
Abstract
The purpose of this study was to investigate the nature and effects of exchanging emotional support via a smartphone-based support group for patients with alcohol dependence. Of the 349 patients who met the Diagnostic and Statistical Manual of Mental Disorders (4th ed.) criteria for alcohol dependence, 153 patients participated in the discussion group within the Addiction-Comprehensive Health Enhancement Support System, a smartphone application aimed at reducing relapse. This was developed to prevent problem drinking by offering individuals in recovery for alcohol dependence automated 24/7 recovery support services and frequent assessment of their symptom status as part of their addiction care. The results showed that receiving emotional support from health care providers improved coping self-efficacy. Giving emotional support and receiving emotional support from health care providers acted as a buffer, protecting patients from the harmful effects of emotional distress on risky drinking. Clinicians and researchers should use the features of smartphone-based support groups to reach out to alcoholic patients in need and encourage them to participate in the exchange of emotional support with others.
Keywords
Introduction
According to the 2015 National Survey on Drug Use and Health, 17 million Americans aged 18 years or older were classified as having alcohol use disorder (AUD). However, only 6.7 percent received treatment for alcohol use at any location, such as a hospital, rehabilitation facility, or mental health center. 1 The majority of alcoholics still engage in excessive or uncontrolled drinking after treatment. 2 Continuing care for AUD is scarce because it is financially overburdened, labor-intensive, and unstable. 3
As a potential solution to this problem, mobile communication and network technologies have received considerable scholarly attention. In particular, smartphone technology notably helps individuals with AUD access a variety of health care services in cost-effective, flexible, and efficient ways. 4 More importantly, mobile communication technologies have led to a proliferation of online support groups for people with alcohol dependence. In online alcoholism support groups, emotional support is frequently enacted through mutually supportive communication behaviors,5,6 and group members have been observed to be highly satisfied with the social support they exchange. 7
Despite the growing body of research on online social support in alcoholism treatment, little is known regarding the features and benefits of online social support through mobile interactions in the treatment of alcohol use disorders. Therefore, the primary goal of this study was to investigate the nature and effects of communicating emotional support via smartphone-based online support groups for patients with alcohol dependence.
Smartphone-based support groups and alcoholism treatment
For individuals with chronic diseases wanting to exchange social support, online support groups have been recognized as the most helpful and attractive source. Online support group members can gain access to support when they most need it as they are not constrained by either geography or time. 8 Reduced social cues may also help people feel comfortable in sharing potentially embarrassing information or discussing stigmatized topics. Moreover, interaction in online support groups is typically asynchronous, such that the group members can more effectively manage how and what they contribute to discussions compared to individuals in offline support groups.
Due to these advantages, alcohol-dependent individuals are more likely to engage in online support groups and benefit from group participation. Cunningham 9 found that the participants in online alcoholism support groups showed a significant reduction in alcohol consumption at a 6-month follow-up. These online support groups were particularly efficacious for social support among people with alcohol problems in rural and remote areas. More recently, social support is being exchanged through new modes of online communication, such as smartphones.9–11 Given the growing popularity and advantages of smartphones, it is plausible that smartphone-based support groups create a virtual environment open to sharing experiences and information and providing support to group members. Past research has shown that patients tend to regard smartphone-based support groups as peer social networks or as a means of receiving professional support. 12
Direct and stress-buffering effects of emotional support
Given that online communication is one primary way in which individuals can communicate social support in virtual communities, how to exchange social support online can be categorized into two message-relevant behaviors: message expression and reception. From a message expression-effects paradigm, the construction of social support messages produces several health benefits. Previous research has demonstrated the health-related benefits of the provision of emotional support in online support groups for people with chronic diseases.13–15 According to a message reception-effects paradigm, the reception of social support in online support groups result in a range of health benefits by addressing emotions such as fear, anger, and depression or fulfilling the need for advice or guidance concerning possible solutions to a problem.14,16 The effects of receiving support may vary depending on the type of support provider. In general, social support groups have two main sources of support: (1) peer patients and (2) health care providers. Individuals with similar health problems are well placed to empathize with one another and may thus be a valuable source of social support.17,18 Health care providers are willing to provide emotional support by speaking emphatically regarding patients’ fears and worries.19,20
In light of the several benefits associated with exchanging social support in online support groups, it is assumed that patients benefit from giving and/or receiving emotional support via smartphone-based alcoholism support groups. Emotional support has been empirically demonstrated to be effective in improving treatment for alcoholism. Macdonald 21 found that female alcoholics who had many close and emotionally supportive relationships tended to do better in terms of sobriety than those who were emotionally isolated. Dobkin et al. 22 also found that alcohol-dependent patients with high emotional support reported significant declines in the severity of alcohol abuse.
