
Abstract
Stroke is the leading cause of adult disability worldwide, with 70 percent of survivors exhibiting residual impairments of the upper limb that require frequent in-person visits to rehabilitation clinic over several months. This study explored rehabilitation clinician’s preferences for design features to be included in an mHealth-enabled app for post-stroke upper limb rehabilitation. Data were collected via online survey, sampling participants from Ethiopia (n = 69) and the United States (n = 75). Survey results indicated that Ethiopian and US rehabilitation clinicians have different opinions about the importance of design features that should be included in a stroke tele-rehabilitation system which are likely due to differences in culture, the availability of human and physical resources, and how the field of rehabilitation is organized and managed. Our results, thus, indicate that mHealth technologies must be tailored to the geographical and cultural context of the end users.
Introduction
Stroke is the leading cause of adult disability and the second leading cause of death worldwide. 1 Although the rate of stroke incidence in developed countries has decreased by 42 percent over the last four decades, over the same time period stroke prevalence has more than doubled across sub-Saharan Africa. 2 Furthermore, stroke occurs 10 to 15 years earlier in sub-Saharan Africa than in developed countries,3–5 and stroke survivors from sub-Saharan Africa also exhibit poorer prognoses 6 and more severe long-term physical disabilities than their counterparts from developed nations. 7 , 8 As a result, stroke has a more significant impact on the productive workforce in sub-Saharan Africa than is usually the case in developed countries. 6 , 7
After a stroke, individuals are left with a broad range of disabilities, such as weakness or paralysis, sensory loss, immobility, spasticity, and stroke-related pain. Impaired arm and hand function significantly limits a person’s ability to perform activities of daily living (ADLs), and has a detrimental effect on independent living and economic self-sufficiency. 9 , 10 Fortunately, there is ample evidence that repetitive practice of goal-directed, functional movement (i.e. repetitive functional task practice) facilitates neural reorganization and motor recovery, resulting in improvements in both quality of life and functional independence. 9 , 10 However, conventional stroke therapy is a labor-intensive process, which involves daily one-on-one interactions with therapists that can last for several months. Unfortunately, conventional stroke therapy places a significant burden on health care systems and facilities in sub-Saharan Africa that struggle with a shortage of rehabilitation professionals and technical resources crucial to the delivery of physical rehabilitation services.11–13
One solution is to leverage information and communications technologies (ICTs) and mobile health care (mHealth) systems to provide rehabilitation services at a distance, as these have been demonstrated to reduce the cost and burden of travel, deliver information and services over any distance, and provide continual accurate assessment of a patient’s upper limb function across the rehabilitation program. 14 Conventional stroke rehabilitation protocols (e.g. repetitive functional task practice, constraint-induced movement therapy) are well suited for tele-rehabilitation as they do not require specialized equipment and can be conducted in decentralized locations, such as the patient’s home or community. In general, tele-rehabilitation interventions lead to improvements in clinical outcomes that are similar to or better than conventional rehabilitation, and are accompanied by high levels of patient compliance and satisfaction in developed nations. 15 , 16 Moreover, given the projected increase in the availability of Internet access in sub-Saharan Africa, 17 , 18 the potential to deliver personalized upper limb stroke management in people’s home environment using mHealth solutions can be realized.
That said, when developing and implementing mHealth solutions in underserved populations, designers need to recognize the factors that lead to marginal levels of user uptake and engagement that persists across almost all mHealth categories. 19 The general consensus in the literature is that low levels of mHealth adoption occur when mHealth solutions are not adapted to the local context and capabilities of the end users: coordination and communication among key stakeholders is ineffective, and when initial adoption and sustained implementation does not take into account the health system and ICT structure.20–23 Moreover, the expansion from small pilot projects to a regional or national solution cannot often be realized due to underfunding, unsupportive key government agencies, or a lack of corporate champion willing to fund the project expansion. Thus, ensuring the long-term financial sustainability of a particular mHealth solution requires transitioning from donor funding to alternative sources of revenue generation.
Objective
Ethiopia is the second most populous country in Africa, with a population of over 105 million inhabitants and a landmass of 26,373 square miles (1,104,300 square kilometers). 24 Unfortunately, Ethiopia is also one of the poorest countries in the world, with an estimated 21.9 percent of the population living on less than US$1.90 per day. Stroke is becoming an increasingly serious public health issue in Ethiopia and is one of the most common reasons for hospital admission. 25 , 26 Further compounding the issue is that health services required for stroke care are limited and remain concentrated in urban areas. Thus, many patients who have a stroke present late for medical care (median time = 27 h, interquartile range (IQR): 11.13–70.63 h), 27 face significant delays receiving care upon arrival, and often do not have access to rehabilitation in their communities. In addition, the study and practice of rehabilitation science is an emerging profession in Ethiopia, with the first formal program starting at the University of Gondar (UoG) in 2006. Despite these educational efforts, there remains a shortage of physiotherapists in Ethiopia (n = 350), 28 with one physiotherapist per 300,000 persons.
