
Abstract
Improving antimicrobial prescribing is a difficult process often requiring labour-intensive, multi-modal interventions. Many hospitals have introduced ePrescribing systems but the effect on antimicrobial prescribing, without treatment choice decision support systems, has not been well described. We sought to determine whether the introduction of ePrescribing improved prescribing quality. Patient records for inpatients on four rehabilitation wards, two using ePrescribing and two using the National Medication Chart, during February 2017, were retrospectively reviewed to identify all antimicrobial prescriptions, which were then reviewed for quality. Documentation of indication was significantly better on ePrescribing wards (45/46, 98%) compared to National Medication Chart wards (47/59, 80%). Adherence to guidelines (32/46, 70% vs 33/59, 56%), appropriateness of therapy (42/46, 91% vs 50/59, 85%) and documentation of duration, stop or review dates (35/46, 76% vs 38/59, 64%) did not significantly differ. ePrescribing can improve the quality of antimicrobial prescribing when Antimicrobial Stewardship principles are used in system customisation but cannot address all factors impacting on prescribing quality.
Keywords
Introduction
Antimicrobial resistance is a growing problem worldwide. Due to this increasing antimicrobial resistance, patients with infectious diseases are more likely to have slow responses to antimicrobial treatment, longer hospital stays and increased mortality.1,2 The prevalence of antimicrobial resistance is strongly correlated with the level of antimicrobial use. 3 The problem of increasing levels of resistant bacteria is compounded by a lack of new antimicrobials becoming available that have activity against these organisms. 4 Antimicrobials that can be used to treat more resistant strains are usually more expensive and may have a high risk of toxicity. 5 To ensure that we are able to continue treating infections before new antimicrobials become available, we must use antimicrobials optimally to safeguard our patients and slow the increasing rate of resistance; 6 this is known as Antimicrobial Stewardship (AMS).
AMS is a set of strategies used to improve the use of antimicrobials by encouraging the selection of an optimal drug regimen which includes appropriate choice of drug, dosage, frequency, duration and route of administration. 2 Strategies that have been shown to be improve antimicrobial prescribing include implementation of evidence-based guidelines, restricting supply of broad-spectrum antimicrobials and antimicrobials of last resort, requiring documentation of the indications for antimicrobial treatment, and stop and review dates, and implementing decision support delivered by electronic systems. 7
Adherence to empirical antimicrobial guidelines improves patient outcomes, including in-hospital and 30-day mortality and length of stay. 8 Documenting indication and stop and review dates allows clinicians, including AMS teams, to accurately review prescriptions and improve adherence to guidelines. 9
This study compared the quality of antimicrobial prescribing between wards using ePrescribing and paper-based charts to determine whether coincident AMS measures instituted can improve the quality of antimicrobial prescribing.
Aims
To determine whether there are differences in the quality of antimicrobial prescribing between using paper-based charts and ePrescribing on Older People’s Health (OPH) wards. Quality was determined by reviewing adherence to hospital antimicrobial guidelines, appropriateness of antimicrobials prescribed, documentation of indication and documentation of duration, stop date or review date.
Methods
Auckland City Hospital (ACH) provides secondary care for a population of approximately 500,000 people resident in Auckland and tertiary- or quaternary-level care for patients from other regions of New Zealand. Most wards use the paper-based National Medication Chart (NMC) for prescribing. 10 ePrescribing (MedChart; DXC Technology, Virginia, USA) was introduced to OPH wards in a stepwise fashion, initially in two wards during late 2016 and subsequently in two other wards in mid-2017.
Coincident with the implementation of ePrescribing, the ACH AMS team implemented initiatives intended to improve antimicrobial prescribing on these OPH wards. The initiatives included a mandatory requirement to document an indication when prescribing antimicrobials, a prompt that encouraged prescribers to document the expected duration of dispensing for every antimicrobial and an automatic alert to encourage a treatment review at 48 h after initiating intravenous antimicrobial therapy. Prescription of restricted antimicrobials was given a different prescribing pathway that required an approving clinician and follow-up validation of prescriptions. Local antimicrobial guidelines were imbedded into the prescribing system with diagnosis-based pre-populated order sets for common conditions, for example, cystitis and community-acquired pneumonia.
