
Abstract
Chronic patients could benefit from the technological advances, but the clinical approaches for this kind of patients are still limited. This paper describes a system for chronic patients monitoring both, in home and external environments. For this purpose, we used novel technologies as big data, cloud computing and internet of things (IoT). Additionally, the system has been validated for three use cases: cardiovascular disease (CVD), hypertension (HPN) and chronic obstructive pulmonary disease (COPD), which were selected for their incidence in the population. This system is innovative within e-health, mainly due to the use of a big data architecture based on open-source components, also it provides a scalable and distributed environment for storage and processing of biomedical sensor data. The proposed system enables the incorporation of non-medical data sources in order to improve the self-management of chronic diseases and to develop better strategies for health interventions for chronic and dependents patients.
Keywords
Introduction
According to the World Health Organization, in recent decades, there has been an indisputable increase in chronic diseases in developed countries. This is mainly due to the ageing population and the fact that those diseases were considered merely variations of normal patient conditions. Another important aspect to consider is comorbidity, that is, the simultaneous occurrence of diseases in the same individual. These factors together, chronic diseases and comorbidity, affect the outlook and quality of life of chronic disease patients, especially elder people. The number of people suffering from chronic diseases is continuously growing each year. At the global level, chronic diseases are responsible for 70% of all deaths and 48% of the total healthcare expenditure, and the forecast for the year 2020 suggests that the latter percentage will increase to 60%. Healthcare expenditures increase with the age of the population. 1 It is also well known that the prevalence of multiple chronic conditions increases rapidly with age, and per capita health expenditure increases with the number of chronic conditions.
The impact of chronic diseases on people is very negative. People suffering from chronic diseases have, both objectively and subjectively, a generally worse health status compared to healthy people, and this feeling is stronger if there is comorbidity, especially when the disease(s) affects a person’s daily activities. Additionally, family and friends of chronic patients suffer a negative impact known as ‘caregiver burden’ that involves serious physical, psychological and emotional consequences. Caregiver burden constitutes a vicious circle that also negatively affects the chronic patient.
CVD causes more than 4 million deaths in Europe and more than 1.9 million deaths in the whole European Union (EU). 2 The overall cost of CVD in the EU is estimated to be approximately €196 billion per year. Of the total cost of CVD in the EU, approximately 54% is due to healthcare costs, 24% is due to productivity losses and 22% is due to the informal care of people with CVD.
Despite therapeutic progress, it is common to consider that in the healthcare system the care of chronic patients is not adequate. The healthcare system was organized 20 to 40 ago and is focused mainly on acute diseases and episodic treatments. Improving the healthcare system to better treat chronic patients is likely the most important challenge in the coming years, and it is clearly a necessity rather than an option. To date, treatments for chronic diseases have been characterized by a few drawbacks inherent to the system that prevent greater effectiveness in service. 3 Examples of some of these drawbacks are the following: (1) reactivity, where treatment is performed only if patients are in a critical status and preventive diagnosis practically does not exist or there is no budget available for it, and it tends to be limited to awareness campaigns; and (2) discontinuity in care, where public or private health systems only monitor patients temporarily, and there usually is too much time between each instance of monitoring. Healthcare systems focus only on majorly dependent or very sick patients, and patients must travel to medical centres for tests or medical consultation. Additionally, consultation and emergency services are often saturated for pathologies that do not require more than a simple health check. This involves very significant costs in terms of both public administration and families, and the highest proportion of costs is due to a minority of patients.
Modern e-health services based on the use of information and communication technologies could help avoid those problems and transform the healthcare system in the following ways: (i) preventive: remote patient monitoring can help detect changes in their illness tendency and generate alarms that can be used by caregivers or medical personnel before a critical situation is reached; (ii) proactive: it is possible to have full control of a patient’s situation anytime and anywhere; (iii) participative: all healthcare and social ecosystems (patients, social workers, family members and physicians) can participate in future improvements of the system; and (iv) global: it is possible to apply this concept to all types of patients, independent of their state of illness and thereby reduce the costs related to medical consultation and patient monitoring and consequent treatments, thus allowing a better distribution of costs among different patient types. 4
Considering the aforementioned situation, it is clearly extremely important to develop tools and services that enable new personal healthcare services for both dependent and chronic patients by extensively using information and communication technologies. This approach would greatly help reduce ‘undesired’ costs, which would increase the sustainability of the healthcare system. These new services should be developed as part of a comprehensive health service for dependent and chronic people in relation to their overall health. An outstanding example of those new services is the remote monitoring of chronic patients, which involves multidisciplinary research areas in wireless personal area networks, IoT, big data analytics, cloud computing, information retrieval, activity monitoring and contextualization and behavioural pattern analysis. This will be achieved by recording and monitoring information (in real time or offline) about the most important bio-signals of chronic patients, such as the heart rate, blood oxygen concentration, body temperature and abnormal movement of special body parts. Furthermore, it would also be possible to track the patient’s behaviours in real time and over long periods, thereby providing alerts for signs of physical and/or cognitive deterioration.
Currently, there are many telemonitoring solutions on the market, most of which are tailored to the home environment, in which the measurements that are performed are collected by different monitoring devices and application host-devices. The monitoring data are typically collected in different databases with their own software. Health professionals need to access heterogeneous software platforms, in addition to their own record-keeping systems, to obtain an overall picture of patient’s conditions. Moreover, if the monitoring results are not standardized, it is difficult for health professionals to use the collected data. Based on the current situation, there is still a need for a scalable data storage and high-performance computing infrastructure that enables efficiently storing, processing and sharing health data. 5
In this paper, we present a system implemented for chronic patient monitoring, both indoor and outdoor. We applied the system to three use cases (CVD, HPN and COPD), although it could also be extended to dependent people. The system has been developed in the framework of the Virtual Cloud Carer and IpHealth projects6–8 with the collaboration of four small and medium enterprises (SMEs), three universities and two hospital institutions. The main features of the system are the following: (1) it implements data storage and processing based on big data and IoT in a cloud environment, (2) it allows the integration of diverse data sources (data sensors, personalized alarms and information about patient’s disease), (3) it facilitates communication between the agents involved (patient, medical personnel or health emergencies and caregivers), (4) it enables the decision making of each agent based on big data analysis and (5) it is suitable for chronic and dependent patient monitoring, both outdoors and indoor.
The rest of paper is organized as follows. In Section 2, we review topics related to the present study, such as ‘IoT sensing and remote monitoring’, ‘Integration of heterogeneous data’ and ‘Systems for healthcare’. The architecture of our system based on big data and IoT for indoor and outdoor chronic patient monitoring is described in Section 3. Section 4 presents three use cases (CVD, HPN and COPD) of the proposed system. Section 5 presents and discusses the main results of our work. Finally, the conclusions are presented in Section 6.