To examine the effects of giving and receiving emotional support in alcoholism treatment, this research employed two theoretical frameworks of social support: (1) the direct model and (2) the stress-buffering model. The direct model asserts that social support produces generalized positive outcomes for individuals regardless of the level of stressful life events. There is substantial evidence to prove a direct link between social support and alcoholism treatment outcomes.21,23–25 In a similar vein, the exchange of emotional support may encourage individuals with AUD to cope with their addiction problems. Specifically, giving and receiving emotionally supportive messages in a smartphone-based alcoholism support group is expected to have direct effects on coping self-efficacy and risky drinking days. To test the potential direct effects, we proposed the following hypotheses:
H1. Giving emotional support (H1a), receiving emotional support from peer patients (H1b), and receiving emotional support from health care providers (H1c) will be positively associated with coping self-efficacy.
H2. Giving emotional support (H2a), receiving emotional support from peer patients (H2b), and receiving emotional support from health care providers (H2c) will be negatively associated with risky drinking days.
According to the stress-buffering model of social support, 26 social support improves outcomes in a variety of settings by buffering the effect of stress.26–28 The stress-buffering role of social support has been documented in the context of alcohol involvement such that social support can alleviate the negative effect of stress on alcohol consumption.29–31 From this perspective, it is plausible to predict that giving and receiving emotional support buffer the impact of psychological distress on alcoholism treatment outcomes. Accordingly, we proposed the following hypotheses:
H3. Giving emotional support (H3a), receiving emotional support from peer patients (H3b), and receiving emotional support from health care providers (H3c) will moderate the negative relationship between emotional distress and coping self-efficacy such that this association will be weaker for those who give and receive more emotional support.
H4. Giving emotional support (H4a), receiving emotional support from peer patients (H4b), and receiving emotional support from health care providers (H4c) will moderate the positive relationship between emotional distress and risky drinking days such that this association will be weaker for those who give and receive more emotional support.
Although giving and receiving emotionally supportive messages in a smartphone-based alcoholism support group have the potential to improve AUD treatment outcomes, not all participants may benefit equally from exchanging emotional support. There is evidence that the effects of exchanging emotional support via online patient support groups may differ according to individual difference variables.13,15,32 We assumed that the current state of disorders moderates the effects of giving and receiving emotional support on coping self-efficacy and risky drinking days. Specifically, alcoholic patients with other drug disorders are more likely to experience higher psychological stress and need more emotional support. Thus, exchanging emotional support may be most beneficial for those with alcohol and any other drug disorder (AODD). Based on this reasoning, the following hypothesis was put forward:
H5. Giving and receiving emotional support will be more beneficial to individuals with AODD than those with AUD.
Methods
A-CHESS discussion group and study sample
The University of Wisconsin’s Center for Health Enhancement Systems Studies launched a smartphone-based, relapse-prevention program called Addiction-Comprehensive Health Enhancement Support System (A-CHESS). A-CHESS was designed to improve the management and continuing care in AUD by offering various services at almost any time and place. 4 The smartphone-based support group examined in this study was an online bulletin board-formatted discussion group in A-CHESS (see Figure 1).
A-CHESS discussion group.
This study used data that were originally collected as part of a randomized controlled trial of A-CHESS, including 349 patients who met the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria for alcohol dependence. Of the 349 patients, 170 patients could access the A-CHESS discussion group. The final sample for this study was limited to the 153 patients who either wrote or read at least one message in the A-CHESS discussion group during the 12-month study period. This criterion has been commonly used as a reasonable lower limit for participation in previous studies examining the health benefits of participation in online support groups.11,13–15 Table 1 summarizes the demographic and clinical characteristics of the group participants.
Descriptive characteristics of the study sample.