All patients present on the OPH wards from 1 to 28 February 2017 were included in the review. No other AMS services provided to the OPH wards differed during this time period. The data set included patient National Health Identifier (NHI), date of birth, ethnicity and admission and discharge dates. Inpatient records, including medication charts, were reviewed by T.R.B., a pharmacist, for antimicrobials prescribed and for drug allergies. Laboratory data were reviewed to aid in appropriateness review, looking for relevant microbiology laboratory results and measurements of renal and hepatic function. In total, 10 per cent of data were reviewed and validated by E.J.D., specialist infection pharmacist, for accuracy.
Data were then analysed, by T.R.B. and E.J.D., to determine whether the prescriber adhered to the local ACH guidelines. Each prescription was allocated to one of four categories: adherent, if the guidelines were adhered to; non-adherent, if the guidelines were not adhered to, directed therapy, if treatment was guided by available laboratory information and not applicable where guidelines or microbiology were not available at time of prescription.
The choice of drug was then reviewed using all the collected information to determine whether the chosen antimicrobial was optimal, adequate or sub-optimal according to modified National Antimicrobial Prescribing Survey (NAPS) criteria (Table 1). 11
Modified NAPS criteria.
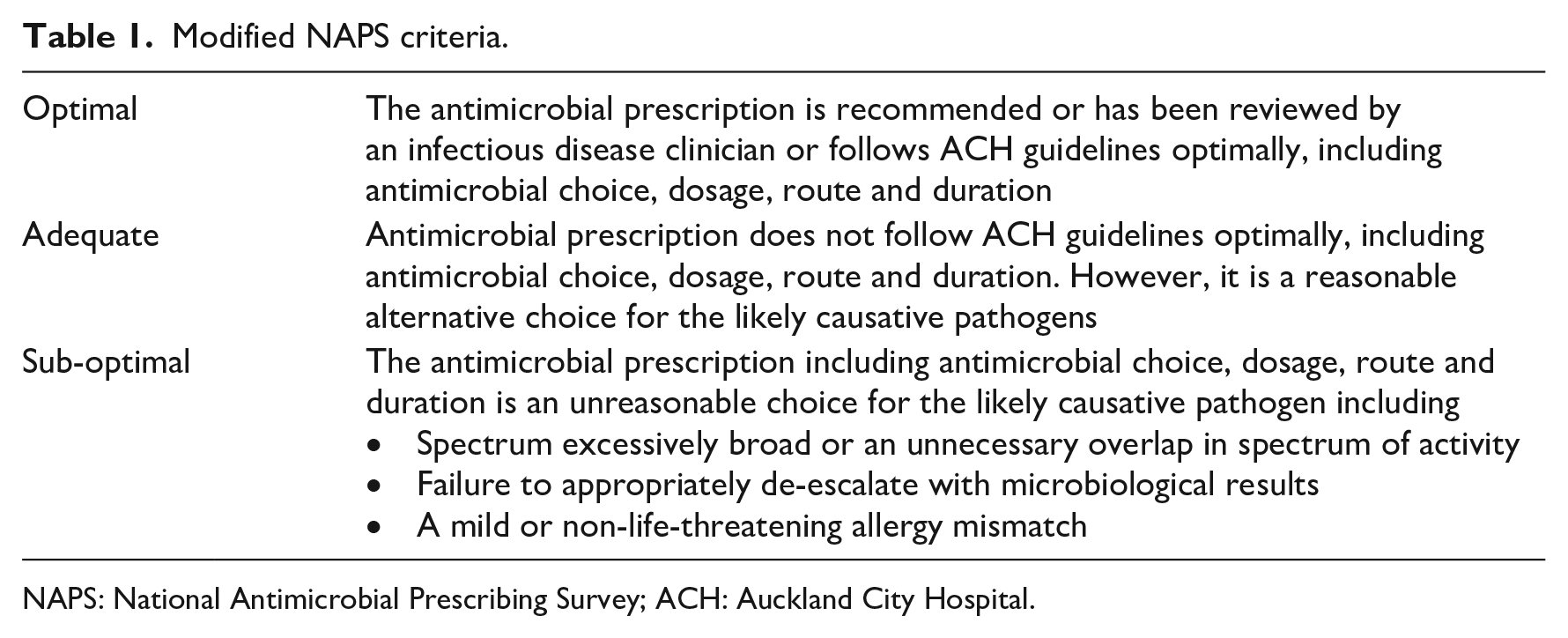
NAPS: National Antimicrobial Prescribing Survey; ACH: Auckland City Hospital.