Related work
At present, the convergence of the technological and health sciences has created an opportunity for a transformational leap forward in the way in which healthcare decisions are made for all individuals. 9 Data volumes are growing at an uncontrollable rate. Large populations, increases in the unhealthy population, technology innovations and evidence-based medicine approaches are some sources contributing to the unprecedented amount of data that is being accumulated. 10 In this new era, medicine is taking on a predictive, preventive, personalized and participatory character (Gibbs, 2014) 11 . Big data plays a major role in these advances in medical practices.12–14 The benefits of big data to healthcare include improving the efficiency and quality of healthcare delivery, managing specific health populations and individuals, detecting diseases at an early stage, providing evidence-based treatment options to patients, and detecting early fraud in healthcare systems. 10 This new era is linked to the advent of IoT.15,16 The rapid evolution of communication technologies, in conjunction with the development of new devices such as wireless personal devices, embedded systems, smart objects and remote sensors, has imposed an extension of the current Internet capabilities towards the Internet of all the objects and devices located around us, which is referred to as the IoT. 16 The IoT can be observed as a wireless network of sensors that interconnects all things in our daily lives. 15 IoT provides an important data source that big data technology can exploit.
IoT, sensing and remote monitoring
IoT technology provides a wide variety of information from many heterogeneous sources. Currently, there are wellness and health-monitoring devices for monitoring parameters such as the heart rate, respiratory rate and effort, inhaled/expired CO2, cardiac output, blood pressure, oxygen consumption, blood oxygenation and glucose. 17 Increased data processing power, faster wireless communications with higher bandwidth, and improved design of microelectronics and sensor devices have mainly contributed to the rapid uptake of wearable devices. 12 Rapid and seamless health data acquisition will contribute to the successful use of big data in medicine. 12
Seamless and real-time biomedical or health monitoring allows the characterization of intra-individual physiologic variation and the inter-individual impact of circadian fluctuations on physiological measures. Advancing technology, such as sensor miniaturization, which allows them to be wearable, and continuous monitoring, has made the development of healthcare remote monitoring systems feasible in recent years.18,19 Technologies such as TEN-HMS 20 or CHAMPION 21 have been developed for monitoring patients with heart failure. Several home monitoring systems for COPD have also been implemented. 22 These systems include facilities for monitoring patients at home, thus potentially avoiding the need to travel to the hospital for maintenance, 23 aiming to also decrease the cost for the patient in terms of disruption in the activities of daily living. In general, mobile health systems aiming to promote adherence may cost-effectively improve the self-management of chronic diseases and enhance compliance with the medical prescription, thereby encouraging and stimulating patients to adopt healthy life styles and promoting empowerment. 24 Currently, the use of wireless devices to monitor patients is achieving a maturity level beyond traditional SMS or alert signals, including web-based solutions for evaluating the information obtained from sensors and wearable sensors for use with chronic heart patients6,25 The functionalities are focused on assistive functionalities. Some indoor solutions for chronic patient monitoring are focused on using sensors as blood pressure or pulse oximeter devices, connecting them to a concentrator or gateway and then transmitting the data to some repository or database. Broadband communications infrastructure can provide additional support for developing this approach. Indeed, this infrastructure can support advanced solutions based on tele-visits, remote assistance and cross-consults of different e-health repositories by an expert’s team. 26 Kim and Chung 27 proposed an emergency monitoring system that uses context motion tracking for chronic disease patients and transmits the data from a patient’s home to a medical centre in real time. A similar system for real-time remote exercise monitoring among cardiac patients has also been proposed. 28 In addition, remote monitoring of permanently implanted critical devices has been implemented at several institutions 29 and offers a safe, feasible, time-saving and cost-effective solution for patients. 30 Furthermore, over the last several years, there has been an increasing number of applications using mobile devices and sensors for healthcare, such as wrist-worn wireless sensors for a medical monitoring system that is specifically designed for patients with HPN or respiratory problems; such systems include the continuous collection and evaluation of several vital signs and are connected to the medical centre using mobile phones. 31 However, the use of different monitoring technologies and different endpoints limits the generalizability of the results obtained from these monitoring systems. A major disadvantage of the proposed systems is that they do not provide an integrated architecture for data capture, storage, processing and analysis and generally do not consider important aspects such as scalability and security. 32
Integration of heterogeneous data
Healthcare and wellness monitoring data are currently gathered on an unprecedented scale. However, the data are collected in a fragmented system, and a user with multiple health-monitoring devices cannot manage or integrate diverse data streams through a single web or mobile application. 17 Furthermore, most of the mobile apps currently available for smartphone users are disconnected from the healthcare delivery system. 33
Currently, initiatives and organizations such as Human API (https://humanapi.co/), Aqua.io (https://aqua.io/), Vivametrica (http://www.vivametrica.com), ‘Here is My Data’ (http://www.hereismydata.com) and ‘Datadonors’ (http://datadonors.org/) address the unification of data from diverse resources. In addition, large databases that bring together disparate types of data and enable multi-variate and deeper analyses of the information for each patient are being developed. In particular, population-based tools have proven useful for comparing one individual’s anatomy to a population or between sub-populations and for the detection, quantification and monitoring of disease progression. 34
In addition to sharing and unifying data, integration of healthcare and wellness data with clinical data must be addressed. 33 This integration of health monitoring and clinical data has great potential to assist both patients and providers in predicting, diagnosing, treating and managing complex or chronic conditions. 17 It is also essential to the further development of the field of cardiovascular research. To accomplish this integration of data, important changes should be made. Improved technological infrastructure is necessary and must be accompanied by an improvement in the predictive models that allows the potential of the health data to be exploited.
Key elements for the integration and exploitation of health data are technologies such as big data and the cloud environment. 35 Individualized care models for patients, that is, personalized medicine, 9 require parallel processing using high-performance computing that can help analyse big data at a much faster rate and thus enable the design of better strategies for health intervention.
Systems for healthcare
Over the last few years, various platforms and systems focused on healthcare have been proposed. Tseng et al., 36 considering the characteristics and needs of the elderly, developed an intelligent health monitoring system for the elderly with low information literacy living in a nursing home. The system monitors the health status of the elderly based on clinical and medical knowledge, provides an easy-to-understand and easy-to-use user interface for the elderly, and automatically sends important or emergency feedback to caregivers via a real-time interactive platform. Jimenez and Torres 19 and Kim and Chung 27 presented prototypes of basic healthcare remote monitoring systems, which send alerts in real time to patients’ relatives or medical doctors if an elderly person is experiencing a problem that could require medical attention or hospitalization. Some initiatives have taken a step forward in the use of technologies for healthcare. This is the case of the Artemis project, 37 a big data platform for the acquisition and storage of patients’ physiological data streams and clinical information system data for use in online real-time analytics, retrospective analyses and data mining. Patients benefit from the system because the earlier detection of signs of medical conditions may lead to earlier intervention, which may, in turn, lead to improved patient outcomes and reduced length of stays. An important aspect of this system is its scalability. This characteristic is also present in cloud computing. More recently, Sultan et al., 38 propose some general design principles for a telemonitoring system with focus on chronic patients.
