
Abstract
Mobile applications (apps) have the potential to improve mental health services. However, there is limited evidence of efficacy or responsiveness to user needs for existing apps. A lack of design methods has contributed to this issue. Developers view mental health apps as stand-alone products and dismiss the complex context of use. Participatory design, particularly an informed participation approach, has potential to improve the design of mental health apps. In this study, we worked with young mobile users and mental health practitioners to examine the informed participation approach for designing apps. Using auto-ethnography and a set of design workshops, the project focused on eliciting design requirements as a factor for successful implementation. We compared resultant ideas and designs with existing apps. Many user requirements revealed were absent in existing apps, suggesting potential advantages to informed participation. The observation of the process, however, showed challenges in engagement that need to be overcome.
Keywords
Introduction
The availability of smartphones makes them an attractive option for providing health services because they make digital and connectivity tools accessible to the public with relatively low cost. 1 The high penetration of smartphones internationally means that mobile health, with its capacity for so-called nomadic modes of interaction between users and mobile devices, presents opportunities for addressing existing healthcare challenges.2,3 Mobile solutions have the potential to revolutionise mental health services, with new mental health–focused applications (apps) added to app stores on a daily basis. Often, these apps are based on a physical health model, substituting food or exercise tracking for mood or sleep tracking. However, there is limited evidence of efficacy for existing mobile mental health (mMH) apps in real-world contexts.4–6 Even apps with proven clinical efficacy do not achieve the desired outcomes in real-world settings, as users may not continuously engage with the app or adhere to the recommended/planned usage scenarios.6,7 Apps are not stand-alone digital solutions; they have the potential to be touchpoints for mental health services, as part of a complex ecosystem of various stakeholders, including the user, their family and friends, mental health practitioners, and relevant private and public health organisations.
Although there is a rich literature around technologies and policies that can empower mMH,4,7 we still do not know much about suitable mMH ‘design’ approaches. Design methodology has the potential to significantly improve the success of mMH solutions, if one defines design as devising courses of action aimed at changing existing situations into preferred ones, 8 aiming to solve wicked and multidimensional problems. 9 Considering the complexity of mental health services, and existence of multiple stakeholder groups with various requirements, using an appropriate design methodology that takes into account these complexities is vital.
In this research, we aimed to assess the feasibility and effectiveness of using an informed participation approach in designing an mMH app with two user groups who are part of the complex mental health ecosystem: young people (users) and mental health practitioners (stakeholders).
Using design approaches in healthcare
Although there are many existing mMH apps, there is little regulation of this market or research into efficacy. Seeking healthcare information in a poorly regulated digital space may mean risk of accessing poor quality or inaccurate resources by people.10,11 Attempts for reviewing and regulating available products have failed up to now, 12 although there are some promising new approaches. 13 Existing research on mMH apps typically views them using technological 14 or clinical 15 lenses, and few rigorous and evidence-based studies have focused on mMH.16–20 Only a small number of available mMH apps can provide evidence of efficacy,18,19,21 and there is evidence that some commercial apps could be potentially harmful.22,23 As a result, public health organisations including the United Kingdom’s National Institute for Health and Care Excellence (NICE) have trialled standards or programmes for improving user experience.24–26 Using and improving design processes and tools rather than just regulating numerous end products may have benefit for healthcare consumers.
In healthcare, design often uses an evidence-based approach built on a core principle of making decisions based on the best available research evidence. 27 Evidence-based design includes a mix of methodologies and tools and is best viewed as a problem-solving approach 2 rather than a method for shaping physical objects and spaces. As healthcare evolves, design methods need to do the same. Existing evidence-based healthcare design approaches do not take into account some subjective, hard-to-measure, and tacit aspects such as user experience. Poor design may affect dropout rate, future treatment-seeking behaviour, and even quality of life after treatment. 28 Previous emphasis has been on adjusting existing design methodologies for developing mMH apps, including rethinking participatory design for users with serious mental health illnesses29,30 and adapting user-centred design process by defining multiple players in the process.31,32,33
Participatory design and informed participation
In light of the challenges of evidence-based design, regulation of apps and adapting design approaches, participatory design is a promising approach for this domain, 34 with a strong connection to healthcare design and delivery via evidence-based practice.35,36 Like other established design methodologies, it can be problematic if the goal is to develop high-quality solutions and implementable results within limited time constraints. 37 Using an informed participation approach has helped to overcome this in some domains.38–41 In informed participation, participants use the information and tools provided by the designers to incrementally obtain ownership of problems and to contribute actively to their solutions. 42 This co-design approach encourages engagement in real-world settings.
In informed participation, the research agenda is open and transparent throughout, and the motives and objectives of data collection methods are known to participants. 43 Traditional science and engineering processes used for designing systems, 44 and even some common user-centred design methods, such as shadowing observations, 45 cannot be categorised as informed participation. In contrast, co-design as an interactive process, evolving with participant engagement, can be considered informed participation. 44
Informed participation allows less engaged or unrepresented communities to have a voice in design.46,47 For mMH research, enabling informed participation presents opportunities, 48 but also challenges. Smartphones provide users with a high level of customisation and flexibility of use, allowing participants to direct the research. However, there are ethical concerns, as these devices are also effective tools for covert data collection. 49
To assess the feasibility and effectiveness of using an informed participation approach, we worked with young people (users) and mental health practitioners (stakeholders). The design project focused on the promotion of good well-being and prevention of mental health issues for young people, including increasing problem-solving and coping skills. We hypothesised that concentrating on feasible requirements-gathering practices within the participatory design approach may help overcome the challenge of involvement in design and development of usable systems. 50 Because it was not possible to fully develop and test the app, we compared the design requirements and concepts developed with existing mMH apps to assess whether the informed participation approach revealed design requirements that have not been considered before.