Comparisons between results from the wards with ePrescribing and the NMC were made using chi-square tests, with p < 0.05 used to determine statistical significance.
The institutional review board at ACH stated that the study was exempt from ethics approval. Patients’ data were collected and stored in accordance with prevailing privacy regulations.
Results
A total of 139 patients, who had a total of 219 admissions to OPH during February 2017, were included: 105 antimicrobial courses were administered to 52 patients; 48% of admissions received antimicrobial therapy. No restricted antimicrobials were prescribed during this period. There was no difference in ethnicity, age and gender between ward types (Table 2.)
Demographics of patients on OPH wards.
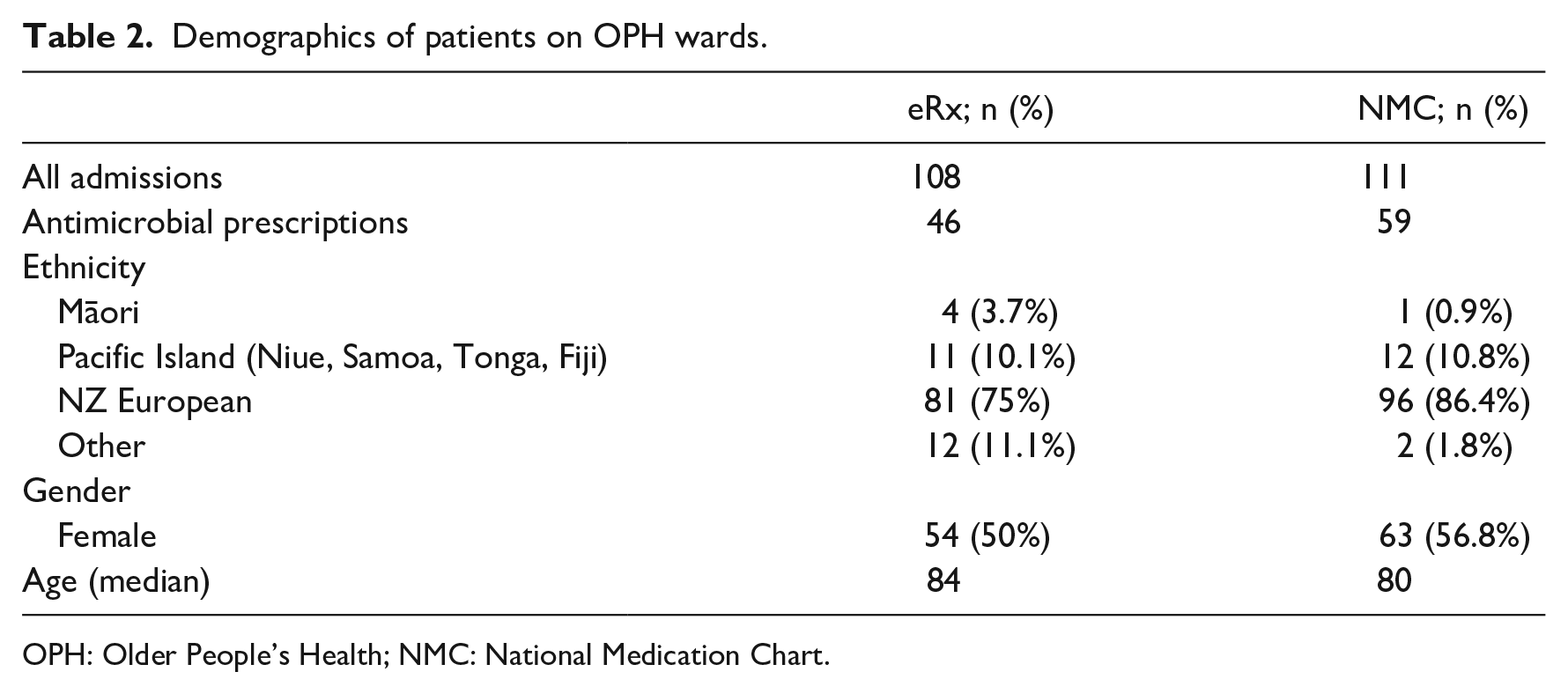
OPH: Older People’s Health; NMC: National Medication Chart.