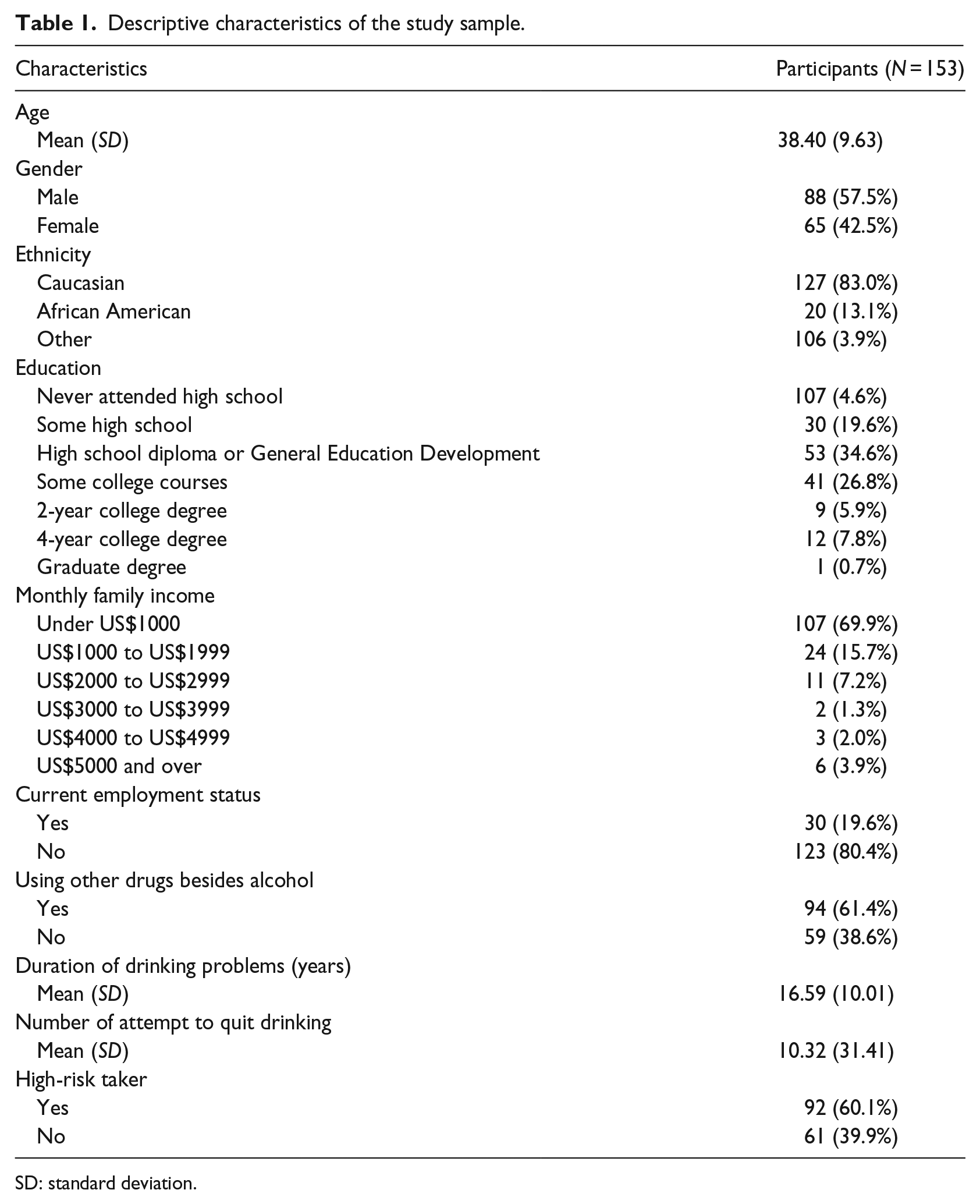
SD: standard deviation.
