
Abstract
Our purpose in this descriptive cross-sectional study was to examine the prevalence of mobile health (mHealth) apps use, factors associated with downloading mHealth apps, and to describe characteristics of mHealth apps use among Jordanian patients in government-sponsored outpatient clinics. A total of 182 (41.6%) of the 438 outpatients who completed questionnaires downloaded mHealth apps. Common reasons for downloading mHealth apps included tracking physical activity, losing weight, learning exercises, as well as monitoring, and controlling diet. More than two thirds of the users (70%) stopped using the apps they downloaded due to loss of interest, lack of anticipated support, too time consuming, or better apps available. The most common personal reasons for never downloading mHealth apps were lack of interest, in good health, and the most common technical reasons included a limited data plan, lack of trust, cost, and complexity of the apps. We also found that gender, age, weight, and educational level influenced the decision whether to download mHealth apps or not. We have shown the potential in mHealth apps use among Jordanian patients is promising, and health care systems must adopt this technology as well as work through population needs and preferences to supply it.
Introduction
Mobile health (mHealth) is the use of medical interventions, supported by smartphone applications (apps), to sustain medical, and public health practice. 1 There is a growing demand within the developing world and the Middle East for the use of smartphone technologies for health information seeking and sharing, accessibility of health resources, and health promotion. 2 Specifically, there is a demand for the use of affordable mHealth services, such as mHealth apps, to provide health education, diagnostic treatment, data collection, remote monitoring services, emergency medical services, and other healthcare services.3–6 mHealth interventions have been shown to improve health related behaviors, including smoking cessation, weight loss, physical activity, and medication adherence among patients in various clinical settings.4,7–10 mHealth interventions may also enhance patients’ knowledge and skills in terms of self-care along the illness trajectory.11,12 Utilizing mHealth apps has the potential to facilitate health information access and support for patients, and reduce patients’ illness-related burden. 13
However, there are several challenges in using mHealth apps for different groups of patients, such as older patients’ lack of familiarity with technology, and cognitive distortion due to illness or medication taking.14–16 In addition to these challenges, mHealth apps might be limited in functionality compared to other digital platforms such as web-based health applications. 14 For instance, mHealth apps could not run large health data due to the limited storage ability and low data processing speed of smartphones.14,17
There is limited information about prevalence, reasons, consistency or non-continuance, and factors and challenges of mHealth apps use among patients in Jordan. Thus, our primary objective for this study was to describe the pattern of mHealth apps use among Jordanian patients in clinical settings. To achieve this objective, we sought to examine the prevalence of using mHealth apps among outpatients in Jordan, and to describe the characteristics and factors associated with their use of mHealth apps. We may take the lead to look into mHealth apps use among Jordanian outpatients. Information describing mHealth apps characteristics and usage patterns among Jordanians in outpatient settings could help policy makers and clinical decision makers to integrate mHealth apps into health care practice in the future. Our results may also suggest a direction for future researchers to define the requirements, usefulness, and usability of reliable mHealth apps in Jordanian clinical settings.
Methods
Design
This is a descriptive cross-sectional study. We sought and obtained the approval for our study protocol by the research ethics committee of the concerned party.
Sample and procedure
We recruited patients from the outpatient clinics in two government-sponsored hospitals located in the middle region of Jordan. The primary investigator contacted nurses from different clinics in both hospitals and invited them to collect data between March and June 2018. Data collectors identified outpatients who met the inclusion criteria for participating in the study during their clinic visits. Inclusion criteria were (a) being 18 years of age or older, (b) able to read and speak Arabic, (c) Jordanian citizenship, and (d) owned a smartphone, which contained the apps store.
The data collectors explained to outpatients before or after their clinical visits about the purpose of the study, anonymity and confidentiality of participation, and ability to withdraw from the study at any time without adverse consequences. After answering their questions and obtaining informed consent, those who agreed to participate in the study were given approximately 1 h to complete the questionnaire in a private area at the hospital.
We calculated the necessary sample size using G* power 3.1.7 software. 18 Using a conventional power estimate of 0.8, with alpha set at 0.05, and medium effect size, we estimated that a logistic regression analysis with eight predictors would require a minimum sample size of 385 participants. We recruited additional participants (n = 65) for the anticipated losses due to incomplete data.
Measurements
In addition to demographic data, we used a questionnaire derived from app-related questions that Krebs and Duncan 19 developed for U.S. mobile phone users. The questionnaire consisted of 25 items in the following domains: (1) participant’s health status and health behaviors (e.g. tobacco use, weight, height, medical diagnoses, physical activity, and eating behaviors), (2) history of and reasons for use/nonuse mHealth apps(s), (3) perceived effectiveness of mHealth apps, and (4) reasons for stopping use. To ensure the validity of the instrument, we first asked a panel of five experts who have experience in health care practice and research to review and revise it. The instrument was then translated into Arabic following the World Health Organization (WHO) recommended method. 20 The process started with a professional translator converting the instrument from English to Arabic, after which we then sent it to a second professional translator, who back-translated the questionnaire to English to check the consistency of their reverse-translation with the English original.
Data analysis
We used the Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM SPSS, Inc, Chicago, IL) to conduct our analyses. We calculated descriptive statistics for all participant characteristics including demographics, health status, and mHealth apps use. We used a binary logistic regression analysis to identify predictors of downloading mHealth apps by adding the following demographic factors of mHealth apps downloads in the final model: age, gender, Body Mass Index (BMI), current medical diagnosis, health status, education, employment, and income. We used a p value of less than 0.05 to determine statistical significance.
Results
Demographic and health characteristics
A total of 53.9% of the 438 participants who completed the questionnaires were female, and 60.3% were 18 to 30 years old. Approximately half (51.4%) of participants reported a monthly income of less than 500 Jordanian Dinner (JD) (equal to 705 US dollars, or 630 Euro), 56.8% were working full time; and 52.5% had a bachelor’s degree or had achieved a higher education level (Table 1).