Method
To ascertain whether a participatory design approach was effective and feasible, we used an action research approach. Action research involves changing practice and improving knowledge about a practice or social system, in which the action researcher is also a practitioner (in this case, a designer, and an ethnographer with no design background who participated in the workshops) and the research is not separated from the action itself.51–53 Participatory design has deep roots in action research and can be considered as reflective practice.54,55 Action research is frequently used to improve and manage changes in healthcare systems and services.56–58 Using a reflective action research approach, we were able to examine the design process as observers engaged in the process, considering its feasibility and effectiveness.
Study design
The study comprised three elements: an auto-ethnography and design learning process with two user groups and a review of currently available mMH apps informed by the findings from the first two elements. The study aimed to analyse the process of using an informed participation approach and not just the products of doing so, meaning that diverse data were gathered.
Two user groups participated:
Young people/users: Seven university students aged 18–20 years not currently enrolled in a design course.
Mental health practitioners/stakeholders: Ten members of the university’s counselling and mental health services team.
Users were invited to participate by an email invitation distributed via undergraduate student mailing lists. We recruited from a sample population across a university (all students aged 18–20 years who were not on a design course) and took all volunteers. Young people were identified as a relevant and under-represented group within design processes. On the recommendation of the university research ethics committee, we sampled from the general student population rather than working specifically with participants with mental health issues. This was an appropriate user group to work with, as we planned to have a well-being and prevention focus, rather than treating specific mental illnesses. Mental health practitioners agreed that coping and problem solving were core skills for improving mental well-being. Despite its importance, well-being and prevention are relatively less explored aspects of mMH. 59
