
Abstract
Patient access to electronic health records gives rise to ethical questions related to the patient-doctor-computer relationship. Our study aims to examine patients’ moral attitudes toward a shared EHR, with a focus on autonomy, information access, and responsibility. A de novo self-administered questionnaire containing three vignettes and 15 statements was distributed among patients in four different settings. A total of 1688 valid questionnaires were collected. Patients’ mean age was 51 years, 61% was female, 50% had a higher degree (college or university), and almost 50% suffered from a chronic illness. Respondents were hesitant to hide sensitive information electronically from their care providers. They also strongly believed hiding information could negatively affect the quality of care provided. Participants preferred to be informed about negative test results in a face-to-face conversation, or would have every patient decide individually how they want to receive results. Patients generally had little experience using patient portal systems and expressed a need for more information on EHRs in this survey. They tended to be hesitant to take up control over their medical data in the EHR and deemed patients share a responsibility for the accuracy of information in their record.
Introduction
Worldwide, there is a strong move toward the digitalization of medical records. In Europe, 27 EU member states had implemented a national electronic health record (EHR) system by 2015. 1 Digitalization generally serves two goals: to create a central source of patient information (either with a national EHR or by connecting local systems through increased interoperability) and to facilitate patient access to the record. Although personal health records (PHRs), patient accessible electronic health records (PAEHRs) and patient portals differ in structure and level of patient-centeredness, they all aim to promote patient engagement and activation.2–5 Implementation of patient access comes with great expectations of improving health outcomes and reducing costs. So far, evidence for these positive effects has been rather limited. Patient safety is improved through the identification of medication errors,6,7 and some studies also find other benefits such as improved patient satisfaction and engagement, and increased medication adherence.3,6–10 Evidence of a positive effect on health outcomes also remains scarce.3,11,12 The global Covid-19 pandemic has rapidly accelerated the digitalization of health care systems and patient-provider interactions, resulting in an even more urgent need to study the effects of this implementation.
Studies examining patients’ perceptions of shared EHR systems have mainly focused on general attitudes or have covered privacy, security, and access issues.13–18 However, wide implementation of patient access also raises ethical questions related to the patient-doctor-computer relationship. We will focus on three ethical topics in this study. The first question concerns patient autonomy, understood as the level of control patients should have over their record. Patients could be extended granular control over their data: this means they would be able to decide who gets access to their record, and which information is or is not made available. The latter question most often arises concerning sensitive information. Some studies show patients prefer granular control, others find only a minority of patients actually restrict access when they have that option available.15,19–22 Second, there are many different ways in which results are released to patients, with variations in timing, type and presentation of information.23–25 Although patients preferred to have direct access to results in one study, they also acknowledged the risk of increased anxiety. 24 Another study found participants preferred face-to-face or phone contact to hear about their results if these could be released in a timely manner. 25 Third, questions arise about responsibility for the accuracy and completeness of available health data in the context of a shared EHR.26–28 Who is responsible when errors cause medical problems in a digital record where patients have granular control and multiple care providers contribute to the record’s content?
We argue it is important to take into account patients’ views to develop (PA)EHR systems that are both ethically sound and patient-centered. 29 Therefore, this study examines patients’ moral attitudes toward a shared EHR, with a focus on autonomy, information availability, and responsibility. To our knowledge, this is the first survey study that explores patients’ views on these ethical questions in the specific context of a shared EHR.
Materials and methods
This study aimed to reach a diverse patient population in a cross-sectional survey conducted in one Belgian province (East-Flanders). Belgium has a tax-funded, mandatory health insurance system comparable to other European countries. The majority of primary care physicians and hospitals have digitalized their records and a national EHR system is in place.30,31 Although patient access has been available for some years at the level of individual healthcare organizations, a national patient portal was just recently implemented. 31 As is the case in other countries, many different types of care providers interact with the EHR, for example, doctors, nurses, and pharmacists, to name a few. However, the main focus of this survey will be on the patient-doctor relationship.
Questionnaire design
The survey consisted of four parts (see Supplemental Appendix A). First, participants were presented with three vignettes or cases, which allowed us to present moral dilemmas in the form of a story, describing key factors more elaborately.32–34 The vignettes were informed by both literature and clinical experience and focused on autonomy, responsibility, and results release. The second part of the questionnaire was comprised of 15 randomly ordered statements covering the same topics in a more general and abstract manner using a 5-point Likert scale. Two of the 15 statements probed different topics: impact on quality of care and privacy compared to paper records. In a third part, consisting of 10 questions (either in a multiple choice or binary form), participants’ experience with and view of EHRs was explored. The last question of this section probed health literacy using the single item literacy screener. 35 The fourth part of the questionnaire collected socio-demographic and medical information.
Although this was set up as an exploratory study, several measures were taken to ensure face and content validity. Face validity was tested with a pilot study conducted among students and personal contacts of the research team, most of which had no experience with EHRs or patient portal systems. Two rounds of piloting and revision were conducted with a total of 25 pilot participants. They completed the questionnaire and provided qualitative feedback on the statements. Content validity was ensured in two steps. First, all co-authors (among which GPs, ethicists, and philosophers) thoroughly examined all vignettes and statements. Second, an exploratory factor analysis of the statements with Cronbach’s alpha was conducted on the complete data set (see “Statistical analysis”). The study was approved by the ethics committee of the University Hospital Ghent (2018/0166).