Characteristics of the study population (n = 438).
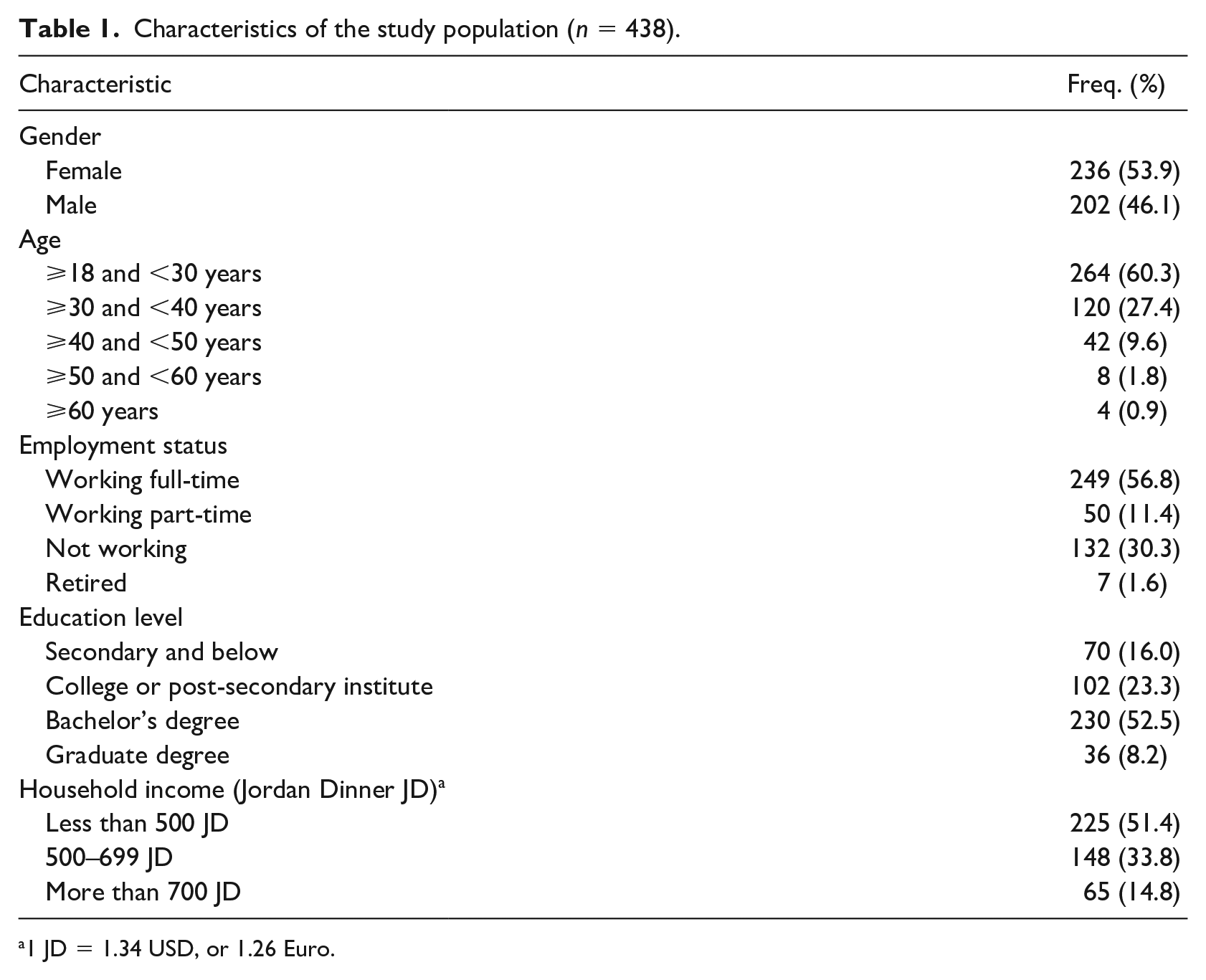
1 JD = 1.34 USD, or 1.26 Euro.
Regarding health status, a total of 58% of the participants exercised at least 15 min once a week and approximately two thirds (66.9%) were nonsmokers. Half of the participants (50.5%) had a BMI in the normal range and the BMI of 36.5% was in the overweight range. However, 47.9% of participants perceived themselves within a normal weight level, and 41.4% perceived themselves as overweight. A total of 78.8% of the participants perceived their health status as very good or excellent and 47.5% perceived their nutritional habits as very good or excellent (Table 2).
Characteristics of health status (n = 438).