Data construction
The data used in this study resulted from a combination of three major data components: (1) messages posted in the A-CHESS discussion group, (2) action log data of the A-CHESS discussion group usage, and (3) pretest and posttest survey data. This data construction process has been commonly used to capture social support communication in online interactions and to gauge the effects on outcomes.11,13–15
To explore emotional support, this study analyzed the entire body of each participant’s discussion messages of the A-CHESS discussion group. Using Provalis Research’s QDA Miner 4.1 and WordStat 6.1, a total of 2746 messages posted by the participants of the A-CHESS discussion group were analyzed. Each discrete message post was the unit of analysis. In the computer-aided content analysis, we performed an extensive review of the relevant literature to establish the coding categories of emotional support, including sympathy, understanding/empathy, encouragement, caring/concern, and affirmation/validation in emotional support categories. After defining these coding categories, we created dictionaries of keywords associated with each category. Using the keyword dictionaries, coding rules were created by establishing a relationship between multiple terms, phrases, or concepts. The coding rules helped specify under what conditions a particular idea or category of ideas should be coded. An idea category consisted of a single term or several words. We integrated the results of the content analysis of emotional support in the A-CHESS discussion group messages with the action log data gathered in the A-CHESS database management system. The action log data collection system enabled us to track a variety of individual participant’s usage statistics. With regard to A-CHESS discussion group usage, these data provided information on which participant wrote and/or read each message. The action-level, content-coded data were finally combined with the pretest and posttest survey data to examine the research questions.
Measures
To measure the expression and reception of emotional support as independent variables, this study used a proportion measure consistent with previous research.13–15 Giving emotional support was measured by the total count of giving emotional support divided by the total number of messages written (M = 0.64, SD = 0.73). Receiving emotional support from peer patients was measured by the total count of receiving emotional support provided by peer patients divided by the total number of messages read (M = 0.79, SD = 0.45). Receiving emotional support from health care providers was measured by the total count of receiving emotional support provided by health care providers divided by the number of messages read (M = 0.12, SD = 0.20).
Coping self-efficacy in resisting alcohol use was assessed using the eight-item Drug-Taking Confidence Questionnaire. 33 Participants were asked to rate how confident they were in resisting the urge to consume alcohol in specific situations on a five-point scale ranging from 1 (not at all confident) to 5 (very confident) (M = 4.20, SD = 0.77, α = 0.89).
Risky drinking days were defined as those on which a patient’s drinking in a 2-h period exceeded four standard drinks for men and three standard drinks for women using the National Institute on Alcohol Abuse and Alcoholism definition of a standard drink as one containing approximately 14 g of pure alcohol. 34 Patients reported the number of risky drinking days that they had in the previous 30 days (M = 1.00, SD = 4.02).
Emotional distress was measured by modifying the negative affect subscale of the International Positive and Negative Affect Schedule Short Form. 35 This scale consisted of 13 items that described negative feelings and emotions. Patients were asked to rate the extent to which they had experienced each particular feeling and emotion during the last month. Responses to each item were recorded on a five-point scale ranging from 1 (almost never) to 5 (almost always), and all scores were averaged to create an index for emotional distress (M = 2.35, SD = 0.90, α = 0.94).
Analytic framework
In this study, two ordinary least squares hierarchical regression analyses were performed to examine the direct and stress-buffering effects of giving and receiving emotional support on coping self-efficacy and risky drinking days. Of the 153 participants, 28 patients with missing data were excluded using listwise deletion, resulting in a sample of 125 patients with complete data for the regression analysis. In each regression model, demographic and clinical controls were entered in the first block. To examine the direct relationships between exchanging emotional support and risky drinking days, the second block consisted of giving emotional support, receiving emotional support from peer patients, and receiving emotional support from health care providers. For the analysis of stress-buffering effects, emotional distress was entered into the third block, and the hypothesized two-way interaction terms were later entered into the final block. Interaction terms were constructed by multiplying the standardized values of the main effect variables to reduce possible multicollinearity problems between the interaction terms and their components.
Results
H1 predicted that the provision and receipt of emotional support would be positively related to coping self-efficacy. As shown in Table 2, only receiving emotional support from health care providers had a positive impact on coping self-efficacy (β = 0.23, p < 0.05). H2 posited that the provision and receipt of emotional support would be negatively related to risky drinking days. However, none of the three behaviors were significantly associated with risky drinking days. Thus, H1 was partially supported, and H2 was not supported.
Hierarchical regression analyses predicting hypothesized outcome variables.
