
Abstract
Church-based programs can act on multiple levels to improve dietary and physical activity behaviors among African Americans and Latinos. However, the effectiveness of these interventions may be limited due to challenges in reaching all congregants or influencing behavior outside of the church setting. To increase intervention impact, we sent mobile messages (text and email) in English or Spanish to congregants (n = 131) from predominantly African American or Latino churches participating in a multi-level, church-based program. To assess feasibility and acceptability, we collected feedback throughout the 4-month messaging intervention and conducted a process evaluation using the messaging platform. We found that the intervention was feasible to implement and acceptable to a racially ethnically diverse study sample with high obesity and overweight rates. While the process evaluation had some limitations (e.g. low response rate), we conclude that mobile messaging is a promising, feasible addition to church-based programs aiming to improve dietary and physical activity behaviors.
Introduction
Obesity increases the risk of many serious illnesses, including type 2 diabetes, hypertension, coronary artery disease, stroke, and certain cancers, 1 and is associated with mental health problems and reduced quality of life. 2 Obesity is highly prevalent across the United States, and certain subgroups, such as African Americans (AAs) and Latinos, are disproportionately affected. Among US adults, 43 percent of Latinos and 48 percent of AAs are obese compared to 33 percent of Whites and 11 percent of Asians. 3 Healthy eating and physical activity can help prevent and address obesity, although factors like genetics, mental health, and other health behaviors also contribute. 2 Dietary and physical activity behaviors are difficult to modify; therefore, multi-level interventions that implement strategies across various levels—for example, intrapersonal, interpersonal, community, and policy—are needed. 4
Faith-based organizations, such as churches, offer a unique opportunity for acting on multiple levels. Churches have a wide reach in AA and Latino communities and are trusted institutions that have historically intervened on social issues, particularly among AAs.5,6 Churches’ physical infrastructure, programs, and social networks can be leveraged to influence not only individuals but also the congregation and neighborhood. 7 Previous church-based interventions with AAs and Latinos have influenced eating and/or physical activity habits through educational approaches,8,9 changes to the food environment at church,10,11 on-site exercise get-togethers, 12 and neighborhood walkability assessments and advocacy. 13 However, such interventions have been limited by challenges with reaching participants for intervention activities and measurement. 14 Congregants’ busy schedules may limit their ability to attend in-person activities, 9 and long-term follow-up with participants can be difficult. 8 Furthermore, while the church environment is important, the home environment remains key, 7 suggesting a need to engage with congregants outside of the church setting.
Mobile messaging may strengthen church-based healthy living programs by engaging more frequently with more congregants. As a “push” technology that reaches participants during daily activities, mobile messaging allows for frequent and tailored communication at a low cost.15,16 Systematic reviews have found mobile messaging to be a promising approach for promoting healthy eating and physical activity.17,18 The majority of studies that employed mobile messaging in church settings, including three studies with AA populations,19–21 found that the approach was promising but required further research. One study reported that respondents did not want to participate in healthy living activities beyond the messages, 20 while the other suggested that messaging be used as part of a more comprehensive response to promoting healthy weight. 19 Another study successfully combined messaging with a structured diet and cooking classes implemented during the 40 days before Easter. 21 Thus, combining mobile messaging with other church-based activities may increase participants’ exposure to healthy living content, but it is unclear how acceptable this approach would be to congregants. Another study described the successful integration of a mobile messaging component into a multi-level, church-based program; however, the study focused on prostate cancer prevention. 22 To the best of our knowledge, there are no prior published articles that examine mobile messaging as part of a multi-level, faith-based program to impact dietary and physical activity behaviors.
This study explores the feasibility and acceptability of using mobile messaging technology to send healthy eating and active living messages to congregants from churches whose membership were predominantly (>80%) AA or Latino (herein described as AA churches and Latino churches) that participated in the pilot implementation of a multi-level, church-based intervention to address obesity. The overall intervention provided evidence of preliminary effectiveness in reducing weight gain, increasing weight loss, and improving diet quality among study participants. 23 Given the novelty of the mobile messaging component of this intervention, we undertook a process evaluation. Prior research suggests that mobile messaging is acceptable among AA15,22,24 and Latino populations, including monolingual Spanish speakers,25–27 as well as older adults.22,28 To our knowledge, this is the first multi-level, church-based intervention to use mobile messaging with both AA and Latino congregations, which presented the challenge of communicating in multiple languages and across cultural contexts.
Method
Community context and partnership
The study took place in Los Angeles County Service Planning Area (SPA) 6, which includes the neighborhoods of South Los Angeles, Lynwood, and Compton. These neighborhoods are characterized by worse health outcomes and greater socioeconomic disadvantage compared to other neighborhoods in the county. Approximately 68 percent of SPA 6 residents are Latino and 28 percent are AA.29,30
The multi-level intervention was developed through a community-based participatory research initiative led by the RAND Corporation (a non-profit research organization), Los Angeles Metropolitan Churches (LAM; a faith-based advocacy organization), and a Community Steering Committee comprising AA and Latino faith leaders and public health organizations in South Los Angeles. 31 Through an extensive community outreach process, which included an innovative consensus-building process called ExpertLens, 32 public health and faith leaders identified community health priorities and selected obesity as the priority health issue. RAND, LAM, and other community partners designed a multi-level, church-based intervention called Eat, Pray, Move (EPM), which included a mobile messaging component. Intervention and evaluation activities were approved by RAND’s Human Subjects Protection Committee.