Cloud computing and big data technology
Currently, cloud computing and big data technologies are becoming increasingly important in healthcare systems. In recent years, various cloud-based architectures have been proposed for use in heart disease treatment (Gibbs, 2014). An example of such systems was proposed by Benharref et al., 39 who presented a service oriented and cloud-based e-health system for the tracking, monitoring and prevention of chronic diseases and reducing their impact. Human medical expertise with state-of-the-art about online service delivery based on cloud computing, service-oriented architecture, data analytics and mobile applications are well described in Bitsaki et al. 40
Big data analytics in healthcare
In addition to technological improvements such as wearable devices, cloud environment and big data technologies, it is necessary to exploit the available data and advance the development of better predictive models. Mining the local information included in electronic health record (EHR) data has already proven to be effective for a wide range of healthcare challenges, such as disease management support 41 and building models for predicting health risk assessment. 12 By capturing continuous vital sign data for populations of patients, we will be able to develop more sophisticated models for a patient’s normal physiology and enable the identification of subtle or activity-specific changes towards pathophysiology early during disease progression. 17 Which physiological variables are most useful or how the data should be collected, filtered and managed are fundamental questions that remain unresolved, 42 but we know how important it is to solve them to achieve more effective predictive models and move closer to personalized medicine.
Big data analytics provides an opportunity for effective and precise medicine. Wang et al. 43 noted that the main benefits derived from big data analytics in healthcare are related to information technology (IT) infrastructure and operational issues. The first type of benefits includes reducing system redundancy, avoiding unnecessary IT costs, transferring data quickly among healthcare IT systems, better using healthcare systems, standardizing processes among various healthcare IT systems and reducing the IT maintenance costs related to data storage. The operational benefits include improving the quality and accuracy of clinical decisions, processing many health records in seconds, reducing patient travel time, immediately accessing clinical data for analysis, shortening the time of diagnostic tests and reducing surgery-related hospitalizations.
This combination of patient’s health heterogeneous data, cloud infrastructure and big data analytics tools can therefore lead us towards personalized medicine that provides chronic patients with better health and better control of their diseases. In addition, it is important that the e-health services for patients allow both indoor and outdoor monitoring to increase the patients’ freedom of movement and reduce the impact on their lives.
Big data and IoT-based architecture for an indoor/outdoor chronic patient monitoring system
We have designed and implemented a big data and IoT-based architecture for a chronic patient monitoring system that works in both home and external environments (indoor/outdoor). The system provides interfaces for the interaction of patients, healthcare professionals and caregivers through big data, IoT and cloud computing approaches. Our system permits the processing of large volumes of data from non-invasive wireless bio-sensors and the appropriate visualization of interfaces for each user type (patients, healthcare professionals and caregivers), in addition to the implementation of security and an ethical mechanism concerning the treatment of medical information. A high-level view of the architecture for the indoor/outdoor chronic patient monitoring system and its associated services is presented in Figure 1.
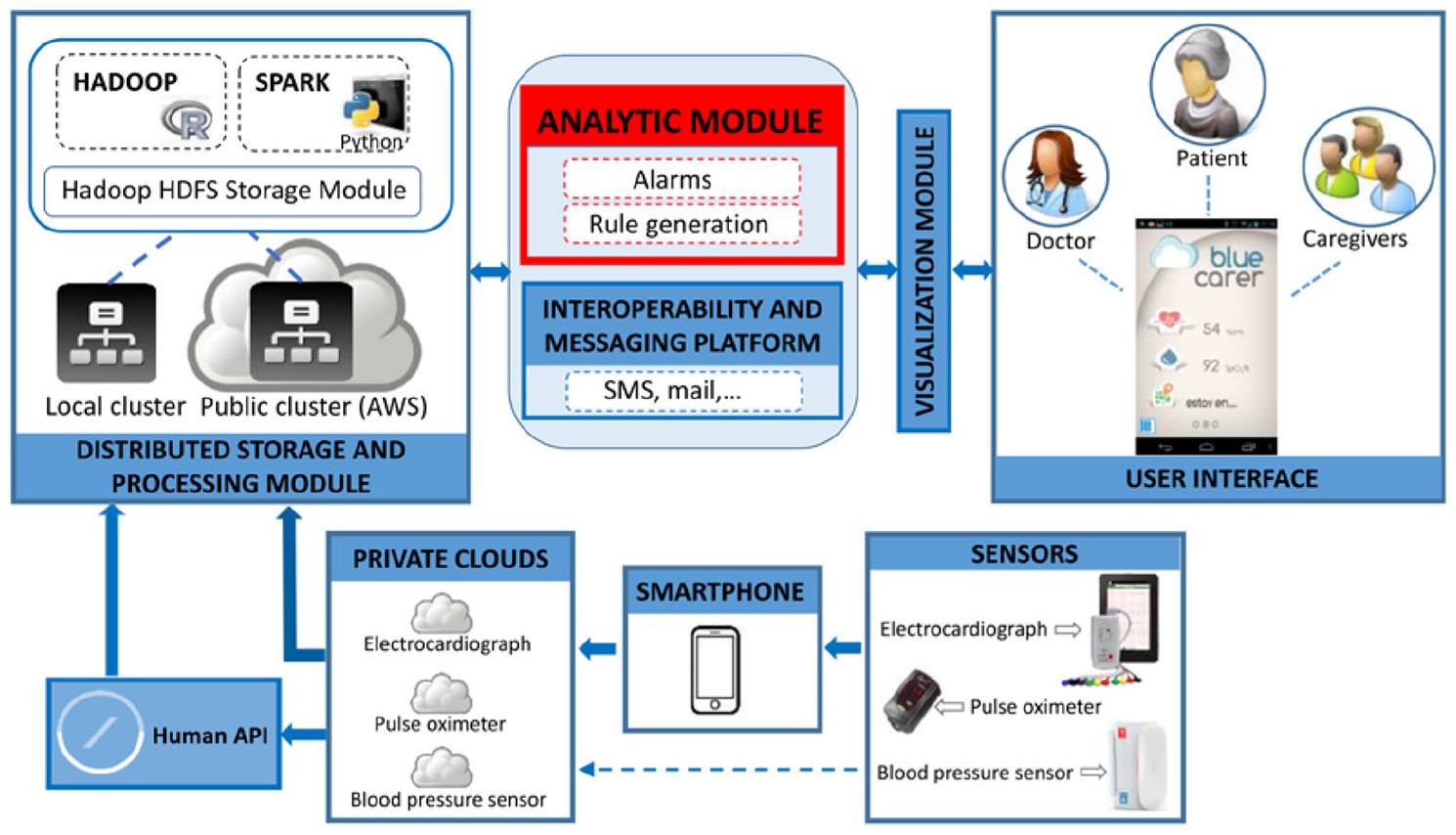
High-level view of the designed architecture for the indoor/outdoor chronic patient monitoring system and associated services. This system is based on big data, cloud computing and IoT.
The elements of the designed and implemented system are described in the following subsections.
