
Abstract
Telerehabilitation programs can be employed to establish communication between patients and healthcare professionals and empower patients performing their training remotely. This study aimed to identify patients’ requirements after a total knee replacement following a self-training rehabilitation program, leading to the design and development of a telerehabilitation program that can meet the stakeholders’ actual needs. System design, development, and testing were conducted in five iterations based on a participatory design approach. Data collection was performed using interviews, observations, prototyping, and questionnaires. It was found that the main barriers facing the existing rehabilitation program were a lack of clear communication, lack of relevant information, and healthcare professional’s feedback. The participants emphasized the main themes of communication, information, training, and motivation in the process of design and development. In using the telerehabilitation program, the patients reported a high level of user-friendliness, flexibility, and a sense of security. This study has identified obstacles in the current rehabilitation program and revealed the potential effectiveness of using asynchronous communication and sensor-based technologies by employing participatory design and development. A higher level of portability and flexibility were observed. However, future studies and development are required to investigate the overall usability and reliability of the telerehabilitation program.
Keywords
Introduction
Studies have shown that postoperative physical rehabilitation programs had a significant influence on health recovery. 1 Therefore, a wide variety of rehabilitation programs are being advised to treat postoperative recovering patients. Accordingly, self-training approaches have been highly recommended for patients recovering from knee surgery. 2 Lee et al. 3 showed that a tailor-made exercise program has a significant positive impact on patients’ adherence and health recovery among senior patients with knee osteoarthritis (KOA). Moreover, it has also been shown that the therapist–patient relationship has a positive influence on the observed clinical outcomes. 4 Baker et al. 5 reported that an in-home training program has a considerable impact on KOA and can lead to substantial improvements in patients’ quality of life.
A telerehabilitation program (TRP) utilizes computers, information, and communication technologies to provide rehabilitation services at a distance. A proper telephysical rehabilitation program enables the healthcare sector to introduce a higher quality of clinical services and allows rural communities to enhance accessibility to the healthcare system.6–8 Previous studies have indicated that the majority of the patients were satisfied and felt more confident due to the TeleHomeCare solutions provided.9,10
As an in-home rehabilitation solution, real-time audio or video communication has been utilized. The efficacy of these solutions on patients’ functional performance,11–13 patients’ and physiotherapists’ satisfaction,14,15 and system costs16–18 has been investigated and has shown positive results.
This study sought to develop a TRP with higher degrees of portability and no dependency on real-time video conference communications. It also sought to satisfy users’ requirements by providing a tailored TRP to patients’ specific needs. Consequently, it is hypothesized that the rehabilitation can be facilitated by a combination of asynchronous communication, sensor-based technologies (utilizing sensors to measure clinical parameters),19,20 and on-demand synchronized, locally stored information services with the TRP. The target group in this study are patients who have undergone a total knee replacement (TKR).
It should be mentioned that the integration of telecommunication and technologies in healthcare services is deemed to be challenging and has had high failure rates.21,22 Lack of a clear understanding of the clinical and practical challenges, as well as specific requirements, had been the factors behind a lower success rate of introduced solutions. 23 Kushniruk and Nøhr 24 showed that participatory development improves the chance of the acceptability of a rehabilitation program because it assembles user input and involves users in the rehabilitation development procedure. In addition, the cost and resource efficiency of this approach were also shown. 25 Although this method increases the complexity of development, it enables the developers to identify the actual requirements, 26 understand the barriers, 27 and lead to a higher end-user involvement 28 and long-term sustainability. 29 As a result, participatory design (PD) and development were utilized in several studies implementing telemedicine and e-health solutions.30–32 In this study, we decided to use the PD method in developing our TRP.24,33
Materials and methods
Participants and the recruitment process
The project participants were divided into two groups of patients, health professionals (two physiotherapists, a nurse, and an orthopedic surgeon), three researchers, four student assistants, and two software developers.
All patients were identified based on criteria by a healthcare professional at Aalborg University Hospital. A letter of invitation to participate in this study (containing project details and workshop schedules) was sent to all patients. The patients could then express their willingness to participate by informing the project director using the contact information provided in the invitation letter.
The first group of patients was selected from the patients who had already completed their regular rehabilitation program. They were actively involved in the system developments and preliminary testing (first phase, details in section “Theoretical framework”). The second group of patients was recruited prior to undergoing their knee surgery to test the TRP system for a period of 2 weeks (in phase two). Therefore, they were able to use the TRP after the surgery. This second group of patients did not participate in the system development process, and they participated only in the second phase of the study.
All patients recruited in the study were based on the following inclusion criteria:
Had or planned to have a primary TKR;
Ability to understand and accept the trial procedure (evaluated by a healthcare professional);
Ability to participate in teamwork (assessed by a healthcare professional);
Resident in municipalities around Aalborg, Denmark;
Discharged or being discharged for a regular rehabilitation treatment program;
No other conflicting disorders (evaluated by a healthcare professional).
Theoretical framework
Self-determination theory (SDT) was used as a theoretical starting point to increase the effectiveness of behavior change interventions for patients after knee surgery. SDT offers a framework for understanding the role of individualization in motivation. The theory highlights how the fulfillment of basic needs such as autonomy, relatedness, and competence are essential for initiating and maintaining changes in lifestyle and health behavior over time. 34
Study design and data collection
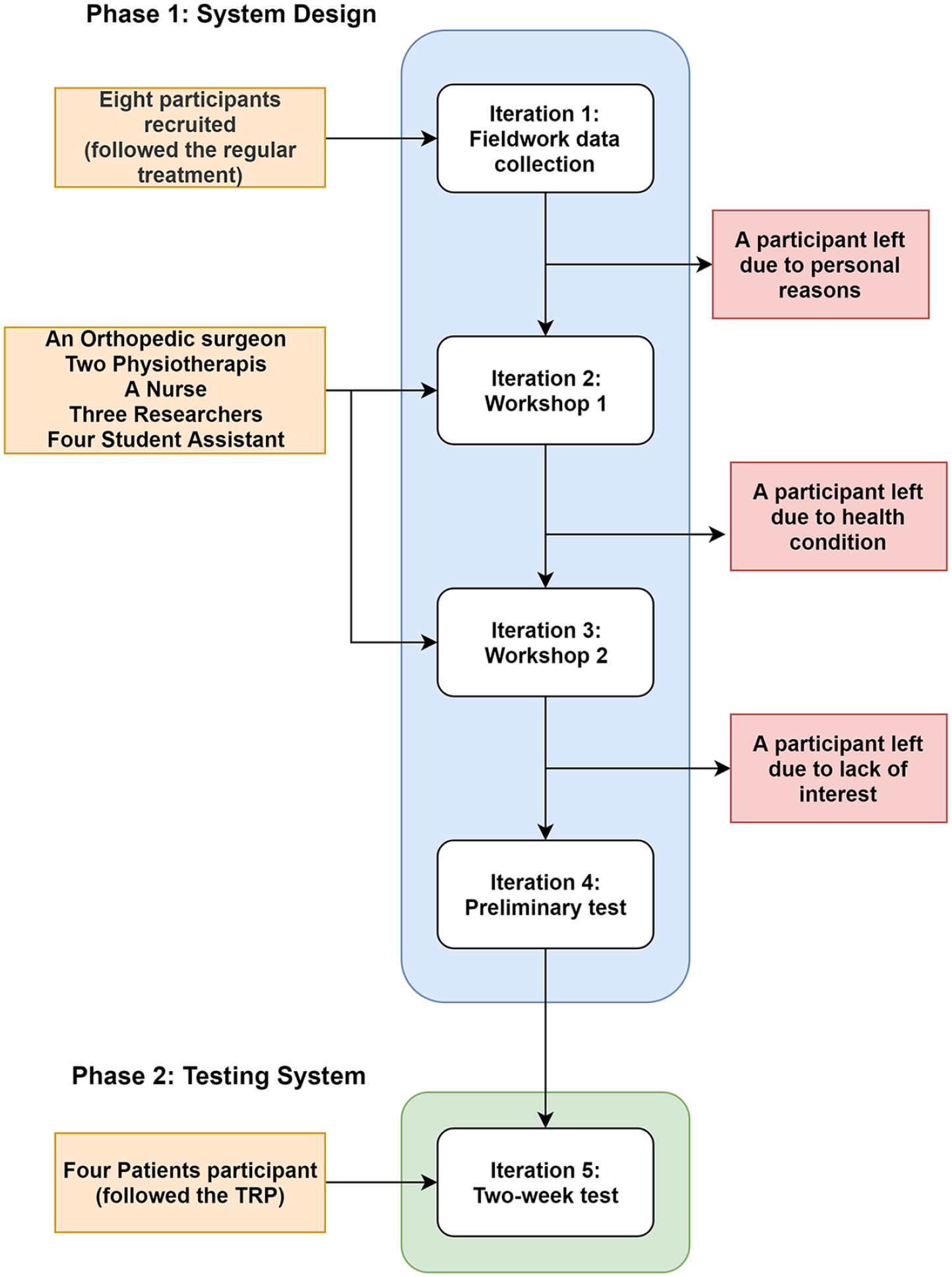
The design and development of the TRP were conducted based on the PD33,35 in two phases and five iterations, as shown in Figure 1. Based on the previous studies, the iterations can be divided into idea generation (telling), development (making), and test and evaluation (acting) activities.33,36 Further details about each iteration are clarified in Figure 1.
