
Abstract
Patients’ online access to their EHR together with the rapid proliferation of medical information on the Internet has changed how patients use information to learn about their health. Patients’ tendency to turn to the Internet to find information about their health and care is well-documented. However, little is known about patients’ information seeking behavior when using online EHRs. By using information horizons as an analytical tool this paper aims to investigate the information behavior of cancer patients who have chosen to view their EHRs (readers) and to those who have not made that option (non-readers). Thirty interviews were conducted with patients. Based on information horizons, it seems that non-reading is associated with living in a narrower information world in comparison to readers. The findings do not suggest that the smallness would be a result of active avoidance of information, or that it would be counterproductive for the patients. The findings suggest, however, that EHRs would benefit from comprehensive linking to authoritative health information sources to help users to understand their contents. In parallel, healthcare professionals should be more aware of their personal role as a key source of health information to those who choose not to read their EHRs.
Keywords
Introduction
A growing body of evidence demonstrates that patients who are more actively involved in their healthcare appear to achieve better health outcomes and incur lower healthcare costs. 1 As a result, healthcare organizations are employing strategies to better engage patients, such as inviting them to review their healthcare records online. A typical outspoken aim of developing online electronic healthcare records (EHRs) is to improve communication and collaboration between the medical professionals and patients, ultimately increasing patients’ involvement in their health and care. 2 In Sweden, patients can access their online EHR, called “Journalen,” through the national patient portal 1177.se. At the end of 2018, all 21 regions in Sweden had implemented Journalen and today over 4 million out of 10 million Swedes have accessed their online EHR. Currently, when patients access Journalen, they find a variety of types of clinical content, including medical notes, a list of prescribed medications, lab results, medical alerts, diagnosis, maternity care records, referrals, and vaccinations. There is evidence that full access to EHRs improves doctor-patient communication, adherence to medical advice, and self-care and helps patients to better prepare for clinic visits.3–6 Moreover, the impact of providing access to information on the patient’s level of anxiety, especially for oncology patients, has been debated by clinicians.7,8 While some opine that patients may experience anxiety when accessing test results independently without a professional present in the situation, others argue that waiting for results is a more significant source of anxiety. 9 In particular, physicians have been concerned that access to EHRs will cause patients distress, confusion, and create additional workload.7,10 Some concerns have also been raised about patients searching for and relying on information from unreliable Internet sources as a result of not understanding the contents of the record. These concerns are legitimate as the Internet has become an important information source for understanding symptoms and treatments.11,12 However, the information quality can vary and patients may not possess the necessary skills to evaluate the information and relate it to their health circumstances. 13 As a consequence, online information can lead to patients’ being misinformed and increase the tendency toward self-diagnosis or self-treatment. 13 However, not all patients seek medical information on the Internet. A study by Kimiafar et al. 14 has shown that healthcare professionals, television health channels, and other patients were the most popular sources of information for breast cancer patients.
In addition to research on the effects of consulting online EHRs, there is a relatively large number of studies on patients’ attitudes to the prospective introduction of such eHealth services.15–19 There is also some research on patients’ information needs and how they use the Internet to receive medical information in general (see e.g. Tan and Goonawardene 20 and Cocco et al. 21 ). However, to the best of our knowledge, there is no research on patients’ information seeking behavior when using online EHRs. Given that an increasing number of patients choose to view their online EHRs, there is reason to believe that the Internet and other information sources are used to seek for clarification when the contents of the record are not understood. Understanding patients’ information needs that arise as a result of reading their online EHRs is important in order to provide them with the right support. This paper presents a schematization of the information behavior and source preferences of cancer patients who have chosen to review their online EHR. The results obtained from analyzing the information behavior of these patients will then be contrasted to the information sources of cancer patients who have chosen to not access their online EHR. The information behavior of cancer patients who prefer to receive abnormal test results—“bad news”—through the online EHR will also be contrasted to those who do not prefer this notification method. In the analysis of information behaviors, information horizon maps are used as an analytical tool.22,23
The remainder of this paper is organized as follows. First, a description of information horizons is provided in the theoretical background, followed by a presentation of the research approach and the main findings. A discussion of the findings is given in the last section of the paper.