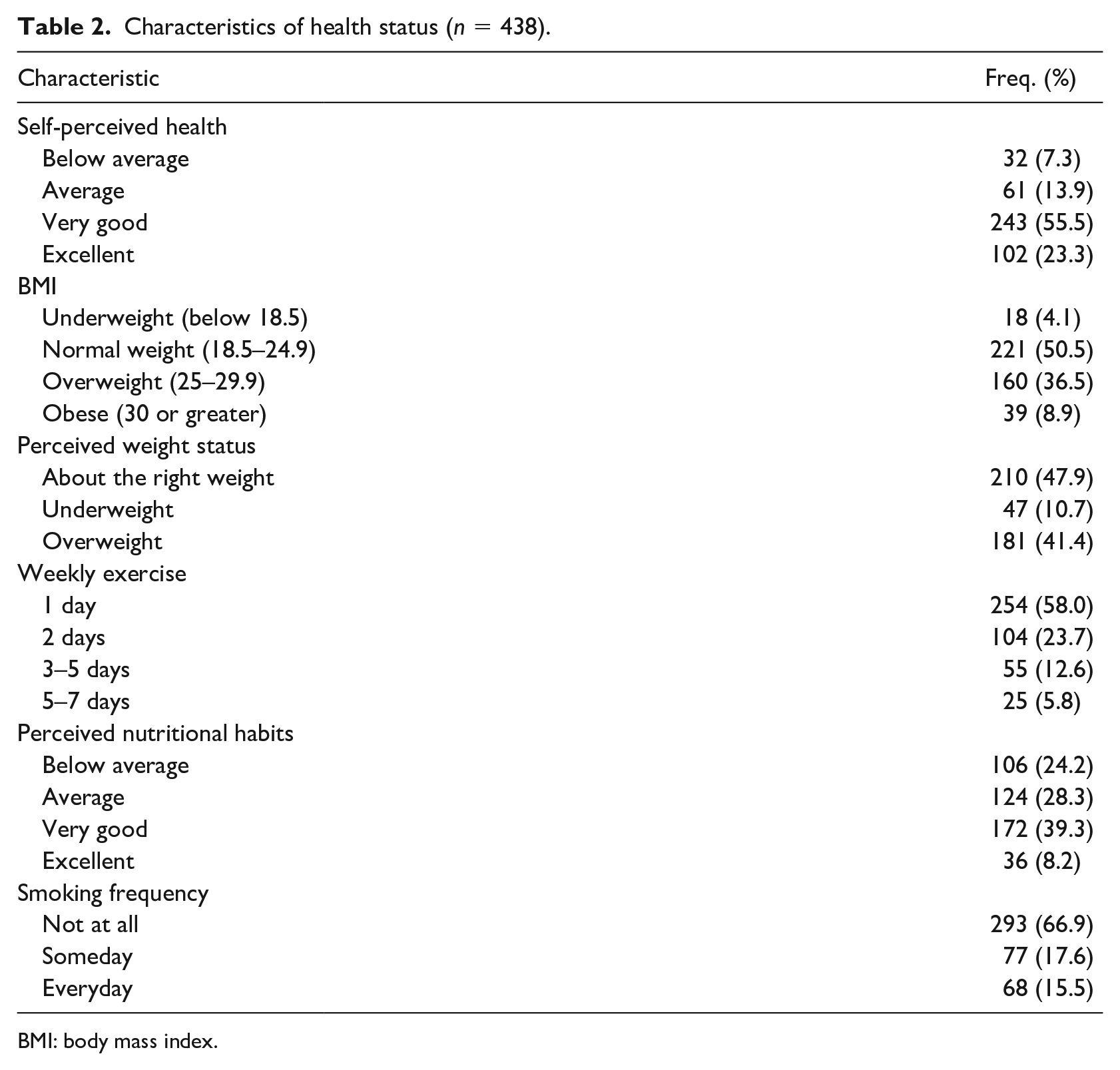
BMI: body mass index.
More than two thirds of participants (69.4%) had no chronic disease. The most prevalent medical diagnoses among participants with chronic diseases included gastric ulcer (9.5%), hypertension (7.6%), depression (6.1%), hyperlipidemia (5.4%), and diabetes (4.0%).
mHealth apps use among patients
Regarding mHealth apps use, 58.4% of participants had never previously downloaded apps related to health, while 41.6% reported that they had downloaded at least one of the mHealth apps. The number of mHealth apps participants had downloaded ranged between 1 and 5 apps (91%); the most frequent reasons for downloading mHealth apps were to track participants’ physical activity (45%), to lose weight (34%), to learn exercises (25.0%), and to monitor and improve eating (24%; Table 3).
Characteristics of mHealth apps use.
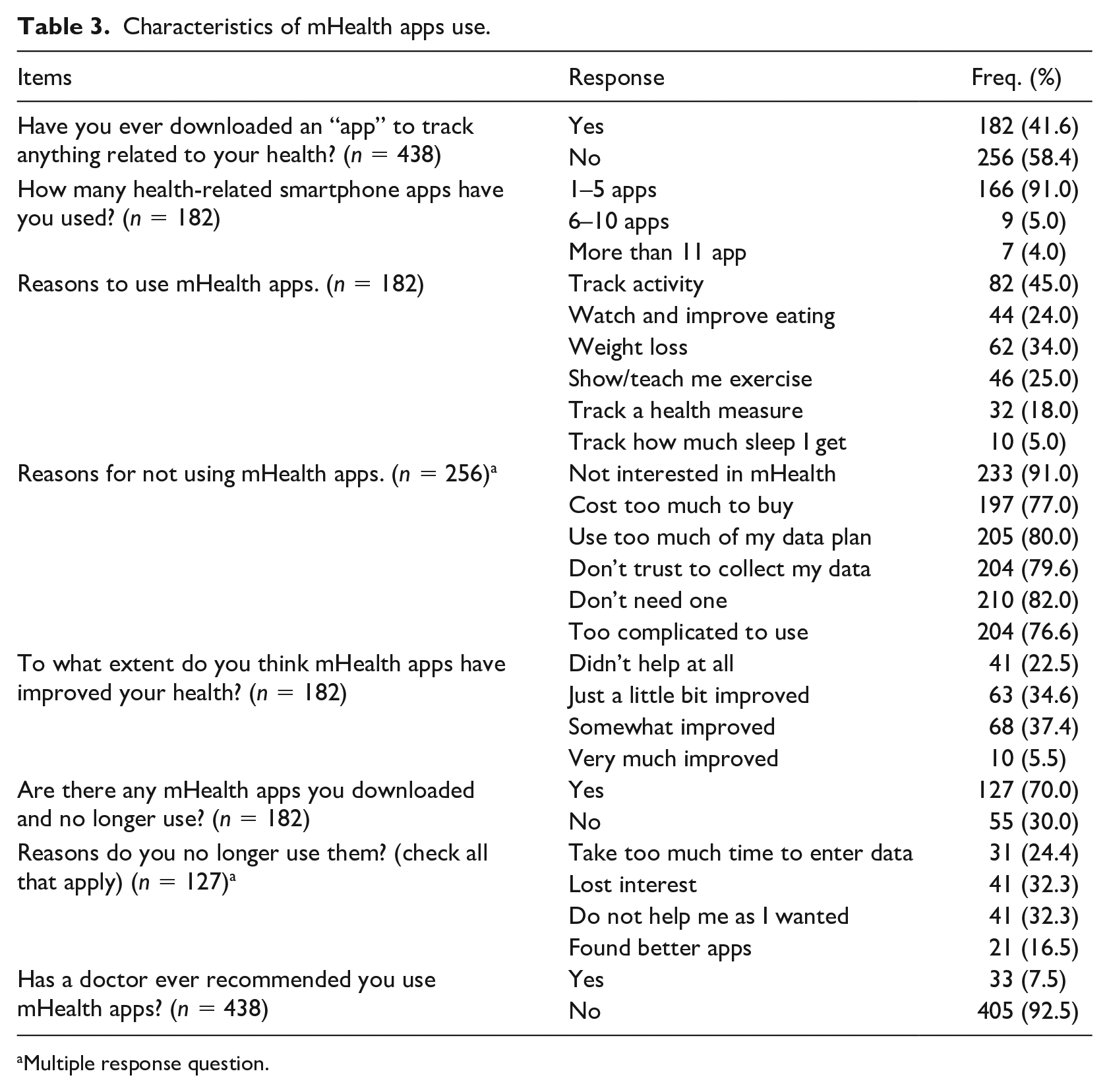
Multiple response question.
