
Abstract
Patient accessible electronic health records have been launched in many countries, and generally, health-care professionals have had strong initial concerns related to the areas patient contact, documentation practices and quality of care. Especially, oncology care was discussed in media when launching patient accessible electronic health records in Sweden. However, few studies have investigated clinician-perceived effects several years after the launch. A survey covering these areas, as well as supposed effects for patients, was distributed to oncology health-care professionals 6 years after the launch of patient accessible electronic health records and answered by N = 176. Results show that patient accessible electronic health records have had small effects within the covered areas, and that the area most affected was documentation practices. Very few significant differences could be found between physicians and nurses. A comparison with results from interviews and surveys conducted shortly after the launch of patient accessible electronic health records clearly indicates that the experienced negative effects are not as big as originally feared.
Introduction
Patient accessible electronic health records (PAEHR) have been launched across the world to increase transparency in health care and to empower patients by giving them access to medical documentation. Through these systems, patients can access their own health records to view, for example, visit notes, diagnoses and test results, by utilizing secure patient portals online. There are studies on PAEHR from the OpenNotes1–3 and Blue Button 4 in the United States, several Nordic countries, 5 Australia, 6 Canada 7 to name a few. Studies have shown that patients appreciate the service provided through PAEHR and in the United States 75 per cent reported better recall of care plans, better self care and a clearer understanding of their condition. 8 Some patient groups also make use of it to follow their care process and some patients prefer receiving information through PAEHR about test results before meeting their physician. 9 However, health-care professionals globally have had initial concerns about PAEHR and some studies show that it has been a very controversial change process, 10 and that health-care professionals express concerns related to increased workload, confused patients and changed documentation practices and so on.11–14
In Sweden, all patients can access PAEHR through a national eHealth portal which is the result of an initiative that started in Region Uppsala in the 1990s. 15 Generally, patients can access medical documentation either with a 2-week delay or directly, and also see referrals, medication list and test results depending on where they have received care. For further information about the launch of the system (called Journalen) and the difference in implementations between regions, see Moll et al. 16 and Hägglund and Scandurra. 17 Previous researches on the implementation of PAEHR in Sweden have investigated the patient perspective,9,16 as well as the implementation process used. 18 Some studies have examined the initial experiences for health-care professionals.19–24 These studies show that a large majority of the health-care professionals had concerns related to contacts with patients. Meetings were assumed to take a longer time due to the need to explain and elaborate with patients and there would be more questions from patients mailing or calling. Moreover, health-care professionals’ initial reaction was that documentation practices would change, and some considered to become more restrictive with what they write in the notes, especially related to some conditions such as cancer and mental health and related to areas such as addiction and obesity. Many assumed that it would also take longer to document in the electronic health-care system knowing that the notes would be read by patients. Many health-care professionals also indicated PAEHR would lead to decreased quality of care including issues with safety and privacy. Health-care professionals were also concerned about the experiences for patients, and that PAEHR might result in many patients being worried and anxious and not understanding the documentation, and that PAEHR would be used as a means to check the health-care professionals’ work.
The aforementioned concerns were initial reactions and it is possible that those opinions change over time, as was shown by results from studies on OpenNotes before and 1 year after the launch which indicates that physicians’ opinions about the PAEHR changes after it has been put in practice. 8 Before launch, physicians expressed concerns similar to the ones described above, but 1 year after the launch they were more positive and saw positive effects related to, for example, relation to patients. A change in attitude was also shown by Wass and Vimarlund 11 in the Swedish context, who also showed that health-care professionals’ perceptions can differ between different types of clinics. These studies did however not cover clinician-perceived long-term effects – a need highlighted in an earlier OpenNotes study. 2
Implementation research has shown that the use of a system changes with time, and initial reactions might be different from the more mature use. 25 There are however very few studies that have investigated the clinician-perceived effects several years after the launch related to the implementation of PAEHR in Europe and especially in the Swedish context. Have the above-mentioned concerns changed over time, and what is the health-care professionals’ experience of their patients reading their records when PAEHR has reached mature use and wider adoption? Some key questions that need answers are as follows:
Do health-care professionals experience that the contact with patients changes after the launch of PAEHR and take a longer time?
In what ways do documentation practices change when patients have the possibility to read the notes?
What are the experienced effects on quality of care?
Are possible changes and effects experienced differently by nurses and doctors?
What are the supposed effects for patients from the health-care professionals’ perspective?
In this article, we aim at answering these questions, and to investigate the experienced effects of PAEHR on the work of oncology health-care professionals, 6 years after launching the system, in the four areas: contacts with patients, documentation practices, quality of care, supposed experiences for patients (see also highlighted text above). The last theme is indirectly related to health-care professionals’ work, since supposed effects for patients might affect general attitudes and the means by which work is carried out.
Method
The study is based on a paper survey distributed to physicians and nurses at the department of blood and tumour diseases at Uppsala University Hospital during autumn 2017 and spring 2018 (i.e. about 6 years after the launch of the system). The survey was approved by the Regional Ethical Review Board in Uppsala, Sweden (EPN 2017/045). The survey method was chosen with the aim to elicit opinions and experiences of how PAEHR has affected work practices for oncology professionals at a major university hospital. The survey was distributed by the head of departments at the hospital to physicians and nurses at department meetings. The hospital organization was responsible for the distribution and collection of surveys in order to obtain as high a response rate as possible. Respondents were informed, on the questionnaire’s first page, about the voluntary participation and the aims of the study, that they remain anonymous through the analyses and that the results will be used in scientific publications.