Data collection
To maximize variability in patient participants, surveys were collected in four different settings between March and December 2018. These settings were waiting rooms of a tertiary hospital, GP surgeries, social services of two national health insurance funds, and the Flemish Patient Platform, an organization which unites and supports more than 100 individual patient organizations. More information on the sampling process can be found in Table 1. To increase accessibility to the survey, either an online survey (LimeSurvey) or a paper questionnaire was used according to the setting. In the case of paper questionnaires, participants were recruited through a consecutive sampling process carried out either by a researcher (LC, in the hospital), by doctors or administrative personnel (GP surgeries) or both (health insurance funds). To maximize variability, GP surgeries were selected based on their location (city, village or rural) and type of practice (solo practice, duo/group, or multidisciplinary practice). The social services of two national health insurance funds were chosen specifically to include more vulnerable patients.
Overview of the sampling locations, types and number of questionnaires distributed, and number of valid questionnaires collected.
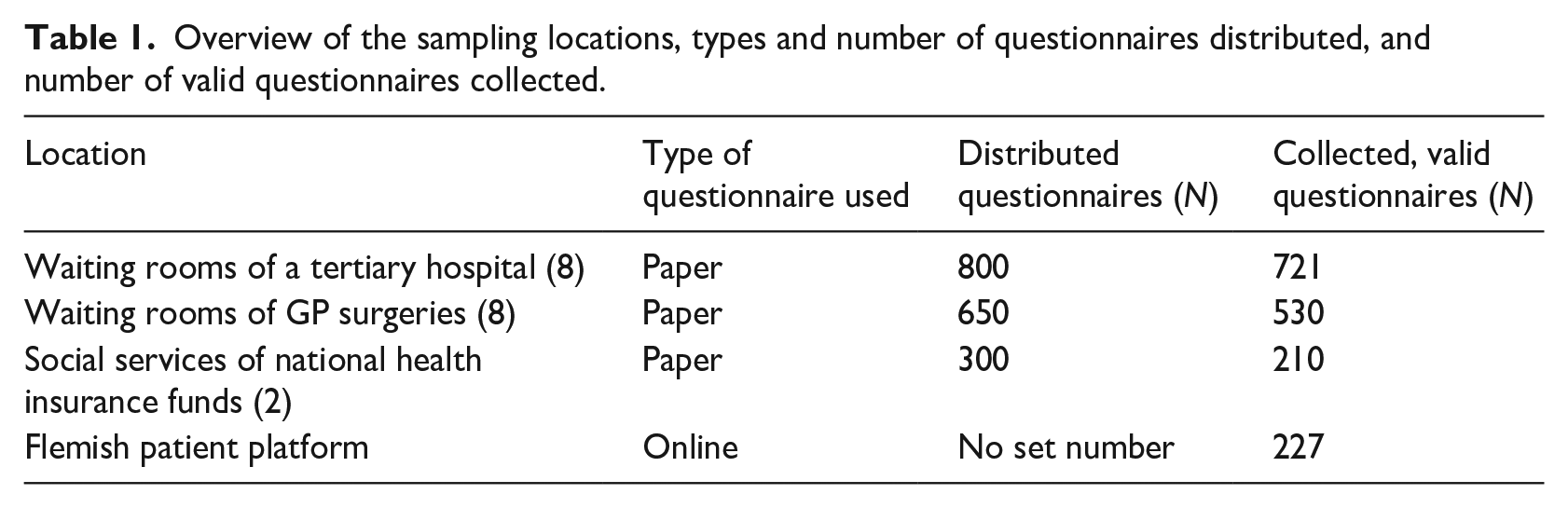
Because of this specific design, no data were collected on non-responders. Eligible participants were at least 18 years old and able to understand the survey questions (Dutch language proficiency). No previous experience with (PA)EHRs was required: the questions were adapted to include patients with a wide range of experience. Participation was anonymous and voluntary.
Statistical analysis
All paper questionnaires were digitalized for use in SPSS (version 25). Questionnaires with missing socio-demographic information were excluded from the sample. Descriptive statistics were used first to explore participants’ responses. Secondly, we analyzed the fifteen statements in an exploratory factor analysis (principal components analysis with varimax rotation), to examine whether or not the resulting factors would correlate with our predetermined themes 36 . This analysis was based on Pearson’s correlation (adhering to an intervalist position that this parametric test is rather insensitive to violations of the normality assumption) and Cronbach’s alpha was used to examine internal consistency and thus test reliability37,38,39 Lastly, a multiple logistic regression analysis was performed to explore associations between responses to questions focusing on autonomy and participants’ sociodemographics.
Results
Characteristics of the study population
A total of 1688 valid questionnaires were collected. The socio-demographic information of the survey population is shown in Table 2. Mean age was 51 years (18–89), 61% was female, and half of the population had a higher degree (university or college). Although 50% of participants stated they suffer from a chronic illness, only 11% perceived their health status as poor or very poor.
