
Abstract
Many telemedicine interventions fail to be implemented in medical care with non-use and discontinued use by patients being among the major reasons. The aim of this scoping review was to provide an overview of barriers associated with non-use and discontinued use of telemedicine. An electronic search was conducted in Pubmed in October 2019 and updated in November 2020, followed by a hand search in the beginning of 2021. All potential articles were screened by two independent reviewers based on predefined inclusion and exclusion criteria. A qualitative content analysis according to Mayring was carried out. The topics ‘intervention’, ‘context of use’ and ‘user’ were chosen as overarching themes. Out of 1377 potentially relevant articles, 73 were included. User-related barriers were mentioned in most of the analysed studies, followed by barriers related to the intervention. The analysis provides the basis for overcoming non-use issues in telemedicine.
Background
Telemedicine allows medical services to be delivered by providers at a distance 1 and has the potential to overcome barriers to classical care such as high costs, large geographical distances or limited access to medical services due to gaps in primary care.2,3
A large number of studies show that telemedicine interventions are both efficient and cost-effective4,5 and have a positive impact on patients’ health behaviour,6,7 medication adherence8–10 and quality of life.11,12 Furthermore, telemedicine has been shown to improve the management of many chronic conditions13–15 and clinical outcomes 16 with equal or even greater effectiveness than analogue interventions. 17 Positive examples for the use of telehealth and mHealth as dimensions of telemedicine exist globally: Denmark, for example, has established both regional patient monitoring mHealth systems and nationwide remote monitoring systems for chronic diseases, while in Sweden especially the latter systems are interlinked with international initiatives and intermediate networks for mobile health care provision exist throughout the country. 18 Also, there is a number of successful examples as to how telemedicine use can enhance the effectiveness of regional integrated care networks (for an overview, see World Health Organisation 18 ). In remote areas, the delivery of acute care via telemedicine is both well-established and highly necessary. 19
Advances in the use of telemedicine and the removal of longstanding barriers towards its use (such as data security and liability issues) have also been made quite recently due to the need to respond to the COVID 19-pandemic. 20
Despite this strong evidence and a constantly growing range of available applications, most telemedicine applications fail to meet the threshold to be implemented into regular care.21,22 Among the main reasons for this so-called scale up-problem are non-use and high drop-out rates, which translate into discontinued use over time.23,24 A systematic review by Donkin et al. 25 observed an average dropout rate of 23% with maximum values of up to 83% in 69 telemedicine studies. A study by Farvolden et al. 26 evaluating a 3-month online web programme for people with panic disorder found that only 1% of all participants (12 out of 1161) completed the intervention.
As discontinued use and non-use are two of the biggest challenges for long-term telemedicine implementation, it is important to identify barriers users face when using telemedicine applications, whether from the start or later on, in order to improve the uptake of future interventions. A systematic review by Harst et al. 27 already investigated factors associated with an increase in user acceptance. In a similar approach, this study aims to identify barriers to the use of telemedicine that are associated with a decrease in acceptance. To the authors’ knowledge, this is the first literature review to address the issue of non-use of telemedicine. The present work concentrates on interventions that fall under the telemedicine definition of Sood et al. 28 and thus enable the care of patients by medical providers over a geographical distance. This focus was chosen because patient cooperation is particularly important for the effective and sustainable use of these applications, especially when they are used for the self-management of chronic diseases. 29
As such, the research question for this scoping review is as follows: Which barriers prevent the uptake and continuous use of telemedicine applications from the patients’ perspective?
Methods
In previous research, non-use was mainly the subject of primary studies. This work was conducted as a scoping review to develop a structured and transparent overview of the previous results in this research field. 30
Inclusion and exclusion criteria
The inclusion and exclusion criteria for this review were formulated using the PICOS criteria population, intervention, comparison, outcome and study design. 31 Since this study was focussed on the non-use of telemedicine interventions rather than their effectiveness, the sub-item “comparison” was not considered in the study selection.
The population studied included patients or groups at risk for chronic diseases as well as their direct social environment. All studies on telemedicine interventions in which patient-centred medical care services were delivered over a geographical distance were included. 28 An exception were game-based interventions, which are a special form of telemedicine 32 and currently of interest for a specialized, that is, younger population 33 and therefore were not included in this research. Studies about online searches for health information were also excluded, as they do not fall under the telemedicine definition.
The outcome examined in this study was user behaviour, whereby only studies that mentioned non-use or barriers to use in the title or abstract were included. With low usability being a known predictor for non-use, studies clearly discovering usability issues were also included. 34 Another requirement for inclusion was the publication in German or English.
Table 1 provides an overview of the predefined inclusion and exclusion criteria.
Inclusion and exclusion criteria according to the PICOS criteria.
Development of the search string
Based on the PICOS criteria, a search string was created in October 2019. A previously piloted search string of Harst et al. 27 whose structure was also based on the PICOS criteria, was used as a template. The sections on the intervention and the study design could be adopted almost unchanged for this review. Since the term telemedicine is not used uniformly in research, 35 the search string by Harst et al. already included the terms for other forms of digital health that are often used synonymously, such as ‘eHealth’ and ‘telehealth’. The sections on population and outcome were adapted according to the inclusion criteria. The search string for the database research can be found in the Appendix 1.
Literature research
A search was conducted in Pubmed in October 2019 and updated in November 2020. In addition, a hand search was performed in January and February 2021. For this purpose, the references of all included studies of the electronic search were examined for further articles that fulfilled the inclusion and exclusion criteria.
Study selection
The selection process was carried out by two independent reviewers. In a first screening, all records of the electronic and manual search were examined for relevant titles and abstracts. Each decision to include or exclude a paper in further research was documented in writing and later discussed by both reviewers. In the subsequent full-text screening of all potentially suitable studies, half of all papers were read by one reviewer and again, reasons for in- and exclusion were documented. In a final discussion between both reviewers, the decision to include or exclude a paper from the analysis was made.
Data extraction
For each included article, the following criteria were recorded: Title, country of origin, year of publication, intervention, barriers and study design. Subsequently, the extracted barriers and factors for non-use were categorised using qualitative content analysis according to Mayring. 36 The topics ‘intervention’, ‘context of use’ and ‘user’ were chosen as overarching themes. This decision was based on relevant literature on user-centred design, in which the characteristics of an intervention, the context of use and the characteristics of the individual user were defined as decisive criteria for the acceptance of technologies. 37 Thus, the categorisation procedure was partly deductive based on Esser and Goosens’ framework and partly inductive based on recurring patterns in the barriers found.
During the development of the categorisation, the results were repeatedly reviewed and discussed by the two reviewers until both agreed on the structure.
Results
The electronic search in Pubmed gained 1266 results. Another 111 papers were identified during the hand search. After screening all titles and abstracts, 1269 articles could be excluded because they did not meet the inclusion criteria. Of the 108 remaining studies, 35 were excluded during the screening of the full texts. Of these, five articles were inaccessible, 18 papers did not describe barriers or non-use, in nine studies the population examined did not meet the inclusion criteria (four times there were no specific diseases or risk factors mentioned, three times healthcare providers were interviewed instead of patients and twice the population was mixed and the statements could not be clearly attributed to the target population of patients) and in two cases no telemedicine intervention was examined.
The remaining 73 studies could be included in the evaluation. Of these, 53 came from the electronic search and 20 from the hand search. A presentation of the selection process according to the PRISMA flow chart 38 is to be found in Figure 1.
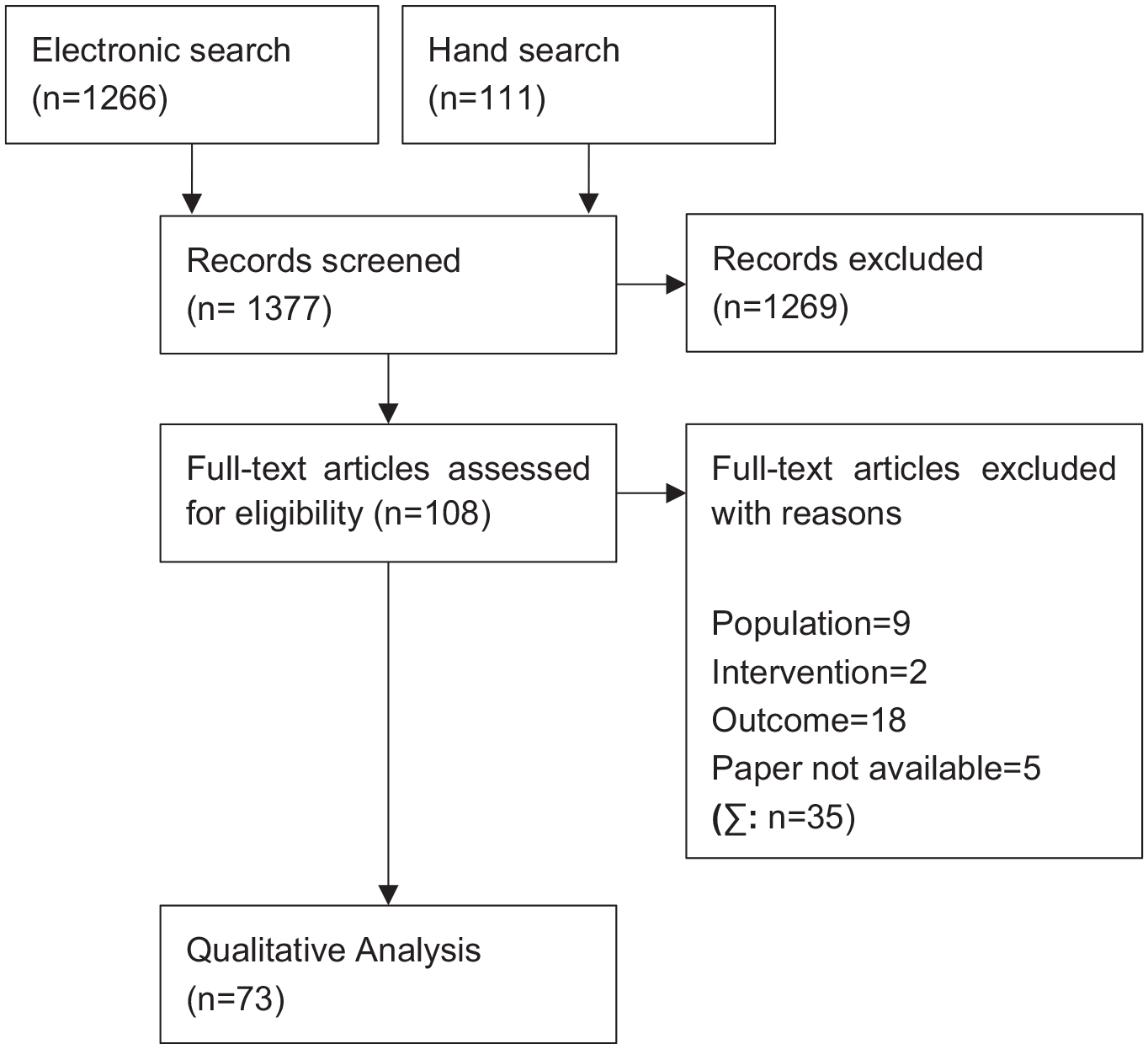
Flow chart of the study selection procedure.