Theoretical background
The information horizons framework was originally developed by Sonnenwald et al. 22 as a spatial method for capturing and visualizing the informational context or “horizon” in which an individual can act. An information horizon may comprise a variety of different information resources ranging from social networks and individuals to documents, tools, experimentation, and observation. The utility of Sonnenwald’s approach has been demonstrated in several different contexts of information science research (e.g. Huvila, 23 Chang and Lee, 24 Savolainen and Kari, 25 and Serola 26 ) and has gained some attention even outside the scope of that particular field. For instance, Maad 27 has studied software development and interactive television using the information horizons approach. Information horizons differ from other spatial approaches and metaphors in information research 28 by its focus on rendering visible information space from the perspective of an actor (i.e. ordinarily a human being). In the earlier literature, information horizons and related notions have been used both as an interpretative framework and as a theoretical basis for data gathering. In the first sense, information horizons have been used as a theory for contextualizing and explaining research data.27,29 The most common approach has been to follow Sonnenwald’s 30 original work and to use information horizons as a method to collect data and analyze the information seekers’ perceived vista of information resources (e.g. Sonnenwald et al., 22 Savolainen and Kari, 25 and Serola 26 ). Informants have been asked to draw their own information horizons and while drawing or afterwards, they have been asked to reflect on the resulting diagrams. Both the diagrams and the discussion records have been used as primary research data. Sonnenwald et al. 22 argue that in comparison to other visual data-gathering and analysis methods, the freeform approach of information horizon maps allows rich post-coordinated data collection, which is not limited by a predetermined selection of questions, dimensions, or scales such as pre-coordinated data gathering (e.g. surveys). 31
The perspectives to information horizons framework and information horizon maps have to some extent varied between different studies. Serola 26 uses informant-drawn information horizon maps both as maps and as memory devices during the interviews whereas Sonnenwald et al. 22 organize the data gathering process in the opposite order. In their study, the data gathering was started with interviews and concluded with a drawing exercise. Most of the commentaries on the information horizons framework have focused on pointing to certain limitations in the approach and complementing the perspective, rather than directly criticizing or rejecting it. Lin and McDonald’s 32 remark that information horizons may be incomplete or severely constrained in the beginning and Shenton and Dixon’s 33 argues that the notion of information universe does not reject the validity of information horizons approach, but do rather confirm Sonnenwald’s 30 original proposal of information horizons as both socially and individually determined vistas. As Hartel 34 notes, as well as Savolainen and Kari’s 25 concept of information source horizon and Huvila’s 23 analytical information horizon maps, extend rather than replace Sonnenwald’s 30 original approach. Whereas the notion of analytical information horizon maps shifts the focus of the approach from user drawn and perceived information space to researcher generated analytical conceptualizations of often collective horizons. 23
The aim of information source horizons is to make a clearer distinction between a physical information source space and a perceived information horizon. 25 In contrast to Sonnenwald, Savolainen and Kari, 25 and following their approach, for example Pálsdóttir, 29 consider information horizons as imaginary fields, which open before the “mind’s eyes” of information seekers. According to this perspective, information horizons do not consist of physical information sources as information source horizons do. Savolainen and Kari 25 also further emphasize on the proximity and distance of information (re)sources by introducing zones of source preferences within the information horizon to explicate the differences between the relevance of the information sources from the information seekers’ point of view. Also, they make a distinction between stable and dynamic information horizons. 25
Method
The empirical material of the study consists of transcripts of (N=) 30 qualitative interviews with cancer patients. The sampling of participants was conducted in two groups (15 patients in each group). Patients in the first group (referred to as readers) had consulted their EHR online, whereas patients in the second group (referred to as non-readers) had not yet used the eHealth service. This diagnosis group was chosen as many physicians in Sweden have expressed concerns that cancer patients’ access to their EHRs will cause them distress and confusion. This was considered particularly problematic if patients access their records during weekends and evenings when no staff is available at healthcare units to answer patients’ questions or deal with their concerns. Moreover, two patients from the readers’ group and three from the non-readers group did not/would not prefer to receive abnormal test results (bad news) by viewing their EHRs online. The age of the patients who participated in the study varied between 30 and 92 years. The median age of readers was 64 and for non-readers 63 years. Nine of the interviewees were men (3 of readers, 6 of non-readers), and 21 were women (12 of non-readers, 9 of on-readers). All patients were diagnosed with cancer and underwent treatment at the time of the interviews. They were also in different stages of their cancer. Some of the patients were diagnosed with cancer recurrence. Others were newly diagnosed. Several of the patients suffered from advanced cancer and were given palliative treatment.