Participants indicated that they most frequently had learned of the mHealth apps via apps stores (74%), followed by friends/family (25.2%), web searches (19.8%), and health professionals (19.8%). A large proportion of the sample (79.9%) reported that they would never pay anything for mHealth apps, and the majority (92.5%) reported that physicians had never recommended mHealth apps to them (Table 3).
Approximately one third of mHealth apps downloaders (32.4%) reported that they used mHealth apps a few times a month, and 65.4% of them spent 1–10 min on days that they used mHealth apps (Figure 1).
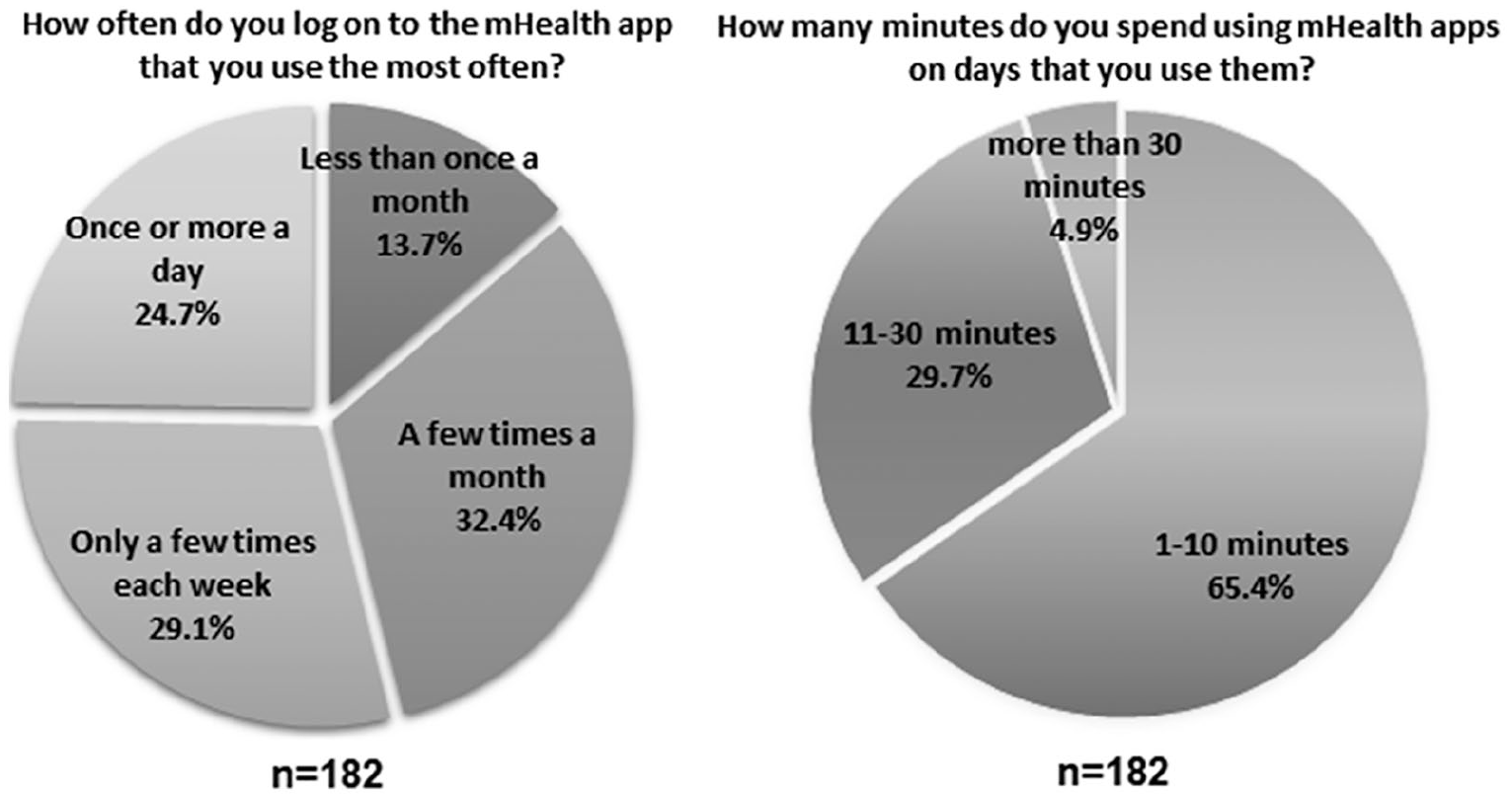
Frequency and duration of using mHealth apps (n = 182).