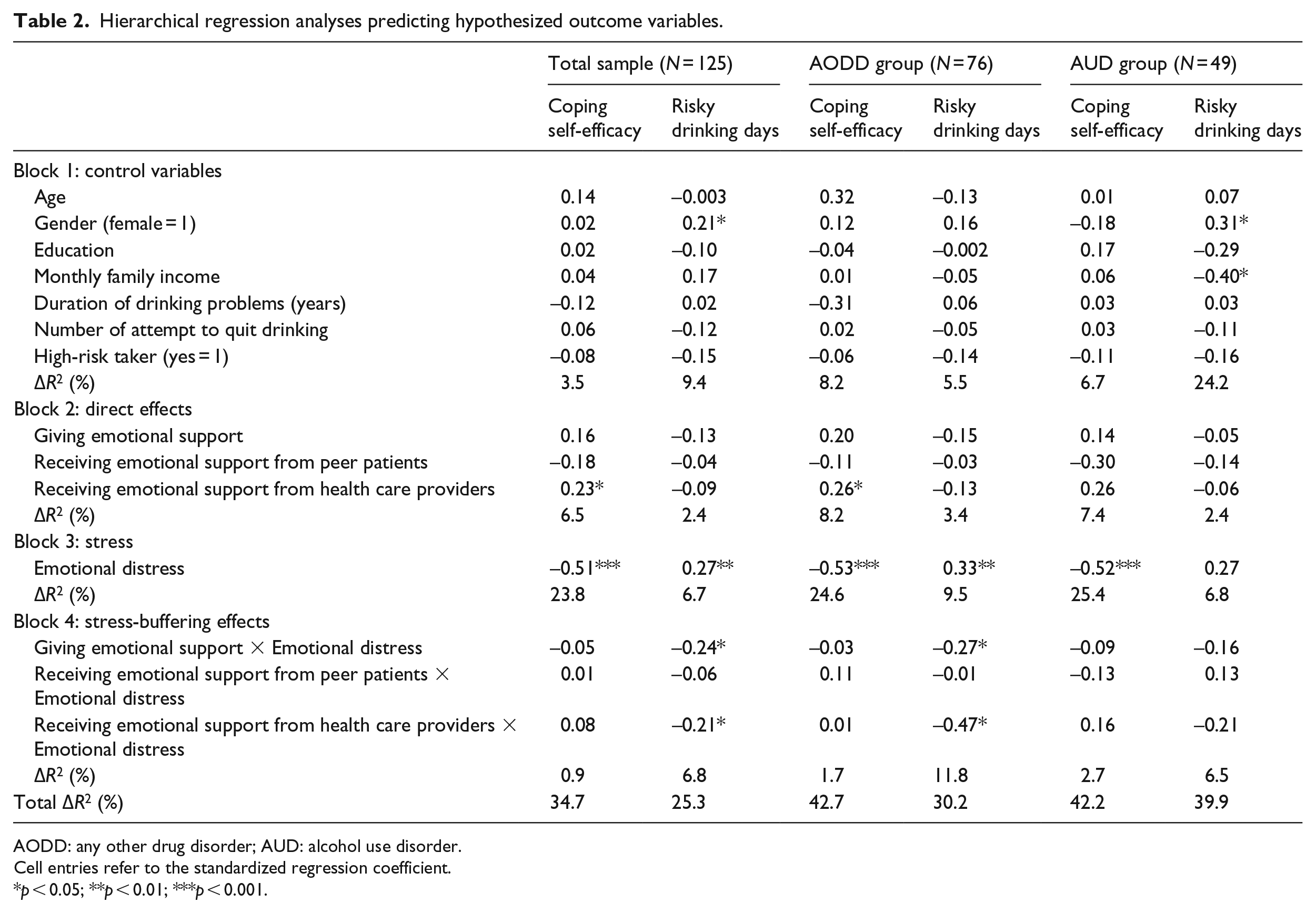
AODD: any other drug disorder; AUD: alcohol use disorder.
Cell entries refer to the standardized regression coefficient.
p < 0.05; **p < 0.01; ***p < 0.001.