Study characteristics
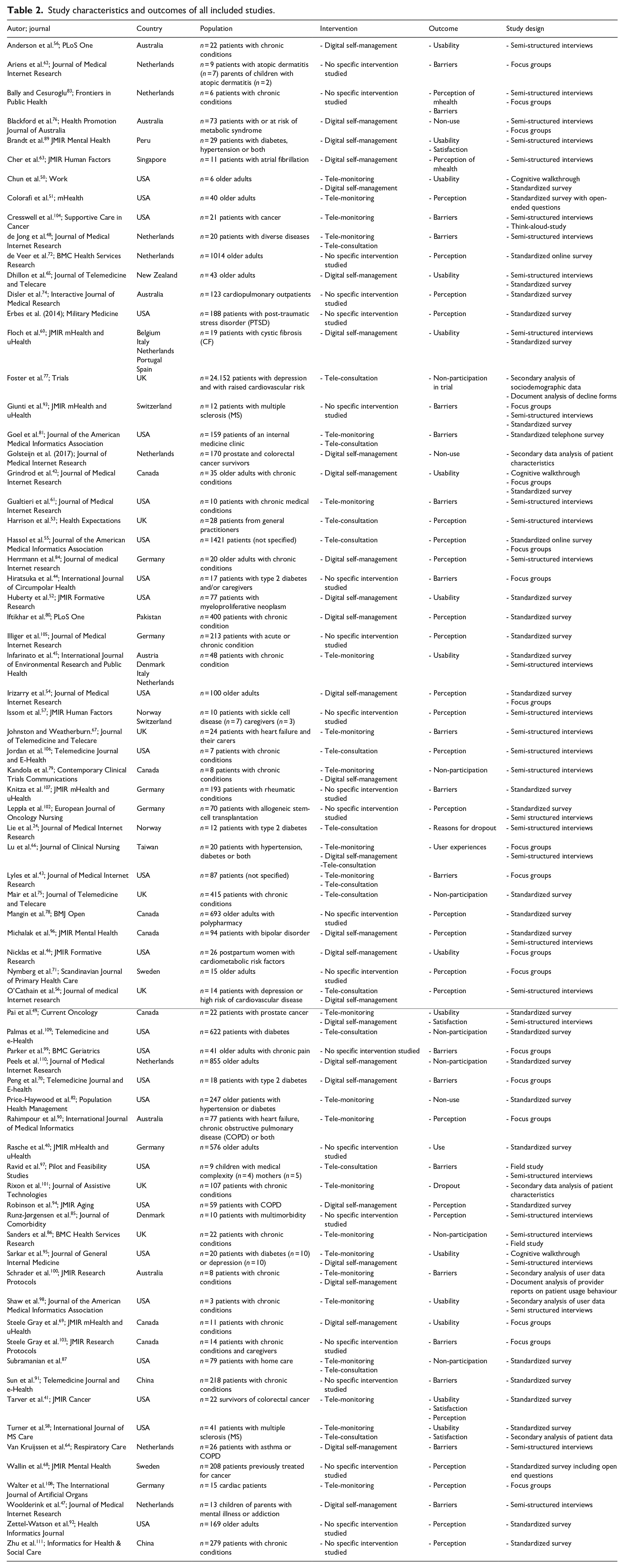
The included articles were published between 2004 and 2020. Most studies came from North America and Western Europe (n = 61), mainly from the USA (n = 27), the Netherlands (n = 10) and the UK (n = 8). Six studies were from Oceania, five from Asia and one from South America. A total of two studies came from countries (Peru and Pakistan) that are currently classified as developing countries by the Development Assistance Committee (DAC). 39
The number of participants varied from three to 24,152 (mean n = 465.29 [SD = 2821.94], median n = 29). The most used methods were standardised questionnaires (n = 34) and semi-structured interviews (n = 31). About 22 studies used multiple methodological approaches. A detailed description of the study characteristics is given in Table 2.
Study characteristics and outcomes of all included studies.
Overview of categorisation with examples.
Characteristics of the population
A total of 54.37% of the subjects studied were female and 45.63% were male (eight papers did not contain information on gender distribution). Most studies reported the mean age of the population (n = 59), which was 59.18 throughout all included studies. In the majority of studies participants already had a manifest disease (n = 67). Often, more than two chronic diseases were present, or the type of disease was not further defined (n = 22). In the remaining cases, the subjects mainly had cardiovascular diseases (n = 9), diabetes (n = 8), mental illnesses (n = 6), cancer (n = 6) and lung diseases (n = 5). A total of 14 studies included patients at risk for chronic diseases, with increased age as the most common risk factor (n = 8), and five studies interviewed relatives.
Interventions
The classification of telemedicine interventions was based on Harst et al.’s 88 categorisation into digital self-management (n = 27), tele-monitoring (n = 23) and tele-consultations (n = 15). The term digital self-management refers to telemedical services that aim to support informed shared decision making, self-care behaviour and health literacy, whereas the term tele-monitoring refers to digital services collecting vital data from patients and reacting to them in a timely manner and the term tele-consultation covers all services in which patients receive medical support from health care providers from a distance. 88 In addition, there were 21 studies that did not address any specific telemedicine intervention. The outcomes studied were predominantly the general attitude of the subjects towards digital health applications (n = 26), barriers (n = 20) and usability (n = 15). The outcomes non-use (n = 3), non-participation (n = 7) and reasons for dropout (n = 2) were examined less frequently.
Categorisation of telemedical barriers
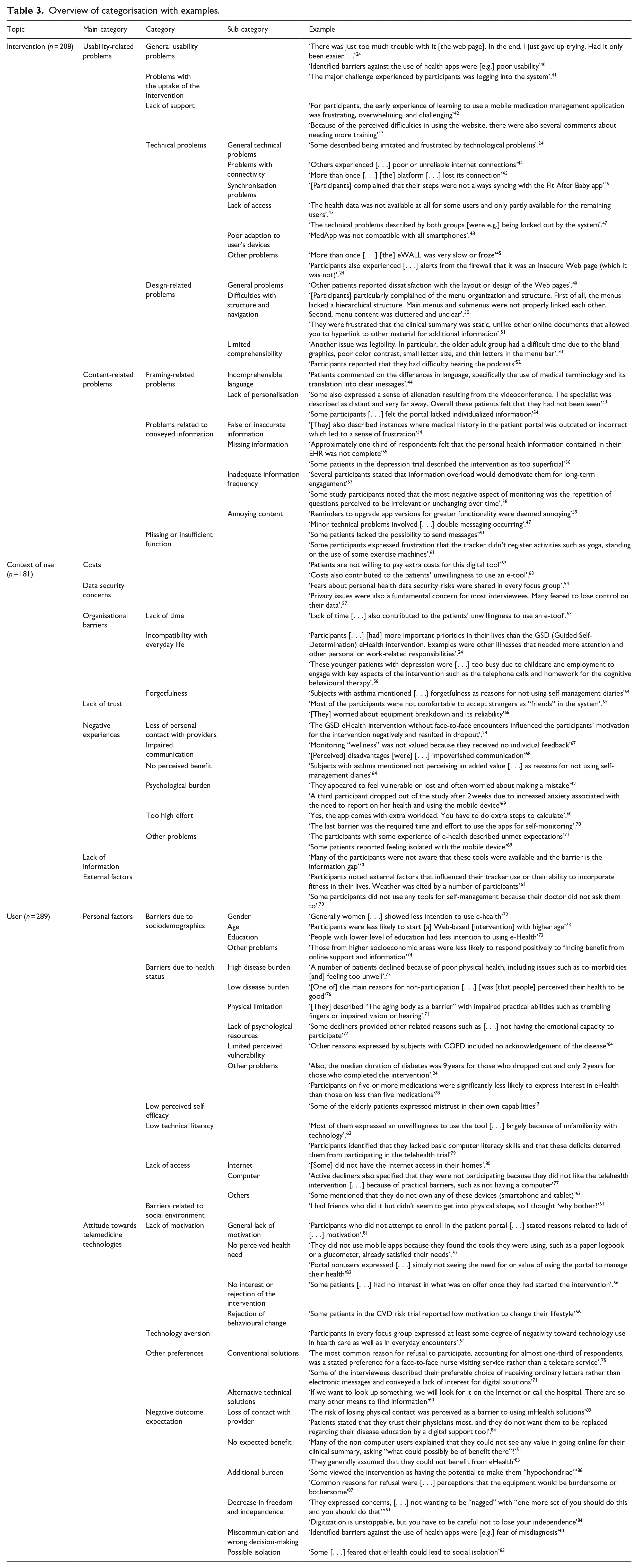
The categorisation was based on the three topics ‘intervention’, ‘context of use’ and ‘user’. Table 3 provides an overview of the categorisation with examples. A complete presentation of the categorisation can be found in the Appendix 2.
Barriers of telemedicine interventions
The topic ‘intervention’ contained 201 citations which were divided into two main categories: ‘usability related problems’ and ‘content related problems’. The
The fifth category
The second main category
Barriers within the context of use
The topic ‘context of use’ contained 181 entries and was divided into seven main categories.
Concerns about
Within the fourth context-related main category,
The fifth main category
The sixth main category,
Barriers related to the user
The topic ‘user’ contained 289 entries and thus accounted for the largest part of the barriers identified. It was divided into two main categories that distinguished between personal factors and attitudes towards health technologies. The main category
The second category,
Another regularly identified barrier and subject of the third category was a
The main category,
The topic of the second category was
Discussion
The aim of this scoping review was to summarize barriers to the uptake and continuous use of telemedicine applications from the patient perspective. While the focus on the patient perspective might seem overly restrictive at the first glance, the rational becomes apparent when considering that especially telemedicine applications used for the self-management of chronic diseases relay heavily on patient adherence. 112 Furthermore, the effects on behaviour change as the target outcome of self-management applications becomes apparent only after a period of up to 6 months of usage, 113 making the issue of continuous use an important one. With the majority of applications analysed in the studies included in this scoping review belonging to the domain of digital self-management and tele-monitoring, which is a necessary component of self-management, 114 the patient focus appears further justified.
While quantifying the relative importance of the three major topics, ‘intervention’, ‘context’ and ‘user’, is potentially biassed due to the subjective nature of qualitative content analysis, it is still of significance that most barriers to uptake and continuous use of any telemedicine application analysed belong to the latter two and are therefore rooted deeply within the user characteristics and his or her social environment and everyday life. Fittingly, the NICE framework for digital health evaluations suggests, as measures for effectiveness for application regarded as telemedicine, a focus on patient-reported experience measures such as satisfaction and engagement. 115
Still, the perception of the intervention, that is, application, itself plays a major role in the usage decision, as depicted in general models of technology acceptance 27 and non-use. 116 In order to ensure a continuous interest in using the application, which is a necessary precondition for its effectiveness in many cases, the results show that content must be neither redundant, nor annoying, let alone false. This underlines, once more, the need for a comprehensive quality assessment of telemedicine applications, as demanded, for example, by the ADA. 114
Despite the focus on patient perspectives on barriers to telemedicine uptake and continuous use, the provider perspective is not completely disregarded but rather represented in the barriers mentioned by potential users in the studies included: the fear for a loss of direct contact to the health care provider and a disruption of the patient-provider relationship is well-documented beyond the results of this study. 117 Such, it becomes apparent that patients do not wish for applications that replace their traditional health care modalities, but rather remove administrative tasks which keep the providers from spending more time tending to their patients’ needs. 118 However, during the current COVID-19 pandemic, telemedicine services were often the only way for patients to access medical services, maintain their personal relationships with health care providers and guarantee the continuity of care during social isolation. Consequently, COVID-19 has caused a leap in telemedicine-supported health care provision.119,120 Both before and during the pandemic, telephones are widely used and accepted in the context of telemedicine, 121 which is a possible explanation for the circumstance that very few barriers to telemedicine identified in this study were associated with telephone services. With the vast majority of our included studies having been conducted before the serious spread of COVID 19 and research on barriers to telemedicine use arising during a pandemic still to come, the current results cannot inform on that subject. Future research based on the methodology presented in this paper therefore is clearly warranted.