ICT can help improve the health sector by harnessing the potential of the growing number of mobile devices in Africa and by offering innovative approaches to health care through new tools and platforms. The ICT sector in Ethiopia has seen substantial growth over the last decade.17,29 From 2010 to 2015, the number of mobile subscribers increased from 6.7 million to 38.8 million people, and the percentage of rural districts with access to telecom services within a 5-km radius increased from 62.1 percent in 2009/2010 to 97 percent in 2014/2015. Looking to the future, the Government of Ethiopia has outlined plans to increase mobile service penetration rate from 43.9 to 100 percent, the number of broadband users from 1.91 million to 39.1 million, Internet and data density from 3.3 to 10 percent, and international link capacity from 27.9 to 1485 Gbs, all the while maintaining mobile service coverage at the current level of 81 percent. 17
For the past 3 years, the Health Equity Institute (USA) and the UoG (Ethiopia) have collaborated to strengthen the research and knowledge production capacity of the UoG and improve stroke care in Ethiopia. Foremost among these efforts are the co-design of an mHealth system for the delivery of personalized upper extremity stroke assessment and rehabilitation for those living in areas without ready access to, or geographic proximity to, rehabilitation services (i.e. the outREACH system). After much consideration, we determined that the business model most likely to yield long-term financial sustainability of the outREACH system is a social entrepreneurial model. Specifically, in our model, US-based for-profit rehabilitation clinics and end users would pay a monthly subscription to access the outREACH system, and the revenue derived from this market would be used to subsidize costs for resource-constrained individuals in Ethiopia. With this in mind, it is essential that the outREACH system consider the unique needs and requirements of both US and Ethiopian users from the outset of the project.
In this phase of the project, we used a user-centered approach to guide the design and development of the outREACH system for use in two culturally diverse contexts (i.e. the United States and Ethiopia). To achieve this aim, health care providers responsible for the clinical evaluation and program prescription of upper limb dysfunction (i.e. occupational therapists (OTs), physical therapists (PTs), and physiotherapists) rated the importance of 52 mHealth application features that could be implemented into the outREACH system. Although this survey is the first of many steps in the outREACH system development and implementation, the results provide invaluable information about the design features that should be included in the system and whether differences exist between clinicians based in Ethiopia and the United States.
Development of system content
In order to determine the possible features that could be implemented into the outREACH system, we first performed a review to identify mHealth apps related to stroke rehabilitation and/or upper limb rehabilitation. In our review of the literature, we did not find any studies reporting on the development or evaluation of mHealth apps. Thus, we also searched the gray literature on the Internet, the Google Play Store, and Apple App Store. Following our identification of existing mobile apps, we obtained expert guidance from a team of five highly qualified and experienced health professionals from various neurorehabilitation disciplines (physical medicine and rehabilitation, occupational therapy, physiotherapy, information technology, public health) with both national and global expertise in the field of upper limb stroke rehabilitation. This process yielded a total of 52 hypothetical mHealth application features that were classified into the following categories: rehabilitation program, clinician–patient communication, scheduling, patient profile, and miscellaneous features.
Methods
Participants
Rehabilitation clinicians from three metropolitan areas in the United States (San Francisco Bay Area, San Diego, and Chicago) and two cities in Ethiopia (Gondar and Addis Ababa) were recruited from professional networks of the authors. To be eligible to participate, rehabilitation clinicians needed to have experience working in outpatient facilities, have sufficient experience in the provision of therapeutic interventions targeting the upper extremity, and sufficient experience working with stroke patients. Approval for this study was granted by the University Institutional Review Board. The minimum number of participants required was determined by a priori power analysis (G*Power 3.1.9.2) 30 that indicated that a total sample of 128 participants (64 in each group) would be needed to achieve 80 percent power at two-sided 5 percent significance level.
Procedure and analysis
Rehabilitation clinicians provided information about their therapist characteristics (e.g. gender, age), clinical experience (e.g. education level, services provided to clients), experience with rehabilitation technologies, and their attitudes toward technology. In addition, rehabilitation clinicians rated the importance of 52 hypothetical mHealth application features. Each feature was rated using a 4-point Likert-type scale (0 = not at all important, 1 = somewhat important, 2 = very important, and 3 = extremely important). At the end of the survey, participants were provided the opportunity to provide written comments in order to share more rich and detailed opinions that could help in app development. All participants provided informed consent and could choose to decline to respond to any survey item. Data were collected with Qualtrics online survey software between September and December 2017.