To recruit stakeholders, the research team attended a meeting of the university counselling and mental health services team and explained the requirements of the study; 10 practitioners volunteered to participate. Informed consent was given by all participants.
Two novel components in the study design specifically engaged with the informed participation approach:
Auto-ethnography. As an instructional tool, this method helps researchers and participants to gain profound understanding of the self and others. 60 The participant retroactively and selectively writes about experiences, combining autobiography and ethnography, and considers systemic relationships. 61 It provided participants with a high level of control and self-awareness.
Design learning workshops. To design with participants, we integrated practical design learning components (design education delivered via lectures and practical sessions) that enabled participants to view themselves as designers. We shared our definition of design and objectives at the start of the project. As a result, participants developed design briefs and ideated and prototyped design concepts for mMH apps.
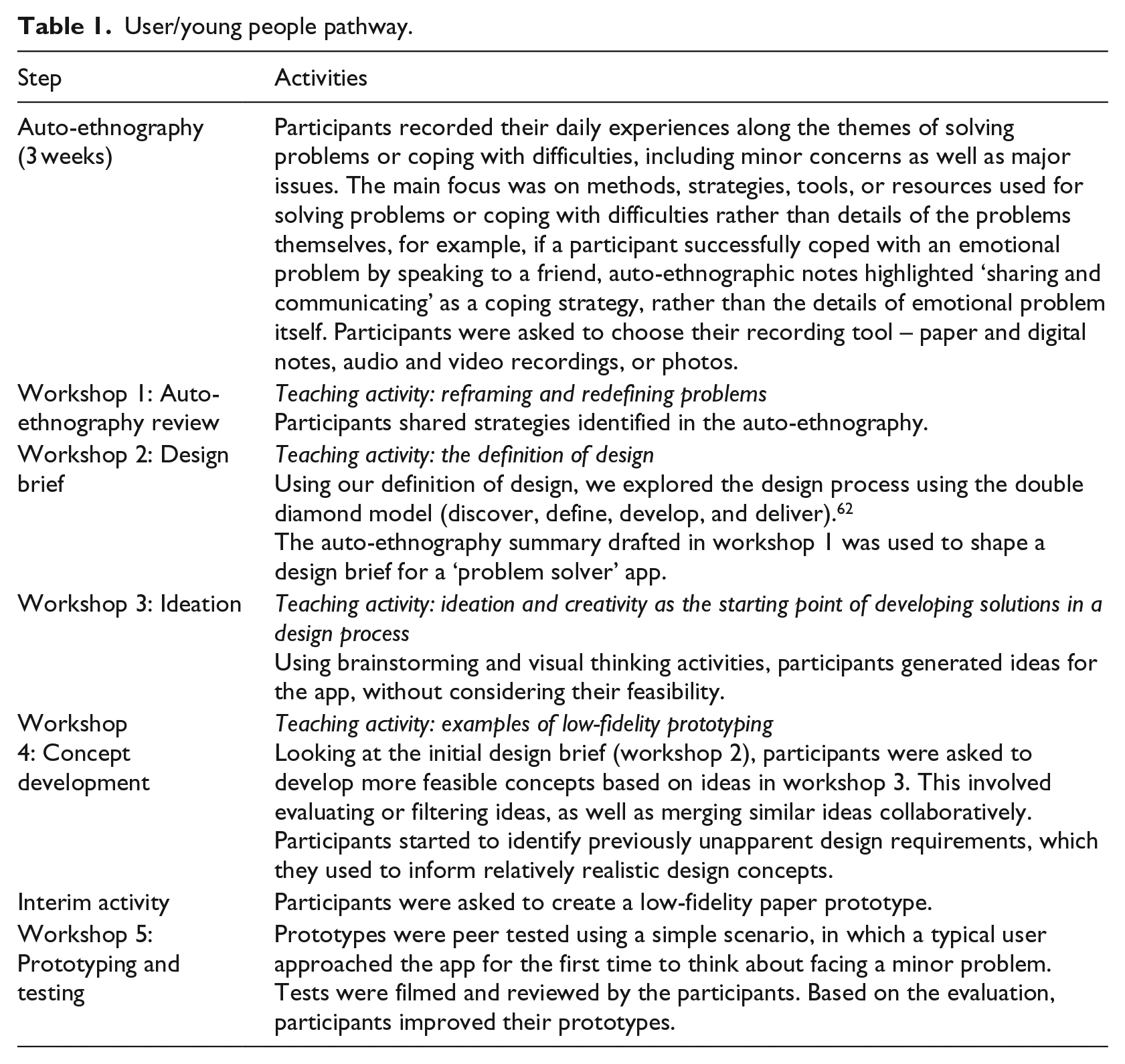
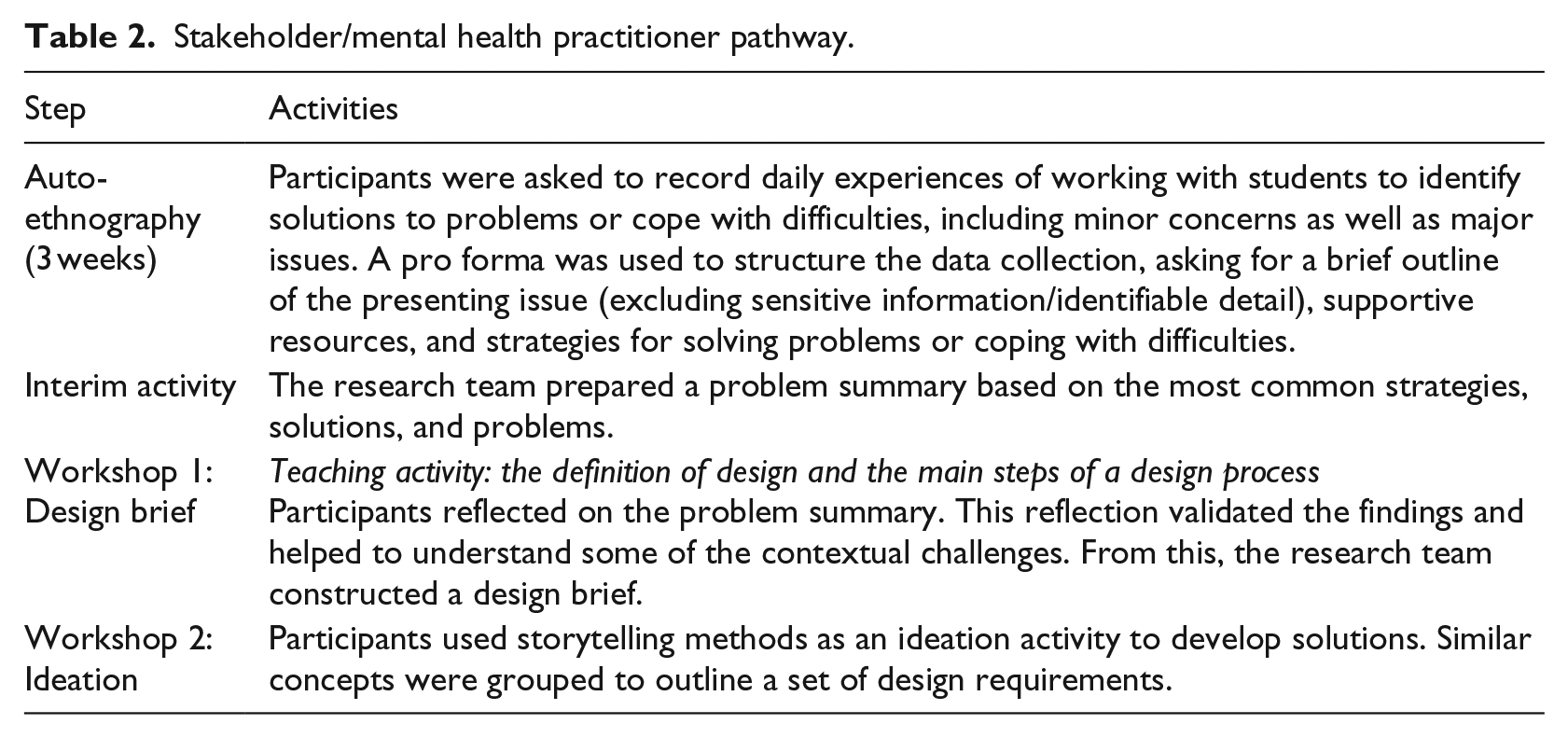
The study comprised two separate pathways for young people, as primary users of mMH apps (Table 1) and practitioners as secondary users/stakeholders (Table 2). Evidence suggests that young people and mental health practitioners are not generally involved in the mMH app design process, so we considered them to be legitimate participants in an informed participation approach. Time constraints meant that stakeholders were able to attend fewer workshops than users, although the nature of activities and objectives remained broadly the same.
User/young people pathway.
Stakeholder/mental health practitioner pathway.