The questionnaire contained 12 multiple-choice questions covering the following areas:
Demography (age and years of working in health care);
Perceived effects on contact with patients;
Perceived effects on documentation practices;
Perceived effects on quality of care;
Attitude towards Journalen;
Effects supposedly experienced by patients.
A few of the questions (4) had binary answers (yes/no) and the rest had either interval choices (the 2 demographic questions) or 4-point Likert-type scale choices (7 questions). The questions were inspired by an earlier study on OpenNotes 3 and identified issues from earlier studies within the consortium that has studied the introduction of PAEHR in Sweden.20–24
In addition to descriptive statistics to illustrate general trends in the data, the Mann–Whitney U test has been used for detecting group-wise differences between answers, on Likert-type scale questions, from physicians and nurses after the conversion (1 = disagree; 4 = agree). The chi-square test was used to detect statistically significant associations between variables for the questions with binary answers (yes/no). All tests were done in the SPSS 25 software.
Results
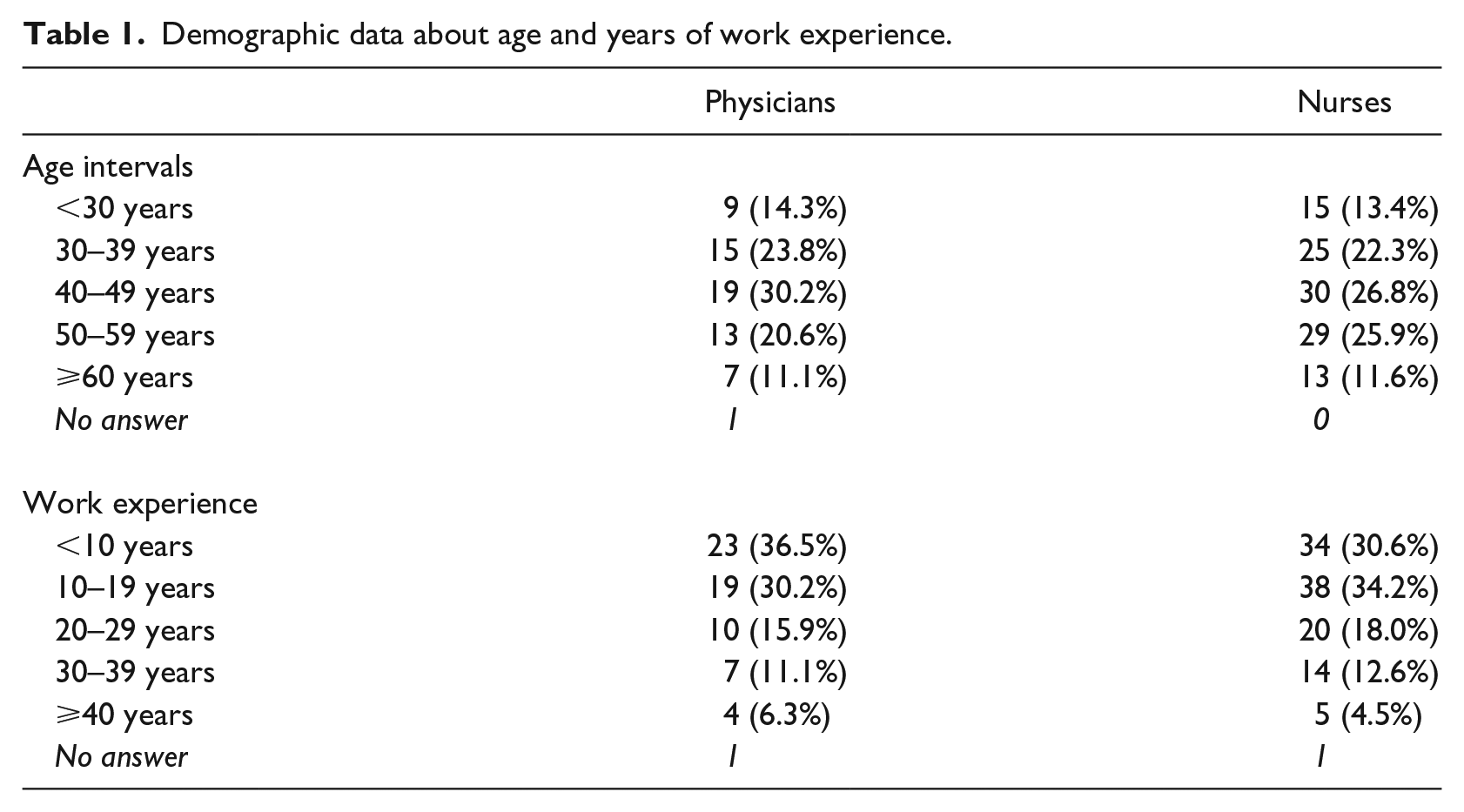
In total, 176/244 health-care professionals (64/75 (85.3%) physicians and 112/169 (66.3%) nurses) answered the survey, giving a total response rate of 72.1 per cent. The majority of the respondents in both groups were between 30 and 59 years old and had less than 20 years of work experience within health care. Detailed demographic results are given in Table 1.
Demographic data about age and years of work experience.
The results in Table 2 show that a large majority of the respondents agree or partly agree that it is generally a good idea to make medical records available through Journalen. This indicates a general positive attitude towards the system and possibilities it brings for patients. The Mann–Whitney test did not show a significant difference between the answers from physicians and nurses, but a tendency of more positive answers from nurses can be observed.
Results regarding the question on the general attitude towards making medical records available in Journalen.