The interviews were based on the semi-structured thematic interview approach. All interviews were conducted by the authors of the paper, taped and transcribed professionally. The interviews lasted between 45 and 60 min. The interviews focused on questions related to patients’ attitudes and experiences of viewing their online EHRs and what they usually do when they do not understand the contents of the record. The Regional Ethical Review Board in Uppsala, Sweden approved the empirical study. Participants were recruited using an information leaflet that was made available in the waiting area at the Department of Oncology at a Swedish university hospital during the summer and autumn of 2013. The analysis approach was based on the method of drawing Analytical Information Horizon Maps (AHIM). 23 The maps that were created are in turn based on the interviewees’ accounts of their information horizons. The interview record was analyzed in its entirety for evidence that could help in creating AIHMs. Typically, the most helpful interview questions in this respect where the ones asking how interviewees managed their own health information (incl. information on their visits to health care providers, conditions, and health), if they used Internet for health information seeking, and what other sources they consulted, but relevant evidence could be in all cases found throughout the transcripts. In analytically especially useful descriptions, the interviewees described their choice of information sources, what types of resources they consulted first and how they proceeded to use other sources. When using AIHMs, researchers draw diagrams for structuring, describing, and analyzing typical information behaviors related to the activities of the interviewed individuals. The method is based on Sonnenwald’s theory of information horizons. As Huvila 23 argues, we consider AIHMs as a viable approach for analyzing multidimensional research data on information behavior. The approach functions as a useful framework for producing critical, comprehensive, and comparable representations of individual and collective information horizons.
The analysis started by summarizing the use of information sources by the interviewees in tabular form. The interviewees were categorized in four groups based on whether they had read their online EHR or not, and if they were willing to receive “bad news” online. This was followed by an iterative drawing of analytical information horizon maps. The drawing of the diagrams began by identifying key information sources and information seeking sequences described or indicated by multiple interviewees. The preliminary diagrams were discussed by all authors and refined in several rounds until a consensus was reached. The notation proposed by Huvila 23 (in Huvila, 23 Figure 1) was used in drawing the maps. Boxes with a dotted line refer to carrier information sources (i.e. sources that possibly lead to interactions with further sources), and boxes with solid lines to entry point information sources (i.e. sources with which information interactions usually begin). Dotted lines indicate links between sources and solid lines emphasized links. Arrows refer to prevalent sequences of use. This step was iterated several times, and through discussions in the group it ended up with elicitation of four different information horizons in the material.