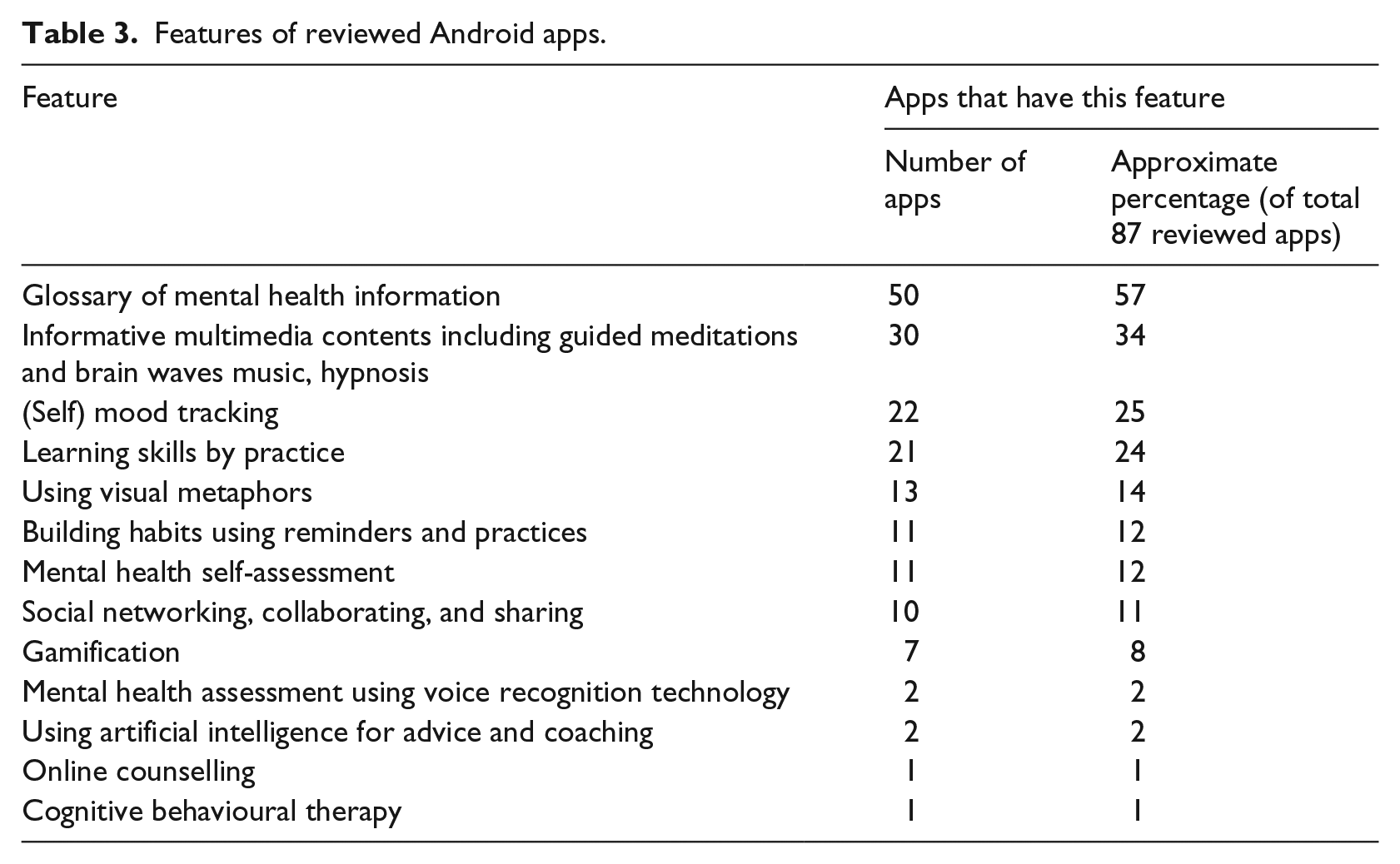
Finally, we compared the pathway outcomes with existing products, looking at mMH apps in the Google Play app store using the keywords ‘problem solving’ and ‘coping’ in the health and fitness, lifestyle, and medical categories. Eighty-seven apps were found based on this search criterion. We searched this app store because Android was the most common mobile operating system worldwide at the time of study. 63 The mMH app content was analysed using a content-driven framework based on classifying the features in the apps themselves, then via another framework constructed from the findings from the user and stakeholder design process.
Data analysis
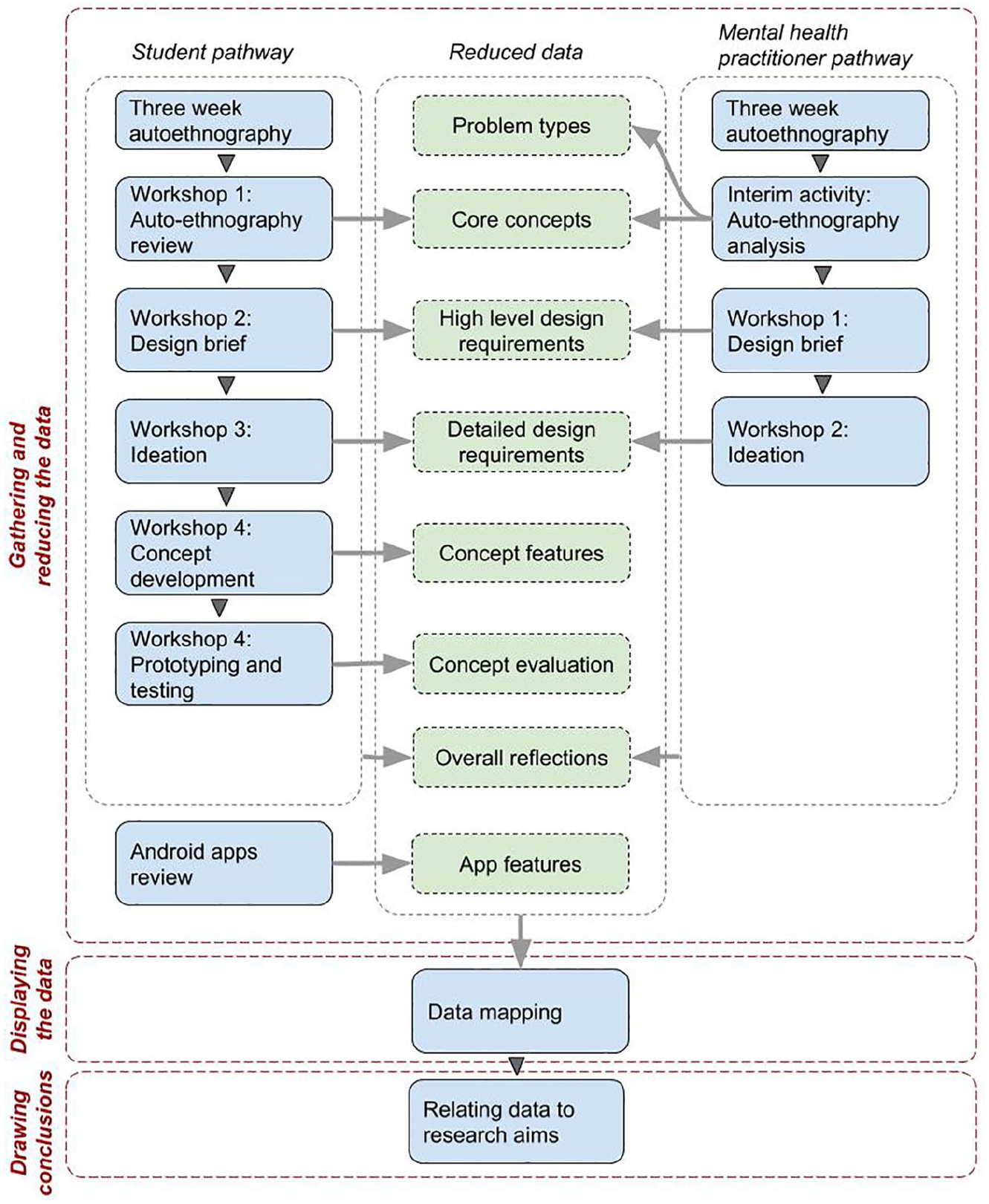
A three-step qualitative analysis was used to gather and reduce (code) the data, visualise the data, and draw conclusions (Figure 1). 64 This was based on a data-driven constant comparison approach, 65 which was closely grounded in observations of the workshops and was also responsive to the action research approach. Data mapping and visualisation helped us to compare results from different data sources and relate outcomes to the research aims.