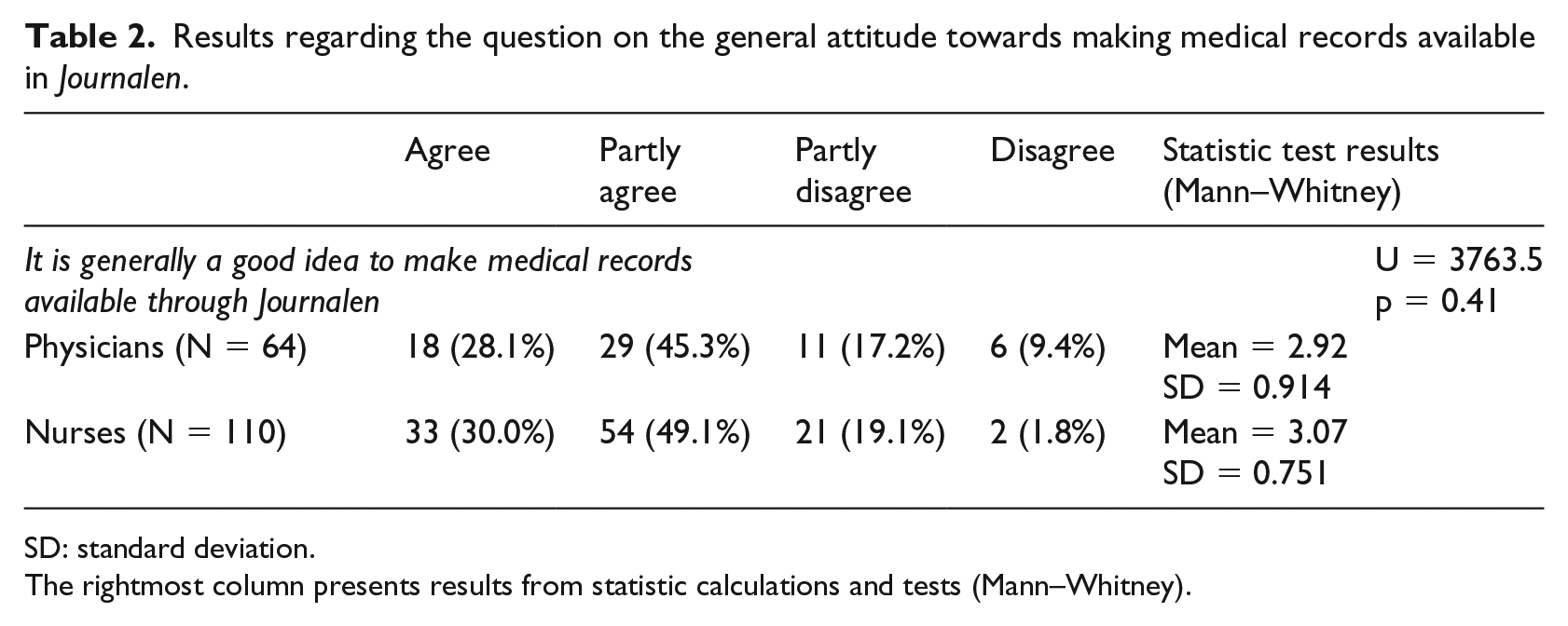
SD: standard deviation.
The rightmost column presents results from statistic calculations and tests (Mann–Whitney).
Contacts with patients
As presented in Table 3, both nurses and physicians experienced some effects on their contact with patients. In most cases, these effects appear to be perceived as moderate (between ‘partly agree’ and ‘partly disagree’). Tendencies that can be seen are that more nurses than physicians agreed that meetings often take a longer time, that physicians are more affected by increased time for phone and email conversations than nurses are, and that nurses experience concern from reading patients stronger than physicians do. According to the Mann–Whitney tests, none of these differences were, however, statistically significant.
Answers to the questions about the effect on contact with patients.
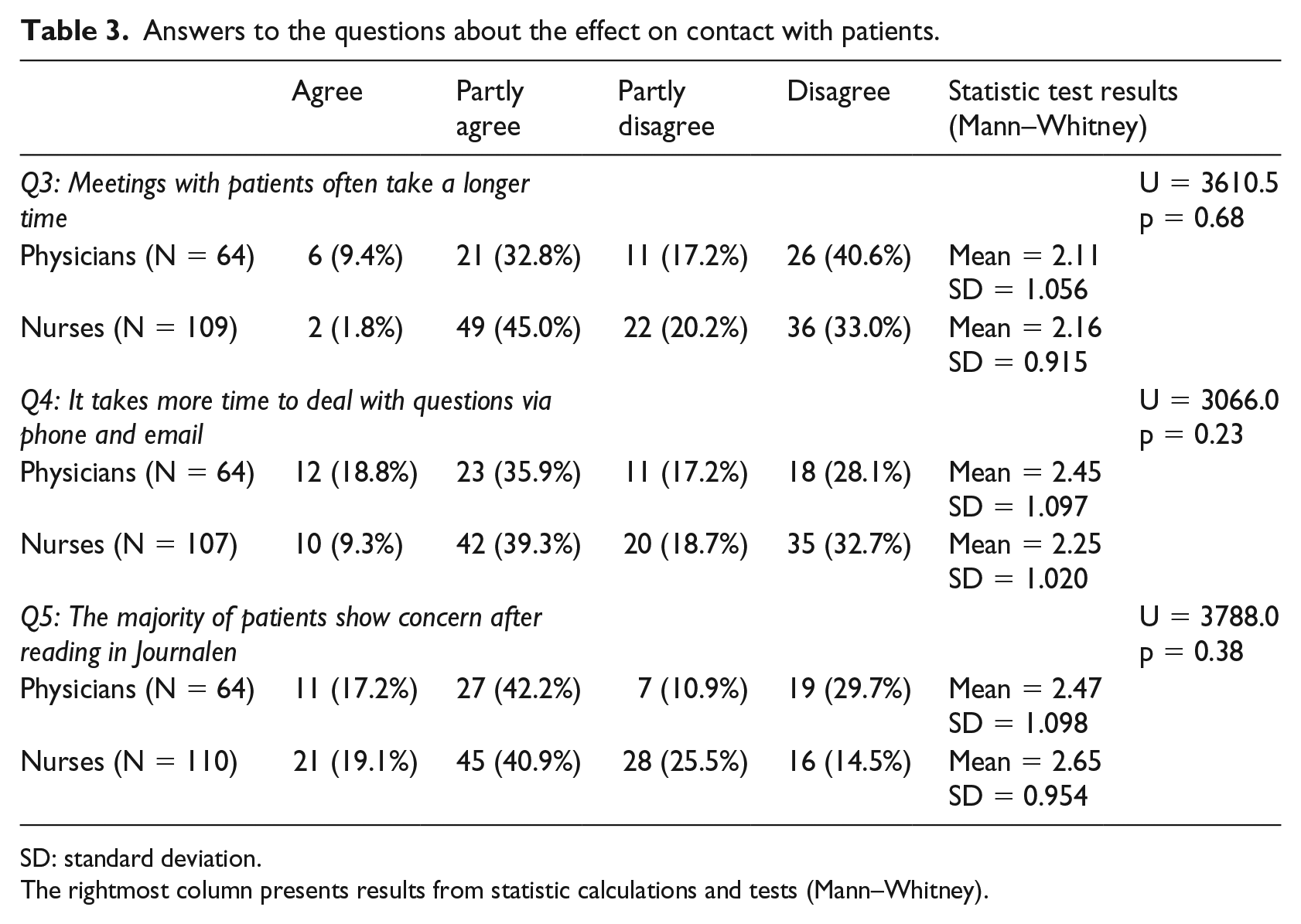
SD: standard deviation.
The rightmost column presents results from statistic calculations and tests (Mann–Whitney).
Documentation practices
