
Abstract
Women with diabetes are at increased risk of adverse maternal and foetal outcomes. Preconception care can minimise risk of complications and improve outcomes, but current provision is inadequate. Electronic health technology, particularly apps, could improve preconception care provision but research is lacking in this area. The aim of this article is to explore the views and experiences of clinicians and women with diabetes regarding the use of a mobile app for preconception care. An exploratory study was conducted. Data were collected using focus group and interviews with 19 participants, comprising 10 clinicians and 9 women with type 1 or 2 diabetes. Data were analysed thematically. Women with diabetes and clinicians highlighted the inadequacy and challenges of current preconception care service provision and expressed a high level of enthusiasm and interest, towards a preconception care app that could support preconception care delivery for women with diabetes and overcome barriers to preconception care service provision and uptake. The acceptability of mobile health technology to both women and clinicians creates an important opportunity to overcome existing barriers to service provision, delivery and uptake, and improve both maternal and foetal outcomes for women with diabetes.
Introduction
There are global concerns about the increase in diabetes mellitus (DM) across the world, and in particular the dramatic rise in prevalence in women, 1 where recent reports indicate a rise of 4.5 million between 2015 to 2017. 1 DM is currently the most common pre-existing medical condition which complicates pregnancy, with both type 1 and type 2 DM creating considerable risks to both mother and child.2–4 DM complicates 1–3 per cent of all pregnancies and the increasing prevalence is due to an increase in the incidence of type 2 DM.5,6 For example, in the United Kingdom, the prevalence of type 1 DM in pregnancy increased from 1.56 to 4.09 per 1000 pregnancies between 1995 and 2012, a 162 per cent increase while the prevalence of type 2 DM in pregnancy increased from 2.34 to 10.62 per 1000 pregnancies between 1995 and 2012, a 354 per cent increase over 17 years. 7 Women with DM are, for example, more likely to experience adverse pregnancy outcomes such as miscarriage, preterm labour and maternal death, with babies at increased risk of birth defects, birth injury and/ or perinatal death.2–4 It is recognised that preconception care (PCC), special care and advice before pregnancy, is an effective way to reduce maternal and foetal risks. Hyperglycaemia at conception is of particular concern and guidelines recommend that all women with DM engage with preconception care to optimise their blood glucose level and health before pregnancy.8–10 Women with type 1 and 2 DM are equally at risk and receive similar preconception care, 8 although a tailored approach is recommended. 5 However, despite evidence on the effectiveness of preconception care in safeguarding maternal and child health,11–13 several research studies, including two systematic reviews synthesising data from various countries, show that current preconception care service provision is inadequate and available to less than 50 per cent of women.10,14,15 Consequently, women with DM have poor understanding of the risks, and/or benefits of preconception care or the consequences of having unplanned pregnancy.15–18
The need to improve preconception care for women with DM has led to a growing interest in the use of eHealth: the cost-effective and secure use of information and communication technologies (ICT) in support of health and health-related fields.19–23 eHealth technologies, particularly smartphones, multimedia and the Internet, are increasingly being used around the world to provide healthcare information and support.24,25 For example, an eHealth preconception counselling programme using CD-ROMs, DVDs and website format to educate women with DM regarding the need to plan for pregnancy and reduce risks, led to significant improvements in perceived benefits of seeking preconception care, knowledge of risks, confidence to plan a pregnancy and improved pregnancy outcomes.13,20–23 Moreover, apps (programmes designed to enhance smartphone functionality) have become extremely popular, and are being used to provide health education, decision support, monitoring and behaviour change interventions.26,27 Evidence shows that women of reproductive age are increasingly turning to websites and mobile health apps to receive health information rather than relying on face-to-face and paper-based delivery methods. 28 eHealth, via the smartphone app, provides an opportunity for women to have easily accessible, comprehensive preconception health information that is evidence-based and available 24 h a day, and which could help optimise women’s health before and during pregnancy. 28
However, the use of eHealth for preconception care of women with DM is still in its infancy. So far, very few studies13,20–23 have used eHealth to provide preconception care to women with DM and none have examined the use of a smartphone app. In a recent systematic review 15 and meta-synthesis, 29 women with DM identified lack of information as a barrier to seeking preconception care and suggested the development of a preconception care app to help improve preconception care knowledge and uptake. 16 Between 2013 and 2017, 3.7 billion health apps were downloaded; 30 hence, given their reach, convenience and accessibility, smartphone apps appear to be well suited to help address the limitations of both in-person and other technology-assisted methods.27,28,31 Despite the proliferation of apps and their suitability for disseminating information and promoting preconception care uptake, 14 there is a lack of knowledge regarding the extent to which an app is a feasible and/or effective platform for providing preconception care to women with DM. Working with women with diabetes and clinicians, a 2-phase study was undertaken to co-create a preconception care app for women with diabetes. 32 This article presents the first phase of the study which aimed to examine clinician and women’s views and experiences regarding preconception care and the use of an app for preconception care of women with DM; the intention was to use this to inform the development of the app in phase 2.