Sensors
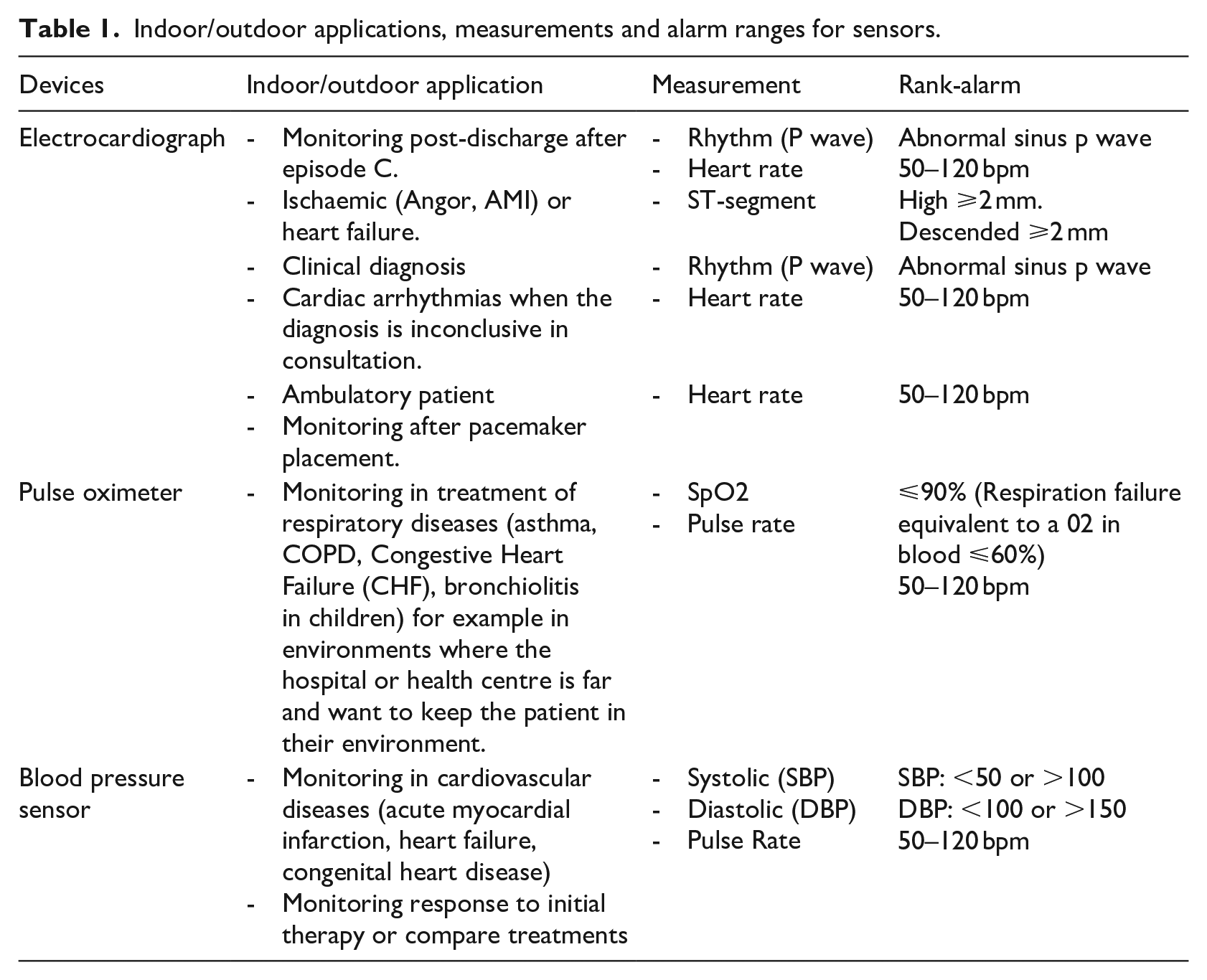
Our system receives biomedical signals of the patients from three types of sensors: electrocardiographs, pulse oximeters and blood pressure monitors. The indoor/outdoor applications, measurements and rank-alarms of each sensor are reported in Table 1.
Indoor/outdoor applications, measurements and alarm ranges for sensors.
Electrocardiograph
The EC-12RM Cardioscopy Mobile (http://www.labtech.hu/products/netecg/ec-12rm) is a compact ECG device that can forward real-time, 12-channel ECG signals to any Android device (tablet or smartphone) via a Bluetooth connection. A cloud application communicates with and receives data from the cardioscope. This application can be used by health professionals since it provides feedback about the condition of the patient and performs a preliminary analysis of the patient.
Pulse oximeter
A wireless finger pulse oximeter (http://www.nonin.com/Onyx9560-OEM) allowed us to remotely monitor the blood oxygen saturation levels and heart rates of patients with chronic diseases; such devices are commonly used in eHealth applications around the world. The transmission of the data from the sensor to the smartphone was performed via secure wireless communication (Bluetooth 2.0 Wireless Technology). The Onyx II is certified for use with Microsoft HealthVault (https://www.healthvault.com/), a free online platform that communicates and receives data from the pulse oximeter for personal health management purposes. This sensor is designed to meet the requirements of the emerging open standards, such as the Bluetooth Health Device Profile (HDP), IEEE11073 and Continua.
Blood pressure sensor
This sensor is a non-invasive blood pressure measurement system (https://ihealthlabs.com/support/blood-pressure-monitors/wireless-blood-pressure-monitor/) that is intended for use in a professional setting or at home. It is designed to measure the systolic and diastolic blood pressures and heart rate of an adult individual (Table 1) by using a technique in which an inflatable cuff is wrapped around the upper arm. The measurement was displayed in the corresponding colour according to the World Health Organization classification. This sensor can determine the blood pressure and pulse, keep a history of measurements and share blood pressure and heart rate data with iOS or Android smartphones. The transmission of the data from the sensor to the smartphone is performed via wireless communication (Bluetooth V3.0 + EDR Class 2 SPP. Frequency Band: 2.402–2.480 GHz). Furthermore, iHealthlabs provides an open API (Application Protocol Interface), ‘iHealth Myvitals’, that is installed on the smartphone; this API allows developers to interact with cloud iHealth’s data. It uses the OEuth (Open Euthorization) 2.0 protocol for authentication and authorization.
The range of values according to the measurements was as follows: 0–300 mmHg (cuff pressure), 60–260 mmHg (systolic), 40–199 mmHg (diastolic) and 40–180 beats/min (pulse rate), with a measurement accuracy of ±3 mmHg for pressure and ±5% for pulse rate.
Smartphone
The chronic patients used smartphones to collect their biomedical data measured by the sensors. The transmission of health data from sensors to the smartphones was performed via Bluetooth technology. Data from the pulse oximeters, electrocardiographs and blood pressure sensors were stored in the manufacturers’ private clouds (see section 3.1). The smartphones enabled storage and sending the data to the private clouds. The Human API platform could be used to integrate the data from these private clouds and put them on the distributed storage and processing module, although the distributed storage and processing module could receive directly the data from the sensors’ private clouds (Figure 1).
The use of a smartphone is not necessary when we use sensors with Wi-Fi connections.
