
Abstract
The article investigates the paradoxical success of a Danish telehealth project introducing the “My Pathway” platform to reduce the length of patient stays while maintaining patient satisfaction. These goals were achieved in the project, which was considered successful despite the lack of actual platform usage. Based on a qualitative, longitudinal case study we investigate this paradox by showing how barriers and facilitators have influenced telehealth adoption and use in the post-implementation process, affecting the overall success of the project. The study makes two contributions. First, it describes dynamics of adoption barriers, that is, that barriers are interrelated and influence adoption to varying degrees over time. Adoption barriers resulted in the telehealth platform not being used and it consequently only influenced the actual project success and goal achievement indirectly. Second, it highlights information management as a critical facilitator in telehealth adoption and use. Information management facilitated achievement of project goals despite the lack of actual use of “My Pathway,” which explains the paradoxical project success. Based on these interpretations, we point to information management as a critical facilitator of the success of telehealth initiatives and provide recommendations for research and practice.
Keywords
Introduction
Information and Communication Technology (ICT) is increasingly being used to provide healthcare services worldwide. Extant literature describes ICT in terms of electronic health (eHealth), mobile health (mHealth), digital health, telehealth, and telemedicine.1–4 According to the World Health Organization 4 (p. 9), telehealth is defined as “the delivery of healthcare services, where distance is a critical factor, by all healthcare professionals using information and communication technologies for the exchange of valid information for the diagnosis, treatment, and prevention of disease and injuries.” Such healthcare services may be delivered through digital platforms.
In 2014, Silkeborg Regional Hospital introduced the digital platform “My Pathway” as part of a larger telehealth project. The goal of the project was to improve patient care by providing enriched and timely information to patients undergoing total hip replacement (THR) while seeking to reduce the length of inpatient stays (LOS) and increase patient satisfaction. 5 Paradoxically, the goal was achieved although healthcare professionals refrained from actively using the platform.5,6 We investigate the paradoxical success of this telehealth project and address knowledge gaps in extant literature.7,8
Extant literature shows that adoption of telehealth helps transform and improve healthcare delivery.1,9–12 More specifically, telehealth contributes to greater efficiency while increasing the quality of care and reducing LOS. 1 As a result, patients spend more of their recovery time at home, and telehealth promises to improve the patient-healthcare professional relationship and communication during the postoperative period. 13 While there is widespread agreement on the potential benefits of telehealth for both patients and healthcare professionals, 12 the benefits have been realized at a much slower pace than anticipated. 14 In recent years, a number of telehealth studies have been published that describe the difficulties and complexities of telehealth projects. Hence, an extensive body of literature has focused on barriers10,15–17 and facilitators2,9,17,18 that influence telehealth adoption and use.
Whereas extant literature describes barriers and facilitators as static, our study contributes a dynamic perspective and show that (1) barriers are interrelated and exert varying degrees of influence over time, and (2) information management plays a central role in overcoming the barriers and achieving telehealth success. To that end, we address the following research question: How have barriers and facilitators influenced telehealth adoption and use during the post-implementation period? In the end, our study reveals that the dynamics of various adoption barriers, combined with information management as a critical facilitator, helped ensure telehealth success despite lack of technology use.
Barriers to telehealth adoption and use
Recent literature reviews of barriers to telehealth adoption and use reveal obstacles across organizational levels and stakeholders, 10 and identify technical, behavioral, economical, and organizational barriers. 19 Complemented by our own systematic literature search, we identify the following barriers as the most frequently reported in the telehealth literature: lack of technical skills, support, and training; lack of resources; lack of organizational communication; perceptions of impersonal care; perceptions of unprofessional care; concerns for privacy and security; rules and regulatory compliance; and resistance to change. Other less frequently reported barriers in the literature include lack of interoperability 20 and process redesign 21 as well as conflicting interests between different stakeholders. 22 Some studies focus narrowly on organizational barriers, such as “the health service provider’s resistance to changing existing practice; tensions between clinical and ethical processes; an unyielding organisational structure; and protectiveness of the traditional patient–clinician relationship” (p. 67). 23
Lack of technical skills, support, and training is frequently reported as an obstacle to telehealth success.1,10,15,16,24–27 Koivunen and Saranto 16 cite limited telehealth experience as a barrier in addition to inadequate skills and support, which suggests that insufficient resources are allocated to implement and integrate telehealth in practice. Thus, lack of resources in the form of requisite investments in changing work practices to accommodate new technologies makes telehealth projects time-consuming and risky.7–9,15,16,27,28 Lack of organizational communication challenges the adoption and success of telehealth technologies.2,7,8,10,16,27 According to Faber et al., 7 the consequences of limited organizational communication include lack of guidelines to and standards for telehealth implementation. In the absence of communication and the consequent ignorance of planned and ongoing projects, healthcare professionals are unable to promote greater use of telehealth. 10 Replacing face-to-face communication and interaction with telehealth2,10,16,25 may create perceptions of impersonal care among both patients and healthcare professionals. In turn, telehealth may foster perceptions of lower-quality care because of the changing relationship between healthcare providers and patients. Moreover, the use of technology in clinical practice may instill in healthcare professionals perceptions of unprofessional care.8,9,15,16 Koivunen et al. 16 report that healthcare professionals feel uncomfortable using technology as part of their clinical practice when technical issues undermine their professional authority. More generally, extant literature documents adoption challenges whenever there is a change in focus from patient care to technical aspects of using telehealth. In addition, perceptions of unprofessional care induce stress and a sense of lack of control. 16 Other barriers are associated with concerns for privacy and security of personal data1,7,10,11,25,28–31 and constraints related to rules and regulatory compliance1,3,7,10 that make it less economically desirable to invest in telehealth. Finally, resistance to change among both patients and healthcare professionals is a common barrier to telehealth adoption and use.1,10,15,16
Facilitators in telehealth adoption and use
While telehealth has the potential to transform and improve healthcare, there is a gap between envisioned benefits and clinical reality. 9 To realize the potential benefits, extant literature points to several facilitators that influence telehealth adoption and use. In the following, we describe and categorize these facilitators as: system performance quality; managerial support; effort expectancy; quality of care; trust; empowerment; time; and support.
A high level of system performance quality is the most frequently mentioned facilitator in the telehealth literature. The level of quality depends on the content, data accuracy, usefulness, degree of flexibility, and system reliability.11,25,26,28 Managerial support constitutes another critical facilitator. 25 This facilitator helps ensure healthcare professionals’ long-term commitment as well as sufficient resources and support for telehealth adoption and use.7,16 Another frequently mentioned facilitator is effort expectancy,11,25,26,28 which is directly related to the ease of using technology. According to Nisha et al., 11 it is particularly influential during the early stages of technology adoption. Similarly, several studies show trust to have a direct, positive effect on intention to use and the perceived value of a technology.11,26 Trust also mediates success by influencing the above-mentioned facilitators and thereby indirectly impacts telehealth projects.11,26 The ability to locate and control relevant health information when needed leads to empowerment of patients. Empowerment is synonymous with enabling patients to assert control and independently decide on appropriate behavior and treatment measures.2,32,33 Safi et al. 2 claim that patients are more enthusiastic about telehealth than healthcare professionals because it affords them greater autonomy during the treatment process. Yet another facilitator is time. Gagnon et al. 25 argue that professionals may believe that telehealth saves time by supporting efficient communication, while Taylor and Coates 27 posit that time for experimentation with technology is essential to figuring out how to use telehealth in daily work practices. Finally, support from, for example, a telehealth champion to troubleshoot problems and disseminate information has a positive effect on the integration of technology into clinical practices. 27
While some studies have established a mediating relationship between facilitators,11,26 extant literature portrays barriers as static entities and fails to clarify how they relate to each other and change over time. Although Faber et al. 7 recognize telehealth adoption and use as a non-linear process due to a noticeable decline in commitment after an initial stage of interest, they do not describe whether barriers follow a similar non-linear, evolutionary process. They emphasize, however, a need for longitudinal studies of how different factors influence telehealth adoption and use over time. 7 Ross et al. 8 postulate a gap between research and practice due to a lack of details regarding implementation and post-implementation processes, which makes it difficult for both researchers and practitioners to utilize the findings of previous studies. The lack of a dynamic perspective on barriers and facilitators in extant literature makes it difficult not only to foresee obstacles and avoid failures, but also to plan successful telehealth projects. Our study addresses these gaps.