Among mHealth apps downloaders, 45.0% of them trusted apps to keep their data secure, 24%, 16%, and 15% reported they somewhat trusted, neither trust nor distrust, or did not trust at all the apps to keep their data secure, respectively. Similarly, 45.1% of mHealth apps downloaders reported that they neither trusted or distrusted mHealth apps to record their data accurately, while others reported that they trusted (35.5%) or did not trust (21.4%) mHealth apps to record their data accurately (Figure 2).
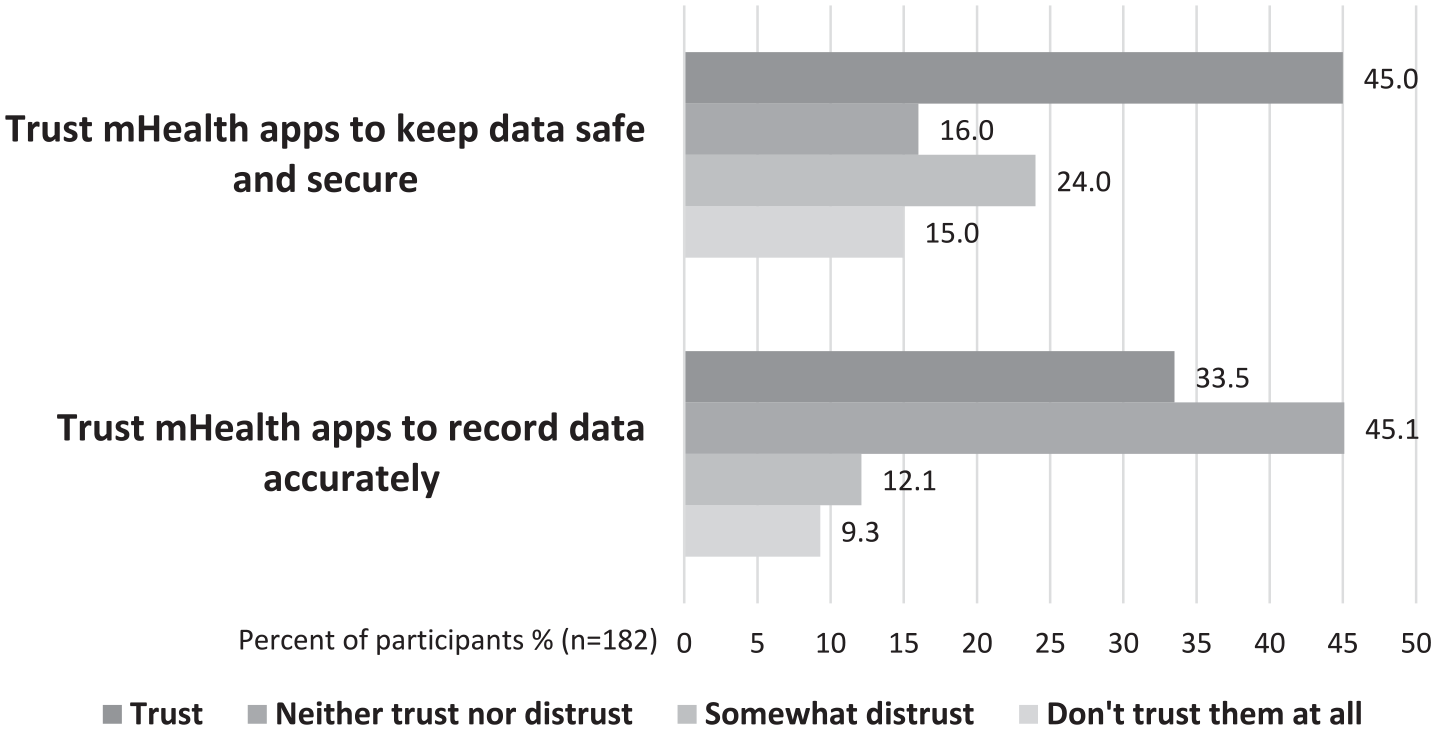
Percent of mHealth apps downloaders trust mHealth apps to record data safely and accurately (n = 182).
mHealth apps discontinuance and non-use
Among mHealth apps downloaders, 70% had discontinued their use of downloaded mHealth apps. The most frequently cited reasons for participants to discontinue the use of their mHealth apps included a loss of interest (33%), the apps did not provide anticipated support (33%), data entry took too much time (24.4%), or they had found better apps (16.5%).Of the participants who had never downloaded an mHealth app (n = 256/438), their most reported reasons for not downloading mHealth apps included a lack of interest (91%), their state of health (82%), that apps consumed too much of their data plan (80%), a lack of trust in apps to collect data (79.6%), expense of the apps (77%), and complexity of the apps (76.6%). See Table 3.
mHealth apps preference and perspective
Those participants who had downloaded one or more mHealth apps reported that mHealth apps improved their health at varying levels: 37.4% reported that they fairly improved, 34.6% reported some improvement, and 22.5% reported no improvement (Table 3).
In terms of using mHealth apps to send messages to doctors, participants either indicated that they were not very interested at all (48.1%), very interested (22.4%), or had a little interest (25.8%). Similarly, 53.2%, 20.3%, and 23.3% of participants reported that they were either not very interested at all, very interested, or a little interested (respectively) in using mHealth apps to make appointments with their doctors. Lastly, 48.2%, 21.9%, and 25.3% of participants reported that they were not very interested at all, very interested, or a little interested in using mHealth apps (respectively) to look at their medical records (Figure 3).