Distributed storage and processing module
The biomedical data were stored in the Hadoop Distributed File System (HDFS) (http://hadoop.apache.org/). To perform parallel processing, our system uses both Hadoop and Spark (http://spark.apache.org/), which are open-source software packages for reliable, scalable and distributed clustering computing. These software tools could be used on a local or private cluster, such as Amazon Web Services. Algorithms in the R and Python programming languages were implemented on Hadoop and Spark, respectively.
In the server and the cloud part, we use a service-oriented architecture (SOA) for standardization and because it enables and facilitates the development of new applications and services that can be seamlessly integrated with existing modules without requiring expert knowledge.
Analytic module
Additionally, it is necessary to develop logic processes to generate alarms based on the threshold of the measures or historical information. This is implemented in the analytical module, which consists of both an alarm generation module and a data analytics module through which the activated alarms are sent to both the chronic patient’s caregivers and healthcare professionals. This is the core of the system to produce early diagnoses and new e-health services based on the analysis of historical data using big data approaches.
In addition to biomedical data collected from patients, the architecture of our system allows us to use public data sources from the Internet, for example, Physionet 7 (https://www.physionet.org/) to obtain more data and thus perform more complete experiments to improve our models. Additionally, the design of our system allows the incorporation of data sources other than medical data, such as temperature, humidity or pollution level, which can improve predictions and may be especially important for chronic patients with respiratory problems. Employing the best predictive models and analytic tools can lead to better health intervention strategies for chronic patients.
Interoperability and messaging platform
The system has also an interoperability and messaging platform for delivering information to all users in the system. This platform uses the latest technological advances in communication (SMS, mail, voice automated systems and PUSH technology) as primary communication channels, although the system architecture also allows communication with users via other channels, such as WhatsApp and app alerts.
Visualization module
The communication among the users (patients, healthcare professionals and caregivers) and both the analytic module and the platform for interoperability and messaging is led by the visualization module. This module allows system users to visualize the results of data analysis performed in the analytic module, such as trends, clusters of elements or abnormalities in biomedical measures. Therefore, it is a fundamental element of the system to achieve better strategies of intervention because such data visualization helps professionals detect abnormalities or even anticipate a certain problem. In addition, it accelerates the process of understanding and interpreting the data.
User interfaces
To enable communication between the users and the designed system, a user interface for smartphones and tablets was implemented. The system allows access for three types of users: patients, healthcare professionals and caregivers. The information displayed and access to the data depend on the user type. Figure 2 shows the appearance of the user interface for patients.

Patient user interface. View of two of the screens of the user interface for patients observed from a smartphone.
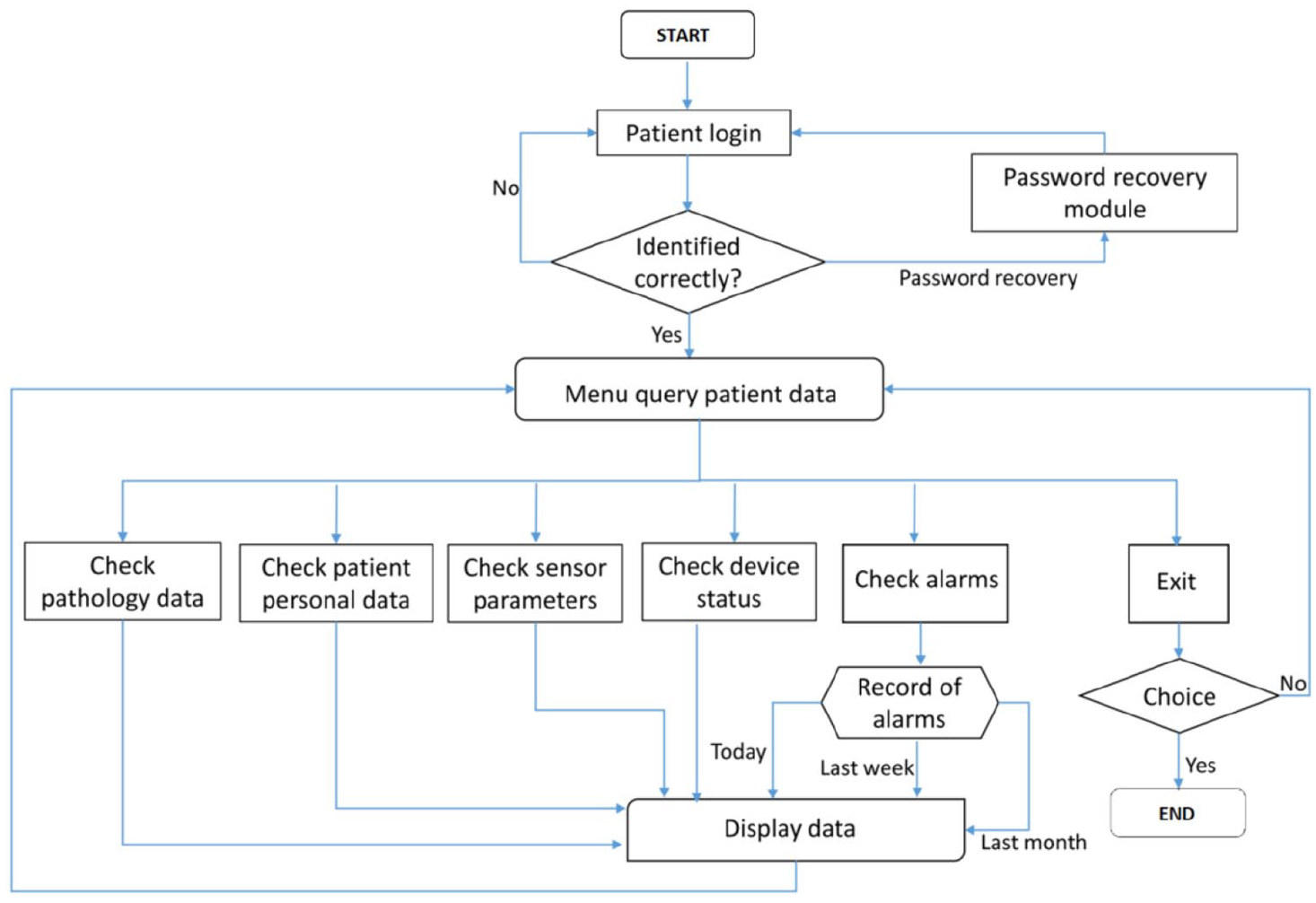
The system allows the patient to consult the following data: (i) pathological information – the system displays a list with details of the pathologies that are associated with the patient and that the system is monitoring; (ii) personal data; (iii) sensor parameters, that is biomedical signals captured by sensors; (iv) device status (e.g. battery, coverage and on/off); and (v) alarms – the system displays a historical information of alarms generated for a patient. A flow chart illustrating the operation of the system for a patient is shown in Figure 3.
In addition to these options available for the patient, the caregiver can do the following:
(1) Write notifications to their patients, and the system will allow the caregiver to send a message to the patient according to the messaging system established for this patient (e.g. SMS or e-mail).