Tables 4 and 5 summarize the results related to changes in documentation practices, caused by patients being able to read their medical records online. Table 4 shows that a majority of both physicians and nurses, at least to some extent, are more restrictive with what they share in their notes, and that some respondents (especially physicians) experience that it takes a longer time to write and edit notes. The Mann–Whitney tests did not show any significant differences in answers between physicians and nurses. Table 5 shows that some of the respondents have changed how they write about cancer – their main medical field – in their notes. Even larger proportions of physicians as well as nurses have changed the way they document other health-related problems like mental issues and obesity. Even though no statistical associations between answers from physicians and nurses were found (Table 5), there is a tendency that physicians are more prone to change how they document cancer as well as mental health, addiction and obesity.
Results from Likert-type scale questions related to changes in documentation practices.
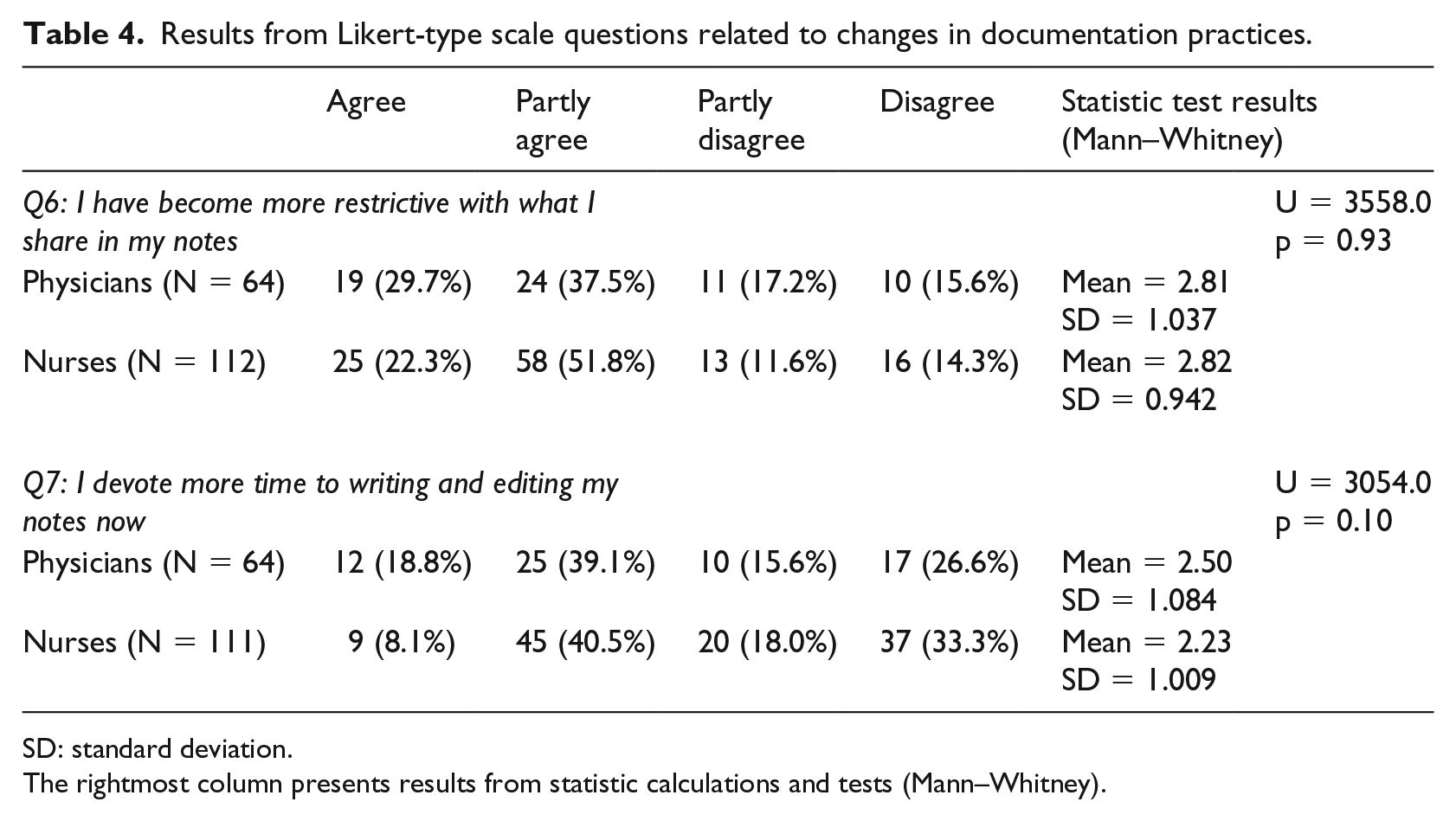
SD: standard deviation.