Preliminary analyses were conducted on the 52 design features to check for differences due to gender, education, clinician experience with stroke, and attitudes toward technology. Analysis did not reveal any systematic differences, and thus data were collapsed across these variables. In order to examine the main effects due to group (The United States vs. Ethiopia), potential differences in importance ratings were examined using individual t tests, separately for each design feature. Although a Likert-type scale produces ordinal data, parametric statistical procedures were selected over nonparametric statistical procedures based on evidence indicating that parametric statistics result in the same conclusions as nonparametric tests 31 and they do not increase the likelihood of a Type I or Type II error. 32
Results
Rehabilitation clinician characteristics
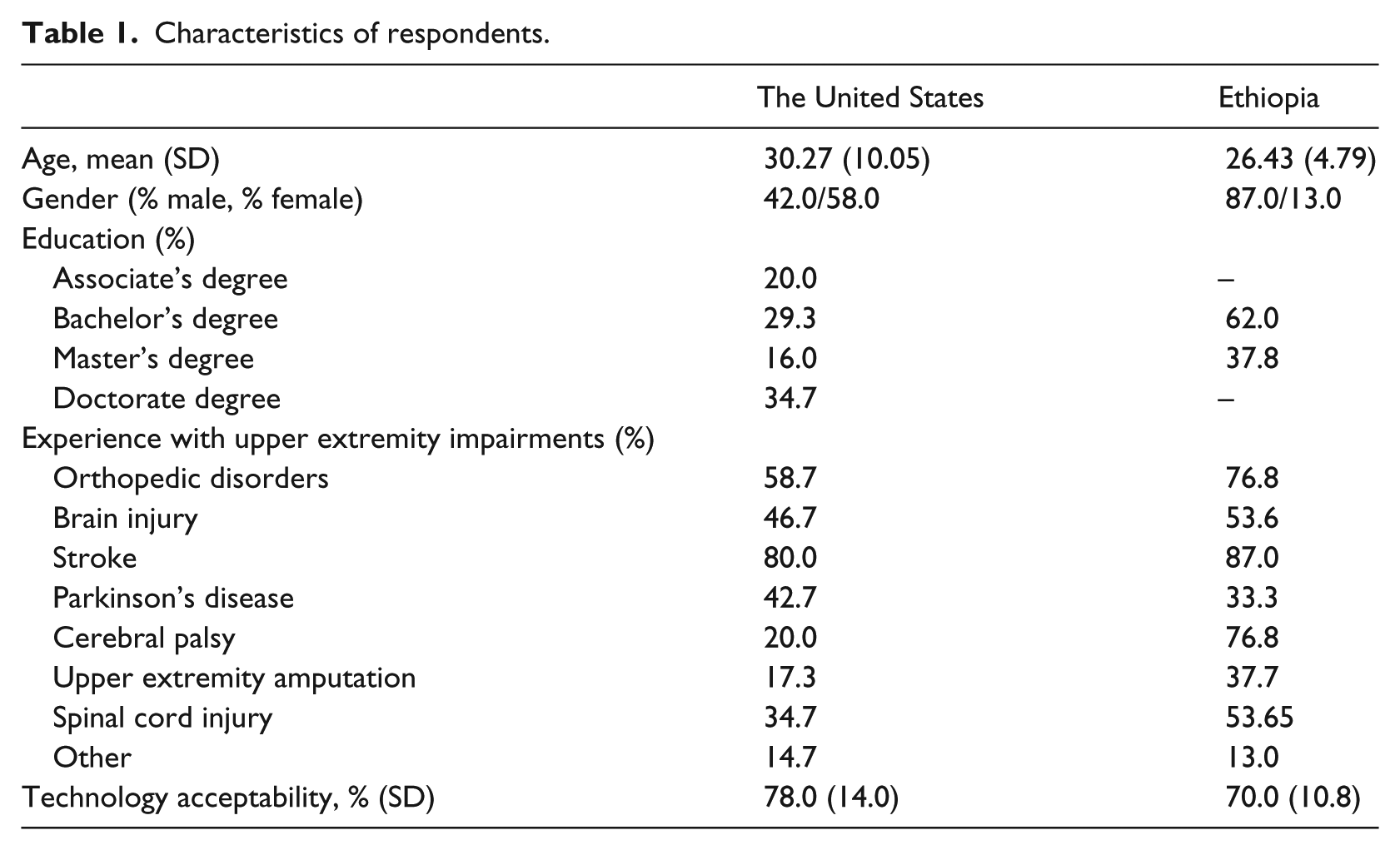
Table 1 presents a side-by-side view of the surveyed clinicians’ characteristics. There were 75 US respondents (male = 42%, female = 58%), who ranged in age from 18 to 61 (mean = 30.27 years, SD = 10.05). PTs comprised 66.6 percent of the sample (n = 50), whereas OTs comprised 33.3 percent of the sample (n = 25). Of the respondents, 34.7 percent (n = 26) had a Doctorate of Physical Therapy, 16 percent (n = 12) had a Master’s degree, 29.3 percent (n = 22) had a Bachelor’s degree, and 20.0 percent (n = 15) had an Associate’s degree. US respondents had experience providing services for clients diagnosed with stroke (n = 60), orthopedic disorders (n = 44), Parkinson’s disease (n = 32), brain injury (n = 35), spinal cord injury (n = 26), cerebral palsy (n = 15), upper extremity amputation (n = 13), and other disorders that required physical therapy (n = 11). There were 69 respondents from Ethiopia (male = 87%, female = 13%), ranging in age from 20 to 40 years (mean = 26.4 years, SD = 4.79). There were no Ethiopian respondents with a Doctorate of Physical Therapy degree, although 62 percent (n = 23) of Ethiopian respondents had a Bachelor’s degree and 37.8 percent (n = 14) had a Master’s degree. Ethiopian respondents had experience providing services for clients diagnosed with stroke (n = 53), cerebral palsy (n = 53), orthopedic disorders (n = 53), brain injury (n = 37), spinal cord injury (n = 37), amputation (n = 26), Parkinson’s disease (n = 23), and other disorders that required physical therapy (n = 9).