(2) Modify the radius of movement of the patient within which the patient can move freely without alarm activation (taking the home of the patient as the centre). The system displays the range that is allowed for the user. This range is measured in kilometres and indicates the distance to which a patient can move away from home without causing an alarm activation.
(3) Global positioning system (GPS) localization of the patient. The system displays on the screen a map, with a dot indicating the place where the patient is located at that moment.
Finally, the healthcare professional has the same options as a caregiver but can also modify the sensor thresholds associated with each of the alarms for a specific patient assigned to him.
Patient platform.
Use cases
The system designed and implemented to remotely monitor chronic patients was evaluated for three use cases, CVD, HPN and COPD, which were selected based on their incidence in the population. The selection of the use cases and the design of the action protocol in accordance with the Madrid Emergency Medical Service (SUMMA 112) was performed in collaboration with medical personnel belonging to the Universidad Europea de Madrid and involved in this work.
For each use case, we tested data transmission from the sensors to the system using the smartphone, the storage of information and the correct behaviour of the alarms (see section 5). The following describes the use cases and the behaviour of the system for each of them.
Cardiovascular disease
The first use case comprises patients with CVD. This disease causes many deaths worldwide each year and leads to enormous costs to health systems, so it is very important to contribute to disease prevention and make health intervention more efficient. One of the biological signals measured in this disease is the heart rate. The three sensors integrated in our system can measure the heart rate. A value greater than 100 in this measure indicates tachycardia and could lead to cardiac arrhythmia. Figure 4 presents the behaviour of our system with the suspicion that the patient suffers from cardiac arrhythmia.
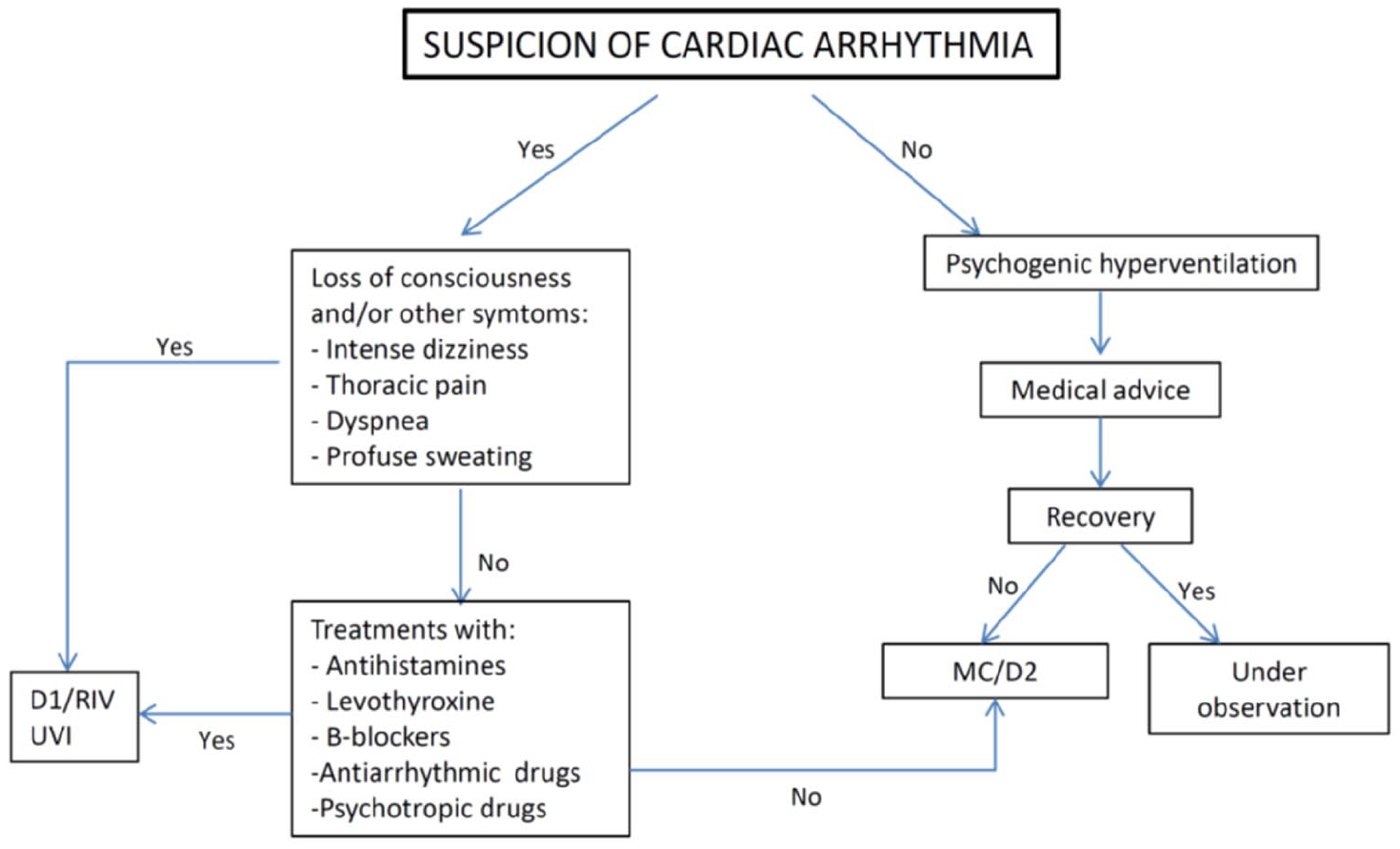
System behaviour in CVS.
Hypertension
The second use case consists in using the system for monitoring patients with HPN. If the blood pressure sensor detected risk levels in terms of the measure (Table 1), the alarm triggered and the system worked based on the flow indicated in Figure 5.