Another major issue raised within the ‘user’ topic is the feeling of inadequate self-efficacy when dealing with telemedicine technology, which point to the importance of the patients’ social network as a support structure 118 and the maintenance of a close provider-patient relationship, as the former will need to explain the application’s purpose and meaningful use to the latter continuously. 122
Taken altogether, the results of this scoping review and subsequent categorization of barriers to telemedicine uptake and continuous use show that patients have a clear understanding of what they expect of a telemedicine application 123 and what they find prevents them from using it. Therefore, the results, again, call for a user-centred design (UCD) approach to the development of telemedicine applications. 37 However, for issues such as displeasing content or a low usability, which was a major barrier to telemedicine use in this review as well, not to become a confounding variable in effectiveness studies, 124 the usage patterns of an application need to be studied as well, for example, using techniques such as think alouds 125 or cognitive walkthroughs. 126 Various models and theories can and should guide these user-centred design processes, as they include variables such as effort and outcome expectancy found as underlying patterns in the coding process for this present work.27,116,127,128
Involving the users in the development process of any telemedicine application also ensures a high degree of personalization of application design and content, which was reported missing in many studies included in this review and in other qualitative studies before. 129 Thereby, UCD also ensures uptake and continuous use of telemedicine is not hampered by barriers perceived by users later on.
Limitations and strengths
The findings of this study may have been influenced by a number of limitations. As only German and English publications were included in the literature search, there is a risk of a language bias. Furthermore, despite a thorough search and the high number of included studies, it is possible that not all relevant studies were identified due to missing keywords in the search string. In addition, only studies that already referred to non-use, discontinued use or usability problems in the title or abstract were included. This approach also carries the risk that relevant articles were not included in this study. Moreover, there were large differences between the investigated studies in terms of sample size, population characteristics and research questions. Most of the included studies came from developed countries, but since the health care system and the technological infrastructure differ between low-, middle- and high-income countries the possibility to draw generalizable conclusions is limited. Furthermore, not all studies investigated an intervention, but instead referred to the attitude of patients and risk groups towards telemedicine in general. In addition, most studies focussed on older adults since they account for many patients and groups at risk. Consequently, it remains unknown whether the identified barriers also apply to younger people.
Due to the scoping approach taken, no quality assessment of the included studies was applied. When further analysing reasons for telemedicine non-use, this is a logical next step.
Among the major strengths of our paper is the broad range of telemedicine applications studied, which guarantees a concise picture of reasons for non-use and discontinued use. Also, the strict application of the four eye-principle to all methodological steps is bound to have minimized bias.
Conclusions
To the knowledge of the authors this is the first literature review about non-use and discontinued use of telemedicine interventions. The presented findings show that user related barriers such as attitude and technical literacy account for most barriers to use, followed by characteristics of the intervention itself such as inaccurate content or poor usability. Future research should consider the quality of the included studies and focus more on multimodal interventions for self-management.
Footnotes
Appendix
Categorization of barriers towards the use of telemedicine.

| Topic | Main category | Category | Sub-category | Example |
|---|---|---|---|---|
| Intervention (n = 201) | Usability | General | ‘Most patients encountered some kind of difficulty in using CONEMO’ 1 | |
| ‘Poor usability has led to incorrect recording and incorrect enzyme dose calculation’. 2 | ||||
| ‘It could be more user-friendly’ 2 | ||||
| ‘There was just too much trouble with it [the web page]. In the end, I just gave up trying. Had it only been easier. . .’ 3 | ||||
| ‘[Some participants] believed the device was complicated’. 4 | ||||
| ‘It is clear from our study that basics of website usability, such as [. . .] content delivery, are also barriers to portal use’. 5 | ||||
| ‘Most participants stated that [. . .] they did not use the website because it was not easy to use on their mobile phones’. 6 | ||||
| ‘This system looks a bit complicated. . .I think our main problem is that it may be difficult to operate’. 7 | ||||
| ‘Identified barriers against the use of health apps were [e.g.] poor usability’ 8 | ||||
| ‘Reasons for this [giving up on using physical activity apps] were [. . .] difficulty of use’ 9 | ||||
| ‘Participants reported few difficulties using home telehealth monitors’. 10 | ||||
| ‘One subject with COPD indicated difficulty in using the diaries’ 11 | ||||
| ‘Users thought they might stop using if [. . .] they find the tool hard to use’ 12 | ||||
| Problems with the uptake of the intervention | ‘[Some had difficulties to] enter [the] password to unlock [the] screen’. 1 | |||
| ‘Most patients [. . .] would have liked to receive more training’. 1 | ||||
| ‘They were confused by multiple passwords and the extra steps required for a HIPAA-secured login’. 13 | ||||
| ‘Rough on-boarding experience’ 14 | ||||
| ‘For participants, the early experience of learning to use a mobile medication management application was frustrating, overwhelming, and challenging’ 15 | ||||
| ‘Participants noted difficulty with using the long preassigned temporary passwords’ 16 | ||||
| ‘Installation of the equipment was the most common problem’ 17 | ||||
| ‘Participants also experienced [. . .] login problems’ 3 | ||||
| ‘[Participants] reported trouble logging in’ 18 | ||||
| ‘The major challenge experienced by participants was logging into the system’. 19 | ||||
| Lack of support | ‘Most patients [. . .] would have liked to receive more training’. 1 | |||
| ‘Half of the patients admitted that they did not know how to handle the technology in the beginning’ 1 | ||||
| ‘Reasons for not attempting enrolment [were] lack of information [. . .] [e.g. missing] instructions’ 20 | ||||
| ‘For participants, the early experience of learning to use a mobile medication management application was frustrating, overwhelming, and challenging’ 15 | ||||
| ‘Some individuals had more difficulty than others, and would likely need significant support, both technical and emotional, to adopt the application into their lives’. 15 | ||||
| ‘[They] described instances where medical history in the patient portal was outdated or incorrect which led to a sense of frustration, as it was not clear what action should be taken to correct it’ 21 | ||||
| ‘However, the purpose of these reflection sheets was described as difficult to understand’ 3 | ||||
| ‘Some patients stated that they still could not completely understand the functions and operating procedures of the telehealth devices’ 4 | ||||
| ‘Many participants needed more concrete support and/or technical assistance for portal use’
5
|
||||
| ‘[Participants] were not clear about what they needed to do each day’ 6 | ||||
| ‘Participants [. . .] felt that the points and badges had little meaning and it was not clear how points were earned’. 6 | ||||
| ‘Some of those who wanted to improve their lifestyle perceived a lack of advice about how to do this’ 22 | ||||
| ‘Portal nonusers mostly expressed concerns about [. . .] lack of support to navigate computers and/or the Internet’ 23 | ||||
| ‘Most comments highlighted concerns about [. . .] lack of technical support’ 23 | ||||
| ‘[Participants] reported [. . .] not knowing where to begin on the website once logged-in’ 18 | ||||
| ‘They were hampered by [. . .] unclear explanations of what data needed to be entered’. 24 ) | ||||
| ‘Other challenges included difficulty entering their patient information’. 19 | ||||
| ‘A few [nonusers] mentioned not having someone to show them how to use it’ 12 | ||||
| Technical problems | General | ‘Reasons for the nonadherence were [. . .] technical issues’ 25 | ||
| ‘Barriers to the use of telemedicine also included technical difficulties with the technology’ 26 | ||||
| ‘The most common were general problems with app functionality’ 27 | ||||
| ‘Patients [. . .] identified technical difficulties [. . .] as barriers’ 28 | ||||
| ‘Some described being irritated and frustrated by technological problems’. 3 | ||||
| ‘Participants identified technical issues that would impact their experiences’ 4 | ||||
| ‘one reported technical difficulties’ 29 | ||||
| ‘Technological [. . .] constraints posed barriers to conducting the discharge videoconference’ 30 | ||||
| ‘Some people [. . .] felt they would have difficulty engaging with the technological requirements of the equipment’ 31 | ||||
| ‘All six participants reported some level of technical difficulty with using the devices’ 32 | ||||
| ‘Patients experienced technical errors’ 33 | ||||
| ‘Both groups [. . .] [described] technical hiccups’ 34 | ||||
| Problems with connectivity | ‘There were some technological and connectivity problems, for example, people did not receive the SMS in time’. 1 | |||
| ‘Disconnection was experienced once’ 25 | ||||
| ‘About 8% reported connectivity obstacles’ 20 | ||||
| ‘Others experienced [. . .] poor or unreliable internet connections’ 26 | ||||
| ‘[One Participant] reported bad or slow internet connection’. 27 | ||||
| ‘More than once [. . .] [the] platform [. . .] lost its connection’ 35 | ||||
| ‘Barriers to mHealth use [were] technology connection problems in apartment building’ 36 | ||||
| ‘Infrastructure/hardware problems, including drop-out of rural Internet’ connections’ 37 | ||||
| ‘All six participants reported some level of technical difficulty with using the devices, particularly connecting the wireless scale’ 32 | ||||
| Synchronization problems | ‘More than once [. . .] [the] platform could not synch’
35
|
|||
| ‘[Participants] complained that their steps were not always syncing with the Fit After Baby app’ 6 | ||||
| Lack of access | ‘Accessibility issues’ 14 | |||
| ‘The most common were general problems [. . .] [like] accessing specific podcasts [. . .] or problems accessing any app content (i.e., could not engage with any podcast)’ 27 | ||||
| ‘The health data was not available at all for some users and only partly available for the remaining users’. 35 | ||||
| ‘Those who had some experience described poor features of the PHCC’s website with [. . .] difficulties to access important information’ 38 | ||||
| ‘[One] patient reported not having access to an operative report’ 39 | ||||
| ‘One patient was unable to access his medical record on one occasion’ 39 | ||||
| ‘One patient reported that he could not log onto the provider Web site and had to restart his computer to do so’. 39 | ||||
| ‘The provider Web site was not available for use on two occasions because the host server system was temporarily down’. 39 | ||||
| ‘Patients experienced [. . .] difficulty in reviewing previously entered open-text data’ 33 | ||||
| ‘The technical problems described by both groups [were e.g.] not being able to log on to group sessions’. 34 | ||||
| ‘The technical problems described by both groups [were e.g.] being locked out by the system’. 34 | ||||
| ‘Minor technical problems involved [. . .] not being able to see [. . .] homework assignments on the screen’ 34 | ||||
| Poor adaption to end devices | ‘MedApp was not compatible with all smartphones’. 25 | |||
| ‘Some (older) versions of operating systems were incompatible with FaceTalk’ 25 | ||||
| ‘One (10%, 1/10) participant was unable to use the device due to incompatibility with her mobile phone operating system’ 40 | ||||
| Others | ‘[Some had difficulties with] low battery duration’ 1 | |||
| ‘One participant could not manage to get sound’ 25 | ||||
| ‘More than once [. . .] [the] eWALL was very slow or froze’ 35 | ||||
| ‘The weighing procedure presented a problem for two patients, who had to stand on the scales for several minutes before the reading stabilized and the data were transferred’. 17 | ||||