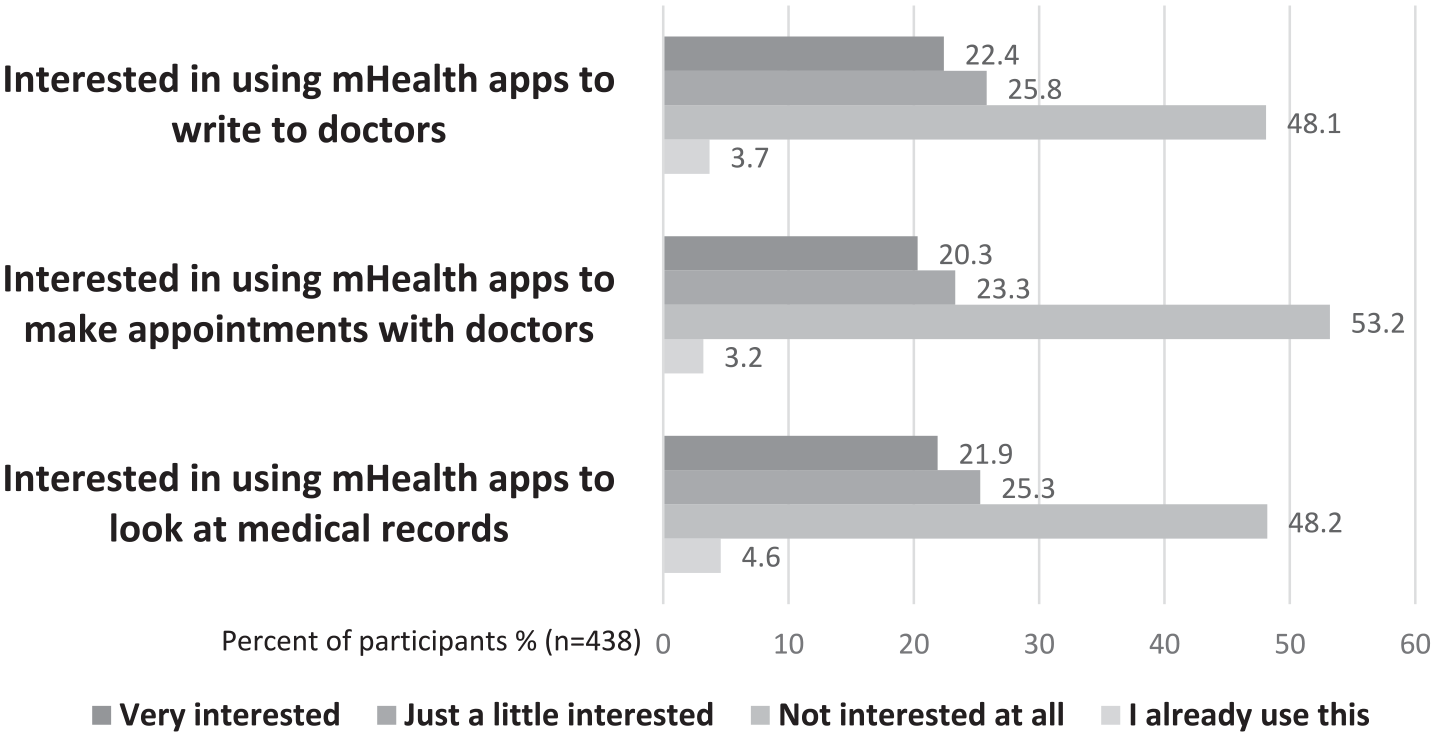
Percent of participants interested in using mHealth apps to communicate with doctors and healthcare system (n = 438).
Factors associated with mHealth apps downloads
We performed binary logistic regressions to predict the effects of gender, age, educational level, employment status, house income, BMI, perceived health status, and chronic disease (one at a time) on the likelihood that participants would have downloaded mHealth apps. We added variables with statistically significant results from the first set of models to a final binary logistic regression model. As dummy variables (used to express a nominal variable by a series of dichotomous variables that each compared one category to the reference) indicated that statistical significance across dichotomous variables of the same nominal variable was inconsistent, we created new binary dummy variables (one dichotomous variable) to represent BMI, educational level, and age. The logistic regression model was statistically significant, χ2 (20) = 37.512, p < 0.010. The model explained 12.0% (Nagelkerke R²) of the variance in downloading mHealth apps and correctly classified 63.1% of cases. Sensitivity was 43.3%, specificity was 77.6%, positive predictive value was 58.33% and negative predictive value was 65.3%. The model indicated that only four predictor variables were statistically significant: age group (p = 0.002), gender (p = 0.029), education (p = 0.022), and BMI (p = 0.015; Table 4). Results of the binary logistic regression indicated that men were less likely than women to download mHealth apps (odds ratio (OR): 0.622, confidence interval (CI): 0.405–0.953). People who were less than 40 years old were more likely (OR: 3.571, CI: 1.623–7.857) to download mHealth apps than were participants of 40 years old and above. Participants of normal BMI and above average BMI were more likely to download mHealth apps than underweight BMI participants (OR: 5.095, CI: 1.368–18.98). Participants who continued post-secondary school education were more likely to download mHealth apps than participants of secondary school or below educational level (OR: 2.155, CI: 1.115–4.167).
Multivariate correlation with downloading mHealth apps.