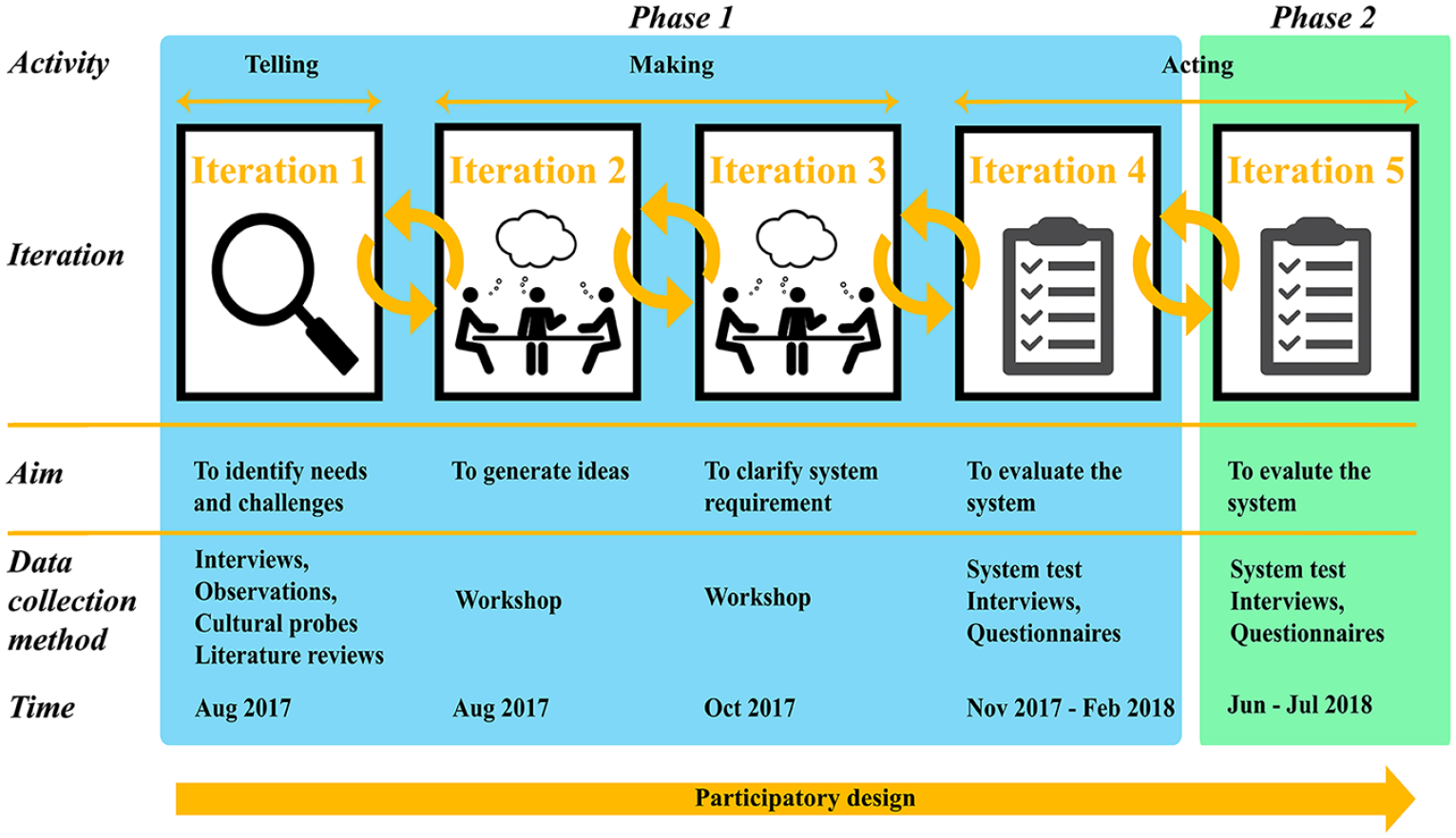
Study design. The study is divided into two phases and five iterations. The aims, data collection methods, and time for each iteration are shown in the figure.
Iteration 1: fieldwork data collection
This iteration sought to identify the needs and challenges of the self-training program. Initially, a review of the literature was conducted in order to investigate the previous relevant studies. This was followed by a semi-structured interview 37 and participant observation 38 at participants’ home. The interview focused on identifying patients’ unresolved needs and challenges posed by the patients’ experiences with the current self-training rehabilitation. Finally, the patients were asked to provide relevant cultural probes39,40 using text messages, emails, or photos within 2 weeks after the interview.
Interviews were tape recorded, and observational notes were documented at the meeting. The interviews stopped when an indication of data saturation was observed. The interviews were transcribed by J.H.S. and A.K.
Iteration 2: first workshop
The primary objective of the first workshop was to generate relevant ideas and draw preliminary paper prototypes, which lasted 2.5 h. Initially, a common ground 33 between the participants was established by the workshop organizer. The participants were divided into two mixed working groups comprising healthcare professionals, patients, researchers, and developers. The workshop was organized in three steps, each of which was involved with identifying the relevant ideas and solutions in three time periods (Figure 2(a)). Pre-printed posters (see Figure 2(b)) were laid on each table showing four possible sites (home, physiotherapy clinic, hospital, and outside) where the patient may need to have access to the rehabilitation program and relevant information (see Figure 2(c)).
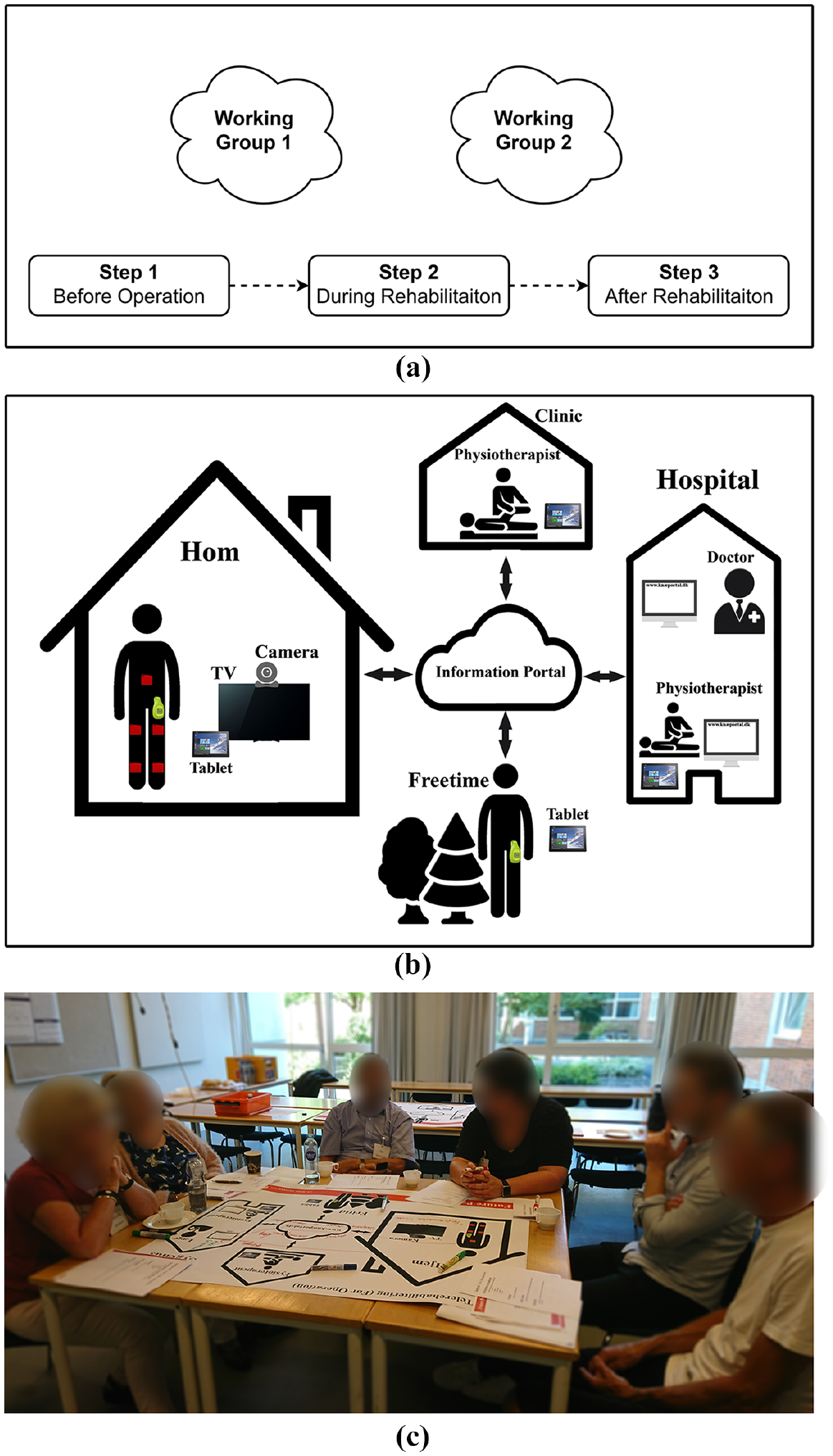
Patient workshop: (a) in the first workshop, participants were organized into two mixed working groups following three steps to generate ideas that could resolve the identified needs, (b) participants were asked to draw and write down their ideas on the given pre-printed sheets showing the possible locations where they might utilize the telerehabilitation system, and (c) the working group was sitting behind a roundtable and generated ideas corresponding to each step.