| ‘Participants also experienced [. . .] alerts from the firewall that it was an insecure Web page (which it was not)’. 3 | ||||
| ‘Barriers to mHealth use [were] concern about battery dying’ 36 | ||||
| ‘Problem with equipment for example, equipment broken, no longer working’ 41 | ||||
| ‘Minor technical problems involved a slow system’ 34 | ||||
| Design | General | ‘Unattractive design’ 14 | ||
| ‘It is clear from our study that basics of website usability, such as simplicity in design [. . .] are also barriers to portal use’. 5 | ||||
| ‘One patient complained about the printer-friendly report layout’. 39 | ||||
| ‘Other patients reported dissatisfaction with the layout or design of the Web pages’. 39 | ||||
| ‘Frustration with design features’ 24 | ||||
| Structure and navigation | ‘Most difficulties were experienced when selecting a time and date for scheduling an activity by changing the numbers using up and down arrows’. 1 | |||
| ‘[Participants] particularly complained of the menu organization and structure. First of all, the menus lacked a hierarchical structure. Main menus and submenus were not properly linked each other. Second, menu content was cluttered and unclear’. 42 | ||||
| ‘The menu contents did not match with users’ mental models when they search the location of the particular information they needed. [. . .] Because of this, users were not able to intuitively find the proper pathways to the intended information’. 42 | ||||
| ‘They were also agitated by navigating from one area to another once inside the patient portal’ 13 | ||||
| ‘They were frustrated that the clinical summary was static, unlike other online documents that allowed you to hyperlink to other material for additional information’. 13 | ||||
| ‘Confusing interface’ 14 | ||||
| ‘Participants commonly struggled with going “back and forth”, essentially, moving forward to enter a medication into their profile and once completed, going back to enter a new medication’ 15 | ||||
| ‘Many first time users struggled with basic touchscreen features’ 15 | ||||
| ‘I didn’t know how to get from a certain screen to another’ 15 | ||||
| ‘Usability issues such as a non-intuitive interface [. . .] were all noted as barriers to technology use’ 43 | ||||
| ‘They described difficulties in navigating the Web page due to errors with the portal’ 3 | ||||
| ‘They were hampered by the need to navigate through multiple screens’ |
||||
| ‘Participants expressed concerns regarding [. . .] potentially confusing interfaces’ 44 | ||||
| ‘Patients were unable to locate different features on the tool’ 33 | ||||
| ‘Subjects with asthma mentioned [. . .] the format being too rigid [. . .] as reasons for not using self-management diaries’ 11 | ||||
| Comprehensibility | ‘[Some found the] volume too loud’ 1 | |||
| ‘Some preferred larger screens’ 45 | ||||
| ‘Another issue was legibility. In particular, the older adult group had a difficult time due to the bland graphics, poor color contrast, small letter size, and thin letters in the menu bar’. 42 | ||||
| ‘In every session, we observed at least one participant, often male, who could not hear the alarms going off’ 15 | ||||
| ‘Others experienced suboptimal image clarity’ 26 | ||||
| ‘Participants reported that they had difficulty [. . .] viewing the podcasts (e.g., too small on the screen)’ 27 | ||||
| ‘Participants reported that they had difficulty hearing the podcasts’ 27 | ||||
| Content | Framing | Language and comprehensibility | ‘Some participants had difficulty understanding the directions in the final Action Plan section of the website’. 46 | |
| ‘A small proportion of participants found the terms “life not worth living” and “worse than death” [. . .] to be challenging. Concerns about the language included that it was frightening; contradicted a belief that life was always worth living; and, invited thoughts of suicide, assisted suicide, or euthanasia. This small group found these phrases unacceptable and recommended changing them’. 46 | ||||
| ‘Patients commented on the differences in language, specifically the use of medical terminology and its translation into clear messages’. 26 | ||||
| ‘Usability issues such as a [. . .] the use of medical terminology were all noted as barriers to technology use’ 43 | ||||
| ‘Perceiving the content as [. . .] incomprehensible’ 3 | ||||
| ‘Four participants described the academic style of information delivery in the webinar as off-putting’ 29 | ||||
| ‘[One] respondent [. . .] explained his decision to decline the trial as being due to a [. . .] lack of confidence with language’ 31 | ||||
| Personalisation | ‘Some participants noted a lack of diversity in terms of age (mostly seniors are depicted) and Canadian culture (e.g., lack of Aboriginal representation)’. 46 | |||
| ‘Overall lack of personalization’ 14 | ||||
| ‘Some also expressed a sense of alienation resulting from the videoconference. The specialist was described as distant and very far away. Overall these patients felt that they had not been seen’ 47 | ||||
| ‘Some participants [. . .] felt the portal lacked individualized information’ 21 | ||||
| ‘Another point to consider is that all participants expressed a lack of specificity and adaptability to SCD particularities in the usual health apps (i.e., normal values for people with SCD are the values indicating a disease in healthy people)’. 48 | ||||
| ‘Some participants did not see the content of the GSD as tailored to their needs and expectations for a diabetes self-management intervention’ 3 | ||||
| ‘They [. . .] could not familiarize themselves with these issues’ 3 | ||||
| ‘They expressed that they lost interest after reading some of the first issues raised in the reflection sheets because they could not familiarize themselves with these issues and did not consider the content relevant to their diabetes’ 3 | ||||
| ‘Infrequent negative experiences were [. . .] feeling unable to relate to the actor in the videos’ 29 | ||||
| ‘Some participants found it difficult to relate to the depiction of a woman living well with BD (Bipolar Disorder) in the videos, resulting in a sense of discouragement or frustration’ 29 | ||||
| ‘Others mentioned that the information in the coaching sessions should be more individualized’ 6 | ||||
| ‘They expressed that women who look like thin models did not reflect what it was like to be a postpartum mom struggling to lose weight’ 6 | ||||
| ‘Portal nonusers expressed concerns about [. . .] lack of personalization’ 23 | ||||
| ‘Communicating with a doctor using technology was perceived as superficial and impersonal’ 49 | ||||
| ‘Participants [perceived a] sense of alienation from such technologies’ 31 | ||||
| ‘Lack of empathy and trust’ 50 | ||||
| ‘[Perceived] disadvantages [were] [. . .] low credibility’ 50 | ||||
| Information | False or inaccurate information | ‘However, most of the patients felt that this [the virtual patient support group] was not useful. Reasons included not wanting to be [. . .] misled by false information’ 45 | ||
| ‘Medication compliance was not correctly reported’. 25 | ||||
| ‘Calculation raised confusion when the recommended dose differed significantly from the usual dose’. 2 | ||||
| ‘We got such a weird advice [. . .] And then it turned out that they did something wrong’ 2 | ||||
| ‘Poor usability has led to incorrect recording and incorrect enzyme dose calculation’. 2 | ||||
| ‘Unrealistic promises’ 14 | ||||
| ‘False information’ 14 | ||||
| ‘Inaccurate measurements’ 14 | ||||
| ‘Approximately 25% of respondents felt that their medical history was not entirely accurate’ 16 | ||||
| ‘Patients reported that outdated prescriptions continued to appear in the EHR as active’ 16 | ||||
| ‘More than once [. . .] domotics measurements were incorrect or did not work’
35
|
||||
| ‘[They] also described instances where medical history in the patient portal was outdated or incorrect which led to a sense of frustration’ 21 | ||||
| ‘Some patients pointed out they did not know whether or not the results of the measurements were accurate’ 4 | ||||
| ‘If the machine frequently failed, patients would doubt the reliability of the measurement’ 4 | ||||
| ‘1 patient [. . .] reported an incorrect psa value in his psa monitoring tool’ 39 | ||||
| ‘Several participants pointed to past experiences with medical instruments to take routine measurements (such as blood pressure devices), which had been inaccurate’. 7 | ||||
| ‘Three participants who withdrew from the trial after they had received the equipment, described [. . .] false alarms due to faulty readings’ 31 | ||||
| ‘Questions often did not appear at the correct times or days’ 33 | ||||
| ‘Incorrect information’ 50 | ||||
| Missing information | ‘Approximately one-third of respondents felt that the personal health information contained in their EHR was not complete’ 16 | |||
| ‘[Some stated that [. . .] eWALL lacked actionable advice on this matter (two times)’ 35 | ||||
| ‘Some found the brevity of the videos limited the amount of useful information conveyed’ 29 | ||||
| ‘Some patients in the depression trial described the intervention as too superficial’ 22 | ||||
| Information frequency | ‘Constant notifications or reminders [were perceived as barriers to the adoption]’ 14 | |||
| ‘Participants expressed feeling overwhelmed by the amount of information being presented all at once’. 15 | ||||
| ‘Several participants stated that information overload would demotivate them for long-term engagement’ 48 | ||||
| ‘Finally, some participants noted that, beyond basic functionality, the website content could also be challenging [. . .] [i.e.] “it’s a lot of reading and it’s overwhelming”’ 5 | ||||
| ‘He went on to explain that he did not want attention focused on his health problems and his aversion to receiving too much information about medical matters’ 31 | ||||
| ‘Some study participants noted that the most negative aspect of monitoring was the repetition of questions perceived to be irrelevant or unchanging over time’. 10 | ||||
| Annoying content | ‘I would find that annoying, yeah [push notification suggesting exercise]’ 51 | |||
| ‘Reminders to upgrade app versions for greater functionality were deemed annoying’ 51 | ||||
| ‘[Some were] bothered by questions about depression’ 1 | ||||
| ‘[Some did not like] repetitive sessions’ 1 | ||||
| ‘Obvious or excessive advertising’ 14 | ||||
| ‘Two participants were rather negative. They found the information nothing new (one time) or dull (one time)’. 35 | ||||
| ‘Most of the participants with ARI (age-related impairments) found the physical rehabilitation training too easy to do and quickly gave up, due to the lack of challenge’ 35 | ||||
| ‘They found their content quite meaningless and irritating’. 35 | ||||
| ‘Other factors that diminished their motivation pertained to perceiving the content as irrelevant’ 3 | ||||
| ‘Portal content is often too complex’ 5 | ||||
| ‘He went on to explain that he did not want attention focused on his health problems and his aversion to receiving too much information about medical matters’ 31 | ||||
| ‘Some study participants noted that the most negative aspect of monitoring was the repetition of questions perceived to be irrelevant or unchanging over time’. 10 | ||||
| ‘Minor technical problems involved [. . .] double messaging occurring’. 34 | ||||
| Missing or insufficient functions | ‘Limitation about fitness-tracking apps not recognizing certain activities was also mentioned by another participant’ 51 | |||
| ‘One of the other major issues mentioned [. . .] was the poor help function and limited search capability’. 42 | ||||
| ‘Problems with notifications were experienced, where no notifications would show for new messages. In addition, typing messages had a delay for one participant and concept messages were not saved when closing the app’. 25 | ||||
| ‘Scanning medication did not work properly’. 25 | ||||
| ‘The BPM occasionally reported an error, which indicated a measurement could not be completed after which the participant had to try again’. 25 | ||||
| ‘Limited applications’ 52 | ||||
| ‘Other reasons for individual concern included [. . .]the lack of a support group’ 53 | ||||
| ‘Some patients lacked the possibility to send messages’ 2 | ||||
| ‘A [. . .] participant’s tracker stopped working’ 40 | ||||
| ‘Some participants expressed frustration that the tracker didn’t register activities such as yoga, standing, or the use of some exercise machines’. 40 | ||||
| ‘Many participants deplored the absence of mechanisms to easily access and control the quality of information’. 48 | ||||
| ‘I answered the questions and tried to send, but it did not send. I tried several times, and I could not do it’. 3 | ||||
| ‘Participants also experienced [. . .] that the nurse had not received the messages they sent’. 3 | ||||
| ‘When I went to the website, I was trying to sign in to all the process but for some reason it didn’t work’. 5 | ||||