Intervention description
The overall EPM intervention aimed to influence dietary and physical activity behaviors through multiple strategies, including sermons, educational material, church produce gardens, cooking and nutrition classes, local food and physical activity mapping and advocacy activities, and ultimately, congregational policy changes that would create a healthier environment at the church. A mobile messaging component was included based on community partner input and the fact that few church-based interventions had incorporated this recent innovation.
Content
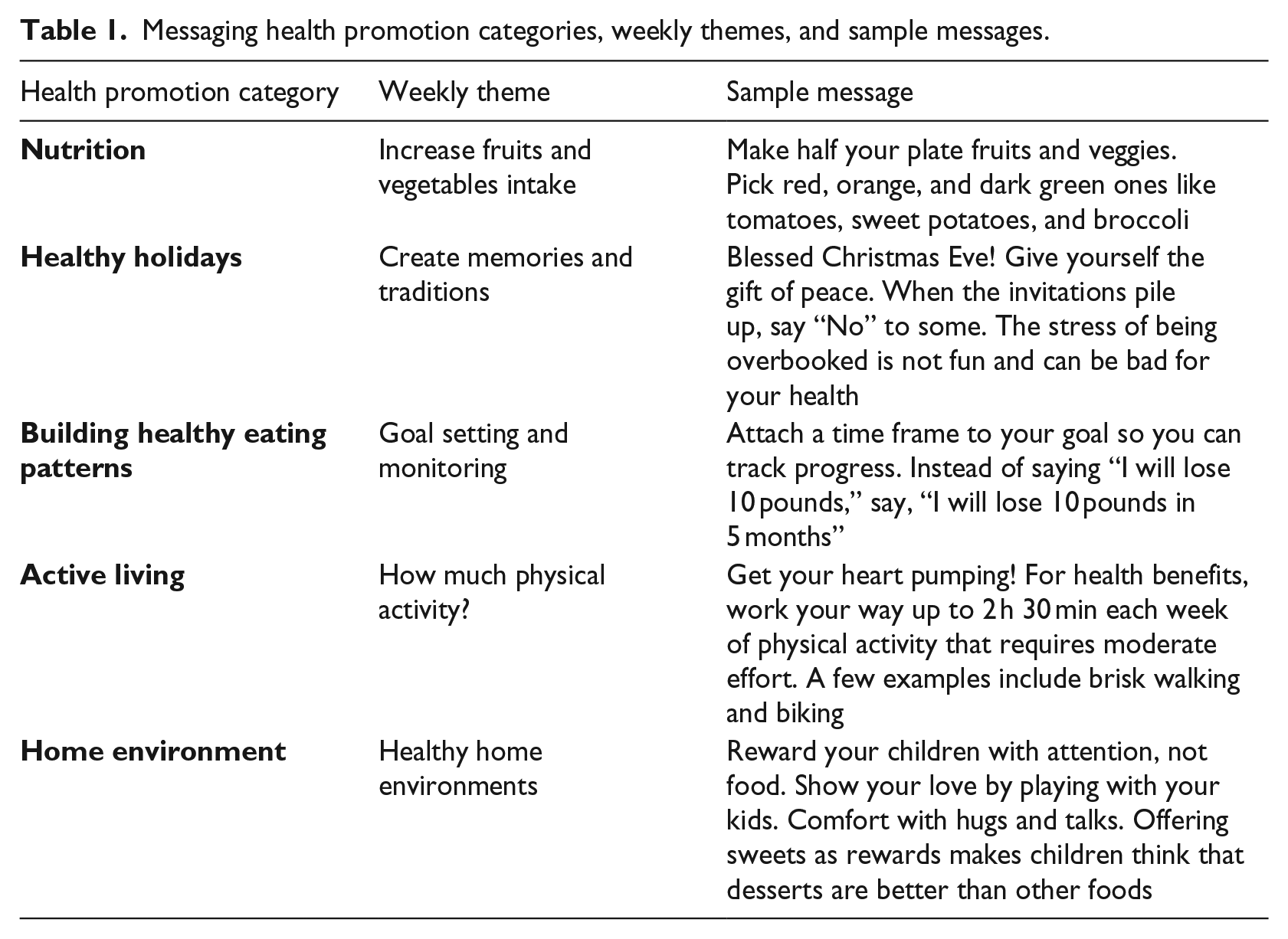
Message content mapped to five healthy eating and physical activity categories, each with weekly health promotion behavior themes linked to other intervention components (i.e. handouts, cooking and exercise classes). Specific themes and corresponding messages were drawn and developed from publicly available resources,33,34 given the advantages to using existing, pre-tested messaging content. 35 Certain messages were tailored for holidays (e.g. Thanksgiving) that occurred during the intervention period. Some messages used spiritual language and others encouraged family- and community-based activities, in line with previous studies that encourage tailoring messages to a specific setting and audience. 22 Messages provided helpful, actionable suggestions rather than simple facts 36 and used positive, non-judgmental language and communicated respect for community traditions. 37 Daily messages were a maximum of 200 characters to facilitate transmission on basic cell phones. Table 1 includes the messaging categories and sample weekly health promotion themes and messages.