Characteristics of respondents.
Perceived importance of features accessible by rehabilitation clinicians
Table 2 compares US and Ethiopian rehabilitation clinicians’ preference ratings for potential design features for an mHealth-enabled app for post-stroke upper limb rehabilitation that would be accessible by clinicians. Overall, both US and Ethiopian respondents agreed that it was very to extremely important (i.e. rankings between 2.5 and 3.0) that a post-stroke upper limb rehabilitation app allow the rehabilitation team to modify a patient’s treatment plan (x̅ = 2.63, P = 0.911), video-record arm function for later analysis (x̅ = 2.60, P = 0.091), automatically log and update performance in a number of factors (x̅ = 2.60, P = 0.601), display prior and future appointments (x̅ = 2.61, P = 0.517), display content in languages relevant to the country or region (x̅ = 2.67, P = 0.497), and have search capabilities (x̅ = 2.67, P = 0.105). In addition, both groups felt that the patient profile features such as medical history (x̅ = 2.81, P = 0.201), medications (x̅ = 2.57, P = 0.963), diagnostic lab and test results (x̅ = 2.57, P = 0.425), prior and future appointments (x̅ = 2.52, P = 0.528), current arm function level (x̅ = 2.74, P = 0.552), and current quality of life, psychological status, and pain level (x̅ = 2.66, P = 0.171) were very to extremely important. Both groups thought it was very important (i.e. rankings between 2.0 and 2.5) that a post-stroke upper limb rehabilitation app graphically depicts patient performance in a number of factors (x̅ = 2.35, P = 0.057), can schedule in-person and home-based appointments (x̅ = 2.45, P = 0.067), have a means to bill patients or insurance companies (x̅ = 2.34, P = 0.495), as well as include the patient’s circle of care information (x̅ = 2.42, P = 0.297) and insurance information (x̅ = 2.03, P = 0.463) in the patient profile features.
Mean (SD) preference ratings for system features accessible by rehabilitation clinicians.
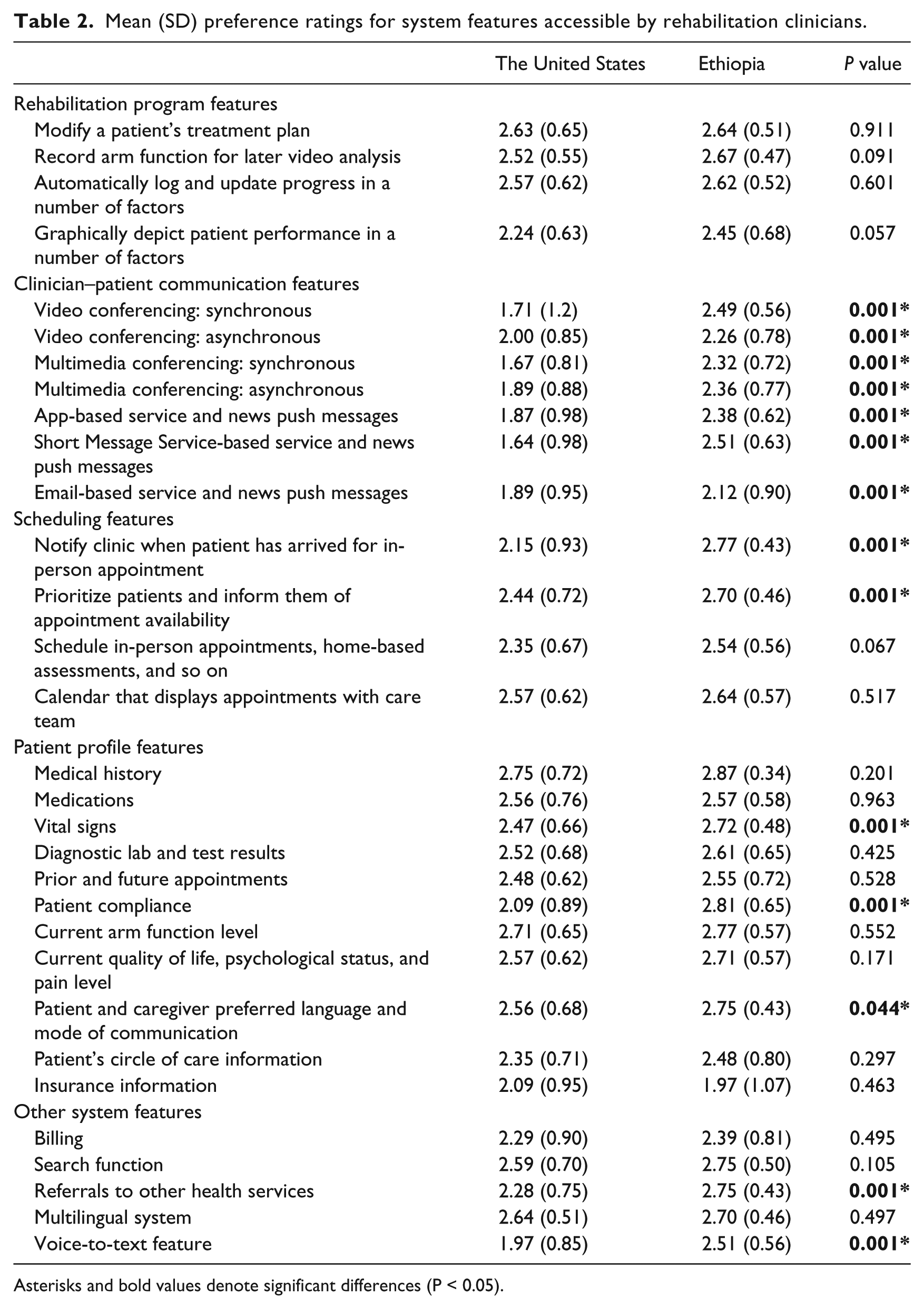
Asterisks and bold values denote significant differences (P < 0.05).
Group differences were observed for a number of design features accessible by rehabilitation clinicians. Although mean ratings differed between US and Ethiopian respondents, both groups thought it was very to extremely important that a tele-rehabilitation system include features that allow the rehabilitation team to collect and display patients’ vital signs (x̅ difference = 0.25, P < 0.001) and include the patients’ and caregivers’ preferred language and mode of communication (x̅ difference = 0.10, P = 0.044). Both groups thought that it was very important (i.e. rankings between 2.0 and 2.5) to allow for clinician–patient communication via asynchronous video conferencing (x̅ difference = 0.26, P < 0.001).