| ‘Those who had some experience described poor features of the PHCC’s website with lack of functions’ 38 | ||||
| ‘One patient reported problems with requesting an appointment’. 39 | ||||
| ‘Patients later reported [. . .] experiencing errors with the portal’ 33 | ||||
| ‘One-time training was not considered to be sufficient’ 33 | ||||
| ‘Reasons for this [giving up on using physical activity apps] were insufficient function [. . .]’ 9 | ||||
| ‘Subjects in this study indicated that the format of the self-management diaries was too rigid (e.g., no open space to write comments and observations)’ 11 | ||||
| ‘Minor technical problems involved [. . .] not being able to see when someone was typing’ 34 | ||||
| Context of use (n = 181) | Costs | ‘Patients are not willing to pay extra costs for this digital tool’ 54 | ||
| ‘The most important barriers to completing the outside-app activities were [. . .] economic constraints’. 1 | ||||
| ‘Costs also contributed to the patients’ unwillingness to use an e-tool’. 45 | ||||
| ‘For many, the cost of the trackers was an impediment to purchase’ 40 | ||||
| ‘Digital solutions are of no use to me, they only increase the cost of medicines’. 55 | ||||
| ‘Costly’ 56 | ||||
| ‘One patient commented on the cost of the daily telephone call which was necessary to transmit the weight data. Although the daily rate was small, the monitoring cost was presented on his quarterly bill as a single total of just over ninety calls’. 17 | ||||
| ‘It is not possible to charge for the service’ 4 | ||||
| ‘Other risks that they talked about were increased costs’ 38 | ||||
| ‘Barriers to mHealth use [were] cost’ 36 | ||||
| ‘Financial [aspects] [. . .] posed barriers to conducting the discharge videoconference’ 30 | ||||
| ‘Reasons for this [giving up on using physical activity apps] were [. . .] extra cost’ 9 | ||||
| Data security | ‘Concerns were raised around access to those data by health insurers’. 51 | |||
| ‘Patients [. . .] have concerns about the privacy and safety of digital care’. 54 | ||||
| ‘Concerning difficulties using the smartphone itself, patients mostly mentioned the fear of getting it stolen’. 1 | ||||
| ‘Some expressed concerns over confidentiality and privacy with a linked system’
45
|
||||
| ‘They expressed concerns over privacy, not wanting to have medical information and social security numbers up on the web’ 13 | ||||
| ‘[Concerns about] security and confidentiality’. 25 | ||||
| ‘Apps require substantial data storage’ 25 | ||||
| ‘There were privacy concerns’ 52 | ||||
| ‘Reasons for concern were given by a small number of respondents (15/111, 13.5%), with privacy and security most common’ 53 | ||||
| ‘Data ownership and access by third parties’ 14 | ||||
| ‘Security concerns [was a] commonly cited barriers to enrollment’
20
|
||||
| ‘[30% expressed some concern] about the confidentiality and security of their online medical information’ 16 | ||||
| ‘Not private’
56
|
||||
| ‘Those surveyed were particularly worried about data protection’ 57 | ||||
| ‘Roughly every fifth participant did not want their doctors to save or process their individual health related data on a mobile device’ 57 | ||||
| ‘Fears about personal health data security risks were shared in every focus group’. 21 | ||||
| ‘Privacy issues were also a fundamental concern for most interviewees. Many feared to lose control on their data’. 48 | ||||
| ‘Patients [. . .] identified [. . .] privacy concerns[. . .] as barriers’ 28 | ||||
| ‘Concerns were data usage, storage [and] transfer’ 58 | ||||
| ‘Usability issues such as [. . .] lack of data protection standards were all noted as barriers to technology use’ 43 | ||||
| ‘[They were] concerned about the security/privacy of their information online’ 5 | ||||
| ‘[One main topic] were concerns about privacy of medical records’ 59 | ||||
| ‘Barriers to mHealth use [were] concerns about privacy’ 36 | ||||
| ‘Portal nonusers expressed concerns about online data security’ 23 | ||||
| ‘Participants expressed some concerns about [. . .] confidentiality’ 7 | ||||
| ‘Identified barriers against the use of health apps were [e.g.] data privacy concerns’ 8 | ||||
| ‘No longer wishes to share data’ 41 | ||||
| ‘Participants expressed concerns regarding privacy and data security’ 44 | ||||
| ‘Reasons for this [giving up on using physical activity apps] were [. . .] security [issues]’ 9 | ||||
| ‘Participants expressed concern about the amount of information they needed to hey needed to input into the CRCS-PHR (Colorectal Cancer Survivor’s Personal Health Record) such as information about provider visits and treatments’. 19 | ||||
| ‘[Perceived] disadvantages [were] [. . .] computer literacy/safety concerns’ 50 | ||||
| ‘Negative aspects of telemonitoring [were] data misuse, device manipulation, mistransfer’ 60 | ||||
| ‘Users thought they might stop using if [. . .] they become concerned with lost data or their privacy’ 12 | ||||
| ‘Some [non-users] are concerned about Internet privacy/security’ 12 | ||||
| Organisation | Lack of time | ‘Reasons given for not using the progress tracker via the website included [. . .] no time’ 61 | ||
| ‘Time [. . .] constraints were also important barriers to doing activities’. 1 | ||||
| ‘Lack of time [. . .] also contributed to the patients’ unwillingness to use an e-tool’. 45 | ||||
| ‘Limited time’ 2 | ||||
| ‘Willingness to persevere [. . .] only for 15 min due to lack of time’ 15 | ||||
| ‘No time for it’ 56 | ||||
| ‘Lack of time’ 17 | ||||
| Compatibility with everyday life | ‘[One of] the main reasons for non-participation [. . .] [was being] too busy, [. . .] work commitments, personal issues [and] travelling ‘
61
|
|||
| ‘Other difficulties mentioned were [. . .] sudden changes in their plans because of external factors (14% of 14), for example, receiving a phone call or someone else needing assistance’. 1 | ||||
| ‘Those who were working long hours prioritized rest over the use of an e-tool’. 45 | ||||
| ‘No priority’ 25 | ||||
| ‘The fourth most common reason for declining was being too busy’ 62 | ||||
| ‘Some decliners provided other related reasons such as not having space in their life to participate in a trial’ 62 | ||||
| ‘[Too] busy’ 20 | ||||
| ‘Participants noted external factors that influenced their tracker use or their ability to incorporate fitness in their lives [. . .] [i.e.] the constraints of jobs and retirement [. . .]’ 40 | ||||
| ‘A third had trouble fitting exercise into her schedule when a family member was hospitalized’ 40 | ||||
| ‘Smartphone use is limited to emergency cases only’ 55 | ||||
| ‘Participants [. . .] [had] more important priorities in their lives than the GSD (Guided Self-Determination) eHealth intervention. Examples were other illnesses that needed more attention and other personal or work-related responsibilities’. 3 | ||||
| ‘Other factors that diminished their motivation pertained to choosing other activities and perspectives in their lives’ 3 | ||||
| ‘Several participants expressed how difficult it was to track dietary intake while taking care of an infant’ 6 | ||||
| ‘These younger patients with depression were [. . .] too busy due to childcare and employment to engage with key aspects of the intervention such as the telephone calls and homework for the cognitive behavioural therapy’. 22 | ||||
| ‘Some interviewees from the depression trial described serious ongoing life events such as the threat of losing disability and unemployment benefits, physical illnesses or coping with family members and friends who were very ill or depressed. These issues caused stress on top of the depression, making engagement with the intervention difficult’. 22 | ||||
| ‘The most important reasons [for refusing participation] were being too busy’ 63 | ||||
| ‘Portal nonusers expressed [. . .] lack of resources’ 23 | ||||
| ‘A respondent talks about how the intervention would increase his dependence on his wife who would be required to help him’ 31 | ||||
| ‘Participants also found that they forgot to do their monitoring when managing acute health issues or other life stresses’ 33 | ||||
| Forgetful-ness | ‘Reasons given for not using the progress tracker via the website included [. . .] [that some] forgot to use it’ 61 | |||
| ‘Respondents did not remember discussing the patient portal with their providers’ 20 | ||||
| ‘I’m very forgetful with passwords’. 5 | ||||
| ‘Two patients forgot their password, and one forgot the Web site address’. 39 | ||||
| ‘Patients later reported forgetting that there was a portal’ 33 | ||||
| ‘Subjects with asthma mentioned [. . .] forgetfulness as reasons for not using self- management diaries’ 11 | ||||
| Lack of trust | ‘Key identified barriers in the implementation and adoption of eHealth interventions included concerns about [. . .] reliability [of provided information]’ 54 | |||
| ‘Most of the participants were not comfortable to accept strangers as “friends” in the system’. 52 | ||||
| ‘Other reasons for individual concern included accuracy of information’ 53 | ||||
| ‘[Some were] worried [. . .] about the technical reliability’ 57 | ||||
| ‘[They] worried about equipment breakdown and its reliability’ 4 | ||||
| ‘Users doubted its quality’. 4 | ||||
| ‘Insecurity with e-health in emergency situations’ 38 | ||||
| ‘Reluctance to rely on a machine’ 36 | ||||
| ‘Concerned about whether healthcare provider will receive information generated by device’ 36 | ||||
| ‘Barriers to mHealth use [were] concern about functional limitations’ 36 | ||||
| ‘Barriers to mHealth use [were] concern about device malfunction’ 36 | ||||
| ‘Participants expressed some concerns about [. . .] equipment reliability’ 7 | ||||
| ‘Participants expressed some concerns about [. . .] adequate HTMS (Home Telecare Management System) technical support’ 7 | ||||
| ‘Identified barriers against the use of health apps were [e.g.] a lack of trust’ 8 | ||||
| ‘Lack of [. . .] trust’ 50 | ||||
| Negative experiences | Loss of personal contact with providers | ‘Disruption of the health care provider-patient relationship’ 14 | ||
| ‘Patients [. . .] articulated some unease about the lack of physical contact and hands-on interaction’ 26 | ||||
| ‘Patients focused on issues of non-verbal communication and personal “connection” or the need to develop a relationship between the patient and the provider’ 26 | ||||
| ‘Patients’ desire to be directly examined by doctor was the major reason for their lack of willingness to use e-mail’ 56 | ||||
| ‘Patients were disappointed that the telemonitoring had not led to an increase in nurse contact’ 17 | ||||
| ‘Patients [. . .] identified [. . .] the inability to perform a physical examination [. . .] as barriers’ 28 | ||||
| ‘The GSD eHealth intervention without face-to-face encounters influenced the participants’ motivation for the intervention negatively and resulted in dropout’. 3 | ||||
| ‘These respondents considered the family member they cared for to be in need of a level of human care and supervision that was impossible to provide via telehealth and telecare equipment’. 31 | ||||
| ‘Lack of face-to-face contact with a therapist’ 50 | ||||
| Impaired communication | ‘[Some disliked that there received] too few phone calls’ 1 | |||
| ‘Four participants of the study expressed disappointment that their friend requests were not responded to’ 52 | ||||
| ‘A small number of patients had to wait for times ranging from 10 min to half an hour for the consultant to arrive’ 47 | ||||
| ‘One patient [. . .] stated that they had been excluded from the consultation’. 47 | ||||
| ‘In contrast to patients who thought they could ask all the questions they wanted, others felt constrained’. 47 | ||||
| ‘Nobody seemed to bother’. 17 | ||||
| ‘Monitoring “wellness” was not valued because they received no individual feedback’ 17 | ||||
| ‘[Participants described an] experience of lack of dialogue’ 3 | ||||
| ‘Communicating with a doctor using technology was perceived as superficial and impersonal’ 49 | ||||
| ‘They described the response to some of these problems as being “slow” and “frustrating”’ 31 | ||||
| ‘Lack of instant feedback’ 50 | ||||
| ‘[perceived] disadvantages [were] [. . .] impoverished communication’ 50 | ||||
| ‘Absence of body language’ 50 | ||||
| ‘Difficulties expressing oneself’ 50 | ||||
| No perceived benefit | ‘Two [people] did not feel that CONEMO improved their psychological health’. 1 | |||
| ‘Two people (7%) thought that the time of the intervention was not sufficient to accomplish groundbreaking improvements’ 1 | ||||
| ‘Solution does not fit the needs of users’ 14 | ||||
| ‘[Some] stated that eWALL could not influence their behavior (Four times)’ 35 | ||||
| ‘Most participants stated that the website was not useful’ 6 | ||||