Demographics of the population with self-perceived health status, medication use and health literacy (N = 1688).
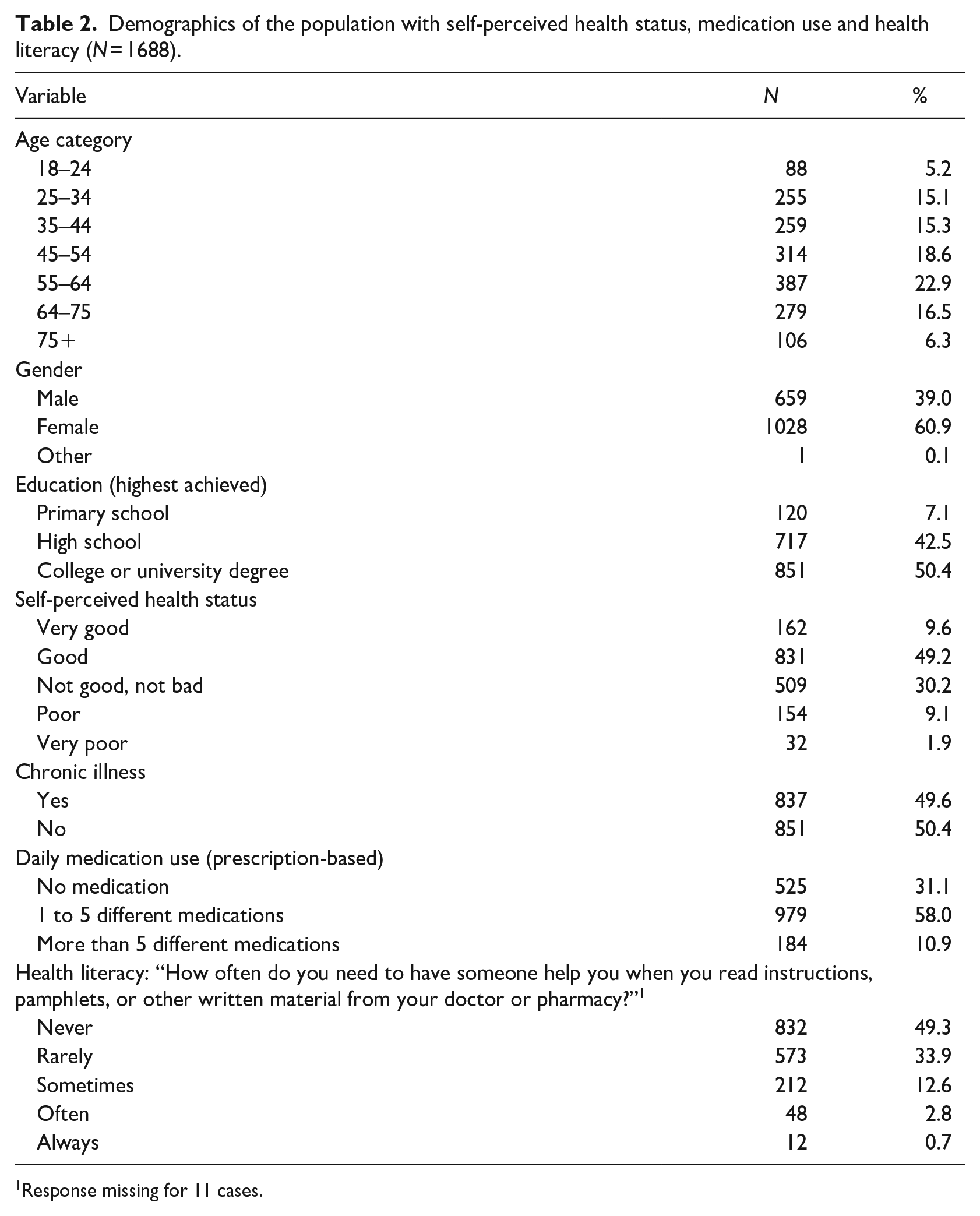
1 Response missing for 11 cases.
A large majority had already heard about EHRs, most often through the media, their GP or the hospital. A very small minority stated they had never heard about EHRs before. Most had access to the internet and had used it to look up medical information. A little over half of the participants had made online appointments with their doctors in the past. Experience with patient portal systems was rare, varying between 4.7% and 5.5% depending on the system. While 61% had given their informed consent to share information digitally, almost 70% of participants said they need more information on EHRs. Table 3 shows the patients’ experience with EHR and digital applications in more detail.
Experience with EHRs and digital applications (N = 1688).