The group facilitators (J.H., B.D.) conducted each step of the workshop based on predefined topics and questions. They emphasized on training, communication, information, motivation, transportation, and physical activities. The prototype of TRP has been developed based on the obtained data.
Iteration 3: second workshop
The second workshop aimed to qualify and clarify the ideas for the development of TRP. The workshop was organized into three parallel and independent working groups (described in Table 1 and Figure 3) and lasted 2.5 h. All participants in the previous workshop were invited to the second workshop.
Description of the second workshop process.
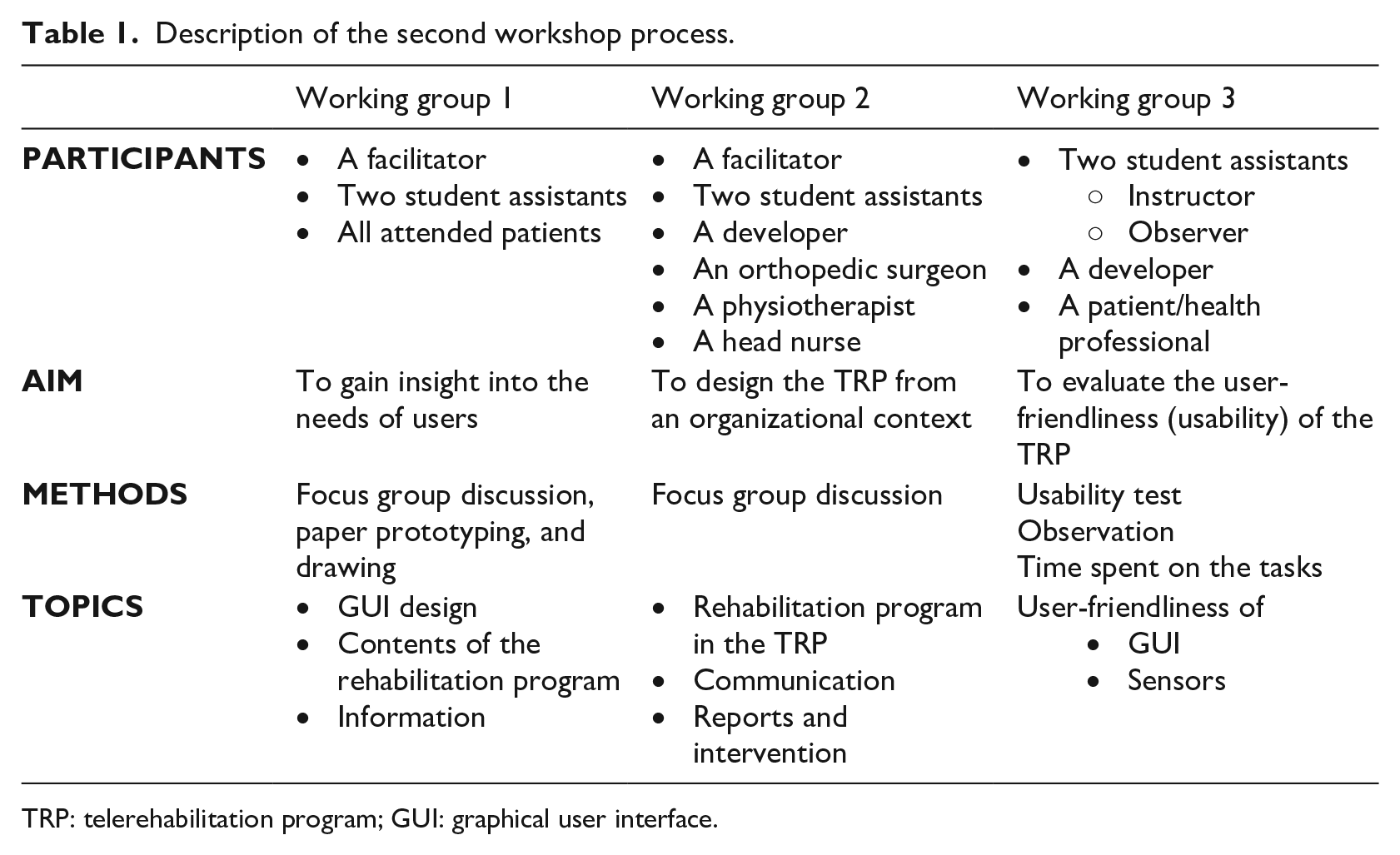
TRP: telerehabilitation program; GUI: graphical user interface.
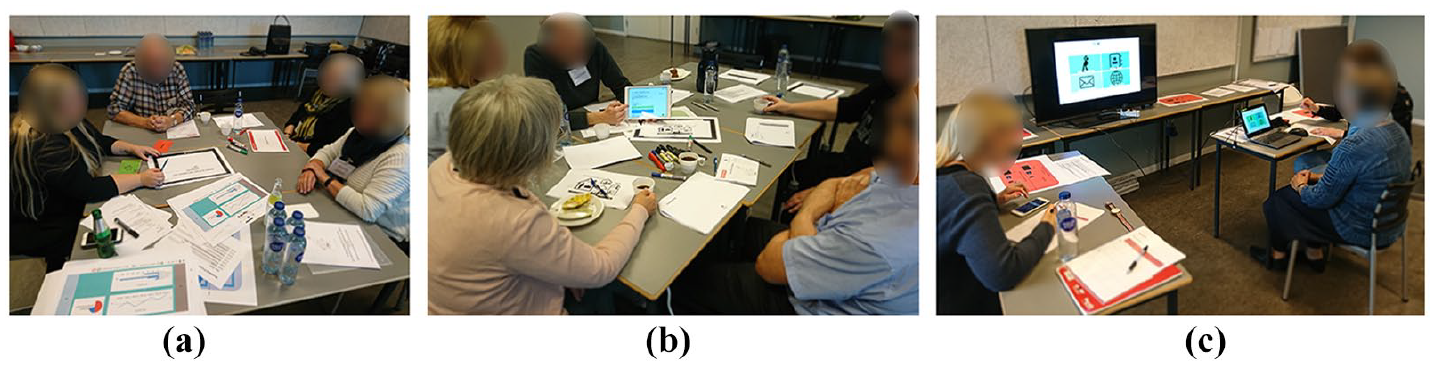
Participants were divided into three working groups: (a) working group one carried out brainstorming and prototyping, (b) the second working group investigated the clinical responsibilities for the TRP, and (c) the third working group carried out the first system test.
The first working group (consisting of the patients, two researchers, and a facilitator) sought to collect insight into the user’s needs and system requirements. Brainstorming, paper prototypes, drawing an idea, graphical user interface (GUI) design,41,42 and guided discussion methods regarding the technical restrictions were all used in order to illuminate the patients’ needs (see Table 1).
A focus group interview 43 was carried out by three healthcare professionals, a developer, and a facilitator in order to develop the ideas on the healthcare sector, clinical responsibilities, and relevant patient-reported outcomes (PRO) during the rehabilitation period. In each phase, the translation of services and healthcare professional supervision into an electronic system was discussed.
In the last group, two student assistants and a developer asked each of the participants (patients and healthcare professionals) to perform five predefined tasks in order to test the developed prototype. The prototype consisted of two wearable sensors and a Microsoft Windows 10 tablet, customized running project-developed software. During the test, one of the researchers was responsible for instructing users and helping them if they encountered any difficulties while completing the tasks. The second researcher collected the verbal and non-verbal responses of patients and the elapsed time for each task.
Iteration 4: preliminary testing TRP at the patient’s home (iteration 1)
The main aim of this iteration was to acquire patients’ feedback by testing the TRP. Two researchers visited each patient’s home. One of the researchers was responsible for instructing the patient and actively engaging with them. The second researcher collected the observational data. The program was evaluated in four steps (see Figure 4). Initially, the patient was instructed on how to use the telerehabilitation program and monitored in several tasks in order to assess the user-friendliness of the TRP. While the patients were completing the tasks, the verbal and non-verbal observations were collected. In the next step, the patients were asked to complete a Likert-type scale questionnaire for evaluating the user-friendliness of TRP. Finally, a semi-structured interview was conducted in order to investigate the patients’ experience and satisfaction with the technology and presented TRP.

The preliminary system test was conducted in the fourth iteration in order to investigate the user-friendliness of the system at the patient’s home.