Study design.
Results
In summary, data collected were auto-ethnographic data and participants’ reflections on these data, ideas in textual and visual formats, low-fidelity prototypes, observation notes mapping the procedure and reflections on each workshop, video recordings of prototype tests and comparison between prototypes, and a review of available mMH apps (Table 3). The fast-paced nature of developing technologies means that descriptions of current technologies quickly become obsolete; for this reason, we have provided an outline of the features included rather than the specific apps.
Features of reviewed Android apps.
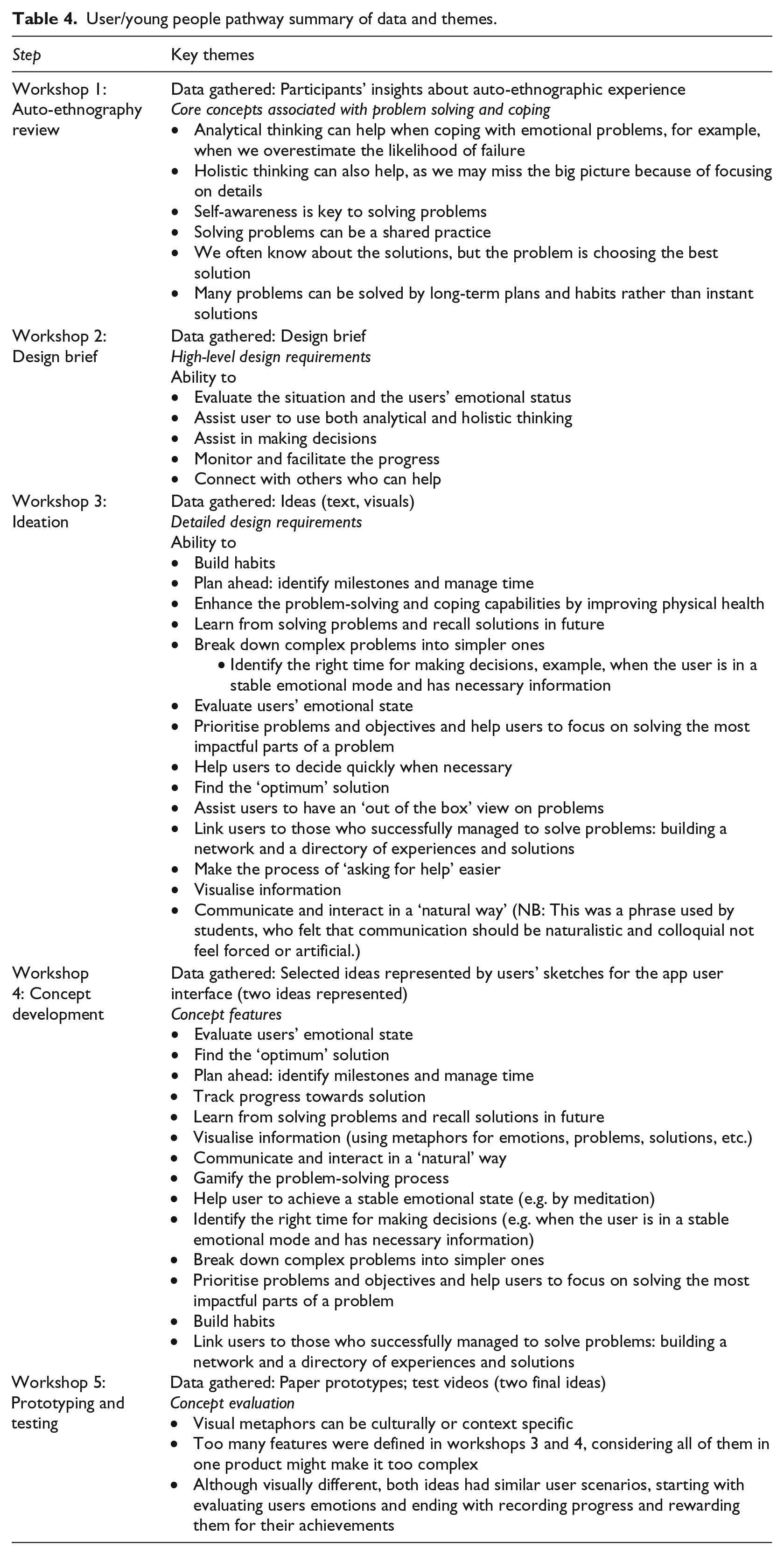
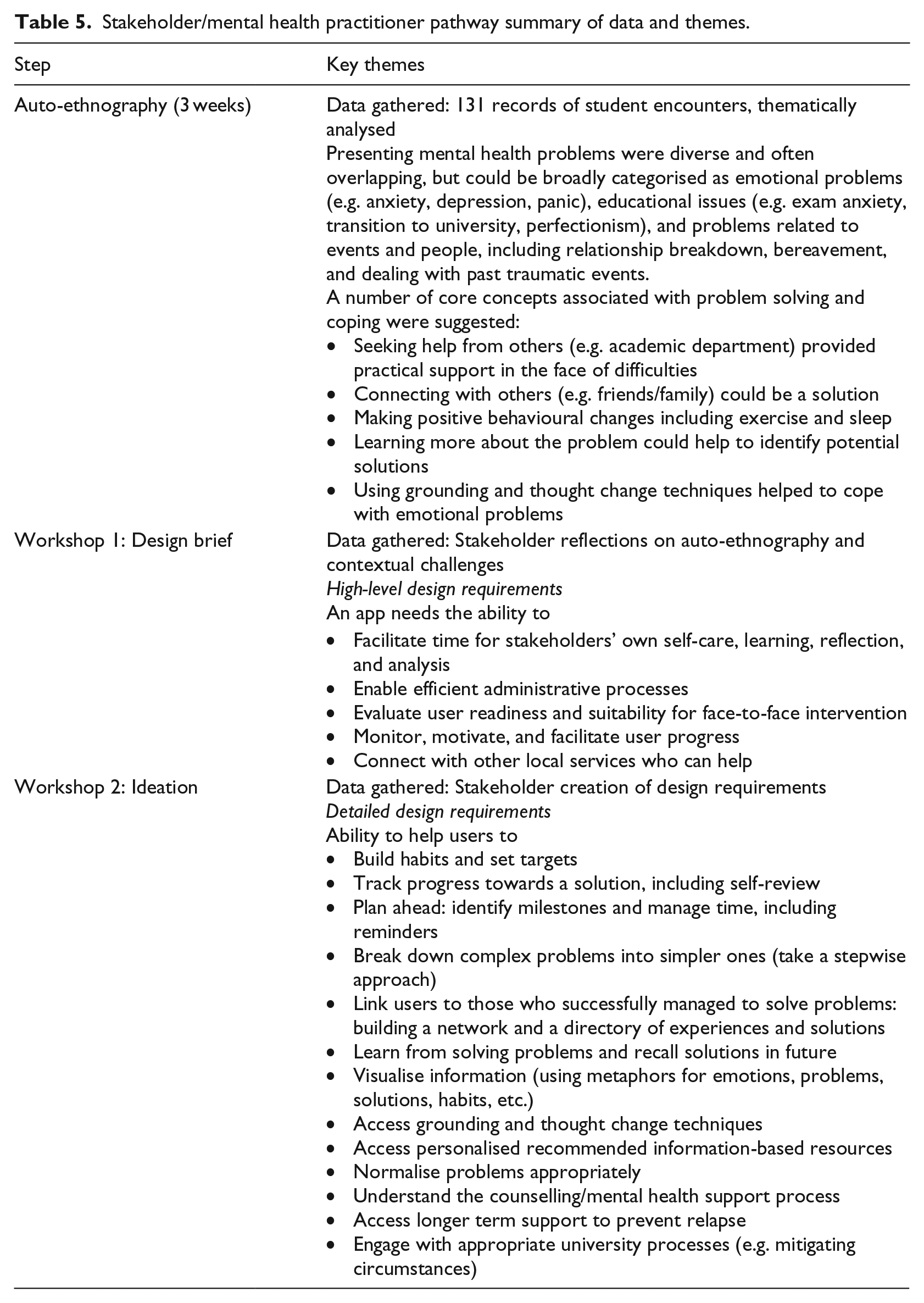
From the data collected, we were able to extract a number of core concepts associated with problem solving and coping, which were then used to identify high-level and detailed design requirements for the users (Table 4) and stakeholders (Table 5). High-level requirements are broad themes identified by the participants. Detailed requirements expand on these high-level themes to provide greater clarity about how these high-level requirements will be achieved. For the users we worked with, we were able to extend this process to identify concept features that an mMH app might have and start to perform concept evaluation with prototypes (Figure 2). Key themes emerging across the data from both participant groups were then compared and similarities and differences highlighted. We then compared the themes in user and stakeholder data with existing mMH apps (Tables 6 and 7). From this process, we were able to address our aim of investigating whether the informed participation approach was effective in identifying design requirements.
User/young people pathway summary of data and themes.
Stakeholder/mental health practitioner pathway summary of data and themes.
Prototype testing in concept evaluation workshop.