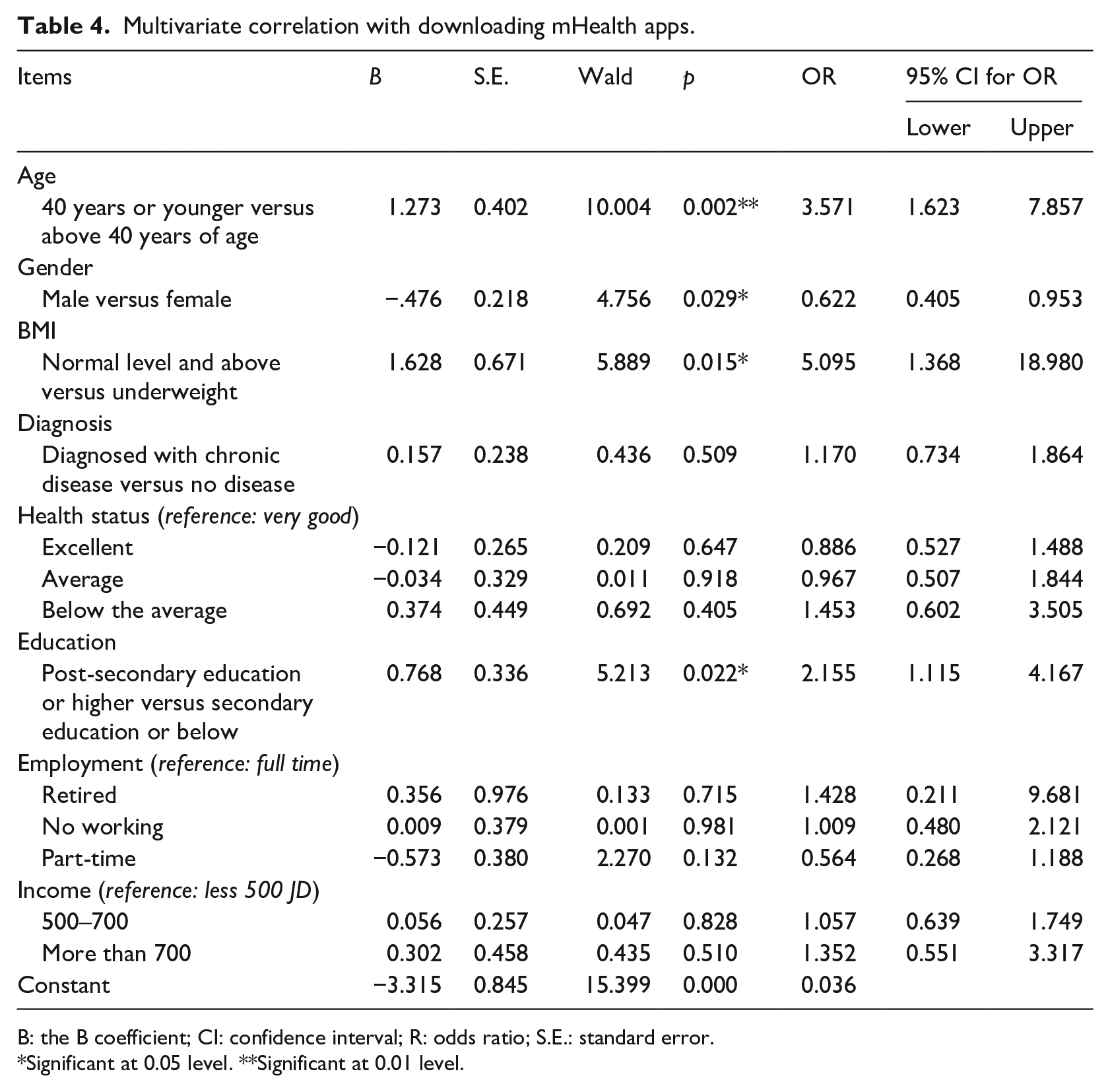
B: the B coefficient; CI: confidence interval; R: odds ratio; S.E.: standard error.
Significant at 0.05 level. **Significant at 0.01 level.
Discussion
Approximately 7–28% of adults with different chronic conditions, and 38.9% of adults without a chronic condition in the United States reported that they used one to five mHealth apps. 21 Another study from the Middle East Region indicated that 34.6% of Egyptian patients were using mHealth apps. 22 We found a relatively higher rate (41.6%) of mHealth apps use among Jordanian patients than American and Egyptian patients. Our findings were consistent with those of another survey in the United States which indicated that most participants downloaded fewer than five mHealth apps, and used their mHealth apps only a few times a week for less than 10 min. 19 We also found that most participants used their mHealth apps to control their physical activity and eating behaviors, which was consistent with the intention of other American, Egyptian, and German populations surveyed.19,22–24
Our findings were consistent with the results of Robbins et al., 21 who examined perceptions of mHealth apps among American people living with or without chronic conditions. Robbins et al. found that approximately one-third of participants reported that mHealth apps could improve health. Another survey in the United States indicated more confident outcomes and suggested that approximately two-thirds of mHealth users reported the usefulness of mHealth apps in achieving health behavior goals. 25
In the developing world, the main factors predicting mHealth apps use among patients were poor access to healthcare, limited primary health care services, a limited healthcare workforce, limited health education programs, and sub-standard healthcare quality.26,27 However, our findings showed some challenges in downloading mHealth apps among patients in the public health sector in Jordan. Most participants who had not downloaded mHealth apps reported that they were uninterested, they did not need mHealth apps, or they found mHealth apps costly and too consuming of their data plans. These findings contradicted our expectations that mHealth apps act as available tools to accessible health care resources in Jordan, but many network and financial challenges can reduce their effectiveness. Policy makers and clinical decision makers should consider the significance of these barriers in planning to develop and integrate mHealth in health care systems based on population needs and community resources.
Patients may not want some of their personal and health condition data to be available in the public domain. 28 Keeping data safe and secure in health care practice is highly important because of the sensitive nature of patients’ records, 29 thus these data should be kept secure and confidential to maintain privacy. 30 Our findings addressed the security and privacy of the personal data as an important challenge, since only about one-third of our participants trusted mHealth apps to keep their records safe and secure. Future plans to encourage patients to engage in mHealth apps use in Jordan should consider how to enhance people’s trust that their information can be kept secure.
mHealth apps can help improve patients’ relationship with their healthcare providers and health care systems by facilitating effective communication. 31 mHealth apps are considered respected channels of communication in developing countries and serve to effectively complement conventional communication strategies between individuals and healthcare providers or system. 27 Patients can communicate with healthcare providers or systems through mHealth apps to request medical consultations and information about their health conditions, make an appointment, and view their medical records.22,31,32 In Jordan, there are specific cultural values concerning the interaction of females and males. mHealth can be a convenient tool to support Jordanian people without compromising their values. Thus, women can use apps to contact their healthcare providers without presenting in the clinic. 26 However, our findings showed that using mHealth apps for communication with healthcare providers and the healthcare system is in its infancy and that Jordanians are less inclined to use mHealth apps for communication compared to people in other worldwide regions. Two-thirds of the U.S. population is interested in using mHealth apps to make appointments, communicate with their doctors, and view their medical records, 19 whereas less than half of the patients in our study were interested in mHealth apps as a communication pathway for medical benefits.