Statement of significance
Preconception care (PCC) reduces risk of adverse outcomes; however, uptake is low and less than 50% of women with diabetes receive PCC.
Electronic health (eHealth) technology, particularly smartphone apps, has the potential to improve PCC provision but research is lacking in this area.
Women with diabetes and clinicians highlighted the inadequacy and challenges of current PCC service provision. Both groups expressed a high level of enthusiasm and interest towards an app that could support PCC delivery for women with diabetes mellitus and overcome barriers to provision and uptake.
Methods
A co-design approach, based on the collaborative activity between researchers and study participants whereby participants take on the role of experts in forming ideas and concepts based on their personal and professional experiences, was adopted. 33 Co-design with service users and clinicians ensures that expectations are closely matched to the intervention and promotes the likelihood of success.33–35 In line with the Medical Research Council (MRC) framework for complex interventions and mobile app development frameworks,34,36,37 focus group and interviews were used to explore the views and experiences of the target population regarding preconception care and the proposed app intervention. Favourable ethical opinion was obtained from United Kingdom National Research Ethics Service Committee East Midlands-Derby. REC reference: 15/EM/0358; IRAS project ID: 178530.
Sampling, recruitment, and consent
A purposive sampling strategy, informed by previous studies using a co-design approach to develop mHealth apps,38,39 was used to ensure a range of views from clinicians and women with DM. 40 All participants who provided informed consent took part in the focus group and interviews. A total of 19 participants, comprising clinicians (n = 9) and women with DM (n = 10), were recruited. A minimum of 12 interviews with clinicians and women with DM was specified at the outset. 41 We continued to recruit participants until data saturation was reached, after 15 interviews, as previously reported by Francis et al. 41 Four successive interviews (already scheduled) were then conducted with no new themes identified. 41 Clinicians were recruited from two NHS district general hospitals and a GP practice in the South of England by a lead research nurse and the study researchers (CHN, JS). Women with DM aged 18–45 years with type 1 or 2 DM were recruited via Social Media (i.e. twitter) due to difficulty with recruiting women with DM who were planning a pregnancy from healthcare settings. Written consent was taken prior to data collection.
Data collection
Participants all received study information sheets which explained why the research was being undertaken and the researcher (CHN) also contacted participants to introduce herself, clarify the reasons for the study and answer questions, prior to data collection. Topic guides informed by the literature,23,42 and piloted with a woman with DM, a clinician and four researchers, were used flexibly between interviews and focus group (Supplemental Appendix 1). Participants were asked about their views of preconception care and previous experience of using an app. Their views, expectations and attitudes towards the development of a preconception care app, as well as their willingness to use or recommend the app, when developed, were also explored. The average time for interviews (n = 16) and the focus group (n = 1) was 30 min, with a range between 20 and 50 min. Data collection was face to face (with eight clinicians at their workplace and one woman with DM at a University in the South of England) or via telephone (with one clinician and nine women with DM); one study researcher (CHN) conducted and digitally recorded all interviews and focus group. Data collection took place between March and October 2016.
Data analysis
Data were transcribed verbatim, with each participant assigned a unique ID code for anonymity. Thematic analysis as described by Braun and Clarke 43 was conducted by (CHN) aided by Nvivo software. Analysis took place while data collection was ongoing; hence, initial findings were explored in more detail in subsequent interviews. Although a mixed inductive and deductive approach was used to elicit themes, the approach was largely inductive. Transcripts were read, and recordings were listened to several times to become familiar with the data, thereafter initial codes were generated and collated into meaningful groups and patterns. Themes were then identified and refined. Portions of the data were independently coded by two other researchers, thereafter the themes were discussed and agreed with the co-authors (NC and JS).
Findings
Demographics
Demographic characteristics of the 19 participants (clinicians, n = 9 and women with DM, n = 10) are shown in Table 1.
Demographic detail of study participants.