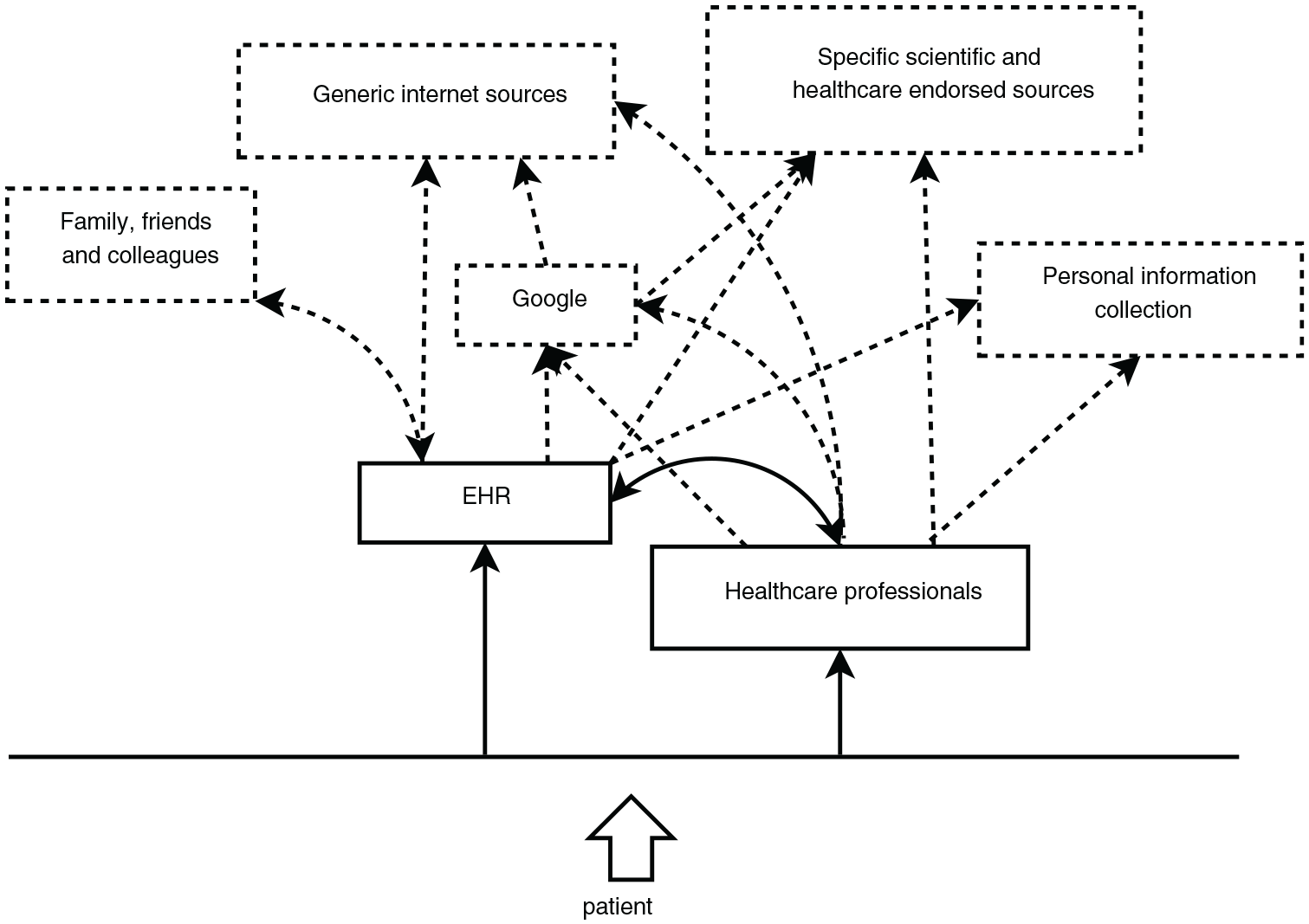
Analytical information horizon map of readers.
Results
When interpreting the Analytical Information Horizon Maps (AHIMs), it is important to consider that the maps represent collective generalizations of archetypal patients (i.e. constructed assemblages of characteristic information behaviors and source preferences of a particular group of patients according to the analyzed interview material) rather than comprehensive aggregates, or exact representations, of individual interviewees’ information horizons. There was considerable variation within and between the groups beyond the horizons represented in the AHIMs. Despite this variation, the authors argue that the maps were capable of capturing essential traits shared by individual informants within the two groups.
Information horizons of readers and non-readers of online EHR
In this section, the information horizons of patients who have read their online EHRs are presented (hereafter referred to as Readers), and those who have not read their health records online (hereafter referred to as non-readers).
Figure 1 shows the AHIM of an archetypal patient who has chosen to read their EHRs online using the eHealth service Journalen. In the Figure, we can see that patients’ principal access point to information is healthcare professionals (the source is closer to the patient i.e. the bottom of the diagram). The online EHRs are another focal entry point. After consulting one of these two sources, one can see from the solid line that it is then typical to consult the other one of these focal entry points. One can also see from the dotted lines that patients who are readers if necessary when using the online EHR continue to use other Internet sources, including specific and generic (often through Google) sources. Navigating from the online EHR directly to specific information sources is less common than using a search engine (Google in the horizon map located between healthcare records and Internet sources). One can see that consulting family and friends, when certain information in the record is not understood, are linked to the use of online EHR rather than to the contacts with healthcare professionals. In comparison to the information horizon of non-readers (Figure 2), the readers tended to have more elaborated information horizons and have a broader variety of named sources than the information horizons of non-readers that can be seen from the large variety of information sources present in Figure 1 than in Figure 2. It seemed that the readers were also more inclined to consult scientific and evidence-based sources than non-readers who tended to rely on general source types and refer to search engines rather than particular sources.