The rightmost column presents results from statistic calculations and tests (Mann–Whitney).
Results from questions with binary (yes/no) answers, related to changes in documentation practices.
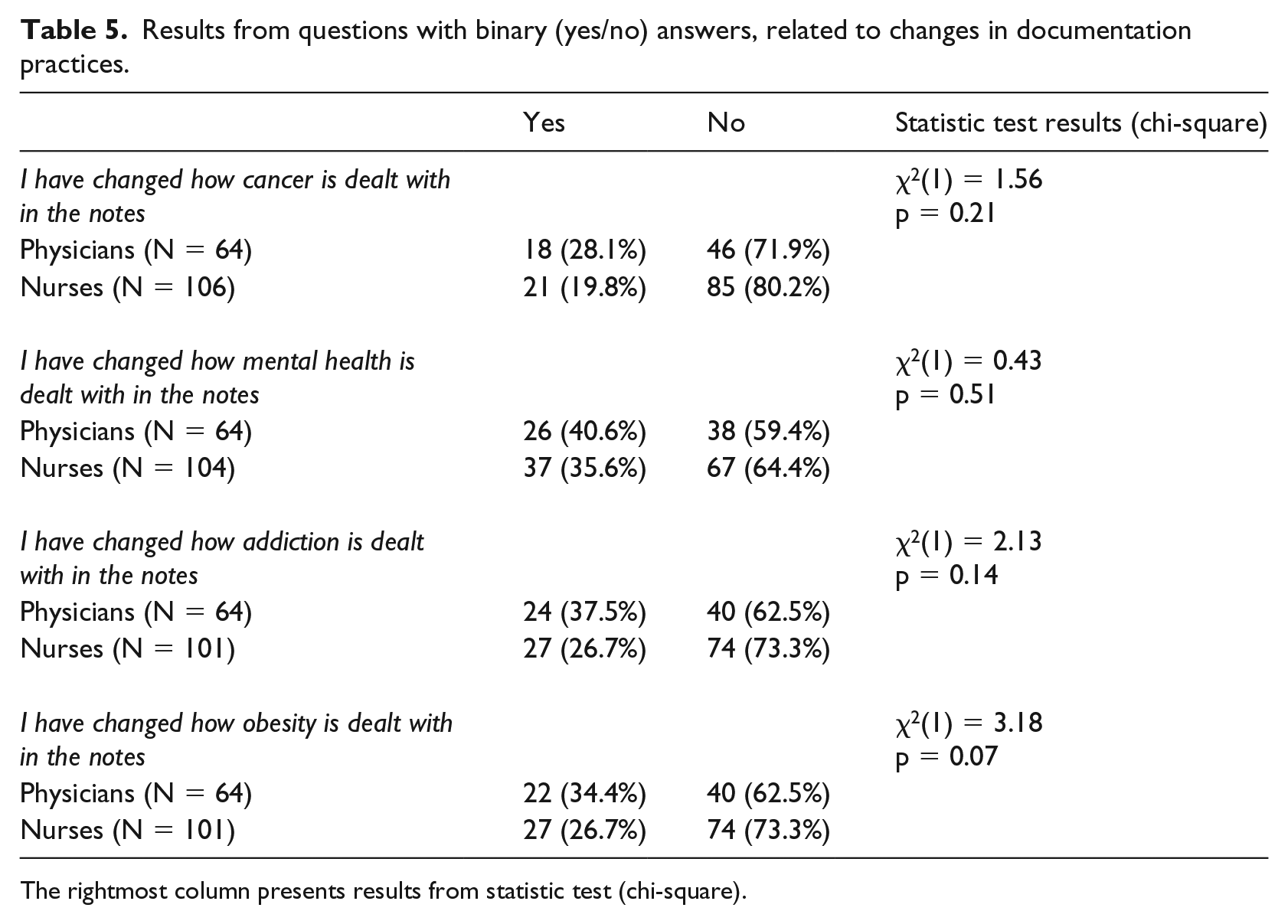
The rightmost column presents results from statistic test (chi-square).
Quality of care
The results from questions related to quality of care (Table 6) show that a clear majority of both nurses and physicians believe that there has been no change regarding effectivity or safety as an effect of patients reading their medical records online. The chi-square test shows a statistically significant association (p = 0.046) between answers from physicians and nurses regarding the effect on care safety. Compared to physicians, a significantly larger proportion of nurses believed that care has become safer.