| ‘Subjects with asthma mentioned not perceiving an added value [. . .] as reasons for not using self-management diaries’ 11 | ||||
| Psychological burden | ‘One participant reported anxiety because of the frequency of blood pressure measurements’. 25 | |||
| ‘They appeared to feel vulnerable or lost and often worried about making a mistake’ 15 | ||||
| ‘Constant monitoring promotes the feeling of sickness’ 55 | ||||
| ‘The most common negative sentiment among participants [. . .] was [. . .] feeling pressured to adopt new communication methods’ 21 | ||||
| ‘Many [were] afraid of making a mistake’ 21 | ||||
| ‘In either case, they experienced anxiety and frustration’. 21 | ||||
| ‘Many [. . .] felt stigmatized by their lack of knowledge’ 21 | ||||
| ‘Being uncomfortable with the issues raised in the reflection sheets or feeling pathologized by the demanding questions were articulated’. 3 | ||||
| ‘[A] common reason for refusal to participate [. . .] [was] anxiety’ 64 | ||||
| ‘Two respondents who withdrew from the trial described how the service changes they experienced caused additional stress’. 31 | ||||
| ‘A third participant dropped out of the study after 2 weeks due to increased anxiety associated with the need to report on her health and using the mobile device’ 33 | ||||
| Too high effort | ‘Communication requires signing in’ 25 | |||
| ‘Sorting out calories values for foods seems a lot of trouble’ 52 | ||||
| ‘Yes, the app comes with extra workload. You have to do extra steps to calculate’. 2 | ||||
| ‘Participants [. . .] shared experiences where they felt burdened by the task of circulating the most current health information even though all health care providers had access to the same electronic health record’. 21 | ||||
| ‘They [. . .] perceived the Web solution as time-consuming and tiring’ 3 | ||||
| ‘Participants stated that it was cumbersome to download and save the PDFs before filling out the reflection sheets’. 3 | ||||
| ‘Participants expressed some frustration with tracking of dietary intake’ 6 | ||||
| ‘Barriers to mHealth use [were being] unwilling to wear a monitor’ 36 | ||||
| ‘The last barrier was the required time and effort to use the apps for self-monitoring’. 65 | ||||
| ‘[Portal users expressed] concerns about [. . .] the cumbersome nature of logging into portal accounts (e.g., remembering passwords, multiple accounts for patients in the same household)’ 23 | ||||
| ‘20% (12/59) thought it was difficult to obtain step count feedback from the pedometer’ 18 | ||||
| ‘36% (21/59) had difficulty uploading their step count data to the website’ 18 | ||||
| ‘The requirements to conduct daily monitoring were “too time consuming”’ 31 | ||||
| ‘The requirements to conduct daily monitoring were “too [. . .] frustrating”’ 31 | ||||
| ‘Interview results highlighted the burden participants felt by the number of devices’ 32 | ||||
| ‘Participants found that data entry became a tedious task’ 33 | ||||
| ‘They did emphasise that they did not want additional equipment for the data transfer’ 60 | ||||
| Others | ‘[Some disliked the] high liability using borrowed phone’ 1 | |||
| ‘Find it annoying to use’ 56 | ||||
| ‘Don’t like to use’ 56 | ||||
| ‘Think it is uncomfortable’ 56 | ||||
| ‘The participants with some experience of e-health described unmet expectations’ 38 | ||||
| ‘Some patients reported feeling isolated with the mobile device’ 33 | ||||
| ‘[Perceived] disadvantages [were] anonymity’ 50 | ||||
| ‘Less effective’ 50 | ||||
| Lack of Information | ‘Unclear purpose’ 14 | |||
| ‘Participants who did not attempt to enrol in the patient portal [. . .] stated reasons related to lack of information’ 20 | ||||
| ‘Moreover, some of the participants stated that they did not fully understand what the intervention entailed when they signed up for it’. 3 | ||||
| ‘Many of the participants were not aware that these tools were available and the barrier is the information gap’ 65 | ||||
| ‘Some patients did not understand what the intervention entailed when they signed up to join the trial’ 22 | ||||
| ‘Eight did not understand the intervention and why they were being offered to join’ 31 | ||||
| ‘Non-users reported that they had never heard of them [health management tools]’ 12 | ||||
| ‘Other prominent factors included [. . .] not knowing what benefits the tools provide’ 12 | ||||
| External factors | ‘Patients from deprived general practices were more likely to decline compared with patients from affluent general practices’ 62 | |||
| ‘Many participants expressed choice confusion due to the number of brands, models, and [of activity trackers] on the market’ 40 | ||||
| ‘Participants noted external factors that influenced their tracker use or their ability to incorporate fitness in their lives. Weather was cited by a number of participants’ 40 | ||||
| ‘Access to technologies should be actively provided to patients, accessibility is seen as a problem by patients’ 55 | ||||
| ‘Doctor far away’ 56 | ||||
| ‘There was insufficient room for two sets of scales in their home’ 17 | ||||
| ‘Some participants also felt the coach check-in should not be the responsibility of the participant but should rather be initiated by the coach’ 6 | ||||
| ‘The main issue that the participants talked about was that there was “Poor communication between health care organizations” IT systems’. As no organization was fully updated with all the information, the participants expressed “disappointment over poor IT systems” thus leading to low confidence in the EMR, which in turn led to a greater mistrust in e-health solutions’ 38 | ||||
| ‘No primary care physician [were a barrier to mHealth use]’ 36 | ||||
| ‘Some participants did not use any tools for self-management because their doctor did not ask them to’. 65 | ||||
| ‘Portal user noted [. . .] variations in provider availability for online appointment scheduling and response times to medical messages’. 23 | ||||
| ‘The home monitor’s reliance on standard telephone lines meant that individuals without landlines (nearly one-quarter of US households and growing annually) were unable to benefit from the service’. 10 | ||||
| ‘Other prominent factors [for non-use] included their doctors not offering an online service’ 12 | ||||
| User (n = 289) | Personal factors | Socio-demo-graphic criteria | Gender | ‘Generally women [. . .] showed less intention to use e-health’ 66 |
| ‘In the CVD risk trial, females (83%, n = 1675) were more likely to decline than males (78%, n = 4357 males)’ 62 | ||||
| ‘In the depression trial males (86%, n = 4570) were more likely to decline than females (84%, n = 9419)’ 62 | ||||
| ‘Male patients were significantly less likely to use text messages’ 56 | ||||
| ‘More men withdrew than women’ 3 | ||||
| Age | ‘Respondents in the older age categories showed less intention to use e-Health’ 66 | |||
| ‘Those in the under 50 years group [were less likely to stated that they would find it useful to have access to support programs and assistance with health problems through the Internet]’ 53 | ||||
| ‘Those in the [. . .] older 60 years group [were less likely to state that they would find it useful to have access to support programs and assistance with health problems through the Internet]’ 53 | ||||
| ‘There was a statistically significant difference, with decliners being younger than acceptors’ 62 | ||||
| ‘Participants were less likely to start [a] Web-based [intervention] with higher age’ 67 | ||||
| ‘Variables [. . .] associated with decreased likelihood of consent [were] increasing age’
64
|
||||
| ‘Respondents aged 70 and older were also less likely to be interested in eHealth than those below age 70’ 59 | ||||
| ‘Similar to other interview respondents, he also seemed surprised to be offered the intervention and stated “we’re [referring to himself and his wife] not old enough are we?”’ 31 | ||||
| Education | ‘People with lower level of education had less intention to using e-Health’ 66 | |||
| ‘Respondents with less formal education (i.e., those who did not finish high school) had more difficulty understanding medical information and test results than did high school graduates’ 16 | ||||
| ‘Results revealed that patients with primary education (OR = 0.403, 95% CI = 0.220–0.738, p = 0.003) and secondary education (OR = 0.323, 95% CI = 0.178–0.587, p < 0.001) were significantly less likely to use email to interact with specialist as compared to patients with tertiary education’. 56 | ||||
| ‘Patients with primary education were also significantly less likely to use text messages’ 56 | ||||
| ‘Factors [like] lower academic attainment [. . .] have been reported as reasons to refuse’ 41 | ||||
| Others | ‘Those from higher socioeconomic areas were less likely to respond positively to finding benefit from online support and information’ 53 | |||
| ‘Patients from BME groups (Black and Minority Ethnicity) were more likely to decline than white patients’ 62 | ||||
| ‘I’ve had enough to do in my professional life with digital things, in my retirement I have no interest in it anymore’ 55 | ||||
| State of health | High disease burden | ‘[One of] the main reasons for non-participation [. . .] were [. . .] health issues’ 61 | ||
| ‘One [patient] [. . .]felt that his health status was too compromised to follow all of the instructions’. 1 | ||||
| ‘Too sick at the time’ 20 | ||||
| ‘Feeling overwhelmed with respect to their health issues’
68
|
||||
| ‘A number of patients declined because of poor physical health, including issues such as co-morbidities [and] feeling too unwell’. 64 | ||||
| ‘I’m too sick’ 63 | ||||
| ‘Barriers to mHealth use [were] health problems [being] too complex’ 36 | ||||
| ‘Factors [like] having diabetes, have been reported as reasons to refuse’ 41 | ||||
| ‘Eight stated that they (or the person they cared for) were too ill or incapacitated’ |
||||
| ‘the degree of illness severity affected performance’ 37 | ||||
| Low disease burden | ‘[One of] the main reasons for non-participation [. . .] [was [that people] perceived their health to be good’ 61 | |||
| ‘However, most of the patients felt that this (the virtual patient support group) was not useful. Reasons included [. . .] feeling that their condition was not serious enough to warrant such a group’ 45 | ||||
| ‘[Participants had the] perception that their condition was not sufficiently advanced or serious enough to require these services’ 68 | ||||
| ‘Other reasons expressed by subjects with COPD included [. . .] not experiencing a disease burden (and therefore forgetting about the diaries)’ 11 | ||||
| Physical limitation of use | ‘The main barrier reported to performing the activities suggested by CONEMO was the users’ health status (36% of 14), such as limited mobility or memory problems’. 1 | |||
| ‘Active decliners also specified that they were not participating because they did not like the telehealth intervention [. . .] because of communication difficulties, such as a visual impairment, which meant that engagement in a telehealth intervention was problematic’ 62 | ||||
| ‘Participants were less likely to start Web-based with [. . .] higher fatigue’ 67 | ||||
| ‘One individual stopped walking due to a fall’ 40 | ||||
| ‘[They] described ‘The aging body as a barrier’ with impaired practical abilities such as trembling fingers or impaired vision or hearing’. 38 | ||||
| ‘I’m physically incapable’ 63 | ||||
| ‘Physical barriers to use included small-sized phone screens and poor eyesight’. 37 | ||||
| ‘Participants expressed concerns regarding [. . .] accessibility (visual or motor impairment issues affecting the use of smartphone and tablets)’ 44 | ||||
| Lack of psychological resources | ‘Some decliners provided other related reasons such as [. . .] not having the emotional capacity to participate’ 62 | |||
| ‘Patients with depression [were] more likely not to accept’ 62 | ||||
| ‘Participants were less likely to start Web-based with [. . .] higher fatigue’ 67 | ||||
| ‘Concern about ability to cope was the second most common reason [for refusal to participate]’ 64 | ||||
| ‘[A] common reason for refusal to participate [. . .] [was] anxiety’. 64 | ||||
| Limited perceived vulnerability | ‘Reasons for the nonadherence were [. . .] when the blood pressure was deemed less relevant for their situation’. 25 | |||
| ‘[One participant did not think that] being aware of health status is fun’ 25 | ||||
| ‘Some patients had a limited understanding of their diagnosis’ 68 | ||||
| ‘No need to fix what wasn’t broken’ 38 | ||||
| ‘Other reasons expressed by subjects with COPD included no acknowledgment of the disease’ 11 | ||||
| Others | ‘The main barrier reported to performing the activities suggested by CONEMO was the users’ health status (36% of 14), such as limited mobility or memory problems’. 1 | |||
| ‘A small number of people also declined because [. . .] they were currently receiving treatment for other health conditions (3.4%, n = 245)’. 62 | ||||