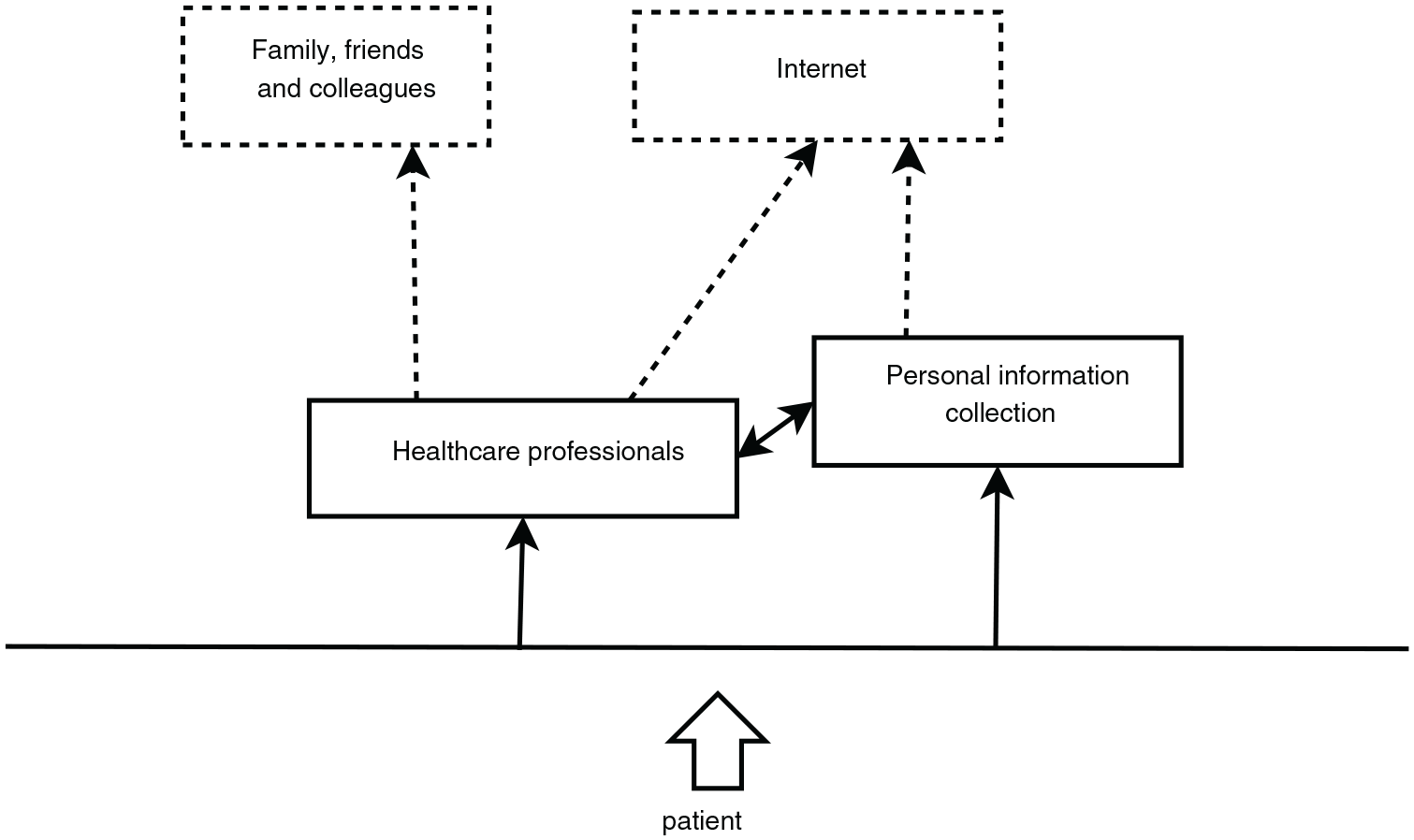
Analytical information horizon map of patients who do not read their EHR online.
In contrast to the readers, the information horizon of an archetypal non-reader (Figure 2) is characterized by the proximity of personal and socially closer sources (family, relatives, personal information collection) and the use of the Internet, which was mentioned in the interview records as a general non-specific source or channel without a specific focus on what Internet sources the patients were using. A typical non-reader was also more inclined to believe that the information they receive during their healthcare visits is sufficient. Hence, they do not seem to have the same need to search for additional information. A major difference between readers and non-readers were also their tendency to keep and store medical information and to see this personal information collection as a central source of information (Figure 2). An example of this was the use of classifiers for paper storage. The majority of all patients had kept some information. However, among readers, it was more common that their collecting had ended after some time and that they did not perceive their information collection anymore as an equally central source of information than before. Among the non-readers, they were keeping all information and they were maintaining and updating their collections of information long after they had fallen ill.
In non-readers’ information horizon (Figure 2), we see that the patients tend to rely on healthcare professionals and personal information collections as the entry-point information sources (i.e. those consulted first). Personal information collection consists of diverse documents and notes about personal health and visits to healthcare. After engaging with either of these sources, information seeking typically continues to the other, and often to the Internet. After discussing with healthcare professionals, a non-reader might also turn to family, friends, or colleagues for additional information, clarification or discussion.