Iteration 5: testing TRP at the patient’s home (second phase)
The primary objective of the second home test was to investigate the preliminary user-friendliness of the revised TRP (further technical details on the TRP are provided in Naeemabadi et al. 44 ), and users’ experiences for the more extended period are given by including those users who did not participate in the development process. The identical data collection methods were reused from the previous iteration.
The patients were identified and recruited before undergoing knee surgery. Two researchers met the patients prior to the operation at the patients’ homes and provided them with the TRP and the relevant instructions. Patients were asked to use the TRP for 2 weeks, and this visit was followed up by a second home visit (after week 2) scheduled in two steps. In the first step, a semi-structured interview was conducted in order to acquire patients’ experience in the rehabilitation process. In the second step, patients were asked to fill out a questionnaire (employed in the previous iteration).
Data analysis
All interviews and observations were transcribed. The data from interviews, observations, documents, and probes were analyzed inspired by Kvale and Brinkmann 45 using NVivo 11.0 (QRS International, Melbourne, Australia) in the same process in the following steps:
The collected data in the first iteration was reviewed and processed to extract the key codes.
The keywords were discussed to ensure intersubjectivity between the authors.
The main themes were identified based on the coded data in the NVivo.
The collected data in each iteration were processed and categorized based on the identified themes.
Results
Eight patients were identified and assigned in the first group. Table 2 represents the demographic data of the users.
Demographic data of participants.
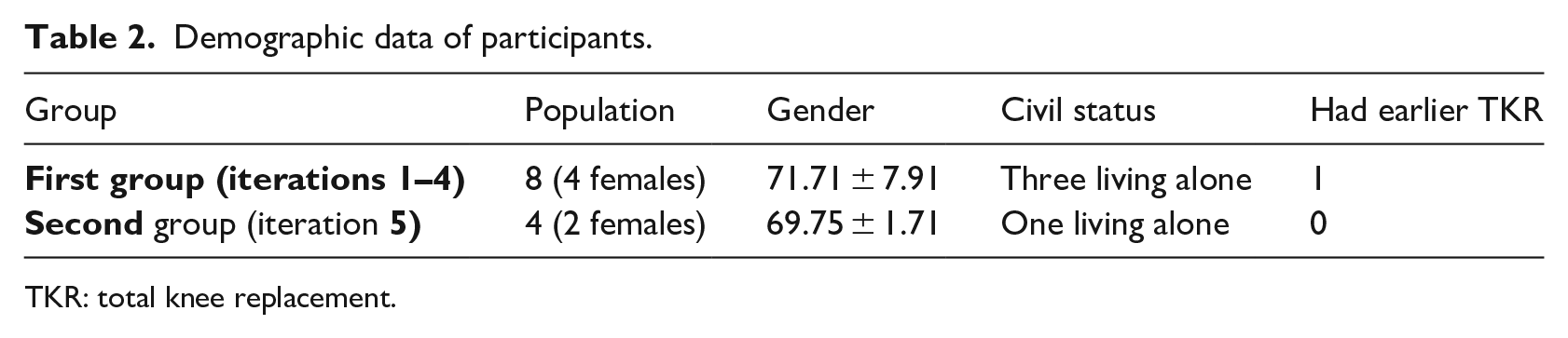
TKR: total knee replacement.
Five of the eight patients in the first group participated in all five iterations. One of the patients left the study after the first iteration (due to personal reasons), one more patient after the second iteration (due to a medical condition), and a third patient left the study after the third iteration (due to lack of interest). All four patients in the second group completed the second phase of the study. Figure 5 shows the graphical presentation of the participant in the study.
Graphical presentation of the participants in the study.
The collected qualitative and quantitative data in each iteration individually are presented in the following sections.
Iteration 1: fieldwork data collection
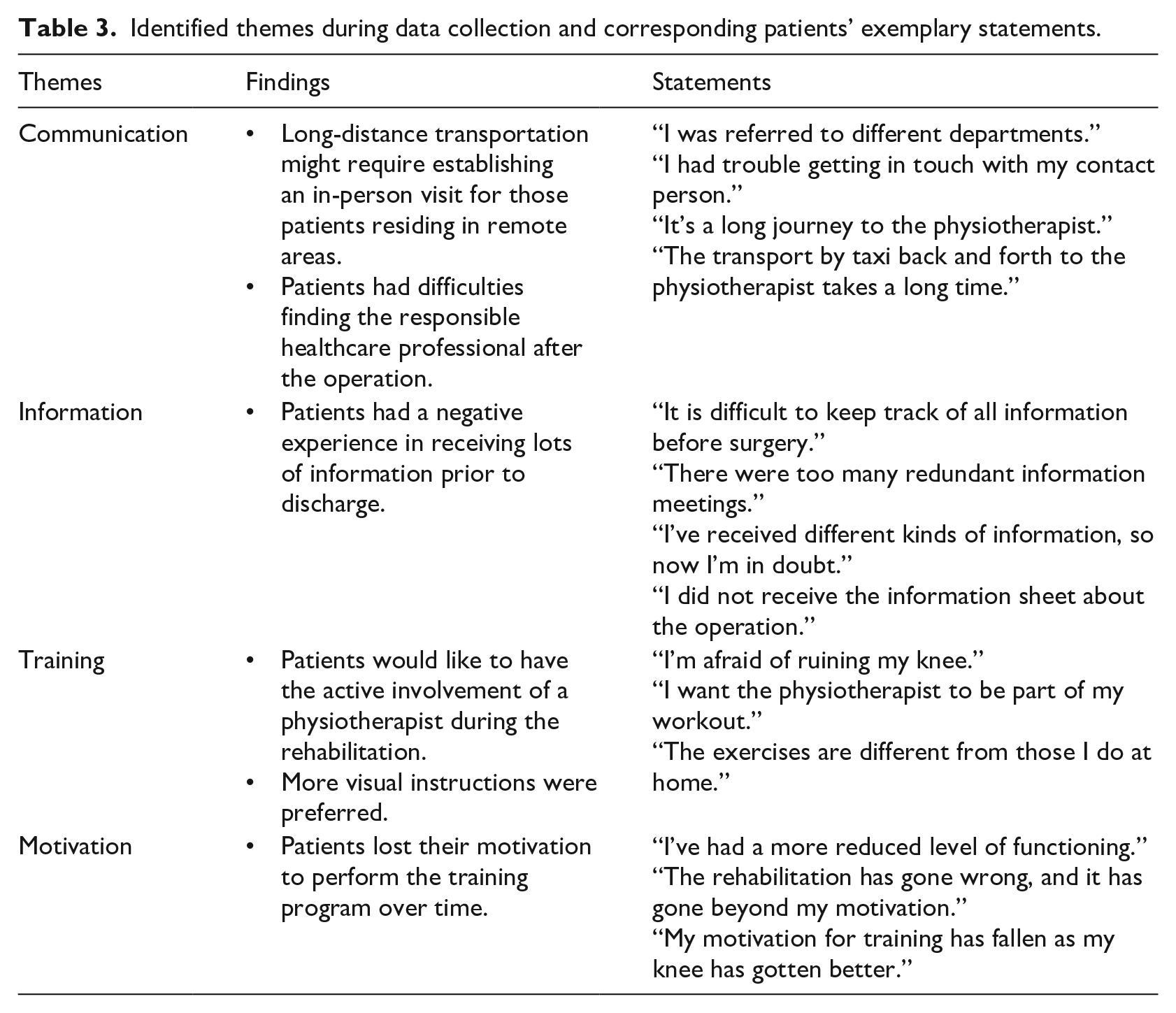
The identified requirements for the TRP were (1) lack of a transparent communication platform, (2) lack of a resource to provide the relevant information, and (3) lack of a healthcare professional’s intervention during home-rehabilitation. Accordingly, the collected data were categorized into four main themes, addressing the challenges and needs observed in the regular self-training program. Table 3 shows the themes and corresponding participant statements collected during the interviews.
Identified themes during data collection and corresponding patients’ exemplary statements.
Iteration 2: first workshop
The preliminary ideas were generated in the first workshop in order to overcome the identified challenges; however, some of the ideas might not be feasible to implement due to limitations in the available technologies. 46 The ideas generated in the workshop were grouped into the five themes (defined in the previous iteration) and are shown in Table 4.
Workshop ideas.