Method
Our investigation constitutes a qualitative, longitudinal case study. 34 The qualitative approach to data collection and analysis allows us to take advantage of several data collection methods and data sources in studying motivations, opinions, and actions 35 of both patients and healthcare professionals, which in turn provides for a comprehensive understanding of the complex phenomenon. 34 The study is longitudinal 34 in the sense that we investigate and account for factors that influenced telehealth adoption and use during the entire post-implementation period. This supports a holistic understanding of the project, experienced challenges, and the successful outcome. By drawing on empirical data collected as part of previous studies5,6 of the same technology and organizational setting, our investigation covers a 5-year period from 2014 to 2018. In the following, we present the case, including the “My Pathway” project and digital platform, followed by an account of our approaches to literature search, data collection and analysis.
Case description
Case site
Silkeborg Regional Hospital (SRH) is a mid-sized Danish hospital. In 2012, SRH was named the region’s most innovative hospital and established the “Center for Planned Surgery.” Today, the Center for Planned Surgery has 480 employees. 36 It is the first of its kind to organizationally merge orthopedic surgery and anesthesiology for the purpose of innovation across areas such as hip, knee, back, and shoulder surgeries. To foster such innovation, the hospital initiated a project in collaboration with the company Visikon to develop the online telehealth platform “My Pathway” to serve the information needs of patients undergoing THR.
“My Pathway”
The online telehealth platform grew out of a telehealth project running from 2008 to 2013.5,37 In 2014, THR-patients were granted access to “My Pathway,” which was available through both a web browser 38 and a mobile application. Using a personal code, patients access the platform and its detailed information about their entire course of treatment, symptoms, post-surgery exercises, and frequently asked questions. The platform does not support two-way communication but provides information through animated videos and illustrations. These make the information more accessible by avoiding technical terms and showing consideration for the anxieties that some patients experience when watching real images of, for example, operations and wounds. 5 Previously, such images were not only perceived as overwhelming by patients but also impeded their understanding of important information about the surgery.6,39
The overall goals of the telehealth project were to reduce LOS while increasing or at least maintaining the same level of patient satisfaction. By informing and educating patients about their treatment and post-operative behavior, previous research has shown that patients feel less anxious being discharged earlier. 40 Increasing patients’ information satisfaction was therefore essential to reducing LOS. 5 Today, LOS has overall been successfully reduced to such an extent that THR patients are able and expected to be discharged after only 24 h. Despite the positive results of the telehealth project (2008–2013), healthcare professionals report unanimously that the telehealth platform is barely being used today by both patients and healthcare professionals.5,6 Our study investigates the telehealth project and the role of adoption barriers and facilitators in accounting for its success despite the lack of technology use.
Literature search strategy
We subscribe to the approach by Fink, 41 who argues that a literature search should be based on a strategy that includes an approach to systematically and rigorously identifying and analyzing an existing body of knowledge. We base our search on the Scopus citation database. According to Mongeon and Paul-Hus, 42 most bibliometric analyses are based on Thomson Reuters’ Web of Science (WoS) and Elsevier’s Scopus. Furthermore, “WoS had been the sole tool for citations analysis until the creation of Scopus and Google Scholar in 2004. However, the low data quality found in Google Scholar raises questions about its suitability for research evaluation” (p. 1). 42 As our article is not a literature review but a case study drawing on extant literature, combined with the fact that Scopus has a much larger journal coverage compared to Web of Science,42,43 we limited our literature search to Scopus. Figure 1 illustrates the literature selection strategy.
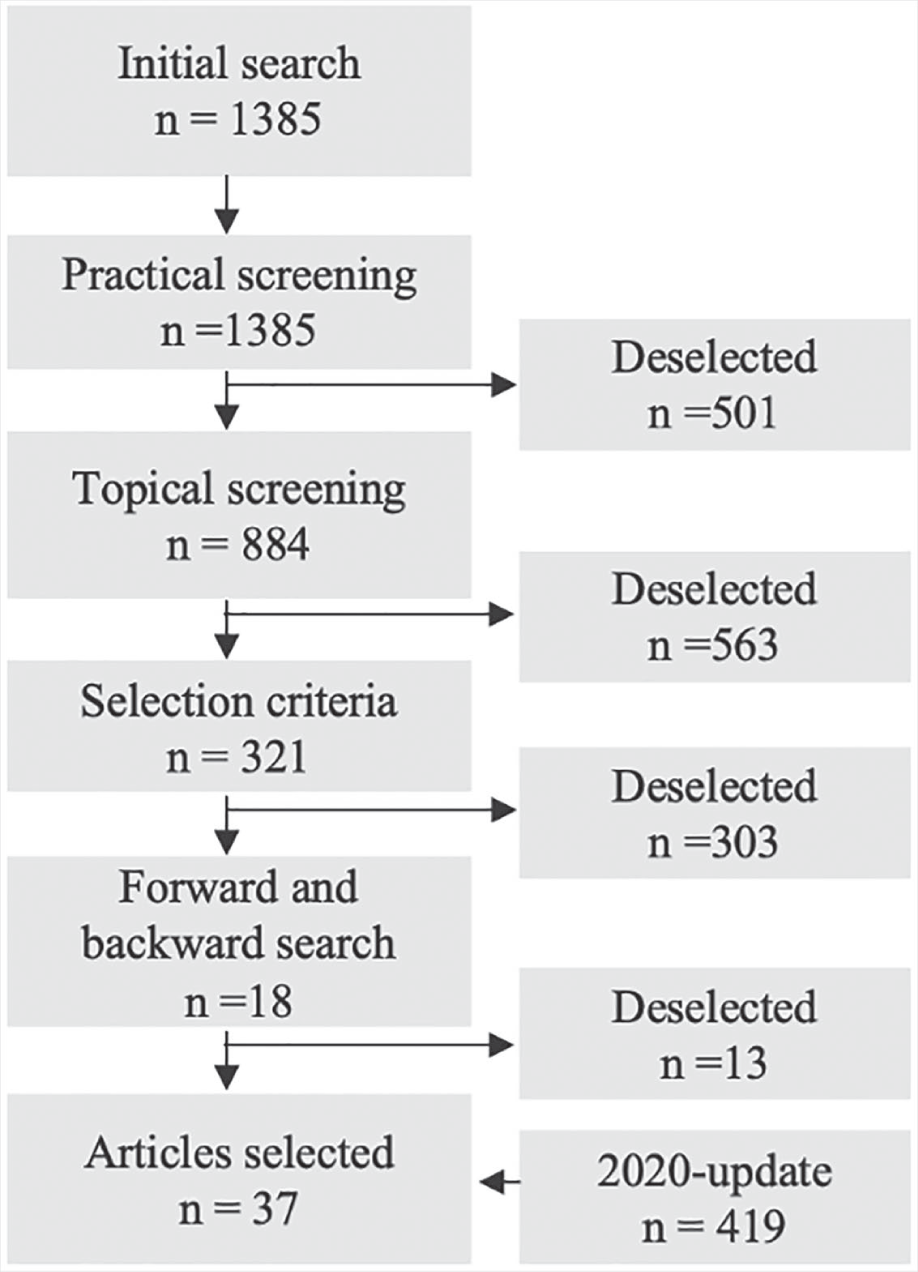
Literature selection strategy.