Results from questions related to effects on the quality of care.
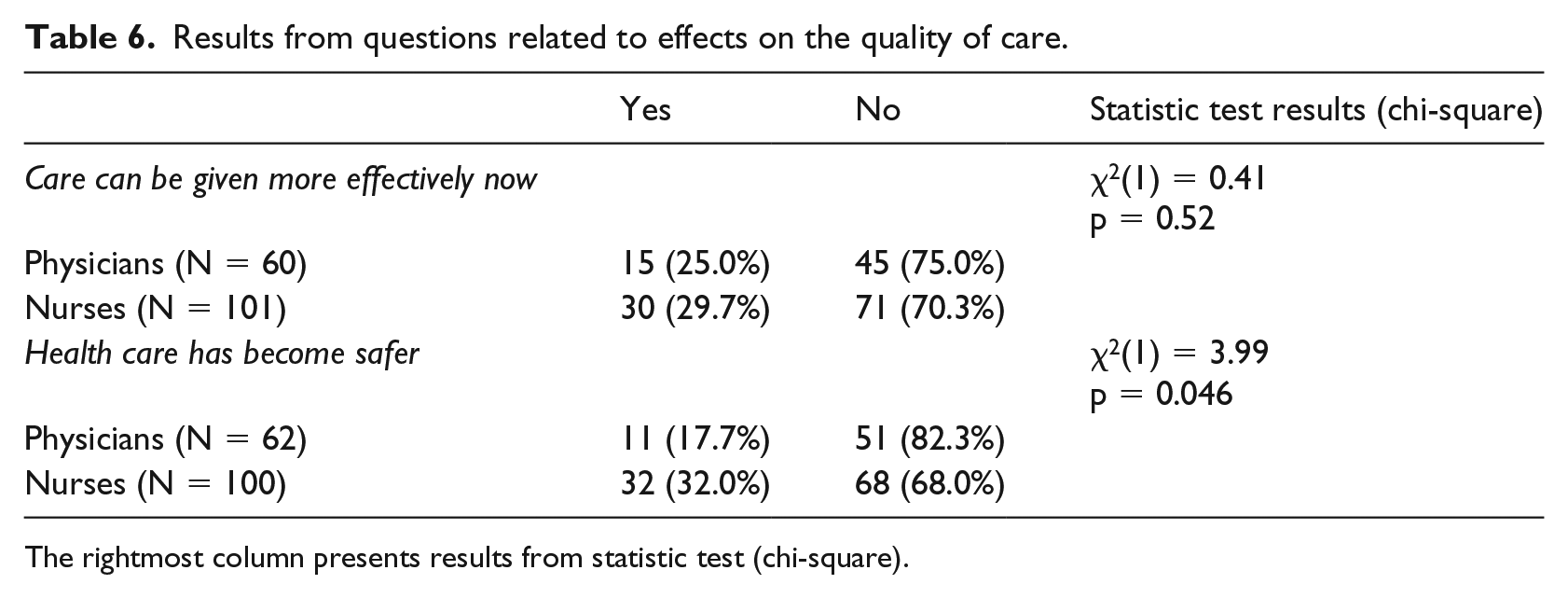
The rightmost column presents results from statistic test (chi-square).
Experiences for patients
In the final question, the respondents indicated, on a binary yes/no scale, which of seven presented effects they believed that the majority of their patients experienced as a result of reading their medical records in Journalen. The results regarding these effects are shown in Table 7. The effect that most respondents (physicians as well as nurses) believed to be true was that patients feel more in control of their own care. The only effect that a minority of both physicians and nurses believed to be true was that patients can take better care of themselves as a result of reading their PAEHR. It is also worth noting that the majority of both physicians and nurses believe that the notes are more confusing than helping and that patients feel more worried than before. The chi-square test showed a significant association between responses from physicians and nurses regarding the effect that patients can understand their health in a better way (p = 0.019) – a significantly larger proportion of nurses believed that this statement was true. No significant associations were found for the other effects. There is a trend, however, that nurses believe the effects to be experienced by patients to a larger extent than physicians.
Summary of results from the binary questions regarding effects that the HCPs believe their patients experience.