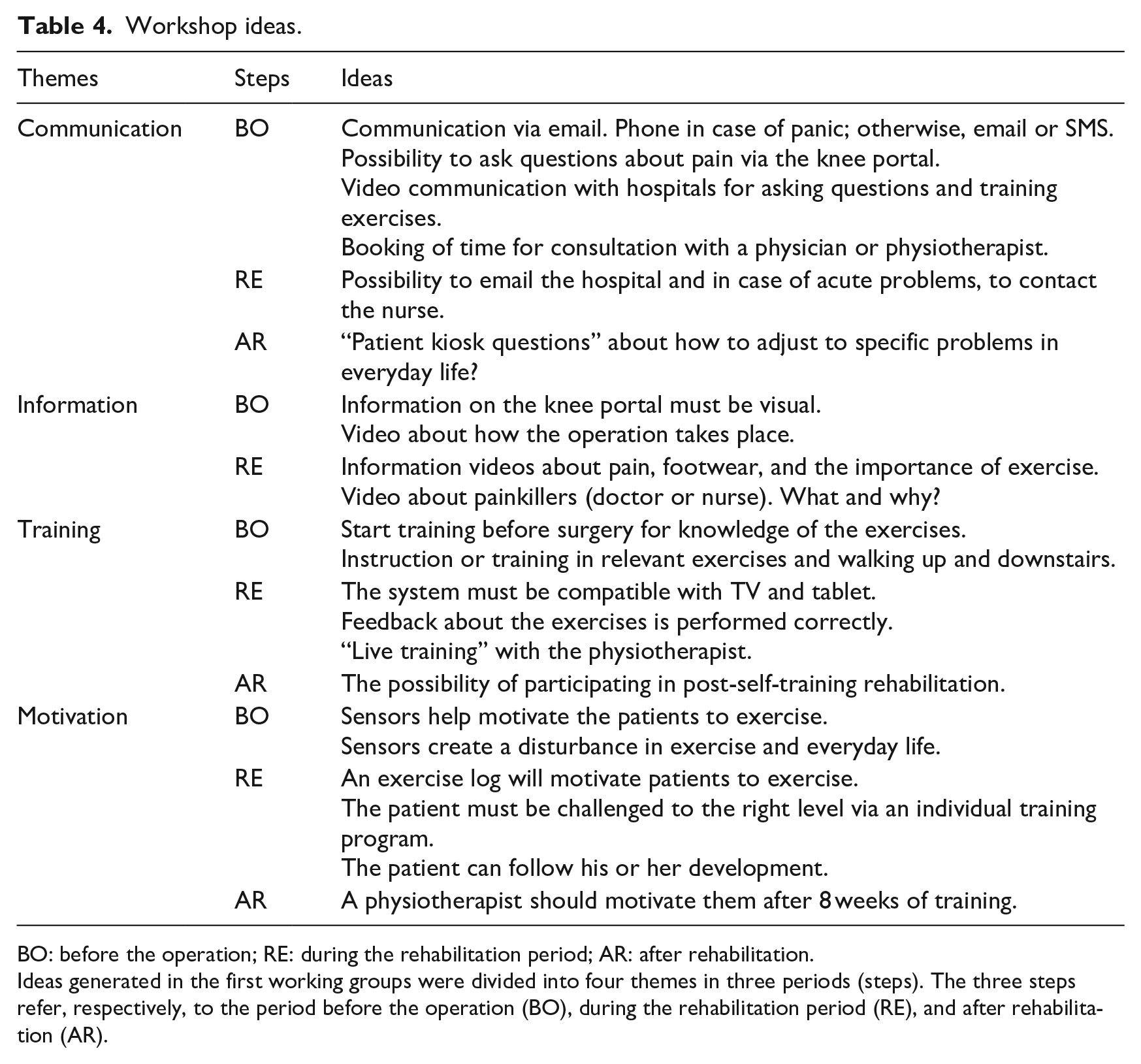
BO: before the operation; RE: during the rehabilitation period; AR: after rehabilitation.
Ideas generated in the first working groups were divided into four themes in three periods (steps). The three steps refer, respectively, to the period before the operation (BO), during the rehabilitation period (RE), and after rehabilitation (AR).
The participants believed that users’ motivations might be improved by healthcare professionals’ feedback and patients’ reports. Moreover, it was suggested that a remote communication platform is established. Also, it was believed that the TRP should offer relevant visual information and instructions for the patients as well as live training (with visual instructions and feedbacks).
Based on users’ feedback from the first workshop, the prototype of the software was developed. The TRP was developed for a 10-in Microsoft Windows 10 Tablet and was compatible with touch screens. Two wireless motion sensors were also utilized to track the user’s exercises based on the provided method in Naeemabadi et al. 47 Figure 6 shows the paper drawing of the home page of the TRP software and the corresponding developed GUI.

Paper drawing of (a) the first page of the application and (b) graphical user interface of the application.
Iteration 3: second workshop
Findings from the first working group are categorized into messaging, training, and information for the patient’s themes and stated in Table 5.
Generated ideas in the first working groups divided into GUI design, contents, and information themes.
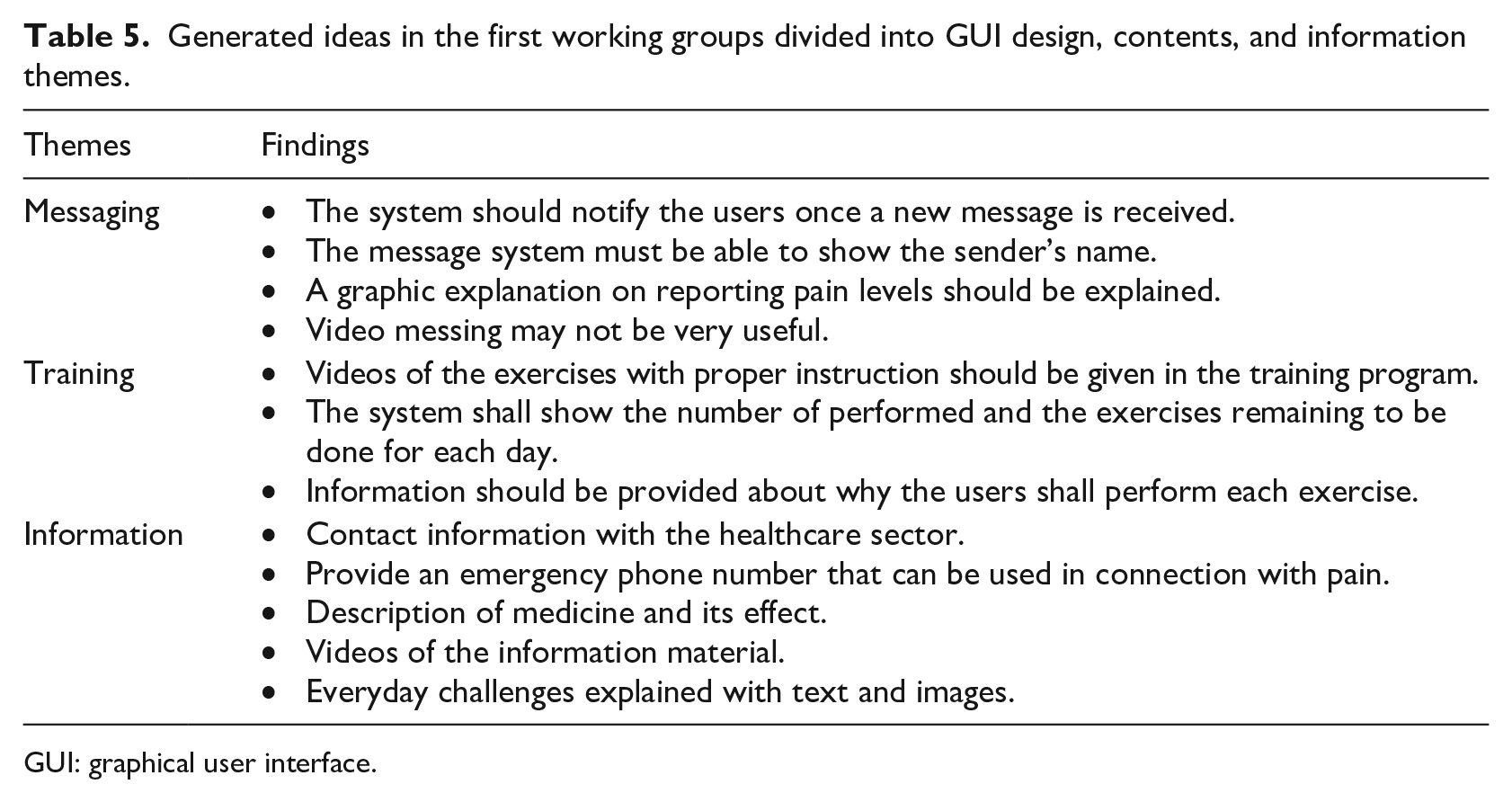
GUI: graphical user interface.
In the second working group, it was decided that the TRP should be based on the following requirements:
Healthcare professionals should have access to the patients’ data with an individualized two-factor authentication;
The TRP should present an 8-week rehabilitation program;
Healthcare professionals should be able to define and update patients’ exercise programs;
The patients are asked to report their pain level and knee circumference every third day;
The patients are asked to report their knee score using the Oxford Knee Score 48 every 14 days;
The healthcare professional should be able to track patients’ reports and adherence to the exercise program visually;
Two-way communication should be established between users.
Finally, in the last working group, both participatory observations and time spent on each task were collected. Table 6 shows the findings of participant-observation conducted while participants were performing the tasks.
The verbal and non-verbal findings collected in the third working group, while the users were performing the given tasks.