We used the following search terms: (telemedicine OR telehealth OR “digital health” OR mHealth OR m-Health OR “mobile health”) AND (barrier OR “success factor” OR “adoption factor” OR facilitator) AND (innovat* OR improv*). The initial search yielded 1385 articles. By applying practical screening criteria, 41 we limited results to journal articles and conference papers in English. As telehealth involves the use of mobile devices and in particular smartphones, only literature from 2007 (the year the first-generation iPhone was released, leading to the popularization of smartphone technology 44 ) and onward is included. Based on this practical screening, the number of articles was reduced to 884. Next, we applied topical screening criteria to exclude non-relevant topics, for example, diabetes and epilepsy. This reduced the number of articles to 321. Subsequently, we read titles and abstracts to distinguish relevant from non-relevant articles based on predefined selection criteria. These selection criteria helped us limit articles to those (1) about orthopedic surgery (relevant to the case and the “My Pathway” platform); (2) with an organizational perspective on telehealth (due to our focus on adoption and use vis-à-vis design and development of the platform); and (3) based on empirical studies from developed countries (due to differences in barriers and facilitators between developed and developing countries 45 ). Applying these criteria limited the number to 18 relevant articles, which are all comparable studies in terms of context (i.e. the same area within highly developed healthcare systems) and focus (i.e. organizational perspective on technology adoption and use). At this stage, we conducted a backward and forward search. 46 Finally, a 2020 search update was made in which we used the same keywords and selection criteria. Eventually, we identified a total of 31 articles as relevant to our study. The articles were coded in a concept-centric manner 46 and divided into barriers and facilitators of telehealth adoption.
Data collection
We followed Miles et al. 47 in our qualitative approach to data collection and analysis. Through abductive reasoning, our study balances an inductive and deductive approach to data collection and analysis. 35 While numerous scholars separate data collection and analysis, Miles et al. 47 recommend collecting and analyzing data concurrently, as it enables researchers to cycle back and forth between interpreting existing data and planning for additional data collection based on emergent needs. Following an iterative process enables us to investigate the actual problem space and ensured that we identify critical telehealth challenges.
A major strength of case studies is the opportunity to collect data from multiple sources of evidence. 34 Since our study investigates how different barriers and facilitators have influenced telehealth adoption and use during the post-implementation period, the use of several sources is necessary. 34 Primary data were to a large extent collected through interviews and observations in the clinical setting. We also rely on secondary data from previous studies5,6 in establishing an overview and understanding of barriers and facilitators in telehealth adoption and use over time. The secondary data derived from two separate studies of the “My Pathway” platform—the first from 2008 to 2013 and the second from 2017. These studies were accessed in the form of articles37,39 and reports.5,6 We collaborated with the authors of these previous studies to combine their findings and parts of the underlying data with the empirical data collected specifically for our investigative purposes. In addition, quantitative data on, for example, LOS and patient satisfaction from a nationwide survey of patient experiences 48 support our study.
Interviews
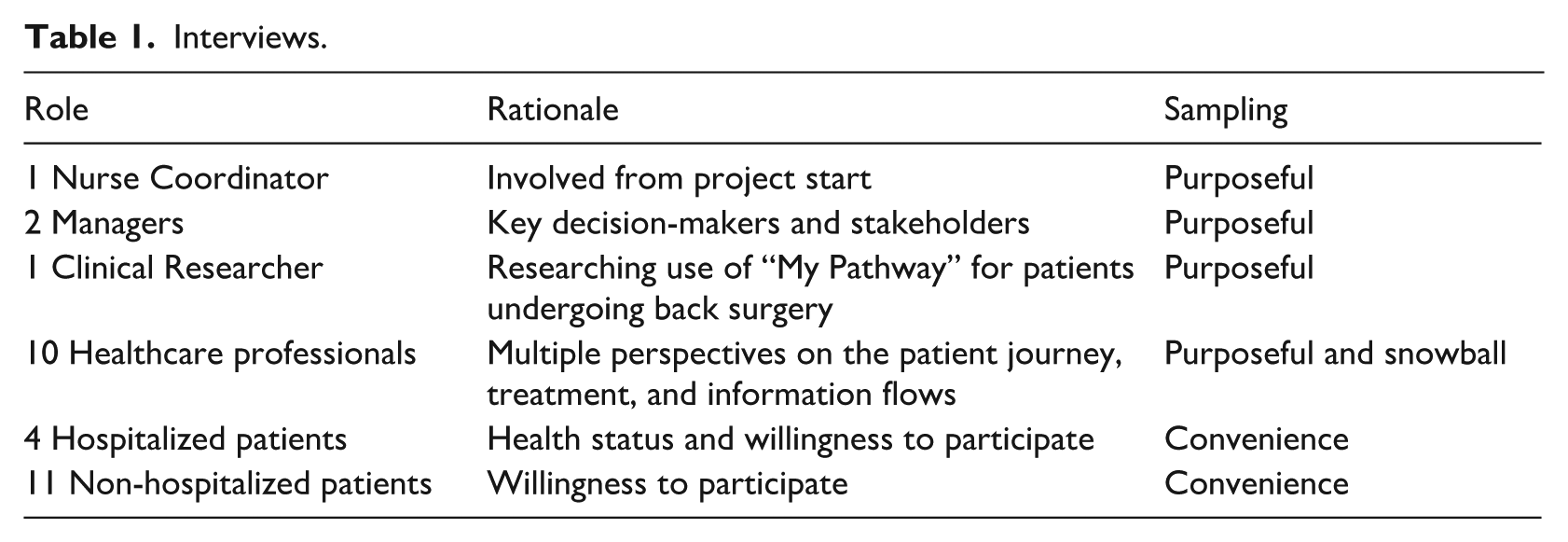
First, we conducted seven explorative interviews to understand the problem space. Five healthcare professionals were interviewed to understand their involvement and perception of the platform, and two patients were interviewed to assess the use and relevance of telehealth from a patient perspective. These healthcare professionals were carefully selected with regard to differences in roles, experiences, and backgrounds. We wanted to interview both novice and senior people, with varying experiences and roles with regard to both patient contact and platform usage working at the Center for Planned Surgery. The purpose was to ensure as broad a perspective on barriers and facilitators of the telehealth project as possible. These interviews provided us with a perception of the problem space (Rowley, 2012) 49 and enabled us to narrow down our research focus. The two explorative patient interviews were conducted as opportunities arose. We prepared interview guides based on acquired knowledge through the literature search, and questions were divided into three categories: (1) use of “My Pathway,” (2) experienced challenges, and (3) identified opportunities. We followed a semi-structured interview approach which allowed us to ask open questions about informants’ experiences with the platform and their perceptions of challenges and opportunities. In-situ adaptation of the interview guides ensured a fit between the questions and the context of the interviews (e.g. at or outside the outpatient clinic and before or during hospitalization). Healthcare professionals were selected through both purposeful and snowball sampling. 35 This sampling strategy allowed us to initially select some informants (purposeful sampling) who then guided us and facilitated contact to other informants (snowball sampling), which provided us with a rich sample of informants. 47 We based the selection of patients on convenience sampling 47 in the sense that we interviewed patients during hospitalization who were well enough and willing to participate.
Second, we conducted 22 semi-structured interviews with patients and healthcare professionals at different points along the patient journey (corresponding to the touchpoints illustrated in Figure 2). We selected informants based on both purposeful (following preselected healthcare professionals across patient journey touchpoints, cf. Figure 2) and convenience sampling (involving patients who were present and willing to participate across touchpoints). Consistent with our abductive approach, which entails collecting and analyzing data concurrently, we continued sampling until having achieved informational saturation.47,50 Again, we based the interviews on interview guides with questions about (1) patients’ satisfaction and experiences with the “My Pathway” platform; and (2) healthcare professionals’ knowledge and perception of the platform in terms of relevance and value creation. All interview guides were prepared collaboratively by the research team based on domain knowledge (two of the authors have been employed at SRH) and extant literature. All interviews were conducted by one of the authors with the support of another experienced, qualitative researcher. They were audio-recorded and transcribed. The interviews contribute to an understanding of technology use (or non-use), barriers and facilitators, as well as patients’ and healthcare professionals’ perceived value of the telehealth platform. An overview of interviews is provided in Table 1.