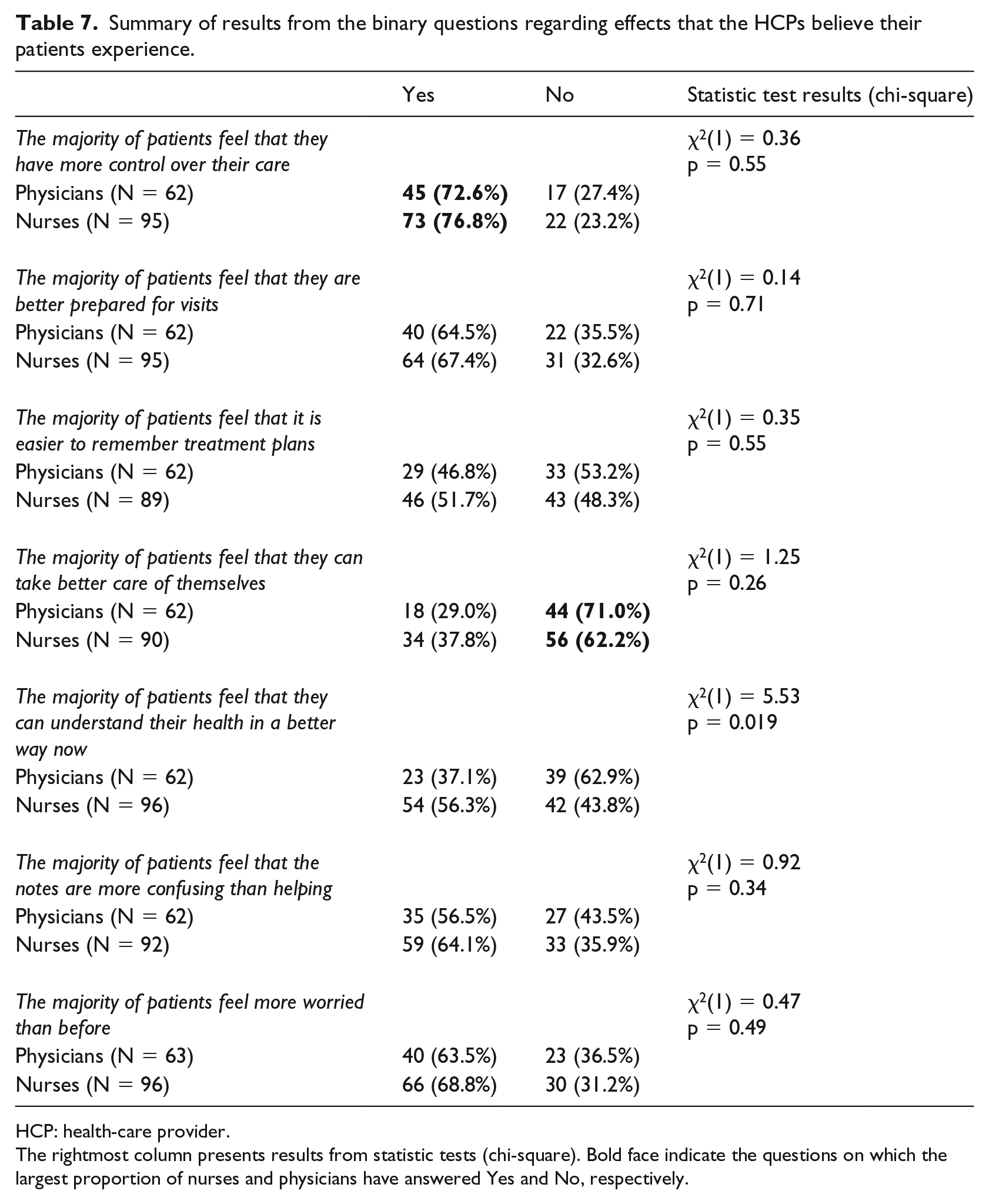
HCP: health-care provider.
The rightmost column presents results from statistic tests (chi-square). Bold face indicate the questions on which the largest proportion of nurses and physicians have answered Yes and No, respectively.
Discussion
The purpose of this study was to investigate the perceived effects of PAEHR on the work of oncology health-care professionals in Region Uppsala in Sweden, 6 years after the launch of the system. The specific focus on oncology enabled the investigation of PAEHR in an area of health care dealing with patients who often have very severe diseases and who have regular contact with health care during a long period of time. These patients may benefit from PAEHR in that they can, for example, follow their own care process and learn about their disease, but at the same time, there is always a possibility that they will be informed for example about a serious progression online before speaking to a physician. Aside from investigating the perceived effect of PAEHR on different areas of work, experiences and perceptions from physicians and nurses were compared to find possible differences between these two groups. The results mainly show moderate effects when it comes to the different areas surveyed, and in most cases, no statistically significant differences between physicians and nurses could be found.
When studies were carried out with physicians shortly after Journalen was launched in Region Uppsala, the responses were mostly negative. Apart from interviews where physicians expressed concerns related to altered patient contact and documentation practices as well as fear of decreased quality of care, 21 a survey showed that a vast majority of the physicians (about 82%) strongly disagreed or disagreed with that Journalen was a good reform. 23 Our present survey study with oncology care professionals shows that the physicians, as well as the nurses, are moderately positive towards Journalen – about 73 per cent of the physicians and 79 per cent of the nurses agreed or partly agreed with that it is generally a good idea to make medical records available through Journalen. Even though questions regarding attitudes towards Journalen were formulated differently in the earlier studies and the present study only focuses on physicians and nurses within oncology, our new results give a strong indication of a more positive attitude among oncology health-care professionals. Scandurra et al. 23 also found a difference in attitudes between physicians and nurses, showing that nurses were more positive towards Journalen. The same tendency, although not as strong, could be found in our study. When contrasting our oncology survey results against results from a recent national patient survey in Sweden conducted by Moll et al. 16 the differences between patients’ and physicians’ attitudes are quite noticeable. In the national patient survey, 97.3 per cent out of the 2587 respondents strongly agreed or agreed that Journalen is a good reform. In Region Uppsala, this number was 97.1 per cent.