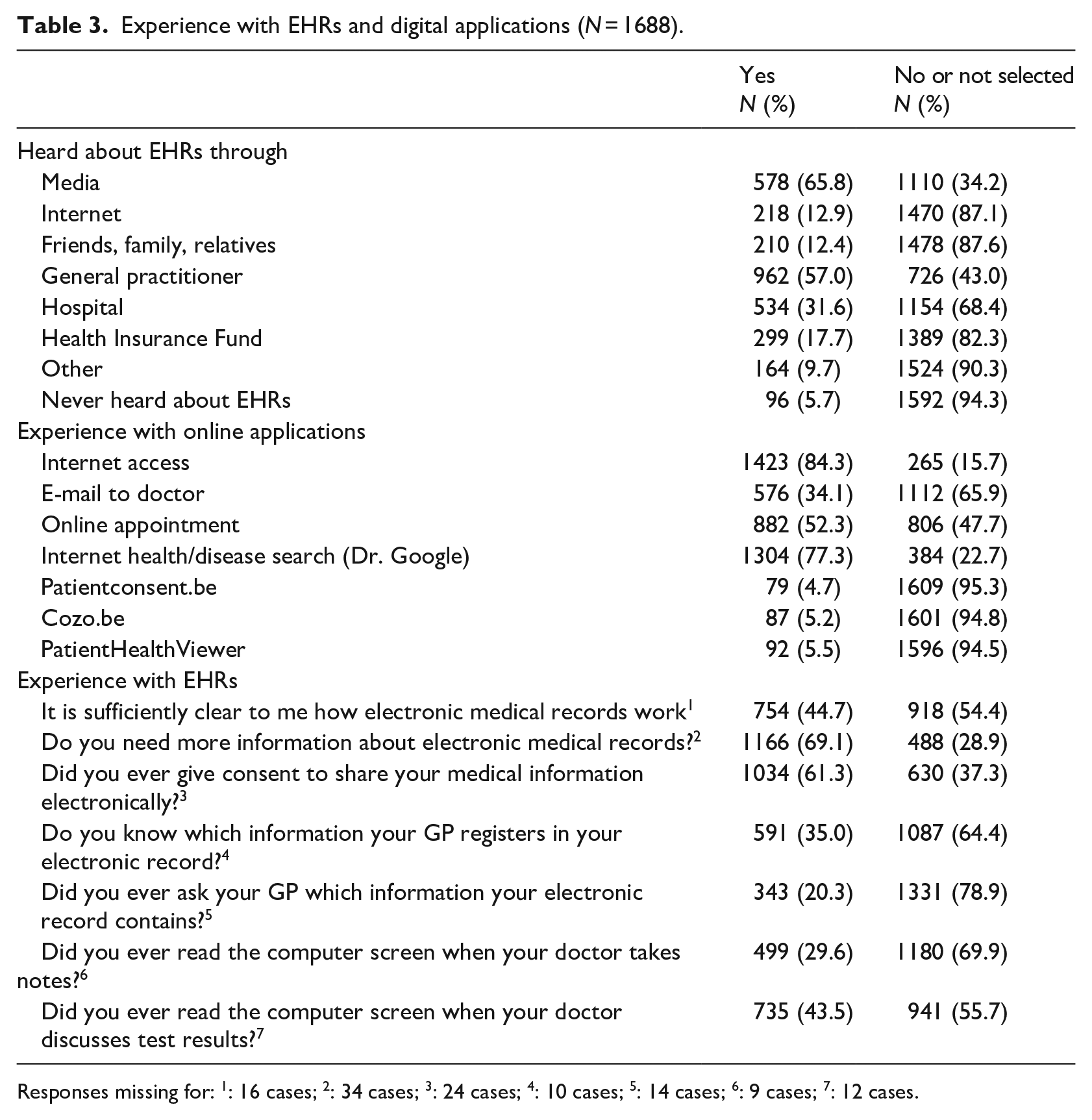
Responses missing for: 1: 16 cases; 2: 34 cases; 3: 24 cases; 4: 10 cases; 5: 14 cases; 6: 9 cases; 7: 12 cases.
Patients’ moral attitudes toward the EHR
Table 4 provides an overview of the responses to the vignettes, while Table 5 shows the answers to the statements. We will discuss the results along the three themes of autonomy, responsibility and information availability.
Participants’ responses to the presented vignettes (N = 1688).