Adherence
There was no difference in adherence to ACH antimicrobial guidelines between ePrescribing and NMC wards. Two prescriptions were unable to be compared to local guidelines as no guideline recommendation existed for the indication, cystitis prophylaxis (Table 3).
Difference in quality markers of antimicrobial prescriptions with or without ePrescribing.
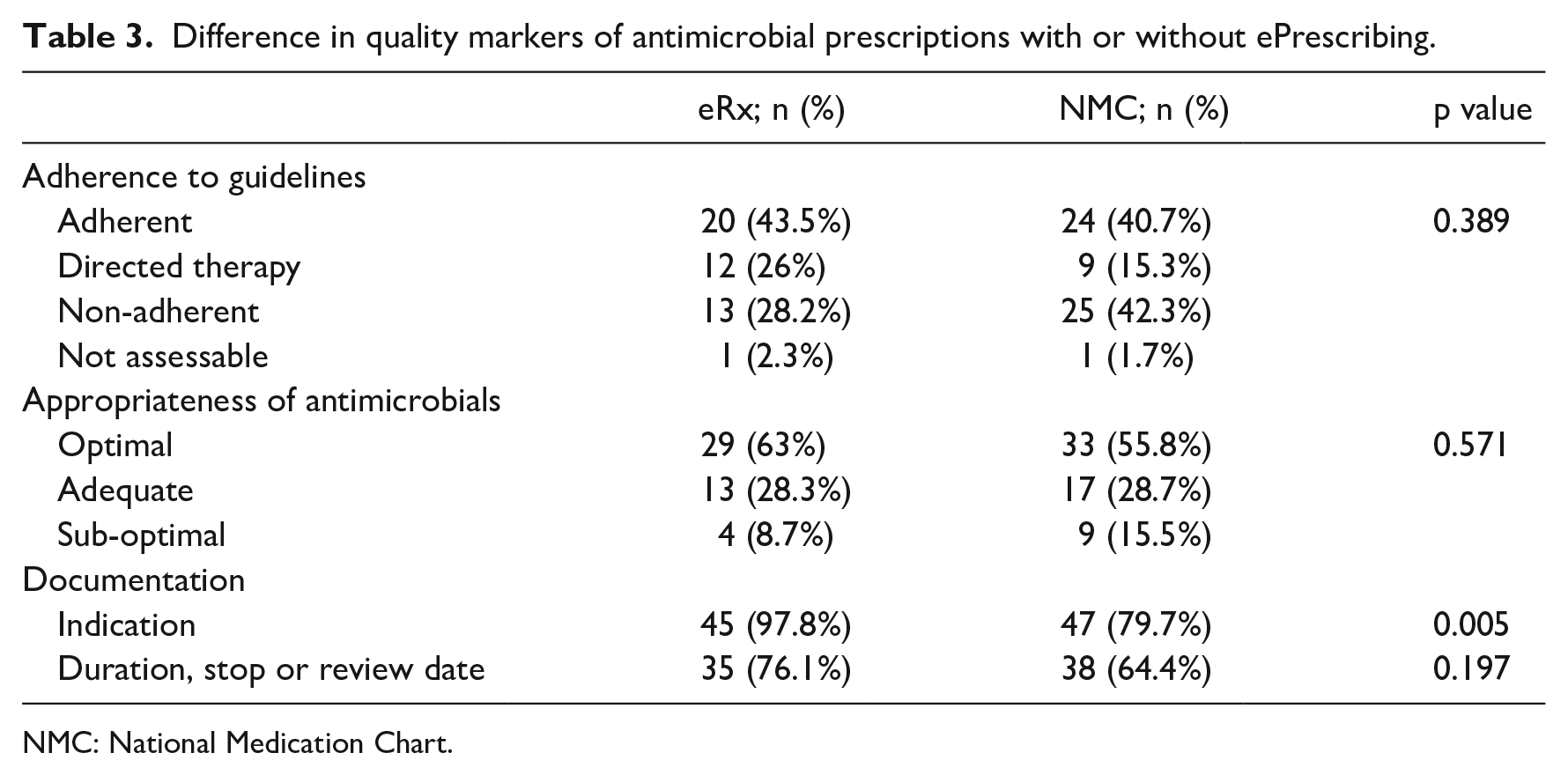
NMC: National Medication Chart.
Appropriateness
Differences in appropriateness were not statistically significant (Table 3). Reasons for determination of non-adherence and sub-optimal prescribing in this study included excessive durations (17/38), unnecessarily broad antimicrobials (12/38), overlap in spectra of antimicrobials (2/38) and antimicrobial treatment not matching susceptibilities (resistant isolates or non-targeted treatment) (3/38).
Documentation
Documentation of indication was significantly better on ePrescribing wards compared to NMC wards and reached statistical significance (Table 3). On ePrescribing wards, the indication was documented in MedChart for 87.2% of prescriptions, 10.6% solely in the clinical notes and 2.2% of prescriptions without a documented indication. On NMC wards, only 11.9% of prescriptions had an indication written on the NMC, with 67.8% of prescriptions having a documented indication in the clinical notes and 20.3% of prescriptions having no indication documented.
Documenting the duration of therapy, stop or review date was better on ePrescribing wards compared to NMC wards but did not achieve statistical significance. Prescribers recorded the duration, stop or review date on MedChart for 67.4% prescriptions, 8.7% solely in the clinical notes and 23.9% of prescriptions had no documentation of this kind at all. On NMC wards, 33.9% of prescriptions had a documented duration, stop or review date written on the NMC, with a further 28.8% written in the clinical notes; 37.3% of prescriptions had no documented duration, stop or review date.
Discussion