While Ethiopian respondents stated that it was very to extremely important that a post-stroke upper limb rehabilitation app be able to notify the rehabilitation team when the patient arrives (x̅ difference = 0.62, P < 0.001), prioritize patients (x̅ difference = 0.26, P < 0.001), and refer patients to other health services (x̅ difference = 0.54, P < 0.001), US rehabilitation clinicians rated the above-mentioned features as very important. Ethiopian respondents rated patient compliance (x̅ difference = 0.72, P < 0.001), voice-to-text (x̅ difference = 0.54, P < 0.001), and Short Message Service -based push messages (x̅ difference = 0.87, P < 0.001) as very to extremely important, while US respondents rated them as somewhat to very important (i.e. rankings between 1.5 and 2.0). Ethiopians rated synchronous video conferencing (x̅ difference = 0.78, P < 0.001), synchronous multimedia conferencing (x̅ difference = 0.65, P < 0.001), asynchronous text or voice conferencing features (x̅ difference = 0.47, P = 0.007), and email-based (x̅ difference = 0.23, P < 0.001) and app-based push messages (x̅ difference = 0.51, P < 0.001) as very important, while US respondents rated them as somewhat to very important.
Perceived importance of features accessible by patients and caregivers
US and Ethiopian rehabilitation clinicians’ preference ratings for potential design features for an mHealth-enabled app for post-stroke upper limb rehabilitation accessible by patients and caregivers are depicted in Table 3. Both groups agreed that it was very to extremely important that the patient/caregiver module of the app include a personalized rehabilitation program tailored to a person’s needs or impairment level (x̅ = 2.66, P = 0.153). Both groups thought it was very important (i.e. rankings between 2.0 and 2.5) that a post-stroke upper limb rehabilitation app allow patients/caregivers to pay for services (x̅ = 2.16, P = 0.247), display content in languages relevant to the country or region (x̅ = 2.42, P = 0.273), remind users to complete their rehabilitation exercises or go to an in-person appointment (x̅ = 2.47, P = 0.177), and display appointments (x̅ = 2.41, P = 0.189).