| ‘Those who were post treatment for a longer time were less likely to use Web-based intervention materials’ 67 | ||||
| ‘Patients who occasionally (OR = 0.269, 95% CI = 0.144–0.504, p < 0.001) or daily smoke (OR = 0.480, 95% CI = 0.305–0.755, p = 0.002) were significantly less likely to use text messages as compared to those who never smoke’. 56 | ||||
| ‘Patients who occasionally smoke were also significantly less likely to use video conference’ 56 | ||||
| ‘The criteria that was on there (information letter), in my view I didn’t qualify’. 68 | ||||
| ‘Also, the median duration of diabetes was 9 years for those who dropped out and only 2 years for those who completed the intervention’. 3 | ||||
| ‘Variables [. . .] associated with decreased likelihood of consent [. . .] [were] being on inhaled steroid medication’ 64 | ||||
| ‘Participants on five or more medications were significantly less likely to express interest in eHealth than those on less than five medications’ 59 | ||||
| ‘Barriers to mHealth use [were] forgetfulness/memory problems’ 36 | ||||
| Expectation of self-efficacy | ‘Negative attitude generally, did not feel they can make a difference’ 45 | |||
| ‘Some of the elderly patients expressed mistrust in their own capabilities’ 38 | ||||
| ‘They described [. . .] the elderly’s own insecurity with the digital tools and difficulties to learn new things’. 38 | ||||
| ‘Barriers to mHealth use [were] concern about learning to use technology’ 36 | ||||
| ‘Some participants believed it would be too difficult for elderly people to learn’ 7 | ||||
| ‘Identified barriers against the use of health apps were [e.g.] lack of self-confidence’ 8 | ||||
| ‘Some people [. . .] felt they would have difficulty engaging with the technological requirements of the equipment’ 31 | ||||
| ‘She was not at all certain she wanted to take part because she did not think she would know how to use it’ 31 | ||||
| ‘[Participants had] doubts about their capacity to engage with what they understood to be the operational requirements of the equipment’. 31 | ||||
| Technical literacy | ‘Another obstacle for end-users is a lack of digital skills to work with mHealth solutions. Particularly, older generations may experience difficulties in using mHealth technologies as they need to switch to a new way of working’. 69 | |||
| ‘Reasons given for not using the progress tracker via the website included [. . .] not [being] confident with computers’ 61 | ||||
| ‘Some people did not know how to open the SMS or could only read them with the help of others’ 1 | ||||
| ‘[Some had difficulties to] answer incoming calls’ 1 | ||||
| ‘[Some had difficulties to] switch [their] phone on/off’ 1 | ||||
| ‘Many people experienced difficulties with the interactive tools used in this intervention, such as SMS, Android notifications, and dialogue pop-ups’ 1 | ||||
| ‘Mostly reluctant to use as unfamiliar with technology’ 45 | ||||
| ‘Some mentioned that [. . .] they do not know how to use the internet’. 45 | ||||
| ‘Most of them expressed an unwillingness to use the tool [. . .] largely because of unfamiliarity with technology’. 45 | ||||
| ‘Some did not own a computer nor possess the interest in learning how to use one, stating “I don’t do computer things, I’m a dinosaur”’. 13 | ||||
| ‘Another participant could not accomplish to switch to the front camera’ 25 | ||||
| ‘Other reasons for individual concern included [. . .] [little] computer literacy’ 53 | ||||
| ‘Telehealth-related reasons, in terms of no computer confidence [. . .] were prominent pre-specified reasons’ 62 | ||||
| ‘Lack of computer skills’ 20 | ||||
| ‘Many first time users struggled with basic touchscreen features’ 15 | ||||
| ‘I didn’t know how to get from a certain screen to another’ 15 | ||||
| ‘Don’t know how to use [information technologies]’ 56 | ||||
| ‘Many [. . .] participants noted that they had no computer training as part of their job and retired before computers were a regular part of the working environment’. 21 | ||||
| ‘Unfamiliarity with the use of text message and video conference was cited as the main reason for patients’ reluctance to use these information technologies’ 21 | ||||
| ‘One participant expressed that some elders may not be comfortable with the video technology’ 28 | ||||
| ‘The main reason is I don’t do the Internet. That was, the main thing’ 68 | ||||
| ‘Four participants expressed concerns about the level of technological skill required for telehealth’ 68 | ||||
| ‘Participants identified that they lacked basic computer literacy skills and that these deficits deterred them from participating in the telehealth trial’ 68 | ||||
| ‘Patients lacked the skills [. . .] to do a search’ 58 | ||||
| ‘Users were concerned about the utility of the service, because they were unfamiliar with the operating procedures’ 4 | ||||
| ‘Not technically savvy’ 5 | ||||
| ‘There were participants that reported low experience of digital tools’ 38 | ||||
| ‘Some of the participants experienced “Too high knowledge demands on elderly”’. 38 | ||||
| ‘They described [. . .] the elderly’s own insecurity with the digital tools and difficulties to learn new things’. 38 | ||||
| ‘A majority of patients expressed “Lack of experiences and knowledge” of digital tools’ 38 | ||||
| ‘The most important reasons were [. . .] feeling uncomfortable with the technology’ 63 | ||||
| ‘Barriers to mHealth use [were] lack of familiarity with technology’ 36 | ||||
| ‘Barriers to mHealth use [were] concern about learning to use technology’ 36 | ||||
| ‘Barriers to mHealth use [were] concern about [. . .] incorrect use by patient’ 36 | ||||
| ‘They faced a technical literacy barrier. One participant said, “I’ve never used it [these apps] because I never got it to work the way I wanted it to”’ 65 | ||||
| ‘Patients with lower perceived eHealth literacy were less likely to express interest in using websites or smartphone applications to track their health despite having access to computers, cell phones, and the Internet’. 23 | ||||
| ‘Participants [. . .] found it difficult to use the different modes on the pedometer’ 18 | ||||
| ‘Some people [. . .] felt they would have difficulty engaging with the technological requirements of the equipment’ 31 | ||||
| ‘The three participants who withdrew from the trial after they had received the equipment, described some technical difficulties they had in getting the equipment to work’ 31 | ||||
| ‘Lack of confidence with technology’ 31 | ||||
| ‘She was not at all certain she wanted to take part because she did not think she would know how to use it’ 31 | ||||
| ‘[Participants had] doubts about their capacity to engage with what they understood to be the operational requirements of the equipment’. 31 | ||||
| ‘[One] respondent [. . .] explained his decision to decline the trial as being due to [. . .] a lack of confidence with technology’
24
|
||||
| ‘Participants often had difficulty retrieving data, such as appointments entered into the caregiving apps’. 24 | ||||
| ‘[Users had a] general lack of basic knowledge and confidence for use of IT’ 37 | ||||
| ‘All six participants reported some level of technical difficulty with using the devices, particularly connecting the wireless scale’ 32 | ||||
| ‘Participants [. . .] expressed common concerns regarding their adoption [of eHealth technologies]. Specifically, they mentioned [. . .] entry errors’ 44 | ||||
| ‘Other challenges included inexperience and lack of computer literacy’. 19 | ||||
| ‘[perceived] disadvantages [were] [. . .] computer literacy/safety concerns’ 50 | ||||
| Access | Internet | ‘Telehealth-related reasons, in terms of [. . .] no internet access, were prominent prespecified reasons’ 62 | ||
| ‘About 4% of participants reported lack of access to the internet as a barrier’ 20 | ||||
| ‘[Some] did not have the Internet access in their homes’. 56 | ||||
| ‘In contrast, many participants in the no portal, low health literacy group mentioned having had little experience using computers and did not have the Internet access in their homes’. 21 | ||||
| ‘Limited Internet access was also perceived as a key barrier for a smaller number of participants’ 68 | ||||
| ‘Patients [. . .] had no internet access’ 58 | ||||
| Computer | ‘Some did not own a computer’ 13 | |||
| ‘Other reasons for individual concern included [. . .] [little] access [to computers]’ 53 | ||||
| ‘Active decliners also specified that they were not participating because they did not like the telehealth intervention [. . .] because of practical barriers, such as not having a computer’ 62 | ||||
| ‘No computer/internet access’ 20 | ||||
| Others | ‘Some mentioned that they do not own any of these devices (smartphone and tablet)’ 45 | |||
| ‘Accessibility is seen as a problem by patients’ 55 | ||||
| ‘We live on a piece of property that’s very remote, no electricity’ 68 | ||||
| Social environment | ‘Negative word of mouth from peers or health care providers’ 14 | |||
| ‘I had friends who did it but didn’t seem to get into physical shape, so I thought “why bother?”’ 40 | ||||
| ‘Rejection of digital solutions in the presence of a digital affine partner’ 55 | ||||
| Attitudes towards tele-medicine technologies | Lack of motivation | General | ‘Reasons given for not using the progress tracker via the website included [. . .] no motivation’ 61 | |
| ‘Low motivation has a negative impact on the quality of records’ 2 | ||||
| ‘Participants who did not attempt to enrol in the patient portal [. . .] stated reasons related to lack of [. . .] motivation’. 20 | ||||
| ‘The most common reasons cited for not attempting enrolment were related to lack of information or motivation, particularly being [. . .] [too] lazy’ 20 | ||||
| ‘Willingness to persevere [. . .] only for 15 min due to impatience’ 15 | ||||
| ‘We observed that many participants were reluctant to learn by trial and error’. 15 | ||||
| ‘Patients lacked the [. . .] motivation to do a search’ 58 | ||||
| ‘Lack of motivation [. . .] will undoubtedly lead to low adoption rates’. 23 | ||||
| ‘Portal nonusers expressed [. . .] lack of [. . .] desire for skills’ 23 | ||||
| ‘Some subjects with COPD had difficulty in starting a self-management diary’ 11 | ||||
| ‘Unable to motivate’ 50 | ||||
| No health need | ‘Reasons given for not using the progress tracker via the website included [. . .] [being] happy with current method [of activity tracking]’ 61 | |||
| ‘[One of] the main reasons for non-participation [. . .] [was having] their own exercise program’ 61 | ||||
| ‘My daughter started looking at the app and said she had no patience for that and would not use it at school. [. . .] She does not want to bother with it as she already knows the enzyme dosage and do it herself alone’ 2 | ||||
| ‘A lack of perceived health need was the second most frequent option in the pre-specified reasons (40.1%, n = 2852)’. 62 | ||||
| ‘A small number of people also declined because they were satisfied with their current level of support, such as having regular health checks (3.1%, n = 222)’ 62 | ||||
| ‘I feel fully informed by my physician about my medicine and do not need digital support’. 55 | ||||
| ‘A number of patient participants identified that they did not see a need for such health programs personally’. 68 | ||||
| ‘Patients [. . .] found the information from their physician sufficient’ 58 | ||||
| ‘No need to fix what wasn’t broken’ 38 | ||||
| ‘Feel like they “don’t need it”’ 36 | ||||
| ‘They did not use mobile apps because they found the tools they were using, such as a paper logbook or a glucometer, already satisfied their needs’. 65 | ||||
| ‘Portal nonusers expressed [. . .] simply not seeing the need for or value of using the portal to manage their health’ 23 | ||||
| ‘Confident in their own self-management routines, they saw no need for self-management tools’ 49 | ||||
| ‘Respondents often described their satisfaction with current services and how they preferred the existing care relationships that they had with health care providers’ 31 | ||||
| ‘The most common reasons for refusals were [. . .] [e.g.] that routine health care was sufficient’ 70 | ||||
| ‘Some do not see the need [for online health management tools]’ 12 | ||||
| No interest or rejection of the intervention | ‘Users who had reached their goal were not stimulated to achieve further’ |
|||
| ‘[One of] the main reasons for non-participation [. . .] [was] not [being] interested in the program’ 61 | ||||
| ‘Patients felt that e-tools were impractical and were unwilling to learn how to use one’. 45 | ||||
| ‘The overwhelming majority of patients reported that they would not go online to view their clinical summary or other medical records’. 13 | ||||
| ‘No interest to develop digital know-how’ 55 | ||||