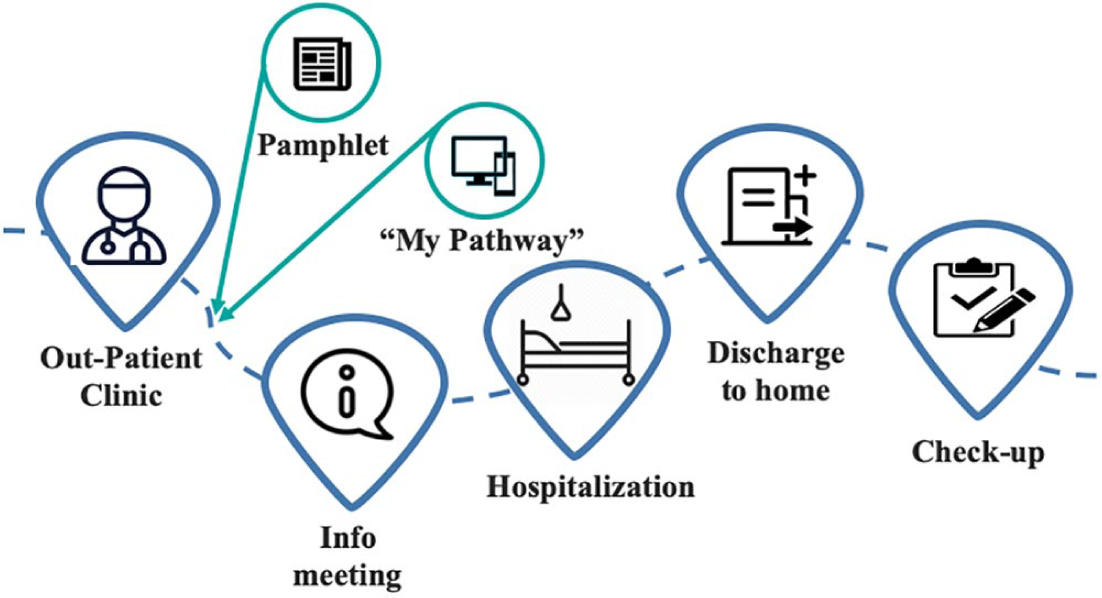
The journey for THR patients at SRH.
Interviews.
Observing the patient journey
Based on insights from the explorative interviews, we decided to observe the patient journey to better understand the use and value of technology (or lack thereof). It was an option to acquire first-hand experience of patient-healthcare professional interactions and communication that arose during data collection. Therefore, we examined patients’ experiences at different touchpoints, that is when they were in touch with the hospital. 51 Figure 2 illustrates the five identified touchpoints along the patient journey. The first touchpoint between patients and healthcare professionals is at the outpatient clinic where patients are informed about the patient journey and relevant sources of information, including the “My Pathway” platform. At the next touchpoint, groups of patients are invited to information meetings where healthcare professionals explain the course of treatment in detail. One to two months later the patient is hospitalized and receives surgery on the same day. Ideally, the patient is discharged within a day. Lastly, the patient is summoned for a checkup three weeks after surgery.
We observed each touchpoint, and subsequently interviewed 22 patients and healthcare professionals. The interviews focused on patients’ information needs and satisfaction along the patient journey as well as their attitudes toward and experiences with the telehealth platform. At each touchpoint, we observed and interviewed two different healthcare professionals. The healthcare professionals were asked about their use of telehealth and their perceptions of value creation through telehealth use at that particular touchpoint.
In addition to the observations and interviews, every patient attending the information meeting was asked to participate in a survey about their knowledge and use of the platform for the purpose of assessing its perceived relevance.
Data analysis
The analysis of the primary data followed Miles et al. 47 We analyzed transcripts and field notes through an abductive coding process. This allowed us to identify relevant data points that help explain barriers’ and facilitators’ varying influence at different points in time during the patient journey—seen from the perspective of both patients and healthcare professionals. Consistent with this abductive coding approach, the empirical data were coded and analyzed both deductively and inductively. Deductively, we interrogated and categorized the empirical data based on concepts and insights from the literature, including the identified adoption barriers and facilitators. Inductively, we performed a thematic analysis to identify themes and questions that were salient in the case but perhaps not described in extant literature.47,50 Miles et al. 47 suggest an iterative coding process divided into two main steps: first-cycle coding and second-cycle coding. Our abductive approach followed these steps.
Step 1: First-cycle coding
Codes are labels that assign symbolic meaning to data collected as part of the study. 47 Through first-cycle coding, we assigned codes to chunks of data that appeared relevant and noteworthy for understanding telehealth as an empirical phenomenon and addressing the research question of how barriers and facilitators influenced telehealth adoption and use during the post-implementation period. The coding process resulted in 34 codes, including ownership, individual initiative, spillover effect, information satisfaction, and ease of integration.
Step 2: Second-cycle coding
Second-cycle coding is an approach to aggregate and synthesize first-cycle codes into fewer, higher-level codes or categories. This was an iterative process of going back and forth between the literature and the empirical data. 47 We compared and related first-cycle codes to the categories derived from our concept-centric literature search (those related to “Barriers of adoption” and “Success factors” in Table 2) and we supplemented with additional codes that emerged in vivo. Many first-cycle codes did not fit the literature-based categories. Through second-cycle coding, six additional categories emerged: effects of telehealth, lack of purpose, lack of IT management skills, willingness to adapt, (intention to) use, and information satisfaction.
Coding scheme.
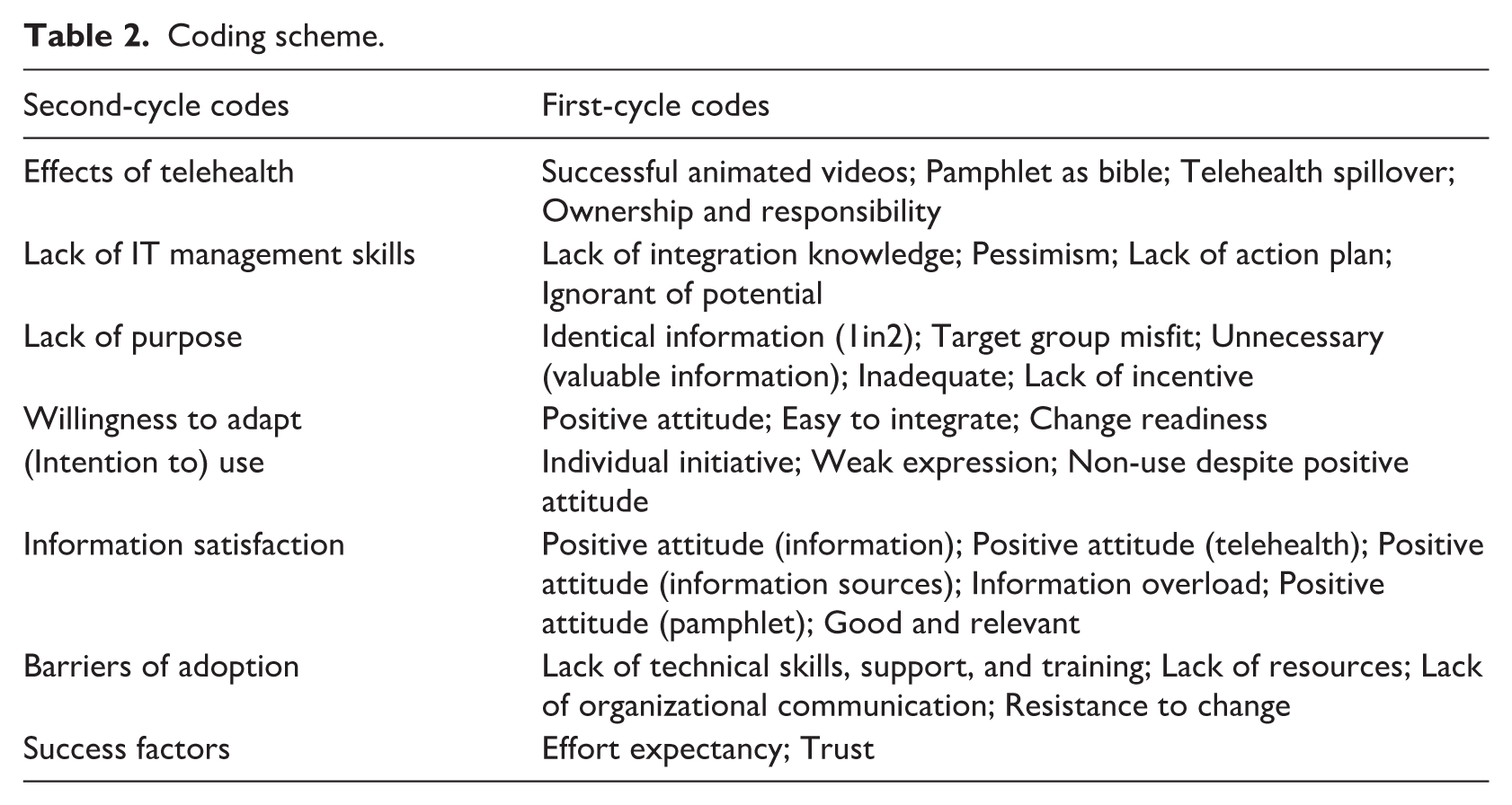
Table 2 shows the coding scheme that was, on the one hand, used during first- and second-cycle coding and, on the other hand, the result of these data analysis steps (cf., our abductive approach).