Messaging health promotion categories, weekly themes, and sample messages.
The mobile messaging platform can also be used to bolster involvement in other activities. 22 Thus, we also sent church-specific reminders about other EPM intervention activities. Communication with participants was mostly unidirectional, except for an initial request asking participants to confirm receipt and occasional (unsolicited) feedback and questions from participants.
Modality and language
Study participants opted to receive messages via text or email. While text has been used most frequently for mobile messaging health interventions, 38 email has also been employed 39 and may be preferred by some people. 40 Our participants chose to receive messages in English or Spanish, similar to other bilingual interventions.26,27 The few messages that were not already available in Spanish were translated by a native Spanish-speaking team member and reviewed by three other bilingual team members.
Frequency and timing
Since mobile health messaging has been shown more effective with greater frequency over a longer period of time,28,41 we sent a daily message over a 4-month period, for a total of 119 messages. Messages were sent at 9 am so participants could read them throughout the day. 22
Recruitment
We enrolled participants in the messaging component during baseline data collection at each church to reduce sign-up burden on participants. 42 Requiring people to opt-in later has been shown to hinder recruitment of participants from lower socioeconomic groups.24,43 Contact information was collected from the consent forms after participants verbally consented to participate in the messaging component.
Messaging platform
We sent messages using a secure cloud-based platform that could send both email and text messages and manage multiple contact lists, such as a list of all English-speaking or Spanish-speaking participants and lists specific to each church for event reminders. Incoming messages from participants could be viewed and answered within the platform by research staff but were not accessible to other participants.
Process evaluation analysis
Two AA Protestant churches and one Latino Catholic church participated in the intervention. A total of 156 adults from these three intervention churches enrolled in the study, which included baseline and follow-up surveys and biometric screenings, and were eligible to participate in the mobile messaging component.
Demographic and health characteristics for the messaging intervention sample came from the study’s baseline and follow-up surveys. The research team tracked spontaneous feedback and opt-out requests from participants throughout the intervention. After the messaging intervention was complete, process evaluation questions were administered via text and email to assess participant satisfaction. Bivariate analyses were conducted on the six multiple-choice survey items. Frequencies were calculated and stratified by messaging modality, church type, and language preference. To determine whether there were significant differences in responses to the six items by message modality (text vs email), language (English vs Spanish), and church type (predominately Latino vs AA), we used Fisher’s exact test of independence. Because we conducted 18 tests, we applied the Holm–Bonferroni sequential correction for multiple comparisons. Quantitative analysis was conducted in Stata 15. 44
Open-ended questions followed each multiple-choice item to encourage participants to expand on their answers. Responses were analyzed using a combination of identifying relevant constructs related to health behavior theory a priori and an inductive approach that involved reviewing responses and composing a list of emergent themes. 45 Qualitative analysts coded the responses and calculated frequencies of the themes.
Evaluation framework
Many health behavior theories have been used as the basis for evaluating mobile messaging interventions.46,47 We selected the Health Belief Model, which focuses on the perceived susceptibility and severity of an illness, as well as the perceived benefits of, barriers to, and self-efficacy for changing health behaviors. Sociodemographic and other variables can moderate these beliefs, and cues to action are necessary to trigger behaviors. 48 Several studies have used the Health Belief Model and mobile messaging to change a variety of health behaviors;49–52 however, there is a need to better understand how the theory’s constructs align with the mechanisms of a mobile messaging intervention.41,47
Results
Over 15,500 healthy eating and active living messages were sent during the 4-month messaging intervention period, excluding event announcements (e.g. cooking class reminders).