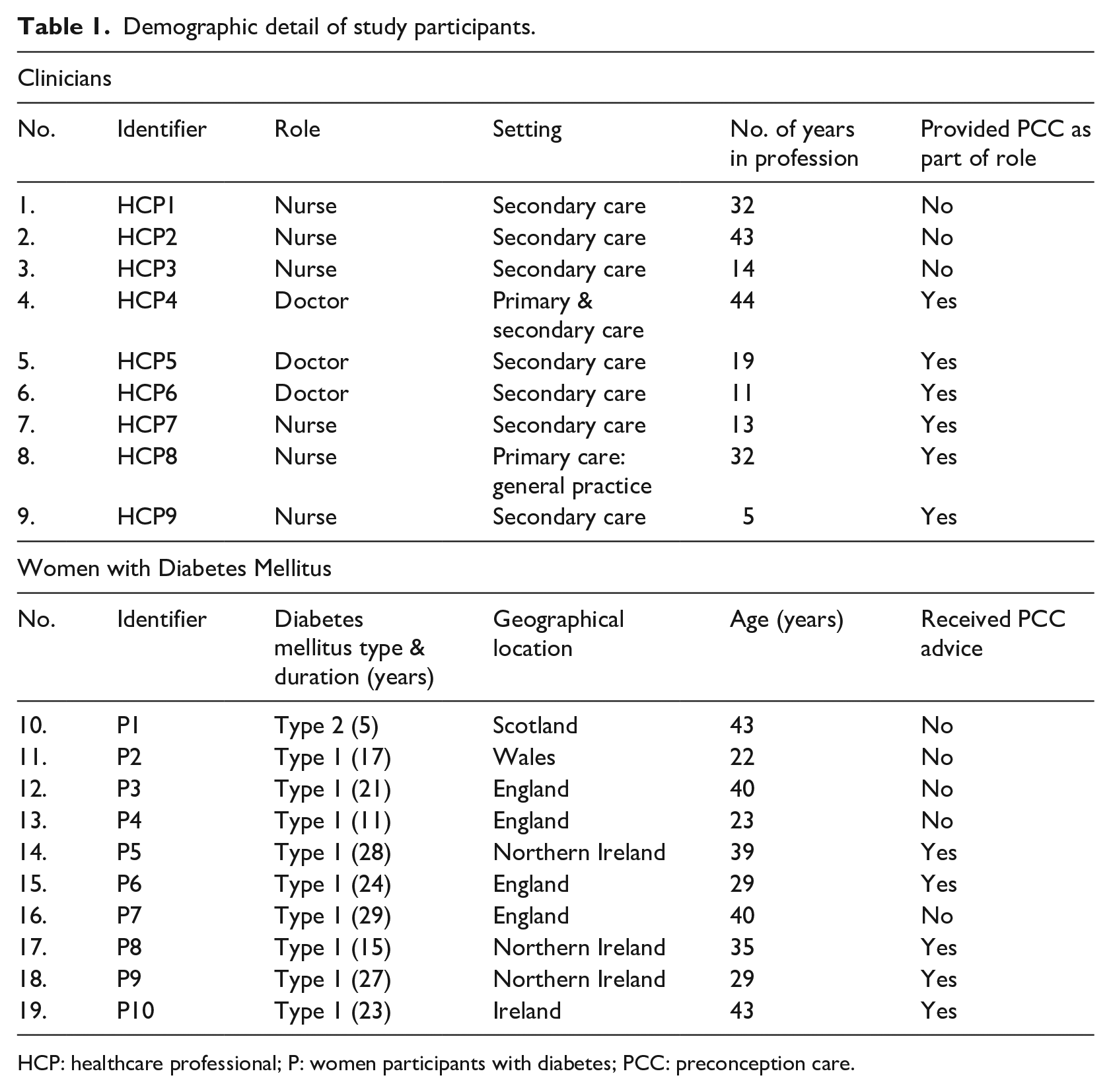
HCP: healthcare professional; P: women participants with diabetes; PCC: preconception care.
Clinicians
Clinicians included nurses (n = 6, diabetes specialist and research nurses) and doctors (n = 3, general practitioner, obstetrician and endocrinologist). Participants had extensive experience in the care of patients with DM with an average of 24 years. Most (n = 7) worked in a hospital which provided specialist diabetes services while (n = 2) worked in general practice. Six clinicians reported that they provided preconception care.