Step 3: Interpretation
We analyzed each of the three data sets (i.e. data from the current and the two previous studies) to identify the most frequently mentioned barriers, changes in their influence over time, and relationships between them. First, we identified statements pertaining to adoption and use of the “My Pathway” platform. We focused in particular on barriers of adoption within and across the three data sets. Second, we visualized relationships between the barriers and how they influence each other based on statements by the informants. This visualization helped us identify relationships that were not readily discernable due to differences in labeling and descriptions of barriers across the data sets. This visualization matured through consecutive draft versions (see Table 3).
Visualizations of barriers.
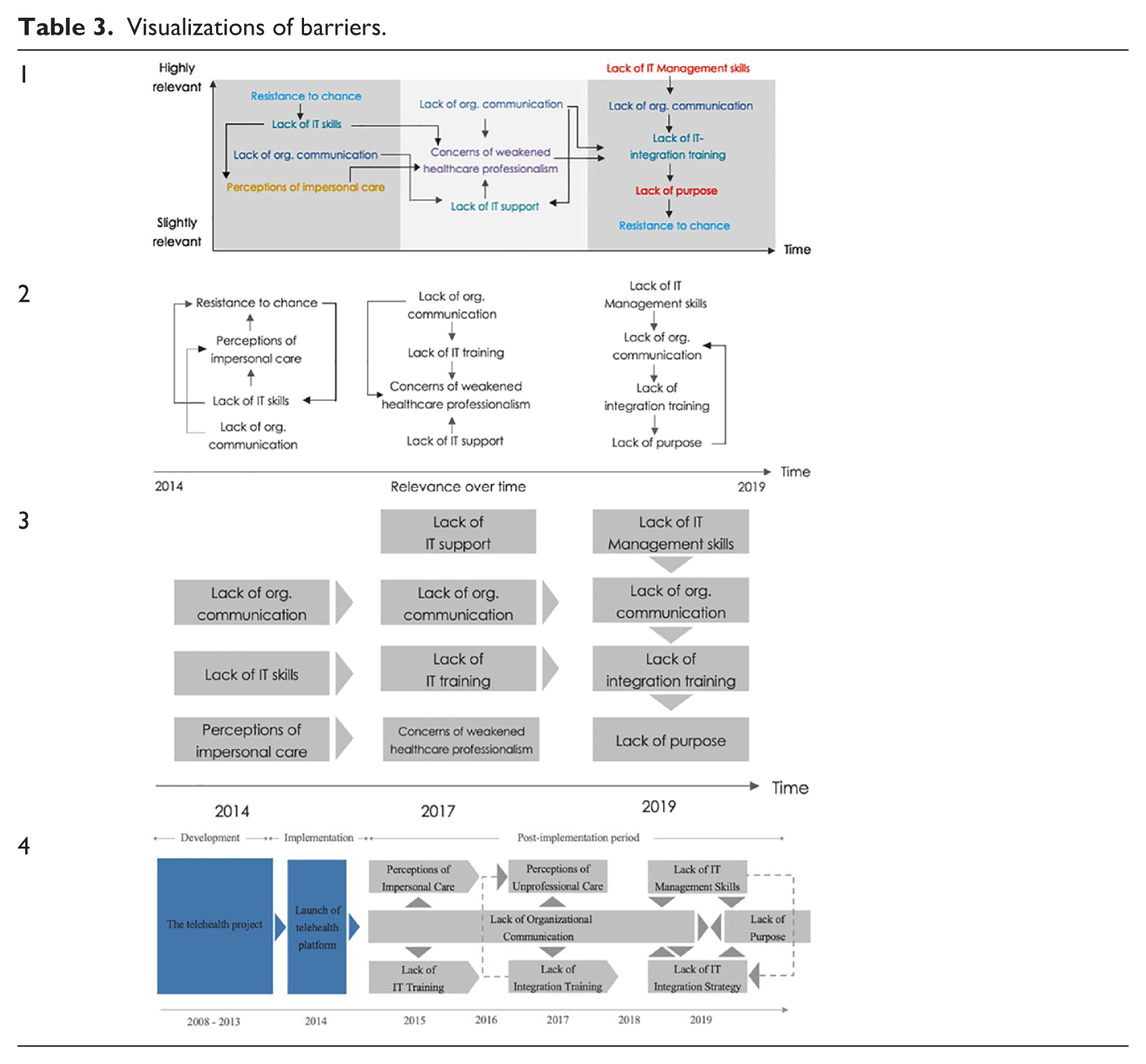
Third, this visualization allowed us to establish a simplified overview of barriers and their varying influence over time (Figure 4) by aggregating, abstracting, and synthesizing the data. The visual representation of barriers and their influence over time helped us identify relationships despite differences in naming across the three data sets.
Results
In this section, we present what appears to be an unsuccessful telehealth project in that the technology is not used. However, project goals were paradoxically achieved, although healthcare professionals and patients refrained from actively using the “My Pathway” platform. As described in the “Method” section, the results derived from analyses of data from our and previous studies.5,6 References to these project sources are included for documentation purposes. The project succeeded in improving patient care by providing enriched and timely information to the patients while reducing LOS and increasing patient satisfaction. 5 The results of our investigation show how barriers and facilitators influenced telehealth adoption and use during the post-implementation period, which in turn explains the success of the telehealth project despite lack of technology use.
The puzzle of the paradoxical success
Five years after the introduction of the “My Pathway” platform, the telehealth project achieved its goals of reducing LOS without compromising patient satisfaction. 5 In fact, patient satisfaction has been increasing over the past 5 years. By defining success in terms of reaching project goals, the telehealth project has been successful. Figure 3 illustrates both the positive trend of the measurements and influence on the patient journey since the introduction of the telehealth platform in 2014. Over the five-year period, average LOS fell from two to one and a half days while patient satisfaction increased almost a quarter of a point on a five-point Likert scale.