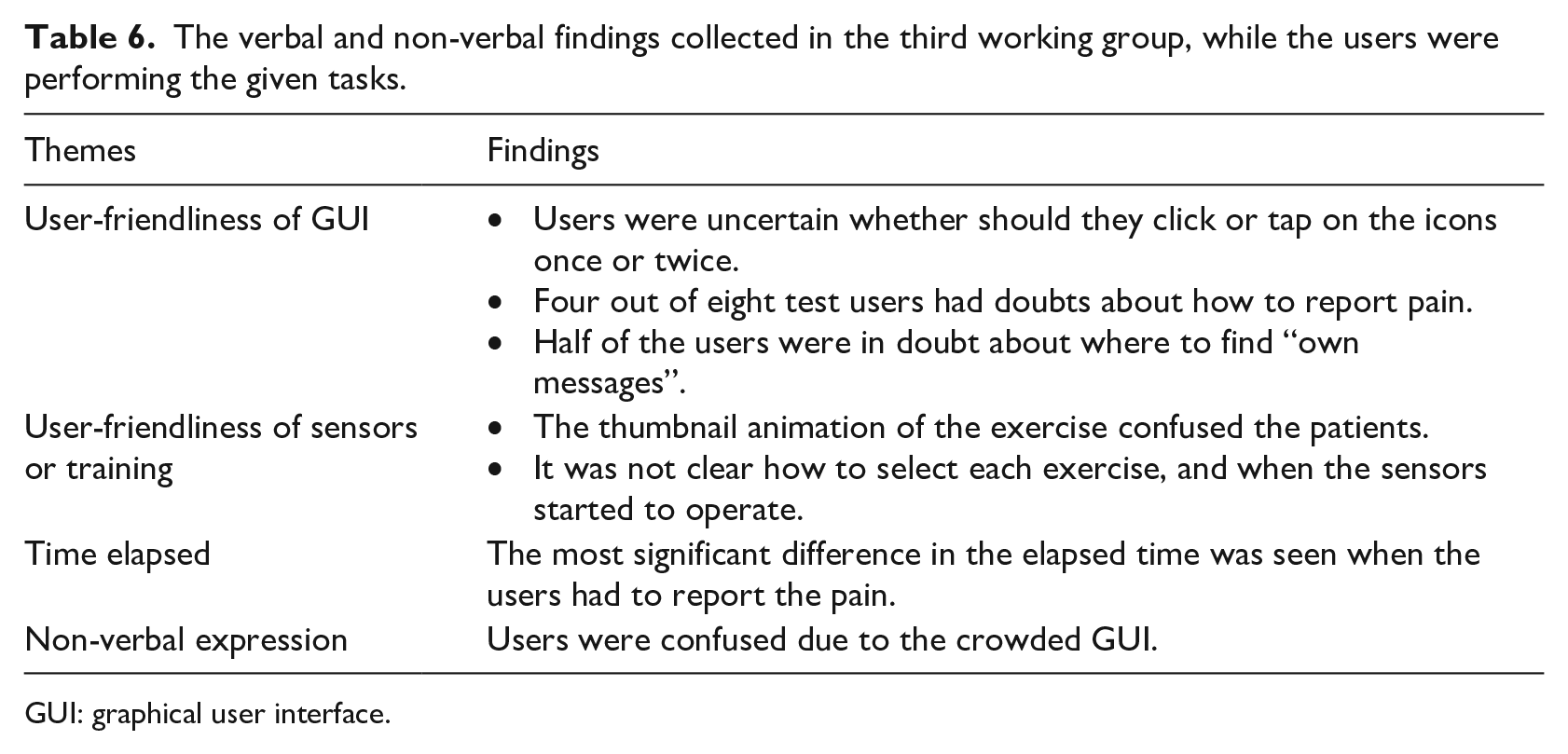
GUI: graphical user interface.
Iteration 4: home test
The qualitative findings of the interview were grouped into four themes. These are shown in Table 7.
Themes and findings in the first home test.
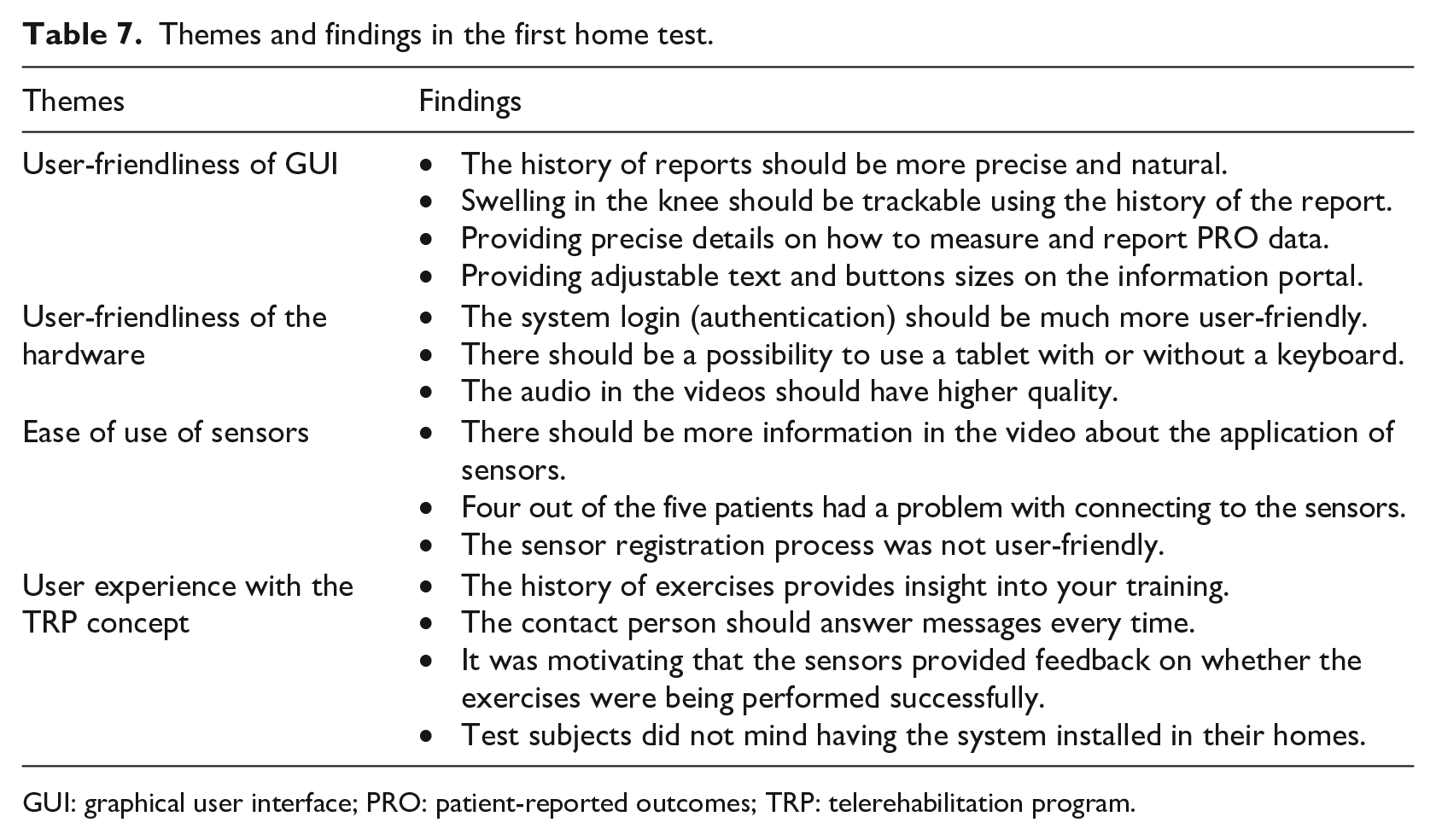
GUI: graphical user interface; PRO: patient-reported outcomes; TRP: telerehabilitation program.
The finding on the user-friendliness of the TRP was divided into five categories: hardware, reporting system (PRO data), communication, information, and training using the wearable sensors. Figure 7 shows the reported users’ experiences with TRP. Figure 7 indicates that the overall user-friendliness of the TRP was high to very high. It should be mentioned that the patients reported a lower level of satisfaction in the area of communication and training with the wearable sensors.