One of the main reasons for conducting the survey study at this point was to follow up on results from earlier studies conducted less than a year after the implementation of Journalen in Region Uppsala. When it comes to contact with patients, the present survey shows that the perceived effects of Journalen are small, regarding patients showing concern for content in Journalen and the increased time for answering phone calls and emails. Thus, the problems related to worried patients and increasing time devoted to calls do not seem to be as severe as the health-care professionals feared 1 year after the launch of Journalen. 21 The survey results also show little support for the fear of visits taking more time due to questions based on the content in Journalen as the majority of the respondents in our study did not experience this effect. When it comes to documentation practices, the results show that the majority of both nurses and physicians agree or partly agree that they are more restrictive in their notes as a consequence of Journalen. This provides support for the concerns mentioned in earlier interviews with oncologists. 21 In the earlier interviews, physicians mentioned, however, that they would probably change the way they write about cancer in their notes, but the present survey results indicate that the majority of both nurses and physicians have not made any change regarding that disease category. The same goes for other conditions like obesity, addiction and mental health issues, even though a larger proportion of respondents indicate that they have made a change in the documentation related to those conditions. The recent survey study conducted by Petersson and Erlingsdóttir 26 showed that health-care professionals in psychiatric care also feared that they would be more restrictive in their notes after the launch of psychiatry records in Journalen. Their follow-up survey study 27 showed that large proportions of both psychologists and physicians in psychiatric care were indeed less candid in their documentation after the launch. These results indicate that mental health notes might be more affected than for example notes about cancer in this respect. This issue calls for further research regarding comparisons between different types of notes that the patient can access. When it comes to quality of care, the majority of both physicians and nurses did not see an improvement regarding effectivity or safety. These results are in line with studies performed shortly after the launch in Sweden,21,22 but in contrast to results from, for example, OpenNotes 8 showing that physicians saw benefits in these areas. This could be attributed to the differences between health-care professionals’ perception from different clinics indicated by Wass and Vimarlund. 11
The responses regarding the supposed experiences for patients (Table 7) indicate that the respondents, and especially the nurses, believe that there are some positive effects of PAEHR for patients. On the other hand, the results also show that the majority of both physicians and nurses believe that the notes are confusing for most patients and that patients feel more worried now. These results are in line with earlier interviews conducted by Grünloh et al. 21 where physicians said that they were concerned about that patients would get worried and start calling or emailing (e.g. about notes about severe diagnoses that they find in the records). It is noticeable that a larger proportion of respondents believed that patients feel more worried than the proportion that has actually experienced worry from reading patients.
Some of the results of this study are interesting from a gender perspective. Nurses in oncology are mostly women, whereas the physicians are a more mixed group. Women are traditionally expected to be more caring, and gentleness and empathy are attributes stronger associated with women than with men in many cultures and contexts. 28 Hence, the tendency that nurses experience worry from patients stronger than physicians do might be a result of the gendered norms related to nursing as a female-dominated profession. Perhaps patients express worry to a higher degree with nurses given that they are often women than with physicians who comprise a more mixed group when it comes to gender. These results could also be a consequence of women doing gender and being more receptive to patients’ worries related to PAEHR and hence reporting in the survey that patients are worried more often. The fact that a larger proportion of nurses than physicians believed that the majority of patients are confused by the notes and feel more worried now could also be attributed to this. Another example where the results might be attributed to doing gender is that nurses adapt their way of documenting to a larger extent than physicians. The nurses who do this could be seen as a doing gender in being caring and gentle towards other people, and hence fulfilling expected behaviour.
Limitations
Although the response rate was relatively high, 176 responses from 64 physicians and 112 nurses is a limited sample and hence the generalizability is limited. Another limitation is the focus on oncology health-care professionals and the particular hospital Uppsala University Hospital. This focus enabled a comparison of results between the present survey study and earlier studies performed at the same site, but generalizations to other regions and medical professions are not appropriate to make in this case. Even though it is reasonable to believe that time constraint is the main reason for drop-outs, it is not possible to rule out the possibility that the group of non-responders are more negative towards the system.
The comparisons we made between our survey results and results from earlier interviews and surveys are also limited by the fact that research methods and questions differ between the studies. Although the comparisons made above gave many indications of differences between supposed and real effects of PAEHR, the differences in methods used still need to be kept in mind when judging those results.
It is also important to note that some questions, for example, regarding the change in documentation practices, might be conceived as sensitive in that changes might not be in accordance with ethical standards. Even though the questionnaire was anonymous, this has to be kept in mind when judging the results.
Conclusion and future work
The results from our survey study indicate that PAEHR have had effects when it comes to the work of oncology care professionals. The clinician-perceived effects seemed to be largest when it comes to documentation practices – around 70 per cent of both physicians and nurses agreed or partly agreed that they were more restrictive in their notes now. When considering changes in notes with regard to specific disease groups, the effects were clearest when it came to notes about mental health and addictions. A vast majority of both physicians and nurses also agreed or partly agreed that it was generally a good idea to make medical records available in Journalen. Comparisons with earlier studies, mostly focusing on supposed and/or short-term effects of PAEHR, indicate that the perceived effects 6 years after the launch of the system are far from the ones put forward in the earlier studies.
The results show that both physicians and nurses see the value of the PAEHR for patients, especially regarding an increased feeling of control and a better possibility to prepare for visits. The majority also think that the notes are confusing to most patients and that most patients feel more worry after being able to access notes in their PAEHR. In future studies, it would be interesting to conduct a similar survey study with cancer patients in order to see whether the health-care professionals are indeed right about these supposed effects on their patients. Since the present study indicated discrepancies between supposed or perceived short-term effects and perceived effects measured 6 years after the launch in Region Uppsala, regarding all of the themes in focus, it would also be worthwhile to run a national survey study with oncology health-care professionals as well as health-care professionals in other disciplines to see to what extent our results can be generalized to other regions and medical disciplines.
Footnotes
Acknowledgements
The authors would like to thank especially the business developer within the area of blood and tumour diseases at Uppsala University Hospital and the heads of the involved departments for helping with the vital task of distributing and collecting the surveys. The authors also want to thank their colleague Christiane Grünloh, for her valuable feedback on the first draft of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Forte (Swedish Research Council for Health, Working Life and Welfare) (grant number 2016-07153).