| ‘They expressed that they lost interest after reading some of the first issues raised in the reflection sheets because they could not familiarize themselves with these issues and did not consider the content relevant to their diabetes’ 3 | ||||
| ‘Participants continued to express confusion about point accumulation and also felt that the point and reward system was not motivating’ 6 | ||||
| ‘Some of the interviewees described their preferable choice of receiving ordinary letters rather than electronic messages and conveyed a lack of interest for digital solutions’ 38 | ||||
| ‘Some patients [. . .] had no interest in what was on offer once they had started the intervention’. 22 | ||||
| ‘About half of the participants expressed disinterest in eHealth technologies, which they considered of limited value’ 49 | ||||
| ‘About 11 did not think they needed TH (Telehealth) or TC (Telecare) and/or did not want it’ 31 | ||||
| ‘She was not at all certain she wanted to take part [. . .] because she did not think it would help’ 31 | ||||
| ‘Users thought they might stop using if [. . .] they no longer have a need for the tool’ 12 | ||||
| Rejection of behavioural change | ‘[One of] the main reasons for non-participation [. . .] [was being] unwilling to change’. 61 | |||
| ‘Other difficulties mentioned were the low motivation to do activities’ 1 | ||||
| ‘Some patients in the CVD risk trial reported low motivation to change their lifestyle’ 22 | ||||
| ‘A low intention to be physically active was a strong predictor for dropout’ 71 | ||||
| Technology aversion | ‘[Some did not like] using smartphones for intervention’ 1 | |||
| ‘[Some were] afraid to use technology’ 1 | ||||
| ‘Nearly two-thirds of the non-Internet-users did not intend to use e-Health applications if asked to use them’ 66 | ||||
| ‘Refusal to use information and communications technologies’ 14 | ||||
| ‘About 30% reported negative attitudes toward the patient portal’ 20 | ||||
| ‘Digital solutions are seen as something for the younger generation’ 55 | ||||
| ‘General rejection of digital solutions’ 55 | ||||
| ‘[The] majority of respondents were reluctant to use e-mail and video conference for making contact with health care providers’. 56 | ||||
| ‘Participants in every focus group expressed at least some degree of negativity toward technology use in health care as well as in everyday encounters’. 21 | ||||
| ‘The patients with limited experiences of digital tools expressed “Dislike of text messages for health monitoring and lifestyle advices”’ 38 | ||||
| ‘Barriers to mHealth use [were being] unwilling to wear a monitor’ 36 | ||||
| ‘At least one patient in each focus group referred to herself or himself as the elderly people who feared and avoided to be confronted with modern technology such as HTMS (Home Telecare Management System)’. 7 | ||||
| ‘Some patients [. . .] expressed their computer anxiety’ 7 | ||||
| ‘The most frequent reason for withdrawing [. . .] was because the participant [. . .] rejected the equipment after trying for a period of time’ 41 | ||||
| ‘[Some] did not want it [Telehealth or Telecare]’ 31 | ||||
| ‘Device fatigue could be a significant challenge, which was apparent after only 4 weeks’. 32 | ||||
| ‘They did emphasise that they did not want additional equipment for the data transfer’ 60 | ||||
| ‘Technology anxiety has a negative and indirect influence on adoption intention of MCDMS [mobile chronic disease management systems] because it reduces ease of use perception’. 72 | ||||
| Other preferences | Conventional solutions | ‘Particularly older patients preferred personal contact with their GP’ 69 | ||
| ‘Generally preferred paper-based tools for education and recording BP measurements’ 45 | ||||
| ‘Patients preferred the booklet of dietary restrictions that are currently provided to them by the AF clinic as opposed to having this information in an e-tool’. 45 | ||||
| ‘Active decliners also specified that they were not participating because they did not like the telehealth intervention [. . .], primarily because it was being delivered remotely rather than face-to-face’ 62 | ||||
| ‘Given the choice, participants preferred an in-person conversation for important information’ 15 | ||||
| ‘Many patients expressed a preference for a face-to-face consultation if an examination was necessary’. 47 | ||||
| ‘They preferred in-person communication for instructions about treatment’ 16 | ||||
| ‘I only want personal contact with physician’ 58 | ||||
| ‘[Participants stated] a preference for face-to-face encounters’ 3 | ||||
| ‘Many stated preferences for face-to-face or phone communication’ 5 | ||||
| ‘The most common reason for refusal to participate, accounting for almost one-third of respondents, was a stated preference for a face-to-face nurse visiting service rather than a telecare service’. 64 | ||||
| ‘Preference for in-person services was described by some participants’ 29 | ||||
| ‘Some of the interviewees described their preferable choice of receiving ordinary letters rather than electronic messages and conveyed a lack of interest for digital solutions’ 38 | ||||
| ‘Participants expressed a clear preference for face-to-face consultations’ 49 | ||||
| ‘Respondents often described their satisfaction with current services and how they preferred the existing care relationships that they had with health care providers’ 31 | ||||
| ‘Other reasons expressed by subjects with COPD included [. . .] having a preference for face-to-face contact’. 11 | ||||
| Other technical solutions | ‘Preferred smartphone based’ 45 | |||
| ‘Some preferred larger screens’ 45 | ||||
| ‘If we want to look up something, we will look for it on the Internet or call the hospital. There are so many other means to find information’ 2 | ||||
| ‘Prefer phone over email’ 20 | ||||
| ‘About 37% said they prefer to call the provider’s office to discuss health matters rather than communicate electronically’ 20 | ||||
| ‘Portal nonusers most frequently cited preference for phone communication as the most common reason for not using the portal’ 23 | ||||
| Negative outcome expectation | Loss of contact with provider | ‘Participants also reported disadvantages of the Web-based tools. Patients think that there will be less personal contact with the caregiver’ 54 | ||
| ‘The risk of losing physical contact was perceived as a barrier to using mHealth solutions’ 69 | ||||
| ‘Some participants worried that [. . .] the applications were replacing the expertise of the pharmacist’ 15 | ||||
| ‘Patients stated that they trust their physicians most, and they do not want them to be replaced regarding their disease education by a digital support tool’. 55 | ||||
| ‘Some even expressed concern that portals would decrease their existing quality of care or be used to replace face-to-face visits altogether’ 5 | ||||
| ‘[One main topic were] concerns about the loss of human connection/interaction and communication with clinicians’ 59 | ||||
| ‘[They feared] that technology might replace human contact’ 38 | ||||
| ‘Concern about lack of human interaction’ 36 | ||||
| ‘[Portal users expressed] concerns about [. . .] variations in provider availability for online appointment scheduling and response times to medical messages’. 23 | ||||
| ‘Participants expressed some concerns about [. . .] [the] lack of physical presence of a health care worker’ 7 | ||||
| ‘One woman did not want remote eHealth consultations to replace her regular control visits’ 49 | ||||
| ‘Some patients [. . .] felt that the tool could become a replacement for in person consultation’. 33 | ||||
| ‘Participants expressed concerns regarding [. . .] the loss of necessary visits’ 44 | ||||
| No expected benefit | ‘Many of the non-computer users explained that they could not see any value in going online for their clinical summary, asking “what could possibly be of benefit there”?’ 13 | |||
| ‘People who did not believe in the possible advantages of e-Health [. . .] were less inclined to use e-Health’. 66 | ||||
| ‘Didn’t think it would be useful’ 20 | ||||
| ‘Lack of perceived value of trackers’ 40 | ||||
| ‘Digital solutions are only for profit maximization’ 55 | ||||
| ‘Digital solutions [. . .] bring no added value’ 55 | ||||
| ‘Don’t think it is useful’ 56 | ||||
| ‘These participants questioned the value or potential benefit that they may receive’. 68 | ||||
| ‘Patients [. . .] did not think it would be helpful’ 58 | ||||
| ‘I don’t find this useful’ 58 | ||||
| ‘The most important reasons [for refusing participation] were [. . .] the belief that the technology could not help them’. 63 | ||||
| ‘Portal nonusers expressed [. . .] limited perceived value of using portals’ 23 | ||||
| ‘Reasons [for non-participation were that[ parents did not feel [the] conference would be valuable’ 30 | ||||
| ‘They generally assumed that they could not benefit from eHealth’ 49 | ||||
| ‘They often assumed that eHealth is being implemented not to benefit patients, but to address resource challenges’ 49 | ||||
| ‘About 11 did not think they needed TH (Telehealth) or TC (Telecare) and/or did not want it’ 31 | ||||
| ‘She did not think it would help’ 31 | ||||
| ‘The most common reasons for refusals were [e.g.] lack of perceived addition benefit of telemedicine’ 70 | ||||
| ‘Perceived risk exerts a marginal significant and negative influence’ 72 | ||||
| Additional burden | ‘However, most of the patients felt that this [the virtual patient support group] was not useful. Reasons included not wanting to be overburdened with reading about other patients’ issues’ 45 | |||
| ‘[Patients had] the perception that e-tools would be complicated and troublesome’. 45 | ||||
| ‘12.4%–17.6% thought it [e-Health] would not [be easy to use]’ 66 | ||||
| ‘Promotes competition among multiple sclerosis peers’ 14 | ||||
| ‘Some participants worried that too much information was dangerous’ 15 | ||||
| ‘About 10% [of the respondents who never attempted to enroll] thought the patient portal would be too complicated to use’. 20 | ||||
| ‘Thought it would take too much time’ 20 | ||||
| ‘Increasing knowledge of medical condition can be worrisome for the patient’
55
|
||||
| ‘Constant monitoring promotes the feeling of sickness’ 55 | ||||
| ‘Digital solutions can distract from reality’ 55 | ||||
| ‘[They] were worried that the devices might be too complicated to use in a health context’ 57 | ||||
| ‘Some participants explained that they were concerned that the intervention required too much time’ 68 | ||||
| ‘Some [. . ..] [were] describing an additional risk of increased anxiety between the regular visits at the PHCC’. 38 | ||||
| ‘Too much trouble’ 63 | ||||
| ‘Some participants acknowledged that they did not use apps or other tools for self-management because they did not want to be accountable for their behaviours’. 65 | ||||
| ‘Portal nonusers mostly expressed concerns about [. . .] lack of support to navigate computers and/or the Internet’ 23 | ||||
| ‘Time constraints posed barriers to conducting the discharge videoconference’ 30 | ||||
| ‘Some viewed the intervention as having the potential to make them “hypochondriac”’ 31 | ||||
| ‘Participants expressed concerns regarding [. . .] downloading responsibility onto patients for care management’ 44 | ||||
| ‘Participants expressed concerns regarding [. . .] training requirements’ 44 | ||||
| ‘Common reasons for refusal were [. . .] perceptions that the equipment would be burdensome or bothersome’ 70 | ||||
| ‘Common reasons for refusal were [. . .] an unwillingness to become involved in anything else’ 70 | ||||
| ‘A few [nonusers] mentioned [. . .] that they thought it seemed hard to use’. 12 | ||||
| Decrease in freedom and independence | ‘They expressed concerns, [. . .] not wanting to be “nagged” with “one more set of you should do this and you should do that”’. 13 | |||
| ‘Digital solutions can promote the feeling of being surveilled’ 55 | ||||
| ‘Smartphone-based solutions can lead to dependency on the smartphone’ 55 | ||||
| ‘Digitization is unstoppable, but you have to be careful not to lose your independence’ 55 | ||||
| ‘I just don’t want to be tied down to having to do something at a certain time’ 68 | ||||
| ‘Others viewed the interventions as posing a threat to independence and activity’ 31 | ||||
| Miscommunication and wrong decision- making | ‘Other reasons for individual concern included [. . .]the opportunity for misinterpretation of information’ 53 | |||
| ‘Identified barriers against the use of health apps were [e.g.] fear of misdiagnosis’ 8 | ||||
| ‘Risk of incorrect decisions’ 50 | ||||
| ‘Risk of misunderstandings’ 50 | ||||
| Isolation | ‘Some [. . .] feared that eHealth could lead to social isolation’ 49 | |||
| ‘Participants expressed concerns regarding [. . .] increased social isolation’ 44 | ||||
| ‘I will be alone and isolated at home’ 50 |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.