H3 stated that the negative relationship between emotional distress and coping self-efficacy would be moderated by the provision and receipt of emotional support, such that the negative influence of emotional distress on coping self-efficacy would be weaker for those who exchanged more emotionally supportive messages in a smartphone-based support group. Contrary to our expectations, however, neither giving nor receiving emotional support moderated the negative effect of emotional distress on coping self-efficacy. H4 proposed that the positive relationship between emotional distress and risky drinking days would be moderated by the exchange of emotional support such that the positive influence of emotional distress on risky drinking days would be weaker for those who gave and received more emotional support. As presented in Table 2, two interactions were found to be significant (giving emotional support × emotional distress: β = −0.24, p < 0.05; receiving emotional support from health care providers × emotional distress: β = −0.21, p < 0.05). As shown in Figure 2, the positive effect of emotional distress on risky drinking days was weaker among those who provided high emotional support than those who gave low emotional support. Similarly, emotional distress led to fewer risky drinking days for those who received high emotional support from health care providers compared to those who received low emotional support from health care providers (see Figure 3). Thus, H3 was not supported, and H4 was partially supported.
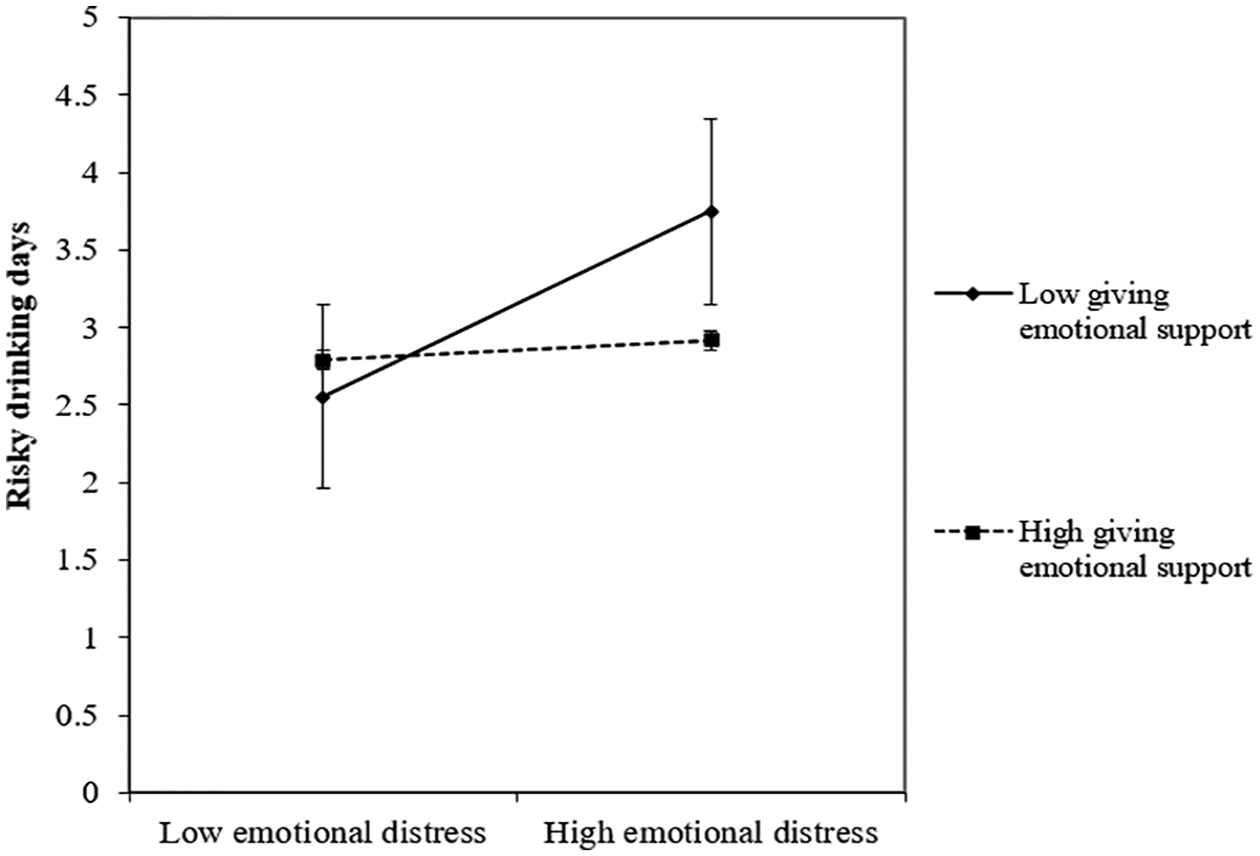
Interaction effect between emotional distress and giving emotional support on risky drinking days.