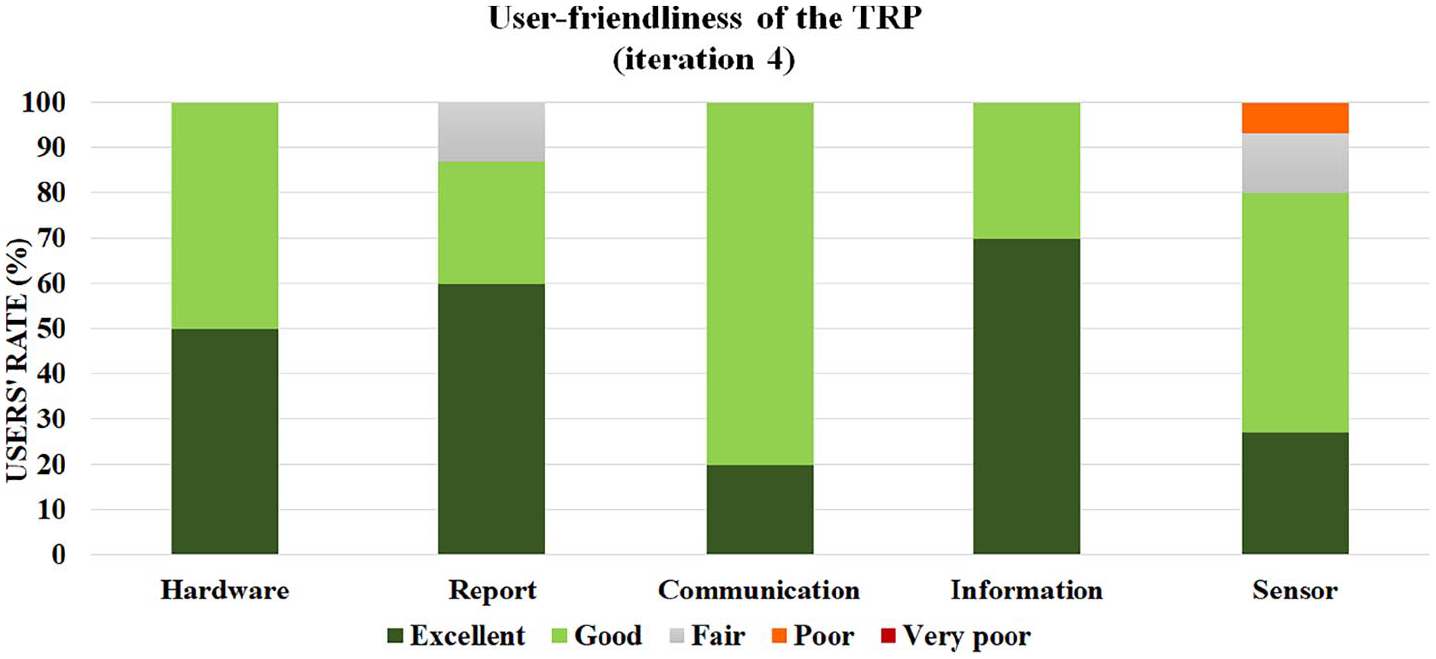
Reported user-friendliness of the developed TRP tested in the fourth iteration using a 5-point Likert-type scale questionnaire.
Iteration 5: telerehabilitation application test for 2 weeks
The themes and finding on the 2-week TRP test are presented in Table 8.
Themes and findings on the 2-week system test (iteration 5).
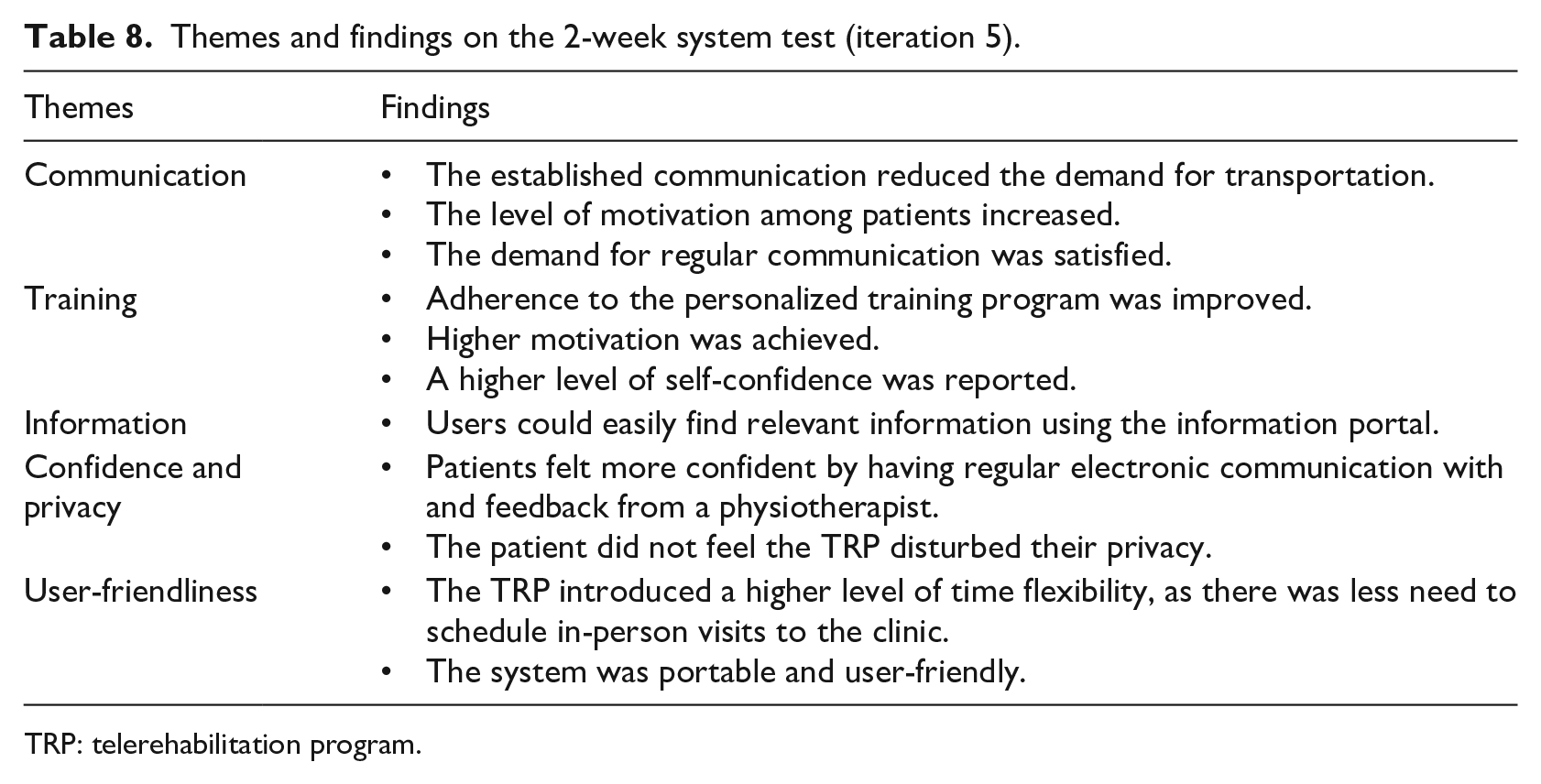
TRP: telerehabilitation program.
The achieved results from the semi-structured interview revealed five distinct groups, reflecting the participants’ experiences while using the TRP and the encountered facilitators and barriers during 2 weeks.
Virtual training
The users stated that the program facilitated training at home and helped them to have higher adherence to the rehabilitation program. Two of the patients remarked that the virtual training assisted and motivated them in carrying out their training exercises:
It has advantages that the program is highly structured, and I do the exercises in a structured order. (ID 206)
The patients also remarked that the TRP motivated them to perform the exercises without any ambiguity:
Because I have said “Yes” to participate in the project, I don’t want to fail to exercise. (ID 205)
One of the patients remarked that group training might motivate her more than exercising at home. She stated,
It is a lonelier form of training than team training, where one can encourage each other, and the individual training requires a lot of discipline. (ID 206)
Communication
All the participants agreed the asynchronous communication platform that was provided was a significant help in facilitating communication with the healthcare professional, and they received the proper support. The patient mentioned that they could resolve many of the challenges and problems using the system. For example,
and if I had problems, you [referring to healthcare professional] were there right away. (ID 205)
Moreover, one of the participants thought that consulting with a healthcare professional motivated him to remain involved in the program. He stated,
I have used the sending messages [using TRP], and it is user-friendly for someone who is not used to computers. (ID 209)
One of the participants also shared his thoughts and experiences using phone calls as the potential alternative to digital communication:
I don’t think there is much support you get from the hospital from that angle. (ID 209)
The majority of the users claim that the system can considerably reduce the need for travel. One of the patients stated that the multimedia services and instructions for the exercises satisfied the requirement for attending the physiotherapy center. One participant mentioned,
It’s great that you can do it at home and be guided in it, so you don’t have to travel back and forth to the physiotherapist. (ID 209)
Information
Almost half of the patients remarked that they were interested in reading the information provided. However, they remarked that the information was provided in the user-friendly platform, and they were able to navigate through various types of information. One of the participants stated,
It’s easy to navigate in, and I’ve read it all several times. (ID 207)
The sense of feeling secure and privacy
The participants believed that physiotherapist’s feedback on the patients’ performance and questions induced a sense of security. A typical remark was
At one point, you [the physiotherapist] wrote to me and gave me feedback on the exercises, and that means something to me that there is some response that it’s being done the right way. (ID 206)
The majority of the participants remarked that the system did not invade their privacy, and they felt comfortable using the program:
I do not feel unpleasant that someone is keeping an eye on me. (ID 206) I did not feel monitored. It’s when the exercises are not made to feel monitored. (ID 209)]
When one of the patients realized that the TRP uses the tablet webcam—the TRP has a tablet webcam, even though it was not used. She added that
I have thought about whether someone could see me if I did not have clothes on while in front of the tablet. (ID 205)
Mobility, flexibility, and user-friendliness of the system
Most of the patients remarked that the TRP introduced a high level of portability and that they could, therefore, use the system outside their home. One of the interviews was conducted at the patient’s summer cottage while the patient was using the program there. Moreover, one of the patients stated that
I have had the system in the summer cottage seven days after surgery. (ID 209)
One of the other patients also remarked that they might have a higher level of flexibility compared to face-to-face rehabilitation:
The advantage is that you can train at home and whenever you want. (ID 207)
Figure 8 shows the experiences of the recruited patients in the second phase of the study after patients had used the final TRP for 2 weeks.