Enrollment and participation rates
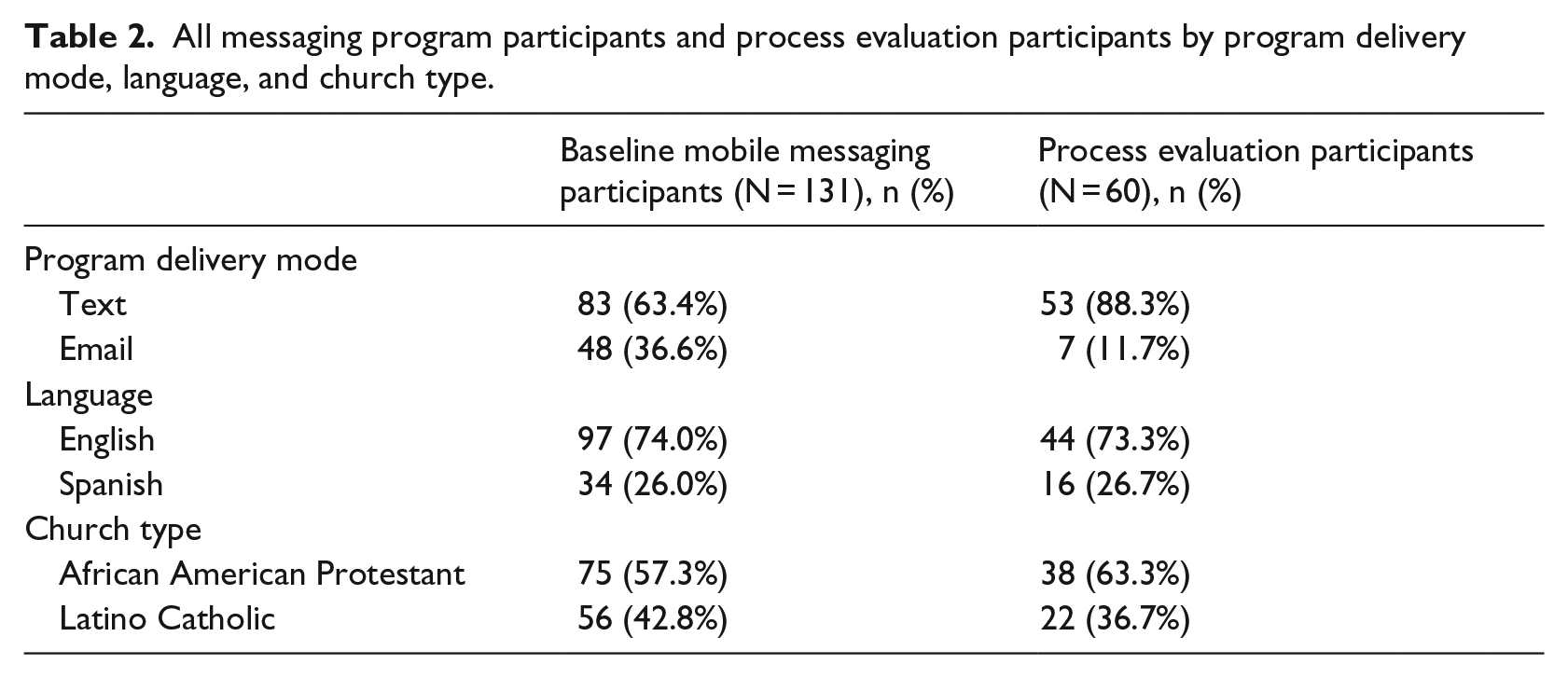
At baseline, 131 (84.0%) of study participants at the three intervention churches (87.2% at the AA churches and 80.0% at the Latino church) agreed to participate in the messaging component and provided contact information. Table 2 shows program delivery mode, language, and church type for two groups of messaging participants (the total enrolled at baseline and the total that participated in post-implementation process evaluation). Most messaging participants preferred to receive messages via text (63.4%) instead of email (36.6%) and in English (74.0%) rather than Spanish (26.0%). During the 4-month implementation period, six people (4.5% of the total that enrolled) opted out of the messaging component. Of the 125 participants completing the messaging intervention, 60 (48%) responded to at least one process evaluation question. In addition, 14 people responded spontaneously during the intervention; some responses were brief (e.g. “Okay”), whereas others were more substantive (e.g. “Yeah you are right thanks I am drinking more water and eating more fruits”).
All messaging program participants and process evaluation participants by program delivery mode, language, and church type.
Participant sociodemographic and health characteristics
Overall, most messaging participants were over 50 years and female. Socioeconomic status varied across church type; 90 percent of AA church participants had at least some post-high school education compared to only 38 percent of Latino participants. Fewer than 5 percent of AA church participants were born outside of the United States compared to over 70 percent at the Latino church.
At the Latino church, 33 percent of participants reported having no health insurance, compared to only 6 percent at the AA churches. Overall, about two-thirds of participants (68.0%) reported excellent, very good, or good health status. More respondents at the Latino church reported fair or poor health (37.8%) than at the AA church (27.6%). According to biometric measures, over half of all participants were obese (body mass index (BMI) > 30.0), and an additional 30 percent were overweight (BMI: 25.0–29.9). Self-reports of previously diagnosed heart disease, hypertension, diabetes, and high cholesterol were higher among participants from AA churches than the Latino church. The majority of study participants were non-smokers. Table 3 shows sociodemographic and health characteristics for the participants.
Sociodemographic and baseline health characteristics of study participants.