Mean (SD) preference ratings for system features accessible by patients and caregivers.
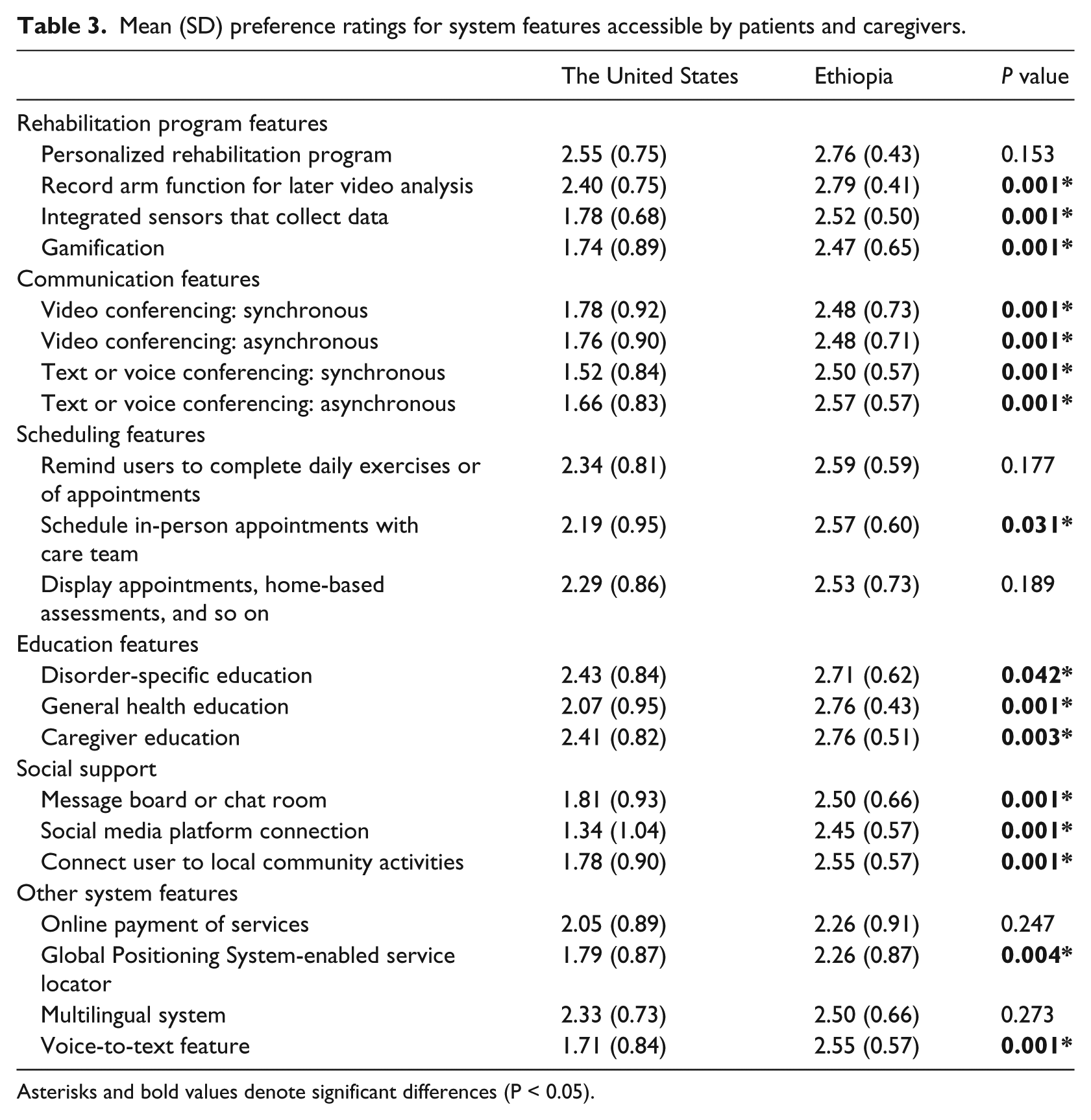
Asterisks and bold values denote significant differences (P < 0.05).
Group differences were observed for a number of design features accessible by patients and caregivers. While Ethiopian respondents stated that it was very to extremely important that a post-stroke upper limb rehabilitation system include features that allow for the recording of a patient’s arm movements for later video analysis by the rehabilitation team (x̅ difference = 0.39, P < 0.001), schedule in-person appointments with the care team (x̅ difference = 0.25, P < 0.001), and provide educational materials focused on stroke care (x̅ difference = 0.28, P = 0.042), general health (x̅ difference = 0.69, P < 0.001), and the caregiver (x̅ difference = 0.35, P = 0.003), US rehabilitation clinicians rated the above-mentioned features as very important.