Information horizons in relation to preferences for receiving bad news through online EHR
Similarly to non-readers, also the patients who preferred to not receive abnormal test results (bad news) by viewing their EHRs online (Figure 3), tended to have a simpler information horizon than those who chose otherwise (Figures 1 and 4). Those who chose to receive bad news seemed to use the online EHR, the Internet, and healthcare professionals as an entry point when they started searching for information (Figure 4). Google seemed to function as an instrument for accessing information to help them to understand the contents of the record, and in communicating with healthcare professionals. In this sense, even if Google is not an information source per se, it functioned as a quasi-source-like proxy. Also, the online EHR was a less important source of information for those who opted out of the possibility to receive bad news through the eHealth service Journalen. Among them, it seemed that reading health-related literature and magazines were more common than among the other group, who tended to seek more often to Internet sites endorsed and maintained by healthcare professionals and, what was somewhat surprising, even to scientific sources (Figure 4).
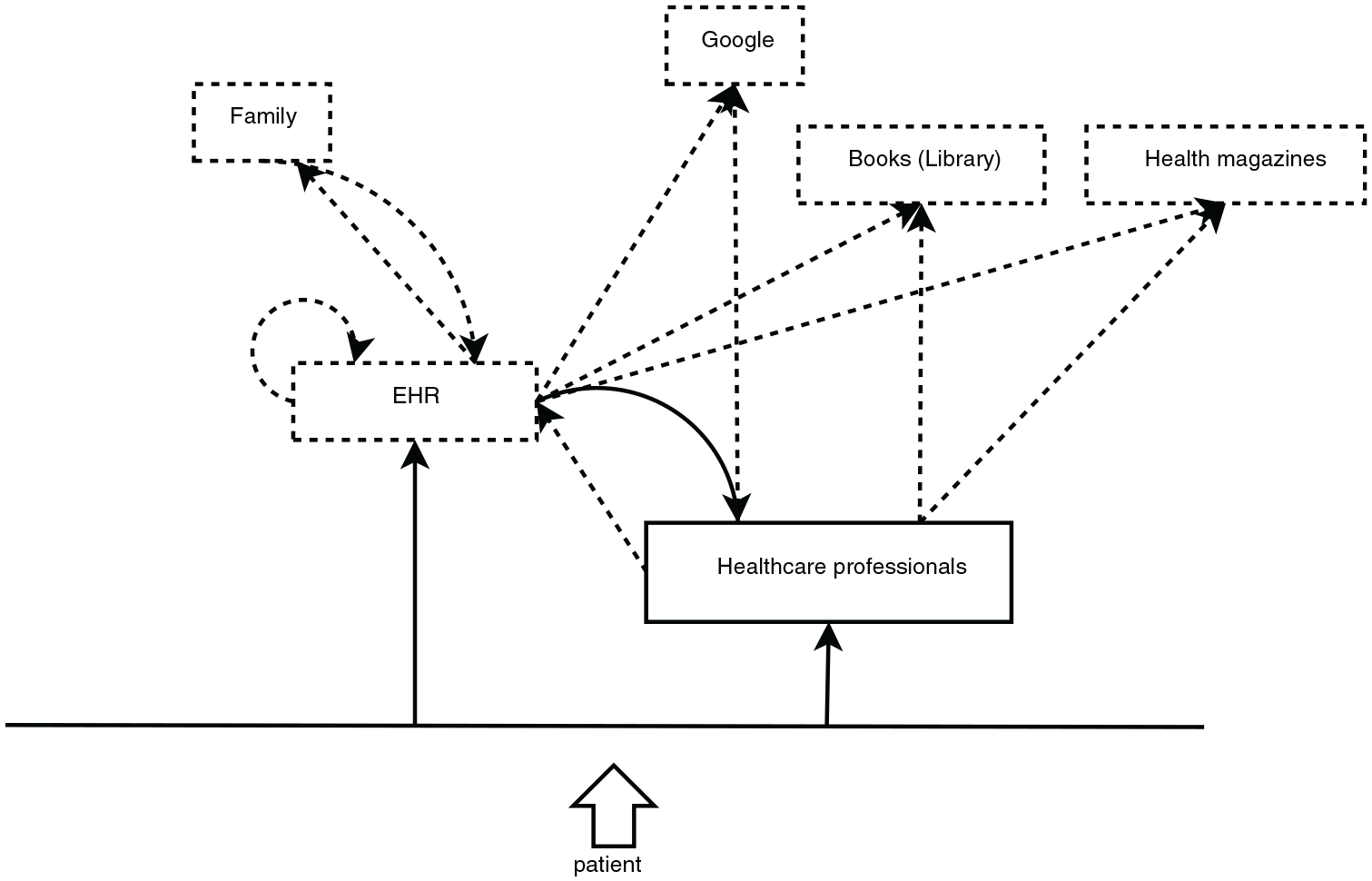
Analytical information horizon map of patients who do not want to receive bad news by viewing their EHR online.