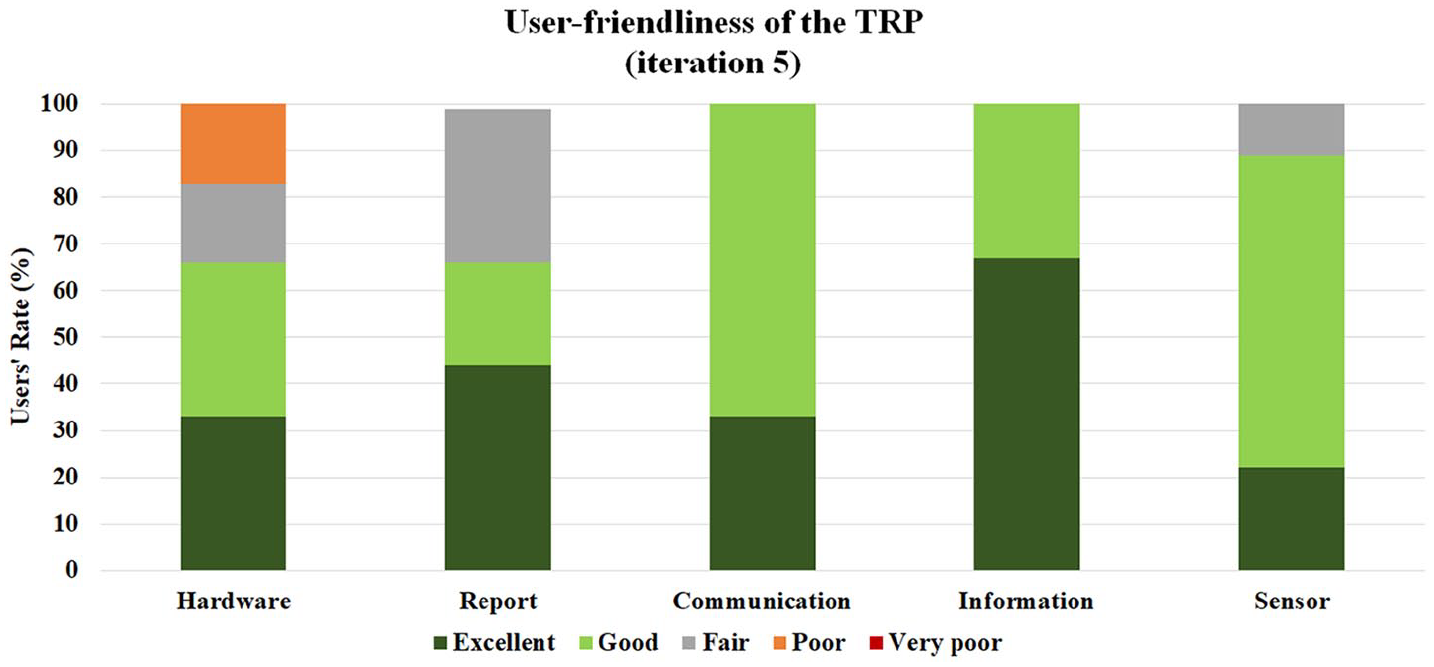
Reported user-friendliness of the final TRP in the last iteration using a 5-point Likert-type scale questionnaire.
Discussion
The aim of this study was to develop an individualized TRP. The program consisted of a fieldwork data collection, two PD workshops, and two system tests and users’ feedback. This achievement of study can be used as a guide for developing a sensor-based TRP that satisfies the patients’ requirements. Therefore, future studies might use these program design specifications to improve the current TRPs for the target.
Therefore, the main stakeholders (patients and healthcare professionals) were invited to participate in the system design and test. Eight participants who previously had regular rehabilitation program and four healthcare professionals were recruited in the development and design process. Three of the former patients were lost in the follow-up, and only five of them attended all the development iterations. Nielsen and Landauer 49 suggested that a sample of five users can uncover 75–80 percent of the usability issues in the design of user-centered systems. Hence, five patients are considered to be adequate to uncover issues for further investigation.
It was found that those patients who received the self-training program after a TKR still faced several challenges in carrying out their training program. Lack of regular healthcare supervision, communication, as well as lack of explicit knowledge of the patient’s adherence to the rehabilitation program were reported as main barriers of the program. Allin et al. 50 also reported that users might need different kinds of information, while some of them may use the Internet to find particular information. Wiklund Axelsson et al. 51 also indicated that the study group reported a feeling of being abandoned due to the lack of continuous communication.
The workshops (iterations 2 and 3) revealed that providing electronic communication between patients and healthcare professionals (i.e. physiotherapists and nurses) can resolve some of the current challenges. Furthermore, the patients expected to have access to relevant information via multimedia content. Healthcare professionals also requested regular patients’ reports on adherence to the exercise and relevant outcomes. As a result, they can provide appropriate feedback or intervention for each patient individually, thus enabling the professionals to prescribe a personalized rehabilitation program for each patient. Also, the users may track their progress in the program. The users emphasized that they are more motivated by establishing two-way communication and interactive report-feedback platform with healthcare professionals. This finding is in line with Petursdottir et al., 52 who reported that motivation might facilitate adherence to the exercise program among individuals with osteoarthritis. Jakobsen et al. 53 also indicated that increased communication among users led to higher user involvement. Danbjørg et al.54,55 emphasized the importance of asynchronous communication between users and healthcare personnel in order to avoid feeling being unsupervised.
The qualitative results from the preliminary system test (iterations 4 and 5) indicated that the patients’ requirements were fulfilled: patients reported that the system had a very high level of user-friendliness. However, the users in the fifth iteration did not participate in the development of the TRP. This might be considered as an advantage of the testing process compared to previous studies that involved the same participants in their study.54,56 The data collected in the last iteration (iteration 5) showed that the patients felt more confident, more secure, more supported, and had a higher level of motivation to follow the personalized rehabilitation program. Danbjørg et al. 55 also obtained a similar finding and indicated that it caused an increase in users’ sense of security. Luna et al. 57 stated that user satisfaction was higher in comparison with conventional methods, which also showed similar results in this study.
PD as a method is an iterative process with several benefits and challenges. The main benefit of this approach is identifying the real user needs as well as establishing a constructive dialogue among the stakeholders, which leads to finding a better match between the requirements and available technologies. In this study, a higher level of satisfaction was reported by the user in the real-world settings (fifth iteration); however, they did not participate in the design process.
Two challenges were observed in this study. First, PD is highly resource-demanding, and the data collection and processing were time-consuming and required the participation of stakeholders, which is in agreement with the findings of Clemensen et al. 33 Furthermore, actively engaging stakeholders in the iterative design process were challenging to achieve and require experienced facilitators. One of the participants left the project due to a lack of interest. That might occur as a result of the heterogeneity of participants’ backgrounds. Danbjørg et al.55,58 also reported difficulties with engaging participants.
This study had four limitations. First, there was a limited number of stakeholders participating in the study (eight patients and four healthcare professionals) and test (four patients) processes. Second, the TRP was tested for only a short period (2 weeks), and patients might have different experiences if followed over an extended period. In addition, the age group of the participants who involved in the development and testing (last iteration) were not in the same range, which might have an impact on the obtained results. Therefore, further studies should investigate the usability and feasibility of TRP with a higher number of patients, for a longer time in the patients’ homes. Finally, the patients with no conflicting health condition participated in the development process; therefore, the recommendations for the system cannot be generalized to the rest of the communities. Further studies are required to conduct with patients with conflicting conditions.
Conclusion
A TRP for patients undergoing TKR was developed using PD. This study developed a sensor-based TRP, and preliminary patient testing showed a high level of patient-reported user-friendliness and acceptability. Future developments, testing, and evaluation with patients and healthcare professionals are required so as to ensure the effectiveness and user-friendliness of the system.
Footnotes
Acknowledgements
The authors thank the Department of Occupational Therapy and Physiotherapy, Aalborg University Hospital and Orthopedic Surgery Research Unit, Research, and Innovation Center, Aalborg University Hospital, for participating in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted according to the Declaration of Helsinki, and all participants signed an informed consent form. This study was submitted to the local Ethics Committee for review, and as no intervention will be performed, it is not necessary to report this study to the Ethics Committee, according to national legislation in Denmark (S-20180012). Ethical approval for the second phase of this study was obtained from the local Ethics Committee (ID: N-20110171).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Aage and Johanne Louis-Hansen Foundation and Aalborg University.