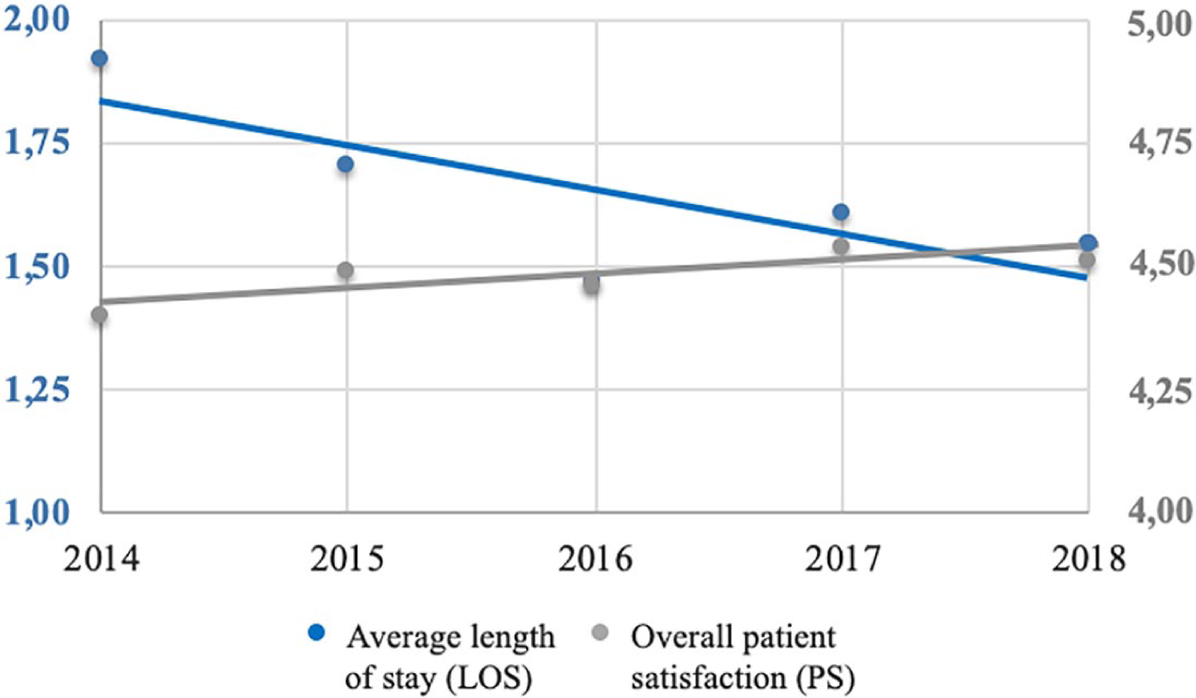
LOS and patient satisfaction 2014–2018.
The positive LOS trend is, however, not the result of telehealth use. Rather, “My Pathway” serves as a means to increase and enrich information flows, which have a positive effect on the level of patient satisfaction. Since the measurement of patient satisfaction in Figure 3 is an overall score based on 38 questions (part of standard hospital quality measurements), it is relevant to determine whether the increase in patient satisfaction is caused by greater information satisfaction over time. This is a reasonable assumption given that all sources of information were influenced by the telehealth project. When looking closer at scores related to information satisfaction (Table 4), it is evident that information satisfaction both “before and during” hospitalization and “upon discharge” display a positive trend from 2014 to 2017. We can only assume that there is a correlation between information satisfaction and patient satisfaction. Manager #14 explains how the enriched information flow has increased information satisfaction among more vulnerable patients: “Some patients are very satisfied. They are no longer sickened by the information they are getting as it is animated and therefore harmless to watch.” Comparing Figure 3 and Table 4, there is on the one hand an increase in overall patient satisfaction across the time period and, on the other hand, an increase in patient satisfaction with the information before and during hospitalization as well as upon discharge from the hospital.
Patient satisfaction with the information provided, measured on a scale from 1 to 5.
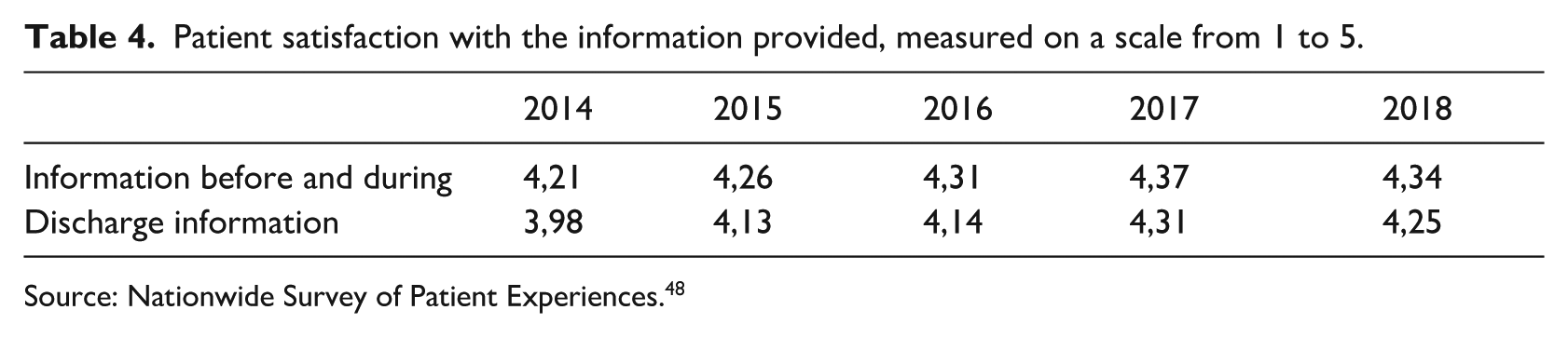
Source: Nationwide Survey of Patient Experiences. 48
Our analysis of the qualitative data shows, however, that the telehealth project contributed to an increase in information and change in means of information dissemination through the introduction of the telehealth platform “My Pathway.” Patient #14 states: “I have been very well informed. It is so detailed. It is an incredible information that you are getting [as patient]!” Therefore, it is paradoxical that healthcare professionals claim that both patients and healthcare professionals barely use the telehealth platform.5,6 The use of telehealth is not the primary reason for the high level of patient satisfaction. In 2017, two thirds of interviewed healthcare professionals reported that they had not accessed the platform since its introduction in 2014 6 and had consequently never used or suggested the platform as a means of communication with patients.
Today, “My Pathway” is officially integrated into the two first touchpoints along the patient journey. Yet one third of patients attending the information meeting (touchpoint #2) claim not to have heard about the platform, even though all patients are given an information flyer about “My Pathway” at the outpatient clinic (touchpoint #1). Thus, the study provides a paradoxical example of a successful telehealth project despite lack of technology use. To explain this puzzle, in the next section we look closely at the barriers and facilitators influencing telehealth adoption and use.
Barriers’ influence on telehealth adoption
By carefully examining the role of telehealth at SRH by interviewing and observing patients and healthcare professionals, we were able to show how different barriers have influenced technology use. As illustrated in Figure 4, barriers have exerted varying influence at different points in time during the post-implementation period, and the barriers were interrelated in the sense of influencing each other. In addition, Figure 4 provides a simplified overview of the process of telehealth adoption and use—from introduction of the “My Pathway” platform until today. The gray rectangles represent the most significant barriers during the post-implementation period, and the pentagons are used to highlight barriers that have changed meaning during the post-implementation period. For example, healthcare professionals’ concerns related to patient care have changed from being about impersonal care (perceptions of impersonal care) to fear of providing unprofessional care (perceptions of unprofessional care). The arrows indicate that one barrier has influenced or given rise to the other.