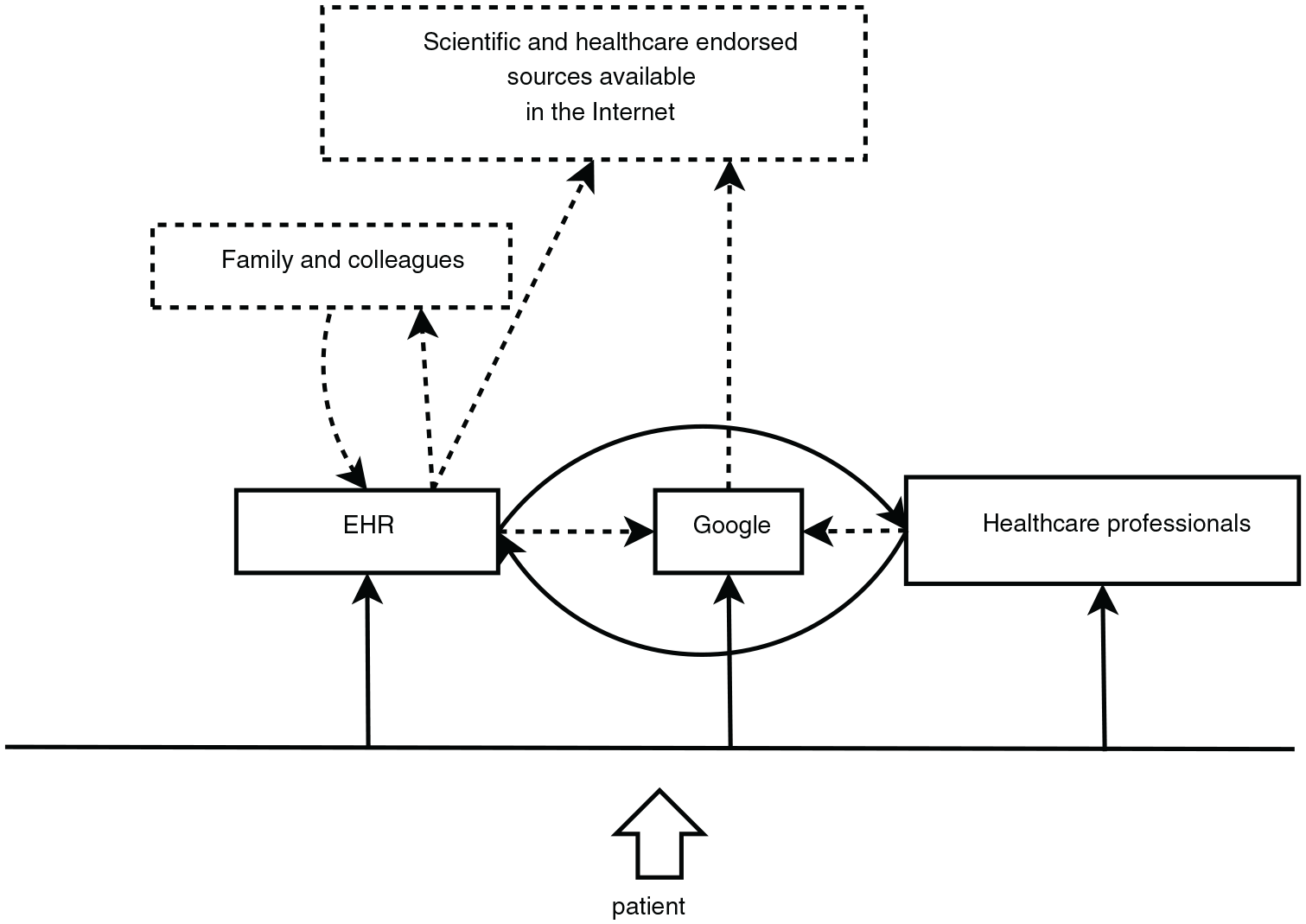
Analytical information horizon map of patients who chose to receive bad news by viewing their online EHR.
As presented in Figure 3, patients who do not want to receive bad news by viewing their EHRs online consult occasionally their healthcare record as a first, entry-point information source but tend more to first engage with healthcare professionals in their information needs. In addition to Google (explicitly mentioned by several patients), clarifications and additional information are sought from library books and health magazines. This was characteristic for these particular types of patients. Consultations of healthcare records tended to lead to discussions with family members, reading other parts of the record, and to a certain extent to the use of Google/Internet sources.