Women with DM
Women with DM were geographically dispersed and resided across the United Kingdom (UK) and Republic of Ireland. The average age of women was 34 years and majority (n = 9) had T1DM with an average diabetes duration of 22 years. Only half (n = 5) had received preconception care from clinicians. Of the remaining five who had not received preconception care, three reported unplanned pregnancy and one reported two miscarriages.
Themes
Two major themes and a number of sub-themes were generated from the data (Table 2). The current state of preconception care is presented first, with a focus on how preconception care is understood, provided and experienced; this is followed by views on the adoption of technology, focusing specifically on use of technology for healthcare information and acceptability of a preconception care app. Clinician and women’s feedback were thematically consistent and data from both groups of participants are presented together. In the following sections, excerpts from the transcripts are referenced using HCP, for a clinician, and P, for a woman with diabetes, followed by a number for each participant in that group.
Themes and sub-themes.
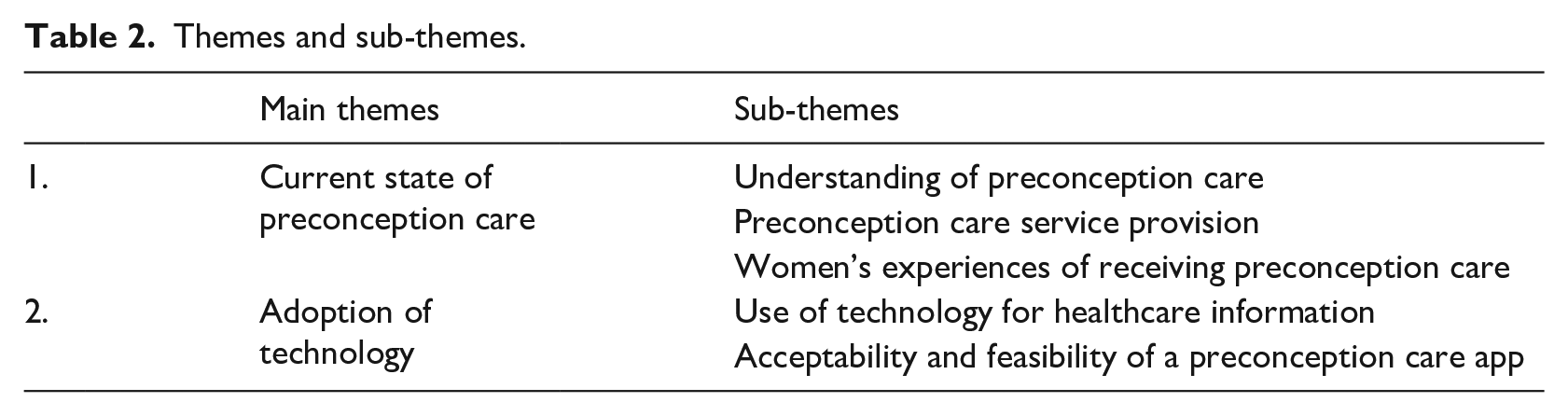
Current state of preconception care
The limitations of current preconception care provision and service delivery, in terms of accessibility, quality of information provided, pregnancy planning, clinician-patient encounter, understanding and uptake were discussed by both groups of participants.
Understanding of preconception care
Understanding of preconception care varied between different groups of participants (n = 19); clinicians were understandably more aware of preconception care and pregnancy-related complications than women, whose understanding appeared to be limited and sometimes non-existent. For example, clinicians discussed how preconception care helped to improve diabetes control and reduce risk of complications during pregnancy, whereas women believed the focus of preconception care was only diabetes control.
Preconception care is, care provided to women planning to become pregnant all in an attempt to optimise their health status before they become pregnant . . . just to make sure that their diabetes is under control . . . and they don’t have complications for which pregnancy would be a contraindication. (HCP5) It’s just really getting ready for your pregnancy more than anything else and the care which the hospital can offer you. Also, there really isn’t much, it’s all . . . working on HbA1c I think for most people. (P5)
Both groups of participants were generally aware of the need to improve blood glucose control before pregnancy, but some women did not understand the significance of this or the need to maintain good blood glucose control during early pregnancy. The adverse effect of high blood glucose levels on the pregnancy or the likelihood of experiencing pregnancy-related complications was also poorly understood.