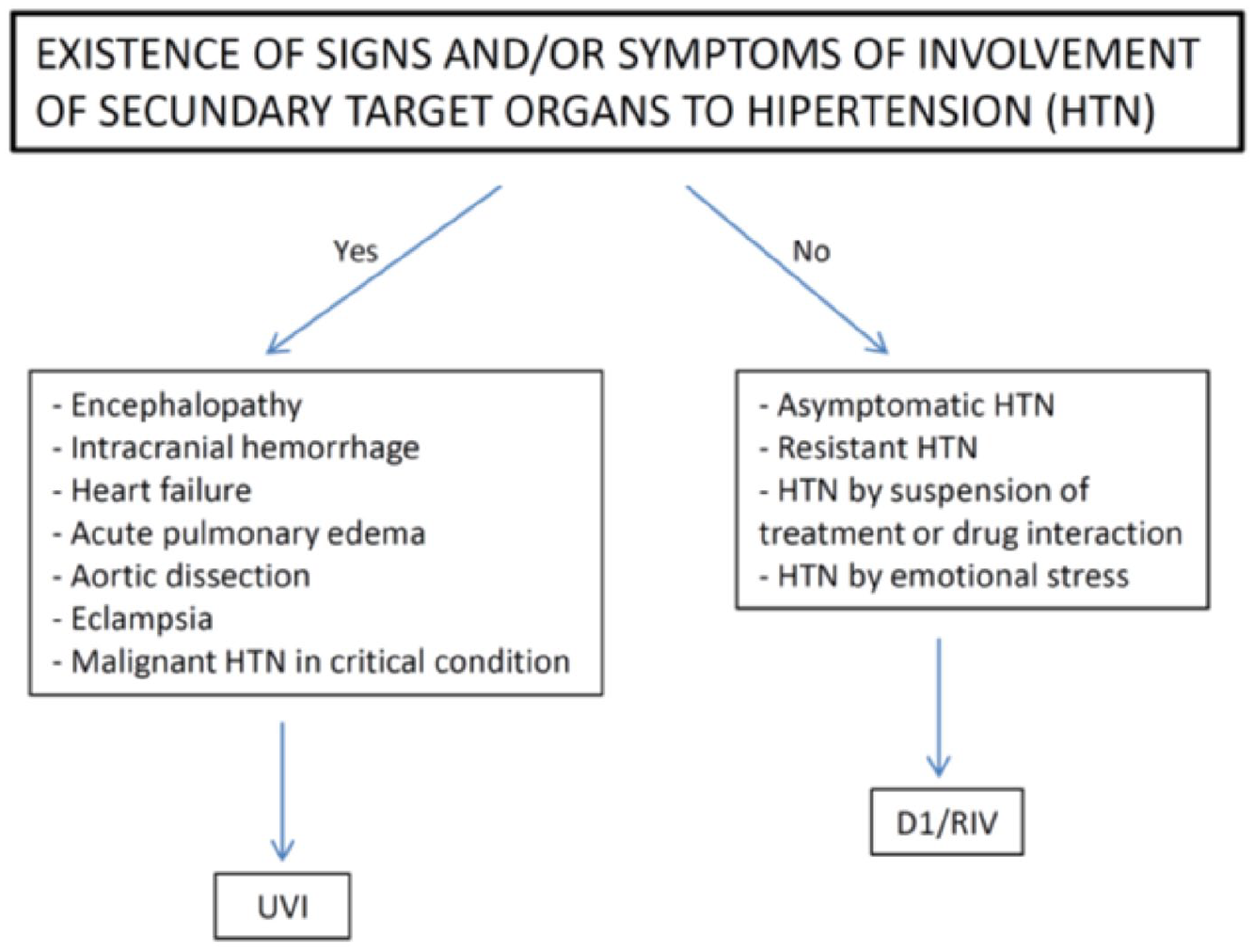
System behaviour in HPN.
Patients who need an exhaustive control of blood pressure are normally high-risk patients with previous chronic disease episodes or non-adherent patients. The remote control of blood pressure of a patient, results in, among other things, the possibility of the early detection of risk symptoms and immediate intervention, if necessary. Monitoring also helps establish the correct dose of drug and improve drug adherence. Moreover, the possibility of storing pulse and blood pressure measures from 100s of 1000s of hypertensive patients can help in the comprehension of this disease. If big data techniques are used to analyse and correlate the common characteristics and life styles of hypertensive patients, it will finally be possible to detect the disease in advance and prevent its consequences.
Chronic obstructive pulmonary disease
Finally, the last use case for which we applied our system was patients with COPD. Currently, there are sufficient data that demonstrate that for patients with COPD, monitoring the therapy with ambulatory oxygen using pulse oximeters (oxygen saturation) can help make decisions about seamless prescription (however, patients should be reviewed at least once per year in the clinic to measure arterial oxygen and carbon dioxide pressure). Moreover, supervising these values can help doctors and improve patient’s adherence to the treatment. The cut-off point for reviewing current oxygen therapy is 92% (oxygen saturation). 44 Thus, oxygen saturation levels in blood lower than 90% indicate a potential poor oxygenation. If there is a suspicion based on the data that there is an acute respiratory failure, the system acts based on the protocol outlined in Figure 6.
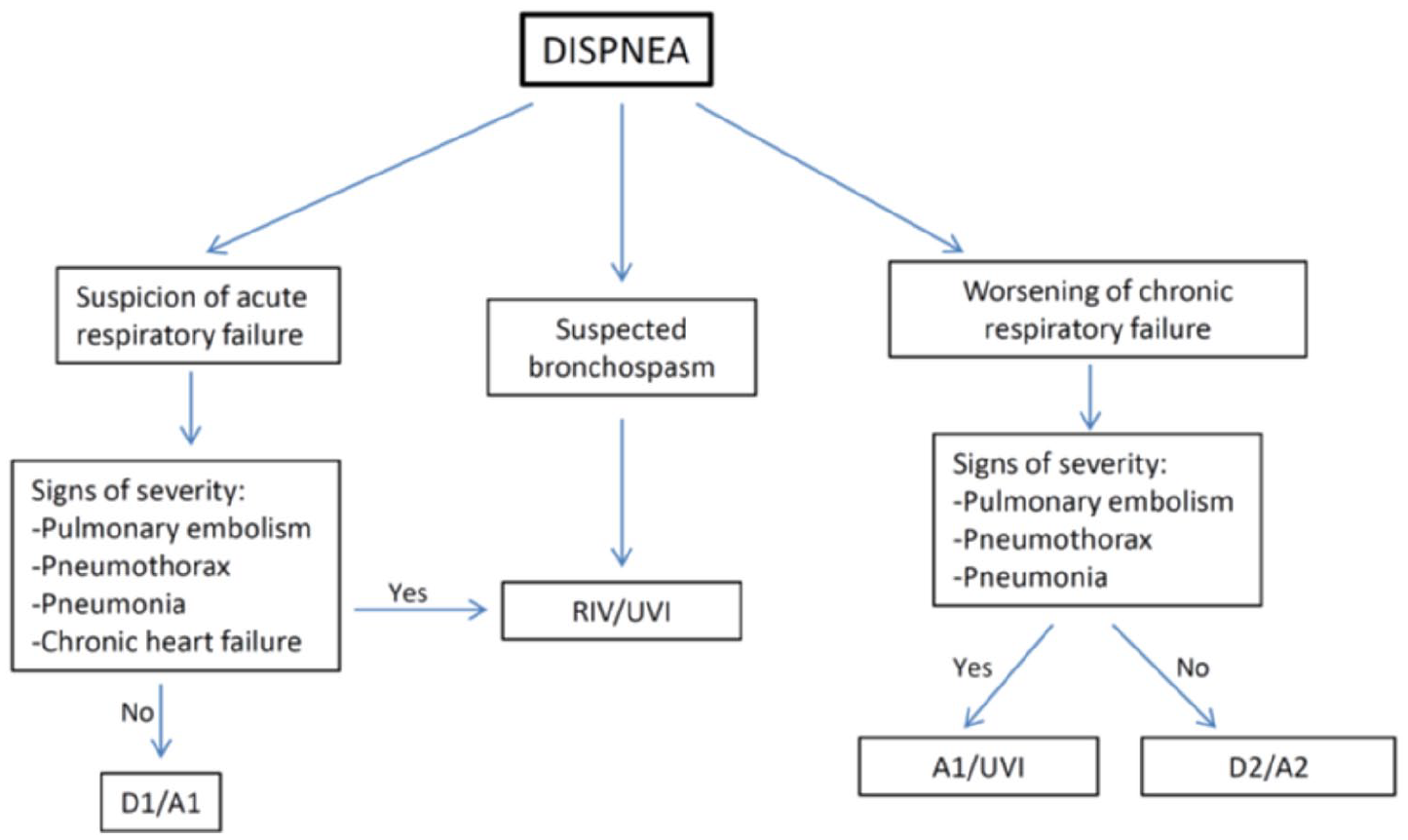
System behaviour in COPD.
