of the social world, with special emphasis on the contradictions of activity systems and the dynamic nature of a community. The contradictions in our case between the elements of the AT depict the challenges of the trauma team operating in an austere environment. By applying this framework, we place particular attention to the teamwork and how its activities might impact on the complex trauma patient management.
The collected data of the field notes were coded qualitatively with directed content analysis 19 mapping elements of the AT framework to the elements of the trauma team. Data that could not be coded were identified and analyzed later to determine if they represented a new category or a subcategory of an existing code. That resulted in a list of challenges for teams managing complex trauma.
To validate the structured list of challenges, we triangulated the data with content from relevant published literature using a backward reference tracing technique 29 (p. 353). In particular, four previous systematic literature reviews about simulation training for trauma teams were identified,30–33 and their references were further examined to validate the identified competencies, as well as to identify suggested simulation technologies that have the potential to train the competencies. Furthermore, in order to gain an overview of recent technologies used in simulation, relevant literature was identified with a purposive sampling in MEDLINE using the search phrases: “Trauma training” AND “simulation” filtered for the years 2018–2021. After removing the duplicates, 56 studies were considered for the literature review. The framework suggested by Jacob A. Quick 15 was used in order to categorize the different types of simulation identified from the different studies in a consistent way. In those rare cases, it was deemed necessary, and the framework was extended with emerging technologies which were not considered in the original.
Ethical approval
Ethical approval was requested from the Swedish Ethical Review Authority (Diarienr. 2016/1701-31) and it was not processed, as the authority did not have any objections about our research since it is not covered by the Swedish Ethical Review Act. The ethical approval is therefore not required. An amendment was made in 2020 (Diarienr: 2020-01660) and the same response was acquired from the Swedish Ethical Review Authority, about exemption from the requirement to obtain an ethical approval.
Names and ethnicities during the field observations were not recorded, and data about the observed participants that could leave them identifiable were left out.
Results
Ethnographic field observations
The DSTC course that took place at Sahlgrenska Academy, University of Gothenburg, during February 2019 included 24 participants with backgrounds in surgery, orthopedics, anesthesia, radiology, and nursing. After participating in the course lectures, the participants were divided into three new teams taking part in live-tissue training. The teams managed lab animals that had been inflicted with complex wounds. The sessions were guided by course instructors. The instructors described the situation to add authenticity to the simulations and time pressure by emphasizing to the participants that they have to act fast. The instructors also guided the participants when needed, asking individuals to act as team leaders and to manage the complex trauma cases in the given time. NS observed the trauma management and made field notes. As NS interacted with the team members in a “marginal participant role” and asked questions to enhance her understanding after their training, direct quotes were transcribed too.
The VW19 exercise involved 26 NATO allies and 13 partners. More than 2,500 participants from 39 countries participated to train and assess their medical competences together in a dynamic environment. The authors observed the ROLE2 simulated centers which were emergency rooms with intensive care facilities. The simulated complex trauma cases consisting both of mannequins and human actors arrived there with civilian or military ambulances with different kinds of injuries. They were triaged and treated by the trauma teams, and depending on the injury, sent to operation or to one of the intensive care units or wards pending further transport.