I don’t really know much. I mean I’m sure it’s more difficult to control your blood glucose levels but yeah I’m not really sure. (P4) It [pregnancy-related complications] is not something that I know of personally, it’s not something I know much about. (P1)
A lack of knowledge about folic acid was also apparent. While clinicians seemed to understand the importance and role of a high dose (5 mg) folic acid in preventing birth defects, for example, they were uncertain about its timing and duration. Women participants similarly reported a lack of information regarding the use of folic acid.
Ladies with diabetes need to be on 5mg of folic acid rather than the 400 microgrammes that is readily available over the counter, so they need to go ask for it be specifically prescribed. (HCP6) Well, I don’t really know too much about it [folic acid] . . . I don’t really know too much on the subject. (P2) It’s something that I was sort of told to take when I was expecting my daughter, but I didn’t actually take it . . . I think partly because in my own mind, I had miscarried twice before I had my daughters and both times I had taken folic acid . . . I would be lying if I said I knew why [I was told to take it]. (P1)
Preconception care service provision
The possibility that women with DM could be on teratogenic medications, such as statins and angiotensin converting enzyme (ACE) inhibitors, which could adversely affect the foetus during pregnancy was reported by clinicians to be an issue of key concern. Clinicians felt that it was particularly important for younger women, those with type 2 DM and older women (over 35 years) to be closely monitored during the preconception period in order to identify and reduce the risk of complications.
It’s so important and generally it can be just taking time to get their control good, getting them onto folic acid. Yeah and especially ladies with type 2, younger age and women having babies later, you’ve got the risks that they might be on tablets that they shouldn’t be on for the pregnancy and that’s kind of a key thing. (HCP7)
However, younger and older women with type 1 and 2 DM (n = 5) in this study, whose ages spanned between 22 and 43 years, could not recall receiving any preconception care advice from their care team.
Given perhaps that I’m a student maybe my diabetes team don’t look at me as being of childbearing age . . . but I have never had any like any particular input [preconception care advice] from my care team . . . but I would have thought that being like a 22-year-old female, they would have like warned – like talked more to me about [preconception care], and like the importance of it. (P2) My first pregnancy was a massive shock . . . I just happened to do a test one day and it was positive and that was that, so I didn’t actually have anything pre-gestation at all. (P7)
Clinicians further reported that in their experience, many women with DM did not plan or discuss pregnancy plans with their healthcare team because they were uncertain and anxious about pregnancy. Women therefore preferred to wait until they had established that the baby was healthy, usually after the first trimester, before discussing pregnancy-related issues with clinicians.
Women’s experiences of receiving preconception care
Of the five participants who reported receiving preconception care, only two women were satisfied with the level of preconception care advice and support received from their diabetes team. The majority of women felt their preconception care experience was sub-optimal and explained that various opportunities such as clinic appointments or consultations which they believed could be used by clinicians to provide comprehensive preconception care advice were not properly utilised.
So, preconception I didn’t get any advice at all which really isn’t good enough . . . I could remember several appointments with the consultant at the hospital [and] them always saying ‘oh your levels are too high’ but never ever giving me, ‘if you keep below this number things will be better’. (P3)
Women reported generally not getting enough information from clinicians. They believed that vital preconception information such as the need to take 5 mg folic acid at least 3 months before conception or the glycated haemoglobin (HbA1c; a laboratory test which reflects the degree of control of blood glucose over the preceding 2–3 months) level to aim for, were sometimes not provided.
Some diabetes care teams don’t tell girls that they need to be on the 5 [mg folic acid] instead of the 4 [μg folic acid] and they don’t tell them to try and get their HbA1c in good order or their basal rates checked which I think is a bit silly really . . . in clinics they are just given so little information. (P5)
Women believed that clinicians had an unsupportive attitude towards pregnancy in women with DM and felt that they were often only told about adverse outcomes of pregnancy. Hence, women with DM felt discouraged about disclosing their pregnancy intentions or seeking preconception care advice from clinicians.
A lot of diabetes management come from like scare tactics and from what I gather with pregnancy that can be the same, so it’s all like ‘oh you are gonna do this otherwise you are gonna give birth to some deformed child’ which is quite negative. (P5). Particularly in diabetes I think sometimes it’s very difficult because people often feel reluctant to be honest with healthcare professionals because they feel that they are judged a lot of the time and sometimes I think people don’t always want to go to somebody who is medical to find things out. (P7)
Adoption of technology
It was identified from the data that women with DM were reticent to approach clinicians for preconception care advice due to their attitudes and approach to preconception care service provision, many therefore preferred to seek health information from other sources (e.g. technology). Participants highlighted the benefits of using technology for health information and expressed enthusiasm for a preconception care app that could help address some of the shortfalls in current service provision.