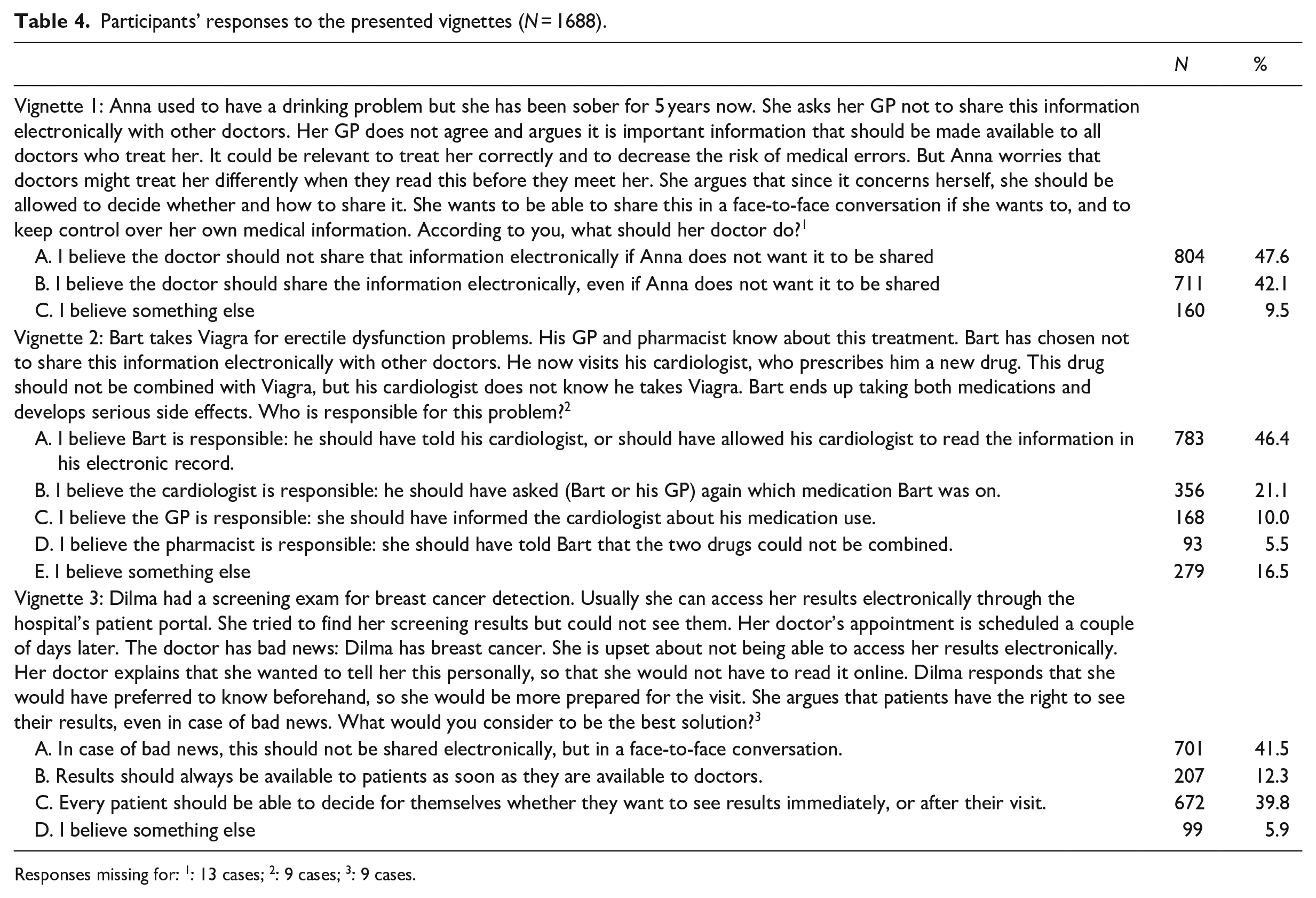
Responses missing for: 1: 13 cases; 2: 9 cases; 3: 9 cases.
Participants’ responses to the statements (N = 1688).
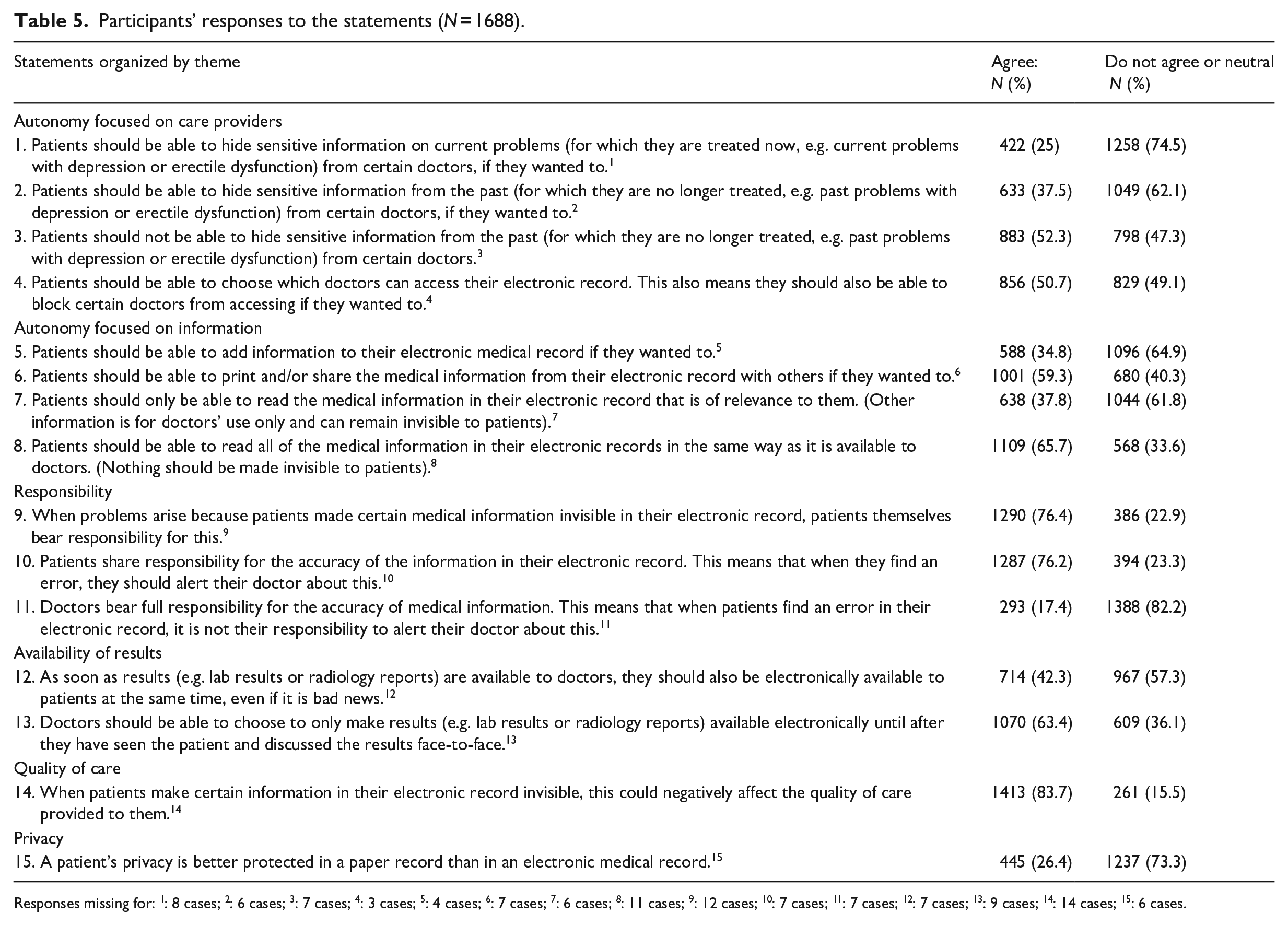
Responses missing for: 1: 8 cases; 2: 6 cases; 3: 7 cases; 4: 3 cases; 5: 4 cases; 6: 7 cases; 7: 6 cases; 8: 11 cases; 9: 12 cases; 10: 7 cases; 11: 7 cases; 12: 7 cases; 13: 9 cases; 14: 14 cases; 15: 6 cases.
Autonomy
While almost 48% of participants preferred to give the vignette case patient granular control over her information, 42% thought the doctor should share the information despite the patient’s objection. Patients who chose neither of these options often suggested to discuss the consequences of hiding information more in-depth with the patient.
Respondents were reluctant to hide sensitive information from their doctors electronically, more so in the case of current illness than for information on past problems (25% and 37.5%, respectively). Half of the participants thought patients should be able to control which doctor has access to their record. They were rather hesitant toward the ability to add information to their record. However, two thirds (65.7%) preferred to be able to read all information in the EHR without anything remaining hidden from them.
Responsibility
About 46% singled out the patient as responsible in the second vignette. Conversely, almost 37% of the patients considered one of the care providers responsible for the situation. Quite a large group of 16.5% turned to the open answer, of which almost all suggested a shared responsibility between the patient and one or more care providers, or between multiple care providers.