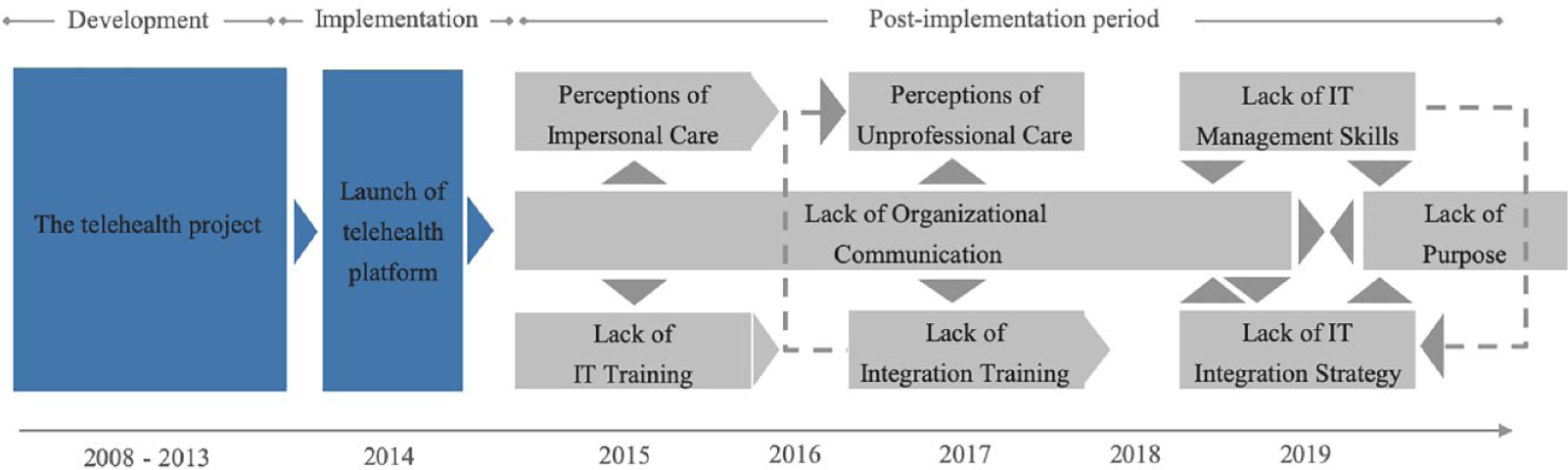
Influence of dynamic barriers over time.
As Figure 4 illustrates, lack of organizational communication is a critical barrier to telehealth adoption and use. Since its introduction in 2014, there has been next to no organizational communication about the use or integration of the telehealth platform. Healthcare professional #1 states: “As far as I know, nobody ever told us how to use it. I do not recall there has ever been an attempt to integrate it.” In 2017, healthcare professionals reported that the continued lack of communication had resulted in their lacking an understanding of why the platform had been introduced. Healthcare professional #14 states: “When we haven’t really seen it, we can’t know what it is or why we should use it.” Toward the end of 2017, healthcare professionals were granted employee access to the platform, which had previously been accessible to patients only. According to healthcare professional #1: “The employee-access helped a bit [in terms of healthcare professionals’ use of telehealth], but not many knew about it.” Therefore, the lack of communication is still a barrier of adoption and use despite efforts to promote the platform.
The barriers perceptions of impersonal care and perceptions of unprofessional care had previously impeded the adoption and use of “My Pathway,” but their influence has gradually diminished during the post-implementation period, concurrently with healthcare practitioners growing accustomed to the platform. While both patients and healthcare professionals previously expressed concerns regarding the impact on the patient-healthcare professional relationship, it does not seem to influence the use of telehealth today. On the contrary, the focus on information management resulting in an increase in patient-relevant information has led to patients desiring an easy way of procuring information through, for example, technology over a strong patient-healthcare professional relationship. This is reflected in the following statement by patient #4: “I would rather get answers in the app than by calling a nurse.”
Another barrier that was previously an obstacle to healthcare professionals’ use of telehealth is the lack of IT skills that made the lack of IT training and lack of integration training key barriers to telehealth adoption. Concurrently with healthcare professionals acquiring technical skills in their private lives 6 through increased technology use (e.g. through diffusion of smartphones and apps), they perceived their level of competence as satisfactory in 2017. The lack of integration training and the consequent lack of knowledge of how to integrate the technology into everyday work practices impeded the healthcare professionals in adopting and using “My Pathway.” Later, perceptions of unprofessional care were a major obstacle to healthcare professionals using the platform. Of all healthcare professionals, 73% did not feel comfortable using the platform in communication with patients. 6 They feared that patients would question their authority and professionalism if their technical skills were inadequate or if the technology was faulty. 6 In 2019, their attitude had changed and healthcare professionals were positive toward adopting and using telehealth. They showed no concern for lack of integration training. However, healthcare professionals hesitated to integrate telehealth into their daily work practices due to the lack of IT integration strategy. They lacked an incentive or a reason for using it. This is elaborated by healthcare professional #5, who states: “I don’t use it. But if we were told [by management] to use the platform, then I think it would be a good idea.” The lack of IT integration strategy, which is closely linked to lack of organizational communication, further fueled the perceived lack of purpose of using the platform.
Our analysis reveals that the lack of organizational communication was rooted in managers’ lack of IT management skills. This was articulated by manager #4: “We were just left behind with the technology, and the question ‘can we bring it to life?’ We cannot just go out and tell our employees ‘how to do’ in the middle of the ward, so then what do we do?” Manager #14 elaborated: “The reason, why we haven’t integrated it, is because we do not know how to.” The lack of IT management skills is also related to the perceived lack of purpose. Manager #4 clarifies: “Fundamentally, it is because we have little knowledge of what we actually should use it for.” The lack of purpose and lack of organizational communication are thus interrelated barriers in the sense that they fuel one another.
Despite the lack of technology use on account of the barriers to telehealth adoption and use, patients were satisfied with the information level. Healthcare professional #8 states: “Patients explain that they are extremely well informed and that it has never been necessary to access the platform.” Healthcare professional #5 agrees: “I have not quite felt the incentive to use it, because I feel that I am giving sufficient information already.” The high degree of patient satisfaction is attributable to healthcare professionals’ focus on information dissemination and management. In the following we describe information management as a critical facilitator that helps explain the telehealth project’s success despite the barriers of adoption and lack of technology use.
The crucial role of information management
In 2019, patients expressed satisfaction with the information that they received. Patient #6 states: “The information level is just fantastic. We were taken by the hand through the entire course of treatment.” Patient #14 adds: “I think it has been really good. They have treated me exceptionally well!” Despite these positive comments, none of the patients mentioned the platform as their preferred source of information. Instead, patient #10 explains: “It works fine as a supplement to the pamphlet, but well. . . it is basically the same information. And I prefer the pamphlet.” In fact, patients generally referred to the physical pamphlet as the primary source of information. This was, for example, expressed by patient #14: “I have been so well informed because of the pamphlet. It is so detailed.” Patient #1 supplemented: “I used the pamphlet, where all information is provided, so it has not really been relevant to seek other sources of information.” Meanwhile, our investigation shows that the physical pamphlet was changed in light of the telehealth project. In 2019, the written information built upon the animated videos developed for the telehealth platform. Healthcare professional #3 explains: “The part about using animated illustrations works really well—that is also why our pamphlet is built around them.” For example, screenshots from the animated videos replaced photos of real scars. Both the pamphlet and the platform tell the same story, but with the latter containing additional and interactive information.
Due to lack of organizational communication, healthcare professionals were introduced to the telehealth platform but had no guidelines on how to integrate it into their daily work practices. According to manager #4: “It was never really implemented. What are my digital communication competences, and how can we include it in our procedures? Seriously, I do not know anything about it.” Therefore, healthcare professionals have individually taken initiatives to integrate and utilize parts of the technology. This was illustrated by manager #4: “When we launched the platform, it was the coordinator responsible for the overall patient pathway who took the lead and decided how she wanted to use it.” The coordinator suggested that the animated video be shown at the information meeting. As a consequence, the information meeting was built around the platform in 2019—either by using photos from the animations or by showing the video of the patient journey and each step of the treatment. The telehealth animations had thus become a way of informing and displaying the patient journey to new patients. Another example of how information was managed and spilled over was healthcare professionals using telehealth to strengthen their communication with patients. Healthcare professional #8 states: “When you say ‘My Pathway,’ I think of the fact that everything has been animated. I am a huge fan of the animations and that you can illustrate and ‘add layers’ on, for example, muscles, when I speak with the patient.” The lack of organizational communication necessitated that healthcare professionals manage patient-relevant information (i.e. information management), which in turn had noticeable spillover effects on the information meeting, the pamphlet, and the way healthcare professionals communicated with patients. Therefore, our analysis shows that their focus on information management—in the sense of disseminating and managing patient-relevant information—has enriched information across all sources. This helps explain why telehealth played an important role in increasing the level of information satisfaction among patients despite lack of technology use.