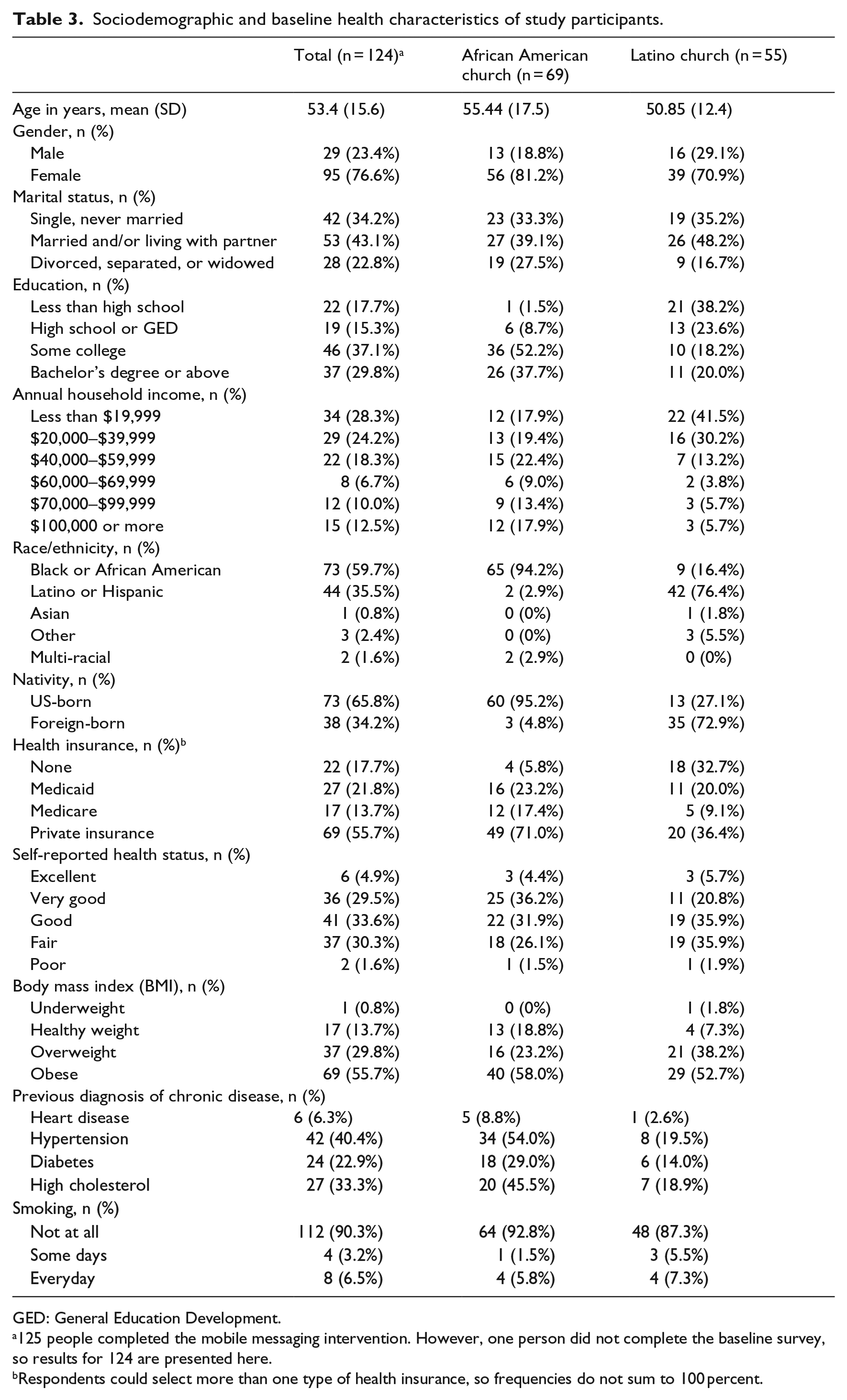
GED: General Education Development.
125 people completed the mobile messaging intervention. However, one person did not complete the baseline survey, so results for 124 are presented here.
Respondents could select more than one type of health insurance, so frequencies do not sum to 100 percent.
Logistical and technological barriers to implementation
Initially, it was difficult to decipher some handwritten email addresses and phone numbers from consent forms; this may have contributed to erroneous contact information. We also encountered some technological challenges. For instance, occasionally text messages arrived scrambled because of the way that standard mobile phone software handled Spanish language characters such as accents. Furthermore, due to limitations in the underlying technology, it was not feasible to confirm if the text messages were received by participants. We were only able to conservatively estimate the number of participants who viewed messages based on whether they responded to us or opened an email or attachment. We confirmed that 86 participants, or 65 percent of the 131 participants included initially, received and viewed at least one message.
Process evaluation results
Process evaluation item-level response rates ranged between 21 and 33 percent for close-ended process evaluation questions. Furthermore, 35 percent provided valid open-ended responses to at least one question. Table 4 shows the responses to close-ended questions by messaging mode, participant language preference, and church type. There were no statistically significant differences in the responses to the six items based on message mode, language, or church type. The results are summarized by theme below with exemplary quotes from respondents. The percentages reported use the total number of respondents for that particular item as a denominator. All respondents quoted received messages via text message unless email is noted.
Responses to close-ended process evaluation questions.