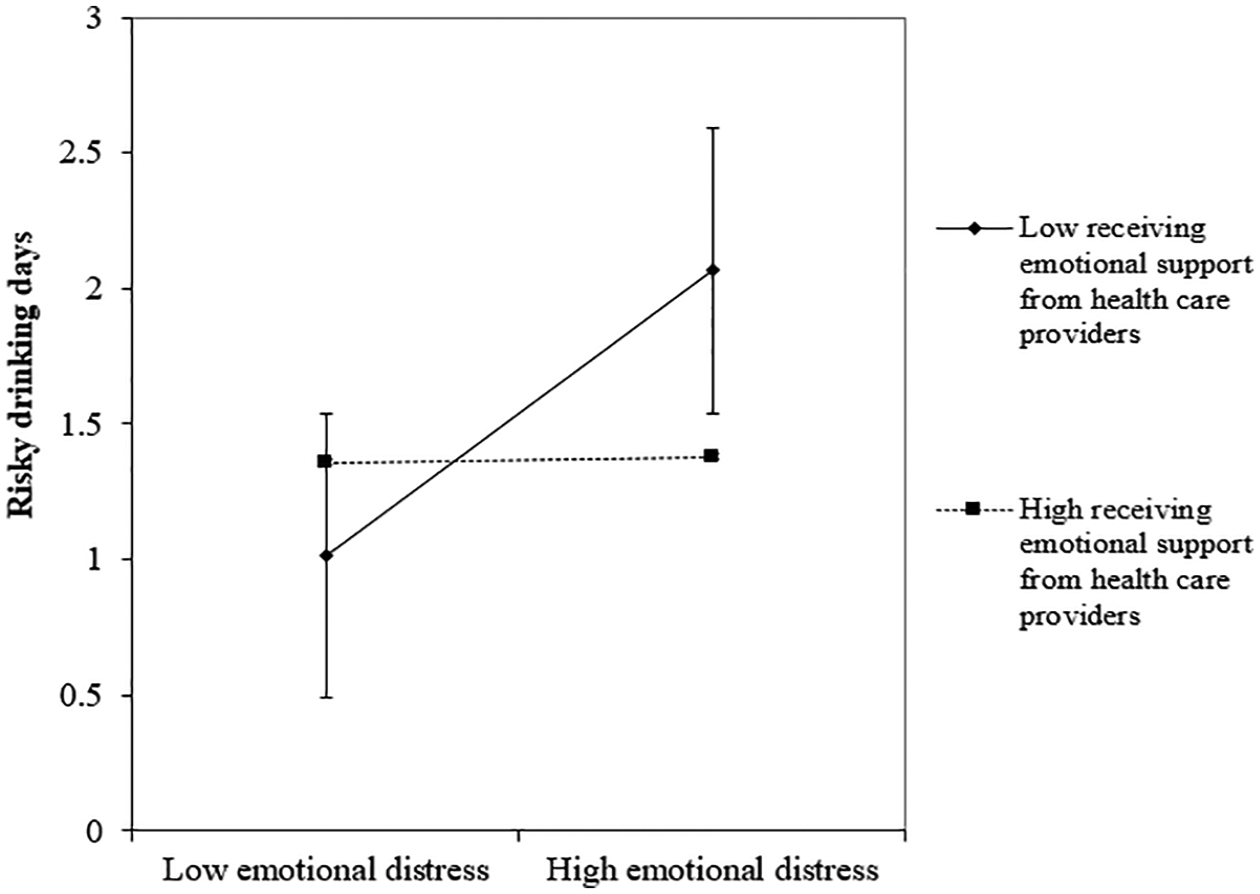
Interaction effect between emotional distress and receiving emotional support from health care providers on risky drinking days.
H5 proposed that people with AODD will benefit more from giving and receiving emotional support than those with AUD. As shown in Table 2, significant effects of giving and receiving emotional support from health care providers were found in the group of AODD, but not the group of AUD. Hence, H5 was partially supported.