Activity Theory framework to structure the elements of a complex trauma team
The elements of the AT framework were mapped to the elements of a complex trauma team as follows: Tools: equipment, resources; subject: team leader; rules: guidelines, procedures; community: team members; division of labor: delegation of roles; objective: complex trauma management (Figure 1). Elements of the activity theory mapped to the elements of a complex trauma team.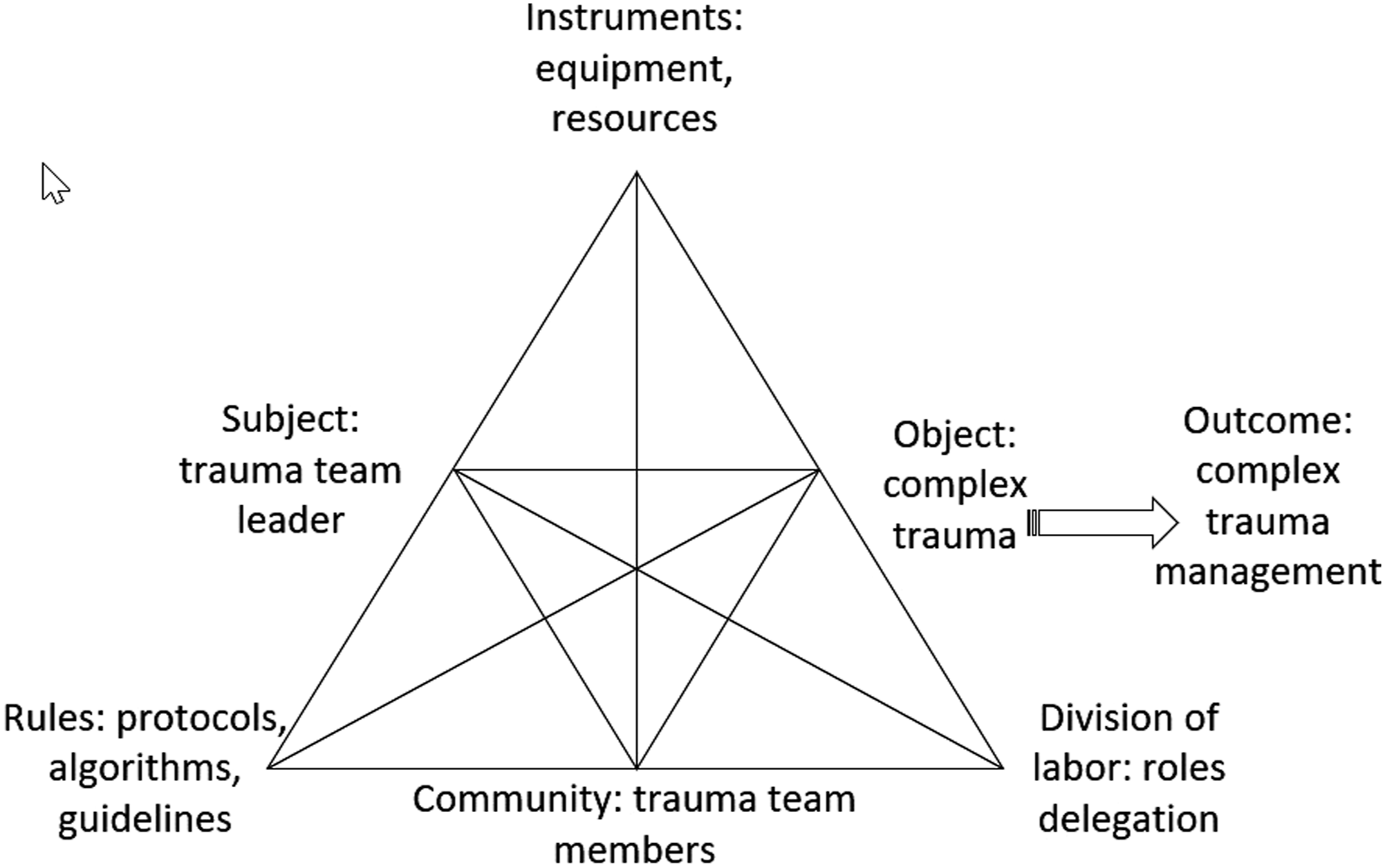
In particular, we understand the subject and the community as the team leader and the trauma team members, respectively, since the community represents all actors involved in the activity system and we isolate the team leader as the main subject of the activity system. We understand the rules as protocols and guidelines regulating activities in the system; tools (or instruments) as the equipment and the resources used by the complex trauma team; and division of labor as the social strata, hierarchical structure of activity, and the division of activities among actors in the system which is the delegated roles that each member in the team has.
Structured list of competencies generated from analyzing the field notes with the mapped elements of the activity theory; examples of simulation technologies that can be used to address the identified competencies.