Use of technology for healthcare information
Women participants reported using technology to supplement information received from clinicians and fill knowledge gaps. Both clinicians and women participants in the study expressed a liking for technology due to its usefulness and convenience, and apps in particular were reported to improve knowledge by making information easily accessible.
We are in the realm of technology and so it’s become part and parcel of a lot of activities and service provision, so it’s something which more or less brings a lot of information to the doorstep of the patients. (HCP5) I google quite a lot of things, I know. Dr Google in all things. I have practically got my phone glued to my hands . . . if I need to know, if like something comes to mind that I want to think of, it’s usually my phone that I tend to use. (P2)
Both groups of participants reported that apps were pervasive and increasingly being used by women with DM to manage different aspects of their reproductive and diabetes health. Women in the study generally used numerous apps for different purposes and had wide ranging experience. They were also more likely to use an app that was simple and beneficial.
You can use an app almost for everything now. So, you enter your details and then you can keep track of your period and everything. So, you can also add all the other things that you need to check, so [if] it’s blood glucose or if you have to do some other tests. (HCP3) So, I use an iPhone where I use the kind of regular Facebook, Instagram, Twitter, I have my bank apps, I have the train line apps, I have a libraries app that I use, I have a weather app but again I’m not a huge app person . . . but if something is easy to use and helpful, then it would be something I would use regularly. (P9)
However, despite the pervasiveness of information and communication technology (ICT), women with DM who consulted technology for information noted that preconception care information, especially for women with DM, was lacking. One woman expressed concern about this lack of readily available information.
When you google it . . . there doesn’t seem to be much out there about like preconception especially with diabetes because obviously, it needs to be tightly controlled, your blood sugar and things, but there doesn’t seem to be much. (P2)
Acceptability and feasibility of a preconception care app
There was a consensus among all participants that apps were generally easy to use and appealed to women of different age groups. They felt that an app with preconception care information would be of benefit to women with DM who were planning a pregnancy, as they were motivated to stay healthy in order to achieve good pregnancy outcomes.
I think it’s a great idea to be honest. I mean everything now is apps and technology, and there is nobody who doesn’t know, even my mum knows how to use an iPhone and she is nearly 60 so it would be a great idea. (P8) I think great because that’s what people use . . . most women can intuitively work through [apps] regardless of age and stage . . . I’m working with a girl . . . she wants to start a pregnancy in the best possible shape both physically and biochemically. . . if there was any kind of [preconception care] app for her, that’s the sort of person who would benefit from it. (HCP8)
Most clinicians further recognised the challenge involved in persuading women to discuss their pregnancy intentions and/or establish rapport with them prior to pregnancy. They felt that a preconception care app would help inform women of the importance of working with their healthcare providers in order to attain good pregnancy outcomes, which could also help improve engagement. Women agreed that the convenience of a preconception care app would not only appeal to many women with DM but it also had the potential to increase uptake.
It would bring about the engagement with the service providers so that they know they should work together for their own benefit. So, I think it’s a really good thing and if they’ve got the app by them, to be looking at, at their leisure . . . it’s even more appealing. (HCP5) You might actually get more women actively seeking it [preconception care], if that sort of thing was available . . . I think I would be more likely to look it up like that now than see the diabetic specialist or whatever, I think I would probably do that first. (P3)
In addition, both groups of participants reported that women with DM had a close relationship with their phones, and a preconception care app with information on diet, blood glucose control, folic acid, and so on would be an ideal way for women to receive pertinent preconception care advice. Most importantly the need to make preconception care information more accessible to women with DM was highlighted.
Overall, views on potential use of the app for preconception care were positive. Most clinicians and all women acknowledged that women with DM need preconception care advice and although the use of an app for preconception care was a novel approach, the incorporation of preconception care information within an easily accessible and highly accessed platform had the potential to provide more women with preconception care information.
So, women do need [preconception care] advice and if you are going to put it in an app and it’s something that’s easily accessible then it’s a good idea. (HCP4) It [preconception care]’s not something that I know of personally, it’s not something I know much about so to be able to have an app to go into and get information from, I think is really important. (P1)
Another woman reported the urgent need for a preconception care app and noted that for women who were not provided with preconception care information by their healthcare team, a preconception care app was an ideal way to deliver relevant information.