Discussion
Smartphone technologies show promise as an efficacious and cost-effective tools for recovery management of chronic diseases. 36 Given that alcoholism is a chronic disease and acute treatment is only the beginning of care for alcoholism, it is very important to offer ongoing support for relapse prevention after patients with alcohol dependence complete residential treatment. 10 Despite the fact that alcoholic patients actively share social support in smartphone-based support groups,10,11 relatively little is known regarding the role and effectiveness of social support communication in such groups in the treatment of alcohol use disorders. Based on the direct and stress-buffering models of social support, 26 this study thus examined whether giving and receiving emotional support via a smartphone-based support group contributes to recovery from alcoholism.
Regarding the direct effects of giving and receiving emotional support, only receipt of emotional support from health care providers positively influenced coping self-efficacy. This finding aligns with previous findings that health care providers play a significant role in assisting patients with problem-solving coping/illness regulation by providing helpful emotional support.19,37 Although emotional support generally is considered a resource outside of typical clinical settings, health care provider–patient communication itself is a form of emotional support that can include encouragement, praise, reassurance, advice, and advocacy. 38 In particular, health care providers are most effective when they provide a combination of direct assistance, advice, or guidance and emotional support. 19 In the A-CHESS group, the health care providers would provide both emotional and informational support aiming to improve patients’ confidence in being able to cope with alcohol use disorders. However, contrary to expectations, receiving emotional support from peer patients did not exert significant effects on the AUD treatment outcomes. In the treatment of addiction, peer support cannot replace the need for social support from health care professionals because peers do not have the sufficient skills and knowledge required to manage psychiatric conditions or high-risk situations. 39 Furthermore, peer support work can be exhausting and emotionally challenging due to sharing and coping with the difficult experiences of peer group members. 40
The buffering effects of giving and receiving emotional support are also a meaningful finding of this study. Specifically, there was a strong positive relationship between emotional distress and risky drinking days for people who gave and received low emotional support, whereas there was a weak relationship between emotional distress and risky drinking days for those who exchanged high emotional support. These results empirically support the claim that social support communication protects (i.e. buffers) alcoholic patients from the deleterious effects of stress on alcohol consumption. 31 In other words, giving emotional support and receiving emotional support from health care providers act as a buffer, protecting patients from the harmful effects of emotional distress on risky drinking. The effect of giving emotional support merits further discussion. According to helper therapy principles, 41 people who give social support to others engage in self-reflection by evaluating their own problems objectively and learning effective coping skills, which ultimately leads to a reduction in levels of emotional distress. 42 Thus, the decreased emotional distress can lead to fewer unhealthy behaviors, including risky drinking.
Notably, the benefits of receiving emotional support from health care providers were obtained for only alcoholic patients with other drug use disorders. According to the optimal matching hypothesis, 43 the effects of social support are enhanced when its provision is matched with the need for support. The presence of multiple disorders would cause greater mental and emotional instability. In this situation, emotional support from health care providers could be profoundly effective to satisfy the high demands of emotional support for those with AODD.
This study has several limitations. First, we focused on only the online bulletin board-formatted discussion group that was accessible through patients’ smartphones. Future research should attempt to replicate the findings using different types of smartphone communication applications. Second, we did not examine the different types of social support such as emotional, informational, instrumental, and appraisal support. Given that different types of social support influence the nature and process of alcoholism treatment in different ways, future researchers should identify and compare the differential impact of types of social support exchanged in smartphone-based alcoholism support groups. Finally, this study was conducted with a US population and the findings may vary if conducted elsewhere, considering the different factors in other countries. Thus, we should be careful when attempting to generalize the results of this study to other countries or cultures.
The findings of this study suggest two practical implications. First, clinicians and researchers should use the features of smartphone-based support groups to reach out to alcoholic patients in need and encourage them to participate in the exchange of emotional support. Second, our findings are applicable to the design and implementation of smartphone-based support groups. Given that the provision and receipt of emotional support play distinct roles in the treatment of alcohol use disorders, group moderators should strategically promote the roles of support providers and recipients among the group participants. Finally, smartphone-based support groups can encounter disadvantages such as group participants’ privacy and security concerns, differences in people’s digital skills or literacy, and increased costs. Thus, it is necessary to address the challenges associated with improving the effectiveness of smartphone-based alcoholism support groups.
Footnotes
Declaration of conflicting interests
The authors(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant R01 AA017192 from the National Institute on Alcohol Abuse and Alcoholism.