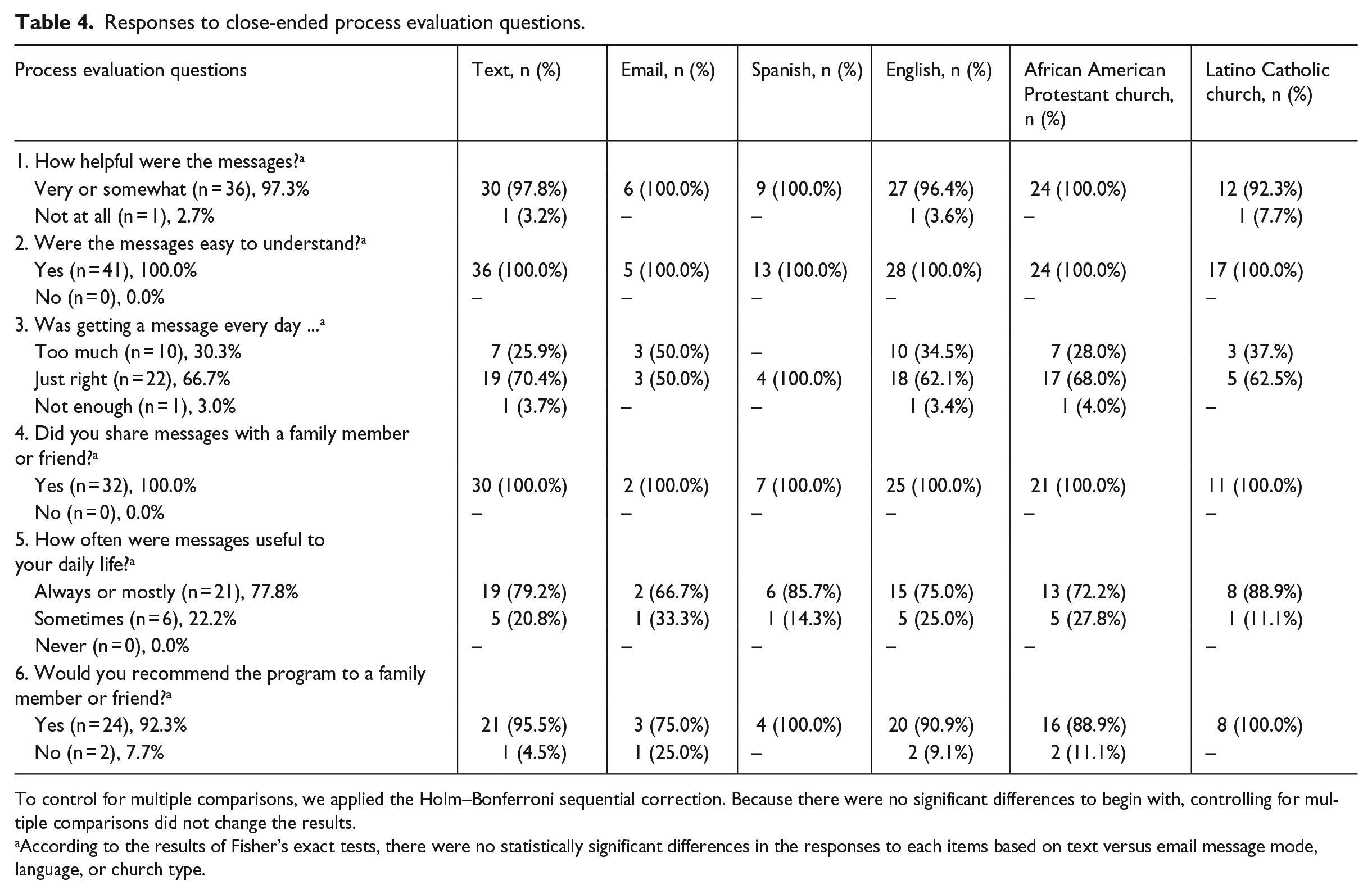
To control for multiple comparisons, we applied the Holm–Bonferroni sequential correction. Because there were no significant differences to begin with, controlling for multiple comparisons did not change the results.
According to the results of Fisher’s exact tests, there were no statistically significant differences in the responses to each items based on text versus email message mode, language, or church type.
Additional themes arose from the open-ended responses, including some that mapped to the Health Belief Model (positive cues to action, helped address barriers to healthy living, promoted self-efficacy, encouraged healthy behaviors, and reinforced existing knowledge). These findings are detailed below.
Message helpfulness
A total of 37 participants (29.6%) responded to the question assessing perceived helpfulness of the messages. A clear majority of respondents (97.3%) said that the messages were either very or somewhat helpful. A 54-year-old woman from an AA church conveyed what she found useful, saying, “it was healthy and helpful information to share that would benefit the health and well-being of my family members and friends.” A total of 11 people said that the messages were useful since they were generally informative—for example, “helped me to be mindful of the types of food I was eating,” (60-year-old woman, Latino church). Only one respondent (Latino church) reported that the messages were not at all helpful.
In terms of how the messages influenced health behavior, six people said that the messages were useful because they helped them address perceived barriers to healthy living. A 65-year-old woman (AA church) commented, “it allowed me to see what I can do differently with my cooking to still have flavor but be healthier for me in the long run.”
Messages as positive cues to action
A dozen participants indicated that the healthy living messages served as a cue to engage in healthy behaviors. A 57-year-old woman (AA church) commented, “the messages were always coming and it allowed me to think twice about a snack or taking a 4 hr nap when I could be doing something better for my health.” Six respondents said they had changed a particular behavior due to the messages.