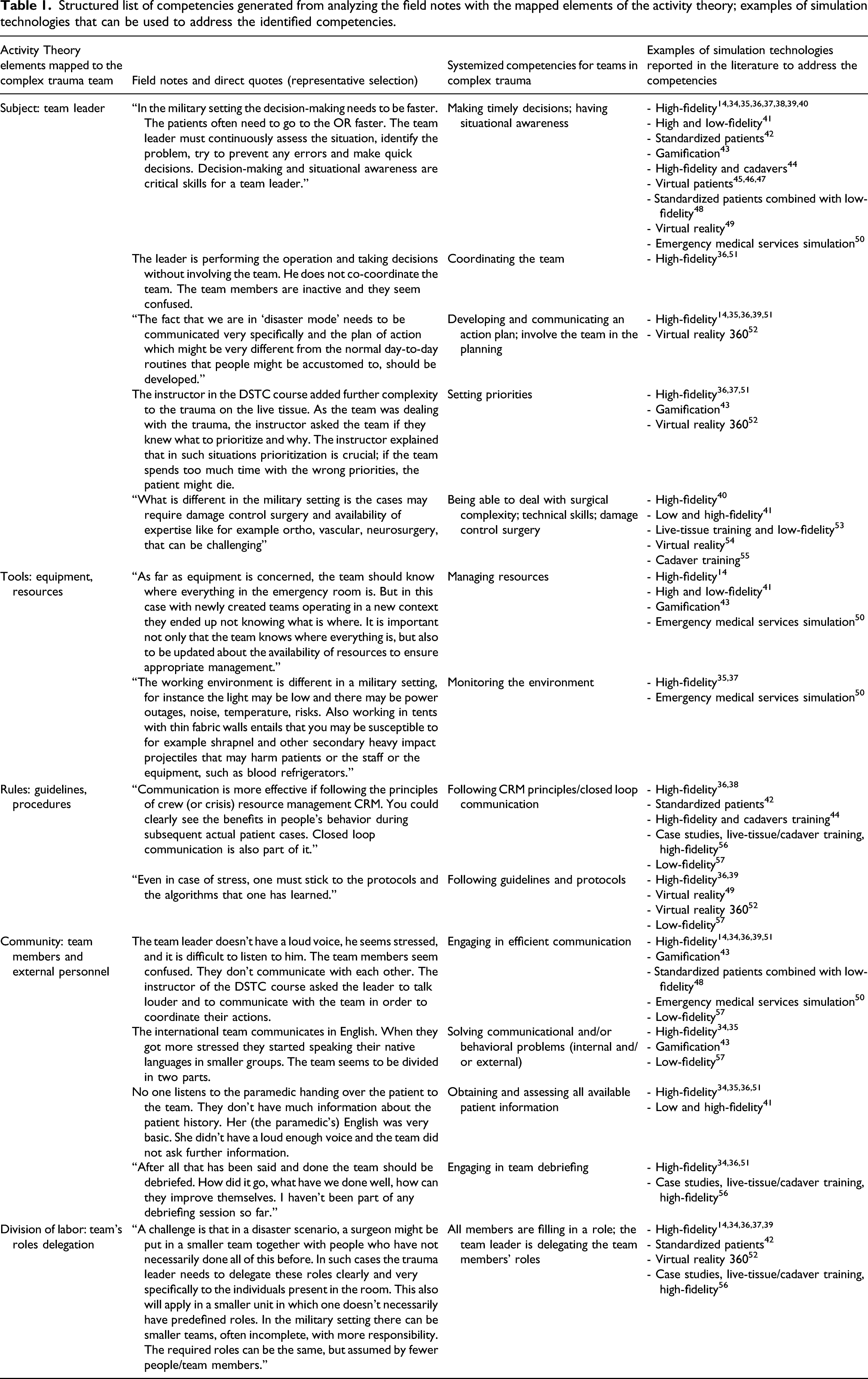
Our results systemize the competencies that need to be trained by civilian teams to manage complex trauma in an austere environment and provide recommendations about which simulation technologies could be used in training of those competencies based on published studies.
Discussion
This study contributes to understanding the competencies required for teams managing civilian and military complex trauma, informed by observations, and how they can be trained with simulation technologies. The starting point was the field notes from the ethnographic observations that were analyzed with directed content analysis, using the elements of the complex trauma team mapped to the AT framework as codes. A literature review was conducted to verify the competencies identified and to indicate examples of simulation interventions that have been applied to train these competencies.
The ethnographic method allowed us to rely on our own experience and intuition to select noteworthy incidents out of the flow of ongoing activity. 22 We acknowledge that our background could have influenced the ethnographic observations and the field notes. NS who participated in the DSTC course and the VW19 exercise and synthesized the field notes, has a background in medical informatics which allowed an uninfluenced approach to the observations. LS and KB have a background in military trauma that shaped the discussion of the data collected and informed the analyses from the medical subject matter point of view.