Healthcare providers could accelerate the adoption of new health technologies to improve patient engagement in health management thereby encouraging their patients toward improved health outcomes. 33 Our findings indicated that <7.5% of physicians in outpatient clinics recommended that their patients use mHealth apps. This result contradicts a report from the literature indicating that more than a third of United States physicians recommended apps to patients. 34 Health care providers could encourage people with constricted health access and resources to use mHealth apps to decrease the gap to access health care among Jordanian patients. However, healthcare providers would need to standardize their apps recommendation, and selection of mHealth apps to ensure utility, safety, and impact. 35
Our findings provided evidence that BMI, education, age, and gender differences influenced the download of mHealth apps among patients in Jordan. Our findings here were similar to surveys from the United States indicating that people who are more likely to download mHealth apps tended to be younger, more educated, and have a higher BMI.19,24 However, the results of another population-based survey in Germany contradicted our findings and showed that gender, education, and BMI were not significant predictor variables of downloading mHealth apps. 23 The educational level appears to be more important than other factors representing socioeconomic status such as income and race. 24 Educational differences may reflect skills and confidence with the use of technology and possibly social norms relevant to perceived value. 24 Regarding the age differences, older individuals are slower to accept any new technology compared to younger individuals. 15 For that reason, purposeful training in technology can increase older users’ acceptance of mHealth apps in Jordan. The reasons for gender and BMI differences are less clear, but may reflect differences in health-seeking behavior and interest in healthy lifestyle practice. 24 We also found no difference in mHealth apps download between participants with or without chronic disease, which differs from Ernsting and colleagues’ survey results indicating that individuals diagnosed with chronic conditions were more likely to download mHealth apps compared to individuals without chronic conditions. 36
Limitations
In terms of limitations, our sample was skewed toward younger and low poverty level patients. A more generalized sample across age and income would likely have yielded different results as patterns of use and preference are likely to be different in older or under low poverty level populations. One example of sampling bias is that we surveyed patients in outpatient clinics and failed to approach inpatient settings. As well, outpatients without chronic illness represented more than two thirds of the sample. Furthermore, we conducted our study in the mid region cities of Jordan where other regions and rural areas were not represented; thus, our sample did not represent patients across Jordan. As well, we did not include patients from private, university, and military hospitals in or survey. Thus, our results are limited and may not capture all potential uses or types of mHealth apps. It would be challenging to address the diverse uses and types of mHealth apps. It should be also noticed that “mHealth apps download” and “mHealth apps use” were convergent terms in our study context. We employed the term “download” to describe the actual behavior being conducted (downloading mHealth apps) and then describe the pattern of use and how participants engaged with mHealth apps.
Future research
Our study shed light on the prevalence of using mHealth apps among outpatients in Jordan, and described the characteristics and factors associated with their use of mHealth apps. Further research should be conducted to investigate additional reasons for using mHealth apps, such as managing symptoms, managing medication, or tracking blood results. To achieve this goal, researchers should address the limitations in their measurement tools to thoroughly identify the reasons for using mHealth apps among outpatients in Jordanian governmental hospitals. 21 As well, future research should include a qualitative design and usability testing to ensure the mHealth apps meet the expectations and needs of outpatients in Jordan and further define the requirements of authentic mHealth apps. 37 We found gender, age, weight, and education level were associated with level of mHealth apps use among Jordanian outpatients. Specifically, previous studies have indicated that mHealth apps use is different across age groups and genders.19,38 Researchers need to explore the potential age and gender differences in mHealth apps use and the reasons for these differences. For future research, the effects of mHealth apps use on health outcomes of Jordanian outpatients should be analyzed using longitudinal or experimental research designs. We did not report whether and how the mHealth apps usage frequency or duration improved health outcomes. Future researchers need to examine rigorously whether and how the effects of mHealth apps on health outcomes vary by usage frequency and duration. Maintaining mHealth apps use over time during future studies is a major moderator of mHealth apps effectiveness and is likely to influence participants’ long-term health outcomes. 37 We have shown that the majority of participants had discontinued their use of downloaded mHealth apps. In addition to the growing concerns about barriers to continuous mHealth apps use among outpatients and how to overcome these barriers, researchers have commented on the importance of developing assessment tools to explore the facilitators for and barriers against maintaining mHealth engagement.39,40 Future researchers, thus, should not only consider the influence of the mHealth apps on participants’ health but also monitor, analyze, and report mHealth apps use by participants. We also demonstrated that the vast majority of participants reported that physicians had never recommended the use of the mHealth apps to them. Further evidence is also needed to understand health professionals’ attitude toward and their lack of interest in mHealth apps use among their outpatients.
Conclusion
The use of mHealth apps among Jordanian patients is promising and the potential in mHealth apps is great. Health care systems in Jordan should adopt this technology and work through population needs, preferences, and characteristics, as well as the health system barriers to integrate the mHealth services in health care management plans. Moreover, mHealth apps developers should consider patients’ concerns (e.g. cost, data plan, and privacy) to increase mHealth adoption.
Footnotes
Author’s note
Anas Husam Khalifeh is now affiliated with Hittien College and Prince Hamzah Hospital, Jordan.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.