Comprehensibility
Everyone who responded to the comprehensibility item (n = 41) said that the messages were easy to understand, indicating a high level of comprehensibility from English- and Spanish-speaking participants. A 66-year-old man (AA church) said the messages were “explained clearly,” and a 45-year-old female Spanish-speaking participant said the messages were easy to understand and implement in her daily life.
Frequency
Most respondents (n = 22 or 66.7%) replied that daily messages were “just right,” while 10 respondents (30.3%) said they were excessive. A 57-year-old man (AA church) stated that the messages were “not overbearing. Perfect! No one wants to be texted every minute of the day lol.” In contrast, one woman (AA church) said the messages were too frequent and bothered her while she was in class.
Content relevance
Most respondents (n = 21 or 77.8%) said that the messages were always or mostly useful to their daily life. Remaining respondents said that messages were sometimes useful. A Spanish-speaking 53-year-old man said the messages specifically motivated him to eat more vegetables. Similarly, a 57-year-old woman (AA church) commented, “the messages helped me a lot when it came to cooking at home, watching TV while snacking, and exercising.”
Seven participants commented that information in the messages was not novel, although this was not necessarily portrayed as a negative. For instance, a 67-year-old female email recipient (AA church) commented, “Some of the information I already knew—I’m glad to know I’m doing it right.”
In their open responses, 18 participants commented most on diet-related messages compared to messages about cooking or physical activity. A 67-year-old female email participant from an AA church described, “I’m making eating healthier my goal.”
Message sharing and program recommendation
The 32 respondents to this item reported sharing at least one message with another person. In total, 16 people elaborated, such as a 48-year-old Spanish-speaking woman who liked being able to either forward a text or verbally share the information. Moreover, 24 respondents (92.3%) said they would recommend the program to a family member or friend. Only two respondents said they would not recommend it.
Self-efficacy, encouragement, and reinforcement
Five people responded that the messages increased their self-efficacy. For instance, a 39-year-old Spanish-speaking woman stated, “I learned how to cook and how to eat healthy.” Relatedly, eight people described the messages as encouraging. A 29-year-old male from an AA church mentioned, “it doesn’t come across as nagging,” while a 63-year-old Spanish-speaking woman said the messages were motivating.
Discussion
Overall, we found this messaging intervention feasible to implement and acceptable to churchgoing AAs and Latinos with high rates of obesity and chronic diseases. Using process evaluation, we identified various ways in which the messages impacted participants’ health behaviors and decision-making. Furthermore, this study provides new insights about employing mobile messaging, such as enrollment, retention, message content, participant satisfaction, and alignment with health behavior theory.
Potential to reach underserved populations
We recruited participants and delivered healthy living messages within a multi-level, church-based intervention and demonstrated the acceptability of this intervention among a population that is underrepresented in health research. 53 While previous studies have conducted messaging interventions with AA15,22 or Latino populations,24–26 we are not aware of any previous mobile messaging interventions that served members of both communities through a single, faith-based program. Our process evaluation showed high acceptability in AA and Latino churches, and there were no significant differences in responses to multiple-choice items across the two church types. Moreover, our study sample comprised predominately older (average age: 53 years), mostly female (76.6%) AAs and Latinos. While one study suggested older churchgoing AAs would not be receptive to health information transmitted electronically, 54 our study found high satisfaction with a mobile messaging intervention across the entire sample, including among older adults. In addition, these study participants reported, with the exception of smoking, relatively high rates of cardiovascular risk factors. 55 The majority of Latino study participants (72.9%) were foreign-born, and a third reported having no health insurance (32.7%). Chronic diseases are more likely to go undiagnosed among recent Mexican immigrants compared to the US-born, 56 and among individuals without health insurance. 57 These factors indicate even greater health risk than what we observed.
Over a quarter (26.0%) of all participants opted to receive messages in Spanish. Satisfaction rates were high among both Spanish and English speakers, indicating that mobile messaging may be an effective approach for engaging with foreign-born Latinos, who may experience language and trust barriers that limit their participation in research studies. 58
Our recruitment practices incorporated lessons learned from prior studies to increase the study’s reach. For instance, by enrolling participants on-site, we were able to avoid low or biased enrollment. 24 Over a third of participants chose email, which might have reduced barriers to participation among participants concerned about wireless charges or who considered text messages too intrusive. 40
High acceptability and satisfaction with daily health promotion messaging
The process evaluation results demonstrated that respondents considered the messages helpful and encouraging. Many said that they would recommend the program to a friend, which is an indication of satisfaction, 59 and the frequency of messages (daily) was generally acceptable. These positive responses were consistent across the email and text modalities, for both Spanish and English speakers, and for participants from AA as well as Latino churches. More respondents mentioned an impact on their eating habits than on physical activity. This may reflect that a stronger dosage of messages had greater impact, 41 as 8 of the 17 weeks specifically targeted healthy eating, and only 4 weeks focused on physical activity (the other 5 weeks covered a mix of topics).