The trend to assign (a shared) responsibility for the information in the EHR to patients upholds in the statements as well, and even more strongly so, where 76.2% believed patients to be accountable for negative consequences resulting from hiding information and agreed to patients bearing a shared responsibility for the accuracy of information in their record. Only 17.4% considered doctors solely responsible for the accuracy of information. A large majority (83.7%) believed that hiding information could negatively affect the quality of care provided.
Information availability
Only a small minority of participants (12.3%) preferred to have results directly released to the patient in the vignette. In this specific case of “bad news,” 41.5% preferred a face-to-face conversation. A similar proportion (39.8%) thought a patient should be able to choose how they want to be informed. In the statements section, almost two-thirds of the respondents agreed to the proposal that doctors should be able to delay electronic results release until after a visit. However, 42.3% would prefer immediate release when given the option, even in the case of bad news.
Factor analysis
We analyzed the 15 statements in an exploratory factor analysis, to examine whether or not the resulting factors would correlate with our predetermined themes. First, the factorability of the items was checked. Bartlett’s test of sphericity was significant (χ2 (105) = 4640.72, p < 0.001), and the Kaiser-Meyer-Olkin measure of sampling adequacy was .74, suggesting it was acceptable to proceed with the analysis. Also, communalities were all above .3, confirming that each statement shared some common variance with other statements. Principal components analysis was performed and identified five factors with initial eigenvalues greater than 1. A varimax rotation was applied based on the component correlation matrix of an oblimin solution where none of the values was greater than .5. The component matrix is added in Table 6.
Factor loadings and communalities based on a principal components analysis with varimax rotation for the 15 statements used in the questionnaire.