Results and discussion
Design and implementation of the system based on IoT and big data for chronic patient monitoring
We designed and implemented a system for chronic patient monitoring in home and external environments with interfaces for interactions among patients, healthcare professionals and caregivers (see section 3). The main difference between our system and other solutions for remote patient monitoring is that our system provides a distributed and scalable environment (big data tools) for the storage and processing of a large amount of biomedical data from sensors. In addition, patients, healthcare professionals and caregivers can access the information via a user interface. As we can see in Figures 4 to 6 when the systems detects some risk due to measures out of range, an alarm is generated to caregivers and medical personnel for an early diagnose and prescribe an initial treatment. The design of our architecture allows the scalability of the system for storage, RAM and cluster nodes increments. Our architecture also allows the analytic module to be modified, for example, by including new models and data analyses or by adding non-medical data and public medical data sources from the Internet (e.g. Physionet) to improve or add functionalities, which can lead to improvements in self-management of chronic diseases and better health intervention strategies for chronic patients.
Real-time remote monitoring of patients and the data from several Internet sources (medical or non-medical) that can be used to improve the algorithms are factors that require the use of big data architectures that can store and process such large quantities of data. However, the existing remote monitoring systems do not usually incorporate this technology. For this reason, we focus this work on the design and use of technologies based on big data and IoT for monitoring biomedical signals and aiding in the monitoring of biomedical signals, in addition to the management and self-management of the disease.
Although there are commercial tools for big data storing and processing, our system was designed and implemented with open-source components. The most important problem encountered in the architecture implementation was determining which components were suitable for storing and processing large volumes of data. For this, we used the Hadoop environment, which allows the storage and processing of big data. The first option for setting up the Hadoop environment was to install a Cloudera Hadoop distribution on a cluster of four virtual machines, each with two processors and 8 GB of RAM, all on a physical server with 24 processor cores, 64 GB of RAM and 3 TB of disk space. This configuration caused us many problems due to the high demand of resources that Cloudera needed to manage the cluster, resulting in an unexpected operation of the nodes. Specifically, Cloudera needed many resources in the namenode, which oversees and coordinates the data storage function (HDFS), and this led to unexpected operation of the rest of the cluster nodes.
For this reason, we rejected this option and considered a second option, which consisted of maintaining the cluster with the same physical characteristics per machine but manually installing the components required for data processing. In this case, the behaviour was better because only the indispensable elements for executing the experiments were installed, thus reducing the consumption of resources associated with unnecessary tasks.
Evaluation of the system on the use cases
The system that we designed and implemented was subjected to a conceptual assessment on the use cases for which it was designed. The architecture design was modified during the evaluation process to achieve a more robust and valid system (see section 5.1). The results of the final evaluation demonstrated the validity of the system for the proposed task. The evaluation process performed is detailed in the following subsections.
Transmission and storing of data
Technical team volunteers (simulating the potential patients) participated in the system evaluation process, allowing us to register their biomedical signals through wireless sensors over several hours (<12 h). The signals from continuous remote monitoring via pulse oximeters, electrocardiographs and blood pressure sensors were correctly received by the smartphone and stored and processed into the system, which was located approximately 20 km from the volunteers.
Interface
At this stage, it was verified that the data collected by the sensors were correctly visualized both in the interface close to the user (patient interface) and in an interface located approximately 20 km from the user (healthcare professional interface). For each of the interfaces (patients, healthcare professionals and caregivers), its components were found to function as designed. Users could access the data, modify information and send or receive messages according to the options offered to each user (see section 3.7).
Alarms
Finally, we checked the correct performance of the alarms. For this test, patients received verbal instructions to modify their breathing rate and body movement; this resulted in a modification of their recorded biomedical signals and caused alarms to activate if the signals reached the alert range (Table 1).
The results of the evaluation of the system with the experimental conditions previously described were positive; however, it is important to contextualize these results. Considering the size of the sample, the duration of the recordings and the measurements of the different sensors, the size of the stored data was on the order of gigabytes. This is not an excessively large data volume; however, the data volume would be increased significantly if we performed real-time monitoring over long periods or if we increased the number of patients. The architecture was designed based on big data and with the possibility of scalability according to these considerations.
Implications
We designed and implemented a system for chronic patient monitoring in home and external environments with interfaces for interactions among patients, healthcare professionals and caregivers. The main contribution and innovation of this system in the field of health informatics is its architecture, based on big data technologies using open-source components and providing a distributed and scalable environment for processing a large amount of biomedical data coming from sensors and also enrich this information incorporating non-medical data sources, the final goal is to help to chronic patients and health professionals in the management of chronic diseases.
Conclusions
The results of this work include the design, implementation and validation of a system for chronic patient monitoring in home and external environments with interfaces for interaction among patients, healthcare professionals and caregivers. We evaluated the system for three user cases, CVD, HPN and COPD, which were selected based on their incidence in the population. Our system analysis is based on biomedical data from sensors worn by patients. This feature enables our system to perform both indoor and outdoor monitoring, which results in an improvement in self-management of chronic diseases and a stimulus for patients to adopt healthy life styles. The design of our system also enables the incorporation of non-medical data sources, which can result in improvements in the self-management of chronic diseases and better health intervention strategies for chronic disease patients.
Supplemental Material
sj-pdf-1-jhi-10.1177_14604582211030956 – Supplemental material for Chronic patient remote monitoring through the application of big data and internet of things
Supplemental material, sj-pdf-1-jhi-10.1177_14604582211030956 for Chronic patient remote monitoring through the application of big data and internet of things by María Luz Morales-Botello, Diego Gachet, Manuel de Buenaga, Fernando Aparicio, María J Busto and Juan Ramón Ascanio in Health Informatics Journal
Supplemental Material
sj-pdf-2-jhi-10.1177_14604582211030956 – Supplemental material for Chronic patient remote monitoring through the application of big data and internet of things
Supplemental material, sj-pdf-2-jhi-10.1177_14604582211030956 for Chronic patient remote monitoring through the application of big data and internet of things by María Luz Morales-Botello, Diego Gachet, Manuel de Buenaga, Fernando Aparicio, María J Busto and Juan Ramón Ascanio in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been partially supported by the Spanish Ministry of Science and Innovation through the National Programme for Research Aimed at the Challenges of Society (IPHealth, TIN-2013-47153-C3-1).
Informed consent
The designed and implemented system was evaluated with technical team volunteers (simulating the potential patients). This team had full knowledge of all the details of the investigation and agreed to participate in the system evaluation process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.