Ethiopian respondents rated integrated sensors (x̅ difference = 0.74, P < 0.001), synchronous multimedia conferencing (x̅ difference = 0.98, P < 0.001), asynchronous multimedia conferencing (x̅ difference = 0.91, P < 0.001), message boards or chat room (x̅ difference = 0.69, P < 0.001), connection to local community activities that might be of interest to the patient (x̅ difference = 0.77, P < 0.001), and voice-to-text (x̅ difference = 0.84, P < 0.001) as very to extremely important, while US respondents rated them as somewhat to very important (i.e. rankings between 1.5 and 2.0). Ethiopians rated gamification (x̅ difference = 0.73, P < 0.001), synchronous video conferencing (x̅ difference = 0.70, P < 0.001), asynchronous video conferencing (x̅ difference = 0.72, P = 0.007), connection to social media platforms (x̅ difference = 1.11, P < 0.001), and GPS-enabled service locator (x̅ difference = 0.47, P = 0.004) as very important, while US respondents rated them as somewhat to very important.
Discussion
After a stroke, individuals are left with persistent upper limb impairments that require intensive and often daily rehabilitation therapy. Given that stroke treatment plans are developed by trained medical staff, this study surveyed rehabilitation clinicians to determine important design features for an mHealth-enabled app for personalized upper limb motor rehabilitation due to stroke, and to elucidate whether design feature preferences differed depending on the geographical location in which the respondents practiced.
We found that US and Ethiopian respondents have differing opinions about the importance of clinician–patient communication features. Overall, Ethiopian respondents rated video and multimedia conferencing to be necessary features in an mHealth rehabilitation system, regardless of whether the communication mode was synchronous or asynchronous. In contrast, US clinicians considered these communication features to be less important in a post-stroke mHealth system. This unexpected finding can be explained by understanding current rehabilitation therapy management practices in the United States. 33 , 34 For example, Chorzewski 34 reported that 27 percent of PTs see 15 or more patients in a workday (i.e. an 8-h shift) and that 55 percent of PTs regularly double-book patients. The high patient volume and productivity standards demanded of US rehabilitation clinicians may leave them feeling that they do not have the time to respond to tele-rehabilitation patient queries in addition to performing documentation and administration tasks, and meeting clinic billable productivity standards. While it might be tempting to design an upper limb motor rehabilitation app without clinician–patient communication features, this would undoubtedly reduce the degree to which the patient feels connected to their clinician and their confidence about their capabilities to recover, which in turn would lead to lower levels of patient motivation, program adherence, 35 satisfaction with care, and functional recovery. 34 In light of these findings, it is recommended that the mHealth rehabilitation app contain modules educating rehabilitation clinicians about the importance of rapport-building and therapeutic alliance development (regardless of physical location), as this will improve user engagement and satisfaction, as well as long-term sustainability of the mHealth project.
Our study also indicated that only Ethiopian rehabilitation clinicians felt that it was very to extremely important that a post-stroke upper limb rehabilitation app contain social support (e.g. message board or chat rooms, connections to social media platforms, connections to local community activities) and gamification features (e.g. badges, points and levels, challenges and quests). These group differences were of particular interest given the compelling evidence indicating that these features improve patient engagement and motivation, 36 and bolster post-stroke recovery of upper limb function. 37 , 38 While speculative, it is possible that Ethiopians rated social support features as more important than their US counterparts because approximately 80 percent of Ethiopians live in rural areas 39 far removed from easily accessible health care and other services. Because of these constraints, Ethiopians are more likely to develop and utilize support networks of friends and family, look to their communities for moral support and crisis management assistance, and create solutions developed by members of their community, 40 compared to the individuals in the United States who are more likely to utilize formal health care systems. 41 The high ratings given to gamification mechanisms provided by Ethiopian clinicians can be explained by understanding its economic, geographical, and cultural background. Ethiopia is the second largest country in sub-Saharan Africa and has one of the highest poverty rates in the world, with 33.5 percent of the population living below the international poverty line (US$1.90/day). 41 Around 80 to 85 percent of Ethiopians are engaged in subsistence agriculture, living on less than US$0.50 per day, 42 and focus their energies on growing enough food to feed themselves and their families. 43 , 44 Thus, when a family member has a stroke and cannot farm because of physical impairments, the resultant effect on the family unit and the community as a whole can be devastating. Rehabilitation clinicians practicing in Ethiopia are undoubtedly aware of the lifestyle of their patients, and how gamification features may enhance motivation and upper limb function recovery, as well as potentially facilitate an individual’s ability to return to work.