Conducting field observations allowed us to understand the challenges of a complex trauma team in a non-dualistic worldview, meaning that the activities of the team are not separated from the human actors (trauma team leaders and trauma team members): ‘‘Human behavior, unlike that of physical objects, cannot be understood without reference to the meanings and purposes attached by human actors to their activities.’’ 58
Our methodology is in line with socio-cognitive approaches to analysis of non-technical skills training where it is emphasized to consider also the environment where the learners are situated and the interactions with other participants to form a complete picture of the educational experience. 59 The AT allowed us to obtain as a result a structured list of competencies that the teams need to train to prepare managing complex trauma in an austere environment. One limitation of AT in emergency situations is that it does not capture time; an important variable especially in the context of complex trauma that was captured by transcribing the observations.
The main advantage of our methodology is that the Activity Theoretical analysis helped us structure and focus the observations and analysis without overseeing important aspects. A potential limitation is that the use of the Activity Theoretical analysis can bias the deductive analysis so that certain variables are overemphasized whereas others are overlooked. To support the trustworthiness of our approach, we report on the process of content analysis accurately by presenting examples that guided our coding. In addition, generating codes deductively rather than inductively may contribute to higher reliability according to the literature. 60 To validate our results, we conducted a literature review.
The environmental differences of military and civilian medical setting may involve challenges due to, for instance, temperature differences affecting the equipment, the patient, and the chemical stability of drugs. Moreover, the resources available in an austere environment may differ from those in hospitals. The culture and economic status of the country is an additional important factor.
Some of the challenges observed regarded the roles delegation and in particular in the case of an incomplete team; the roles may be the same among civilian and military teams, but in a military environment, they can be shared among fewer team members. Ability to communicate with the team, solve potential communicational problems, engage in debriefing, and ensuring that all members fill in a role are important to consider as they can lead to suboptimal management. For instance, team members in one international team, collaborating for first time, started to communicate in their native languages in smaller groups when under high stress. Failure to communicate within the team may have serious implications. This is in accordance with previous studies showing that errors in communication are estimated to occur in more than 50% of trauma resuscitations and is among the main reasons for suboptimal performance of the trauma team and team leader. 7
Competencies related to technical skills, surgical complexity, damage control surgery, and the availability of specific expertise as, for instance, ortho, vascular, and neurosurgeons were discussed by the exercise participants. Other non-technical skills such as decision-making, situational awareness, and setting priorities were observed to be challenging for the team leader and can be associated partly to the fact that the type of injuries (gun shot and blast injuries) are actually not commonplace in the civilian healthcare but also due to the fact that managing complex trauma in an austere setting requires a specific mindset. 46 The adherence to well-established protocols and guidelines and in particular the lack of standardized protocols has also been introduced before as one of the challenges of civilian and military healthcare collaboration. 61 Our results are in accordance with previous research, discussing behaviors, competencies, and challenges of teams in emergency medicine.62,63
Simulation technology entails new possibilities in the areas of contextual learning, active learning, and individualized learning, and has the potential to support the training of the competencies. Four previous systematic reviews about trauma teams and simulation were identified and their references were examined, to verify the identified competencies, and to identify the suggested simulation that can address these competencies. To gain an overview of more recent and emerging technologies, an exploratory search in MEDLINE was performed for the years 2018–2021.
The systematic reviews concluded that simulation training can have a positive impact on acquisition of non-technical skills of trauma teams,30,31,33 but only one of them focused specifically on one type of simulation (manikin-based simulation) even though without a clear distinction between low and high-fidelity manikins. 32 Future reviews should examine the linkage of specific simulation types and competencies.
The most frequently discussed simulation was high-fidelity simulators, defined by having “features that incorporate all body systems so that the facilitator can customize each patient encounter.’’ 15 Although high-fidelity simulations have been mainly used to teach procedures and technical skills, the identified literature indicates their use in order to train non-technical skills and competencies such as communication, team coordination, delegation or roles and tasks.
Our study systematizes competencies needed to be trained by teams managing complex civilian and military trauma and aligns them with those available simulation technologies that were reported in the literature to address those competencies. An open question remains whether some of the suggested simulation technologies could be used to address more competencies than the suggested ones. Future research could also explore which of these technologies are most effective in achieving higher performance of civilian and military trauma teams, as well as which design characteristics of those interventions lead to improved competencies and eventually patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Swedish Armed Forces, Centre for Defence Medicine, Department of Research and Development.