In this study, we found that the documentation of the indication for treatment was higher on OPH wards using ePrescribing when compared to OPH wards using paper-based NMCs, although rates of adherence to hospital guidelines and of appropriate antimicrobial selection did not show a statistically significant difference.
The main weakness of the study is that it is retrospective and based on clinical documentation. Assessment of adherence to guidelines relies on documentation of salient history in the clinical record which may not always be sufficient to describe the clinical decision-making process of the prescriber. There was also a relatively small sample size making statistical significance difficult to achieve; however, this was achieved for documentation of indication.
A strength of this study was inclusion of all OPH patients during the study period with documentation allowing for review of all prescriptions and only two treatments prescribed where no hospital guideline existed for comparison.
Adherence to guidelines and the appropriate use of antimicrobials are difficult to improve with single interventions.12–14 Our study did not show improvement in adherence with the use of ePrescribing. Electronic prescribing systems have previously been shown to improve guideline adherence and appropriateness of therapy; however, this has been demonstrated when the system has been used, or integrated, with empiric treatment decision support systems, which was not the case in our study or organisation. 15 Another reason reported for non-adherence to guidelines is inaccessibility, 16 and by embedding the guidelines with standard order sets, ePrescribing can overcome this barrier, although use of order sets requires users to use a different prescribing pathway which may be different than their standard practice. There are additionally a number of other reasons prescribers do not adhere to guidelines including perceived correctness of content, superior clinical judgement and prescribing etiquette within the team. 14 It is unlikely that any of these reasons would be overcome by integration of guidelines within a prescribing system.