Discussion and conclusions
The analysis of the interview data and drawings of AHIMs revealed four distinct vistas to information characterized by different sets of sources and topologies of seeking information. These vistas are presented in the four different information horizon maps. As shown by the analysis, healthcare professionals are the entry point to information for both readers and non-readers. Since healthcare professionals are the main source of information, they must take the time to inform, listen, and urge patients to ask questions. Ensuring that patients have appropriate information is essential for providing the best care. An important distinction between readers and non-readers is that non-readers are outsourcing their trust in information to healthcare professionals. This result indicates that they are more inclined to believe that the information they receive during their visit is sufficient. The readers’ information needs, however, do not end at a patient meeting as accessing online EHRs often generate questions related to the content in the health record. Hence readers, in contrast to non-readers who tended to rely on the general source type and refer to search engines, often use specific and healthcare endorsed Internet sources. Considering the amount of misleading information on the Internet,11–13 healthcare professionals should take greater responsibility in educating patients as to how to safely surf the Internet for medical information. In future research, it would be interesting to study how online EHRs could be further developed to support the patient’s need for additional information. Embedding context-specific hyperlinks directly connected to medical terms in the EHR is one such example, studied by for example, Ancker et al., 35 that needs further exploration. Moreover, since readers after consulting their online EHR are more prone to use family, friends, and colleagues as sources of knowledge creation and advice, providing them with easy access to online support groups and discussion forums directly from the online EHR may be an appreciated feature that future research should look more closely into. The analysis has also shown that there are differences in preferences for information seeking between those who prefer to receive “bad news” by reading their online EHR and those who chose otherwise. Patients who opted to read “bad news” seemed to use Internet sources endorsed by healthcare professionals and scientific sources, as a meta-instrument for helping them to understand the contents of the health record, and in communicating with healthcare, whereas the patient in the other group (non-bad news) are using it as a source of and channel to find medical information.
A closer look at the maps shows thus, that there seem to be similarities between non-reading and non-reading of bad news, and similarities between the opposite approaches of reading EHRs online and preferring to read bad news. Based on the information horizons in the two larger groups, it seems that non-reading is associated with living in a smaller and narrower information world (cf. the theory of life in the round, Chatman 36 ) in comparison to readers. The findings do not, however, suggest that the smallness is a result of active avoidance of 37 or severely limited access to information, or that it would be counterproductive for the patients. 38 The non-readers seem to be content with their information horizon, the information they receive from a limited number of sources and using the Internet as a supplement. The study findings are also interesting from a personal medical information management perspective. 39 The differences between the information horizons of readers and non-readers could suggest that the significance of active management of personal medical information is shifting toward the online EHR, and the need and interest to keep personal collections may be diminishing, perhaps as a whole, and at least for the patients who are actively reading their EHRs and complementing their information needs by refining 40 (i.e. searching again when necessary) information online.
From a methodological perspective, the present study shows how the notion of information horizon and analytical information horizon mapping can be useful tools in health informatics and eHealth research. The approach provides a holistic qualitative framework for contextualizing and explicating the informational situation and environment of individuals and groups. In contrast to the tendencies of systems and technology orientation in earlier research, information horizons provide a framework for taking the health information behavior of individual actors and groups, whether patients or professionals, as urged by Huvila et al., 41 more comprehensively into account than before. The obvious limitation of the approach is its non-confirmatory nature and, in the case of analytical information horizons mapping, the inherent bias relating to the interpretation made by the researcher. At the same time, however, it can provide a much more thorough and broad evidence-based understanding of how individuals think and navigate when interacting with information than approaches focused on individual interactions. Moreover, the qualitative approach allowed us to get a more comprehensive understanding of the preferences and perspectives of the informants than a quantitative research design. However, the current approach also has obvious limitations. The qualitative research design and the fact that the study is based on a convenience sample of patients limits the possibilities to generalize findings in other than analytical sense. It is also conceivable that the interviewees had an interest in the EHRs because they chose to volunteer to participate in the study. Considering the sampling approach, the group of interviewees is not representative of a larger population, but we argue that it is still useful considering the exploratory aim of the present study.
Footnotes
Funding
The author(s) disclosed of the following financial support for the research, authorship, and/or publication of this article. This work was partly supported by NordForsk through the funding to Nordic eHealth for Patients: Benchmarking and Developing for the Future (NORDeHEALTH), project number 100477.