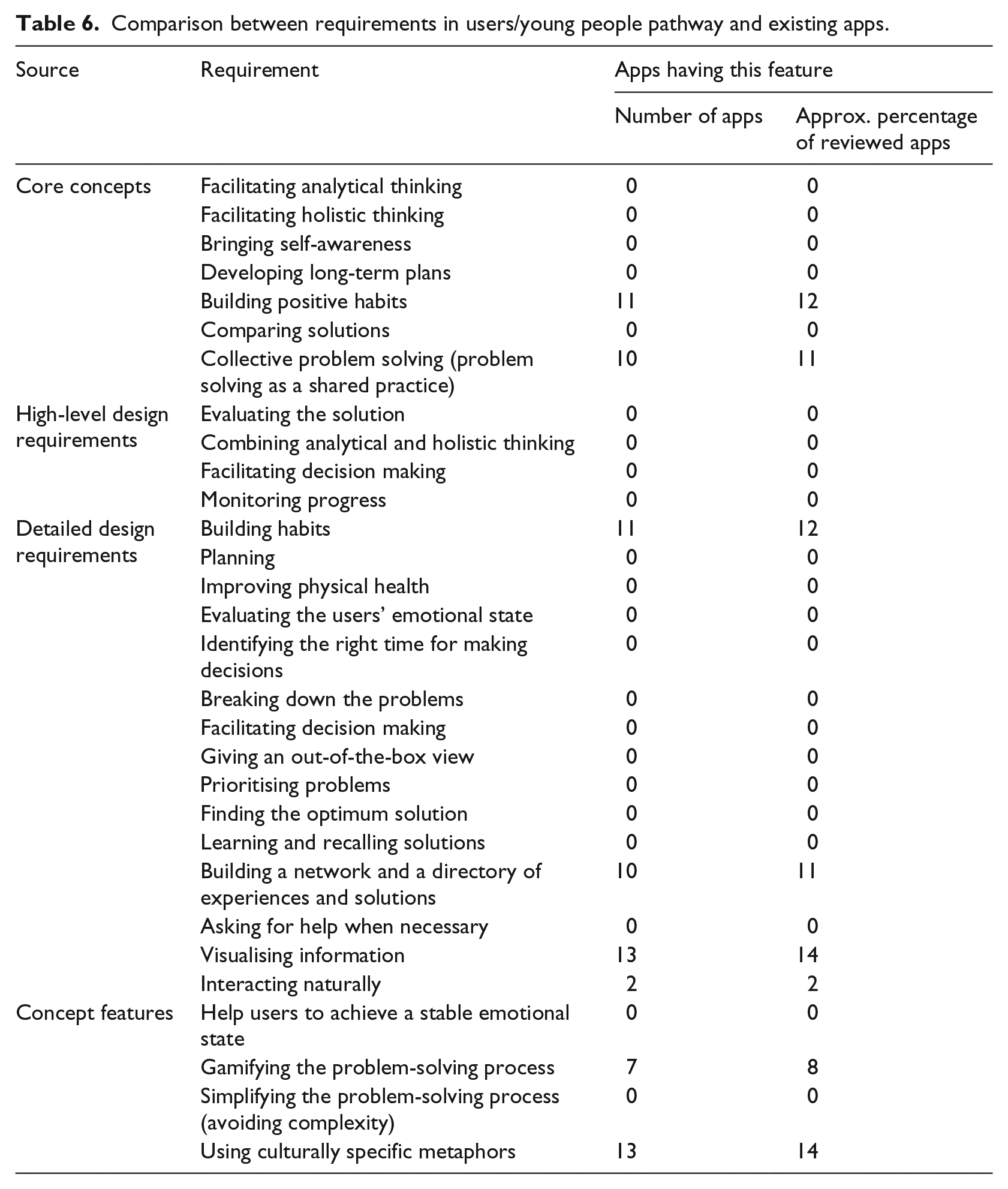
Comparison between requirements in users/young people pathway and existing apps.
Comparison between requirements in stakeholder/mental health practitioner pathway and existing apps.
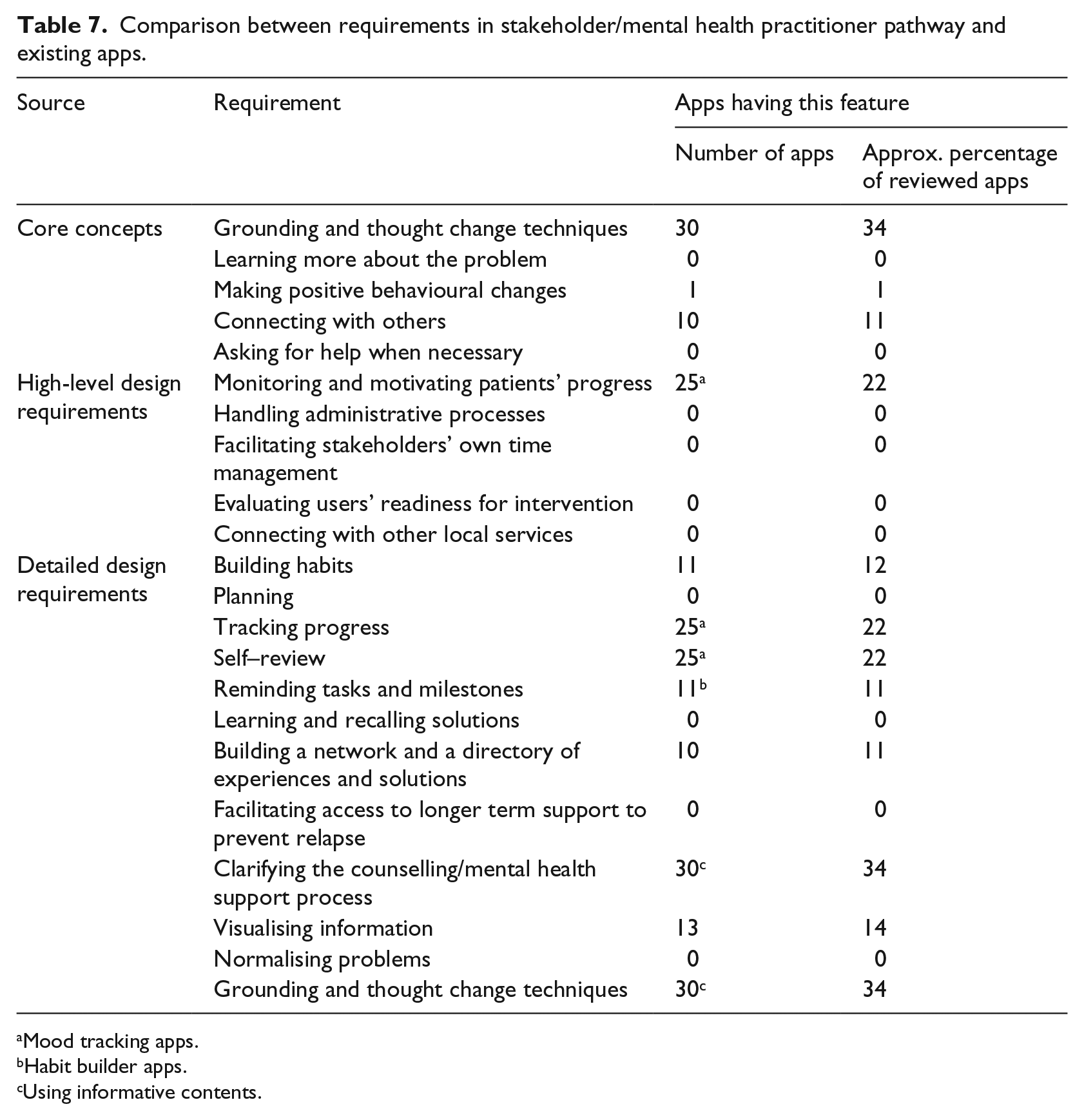
Mood tracking apps.