I think it’s probably the best way to get information across to people like myself who obviously haven’t been informed of like the importance of preconception especially in diabetes . . . I think it’s a good idea. To get the message out there . . . to have some understanding is more important than having no understanding. (P2)
Participants expressed confidence in women’s ability to engage and interact with the app, and to use it effectively for preconception care. Women noted the difficulties in accessing preconception care information via the traditional means such as clinicians or leaflets, noting that while access to both could not always be guaranteed, a preconception care app would provide a readily available repository of information which could help improve access to preconception care.
I think having something there that I know that I can always reach for and look at if I am suddenly having any question or a concern or I’m looking for more information because you can’t always call a doctor and you can’t always go look on a pamphlet or search online. (P4) It would be good to have somewhere to go to get information specifically for diabetes and preconception. (P9)
Both groups of participants further noted that a preconception care app would provide a handy, yet discrete way for women to access preconception car information. Hence, the majority of clinicians were enthusiastic about integrating the app into their consultations, adopting it within their organisations and recommending it to women with DM in their care while women participants were eager to use it and recommend it to other women with DM, when developed.
Discussion
To our knowledge, this is the first study to examine clinician and women’s views regarding the use of an app for preconception for women with DM. The findings reveal that in line with previous studies,11,13,14,17 women with DM continue to experience fragmented and inadequate preconception care and hence have poor understanding and/or awareness of preconception care and its importance in reducing pregnancy-related complications. It is evident that current approaches to preconception care service provision are hindered by problems within healthcare systems. For example, in the United Kingdom, the demand for health care is growing at 4 per cent but funding by only 1 per cent. 44 Increased demand for services combined with staff shortages and delayed or cancelled clinics results in reduced access and/or opportunities to receive care. 45 Although guidelines8–10 recommend annual preconception care information be given to all women of childbearing age, the extent to which this is achieved is limited. Several studies have called for a more innovative and sustainable solution to preconception care delivery for women with DM and increasing patients’ access to information via smartphones and apps.14–16 The proposed preconception care app provides the opportunity to overcome current difficulties and improve preconception care information provision to women with DM.
Participants in this study believed that preconception care provided via eHealth technology, specifically via a smartphone app, could provide a more flexible and convenient way to access preconception care, improve pregnancy planning and overcome long-standing shortfalls in service provision. eHealth, specifically the smartphone app, is instrumental in making care more accessible, particularly where resources are limited, and enabling individuals to be more actively involved in their healthcare. 27 Their use is also supported by the World Health Organisation (WHO) eHealth strategy, United Nations (2030) sustainable development goals and the global consensus on preconception care25,46,47 as an important way of giving patients more control over their health and care and providing cost-effective patient-centred care. eHealth is increasingly being used around the world to prevent and monitor diseases, provide health education and encourage self-management; it has ensured that patients can access healthcare from a variety of locations, not just at the clinic or hospital. 25 This is of particular importance to future preconception care service delivery given that current preconception care strategies (mainly provided in clinic settings) continually fail to meet the preconception care needs of women with DM.8,14,15,17
This study highlights that many women with DM do not plan or discuss pregnancy intentions with the healthcare team and only present to medical care after pregnancy has occurred. Several studies18,48 have reported that inadequate information and preparation for pregnancy contribute to women’s anxiety and fear of pregnancy complicated by DM, hence discouraging women from seeking preconception care. Women in this study also described how ‘scare tactics’ have made them feel less inclined to consult their health care professionals for preconception care. It is evident that the way preconception care advice is framed affects women’s decision to seek (or not seek) preconception care.17,49 For example, advice framed in a motivating, positive and supportive way is more likely to be heard and translated into action.15,17 Several studies15,16 have suggested that clinicians focus on positive aspects of pregnancy for women with DM, rather than only on the problematic aspects. Hence, it is important that the proposed preconception care app adopts a positive approach in order to improve uptake, and motivate and support women during the preconception period.