Prior health promotion mobile messaging studies have sent messages at a variety of frequencies, including daily for 1 month, 60 thrice daily for 12 weeks, 25 or four messages weekly for 6 months. 61 Greater frequency and longer intervention are considered more effective for behavior change.28,41 We found that delivering daily messages for 4 months was feasible and acceptable to most participants. As nearly one-third (30.3%) of the sample thought daily messages were excessive, future interventions may consider offering varying levels of frequency.
Drop-out rates are another indication of participant satisfaction. 59 Drop-out has tended to be low for mobile messaging interventions; 62 for instance, a study that augmented weight loss workshops with text messages experienced 16 percent drop-out. 63 Similarly, this study’s 4.5 percent drop-out rate was low. This may reflect the relatively passive nature of our intervention, as participants could have stopped reviewing the messages without requesting to drop-out. Other factors may include use of positive, encouraging messages. Prior research found that participants preferred such content,37,64 and our participants confirmed this in their feedback. Moreover, because this mobile messaging program was integrated into a larger church-based intervention, which itself was developed using a community-based participatory process, participants may have felt more connected to the intervention and its goals. Our findings align with church-based prostate cancer programming where less than 2 percent of participants requested to stop receiving text messages. 22
Limitations
A limitation of this study, like some other mobile messaging studies,22,65 was that the underlying technology made the intervention more passive and made it difficult to confirm how many respondents viewed the messages, thus impeding our understanding of the intervention’s reach. It is also possible that some messages were not received due to erroneous contact information or unknown technical glitches. Relying on handwritten contact information from participants also contributed to initial legibility issues. Future studies should consider having participants write contact information twice and/or enter it directly into an electronic database.
Another limitation was a low response rate to the process evaluation questions. Fewer than half of the mobile messaging participants responded to any process evaluation questions, and the per-item response rate was never more than 33 percent. It is possible that some participants became accustomed to passively receiving messages and did not feel the need to respond. Regardless, a low response rate may imply biased responses, depending on the reasons for non-response, 66 and this limits the interpretability of our findings. The brevity of text messages may have also limited the ability of some respondents to describe their experiences. Close-ended questions related to Health Belief Model constructs may have been more informative than open-ended questions in elucidating how well that theory explains participants’ experiences. Furthermore, while mobile modalities are increasingly used for data collection due to their convenience and relative accuracy compared to traditional approaches,67–70 future process evaluations might consider in-person or phone interviews to increase response rates and/or allow for richer open-ended responses.
Recommendations for future research and practice
Future interventions might enhance mobile messaging effectiveness through various approaches. First, while our messages were sometimes tailored to the church, they were rarely personalized for individuals. Personalizing messages to an individual’s baseline health behaviors—for instance, not sending messages about soda consumption to participants who report not drinking soda—could make the content more relevant. 61 In addition, participants could draft their own motivational messages and/or choose which messages they want to receive.15,25 While we responded to messages from respondents who contacted us, our intervention primarily used one-way communication; future interventions should consider encouraging bidirectional communication to foster greater engagement. 28 Moreover, future interventions could consider additional technology, for example, wearable devices such as pedometers, to enable remote monitoring and feedback. 71
The process evaluation response rate was considerably lower among email recipients than text recipients, confirming prior findings that in dual-modality messaging interventions, email participants were less engaged. 40 We did not find evidence that the text message participants considered the intervention more intrusive than email participants. Future interventions may consider using text messages as a default and offer email only to those who explicitly decline texts.
Future studies should continue testing which behavior theories best align with the effects of mobile messaging. 46 We found that the Health Belief Model’s cue to action construct was useful in explaining how this intervention influenced participants’ eating, cooking, and physical activity behaviors. There was little evidence for other Health Belief Model constructs, potentially because the process evaluation did not include explicit questions about them.
Conclusion
This study presents new approaches to participant recruitment and message content and describes participant responses to a church-based mobile messaging program. We provide evidence that the intervention was acceptable to attendees of AA Protestant churches and Latino Catholic churches, including monolingual Spanish speakers and older adults. We conclude that mobile messaging can be integrated into a multi-level church-based healthy living intervention with sociodemographically diverse participants.
Footnotes
Acknowledgements
The authors wish to thank Vish Chatterji and Edward Skolarus for their support in configuring their message platform OpenVersa to send our daily messages. They are also grateful to the study’s Community Steering Committee, especially Rev. Michael A. Mata and Rev. Dr. Clyde W. Oden, who provided excellent guidance and counsel throughout the study. Finally, they acknowledge Rachana Seelam at RAND, who provided programming assistance; Beth Ann Griffin, who provided guidance regarding our statistical analysis; and Dominic Lathos of the Episcopal Urban Intern Program, who helped implement the process evaluation and code interviews.
Declaring of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was supported by the National Institute of Minority Health and Health Disparities (grant no. R24MD007943, K.P.D.); Dr D.D.P. was supported by the Agency for Healthcare Research and Quality (grant no. T32HS00046). The contents of this article are solely the responsibility of the authors and do not represent the official views of NIMHD or AHRQ.