This study is the first of its kind to provide an example of a telehealth project that paradoxically succeeded in reaching its goals despite lack of technology use. Although the platform did not play as prominent a role as it was intended in the telehealth project, our analysis reveals that it nevertheless influenced its success. Due to barriers to healthcare adoption and use, healthcare professionals had no incentives to use the telehealth platform, which led to improvisation and novel use of the technology-embedded information. The lack of organizational communication led to a perceived lack of purpose, which in turn resulted in lack of technology use and created a need for information management. In the absence of healthcare platform usage, which was intended an important information dissemination role, healthcare professionals engaged in information management by integrating the information available on the platform in processes and artefacts used at different touchpoints along the patient journey. Thus, “My Pathway” became a catalyst for new processes despite lack of platform usage due, for example, to spillover effects from animated videos to illustrations in the pamphlet.
Discussion
Principal findings
This study responds to the knowledge gaps identified by Faber et al. 7 and Ross et al. 8 by demonstrating how telehealth barriers and facilitators influenced adoption and use of the “My Pathway” platform during the post-implementation period. We extend extant literature through two main contributions. First, in contrast to extant literature that depicts barriers of adoption as static,11,26 our study suggests that barriers are dynamic and interrelated with varying influence at different points in time during the post-implementation period. Currently, extant telehealth literature has examined barriers as static entities that do not change nor influence each other over time.10,13,15,16 Hence, extant literature fails to account for the fact that barriers have varying influence over time depending on context and circumstances. Similar to other telehealth studies, Kruse et al. 10 evaluate barriers’ influence based on the frequency with which they are mentioned in extant literature. Our study questions the premise of such an evaluation and suggests that barriers’ influence is context dependent and may vary over time with the phase of implementation, for example, technology introduction and post-implementation. We demonstrate this in the context of telehealth adoption and use at SRH and thereby respond to Ross et al.’s 8 call for more research in light of existing knowledge gaps with regard to the context and process of telehealth adoption and use. Based on an investigation of an implementation process, Faber et al. 7 posit that telehealth is not a linear process due to changes in management commitment. By demonstrating that barriers are interrelated and vary in importance during the post-implementation period, our study confirms that telehealth adoption and use is a non-linear process. Thereby, we contribute to state-of-art knowledge by suggesting a new and dynamic perspective on barriers of adoption and use.
Second, this study contributes to extant research by revealing the crucial role of information management, which is shown to be a critical facilitator in achieving the goals of the telehealth project despite lack of technology use. While extant literature describes information management as one among several factors that influence technology use, for example low effort expectancy and high system performance quality,26,28 our study identifies information management as the most critical facilitator of the telehealth project’s success. Extant literature lists multiple factors that influence the success of telehealth adoption and use.2,9,18,25,26,27 While these facilitators contribute to successful outcomes,9,26,28 also in the case of “My Pathway” (specifically, effort expectancy and trust), our study does not investigate what could have facilitated greater telehealth adoption and use. Rather, we investigate the barriers and facilitators that influenced the witnessed adoption and use. Our study identifies information management as a critical facilitator that counteracted the adoption barriers and promoted telehealth success despite lack of technology use.
Implications for research
Having documented that barriers are dynamic in nature, we encourage future research investigating patterns of change. To what extent is it possible to predict how barriers change and influence each other over time? Furthermore, what are appropriate response strategies in coping with obstacles to telehealth adoption and use? In addressing such questions, it might be possible to develop a contingency theory articulating when to do what in response to particular obstacles, that is barriers to telehealth adoption and use. By providing such knowledge, it becomes possible to better cope with barriers in an appropriate and timely manner. Moreover, as our study identifies information management as a critical facilitator counteracting barriers to adoption and use of the “My Pathway” platform, more research is needed with a focus on the interplay between critical facilitators and barriers. One important question to explore is how and under which conditions critical facilitators mitigate or nullify telehealth adoption barriers.
In summary, we recommend that researchers:
investigate and theorize how adoption barriers influence each other over time,
study managerial action in the face of challenges to telehealth adoption and use with the aim of inferring and theorizing response patterns,
explore how various factors facilitate telehealth adoption and use despite barriers.
Managerial implications
By providing a new perspective on telehealth adoption and use, our study provides practitioners with suggestions in terms of how to cope with barriers. First, practitioners are cautioned against addressing any one barrier in isolation as they are interrelated with varying influence over time. A barrier may be influenced by other barriers and consequently grow or diminish in importance over time. Therefore, practitioners are encouraged to follow up on obstacles continuously and respond to the barriers as they arise during a project. As our case study illustrates, barriers can be overcome. Applying a risk management and mitigation perspective and identifying, monitoring, and mitigating barriers like project risks may be an appropriate management approach.
Second, our findings inform managerial decision-making more broadly in three ways: (a) as management of ICT is important to the future of healthcare, our findings underscore the need for IT management skills as a perquisite for coping with telehealth adoption and use; (b) organizational communication about the purpose and goals of telehealth as well as information about planned projects and technologies help prevent perceptions of lack of purpose among healthcare professionals and patients, which is closely linked to other barriers; and (c) the findings show that information management is key to ensuring patient satisfaction, which suggests that healthcare professionals should actively manage information across technologies (low and high tech) and media (analog versus digital) to increase the likelihood of telehealth success. Thus, information management is crucial whether designing telehealth platforms or drafting written and verbal communication.
In summary, we recommend that practitioners:
procure IT management skills as a perquisite for telehealth adoption and use,
manage information across technologies and media in support of communication about purpose and goals,
map how different barriers (may) influence telehealth adoption to varying degrees over time,
monitor identified adoption barriers from a risk management perspective.
Limitations
Since our study is based on a single case study, the possibilities of empirical generalization are limited, 34 which lowers the transferability of results. Moreover, “My Pathway” is an information dissemination platform that does not support two-way communication. This has implications for the construct validity since the platform characteristics may differ across telehealth projects and technologies. However, it has no adverse effect on the external validity of the study since the perspective on barriers as being dynamic is still valid irrespective of the specific barriers identified. In other words, despite limited generalizability, we are still able to conclude that barriers are dynamic entities that change over time. Meanwhile, future research into integrative, multi-sided platforms is warranted in light of the limitations of the case study.
Conclusion
This study explains the paradoxical success of a Danish telehealth project by showing how barriers and facilitators influenced adoption and use of the “My Pathway” platform, which led to project goals being achieved despite the lack of platform usage. Although “My Pathway” was central to the telehealth project, the findings show that actual platform usage had little impact on the project’s success due to barriers’ varying influence during the post-implementation period from 2014 to 2018. The barriers resulted in an increased attention to information management, which was the critical facilitator that helps explain the paradox of project success. The study makes two main contributions to extant literature. First, it recognizes barriers as dynamic, interrelated entities that have varying influence over time. Telehealth adoption is shown to be a non-linear process. Second, the study reveals information management as a critical facilitator. An increase in attention to information management may help healthcare professionals respond to barriers and ensure success of telehealth adoption and use.
Footnotes
Acknowledgements
We would like to thank all patients and healthcare professionals participating in the study.
Author contributions
S.D.M. (lead author); D.L.W. (main author); H.K. (author); M.V. (project sponsor); M.T.H. (author).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval/Patient consent
The study complies with ethical standards in health information systems research and applicable data protection laws. Informed consent was obtained from all participants.