Including documentation as a quality marker of antimicrobial prescribing has now been implemented in a number of settings;17–20 however, documentation relating to infection and use of antimicrobials is known to be poor, especially in areas without electronic health records. A previous study of antimicrobial prescribing in surgical patients at ACH demonstrated poor rates of documenting indications (86%), 21 and a European-wide point prevalence survey of 172 hospitals showed only 75% of prescriptions with a documented indication. 22 Documentation of indication forces prescribers to consider the reason for antimicrobial use, enhances continuity of care and enables prescribing review from clinical pharmacists and AMS teams. Inclusion of fixed indication terminology in ePrescribing systems may assist prescribers in selection and reduces variation in analysis, but free-text options are sometimes preferred by clinicians as clinical scenarios may not easily match pre-defined lists. 23 Documentation of duration, stop or review date was lower, regardless of prescribing methods, and in the ePrescribing cohort, although prompted at prescribing, and again at 48 h for those on intravenous therapy, 34% of prescriptions still were not adequately documented. Clinicians may not want to commit to duration or stop date at the time of prescribing, where ePrescribing will apply this automatically, if they are have concerns of antimicrobial therapy being stopped inappropriately early. This may be the case if the clinical scenario or diagnosis changes during the treatment, for example, from pneumonia to empyema. Clinicians, though, should have other means for monitoring and reviewing appropriateness of antimicrobial therapy on a regular basis. 2 There should be no reason for this review not to be documented, especially when prompted with an electronic system.
In this study, documentation of indication was significantly better on wards using ePrescribing, although documentation of duration or stop or review dates was not. Fields where the indication for antimicrobial therapy and the planned duration of antimicrobial therapy could be documented were included in the ePrescribing system. While documentation of the indication was mandatory to complete for antimicrobial prescriptions, documentation of the planned duration or stop date was prompted but not mandatory. Review of the prescription of all intravenous antimicrobials at 48 h was prompted by the ePrescribing system but was not mandatory. Better results were therefore seen with an indicator where entry was mandated rather than optional. This effect has also been seen in other ePrescribing systems where hard stops around restricted antimicrobials significantly improved use. 24
Alert fatigue is a recognised risk of ePrescribing systems and must be balanced against added functionality and prescriber requirements to optimise possible outcomes. 15 Alert fatigue may have contributed to the difference seen between indication and stop and review date documentation. We also found that 12% of prescriptions had the mandatory indication ‘over-ridden’ using blank spaces or non-specific terms such as ‘infection’. The majority of these were adequately documented in the clinical record leaving less than 3% without a documented indication. This may have been a system issue or that the treatment indication may not have been adequately communicated by the senior member of the team responsible for this decision to the more junior member of the team who actually performed the prescribing.
Many different interventions are used in AMS programmes to optimise antimicrobial prescribing and multiple interventions, such as audit and feedback or prescriber education, have often achieved higher rates of prescriber improvement.7,13 The introduction and use of ePrescribing in this study has demonstrated better results for a quality indicator of optimal antimicrobial prescribing compared to traditional paper-based prescribing in OPH and supports further introduction of ePrescribing throughout the organisation where further study should be undertaken to see whether similar results are seen in other hospital specialties.
Conclusion
Our study shows that a key AMS quality indicator was undertaken better with ePrescribing and a mandatory function compared to paper-based prescribing but other indicators were not when soft measures were used. AMS principles and measures should be used with system development for further benefit.
Footnotes
Acknowledgements
The authors thank Associate Professor Mark Thomas for his help in reviewing the manuscript.
Author contributions
All the authors have contributed significantly to the manuscript and have agreed to the contents of the manuscript in its submitted form.
Authors’ note
We confirm that this work is original and has not been published elsewhere nor is it currently under consideration for publication elsewhere. This submission complies with the manuscript checklist.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.