Clinicians and women in this study expressed a high level of interest, support and acceptance of a preconception care app which could help overcome barriers of traditional preconception care practice and contribute to improved pregnancy outcomes for women with DM. Improved, flexible and convenient preconception care access such as that provided via the proposed app for women with DM is vital to reducing high-risk pregnancies and making more effective use of limited healthcare resources. Globally, healthcare systems are struggling with an increased demand associated with the growing burden of chronic diseases including DM.1,44 The findings of this study also indicate agreement with the literature 31 regarding app use to empower patients, extend the reach of health interventions and overcome problems associated with traditional face-to-face care. Women of childbearing age increasingly rely on smartphone apps because of their advanced functionalities (including Internet access combined with photos, videos and geo-positioning capacity), mobility, ease-of-use and portability. 50 About 90 per cent of the time spent on mobile phones is spent on apps, which are preferred over web or computer-based applications, 51 making the preconception care app a valuable tool for giving more women access to preconception care. However, barriers to mobile app usage such as cost of the app, Internet accessibility and data security could affect acceptability of the preconception care app. Hence, it is important that the app is made freely available or very affordable, can be accessed without Internet connection (after initial download), utilises easy to use security features, for example, password protection and regular password update, and provides clear privacy policies regarding data storage/utilisation. 52
A co-design approach was adopted in order to ensure that the preconception care app was acceptable to the target audience (women with DM and clinicians),33–35 and findings suggested that the preconception care app was an ideal way to deliver preconception care to women with DM. This approach to app development contrasts with the more traditional ‘waterfall’ method, a top-down approach that does not include the end user in the development process, and which is associated with problems with use, adoption and attrition. 53 Participants’ involvement and acceptance of the preconception care app has positive implications for the app because participants’ level of acceptance of an app can influence future implementation, uptake, adherence and health outcomes.33,53 Due to the importance of optimising blood glucose levels prior to conception, it is particularly important that the app reaches women with DM before pregnancy; hence, the high level of enthusiasm and acceptance of the app by clinicians and women will play a major role in the successful integration of the app into routine diabetes care (in both primary and secondary care settings). The input of women with DM and clinicians in this phase, is vital to ensure the preconception care app developed in phase 2, has the best chance of success.
Strengths and limitations
To our knowledge, this is the first study to propose the use of an app to improve current preconception care service provision and explore the views of clinicians and women with DM regarding a preconception care app for women with DM. A co-design approach was employed in this study to ensure that the proposed app was suitable and acceptable to both service users and clinicians. The findings of this qualitative study may be transferrable to other similar settings, although women with DM were recruited via social media and therefore may not be representative of the general population of women with DM. Women from a range of geographic areas were included in this study, showing that the challenges and limitations of current preconception care are not an isolated problem; however, women were self-selected as this was an important topic to them and therefore may not reflect experiences of all women with DM. Although the qualitative findings were not validated by quantitative analysis, rigour and trustworthiness were ensured. The analysis of the views of women and clinicians together may have strengthened the article but may also have limited the depth of reporting. Transcripts were anonymised and not returned to participants for comments, and they did not provide feedback on the findings due to the methodological and ethical concerns associated with this process.54–57
Conclusion
Given the dramatic rise in prevalence of DM in women of childbearing age, 1 there is an urgent need to change the way preconception care is delivered in order to optimise maternal and foetal outcomes. Although eHealth has created an opportunity to overcome shortfalls in service provision, its use in preconception care of women with DM is still in its infancy. The acceptability of mobile health technology, in the form of a preconception care app, to both women with DM and clinicians creates an important opportunity to overcome existing barriers to service provision, delivery and uptake, and improve pregnancy outcomes for women with DM. This is important given the considerable shortfalls in current preconception care provision in the United Kingdom and around the world.
Supplemental Material
COREQ_checklist – Supplemental material for Exploratory study of clinician and patient views regarding the use of a preconception care app for women with diabetes
Supplemental material, COREQ_checklist for Exploratory study of clinician and patient views regarding the use of a preconception care app for women with diabetes by Chidiebere Hope Nwolise, Nicola Carey and Jill Shawe in Health Informatics Journal
Supplemental Material
TOPIC_GUIDE – Supplemental material for Exploratory study of clinician and patient views regarding the use of a preconception care app for women with diabetes
Supplemental material, TOPIC_GUIDE for Exploratory study of clinician and patient views regarding the use of a preconception care app for women with diabetes by Chidiebere Hope Nwolise, Nicola Carey and Jill Shawe in Health Informatics Journal
Footnotes
Acknowledgements
The authors thank the clinicians and women who took part in this study, as well as the two researchers (Dr Fiona McGregor and Dr Michelle King-Okoye) who coded portions of the data. The primary author (CHN) was supported by a grant from Funds for Women Graduates (FfWG) until September 2016.
Author contributions
C.H.N. was responsible for the conception, design and writing of the manuscript. N.C. and J.S. assisted with study design and writing of the manuscript. All authors critically reviewed the manuscript and approved the final version submitted for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.