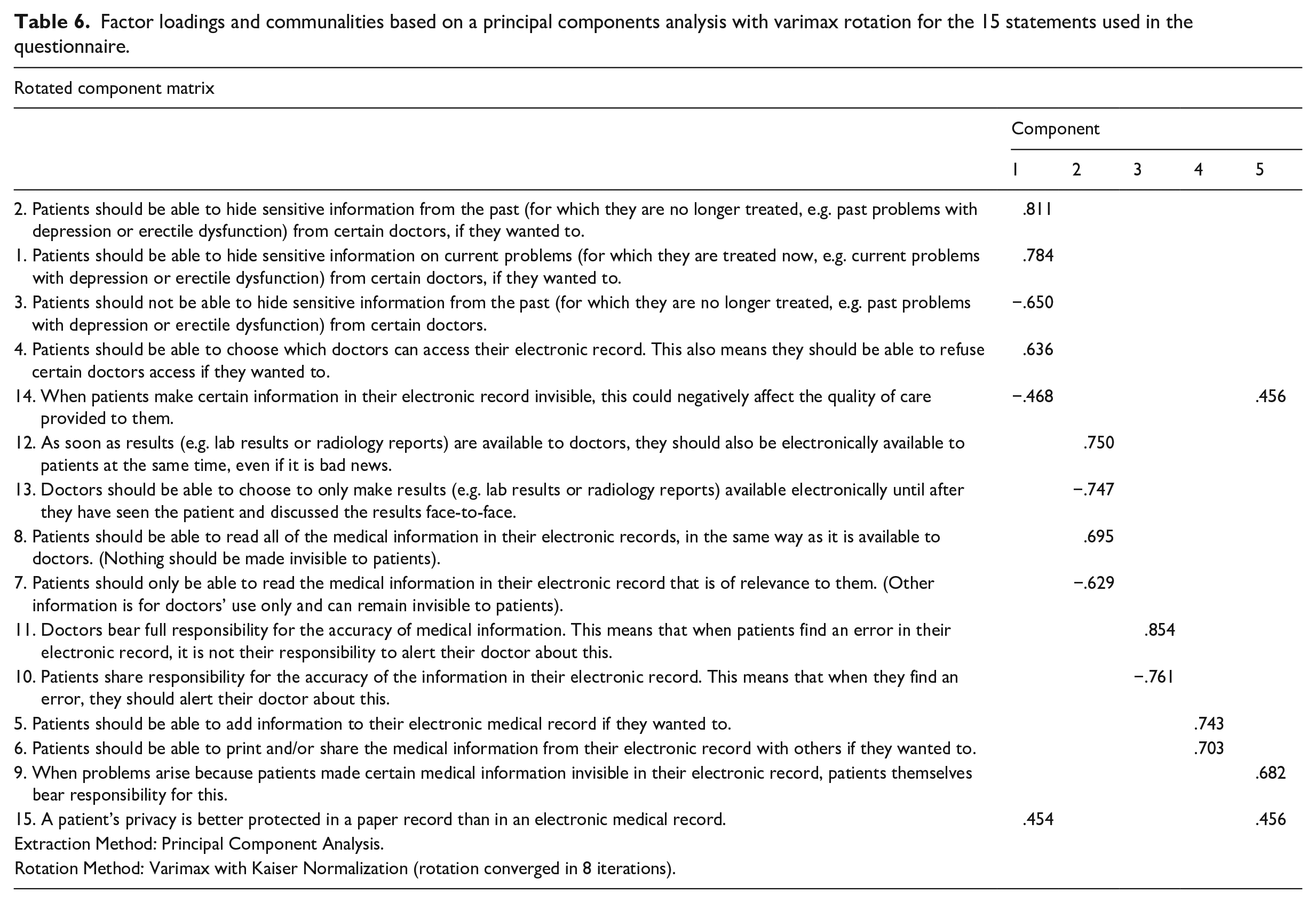
All five factors combined explained 59% of the variance. The first factor had an eigenvalue of 3.22, accounting for 21.5% of the variance in the data and was labeled “autonomy related to care providers.” The second factor accounted for 13.1% of the variance with an eigenvalue of 1.97, being identified as “information access,” while the third factor accounted for 10% of the variance. This factor was labeled “responsibility.” Factors 4 and 5 both had eigenvalues just over 1 and each accounted for 7% of the variance. Factor 4 was called “adding or sharing information,” while factor 5 did not have a clear consistent theme, so we did not take it up into further analyses. The internal consistency for each factor was examined using Cronbach’s alpha. The internal consistency for the first factor was high when item 14 was deleted (Cronbach’s alpha of .76). The second factor had a moderately good consistency of .685. The alpha’s for factors 3 and 4 were lower, suggesting a low reliability (.59 and .39, respectively).
Overall, the theme of autonomy with a focus on care providers was confirmed in this analysis, as was the “information access” theme, although the latter included both results release and access to information (broader than our original theme definition). The responsibility theme did not have a good internal consistency in this factor analysis.
Associations with sociodemographic characteristics
In the final analysis part, we wanted to examine associations between respondents’ answers to the statements and their sociodemographic characteristics. Because the items focused on autonomy showed a good internal consistency in the exploratory factor analysis and matched our predetermined theme, we conducted a binary logistic regression with these statements (1–4) as outcome variables. The model included gender, age, education, self-reported health, and chronic illness as independent variables. Two variables were consistently and significantly correlated with the questions probing autonomy. Participants with a higher degree and patients with poorer self-reported health preferred to have more granular control over their medical record (overall p < 0.01).