Responses from Ethiopia indicated that features giving general health education were considered of high priority, which is perhaps unsurprising in light of the significant increase in stroke prevalence and incidence across sub-Saharan Africa over the past four decades. 2 US respondents did not rate health education features quite as highly, which may be due to the decades-long and highly visible public health risk awareness campaigns extant in the United States 45 and the simultaneous decline in stroke prevalence throughout the United States. 2 However, we believe there are two reasons that general health education features should be included in a tele-rehabilitation app, regardless of the lower rating by US rehabilitation clinicians. First, stroke patients are likely to suffer from comorbid conditions (e.g. diabetes, hypertension), and a general health education feature would be able to provide important personalized resources to help manage these comorbidities while providing resources about stroke recovery. Second, stroke also impacts those who care for them (spouse, family, etc.); thus, providing health education resources targeted toward family members could provide a means to educate them on specific health issues they may themselves face, as well as helping to empower them to feel more confident in caring for the patient.
In addition to these main findings, results of this study indicated that voice-to-text features were rated more important by Ethiopian respondents, which is likely due to differences in literacy rates between the two countries. In Ethiopia, only 49 percent of adults are functionally literate, 46 compared to 86 percent in the United States.36,47 Ethiopian clinicians are accustomed to patients and/or caregivers being unable to read and write, and therefore understand that voice-to-text could be a helpful feature that enables these individuals to communicate quickly and easily with the rehabilitation team.
Compared to US respondents, Ethiopians also felt that integrated sensors that collect quantitative data about movement quality and strategy would be a very important feature and should be included in a stroke tele-rehabilitation app. This finding is congruent with other studies48,49 demonstrating that health care workers in low- and middle-income countries in sub-Saharan Africa have positive attitudes toward computer applications in health care and believe that computer technology could potentially improve patient care and simplify their work. Given the health care utilization barriers that individuals in sub-Saharan Africa face, it is likely that this population would greatly benefit from the development of an intelligent wearable sensor with tele-rehabilitation capabilities. The integration of an intelligent wearable sensor would provide rehabilitation clinicians with quantitative, yet easily understandable, information about upper limb movements, which would enable them to better diagnose the patient and develop patient-specific rehabilitation procedures. On the patient and caregiver side, intelligent wearable sensors would provide a means by which timely performance-based feedback can be provided to the patients, thus enhancing their interactive experiences and engagement. That said, the adoption and use of health technologies is not a simple process and is influenced by the information technology skills of the end user, the organizations’ capacity and readiness to implement and maintain the technology, as well as the usability and acceptability of the technology itself. 50 We believe that the long-term sustainability of technology-supported health care systems intended for use in sub-Saharan Africa (and other resource-constrained populations) can be improved if end users are involved in the design of the systems at an early stage in development. In doing so, barriers at the technology, user, organizational, and regulatory level can be identified. 51
As with all studies, this research had some limitations. First, although our sample of Ethiopian rehabilitation clinicians is large enough to be representative of the larger population of Ethiopian rehabilitation clinicians (n = 69, ~350 practicing rehabilitation clinicians), our sample of 75 US rehabilitation clinicians may not necessarily be reflective of the broader group of 210,900 practicing PTs 52 and 130,400 OTs 53 in the United States. That said, power analysis indicated that a total sample of 128 participants (64 in each group) would be needed to achieve 80 percent power at two-sided 5 percent significance level. A second limitation is that our sample reflects only the opinions of rehabilitation clinicians. Stroke patients and their caregivers may have different perceptions about the features that should be in an mHealth system for post-stroke upper limb rehabilitation. To address this limitation, we have collected usability data from stroke patients and caregivers from both the United States and Ethiopia,54,55 in which a medium fidelity prototype of the outREACH system developed based on the findings of the present study was tested. Last, we obtained information from potential users of the outREACH system via online survey. While this method enabled us to determine important information regarding the needs of the user population, there may be perspectives and experiences that were not captured during the survey. Moreover, we cannot rule out the possibility that cultural or national attitudes toward completing surveys may have influenced our results. As such, in future work, we will use multiple evaluative methods (e.g. moderated usability testing, focus groups) to get a more rich picture of how the outREACH system could be used, and glean greater insights into the cultural, technological, and organizational challenges that could affect implementation. Limitations notwithstanding, we believe that this study offers valuable empirical evidence regarding rehabilitation clinician’s preferences for design features to be included in a post-stroke upper limb rehabilitation system.
Conclusion
The feedback provided by rehabilitation clinicians in this study offer insights into the design features that should be included in a stroke tele-rehabilitation system and highlight the importance of engaging end users in the initial steps of mHealth development so that the system can be appropriately tailored to the geographical and cultural context of the end users. The findings of the present study will be used to inform the technical development of the outREACH system that will allow clinicians to provide rehabilitation services without in-person clinician-to-patient encounters, and care services for individuals who reside in geographically remote areas.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.