Habit builder apps.
Using informative contents.
By examining the core concepts found in user and practitioner auto-ethnographies, we found that core concepts were described differently, but addressed similar issues. For example, stakeholders noted the importance of asking for help and connecting with others. Users focused on problem solving as a shared practice. Detailed design requirements showed greater overlap, and some detailed requirements from stakeholders can be linked to concept features found in the users’ planning of apps. Most features in the final design concepts were directly linked to design requirements outlined earlier in the process. In mapping existing app features, user and stakeholder design requirements, and user concept features, we found that not all requirements and features were present in existing apps.
Data collection also allowed us to address the question of whether an informed participation process was feasible. The data collection process showed that the challenges of implementing the approach include the length of time required for the process. For both users and stakeholders, although there was enthusiasm for the project, limited time was available to learn techniques, generate ideas, and design requirements and produce prototypes. Users, who were unfamiliar with the design approach, also struggled with the openness and ambiguity within the process. This had a negative impact on participation, with one participant (an engineering student) withdrawing from the study because they felt that the process was too vague.
In summary, using an informed participation approach identified design requirements and concepts not currently commonplace in existing mMH apps, which predominantly provided information and/or multimedia content, such as guided meditations. Users focused much more on expanding their options for problem-solving by link building and they wanted to help identify the right time for making decisions. Users wanted an app to help them to identify milestones, manage time, and track progress towards a solution, and to be iterative in learning, recalling solutions in the future. All of this had to be achieved with the mMH app communicating and interacting in a ‘natural’ (note: this was a phrase coined by users, who felt that communication should be naturalistic and colloquial not feel forced or artificial) way.
Mental health practitioners had similar requirements, but also wanted an app to have a focus on helping young people they worked with to normalise problems appropriately, to understand the counselling/mental health support process, and to provide access to grounding and thought change techniques and personalised recommended information-based resources. They considered when an app might be useful, for example, in accessing longer term support to prevent relapse and to help users engage with appropriate processes (e.g. for a university context, exceptional circumstances committees) to support them.
Discussion
Our experience of implementing an informed participation design process demonstrates that it is a promising approach that is effective at outlining user requirements that could not be identified in currently available apps. We particularly focused on design requirements and product features, as we recognised that successful requirements gathering can significantly affect successful implementation. 66 However, the length and ambiguity of the process may still affect user engagement, leading to questions about its feasibility. This mirrors previous studies, which have highlighted that engagement in processes is challenging. 67 Analysis showed that 11 of the 13 features identified in the user pathway final concepts were identified in the earlier steps. Focusing on the auto-ethnography and requirements-gathering steps may be a solution for shortening the process, and consequently improving user engagement.
Users and stakeholders identified different requirements and features, but expressed similar core concepts. These core concepts emphasise a need to learn different thinking and grounding patterns, looking at problem solving as a shared practice, and empowering positive habits and behaviour changes. When online reviews of mMH apps have been analysed, similar calls for discrete social networks within apps have been noted. 68 Both participant groups required a combination of features in their ideal solution, helping them through the whole problem-solving process.
Existing apps are often designed to contain one or two features, without supporting a sustainable and holistic process, which is a weakness of current provision. Apps on the market were mainly information giving (57%) or informative multimedia content (34%). Participants in our research identified much more diverse requirements involving collective problem solving and thinking about how to think and behave differently. When we compared existing apps to the requirements gathered, one significant finding was that our users and stakeholders wanted one app that covered all their requirements, whereas apps tended to concentrate on one or two specific features. Apps that took a more holistic approach were not available.
Paper prototyping showed that sustaining the complexity of these features within one mMH app may be difficult. Instead, creating a suite of apps with a hub may be an option. 69 The requirements identified here were able to address scenarios of use in a detailed, everyday, and comprehensive way. For users, these requirements included the ability to identify and evaluate emotional states to consider when it was an appropriate time to make a decision to solve a problem, and tools to break down complex problems into simple ones. For the stakeholders, it was important that the tool could be appropriately personalised, connecting both to local services and appropriate information resources, and could help the user to understand their problems and the process for solving them in context. Many stakeholder requirements initially focused on addressing service processes, something which is missing in the existing apps. However, their overall design requirements showed that encouraging independence, self-review, and engagement would meet many of these needs.
As we were not able to develop and test beyond the prototyping stage in this small pilot study, future work could consider how open innovation methods, 70 such as innovation jams, 71 may have a role to play in further development. Innovation jams encourage the rapid generation of many ideas by a large cohort, and thus speed up the process of getting from initial idea to finished product. This may assist with engagement.
Strengths and limitations
This was a small-scale study, focused on one particular under-represented group (young people), and it is difficult to generalise the results for designing mMH apps. We did include two major stakeholder groups (young people and mental health service providers), and reflecting on the differences between these two groups brings valuable insight into the use of the methods. As the study was conducted in students without mental health problems, this is also a limitation, and using informed participation approach would require further testing in this population. Future research could examine the informed participation approach at scale, for example, at an organisational level, or with other groups. A strength of the study is that we collected diverse and rich qualitative data and supplemented it with a quantitative review. However, one of the limitations of participatory design in general is a lack of quantitative evaluation methods.
Conclusion
Informed participation can close the gap between ideas, final concepts, and prototypes by enabling users to generate feasible, relevant, and detailed ideas that can communicate anticipated design requirements in further concepts and prototypes. Informed participation had a positive impact on implementability of designs, but this exploratory study also demonstrates the necessity of further rigorous work to develop and evaluate market-ready mMH apps.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of Lancaster University’s Counselling and Mental Health Services Team who gave us generous support by participating in the study, allocating time for the study events, and sharing their valuable insights. The authors would also like to thank their student participants for their time and insight.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.