Discussion
Compared to similar Belgian study populations, our population had a higher proportion of patients with self-reported chronic illness and poor health.40–42 Although the study population is well-educated and most have already heard about EHRs, almost 70% state they need more information. Moreover, only a very small minority have already used one of the patient portal systems (between 4.7% and 5.5% depending on the system) despite the fact that they have been available for quite some time. In Belgium, the existence of different types of patient portals and different system layers might confuse patients. Assuring patients have information about the system and know how to access it, will be a crucial first step: the launch of the national patient portal could positively influence patient engagement. In the Netherlands, the eHealth monitor reports a patient portal use between 2% and 8% among respondents, which is similar to our study, while a Dutch study at a university hospital reported that about a third of participants identified as portal users.43,44 Further research could explore portal adoption barriers—privacy concerns and lack of encouragement of providers have already been identified in previous studies. 3
Participants were generally reluctant to give patients granular control over their EHR data. This differs from other studies where patients preferred to have granular control over their electronic information.15,20 Moreover, almost all (84%) patients agreed that hiding information in the electronic record could negatively impact the quality of care that is provided to them, and 76% agreed that patients themselves are responsible when problems arise due to information being hidden. Both the allocation of responsibility and limitation of granular control are more pronounced in the statements section than in the vignettes, although the trend is similar. We argue that patients consider information disclosure essential to the patient-doctor interaction and to their quality of care. They believe that more information leads to better care, and consider patients responsible for providing that information. We speculate that Anna’s story of the first vignette may introduce some doubt: it raises the question whether more information, especially about sensitive topics, could actually decrease the quality of provided care. In an era of digital information exchange, this gives rise to interesting questions. Could hiding (sensitive) information electronically and disclosing it within a face-to-face conversation improve quality of care in some cases? And with a broader circle of access, can care providers and patients still accurately judge which information is or will be relevant in the EHR?
These questions also relate to the topic of information availability: should we digitally share test results with patients in a more comprehensible way? Participants in our study preferred to hear about bad news in a face-to-face conversation, although more strongly in the vignette than in the statements, or they would allow each patient to choose for themselves how they want to be informed. A mixed methods study recently found that patients often miss an explanation or interpretation when reading results online, suggesting the results are not presented to patients in a meaningful way. 45 Others studies have also emphasized that provider interpretation is beneficial to patients. 24 We speculate that patients first and foremost want access to comprehensible and meaningful information—be it in real-life or digital—and that reading results online could lead to increased anxiety if patients feel they are “on their own” in the patient portal system.
Limitations
This exploratory research project has five major limitations. First, we did not collect information on non-respondents. This choice was deliberate, to limit the burden put on medical personnel who recruited participants for the study. Second, we received feedback from social workers recruiting participants that the study was too difficult and too demanding for vulnerable patients with a low literacy. This type of feedback is very valuable and mostly lacking in similar research projects. Third, the setting of the study limits the transferability to other regions or countries, and more research is needed to conform these findings elsewhere. Fourth, a risk of over-dimensionalization occurs by applying factor analysis to Likert scale data. 46 We adhere to the assumption that parametric tests can be utilized on Likert scale (ordinal) data, but acknowledge the long-standing debate on this topic.37,38,39 Lastly, the content and method of this study were developed based on clinical experience and literature research, resulting in the development of a new questionnaire used within an exploratory research setting. This de novo instrument turned out to have a rather low internal consistency for the responsibility theme. We would suggest future research to focus on the development of a validated instrument based on this exploratory survey, providing a more in-depth exploration of the themes of autonomy and access to information. This validated survey could help to monitor whether patients’ views change due to the current global pandemic’s impact on digitalization in health care.
Conclusion
This study examined patients’ moral intuitions concerning digital information sharing and the EHR. First, participants strongly believe that hiding information could negatively affect quality of care. Second, they hold patients accountable for negative consequences of hiding information and think patients share responsibility for the accuracy of EHR data. And third, our study population does not strongly favor direct results release through a patient portal but prefers either result discussion during a visit or an individual choice option. Patients with poor health or a higher education level seem to value autonomy the most. Considering participants’ lack of experience using patient portal systems and their need for more information about EHRs, efforts should be tailored toward better informing and educating patients about these electronic systems.
Supplemental Material
sj-pdf-2-jhi-10.1177_1460458220980039 – Supplemental material for Patients’ moral attitudes toward electronic health records: Survey study with vignettes and statements
Supplemental material, sj-pdf-2-jhi-10.1177_1460458220980039 for Patients’ moral attitudes toward electronic health records: Survey study with vignettes and statements by Tania Moerenhout, Ignaas Devisch, Laetitia Cooreman, Jodie Bernaerdt, An De Sutter and Veerle Provoost in Health Informatics Journal
Research Data
sj-zsav-1-jhi-10.1177_1460458220980039 – for Patients’ moral attitudes toward electronic health records: Survey study with vignettes and statements
sj-zsav-1-jhi-10.1177_1460458220980039 for Patients’ moral attitudes toward electronic health records: Survey study with vignettes and statements by Tania Moerenhout, Ignaas Devisch, Laetitia Cooreman, Jodie Bernaerdt, An De Sutter and Veerle Provoost in Health Informatics Journal
Footnotes
Acknowledgements
We want to thank all participating doctors, medical and administrative personnel, participants in the pilot study and respondents for the time and effort they invested in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.M. was supported by the Research Foundation Flanders—Fonds Wetenschappelijk Onderzoek [Clinical PhD Fellowship grant number 1700618N]; J.B. was supported by the King Baudouin Foundation [grant number: 2017-J5810430-207488].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.